
Abstract
Background
Follow-up calls in the oncology setting are frequently used to augment care and encourage oral antineoplastic adherence. However, limited data are available on patient populations that would benefit from this intervention versus populations that may require alternative interventions. The purpose of this study was to identify characteristics among patients on oral antineoplastic agents that influence their likelihood to respond to follow-up calls.
Methods
Patients receiving care from one of the eight community oncology clinics within the same branch were analyzed. Patients were included if they were ≥18 years, received a new oral antineoplastic agent that was electronically prescribed between August 2018–October 2018, and picked up their first fill from their pharmacy of choice. Patients received up to six follow-up calls after picking up their first prescription. Calls were categorized as adherent (≥3 monthly interactions) or non-adherent (<3 monthly interactions). Logistic regression models were used to evaluate factors associated with follow-up call adherence. Factors included demographics, cancer stage, marital status, employment, pharmacy setting (internal pharmacy versus external pharmacy), and insurance used by the patient. Descriptive analysis was performed to analyze response rates, cancer diagnosis, and to determine the best time and day patients responded to follow-up calls.
Results
Data from 125 patients were analyzed, of which 65 patients (52%) were adherent to follow-up calls and the mean response rate over six months was 45% (range: 35% -- 54%). High success rates for follow-up calls were seen between 12–3 pm and on Tuesdays and Thursdays. After adjusting for covariates, patients with stage III-IV were 89% less likely to respond to follow-up calls compared to those with stage 0-II (95% CI: 0.02–0.64; p = 0.01), patients with commercial insurance were 79% less likely to adhere to follow-up calls compared to those on government insurance (95% CI: 0.06-0.71; p = 0.01), and patients using an external pharmacy had a 2.8 times increase odds of being adherent (95% CI 0.98-8.34; p = 0.05). All other factors were not significant.
Conclusions
For patients taking oral antineoplastics, non-adherence to follow-up calls was observed in more than 45% of patients receiving care from a community oncology clinic. Findings demonstrated that those with advanced stages of cancer, on commercial insurance, and going to an internal pharmacy were at higher risk for not adhering to follow up calls. Therefore, alternative methods for managing adherence and side effects in these populations are warranted.
Keywords
Introduction
Oral antineoplastics are increasingly being used in the long-term care of cancer patients and also provides a non-invasive route for patients to self-administer at the convenience of their home. 1-3 In addition, another benefit when compared to parenteral infusions, is the decreased cost associated with health care resources for inpatient and ambulatory patient care services.2 However, those on oral chemotherapy regimens present a unique challenge relative to those on traditional infusion chemotherapy, such as adherence and unique toxicities that have the potential to go unreported. 1,4,5 One of the difficulties with oral chemotherapy is that patients tend to decrease or skip a dose when the medication is making them feel ill. Therefore, frequent communication and monitoring are required to ensure patient safety. Follow-up phone calls can offer a solution to these challenges and are a useful way to support appropriate medication management among cancer patients. These calls provide a convenient way to track and assist patients with their medications after clinical visits—when complexities of oncology regimens may arise. In general, follow-up phone calls have been associated with reduced hospital readmissions, increased medication adherence, better health-related quality of life, and improvements in patient knowledge and health-related behaviors.6–8
A single-center study found that adverse events led to 48% of patients self-discontinuing their medications without physician’s consent. When follow-up calls were made as part of this cancer center’s quality initiative to teach patients self-management of their oral chemotherapy, results showed that none of the patients who received follow-up calls discontinued medications on their own, and 17% received physician-directed dose reductions due to adverse events reported during the follow-up calls. 9 In addition, a randomized controlled study examined the impact of a follow-up phone call intervention given by a pharmacist at 72 hours, and at two weeks after hospital discharge. Patients were asked questions about adverse events and appropriate use of their medication. Results from follow-up calls revealed that 10% of patients had questions about their medications, 5% were unsure about how to use their medications, and the pharmacist identified medication-related adverse effects for 20% of the intervention patients. 10 These studies demonstrated the benefits and positive impact of follow-up calls improving patient safety.
Harnessing the benefits of follow-up calls in real-world settings depends on a variety of factors. One key factor for optimal outcomes to follow-up calls is patient responsiveness. Understanding key drivers behind patient responsiveness to follow-up calls will help to optimize these interventions. However, research characterizing responders versus non-responders to follow-up calls in patients receiving oral antineoplastics is lacking. By evaluating trends in characteristics of patients who do not respond to follow-up calls versus those that do, program interventions can be tailored to the patient groups where they provide the most value. Just as medication regimens are selected based on the individual patient, interventions supporting patients to manage their regimens must be tailored according to the type of assistance the patient will most likely benefit from. Previous literature has suggested that tailoring interventions according to patient characteristics may help improve outcomes as well as healthcare resource utilization.11–14
The primary objective of this study was to identify characteristics among patients on oral antineoplastic agents that influence their likelihood to respond to follow-up calls. The secondary objective was to identify response rates and patterns of successful call attempts such as best time and day of the week to conduct follow-up calls.
Methods
Cohort selection
Patients receiving care from one of the eight community oncology clinics in the Fort Worth region and surrounding counties were prospectively identified for this study through electronic medical records. Patients ≥18 were included if they were electronically prescribed a new oral antineoplastic agent between August 2018 to October 2018 and fluent English speakers. In addition, patients had to receive at least one fill from their pharmacy. Patients were excluded if they were enrolled in a clinical trial, did not pick up their first fill from a pharmacy, received a printed copy of their prescription, or relocated to another facility prior to filling their first fill. The study protocol was approved by the University of North Texas Health Science Center Institutional Review Board (IRB # 1398288-5). Due to follow-up calls being a standard of practice at our clinic, patient consent was not required.
Follow-up call procedure
Our study prospectively documented follow-up calls for patients receiving oral antineoplastics. Each patient was enrolled to receive up to six follow-up calls during a six-month time period (i.e., one follow-up call questionnaire per month). Patients were called Monday through Friday between 8am to 5 pm and Saturday from 10 am to 2 pm. Each month, a maximum of three phone call attempts were made. The first call was made on days 1–7. Calls two and three were made on days 7–15 of the month. After the first successful attempt, callers used the same successful attempt to guide future attempts for the following months. During the first successful attempt, if patients stated that “it was not a great time to talk”, callers asked for the best time and day to call the patient back. During each month, if the first call was unsuccessful, additional attempts were made on different days at different times to increase the success of phone calls. Voicemails were not left for any patients. However, because patients received health care services from the community oncology clinic, they were familiar with the associated phone number. In addition, notes were added to the patient’s profile to indicate a follow-up call was made. This allowed patients to get routed back to the right location to complete their follow-up call if they were to call back. During the follow-up calls, patients were asked about medication adherence, side effects, starting new medications (including over-the-counter medications and vitamins), and ER visits. If patients were no longer taking oral antineoplastics, patients were then asked about the reason for discontinuation, and proper disposal.
Characteristics analyzed
The following variables were evaluated to identify characteristics associated with adherence to follow-up calls: age, sex, race (non-Hispanic White, non-Hispanic Black, Hispanic, Asian, or unknown); cancer type (classified into breast, hematological, genitourinary/gynecological, gastrointestinal, brain, and non-small cell lung cancer); insurance type (government or commercial); employment status (employed or unemployed), and marital status (married or not married). Staging was defined by stage 0-II, III-IV, unknown, or other, which pertained to hematological malignancies and brain tumors due to a different staging/grading system. Lastly, we also included pharmacy setting, defined as internal or external pharmacy. The community oncology clinic had an integrated specialty pharmacy within the main branch, also known as medically integrated pharmacies (MIPs). This provided a convenient avenue for patients to pick up their medications within the same facility where they received care. This type of pharmacy was defined as internal pharmacy. If patients received their oral antineoplastic outside of the community oncology practice, this was defined as an external pharmacy. External pharmacies include retail, mail order, or independent pharmacies.
Study measures: Follow-up call adherence
All patients that met the inclusion criteria were included in the analysis. Patients who answered less than three of the six follow-up calls were classified as non-adherent. Patients who answered three or more of the six follow-up calls were classified as adherent.
Response rates were captured by averaging the successful calls by the total number of patients called per month over a six month duration. In addition, patterns of successful call attempts were analyzed by capturing times and days of the week for each successful call and using the highest frequencies to determine success.
Statistical analysis
All statistical analyses were conducted using SAS 9.4. Statistical significance was assessed with two-tailed tests and α = 0.05. Exploratory data analyses with the variables of interest were conducted, including multivariable logistic regression models to identify characteristics associated with adherence to follow up calls. Due to a large number of race/ethnicity missing from the data (n = 18), we conducted two multivariable models, one including all factors, and one only excluding race. In addition, five subjects were missing cancer staging and therefore were excluded from the both regression models. However, these patients were included in the descriptive analysis to determine response rates, and best time and day to call. Odds ratios were calculated for patient characteristics associated with adherence to follow-up calls. All data were reported as the odds ratio (OR), 95% confidence interval (CI), and associated p-value for the specific characteristic. We calculated the mean and standard deviation (SD) for continuous variables, and for categorical variables, we obtained the frequencies.
Results
Of the 143 patients identified, 18 were excluded from the study due to various reasons, including the doctor terminating the prescription prior to the patient picking it up (n = 2); prescriptions were not electronically prescribed, so the patient’s prescription could not be tracked (n=3); the patient passed away prior to the follow-up call (n=3); the patient relocated to another facility (n=2); the patient’s doctor did not fill out the prior authorization (n=1); the patient did not speak English (n=1); or the patient started their medication prior to August 2018 (n=6). Therefore, the cohort analysis included 125 patients.
Patient characteristics
Of the 125 patients analyzed in the study, the mean age was 63 (SD ±12.1). The majority of patients were female (n=98, 78.4%), non-Hispanic White (n = 77, 61.7%), married (86, 68.8%), and unemployed (n=70, 56%). Most patients were diagnosed with breast cancer (n = 84, 67.2%), while hematological (n = 14, 11.2%), genitourinary/gynecological (n = 5, 4.0%), gastrointestinal (n = 15, 12%), brain (n = 6, 4.8%) and non-small cell lung cancer (NSCLC, n = 1, 0.8%) were also represented. The majority of patients had stage 0–II cancers (n = 75, 60%), while 32 patients had stage III–IV (25.6%), 13 were other (10.4%), and 5 were unknown (4%). Most patients used external pharmacies (n = 79, 63.2%) and had insurance provided by the government (n = 38, 30.4%) versus commercially provided (n = 87, 69.6%). (Table 2)
Overall adherence to follow-up calls
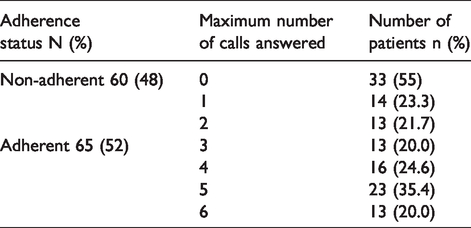
Of the 125 patients, the mean response rate from month one through month six was 45% (range: 35% -- 54%). Adherence to follow-up calls was observed in 65 patients (52%), answering three or more of the six calls made, and 60 patients (48%) were classified as non-adherent to follow-up calls, answering fewer than three of the six calls made. Of the 60 non-adherent patients, 33 (55%) did not answer any calls (Table 1). However, 92 (73.6%) patients answered at least one follow-up call which trended down to 10.4% completing six follow-up calls.
Maximum number of completed calls by adherence status for patients on oral antineoplastics.
Characteristics associated with adherence to follow-up calls
The odds of a successful follow-up call were calculated based on two different multivariable regression models, one including all characteristics and one only excluding race. For the model excluding race, after adjusting for other covariates, factors associated with follow up call adherence were: cancer stage (OR = 0.11, 95% CI: 0.02–0.64); p = 0.01) and insurance type (OR = 0.34, 95% CI 0.13–0.90; p = 0.03) (Table 2). This means that patients with cancer stage noted as “III-IV” had 89% decreased odds of adhering to follow-up calls compared to cancer stage noted as “0-II”. Similarly, patients with commercial insurance had 66% decreased odds of being adherent compared to patients with government insurance. All other factors were not significant.
Characteristics associated with adherence to follow-up calls.
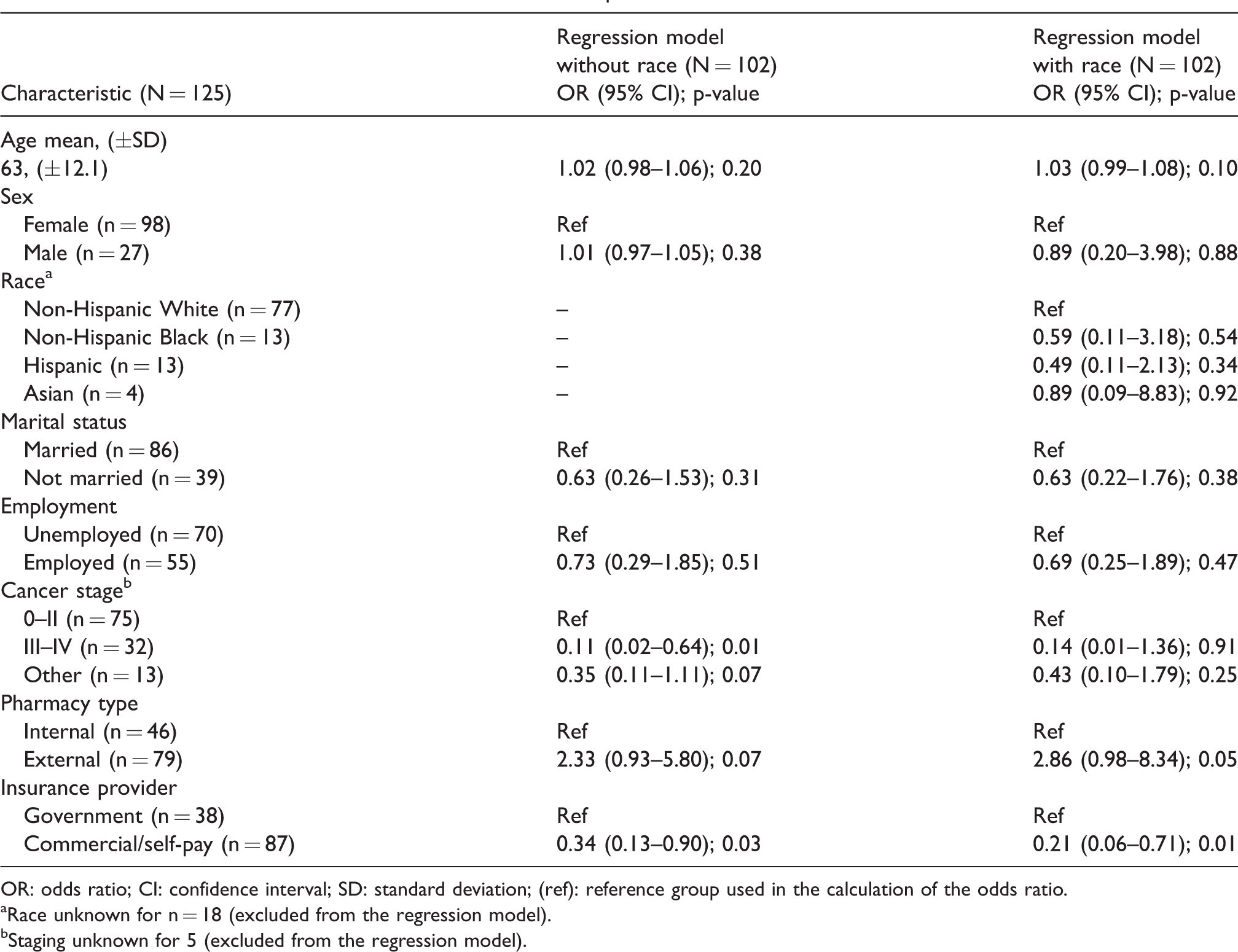
OR: odds ratio; CI: confidence interval; SD: standard deviation; (ref): reference group used in the calculation of the odds ratio.
aRace unknown for n = 18 (excluded from the regression model).
bStaging unknown for 5 (excluded from the regression model).
In the model including race, after adjusting for other covariates, factors associated with follow up call adherence were insurance (OR = 0.21, 95% CI 0.06-0.71; p = 0.01), and pharmacy type (OR = 2.86, 95% CI 0.98-8.34; p = 0.05) was marginally significant (Table 2). This means that patients with commercial insurance had a 79% decrease odds of adhering to follow-up calls compared to those with government insurance. Similiary, patients using an external pharmacy were 2.8 times more likely to be adherent compared to those using an internal pharmacy. All other factors were not significant.
The association of the type of cancer with adherence to follow-up calls was not analyzed, as some of the cancer types did not have enough data points. However, with the exception of breast cancer and genitourinary/gynecological disease, the majority of the patients with other types of cancer were non-adherent to follow-up calls: 83% of patients with brain cancer, 73% of patients with gastrointestinal cancer, and 67% of those with hematological cancers. The only patient in the study with NSCLC was also non-adherent to follow-up calls (Figure 1).
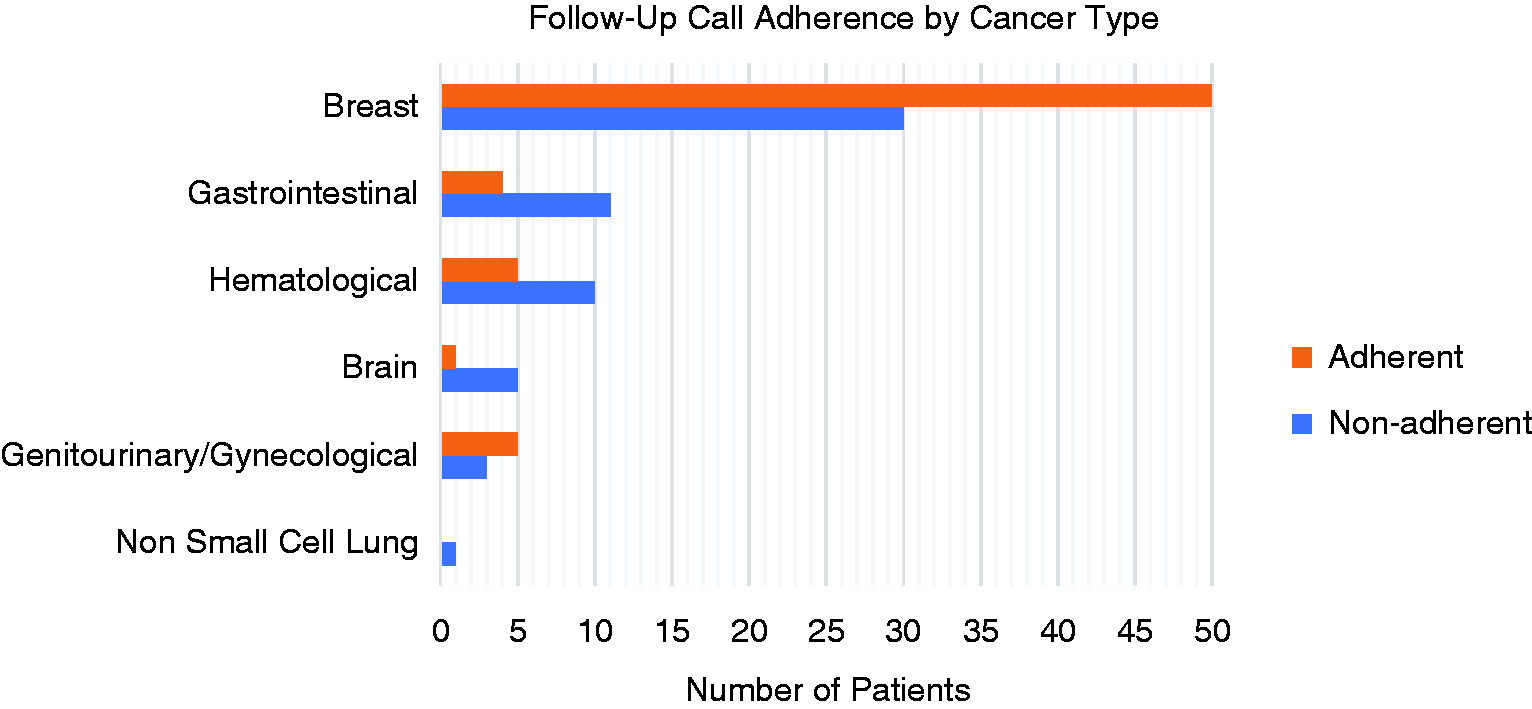
Patients who answered three or more calls were considered adherent, while patients answering less than three were considered non-adherent. Adherence rates were recorded by cancer type. Adherence rates were 62.5% for breast, 27% for gastrointestinal, 33% for hematological, 16.6% for brain, 62.5% for GU/Gyn, and 0% for lung.
Association of the timing of follow-up calls with call success
Patients were called Monday through Friday between 8 am and 5 pm and Saturday from 10 am to 2 pm. Patterns of high response rates were observed between the hours of 12 and 3 pm (Figure 2). Calls made on Tuesdays (24%) and Thursdays (26%) had the highest success rates, with Wednesdays (4%) being the least favorable day to call (Figure 3).
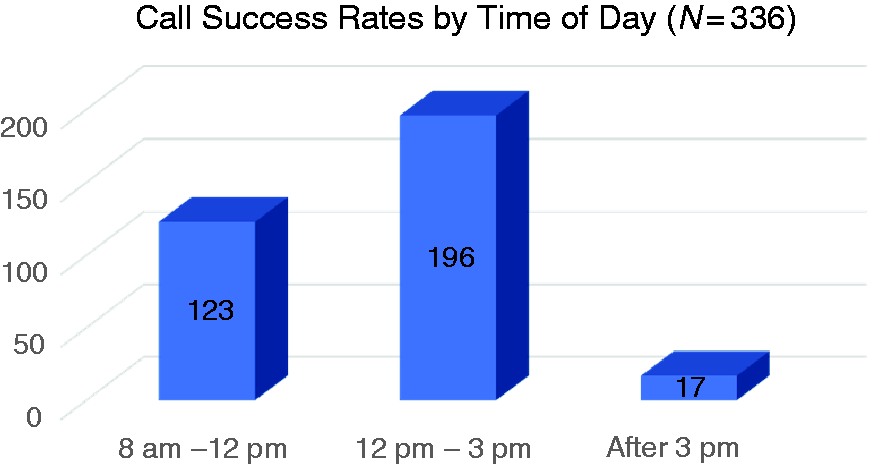
Patient follow-up calls were made at different times of the day. The number of successful calls during each time frame was recorded. Call success was defined as the patient answering the call during one of the three attempts made to reach them. Success rates were 37% from 8 am to 12 pm, 58% from 12 pm to 3pm, and 5% after 3 pm.
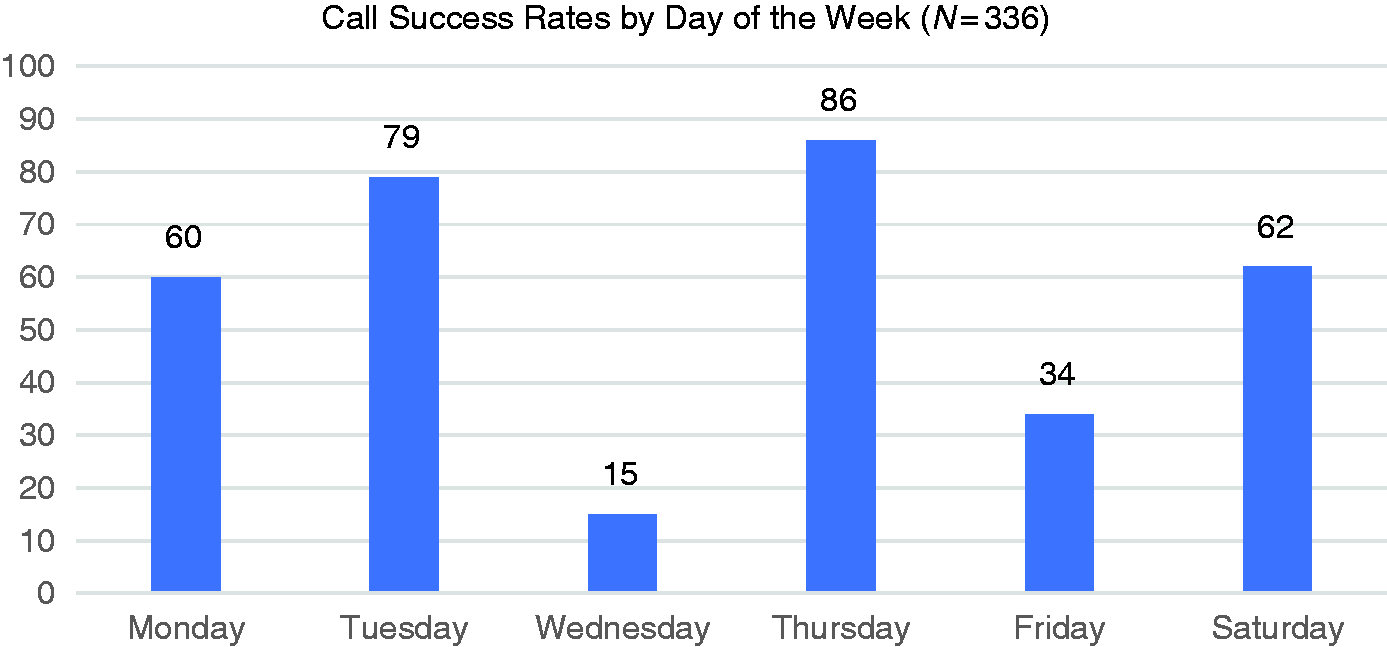
Patient follow-up calls were made on different days of the week. The number of successful calls during each day was recorded. Call success was defined as the patient answering the call during one of the three attempts made to reach them. Success rates were 18% for Monday, 24% for Tuesday, 4% for Wednesday, 26% for Thursday, 10% for Friday, and 18% for Saturday.
Discussion
Having an outlet such as follow-up calls can create an opportunity for patients to adhere to the dosing schedule, report adverse events or new medications, and address any concerns. However, patients can only benefit from follow-up calls if they are responsive. The purpose of our study was to investigate patient characteristics associated with successfully answering follow-up calls related to their prescribed oral antineoplastic treatment. Characteristics that were significantly associated with adherence to follow-up calls were pharmacy type, insurance, and staging.
The multivariable model that included race/ethnicity demonstrated that patients receiving oral antineoplastics from external pharmacies were more likely to adhere to follow-up calls. This is interesting and surprising because one benefit to a medically integrated pharmacy is for patients to receive more personal and coordinated care. Therefore, we hypothesized that internal pharmacy patients would have an increase odds of adherence to follow-up calls, but our study showed the exact opposite. Findings could be related to external pharmacy patients receiving fewer calls (clinical only) versus internal pharmacy patients receiving more calls (clinical and pharmacy-related), causing adherence differences. For example, a person who receives fewer calls from their oncology clinic could potentially be more prone to answering calls when they arise because they could be worried about the purpose of the call. It is still important to note that internal pharmacies provide several benefits such as being a “one-stop-shop” for patients, providing financial assistance to reduce medication related costs, and providing easier access for the oncology care team to communicate with pharmacists, which could be a barrier for external pharmacies. Findings from our study demonstrated a decline in adherence to follow-up calls for patients filling their oral antineoplastics at an internal pharmacy. However, there are potential proactive solutions to increase adherence such as utilizing face-to-face interactions during the first medication-pick-up to identify the best time and day to call them prior to making the first follow-up call. After this encounter, pharmacy staff could send reminders through text messages or emails prior to each follow-up call.
For both regression models, patients with commercial insurance were less likely to adhere to follow-up calls compared to those on governement insurance. This was surprising because privately insured patients tend to have more resources that would infer improved compliance compared to the Medicare or Medicaid groups, who are generally older, have poorer health, and in a lower-economic status.15,16 Future studies evaluating these differences are warranted to further investigate why differences were seen between follow-up call adherence in commercial versus government insurance recipients.
Race/ethnicity was not a significant factor when analyzed with other covariates. This was also surprising, as other studies identified disparities in medication adherence for minority patients and we thought this trend would be similar for follow-up call adherence. 17 In addition, a previous study identified that minorities have a higher proportion of barriers around access to care that could lead to adherence issues. 18 However, since community oncology practices improve access to care, this could be a potential reason why racial disparities were not seen in the studied population. Findings also demonstrated non-significant associations between age or sex with the adherence to follow-up calls. This was another interesting finding because previous studies found that females have poorer medication adherence compared to males, 19 suggesting that this would be a population that would likely benefit from follow-up calls.19
The majority of patients in our study were diagnosed with breast cancer, so an analysis to determine the association of cancer type and and adherence to follow-up calls could not be performed. However, we observed that patients with cancer types that have a five-year survival rate of less than 70%, such as brain cancers, non-small cell lung cancer, select hematological malignancies and gastrointestinal cancers, had a follow-up adherence rate of 34% or less. However, patients with cancers associated with higher survival rates such as breast and select genitourinary cancers (i.e. kidney and prostate), had a follow-up call adherence rate of 62.5%. Since patients with poorer survival were less likely to answer follow-up calls, it supported our findings which demonstrated that adults with stage III-IV were less likely to adhere to follow-up calls. This reveals a critical need to find additional assessments for future studies to investigate why patients with cancers that have poorer survival outcomes or advance disease are less likely to answer follow-up calls.
Several studies have evaluated telephone call interventions among patients on oral chemotherapy, but did not report the number of patients excluded from the intervention due to non-response.7,10,19-22 However, to our knowledge, this is the first study assessing oncology follow-up call response rates. The mean response rate throughout the six months was less than 50%. We also found that 52% of patients enrolled in the study were adherent to follow-up calls, while 25% of the total population did not answer any phone calls. The low adherence and response rates are alarming because patients who do not answer the phone are unable to receive the benefits that follow-up calls offer. However, during follow-up calls, voicemails were not left for the patients, so this could also be a potential factor for low response rates.
Results from our study also demonstrated higher response rates for follow-up calls made on Tuesdays and Thursdays and between the hours of 12 pm and 3 pm. Although we initially expected to see higher success calls on Saturdays and lower calls during the weekdays, it is important to note the majority of our population were unemployed which could be linked to the successful time frames. The timing of unsuccessful calls were not collected, so a direct comparison to successful calls for adherent patients could not be made. Future studies can assess if there are differences in call time preference for patients who are adherent versus those who are non-adherent to calls.
A relatively small sample size is one limitation of our study. Due to the lack of previous similar studies to guide us in sample size calculation, we did not perform a priori sample size calculation while designing this study. Our adjusted model from Table 2 includes 8 variables and the intercept parameter. As such, we have around 14 subjects per variable which is little less than the often-used rule of thumb of 20 subjects per variable relied by biostatisticians. A second limitation was not having a large number of patients for each diagnosis to see if statistical significance exists amongst cancer types. Lastly, the third limitation was that voicemails were not left for patients. Although patients were familiar with the phone number of the clinic, some could have thought it was a refill request reminder and didn’t know it was the clinic calling for follow-up call adherence. However, the information gathered in this study will be important for clinics interested in using follow-up calls as a form of intervention. Our results show that follow-up calls may not be a one size fits all approach and that other strategies may be needed to reach patients. Further studies evaluating adherence rates for follow-up calls across different centers are needed to further understand if these findings are common among other community clinics.
Conclusion
Follow-up calls are useful in monitoring patients who are receiving oral antineoplastics. However, non-adherence to follow-up calls was observed in more than 45% of patients receiving care from a community oncology clinic. Characteristics associated with a decrease in follow-up call adherence include patients with advanced stages of cancer, on commercial insurance, and going to an internal pharmacy. Further studies evaluating adherence and response rates for follow-up calls across different centers are needed to further understand if these findings are common among other community oncology clinics.
Footnotes
Acknowledgements
The authors would like to thank Joanna Garcia for data management and project development, Brook Amen for conducting an extensive literature search, Trisha Berger for editing the first manuscript draft, and Barry Russo and John Clagg for assisting with project development.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The primary author, Shanada Monestime, received funding support for the research from SaferCare Texas.