
Abstract
Introduction
Pembrolizumab is an anti-PD-1 monoclonal antibody, approved and under development for numerous indications in oncology. It is available as either lyophilized powder for reconstitution or ready-to-use solution. Both are required to be diluted in saline or dextrose solution prior to intravenous infusion. After dilution, the recommendation per summary of product characteristics is 24 h at 2–8℃ and 6 h at room temperature. The purpose of this study was to investigate the physicochemical stability of pembrolizumab diluted solution (1 mg/mL) at both refrigerated and room temperature conditions for an extended period.
Methods
Under aseptic conditions, pembrolizumab was diluted in 250 mL of saline injection in polyolefin bags to obtain the final protein concentration of 1 mg/mL. Thus, prepared bags were then stored at either 5℃ ± 3℃, refrigerator exposing the product to ambient light or room temperature (20℃ ± 3℃) on the benchtop.
Results
Using several analytical methods, it was demonstrated that pembrolizumab solution for infusion, diluted in normal saline can be stored in polyolefin infusion bags for at least 1 week at 5℃ or RT with no evidence of chemical or physical instability. No aggregation was observed.
Conclusion
Thus, the practical use of aseptically prepared diluted pembrolizumab in saline can be safely extended to optimize the workload of centralized preparation units and to minimize costs. However, it is the responsibility of the end-user to maintain overall quality of prepared admixture solution that is administered to patient, by following aseptic compounding process as recommended in the packaging insert.
Introduction
Pembrolizumab (Keytruda®) is a humanized IgG4 isotype antibody used in cancer immunotherapy by blocking a protective mechanism of cancer cells and thereby allowing the immune system to destroy them. 1 It targets the programmed cell death 1 (PD-1) receptors of lymphocytes. It was approved for the treatment of multiple cancers. It is available as powder for solution for infusion 50 mg/vial or solution for infusion 100 mg/vial. Prior to administration, under aseptic condition the powder for solution for infusion vial is reconstituted with sterile water for injection and the required volume for dosage is withdrawn and transferred into an IV bag containing 0.9% NaCl injection or 5% dextrose injection. The final concentration of the diluted solution should be between 1 mg/mL to 10 mg/mL. Prescribing information (PI) recommends administering the diluted solution intravenously through an intravenous line containing a sterile, nonpyrogenic, low-protein binding 0.2 µm to 5 µm in-line or add-on filter. 2 When the diluted solution in the infusion bag cannot be administered immediately, then it can be stored up to 6 h at room temperature or for up to 24 h in refrigerated condition.
Per the recommendation in PI, the stability of diluted pembrolizumab is limited to 24 h at refrigerated condition. The recommended stability limits were only based on the possible risk of microbiological contamination and its proliferation in diluted admixture bag data generated at the time of original submission and not on physicochemical stability. Typically, protein therapeutics administered by IV infusion are prepared aseptically in a hospital pharmacy or manufactured in advance in a compounding facility following appropriate procedures. Hence, the ready to administer preparations are likely to be held longer under refrigerated condition before use. The limited admixture solution stability presents a challenge for health care provider and hospital pharmacies that provide centralized support for admixture preparation. There are examples in the literature where studies showed physicochemical stability for longer in-use period than those recommended in PI for commercial products.3–9
In some instances, compounding pharmacies perform physicochemical stability studies or rely on third party published studies to justify the use beyond the recommended period.3–10 The caveat in such instances is the lack of adequate and product specific method panels and assessment criteria. In addition, there is no guiding regulatory recommendation on in-use stability, specifically with respect to appropriate analytical testing and acceptance criteria. Therefore, considering flexibility in administration, extended stability could enable in-advance batch preparation for dose banding inducing workload optimization and significant resource saving for hospital pharmacy-based centralized preparation units. Only one independent study by Slade Health concerning the stability of diluted pembrolizumab in an infusion bag is currently available. 11 In their memorandum to customers, the stability of compounded pembrolizumab in 0.9% saline was revised from 24 h to 14 days. However, this was based only on protein concentration and there was no indication of use of appropriate methods to evaluate other critical quality attributes of the molecule—especially the physicochemical stability of pembrolizumab was not ascertained. Hence, it is critical to understand the physicochemical stability of pembrolizumab in saline admixture solution especially in terms of aggregation, a key parameter of the protein stability.
The interaction and duration of drug contact with various surfaces such as IV infusion bags, IV lines and in-line filters could potentially affect the physicochemical stability and drug recovery. Such incompatibilities are evaluated during the development process where various administration components are evaluated for compatibility. In addition, the preparation process may inadvertently introduce nosocomial microbial contamination if proper aseptic techniques and conditions are not followed. Therefore, physicochemical stability, microbial proliferation, and recovery of activity after dilution are typically evaluated during drug development process. 12 This provides the rationale for the recommendation of in-use time in the PI.
Therefore, the objective of this study was to assess the physical and chemical stability of diluted pembrolizumab at 1 mg/mL concentration as a worst-case representation after storage for up to two weeks at 5℃ and room temperature.
Materials and methods
Pembrolizumab solution for infusion, 100 mg/vial filled into 10 mL vials, with 13 mm opening, closed with a 13 mm gray-colored elastomeric stopper, and sealed with an aluminum crimp cap was used. This material represents the commercially available pembrolizumab solution for infusion 100 mg/vial. Admixture used in the study was 250 mL 0.9% normal NaCl USP polyolefin (non-PVC) bag (B Braun L8002). Though the prescribing information recommends the use of normal saline and 5% dextrose injection, this study was done only using normal saline based on prior knowledge where the physico-chemical stability of pembrolizumab admixture solution showed no difference between the two diluents. Moreover, due to high ionic strength, normal saline is considered as a worst-case representation.
Under aseptic conditions, pembrolizumab was diluted by 0.9% NaCl in 250 mL polyolefin bags to obtain the final protein concentration of 1 mg/mL. To begin, approximately, 30 mL of saline was removed from the bag accounting for overfill in bags. Using a sterile needle and syringe 10 mL of pembrolizumab solution for infusion (25 mg/mL) was aseptically introduced into the IV bag. The final protein concentration of 1 mg/mL was chosen as a worst-case representation as at this dilution the stabilizing excipients added to drug product (DP) are at the lowest level. In addition, protein to salt ratio is higher at this dilution rendering it worst case from physicochemical stability perspective.
Once prepared, the bags were gently mixed manually by inverting them 10 times and then stored at either 5℃ ± 3℃, refrigerator (with sliding glass door) exposing the product to ambient light or room temperature (20℃ ± 3℃) on the benchtop. Periodically, samples were pulled from the admixture bags for analytical testing at predefined time points. While, visual appearance, particulate matter testing by HIAC, protein concentration by UV280 and pH were performed immediately after sampling, the remaining analytical samples were frozen at −70℃ in polypropylene tubes and tested at the end of the study.
Due to the structural complexity of protein, it is well known that several complementary analytical methods are needed to fully assess the physicochemical stability.13,14 Therefore, size exclusion HPLC (SEC) for aggregation/ fragmentation, percentage of IgG reduced by capillary electrophoresis sodium dodecyl sulfate (CE-SDS) gradient ion exchange HPLC (IEX) for charge variants, ELISA for potency, hydrophobic interaction chromatography (HIC) HPLC for oxidation, particle counting by HIAC for sub-visible particulate matter and visual observation for visible particles were used in this study. All these analytical procedures used in this study were previously validated as stability-indicating methods for pembrolizumab solution for infusion. Appropriate modifications in the HPLC methods were done to account for dilute solution and presence of high salt content in the sample matrix.
Results and discussions
FDA guidance for industry regarding end-user manipulation of biological products outside of the description in the approved Biological License Application (BLA) describes the required physicochemical characterization for beyond the use date. 15 This includes appearance, color and clarity, visible particles, sub-visible particles, protein content, product-related impurities including minimum-protein aggregation, size and charge variants, and potency. 4 The results of the in-use stability of diluted pembrolizumab (1 mg/mL) in saline infusion bag stored at room temperature and refrigerated condition are discussed below under physical, chemical, and biological stability.
Physical stability
Physical stability of diluted pembrolizumab (1 mg/mL) in saline infusion bag after different storage conditions.
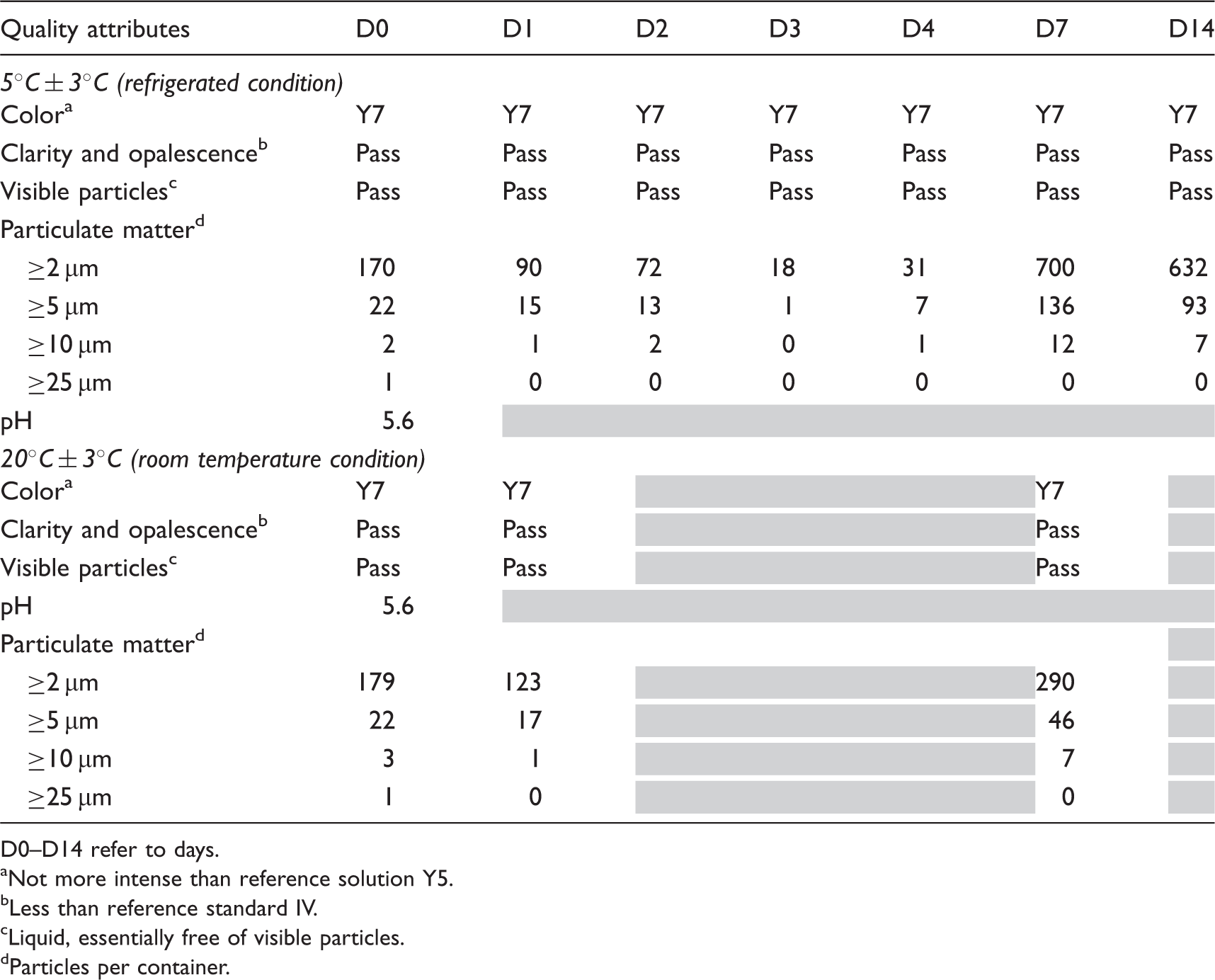
D0–D14 refer to days.
Not more intense than reference solution Y5.
Less than reference standard IV.
Liquid, essentially free of visible particles.
Particles per container.
The method used for visible particle is similar as that used for the DP release and stability testing. There was no visible particle observed at either temperature conditions. Sub-visible particle counts in the range of ≥2 µm to ≥25 µm was measured using light obscuration and there was no increasing trend observed in ≥10 µm and ≥25 µm counts. However, there was a clear increase in ≥2 µm particle count after day 7 (D7) at both conditions. Sub-visible particles in the range of ≥2 µm and ≥5 µm are gathered for information only and it is not surprising that the ≥2 µm counts would increase. It is consistent with drug product characterization studies. In addition, pH of the solution was measured at D0 and it is similar to the DP pH value. Based on prior knowledge, pH is not expected to change during infusion bag storage; hence it was measured only at initial.
Chemical stability
Chemical stability of diluted pembrolizumab (1 mg/mL) in saline infusion bag after different storage conditions.
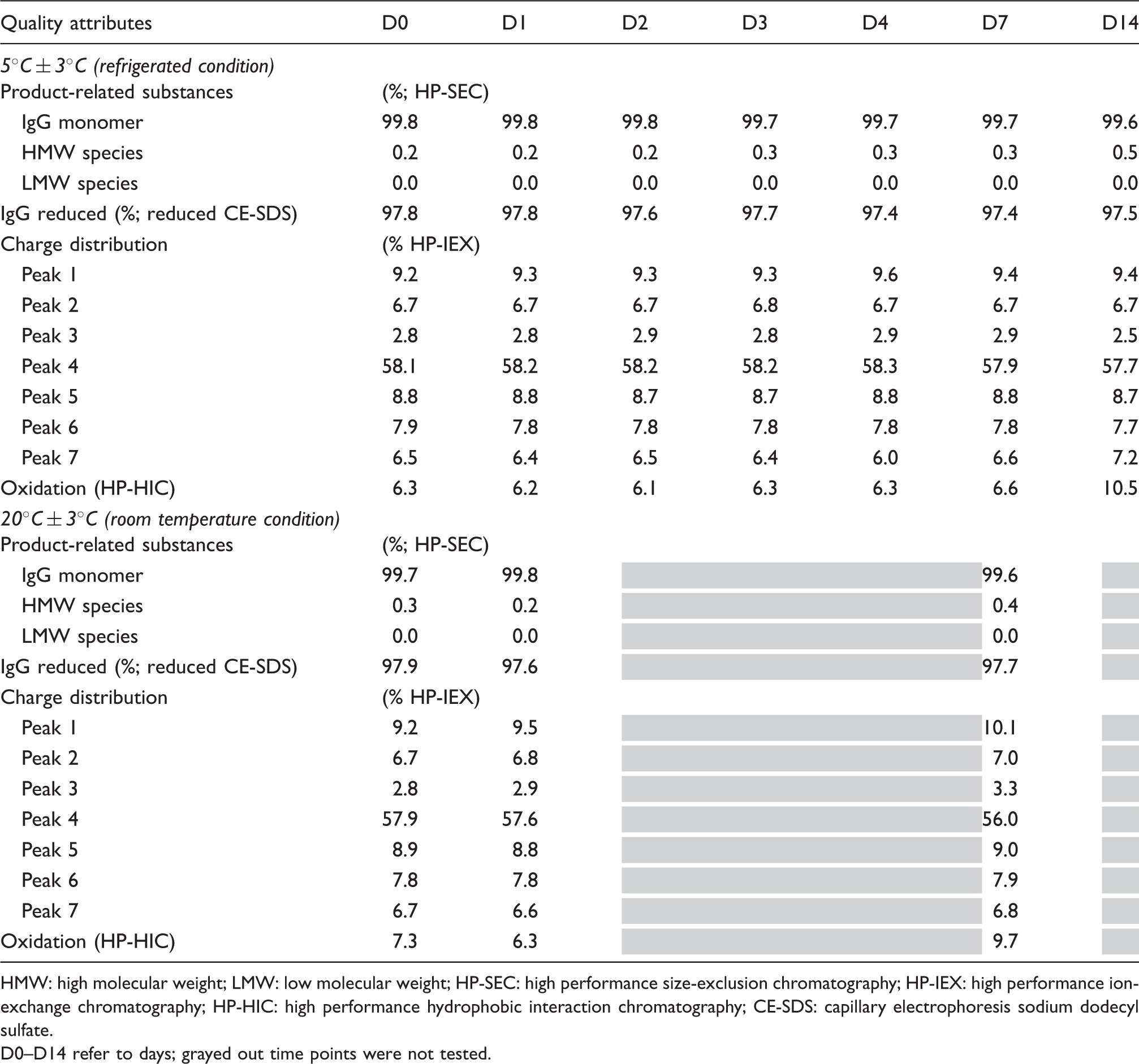
HMW: high molecular weight; LMW: low molecular weight; HP-SEC: high performance size-exclusion chromatography; HP-IEX: high performance ion-exchange chromatography; HP-HIC: high performance hydrophobic interaction chromatography; CE-SDS: capillary electrophoresis sodium dodecyl sulfate.
D0–D14 refer to days; grayed out time points were not tested.
Biological potency and protein concentration of pembrolizumab in diluted solution (1 mg/mL) in saline infusion bag at different storage conditions.
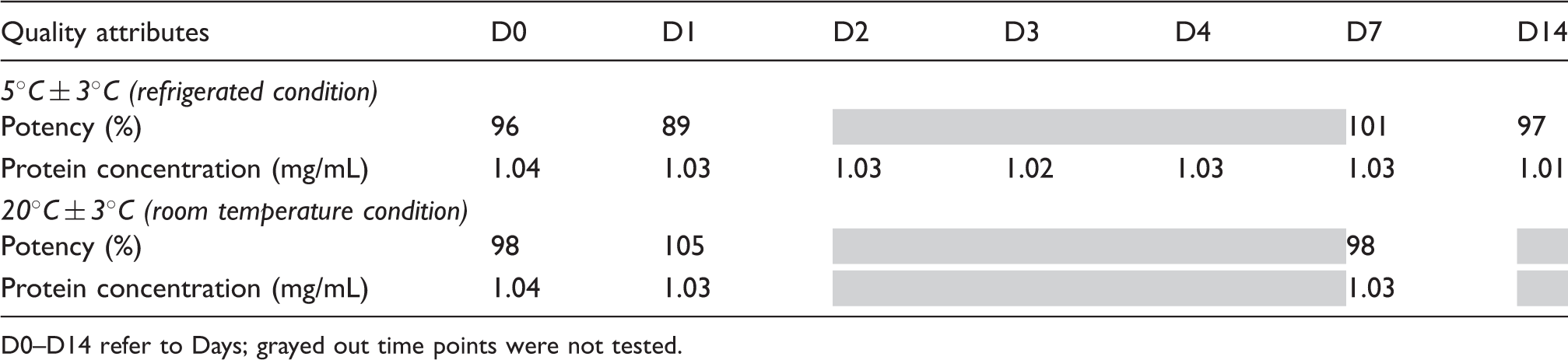
D0–D14 refer to Days; grayed out time points were not tested.
The percentage IgG monomer is determined by HP-SEC, which enables separation of low-molecular-weight (LMW) and high-molecular-weight (HMW) species from the antibody monomer based on their molecular size. At the initial state (D0), the admixture solution showed a major peak in HP-SEC, corresponding to the native protein, and a small peak revealing small fraction of HMW. There was no other peak indicating the absence of LMW species due to fragmentation. This profile remained unchanged throughout the duration of the study at both conditions (Table 2). However, there was a slight increase in HMW from 0.2% (D0) to 0.4% (D7 at RT and D14 at 5℃) but within the range of experience seen in the drug product.
Reduced CE-SDS is used to determine the percentage IgG reduced (intact light and heavy chains) of the antibody after reduction of the disulfide bonds present in the antibody. As seen in Table 2, there was no change in IgG monomer reduced across the condition at different time points studied.
HP-IEX is used to separate and quantify the charge variants of pembrolizumab and it shows a chromatographic profile (at D0) consisting of seven peaks. The individual peak percentages are provided in Table 2. In both storage conditions, the relative proportion of each peak remained unchanged at D14 (5℃).
Product-related impurities in pembrolizumab admixed solution was assessed by HP-HIC to separate and quantify oxidized variants of pembrolizumab. The HP-HIC method monitors the oxidation of sensitive amino acid(s) in the molecule. As seen in Table 2, oxidation impurity showed no change from D0 to D7 at refrigerated condition. There was steep increase in the impurity at D14; however, it is within the range of experience seen with admixture solutions. Similarly, at room temperature condition, the impurity values remained within the range of experience for admixture solution.
Functional activity
Evaluation of the functional activity of pembrolizumab included an assessment of its ability to compete with PD-1 ligand (PD-L1) for binding to PD-1 in a Potency ELISA (enzyme-linked immunosorbent assay). The potency ELISA method uses a recombinant human PD-1 Fc chimera immobilized on an ELISA plate.
The relative potency (Table 3) as determined by potency ELISA ranges from 89% to 105% across the samples from different conditions at various time points. The ability of diluted pembrolizumab (1 mg/mL) to compete with the ligand on D7 at both temperature conditions and on D14 at refrigerated condition has been compared with the functional activity at D0. The biological activity assay demonstrated similar potency at D7 (RT) and D14 (2–8℃) to D0. The protein concentration of each sample as determined by ultraviolet (UV) spectroscopy showed no difference across the temperature conditions at all time points tested.
Conclusions
The stability of pembrolizumab in admixture solution using several orthogonal methods demonstrated that diluted pembrolizumab in saline infusion bag stored at 5℃ and room temperature remained stable for at least one week. No physical instability was observed, translated by the absence of aggregation by HIAC, HP-SEC, and visual. Charge variants profiles in HP-IEX, oxidation impurity (HP-HIC) remained unchanged or within the range of previous experience for at least one week. Also, the functional ability of pembrolizumab to bind with PD-1 remained stable over two weeks at refrigerated condition. These results indicated that the time frame for the practical use of admixture solution could potentially be extended to at least one week at refrigerated condition by following the aseptic compounding process as recommended in the packaging insert.
It is difficult to predict all the possible conditions under which the product will be opened, diluted, stored, and transported. The end user/healthcare professional is responsible for maintaining the quality of the product that is administered to the patient. To help the user with this responsibility, the applicant conducts appropriate studies and provides the relevant information in the user information texts such as summary of product characteristics and PI. Though, chemical and physical in-use stability has been demonstrated in normal saline injection for at least one week at 5℃ and RT, whenever possible the aseptically prepared admixture solution should be used immediately, if not, in-use storage time and conditions are the responsibility of the end-user. Though, the prescribing information for pembrolizumab recommends the use of normal saline and 5% dextrose injection this study was done only using normal saline based on prior knowledge where the physico-chemical stability of pembrolizumab admixture solution showed no difference between the two diluents. Moreover, due to high ionic strength, normal saline is considered as a worst-case representation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclaimer
Opinions, recommendations, and views expressed in this publication are of the authors and should not be construed to represent the views or recommendation of Merck & Co., Inc., Kenilworth, NJ, USA. Authors recommend the practitioners to consult the product's current approved market specific prescribing information.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.