
Abstract
Introduction
Ibrutinib is an oral inhibitor of Bruton’s tyrosine kinase that is used for a variety of B cell hematological malignancies. Skin and subcutaneous tissue manifestations have been reported and were witnessed in up to 32% of the patients on ibrutinib. The mechanism in which ibrutinib can cause skin toxicities has been thought due to the inhibition of epidermal growth factor; c-Kit and platelet-derived growth factor receptor). Here, we report a case of an elderly chronic lymphocytic leukemia patient who developed multiple inflamed lesions and lower limb cellulitis in 100 days after initiating ibrutinib therapy.
Case report
A 68-year-old male patient with relapsed chronic lymphocytic leukemia was started on ibrutinib 420 mg orally daily following multiple lines of therapy. Three months following ibrutinib, the patient developed multiple hyper pigmented lesions over both forearms then over both thighs; buttocks and lower limbs. The lesions were labeled as ecthyma and cellulitis that started as papules, which progressed to pustules.
Management and outcomes
The patient required admission in which he received prolonged course of antibiotics. Biopsy from the wound showed soft tissue fragment infiltrated by acute and chronic inflammatory cells with necrosis; rare foreign body giant cells and granulation tissue formation; suggestive of abscess. Subsequently, ibrutinib was stopped permanently.
Discussion
This is the first case description of an ibrutinib-associated sever skin toxicity in Qatar. The provided information regarding the clinical descriptions of toxicity profiles in general and skin-based in particular is valuable information for daily clinical practice, especially when selecting the optimum first-line treatment for the patient.
Keywords
Introduction
Ibrutinib is an oral Bruton’s tyrosine kinase (BTK) inhibitor. It is approved by the United States (US) Food and Drug Administration (FDA) for a variety of B cell hematological malignancies including chronic lymphocytic leukemia (CLL); mantle cell lymphoma (MCL) and Waldenstrom macroglobulinemia (WM).1,2 Cutaneous adverse effects of ibrutinib include rash (12% to 29%); petechiae; pruritus (11% to 14%) and skin infections (14% to 16%).1–3 Several cases have reported variable skin toxicities to ibrutinib therapy in CLL; MCL and WM patients.4–10 Here, we report an elderly CLL patient who developed multiple inflamed skin lesions and cellulitis after 100 days from initiating ibrutinib.
Case presentation
A 68-year-old white male patient, who is a known case of hypertension; chronic artery disease; dyslipidemia; hypothyroidism and prostate cancer was diagnosed with CLL Stage III in 2008. The patient’s home medications included: levothyroxine 100 mcg daily; rosuvastatin 10 mg daily; amlodipine 5 mg daily and vitamin D2 50,000 IU weekly. The patient was kept under watch and wait approach as his complete blood count (CBC) parameters were under acceptable range. In 2012, his white blood count (WBC) started to increase; platelet count started to drop and his bone marrow exam was consistent with disease progression. The patient received a total of six cycles of chemotherapy Bendamustine and Rituximab (BR) in 2013, which was complicated by intractable diarrhea and reactivation of hepatitis B. The patient was followed by gastroenterology team and was kept on tenofovir disoproxil 245 mg daily. The patient completed his treatment course and was in remission until February 2015 when he started complaining from cervical lymphadenopathy. Images were requested accordingly, including computerized tomography (CT) of thorax and abdomen on February 2015, which showed newly developed multiple mediastinal; axillary; retroperitoneal and mesenteric lymph node.
In June 2015, the patient started complaining from B symptoms manifested by weight loss; anorexia; on and off fever along with Coombs positive anemia that failed to respond to steroids and increased in transfusion demands. Repeated CT was performed which showed stationary course of the disease and bone marrow findings were consistent with persistent bone marrow involvement by B-cell CLL (11 q deletion) with increased prolymphocytes. Thus, the patient was started on ibrutinib 420 mg orally daily.
Ibrutinib treatment course
In July 2015, the patient developed clostridium difficile infection; which was treated and he was stable until October 2015 when he stated to have multiple skin lesions labeled as ecthyma and cellulitis that started as papules, which progressed to pustules. In addition, hyperpigmented lesions started to progress over both forearms then over both thighs; buttocks and lower limbs. The patient was followed by dermatology upon which he was prescribed local antibiotic cream (fusidic acid 2% twice daily) and lotions. However, the skin lesions were persistent over his left lower limb for about one month without any improvement.
The patient was admitted on March 2016 for further investigations. Consequently, wound incision and drainage was performed along with regular follow-up with wound care. Biopsy from the wound showed soft tissue fragment infiltrated by acute and chronic inflammatory cells with necrosis; rare foreign body giant cells and granulation tissue formation; suggestive of abscess. Culture from the tissue showed Staphylococcus aureus sensitive strain and the patient was started on ciprofloxacin 500 mg orally every 12 h and clindamycin 450 mg orally every 6 h. Work up for tuberculosis was negative as well as Epstein bar virus and cytomegalovirus. Ibrutinib treatment was stopped and it was decided not to resume ibrutinib treatment again (Figure 1).
Multiple inflamed skin lesions, marked as cellulitis on both arms and legs.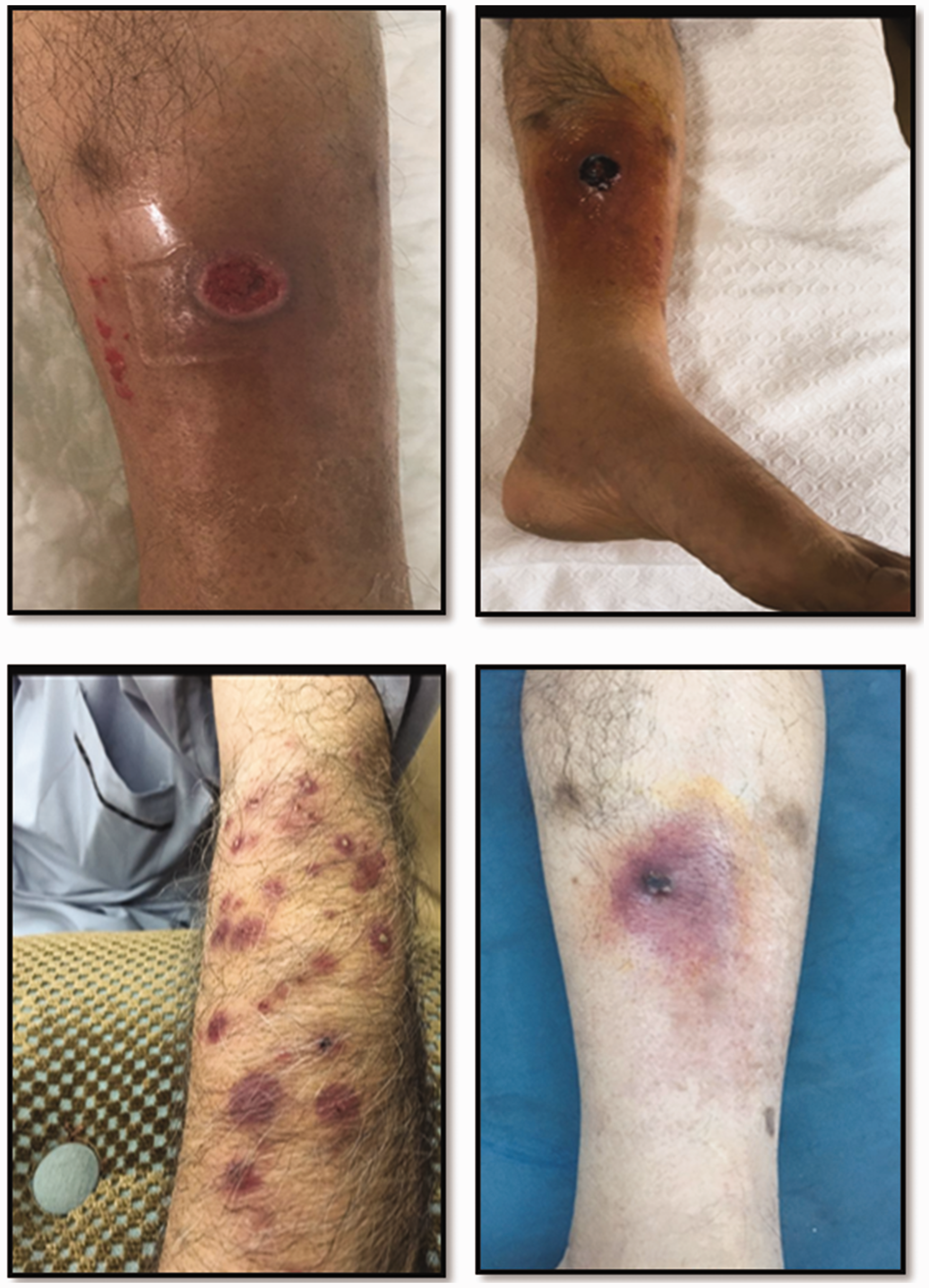
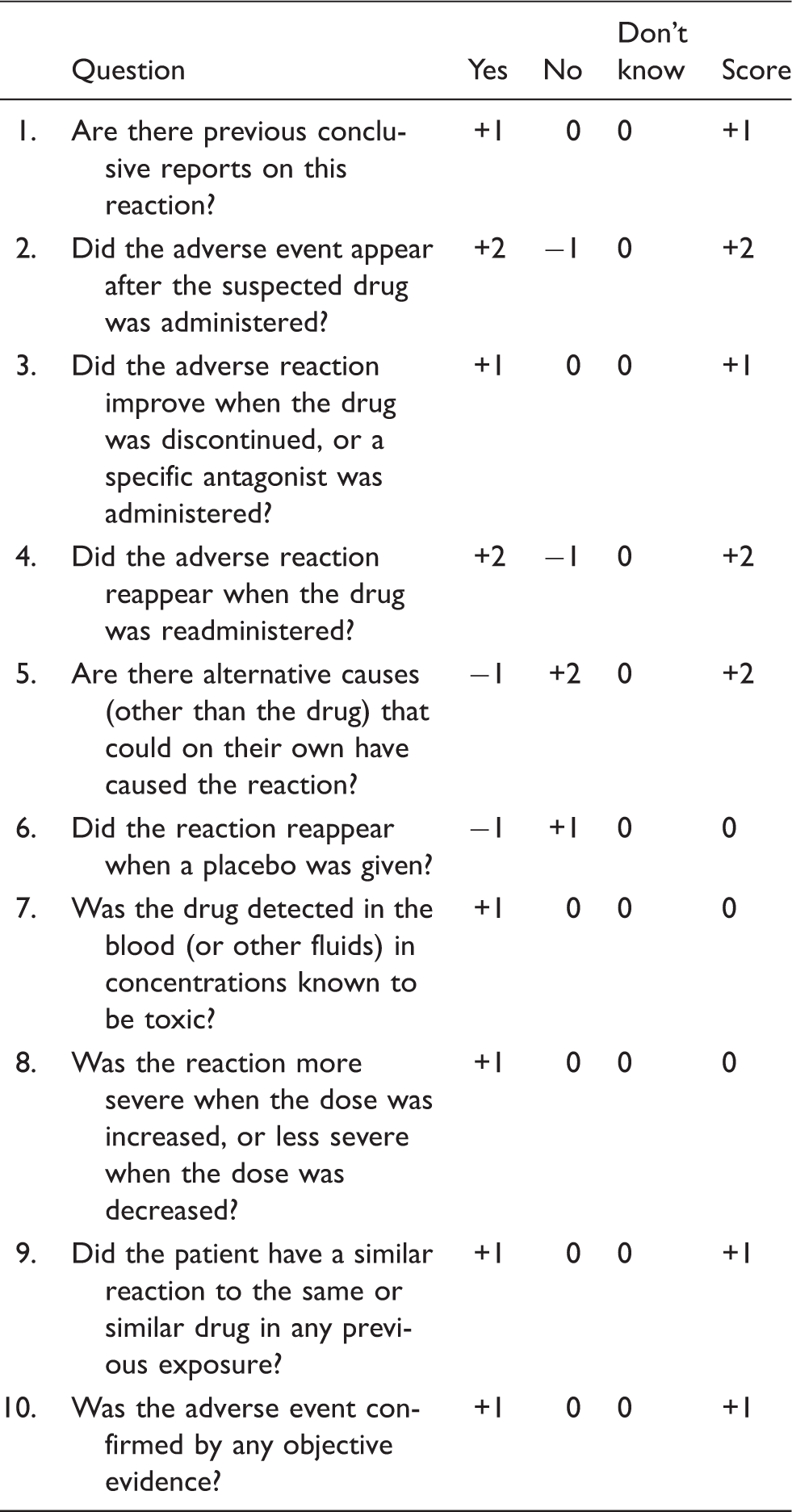
Causality assessment
Naranjo adverse drug reactions probability Scale.
Discussion
With respect to ibrutinib’s side effect profile, it is worth mentioning that it is associated with a 25% incidence of cutaneous rashes according to Pharmacyclics Pharmaceuticals FDA-approved patient information.1–3 Cutaneous adverse effects of ibrutinib include rash (12% to 29%); petechiae; pruritus (11% to 14%) and skin infections (14% to 16%).1–3 Several cases have reported variable skin toxicities to ibrutinib therapy in CLL; MCL and WM patients.4,12,13 A thorough database search to review the literature for any evidence regarding ibrutinib-associated dermatological adverse events was performed. In early phase clinical trials, ibrutinib was tested as monotherapy in MCL, CLL and small lymphocytic leukemia (SLL), and it was associated with a frequency of 13–27% of rash occurrence.2–6 An open-label, multicenter, phase 1 b/2 trial published in the lancet oncology in 2014 included 31 patients at least 65 years old previously untreated with symptomatic CLL or SLL requiring therapy. Patients received 28 days cycles of once daily ibrutinib 420 mg or ibrutinib 840 mg. The primary endpoint was safety of the dose-fixed regimen with respect to frequency and severity of adverse events. Adverse events reported from first dose up to 30 days of last dose of ibrutinib were petechiae (16%) and 13% in each of the following: cellulitis; erythema and rash pruritus.
In addition to being a BTK inhibitor and despite having high selectivity for BTK, it exerts off-target effects on other kinases, such as epidermal growth factor receptor (EGFR). Ibrutinib was shown to effectively inhibit EGFR in a dose-dependent manner. Inhibition of EGFR is known to enhance apoptosis and inhibit cell cycle progression, which stimulates apoptosis and inflammation. As cutaneous eruptions are considered common side effects to EGFR inhibition by other tyrosine kinase inhibitors, ibrutinib-induced rash may be attributed to inhibition of EGFR. 8 Another proposed mechanism of ibrutinib-induced drug eruption is through inhibition of c-Kit and platelet-derived growth factor receptor (PDGFR), similar to imatinib which is a tyrosine kinase inhibitor used in the treatment of chronic myeloid leukemia (CML). 10
A case report published in the American journal of hematology in 2015 presented a 67-year-old man with 17 p deletion CLL who was started on ibrutinib 420 mg PO daily. Two weeks after therapy initiation, the patient developed a painless, non-pruritic rash in the form of a diffuse distribution of bright red edematous papules, 0.5–1 cm in diameter that began on his wrists and then spread to his entire body. The rash also involved his palms and soles and had a peripheral-to-central pattern of spread. His absolute eosinophil count was within the normal range (100/mm3). Ibrutinib was suspended and after several days his rash had completely resolved. Since the patient was on allopurinol which can cause the rash, allopurinol was stopped and the patient was restarted on a lower ibrutinib dose 140 mg oral once daily. After a single dose, he developed recurrence of his full-body rash then ibrutinib was again stopped. The rash again disappeared within several days of stopping ibrutinib. As the clinical features distinguishing the rash from an allopurinol-mediated rash is edematous papules in contrast to the morbilliform rash associated with allopurinol, the associated toxicity was attributed to ibrutinib.
A single center experience published in the British journal of hematology included 14 patients (13 CLL, 1 MCL) who developed rash while receiving ibrutinib at the Stanford Cancer Center. There were two distinct rash subtypes observed: (i) a no palpable, largely asymptomatic petechial rash and (ii) a palpable eruption characterized by pruritic, non-blanching, violaceous papules clinically resembling leucocytoclastic vasculitis. The study concluded that the early onset (15 days after drug initiation) palpable purpuric rash varied in severity and resulted in temporary stop of the medication, while the late onset (80 days after drug initiation) non-palpable rash was mild and required no dose adjustment of ibrutinib. 7
Another case report published in the American journal of dermatopathology in 2016 presented a 70-year-old white male patient with stage CLL who was being treated with ibrutinib and rituximab. He developed a distinguishable eruption in the form of bilateral, purpuric, painful cutaneous nodules which resolved when the drug was discontinued. The reason why the authors believe that ibrutinib is the causative factor is the appearance of the nodules during the fourth month of therapy which increased in size, sensitivity and number until the drug was stopped at six months. At that point, they regressed and disappeared completely within six weeks. 1 In addition, a case report published in skin diseases and skin care in 2017 regarding a 59-year-old Caucasian male with a history of CLL who was being treated for two years with ibrutinib 420 mg once daily. The patient was tolerating it quite well and reported no adverse effects until one day he presented with a five days old pruritic maculopapular rash with multiple hemorrhagic bullae involving skin, palms which was first diagnosed as varicella zoster and he was given oral acyclovir but the rash was getting worse. It first appeared on the palms as reddish raised lesions then black colored blisters started to appear followed by lesions on the trunk of the body, lower extremities as well as around his mouth. It was associated with swelling of the lips and bilateral hands. Ibrutinib was stopped and the patient was given IV steroids and antihistamines. The rash started to resolve and became less itchy and the bullae decreased in size in the next three days. 9
Moreover, the first case report for ibrutinib-induced Sweet syndrome was published in the American journal of dermatopathology regarding a 64-year-old woman with 12 p deletion CLL who was treated with ibrutinib and developed several erythematous, painful, palpable red to violaceous papulo-nodular skin lesions in the limbs; neck and face one year after therapy initiation. She was diagnosed with neutrophilic dermatosis based on skin biopsy. Ibrutinib was stopped and topical steroids were given after which a rapid resolution of the rash occurred. Ibrutinib was restarted at a lower dose (280 mg once daily) three months later and there was no recurrence of her cutaneous lesions. However, when the dose increased to 420 mg once daily, recurrence of the Sweet syndrome occurred which led to treatment cessation after which they completely disappeared. 14 Here, ibrutinib skin adverse events were shown to be dose-dependent and this effect has been observed in Sweet syndrome associated with imatinib, another tyrosine kinase inhibitor. 15
Ibrutinib-associated skin toxicity was also reported in patients with WM. A case report published in dermatology reports in 2017 described a case of a 79-year-old male patient with WM receiving ibrutinib who after 12 weeks of initiating ibrutinib developed a painless red maculopapular non-pruritic rash which started from the groins and wrists then spread to extremities, trunk and face. The rash resolved with two weeks of topical steroids and with no modification (tapering, suspending or discontinuation) of ibrutinib regimen. This was the first case report to present ibrutinib-associated rash in a WM patient and the patient had similar presentation to the one reported in the American journal of hematology in 2015 but later onset (12 weeks vs. 2 weeks). 8
So far three subtypes of ibrutinib-related skin inflammation have been reported in the literature: (1) leukocytoclastic vasculitis like pruritic violaceous palpable purpura, (2) painless non-pruritic edematous papules with centripetal spread and (3) asymptomatic non-palpable petechial rash.2,7 Whether the association with skin toxicity occurrence is dose depended is still unknown. The management of skin toxicities was either complete cessation of the drug, suspending then restarting at a lower dosage or continuation of therapy while observing.
Conclusion
Here, we report an elderly CLL patient who developed multiple skin lesions and cellulitis in 100 days after initiating ibrutinib therapy. This is the first case description of an ibrutinib-associated severe skin toxicity in Qatar. The provided information regarding the clinical descriptions of toxicity profiles in general and skin-based in particular is valuable information for daily clinical practice, especially when selecting the optimum first-line treatment for the patient. Our case report contributes in generating a shared clinical experience that can be useful for recognition and management of ibrutinib-associated skin toxicity. The importance of our valuable data is as high as the increasing demand of ibrutinib use in CLL as well as other approved indications, such as MCL and chronic GVHD
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.