
Abstract
Background
Widespread adoption by patients is imperative for the success of app-based interventions for enhancing adherence to oral anticancer medications. Patients' attitudes and beliefs should be evaluated to understand determinants of their acceptance and adoption of such interventions.
Objective
To identify factors that influence cancer patients' intention to adopt an app-based system for enhancing oral anticancer medication adherence.
Methods
This study was conducted as part of the usability evaluation of an app-based system for enhancing adherence. We followed the grounded theory approach employing audio-recorded face-to-face interviews for data collection from patients taking oral anticancer medications (n = 15) and caregivers of such patients (n = 3). Data analysis involved verbatim transcription of all interviews, coding of the transcripts and field notes, detailed memo writing, and constant comparative evaluation of emergent categories.
Results
A conceptual framework of facilitating and hindering factors for users' adoption intention for an oral anticancer medication adherence app was developed. Findings suggest that facing difficulties in maintaining adherence and patients' perceived superiority of the app over their current methods facilitate adoption intention. In contrast, having to pay, lack of language options and users' perception of low competence in using an app were the hindrance factors.
Conclusion
This study showed that adoption of adherence apps could be explained by technology acceptance constructs, such as performance expectancy. Adoption intention was also facilitated by patients perceived vulnerabilities in maintaining adherence to their medications, which was a health behaviour construct. Implementation of app-based programs should address patients' perceived vulnerabilities and relative advantage of the app over their current methods. Clinicians and app developers should also consider the financial, technological and language barriers for end users.
Keywords
Introduction
With the advent of oral anticancer medications (OAMs), patients are having increased responsibility in managing their medications and thus face the challenges of maintaining optimal adherence.1–5 Studies report suboptimal OAM adherence, which in many cases are comparable to other chronic medications.2,3 This has significant clinical and economic implications related to the increased risk of hospitalization and associated costs of managing complications arising from non-adherence. 6 As a result, health programmes that incorporate effective interventions to improve medication adherence, both in the context of cancer and other chronic conditions, can have significant impact in terms of ensuring positive clinical and economic outcomes.7–9 In this regard, the use of smartphone applications (apps) is increasingly being promoted as an efficient way of improving adherence.10–12 Apps are amenable to delivering various educational and behavioural interventions while enabling caregivers and health professionals to monitor patients' medication consumption patterns.13,14
Continued engagement of end users in the process of development and implementation of adherence apps helps developers in identifying factors that influence acceptability and actual usage by patients and their caregivers.15–17 This is particularly important as the success of an app ultimately depends on acceptance and usage by patients.11,18–20 According to a recent study, 66.0% of surveyed cancer patients were reported to have interest in using apps in the management of OAM adherence. This study showed that patients' age, education level, income and current use of a health app were significantly associated with interest in using an adherence app. 21 Apart from socio-demographic characteristics, the effect of patients' attitudes and beliefs, on their intentions to use adherence apps is not well understood. 21 Thus, more in-depth analysis of the determinants of patients' acceptance of adherence apps is necessary to facilitate adoption of such interventions. 11
Different studies have used various models of technology acceptance and health behaviour theories to explain acceptability of utilizing mobile technologies in health interventions, also known as mobile health (mHealth).11,22,23 Notable examples in this regard are studies using the technology acceptance model (TAM) and its variants, which generally identify perceived usefulness and ease of use of a technology as the main determinants of users' acceptance (assessed by individuals' expressed behavioural intention to use the technology).18,24–31 Studies that used TAM-based models to evaluate acceptance of health technology have confirmed their predictive power of technology acceptance. 28 However, most of these studies incorporate added variables to the original TAM model or its subsequent variants.16,18,26–28,32 This has led to variations in the specification of model components, which in turn is a reason for the absence of a standardised model with universal applications. As a result, it is difficult to find a single model of acceptability of app-based health interventions that is universally accepted. Moreover, there is limited research on the determinants of patients' acceptance of adherence apps in the context of medications for cancer and other chronic disease conditions. This study, therefore, addresses the research question: what factors influence patients' intention to use a mobile app for enhancing OAM adherence?
Methods
Study design
A qualitative study design using the grounded theory approach described by Charmaz was followed in this study. 33 The grounded theory approach was preferred as it enables investigation of important factors without having to subscribe to any one of the existing theories and avoids forcing respondents' opinions into predetermined categories. The study was conducted, between December 2016 and March 2017, as part of the usability evaluation of an in-house developed prototype smartphone app-based e-health system, called MedFC, designed to promote OAM adherence. 34 The prototype system included a smartphone app for patients and a web-based system for clinicians. The smartphone app for patients included features to view the list of medications, access patient medication information leaflet, report and track medication adherence and side effects, and receive medication reminders. Using a web-based system that connected to the patient app via an online server, clinicians were able to build patients' medication list, set up medication reminders, and monitor their adherence and symptom reports. 34 Before commencing each interview, participants were given a brief introduction about the overall functions of the prototype and a chance to explore its different features by themselves. This was done in order to ensure familiarity with an adherence app.
Study participants
This study recruited patients and caregivers from the National Cancer Centre Singapore (NCCS), which is a multidisciplinary cancer care facility treating close to 70% of public sector cancer cases in Singapore. 35 Patients who were taking OAMs, 21 years of age or older, able to speak and understand English and had basic knowledge to use smartphones were eligible. Caregivers of eligible patients were also considered for participation. Spouses or caregivers were allowed to join the patient if the patient requested or agreed to their presence during the interview sessions.
Sampling techniques
During the initial phase of data collection, participants were purposively selected to take part in the study based on their willingness and ability to engage with the prototype adherence app and articulate their experiences and attitudes about the app. As the interviews progressed, the theoretical sampling approach was used to further develop the emerging categories based on analysis of initial interviews. 33 Potential participants were sought in such a way that subsequent interviews would further explicate the emerging grounded theory framework. As recommended by the grounded theory approach, the attainment of theoretical saturation, confirmed by absence of emerging categories in the last three interviews, was used as indicator to cease further participant recruitment.33,36
Data collection
Participant characteristics (N = 18).
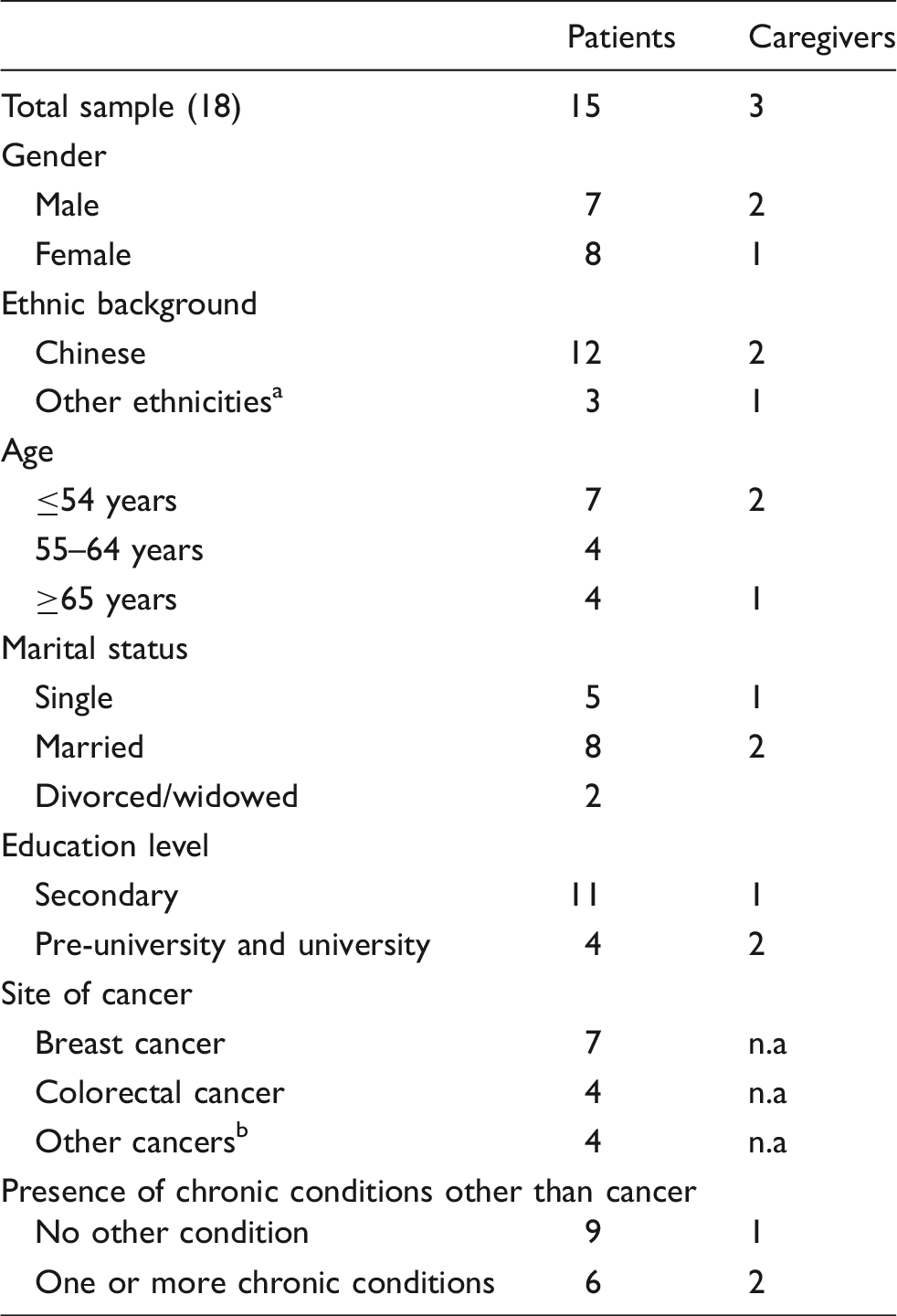
n.a: not applicable.
Other ethnicities: Malay, Indian, Arab.
Other cancers: liver, prostate, stomach.
Data analysis
The Qualitative Data Analysis software in family R (RQDA) was used for analysis. 37 Coding of the interview transcripts was done after each round of interview and followed the three stages (initial, focused and theoretical coding) described by Charmaz. 33 During the initial coding phase, interview transcripts were reviewed line-by-line to inductively identify specific ideas to be coded. As the study progressed, focused coding was done to identify categories based on central codes that emerged during the initial coding stage. In the theoretical coding stage, the theoretical code “intending to use adherence app” was used as an overarching theme that captured the categories identified in focused coding. The constant comparative analysis of codes and interview data was used to refine the final categories and their relations to one another. Coding was done primarily by EA who had a graduate-level training and experience in qualitative study methods. A second researcher, SC independently coded the transcripts, and comparison of interpretations was done. All researchers had access to the data and constant team meetings were held to discuss and compare interpretations. Throughout the process of analysis, extensive memos were written to document the meanings of the codes, distinctions between codes, their relation to the raw data and decisions regarding data collection and analysis. Memos were entered on RQDA, which enabled linking them to categories and codes that were in turn linked to lines of text in the transcripts.
Ethics approval and ethical issues
The SingHealth Centralised Institutional Review Board approved the study protocol, and all participants were included in the study after obtaining their written informed consent. Before commencing analysis, confidentiality of participants' responses was maintained by removing patient names and other potentially identifying information revealed during the interview.
Results
Intending to use adherence app: Considerations for acceptance
In the context of this study, participants' stated intention to use an app for the management of medication adherence determined their acceptance of the app. The factors that influenced participants' acceptance of an adherence app were classified into two categories: facilitating factors and hindering factors. The facilitating factors were identified to be: facing difficulty in maintaining adherence and getting superior features over current methods. In contrast, the hindering factors were: lower perceived competence in using app, having to pay and lacking options for different languages (Figure 1). Detailed description of the factors is provided below.
Intending to use adherence app: patients' and caregivers' perspectives on considerations for acceptance.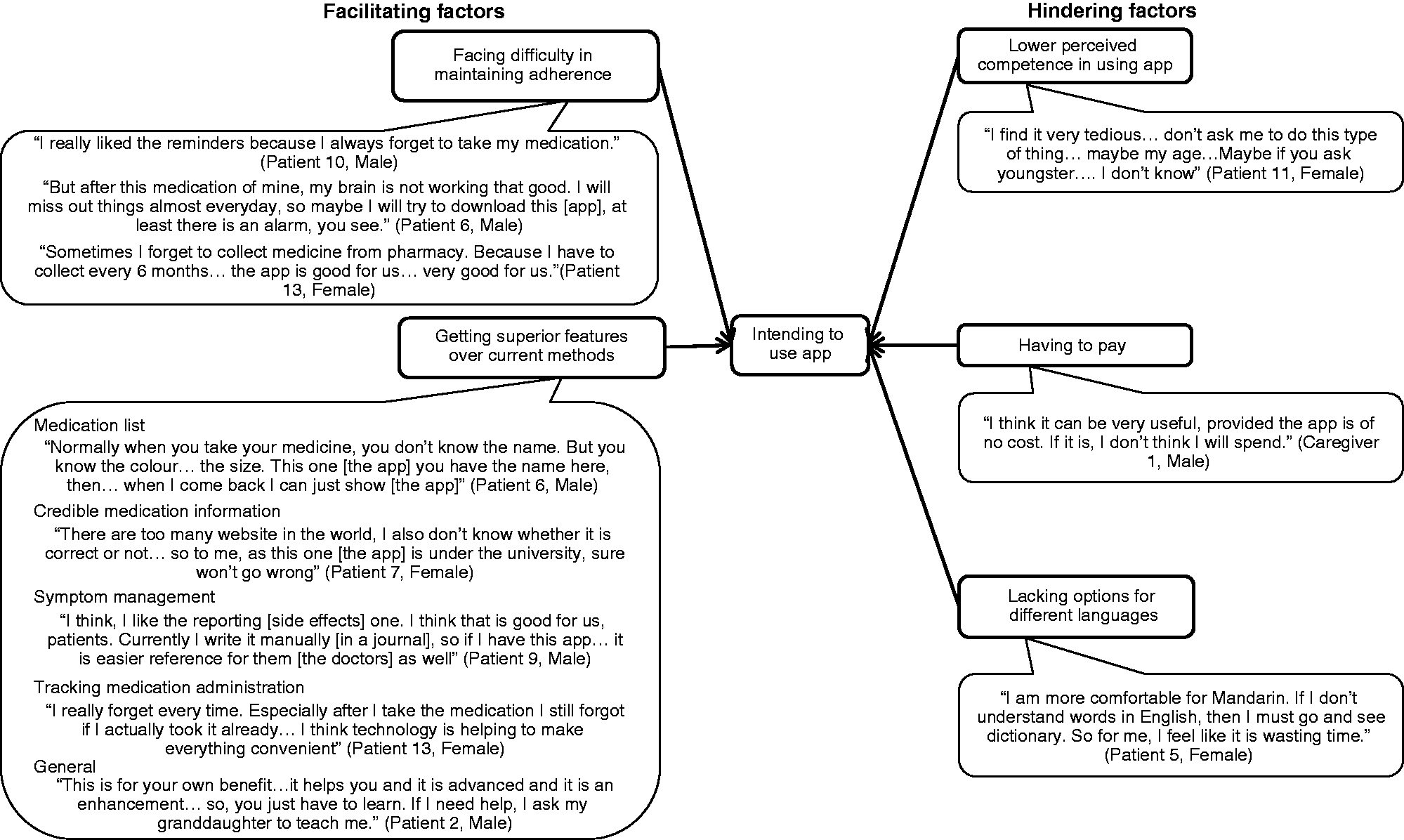
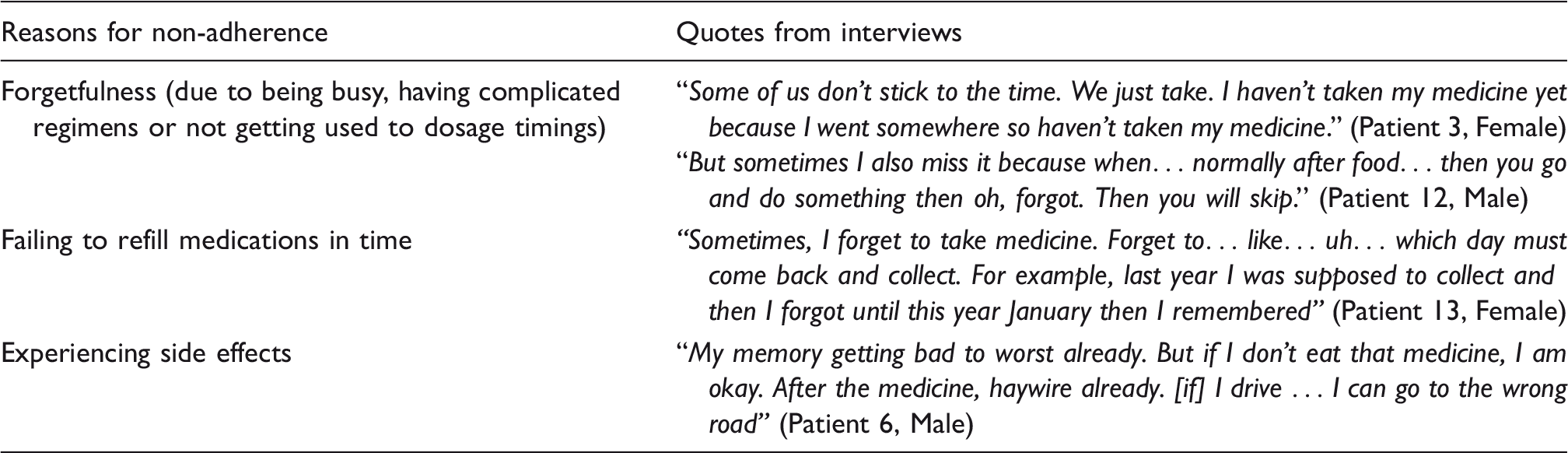
Facing difficulty in maintaining adherence
Patients' reasons for failing to maintain optimal adherence to oral anticancer medications.
Getting superior features over current methods
Strategies used by participants in managing oral anticancer medication-related problems.
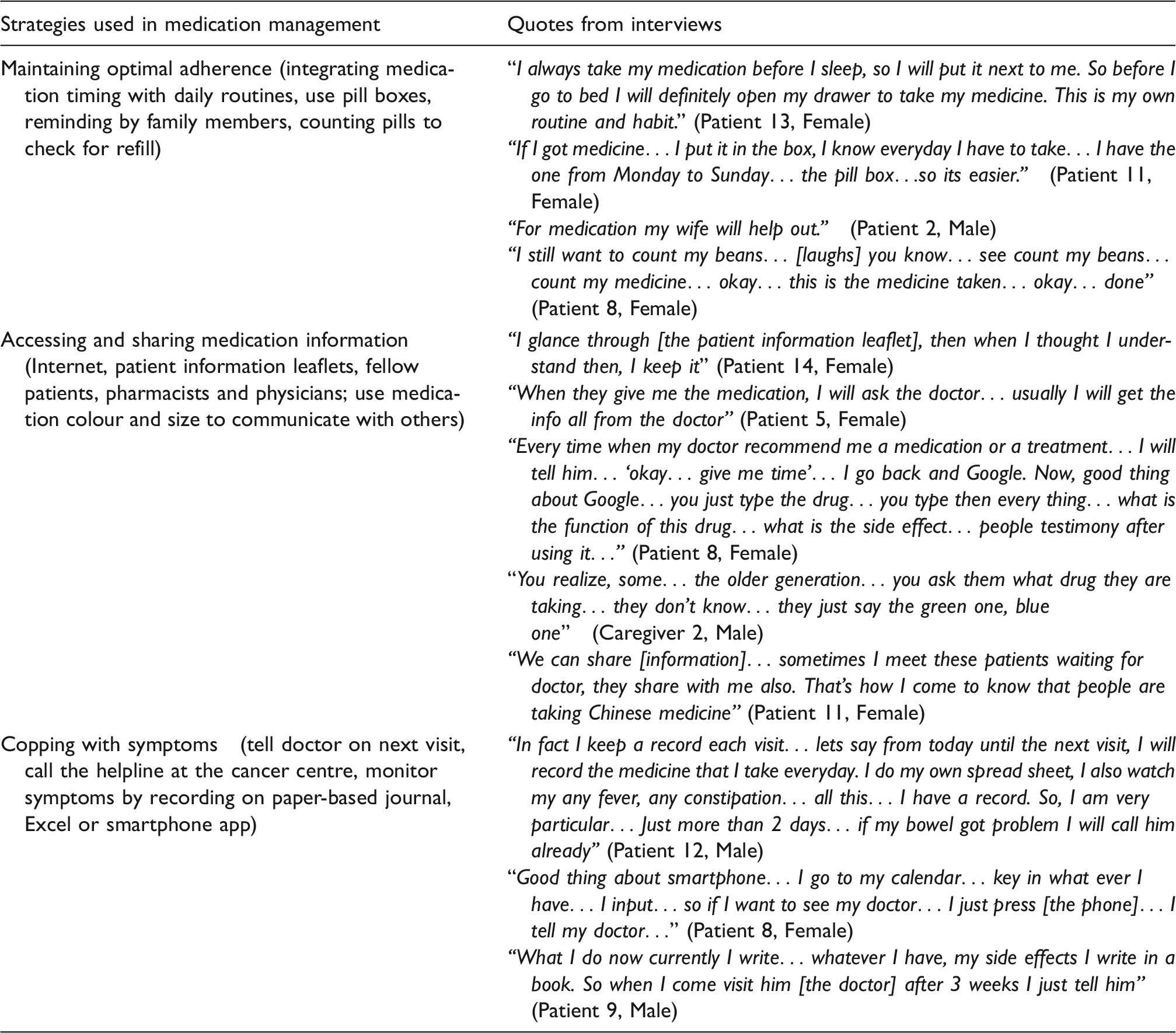
Participants expressed their intentions to use an adherence app because they thought it would either complement or be more useful than their current methods. Potential areas of superiority over participants' current methods as identified from the interviews were: readily available medication list, credibility of medication information, being able to communicate symptom management issues with clinicians and tracking medication administration (Figure 1). In some cases, using the app was considered better, as it was considered a more convenient and accurate reference to patient's list of medications and related information. Some participants explained their intentions to use the app from the point of provision of credible medication information when compared to their current sources of information. Reporting symptoms on an app that directly transmits to the hospital system was considered as a crucial feature that would compel patients to use the app. Participants, who relied on their own memory to remember medication timing, mentioned that they sometimes wondered if they had taken the previous dose of their medication at the time of the next dose or at the end of the day. That made them favour an app that could track medication administration and alert them if they were about to miss a dose (Figure 1).
Lower perceived competence in using app
Participants' belief in their ability to learn and apply skills in using an app was identified as an important barrier to using an adherence app. For some participants, trying to use an app was found to be too difficult (Figure 1). For others, their current skill levels were not that important in their decisions as they thought skills could be learnt by exploration of the different functions of the app by themselves or by seeking help from others.
Having to pay
Having to pay for an app was an important factor in participants' intention to use the app. For some participants, having to pay would discourage them from using the app (Figure 1), and for others, they would only be willing to pay for some specific features in the app that they found crucial.
Lacking options for different languages
The issue of language was raised from two important vantage points. For some, it was a matter of not being able to understand the language, and for others, it was just a matter of being more comfortable with a language other than what was used in the app. As the evaluated version of the app was available in English, the limited language option was identified to be a hindrance for acceptability (Figure 1).
Discussion
This study identified important considerations users make in their intentions to use an adherence app. The conceptual framework developed in this study suggested various facilitating and hindering factors to users' adoption intention of adherence apps. These findings make important contributions to the mHealth technology acceptance research and respond to the continued call for such research on apps and other tech-based tools for medication management. 11
Despite the use of a grounded theory analysis with an inductive approach and efforts to maintain reflexive thinking throughout the process, most of the factors identified in the study fit well within the models of unified model of health technology acceptance proposed by Sun et al. and the extended unified theory of acceptance and utilization of technology (UTAUT-2).26,31 Facing difficulty in maintaining adherence was an important facilitator of adoption intention. This matches with the suggestion by Sun et al. that perceived vulnerability influences behavioural intention to adopt an mHealth intervention. 26 Our study further confirms the importance of including health behaviour constructs in the evaluation of technology acceptance in healthcare settings. This is in line with recommendations, by Holden et al., to treat adoption of health technologies not only as an issue of technology acceptance behaviour but also as a health behaviour. 28 Studies also support the importance of getting superior features over current methods in users' adoption intention. 19 This concept corresponds with the constructs of perceived usefulness and performance expectancy identified in the unified model by Sun et al. and UTAUT-2, respectively.26,31 In this regard, our study provides contexts that need to be considered in the evaluation of user acceptance of adherence apps.
Requirements of payment to use an adherence app were found to be hindrance factors in adoption intention. These were also identified in the response cost and price value constructs of the unified model and UTAUT-2.26,31 This indicates that the cost of such apps should be seriously considered. Given the importance of medication adherence in the reduction of healthcare costs, health systems should also consider free provision of adherence apps to patients who can benefit most from them. 6 In line with other studies, our findings also suggest the effect of perceived competence in using an app on adoption intention.17,26,31 This finding implies the importance of designing user-friendly interfaces and the need to educate patients about how to use an app.
Implications for practice
Clinicians and developers of adherence apps should always remember the fact that many patients employ some methods to cope with their medication management needs. This necessitates designing solutions that have relative advantage over existing methods. Patients generally want enhanced features that offer better convenience, credibility, tracking capabilities and two-way communication with clinicians to enable management of side effects and adherence problems. Such demands go beyond the capabilities of most adherence apps, which focus on medication reminder functions. 10 At this point, it is important to note that the inclusion of additional features do not only facilitate user acceptance but also make the app more effective in improving adherence. This is because adherence is a complex issue influenced by patient knowledge, side effects and motivation to take medication, which necessitates the use of multi-component strategies to address it.4,5,9 Developers should also strive to meet the low level of technology competence and language requirements of potential patients by designing more user-friendly adherence apps with options for multiple languages especially in the context of multicultural environments. 10
Strengths and limitations
The use of a qualitative study design with the grounded theory approach provided an in-depth understanding of the factors that determine acceptability of an OAM adherence app. However, the findings of this study should be interpreted with some limitations in mind. First, it should be noted that the conceptual framework described in this study is based on participants' expressed intentions to use an adherence app, not actual usage. However, the effect of this limitation may not be that significant as various studies have consistently demonstrated that behavioural intention reliably predicts actual usage.24,28 Secondly, patients' opinions may vary with their cultural backgrounds and experiences. Although efforts were made in this study to ensure variations in opinions and depth of understanding, the applicability of the findings in other settings should be interpreted with caution. Further research with quantitative components is required to evaluate the effectiveness of the current conceptual framework in explaining behavioural intentions and continued utilisation of adherence apps in a variety of settings.
Conclusion
A conceptual framework of facilitating and hindering factors for adherence app adoption intention was developed in this study. This framework provides clinicians and app developers' insights on factors that influence the successful adoption of app-based interventions for medication adherence. Developers of adherence apps will benefit from engaging patients early in the design process as this will help in designing an app with relative advantages over patients' current methods. Implementation of app-based programs should also consider the financial, technological and language barriers for end users.
Supplemental Material
Supplemental material for User acceptance of an app-based adherence intervention: Perspectives from patients taking oral anticancer medications
Supplemental material for User acceptance of an app-based adherence intervention: Perspectives from patients taking oral anticancer medications by Eskinder Eshetu Ali, Sharlene Si Ling Chan, Jo Lene Leow, Lita Chew and Kevin Yi-Lwern Yap in Journal of Oncology Pharmacy Practice
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.