
Abstract
To our knowledge, this is the first population-based study on violence experience during pregnancy based on International Classification of Diseases (ICD)-10 classification. This study examined violence before, during, and after childbirth in Finland focusing on prevalence and risk factors. Based on the National Register Data from 2000 to 2020, 0.3% (3,485 of 1,177,569) of pregnant women were identified as having experienced violence. Violence was more common among vulnerable groups, such as young women and those with low socioeconomic status. The discrepancy between previous survey-based evidence and our ICD-based data on violence prevalence highlights the need for improved identification within healthcare.
Introduction
According to the World Health Organization (WHO), violence is a significant societal, social, and health problem that burdens healthcare systems and often remains hidden. Violence in close relationships is referred to as either domestic violence or intimate partner violence (IPV). The WHO defines IPV as the intentional use or threat of power, control, or physical force against another person, leading to physical or mental harm, impaired development, or death. IPV encompasses physical, psychological, sexual, economic, digital, and cultural forms of violence (WHO, n.d.). One in three women worldwide have experienced physical or sexual violence by an intimate partner or sexual violence from a non-partner during their lifetime, as reported by a recent systematic review and meta-analysis (Román-Gálvez et al., 2021).
Pregnancy is recognized as a potential risk period for intimate partner violence, as it may trigger the onset or escalation of violence within the family (Coutinho et al., 2015; O’Doherty et al., 2015). Previously cited systematic review and meta-analysis by Román-Gálvez et al. indicated that 25% of pregnant women have experienced some form of violence. Based on the available data, the estimated prevalence of physical violence during pregnancy was 9.2%, psychological violence was 18.7%, and sexual violence was 5.5% (Román-Gálvez et al., 2021). Another systematic review and meta-analysis found that physical violence is more prevalent during the perinatal period, while psychological violence is most common throughout life (White et al., 2024). Experiences of violence are recurrent, and women who have experienced violence before pregnancy are more likely to experience it during and after pregnancy as well (Finnbogadóttir et al., 2014; White et al., 2024).
Based on a recent scoping review, several sociodemographic risk factors for IPV during the perinatal period have been identified in the Nordic countries (Finnbogadóttir et al., 2024). Younger age and low educational level were identified as significant risk factors for IPV. Being unemployed or facing financial distress also increases the risk of experiencing IPV. Women who are single or not cohabiting with a partner were more likely to be exposed to violence. Importantly, although overall IPV prevalence is relatively high in the Nordic countries, the review found that women who live in the Nordic countries but were born outside the Nordic region experience higher levels of violence compared with Nordic-born women. A history of miscarriages, abortions, or unplanned pregnancies were additional risk factors during the perinatal period. Lifestyle factors such as smoking, alcohol consumption, and illicit drug use during pregnancy were also linked to an increased risk of IPV. Furthermore, having a pre-pregnancy body mass index (BMI) of 30 kg/m2 or higher was associated with a higher likelihood of experiencing violence during pregnancy (Finnbogadóttir et al., 2024).
Although the Nordic countries are ranked among the most equal countries in the world, they have the highest prevalence of IPV in the European Union (EU) (Wemrell et al., 2019). In Nordic countries, gender equality means that people of all genders have equal rights, responsibilities, and opportunities in all areas of life. This paradox highlights that even in societies where everyone is guaranteed equal possibilities and rights regardless of gender, intimate partner violence can remain a significant problem. According to the European Union gender-based violence survey, 52% of women in Denmark, 47% in Finland and 46% in Sweden reported experiencing physical and/or sexual violence during their lifetime (FRA, EIGE & Eurostat, 2024). During pregnancy, the prevalence of IPV varied from 8.5% in Denmark (Andreasen et al., 2023) to 5% in Norway (Sørbø et al., 2013), 3.3% (prenatally and during pregnancy) in Iceland (Lukasse et al., 2014), and 2.5% in Sweden (Finnbogadóttir & Dykes, 2016).
To the best of our knowledge, and as supported by a recent review article, the exposure of pregnant women to IPV during pregnancy has not been systematically investigated applying scientific methods in Finland (Finnbogadóttir et al., 2024). The aim of this study was to investigate the prevalence and risk factors for exposure to violence during the period of 2 months preceding pregnancy, during pregnancy, and the 2 months following childbirth based on real-world evidence gathered from population based national registers covering the period from 2000 to 2020. The main outcome of the study was having a diagnosis indicating exposure to violence, based on the International Classification of Diseases, 10th Revision (ICD-10) criteria. It is also important to form a comprehensive picture of violence during pregnancy in Finland.
Methodology
Data Collection
The data for this study were collected from the Finnish Medical Birth Register (MBR), established in 1987 and maintained by the Institute for Health and Welfare (The Finnish Institute for Health and Welfare (THL), n.d.). The MBR collects extensive data to support safety and quality of maternity and neonatal care with improved and highly reliable data quality due to reforms in 1990, 1996, 2004, and 2017. The register includes information on all live births and stillbirths (birthweight ≥ 500 g or gestational age ≥ 22 weeks), demographics and personal data of pregnant women, details on current and previous pregnancies, and infant data such as birthweight, health status, and interventions during the first week. Data are collected prospectively from hospitals, verified for accuracy, and discrepancies are corrected, ensuring the register is a robust source for research and healthcare planning.
The data gathered from the MBR were supplemented with information on socioeconomic status (SES) from Statistics Finland (Statistics Finland, n.d.) and the ICD-10 criteria ICD-10 diagnoses of violence during the 2 months before pregnancy, throughout pregnancy, and the 2 months after childbirth from the Hospital Discharge Register (HDR) kept by (THL). Encrypted personal identification numbers, unique for each parturient, were used to link the different data sources.
Population
Study population included information on all 1,177,569 births occurred in Finland in 2000‒2020.
Variables
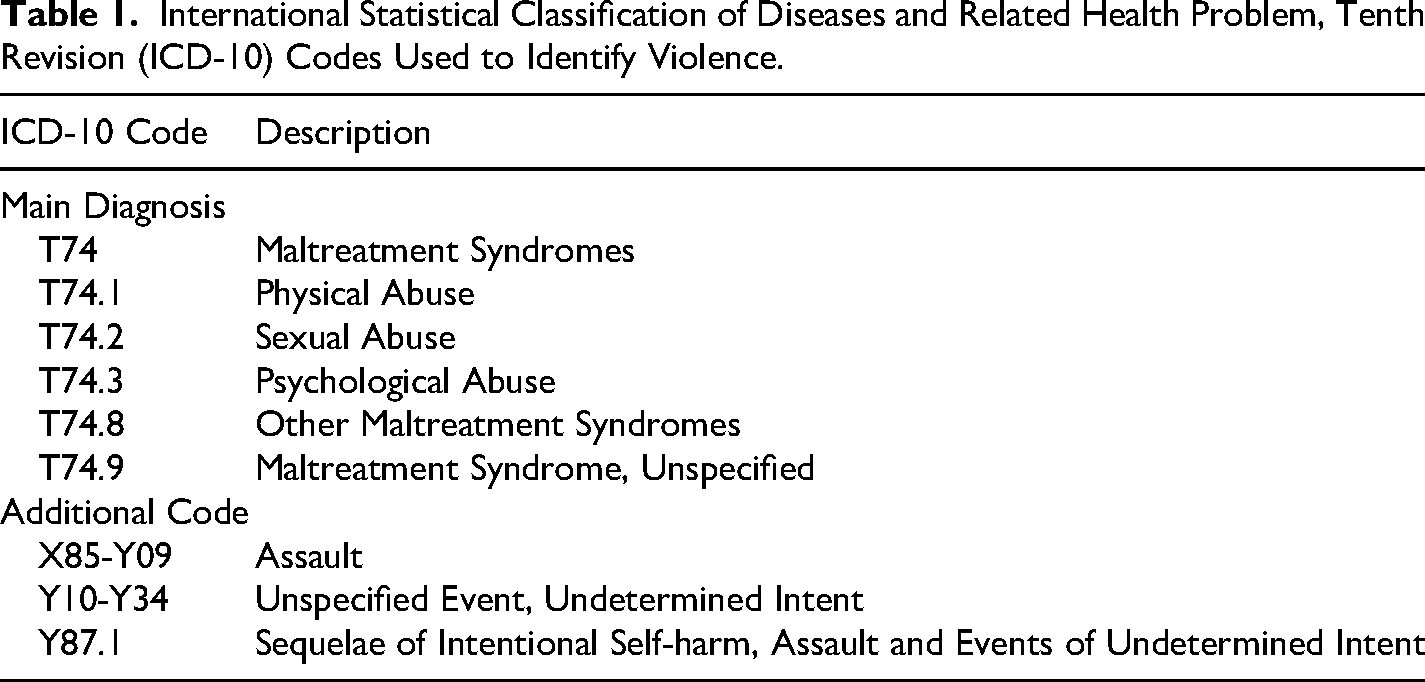
Cases of violence during pregnancy were identified using the main ICD-10 classification diagnoses T74.0-T74.3, T74.8, and T74.9, along with additional codes X85-Y09, Y10-34, and Y87.1 (Table 1), from the MBR and the Hospital Discharge Register. For this study, all ICD-10 diagnoses were pooled and recoded as “yes” if any of the ICD-10 diagnoses were reported, and “no” if none were reported, during the 2 months before pregnancy, throughout pregnancy, and the 2 months after childbirth. ICD-10 codes were used throughout the study period, and no revisions to the coding system were implemented. Prevalences of violence were determined separately for the periods of 2 months before pregnancy, during the first, second, and third trimesters of pregnancy, and 2 months after birth. Additionally, the prevalence of violence was analyzed for the entire study period and separately for four-time intervals: 2000‒2005, 2006‒2010, 2011‒2015, and 2016‒2020.
International Statistical Classification of Diseases and Related Health Problem, Tenth Revision (ICD-10) Codes Used to Identify Violence.
Other variables used in the statistical analyses as covariates were maternal age in years at birth categorized as ≤19, 20‒29, 30‒39 (reference group), and ≥40 years, parity categorized as nulliparous (no previous births) and multiparous (≥1 previous births, reference group), and number of fetuses categorized as one (reference group) or two or more.
Data on the SES reflect a person's position in society, assessed through education, occupation, or employment. For this study, SES was categorized as follows: self-employed (reference group), upper-level employees, lower-level employees, manual workers, students, pensioners (women who are unable to work due to long-term illness or disability), long-term unemployed, others, and unknown. The “others” category included mothers whose occupations could not be classified or mothers who had never worked.
Self-employed persons are those who were engaged in economic activities on their own account and at their own risk. They could be self-employed with employees or without employees, such as own-account workers or freelancers. Upper-level employees work in various expert and managerial roles and typically have university degrees. Lower-level employees generally do not have university degrees and work in office, sales, or healthcare roles. Long-term unemployed referred to women who have been unemployed for at least 6 months, while those unemployed for less than 6 months are classified according to their previous occupation. Women with missing data were classified separately under the category missing.
Marital status was categorized as unmarried (reference group), married, divorced, widowed, and missing information. Gestational diabetes (GDM) was categorized as yes or no (reference group), and in vitro fertilization (IVF) was categorized as yes or no (reference group). Tobacco smoking was categorized as yes or no, and women with missing information were classified under the missing category. Data on tobacco smoking habits were collected during maternity care visits, which are offered free of charge to all pregnant women.
Statistical Analyses
Descriptive analyses to study association between the outcome (violence) and confounding variables (defined above) were reported in numbers and percentages. To examine whether the prevalence of violence, defined based on ICD-10 diagnoses as defined above, changed significantly over time, we conducted a chi-square test of independence. A P-value of <.05 was considered indicative of statistical significance.
Multivariable analyses to study effect of confounding variables on the outcome (violence) were performed using logistic regression analysis with the backward selection method. Both crude and adjusted odds ratios (aOR) with 95% confidence intervals (CIs) were determined. Covariates included in the analyses were maternal age, parity, SES, marital status, tobacco smoking, number of fetuses, GDM, and IVF. All analyses were performed using IBM SPSS Statistics 27.
Ethical Issues
In Finland, the secondary use of health data is regulated by Act on the Secondary Use of Health and Social Data (Findata, Social and Health Data Permit Authority, 2023). Data access was granted based on the study plan approved by Statistics Finland and the Finnish Institute of Health and Welfare in 2021 (TK/1137/07.03.00/2021, THL/4455/14.02.00/2020). Data were analyzed in a secure environment Kapseli maintained by Statistics Finland. Since the study subjects were not contacted, ethical committee statement was not required for register-based studies in Finland.
Results
The study population included all 1,177,569 births in Finland from 2000 to 2020. Violence was observed in 0.29% (n = 3,485) of the pregnancies over the entire study period, with an increasing trend: 0.13% (456 of 340,521) in 2000‒2005, 0.22% (653 of 299,947) in 2006‒2010, 0.35% (1,026 of 292,203) in 2011‒2015, and 0.55% (1,350 of 244,898) in 2016‒2020 (P < .001) (Table 2). Of these women, 9.2% (321 of 3,485) had experienced violence also in their previous pregnancies.
Prevalence of Births (N = 1,177,569) With Diagnosis of Violence During the 2 Months Before Pregnancy, Throughout Pregnancy, and the 2 Months After Childbirth in Finland in 2000–2020.
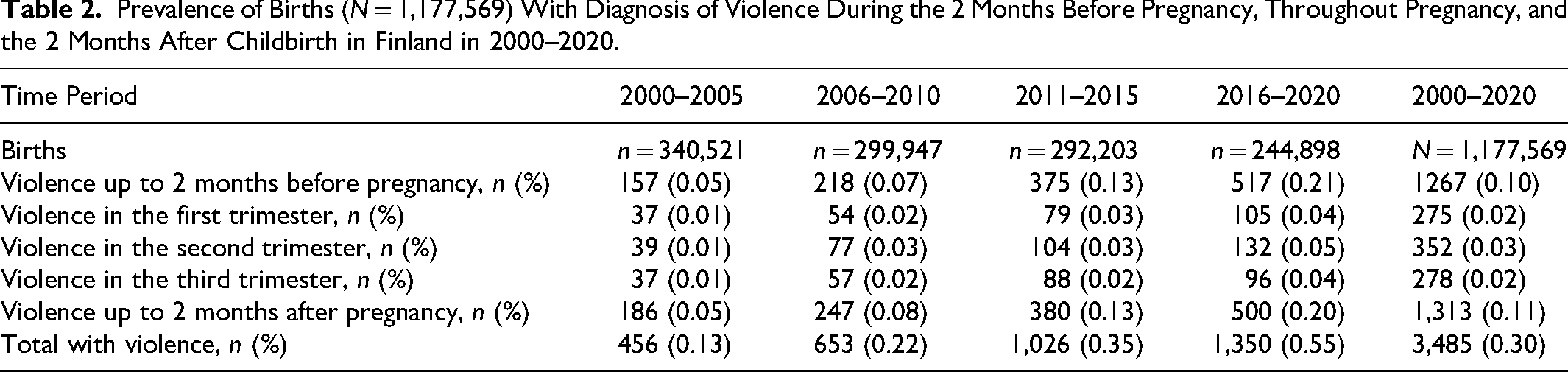
IPV in relation to pregnancy and childbirth across the entire period was reported as follows: IPV prevalence was recorded as 1,267 cases (0.1%) up to 2 months before pregnancy. During pregnancy, prevalence was recorded as 275 cases (0.02%) in the first trimester, 352 cases (0.03%) in the second trimester, and 278 cases (0.02%) in the third trimester. After childbirth, IPV prevalence was recorded as 1,313 cases (0.11%) within 2 months postpartum (Table 2).
The distribution of maternal demographics, tobacco smoking during pregnancy, and obstetric risk factors are reported in Table 3. Maternal age ≤19 years was associated with a 2.8-fold increase (aOR 2.83, 95% CI 2.47‒3.24) and age 20‒29 years with a 1.4-fold increase (aOR 1.38, 95% CI 1.28‒1.50) in the prevalence of violence compared to age 30‒39 years. Nulliparous women had a 1.1-fold increase (aOR 1.12, 95% CI 1.04‒1.21) in the prevalence of violence compared to parous women.
Risk Factors for Violence During the 2 Months Before Pregnancy, Throughout Pregnancy, and the 2 Months After Childbirth in Finland in 2000–2020.
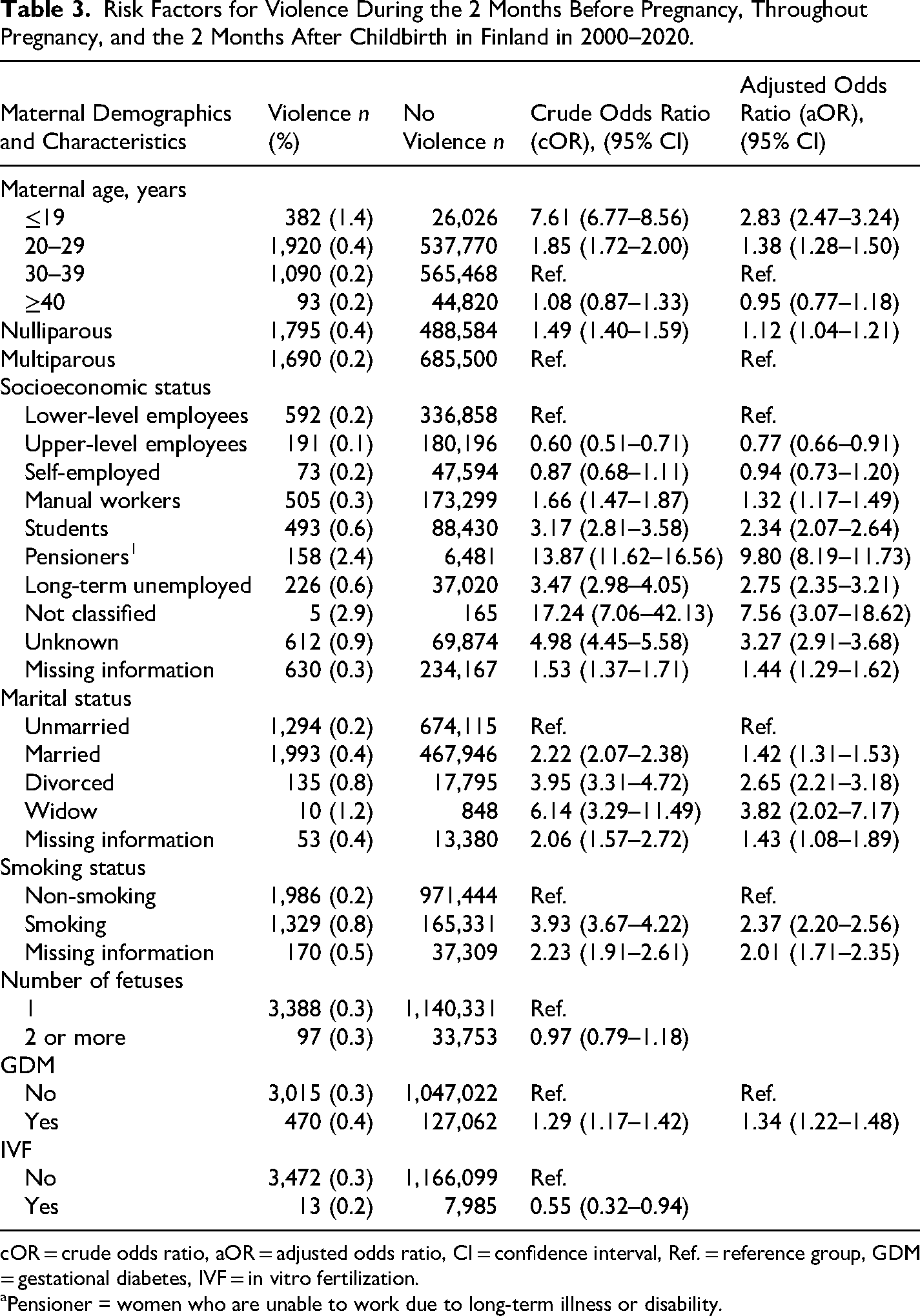
cOR = crude odds ratio, aOR = adjusted odds ratio, CI = confidence interval, Ref. = reference group, GDM = gestational diabetes, IVF = in vitro fertilization.
Pensioner = women who are unable to work due to long-term illness or disability.
Upper-level employees had the lowest prevalence of violence throughout the study period. In contrast, women on long-term illness or disability pension had a 9.8-fold increase (aOR 9.80, 95% CI 8.19‒11.73), the long-term unemployed had a 2.8-fold increase (aOR 2.75, 95% CI 2.35‒3.21), students had a 2.3-fold increase (aOR 2.34, 95% CI 2.07‒2.64), and those with unclassified or unknown information on SES had up to a 7.6-fold increase (aOR 7.56, 95% CI 3.07‒18.62) in the prevalence of violence compared to lower-level employees, as reported in Table 3.
The prevalence of violence in married women was 1.4-fold (aOR 1.42, 95% CI 1.31‒1.53) compared to unmarried women, who had the lowest prevalence of violence. In divorced women, the prevalence of violence was 2.7-fold (aOR 2.65, 95% CI 2.21‒3.18), and in widows, it was 3.8-fold (aOR 3.82, 95% CI 2.02‒7.17) compared to unmarried women. Tobacco smoking was associated with a 2.4-fold increase (aOR 2.37, 95% CI 2.20‒2.56) in the prevalence of violence compared to non-smoking. Having GDM was associated with a 1.3-fold increase in the prevalence of violence (aOR 1.34, 95% CI 1.22‒1.48) compared to women without GDM.
Discussion
In Finland, ICD-10 diagnoses indicating exposure to violence were recorded for 0.3% of pregnant women before, during and after pregnancy between 2000 and 2020. The prevalence increased from 0.13% in 2000–2005 to 0.55% in 2016–2020 (P < .001). To our knowledge, this is the first population-based study to examine violence during pregnancy using ICD-10 diagnoses. Our findings show a clear discrepancy between ICD-coded data and previous survey-based evidence from Finland (Siltala et al., 2023). Their study found that about half of Finnish women have experienced violence during their lifetime, highlighting the seriousness of the issue. While their focus was on lifetime exposure, our study examined violence during pregnancy, a known high-risk period for IVP. The low prevalence in our data likely reflects underreporting rather than a true reduced risk (WHO, 2011). In different countries and cultures, also over time, women can experience and report IPV differently.
Compared to other previous studies from the Nordic countries, the reported prevalence of violence during the 2 months preceding pregnancy, during pregnancy, and the 2 months following childbirth appears remarkably low. In these countries, the prevalence of IPV during pregnancy ranged from approximately 2.5% to 8.5%, with all studies relying on anonymous questionnaire-based data collection (Andreasen et al., 2023; Finnbogadóttir & Dykes, 2016; Lukasse et al., 2014; Sørbø et al., 2013).
Overall, it seems plausible that violence is more readily disclosed in survey settings than in direct communication with healthcare professionals (Keynejad et al., 2021). It has also been suggested that healthcare personnel may hesitate to inquire about violence, even when it appears likely based on observed injuries (Keynejad et al., 2021; Olive, 2017), particularly as clinical focus often remains on treating physical symptoms, while organizational support, clear protocols, and comprehensive understanding of the complex nature of violence may be lacking (Siltala et al., 2023). It is credible that ICD-10 codes within the healthcare system are applied using stricter criteria, prioritizing the most severe and physically evident cases, in contrast to self-reported data from surveys. Even when violence is recognized by healthcare professionals, an ICD diagnosis code may not be assigned, as violence is considered a criminal matter and may be perceived by staff as beyond their professional responsibilities. Furthermore, our data only include hospital settings, excluding cases treated in primary care. It is also important to consider that individuals’ previous experiences with different forms of violence—physical, emotional, or sexual—can influence how they define and identify violence (Gilgun, 2008).
Our results show that pregnant women in certain vulnerable positions, such as students, the long-term unemployed, women on long-term illness or disability pension, those with missing socioeconomic information, as well as young women (<30 years) had more diagnoses indicating violence than women over 30 years of age, lower or upper-level employees, or self-employed pregnant women. These findings are consistent with several previous studies conducted in the Nordic countries, where all residents have universal access to health care services (Finnbogadóttir et al., 2024; Siltala et al., 2023). It could be speculated that violence has been monitored more closely in these groups than among upper-level employees with the highest SES. Furthermore, when pregnant women face coping challenges or are already social work clients, it may be that exposure to violence has been screened more thoroughly and therefore, identified more often than in non-vulnerable pregnant women. However, previous studies have reported that violence occurs in all social classes (Keynejad et al., 2021).
Based on a Cochrane review, there is evidence that screening for violence in healthcare settings doubles the number of women identified as experiencing abuse (O’Doherty et al., 2015). There is also evidence that improving the healthcare response to intimate partner violence requires a more comprehensive understanding of its complex effects on patients. The development of organizational-level practices, such as clear and consistent protocols, interprofessional collaboration, and systematic training, has been highlighted as essential interventions. Furthermore, creating a supportive and safe environment for disclosure, where patients are met with empathy and respect, may enhance trust and facilitate earlier identification and intervention (Husso et al., 2012; O’Doherty et al., 2015; Virkki, 2015; Virkki et al., 2015).
Strengths and Limitations
The main strength of the present study lies in the use of real-world data, covering all pregnancies ending into a birth in Finland from 2000 to 2020, and the ability to link information from several high-quality, population-based registers (Sund, 2012). To the best of our knowledge, these findings are novel, as population-based data on violence prevalence documented using ICD-10 codes have not been previously reported. Additionally, in Finland data on follow-ups during pregnancy and childbirth are collected prospectively in the MBR enhancing the validity of the data.
We have identified some limitations related to the present data that are likely to affect reported prevalence of violence. There are shortcomings in the diagnosis and reporting of cases of violence in healthcare in Finland. In particular, the use of additional codes is still low. A case of violence may have been registered with a diagnosis other than the violence codes (Kivelä, 2020). Further, we do not have accurate information about whether violence was related to intimate relationships. However, it is extremely rare in Finland for a pregnant woman to be subjected to violence without knowing the perpetrator. In Finland, the perpetrator of violence against women is usually a spouse or ex-spouse (Siltala et al., 2023). Furthermore, while register-based data are prone to errors and missing values, the proportion of missing values in this study was very low, less than 1% of the covariates.
Conclusions
IPV is a significant public health issue that affects women across all social and demographic groups, including those in gender-equal societies. In our nationwide cohort, which included all births in Finland from 2000 to 2020, 0.3% of women were identified as having experienced IPV during pregnancy based on healthcare records. However, this proportion is considerably lower than the lifetime prevalence of IPV, estimated at approximately 50% in a recent survey (Siltala et al., 2023), and likely reflects underreporting and limited detection in clinical settings. Experiences and reporting of IPV can vary across countries, cultures, and over time.
In our data, the prevalence of IPV increased markedly over the two decades studied. The prevalence rose from 0.13% in 2000–2005 to 0.55% in 2016–2020, representing more than a four-fold increase, relative risk, RR 4.12, 95% CI 3.70–4.58 (data not shown). This substantial rise highlights a growing need for improved identification, documentation, and support for women experiencing IPV during pregnancy.
Importantly, our findings indicate that pregnancy does not protect against IPV; violence can occur before, during, and after pregnancy. Known risk factors for IPV include young maternal age, low SES, nulliparity, tobacco use, and gestational diabetes. Although IPV during pregnancy appears less frequently in clinical data, global evidence shows that pregnancy and the postpartum period are high-risk times for IPV onset and escalation (WHO, 2011). Systematic screening and improved professional awareness are essential to enhance identification and support. Strengthening healthcare responses to IPV during pregnancy is critical for safeguarding maternal and child health.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the OLVI-Säätiö (grant number 20220397).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.