
Abstract
This study examined Queensland Suicide Register cases from 2000 to 2017 involving histories of intimate partner violence (IPV). Overall, 629 individuals, representing 14.7% of suicides, had perpetrated or were alleged to have perpetrated IPV. Most were men (92.7%), and Indigenous peoples were overrepresented (18.3%). Many had communicated suicidal intent (61.4%) or sought mental healthcare before death (43.9%). Autopsies commonly showed substance misuse, including alcohol, prescription, and illicit drugs. Key antecedents included domestic violence orders, receiving legal documents, and relationship conflict or separation. Factor analysis revealed three themes: chronic mental illness, youth with untreated drug use, and legal proceeding with long-term separation.
Responses to violence have taken a categorical approach, assigning those who engage in violence toward themselves to mental health facilities and those who are violent toward others to prison. The “mad, bad or sad” are incarcerated or institutionalized depending on perceptions of their reasons for offending (Bills, 2017; Lamb & Weinburger, 2017). Despite research dating back to the thirteenth century on the co-occurrence of interpersonal and self-directed violence, this legacy of separation remains in many initiatives for suicide and interpersonal violence prevention (Bills, 2017). The overlap in dangerousness to oneself and to others is often not considered: suicidal people may be of high risk to others as well as themselves.
This overlap occurs with intimate partner violence (IPV) and suicide. For the purposes of this paper, IPV is defined as attempted, threatened, or actual violence committed against a current or former romantic partner and can take the form of physical, sexual, and emotional abuse as well as intimidation and control (see Heyman et al., 2015, 2018). IPV and suicide are both prevalent public health concerns. In Australia, the context for this study, one in four women, and one in 14 men, have experienced IPV since age 15 (Australian Bureau of Statistics, 2023). In 2024, suicide was the 16th leading cause of death in Australia, with 3,307 deaths classified as suicide nationwide (Australian Bureau of Statistics, 2024). The high prevalence of both IPV and suicide underscores the need for further research examining the relationship.
The Australian Context
Australia is the sixth largest nation in the world by land area. Its population is around 27 million people characterized by a diverse demographic composition. The majority of residents are of European descent and there are significant Asian and other migrant communities. Most people live in a small number of very large cities and in urban areas (Australian Bureau of Statistics, 2025). Queensland, the state in which this research was conducted, has a population of 5.67 million people and is in the North of Australia. Economically, Australia is a high-income, developed economy and is among the highest for per-capita incomes globally. Despite this, wealth disparities remain, and there are large socio-economic differences between Indigenous and non-Indigenous populations in particular.
The disparity between Indigenous and non-Indigenous Australians is complex and influenced by the enduring impacts of colonization (Australian Institute of Health and Welfare [AIHW], 2019). Colonization disrupted established social and cultural systems through forced removals, mission life, and sustained government control—undermining traditional authority structures. Policies such as land dispossession and the removal of children into state care caused widespread trauma, transmitted across generations, contributing to higher rates of mental illness, substance use, and difficulties with emotional regulation. Ongoing socioeconomic disadvantage affects access to housing, education, and healthcare with poverty, overcrowding, and financial stress further increasing vulnerability. These challenges are compounded by racism and mistrust of institutions, which can deter help-seeking (AIHW, 2019). Geographic context also plays a role, as Indigenous peoples living in very remote areas often experience different family structures, opportunities, and access to services compared with those in metropolitan settings.
Indigenous Australians have higher rates of IPV and suicide. Research shows Indigenous peoples are more than twice as likely to die by suicide as non-Indigenous people; this rate is even higher in young men (De Leo et al., 2011). Further, Indigenous peoples seem to be less likely, or able, to access help for mental health and substance use problems (Sveticic et al., 2012). Indigenous peoples are also more likely to be victims of IPV. For example, Orr et al. (2021) looked at IPV rates in Western Australia, in which just 3% of the population are Indigenous. They found that for mothers identified as victims of IPV in police data, 44% were Indigenous, and of victims within health data, 73% were Indigenous (see also Orr et al., 2022). This pattern is also shown in IPV escalation. In the Northern Territory, Kerr et al. (2017) found less than 2% of White offenders had three or more incidents in 4 years compared with 32.4% of Indigenous offenders. Similarly, the homicide rate from IPV for Indigenous peoples is far higher than would be expected by proportion of the population (Serpell et al., 2022). This literature demonstrates a need for the investigation of IPV and suicide in Indigenous peoples.
Understanding Suicide and IPV
According to U.S. National Violent Death Reporting System data, IPV contributes to around one in 10 violent deaths, with 39.3% of these being homicides, 11.4% homicide-suicides, and 29.8% suicides (Kafka et al., 2021). The co-occurrence of intra- and interpersonal violence has been consistently shown in the literature, with emerging research suggesting those who commit both forms of violence (often termed “dual-harm”) may have distinct characteristics distinguishing them from perpetrators of only one form of violence (Shafti et al., 2021). Despite lacking an agreed upon theory of this dual-harm construct, researchers have hypothesized models to explain why some individuals exhibit both self-harm and aggressive behaviors; many with overlapping features using a biopsychosocial framework (see Hillbrand, 2014).
Shafti et al. (2021, 2023) proposed a cognitive-emotional model of dual-harm providing a framework for how distal and proximal processes interact, leading to dual-harm. Distally, biological vulnerabilities and environmental factors like adverse childhood experiences combine to develop personality styles that predispose individuals to harmful behaviors. Proximally, these personality styles lead to emotional and interpersonal problems that increase the likelihood of engaging in violence to regulate negative emotions. Critically, this theory incorporates the idea of using violence (toward self and others) to serve an interpersonal purpose, such as establishing autonomy or responding to grievances.
Research examining suicide and IPV specifically aligns with these theories. Barber et al. (2008) sampled 1,503 homicide incidents, and although less than 5% were followed by the perpetrator's suicide, among men who killed intimate or former partners with a firearm, 59% killed themselves (Barber et al., 2008; see also Belfrage & Rying, 2004; MacIsaac et al., 2018; Vatnar et al., 2021). A psychiatric in-patient study found over 90% of suicidal inpatients reported IPV perpetration and victimization in the past year, with most reporting severe and bidirectional IPV (Heru et al., 2006).
Fitzpatrick et al. (2022) used mixed methods for an Australian study examining suicide cases with IPV histories. They found a cumulative, interwoven effect of violence, mental illness, alcohol, and other drug use. These factors contributed to perpetrators’ emotional and interpersonal problems. These included, for some men, fragile masculine identities, fear of abandonment, and a need for control, especially in the context of divorce and custody battles. Similarly, River and Flood (2021) explored emotional styles in men who attempted suicide, and identified learned masculine ideals involving concealing emotions like sadness, while displaying emotions like anger, facilitated violence toward oneself and others. Fear, distress, and sadness were seen as a threat to masculine identities, while annoyance, anger, and rage were viewed as acceptable emotions. This resulted in men engaging in violence toward others as a way of validating their masculine identity. Similarly, nonmasculine emotions were concealed to preserve masculinity, with some resorting to tactics like alcohol and suicide attempts to numb their distress rather than seeking help.
Preserving masculine identities was not the only interpersonal function violence served. Cases from Fitzpatrick et al. (2022) revealed violence and threats of suicide were commonly used to control intimate partners. In some cases, the completed suicides appeared to be intended as a form of punishment and a way to inflict guilt on their partners, as shown by damaged personal items or spiteful messages left at the scene. Similarly, in the three suicide cases examined by River and Flood (2021) where IPV was present, two used suicide as a means of punishing their former partners. Two of the most prevalent intersecting factors for IPV and suicide were mental health problems and substance use.
Mental Health Problems
Mental illness commonly underpins suicide. A recent U.S. study (Schmutte et al., 2021) investigated 174,001 suicide deaths across 37 states and territories from 2003 to 2017. Suicide deaths were more common with people experiencing “serious mental illness.” Serious mental illness was defined as a diagnosis of schizophrenia and/or bipolar disorder, and 8.7% of the suicides had a known serious mental illness. A further 33.0% had other known mental illness—depression/dysthymia, anxiety disorder, obsessive-compulsive disorder, post-traumatic stress disorder, attention-deficit/hyperactivity disorder, or eating disorder. Similar findings have been reported in other samples (e.g., Chesney et al., 2014). The most frequent precipitating factor, observed in roughly 25% of suicides, was intimate partner relationship problems (Schmutte et al., 2021).
A similar pattern exists regarding mental illness and violence. Previous literature has found perpetration of violence associated with mental illnesses such as psychotic disorders (Honings et al., 2016), post-traumatic stress disorder (Hahn et al., 2015), and personality disorders (Collison & Lynam, 2021). Dean et al. (2024) examined violence victimization and perpetration following the onset of mental disorders using the Danish national register and police records, and found personality disorders, substance use disorders, and schizophrenia-spectrum disorders were highest risk. Furthermore, Sariaslan et al. (2020), in a Swedish nationwide cohort study, investigated violence in 250,419 people with psychiatric disorders by comparing them with a matched nonpsychiatric population as well as biological siblings. The disordered population was found to be four times more likely to perpetrate violence, after adjusting for birth order, familial confounders, and individual histories of violence.
Regarding IPV specifically, Hahn et al. (2015) conducted a longitudinal study of 11,625 U.S. men and found individuals experiencing post-traumatic stress disorder were at a significantly higher risk of perpetration. Collison and Lynam's (2021) meta-analysis, including 163 articles, found significant links between IPV perpetration and all personality disorders except histrionic and obsessive-compulsive personality disorders. Antisocial and borderline personality disorders had the strongest relationship with IPV. Yu et al. (2019) followed men with mental illness in Swedish nationwide registries. All psychiatric diagnoses were associated with an increase in IPV. Men with schizophrenia-spectrum disorder, bipolar disorder, depressive disorder, anxiety disorder, and personality disorder were more likely to commit IPV than matched controls (for similar findings, see Arsenault et al., 2000). Comorbid substance misuse also played a significant part in these studies.
Substance Use
There appears to be a strong association between substance use disorders and suicide. Esang and Ahmed (2018) claim suicide risk is increased 10–14 times for people with substance use disorders compared with the general population. Schneider (2009), in a review of psychological autopsy studies, reported substance use disorders were present in between 19% and 63% of suicides depending on the sample, with polysubstance use relevant to many cases. Chesney et al.’s (2014) meta-analysis found suicide risk was highest with opiate use and alcohol use disorder, respectively. Cocaine, amphetamines, and cannabis use were also associated with higher likelihood of suicide. An Australian psychological autopsy study found one in five suicides in Queensland and New South Wales involved decedents with alcohol-use disorders (Kõlves et al., 2017). Relevant to IPV, this research found suicides involving alcohol-use disorder were more likely to follow serious arguments with intimate partners and infidelity than suicides without alcohol-use disorder. Similarly, Graham et al. (2025), utilizing the U.S. National Violent Death Reporting System, identified that IPV-related suicides more frequently had perceived alcohol and/or substance use problems compared to suicides without IPV circumstances.
Specific evidence exists concerning substance use and IPV. Research has identified links to IPV for a variety of substances, such as alcohol (Choenni et al., 2017; Grigorian et al., 2020), performance-enhancing drugs (Ganson et al., 2022), and cannabis (Dellazizzo et al., 2020). The previously mentioned Yu et al. (2019) study, examining instances of IPV perpetrated by men against women, found men with substance use disorders, as a principal or comorbid diagnosis, had the highest risk of IPV. Critically, comparisons with perpetrators’ siblings who do not commit IPV suggest effects are not simply due to environmental, social, and family factors. Qualitatively, in a study of 37 men who had a substance use disorder and used IPV, Gilchrist et al. (2023) found the men took one of three pathways into substance use and IPV. The first was a rule-breaking pathway characterized by early antisocial behavior as a child, broadening to more serious crimes, IPV, and substance use as they aged. The second was chronic long-term substance use, often in response to traumatic events, and followed by violence. The third was insecurity and poor attachment, combined with increasing substance use and then progressing to IPV.
The Present Study
These commonalities and the overlap in dangerousness to self and intimate partners demonstrate a need to understand underlying patterns within cases that involve both IPV and suicide. The purpose of this is, therefore, to shed light on factors in people's lives that can be prevented or changed to reduce suicide and IPV. This research used an Australian sample from the Queensland Suicide Register to explore the case histories of IPV perpetrators who suicided. The following hypotheses were tested:
Many people who have a history of perpetrating IPV will die by suicide. Many people who have a history of perpetrating IPV and die by suicide will have a history of mental health problems and unmet mental health needs. Many people who have a history of perpetrating IPV and die by suicide will have substance use problems and unmet substance use treatment needs.
Method
Ethical approval was sought and provided by the Justice Human Research Ethics Committee (CF/15/13188). Data were extracted from the Queensland Suicide Register (QSR), containing information for all suicides in the State of Queensland, Australia (see Leske et al., 2021). Information sources of the QSR include: a police report of death to a Coroner, a postmortem autopsy report, toxicology reports, and Coroner's findings—including a narrative of the circumstances of death (such as who the deceased person was, and how, when, and where the person died). Documents are crosschecked with records from the National Coronial Information System (NCIS). Consequently, the QSR includes information regarding demographic factors, previous suicidal behavior, details regarding the death, mental health history, substances in the individual's system at the time of death, lifetime events, and criminal history details as well as a commentary. The dataset provides proximal and distal factors relevant to the individual's life and death. Data used in the present study included QSR entries from January 1, 2000 to December 31, 2017. Data were collected based on two criteria: (1) the individual had died by suicide and (2) the individual had been flagged as engaged in IPV. IPV was defined by having been charged with an offense, identified as the respondent on a domestic violence application/order or, in some cases, having harmed or killed an intimate partner prior to ending their own life.
Additional categories were also created surrounding the individual's death. The last known event before death was reviewed and categorized. Eleven categories were created, including argument or conflict, breach of domestic violence order (DVO), IPV incident, homicide, legal documentation or proceedings, police contact or attendance, multiple issues, other non-IPV offenses, separation, time in custody, and not indicated (for absent information). Finally, proximity between the event and death was reviewed and separated into categories labeled: the previous 7 days, after 7 days, or upcoming. Upcoming indicated a future-oriented event (e.g., going to prison) may have been of primary concern for the decedent and a potential trigger for the suicide. The QSR has been shown to be reliable generally (see Leske et al., 2022).
Data Analysis
Data were analyzed with SPSS (Version 29.0.0). Descriptive statistics were used to provide a detailed summary of the sample characteristics and the distribution of key demographic, psychosocial, and contextual variables relevant to the study. These included age, gender, relationship status, and Indigeneity, which allowed for a clear description of the study population. These allow the identification of patterns and variability among the data. Mental health histories, substance use histories, and events preceding suicide were examined separately for Indigenous and non-Indigenous individuals to allow for culturally and contextually informed interpretations and to identify potential differences in risk profiles. Mental health histories included previously communicated intent to suicide, documented mental health diagnoses, and prior engagement with mental health services to provide insight into long-term vulnerability and access to care. Substance abuse histories assessed both lifetime and recent use of alcohol and illicit substances, as well as substances detected at autopsy, offering information on both behavioral patterns and acute intoxication at the time of death. Events proceeding suicide focused on relational, legal, and criminal stressors occurring in the 7 days prior to death, capturing proximal circumstances that may have contributed to suicide risk.
An exploratory factor analysis with oblique rotation was conducted to conceptualize data and relationships between variables relating to IPV and suicide. Exploratory factor analysis was chosen because the latent structure of the variables was not predetermined and because IPV and suicide-related factors were expected to overlap conceptually. Oblique rotation was used to allow factors to correlate, reflecting the theoretical assumption that psychosocial, behavioral, and legal stressors are interrelated rather than independent. This analytic approach allowed the identification of coherent latent dimensions that reduced data complexity while preserving meaningful relationships between variables and allowed for a nuanced framework for understanding different pathways linking IPV and suicide.
Results
Numbers of IPV Perpetrators Who Die by Suicide
Between January 2000 and December 2017, 629 people with histories or allegations of IPV died by suicide in Queensland. The most frequently used method of suicide was hanging—used by 435 people (69.2%). The mean age of this group was 36.8 years (SD = 11.5). The sample consisted of 583 males (92.7%) and 46 females (7.3%). With regard to relationship status, 265 (42.5%) were married or in de facto marriage-like relationships, 177 (28.1%) had separated, 102 (16.3%) had never been married or in a de facto relationship, two (0.3%) were widowed, and the remaining 48 (7.6%) had no known relationship status. A substantial proportion, 115 (18.3%), were identified as Indigenous, while 514 (81.7%) were non-Indigenous. Because of the high proportion of Indigenous peoples in the sample, we present specific statistics for this population.
A study by Kõlves et al. (2015) that analyzed data from 2002 to 2011 on the Queensland Suicide Register (QSR) showed 5,752 people died by suicide in Queensland. Our subsample shows that 14.7% of suicides overall in this period engaged, or were alleged to have engaged, in IPV. Direct comparison data are not available, but there were 135 IPV homicides between the beginning of 2006 and the end of 2017 (Domestic and Family Violence Death Review and Advisory Board, 2018), while there were 476 suicides, indicating that IPV perpetrators were three and a half times more likely to kill themselves than their partners.
Relevant Histories for IPV Perpetrators Who Suicided
Mental health histories of our sample are displayed in Table 1. Most previously communicated intentions of suicide (61.4%) and many previously attempted to end their life (37.4%). Depression was the most frequent mental health condition, with 54% of the sample identified, or suspected, to have been depressed. Many attempted to seek mental health care (43.9%).
History of Suicide Attempts, Mental Health Problems, and Mental Health Treatment.

The substance use histories of the sample are displayed in Table 2. Previous use of illegal substances was frequent (64.4%) as were alcohol problems (25.1%). At the time of death, alcohol was present for most suicides (51.7%) while cannabis (26.2%) and benzodiazepines (25.4%) were also frequent.
Previous Substance Use and Substances Found at Autopsy.

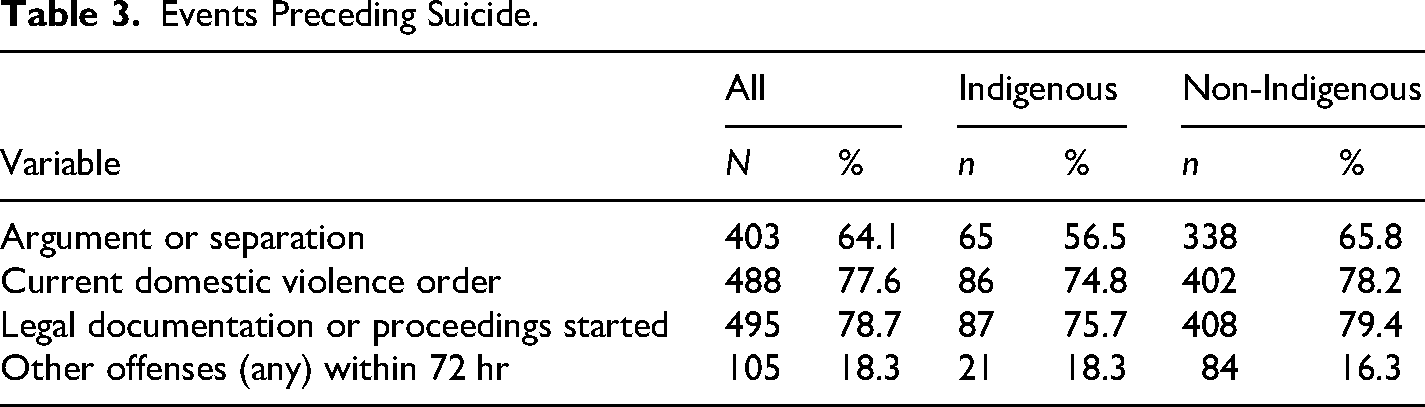
Events within 7 days of the suicide are displayed in Table 3. Domestic violence orders and sending of legal documentation or start of proceedings were most frequent, while argument or separation was also common.
Events Preceding Suicide.
Conceptualizing Factors Relating to IPV Perpetrators’ Suicidal Behaviors
As a way of conceptualizing the data, an exploratory factor analysis with oblique rotation (oblimin) was conducted. The initial factor analysis was conducted using items displayed in Tables 1–3, as well as gender and age. To avoid multicollinearity between items of “any previous suicide attempt” and “suicide attempt in the last 12 months,” “any previous communication of intent to suicide” and “communication of intent to suicide in the last 12 months,” the “any” item was used. In addition, “any mental health care provided” was dropped because of the other items with which it overlapped (e.g., outpatient and inpatient care). Using an Eigen value of >1, a nine-factor solution explaining 57.2% of the variance was revealed. This was difficult to interpret, so for simplicity, a three-factor solution was forced, explaining 30.0% of the variance (see Table 4). The Kaiser–Meyer–Olkin (KMO) measure verified the sampling adequacy three-factor model for the analysis, KMO = .70. Bartlett's test of sphericity χ2(325) = 2,622.59 indicated the correlation structure was adequate for factor analysis.
Exploratory Factor Analysis Examining Relationships Between Variables.
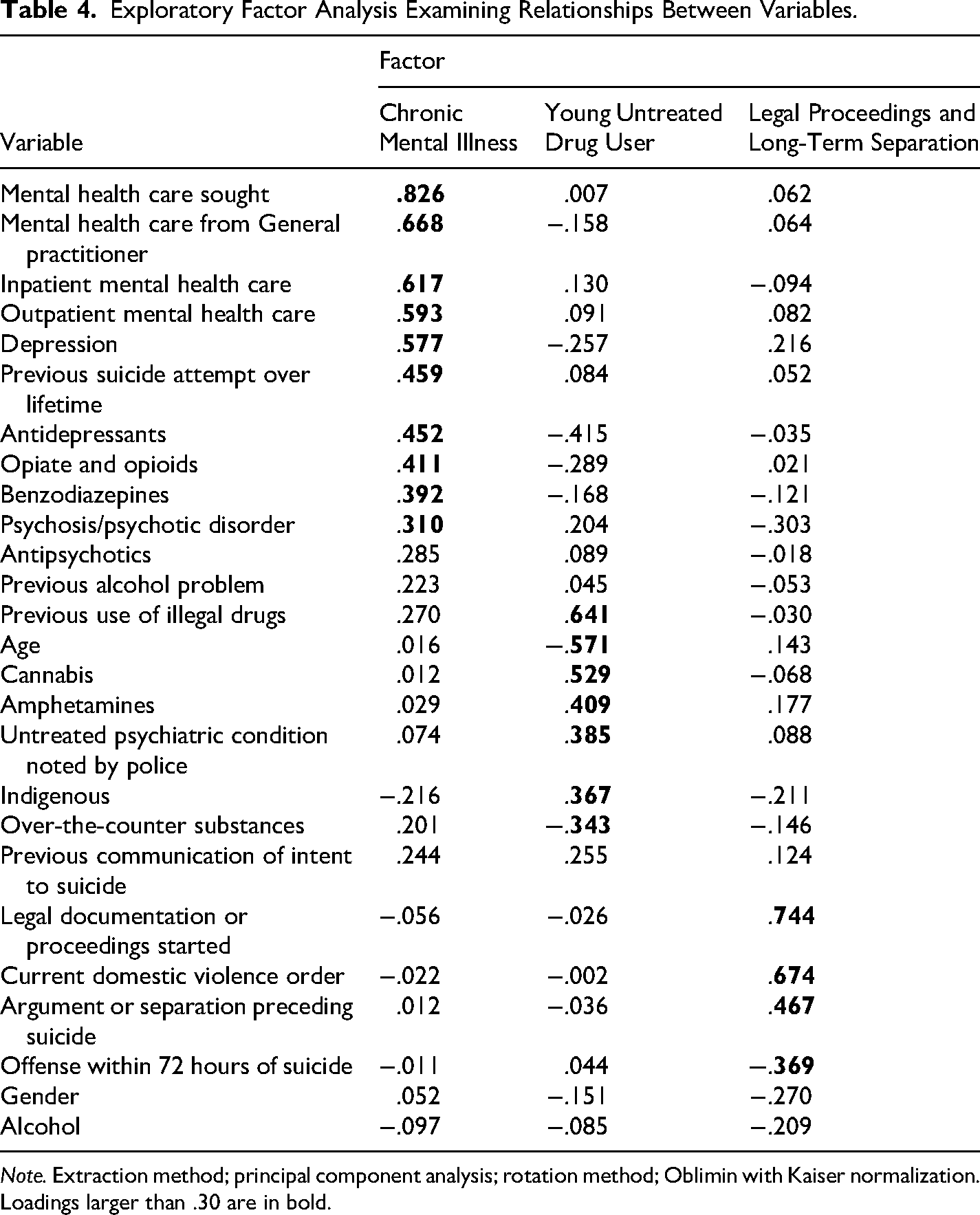
Note. Extraction method; principal component analysis; rotation method; Oblimin with Kaiser normalization. Loadings larger than .30 are in bold.
The first factor, “chronic mental illness,” was characterized by previous suicide attempts, seeking mental health care from their general practitioner, and inpatient and outpatient mental health care. Depression and psychosis or psychotic disorders were more frequent than other factors and correspondingly antidepressants and benzodiazepines were more likely to be present at autopsy—as were opiates and opioids. The second factor, “young, untreated, drug user,” was characterized by younger age, previous use of illegal drugs, and cannabis and amphetamines present at autopsy. Decedents were more likely to be Indigenous. Police inquiries indicated they were more likely to have an untreated psychiatric condition. They were less likely than other factors to have over-the-counter drugs present at autopsy. The final factor, “legal proceedings and long-term separation,” was more likely to be involved in legal proceedings, have a current domestic violence order, and experience arguments or separation preceding the suicide. They were less likely to have committed an offense in the previous 72 hours.
Discussion
The first hypothesis, that many people with a history of perpetrating IPV will die by suicide, was confirmed, 629 people who ended their lives had perpetrated IPV or had allegations of IPV made against them. It was possible to compare these numbers with the total number of suicides reported between 2002 and 2011 (Kõlves et al., 2015). Nearly 15% of the total suicides involved alleged or confirmed IPV perpetrators, a substantial proportion. Comparison with the IPV homicide data for Queensland indicates perpetrators are over three times more likely to kill themselves than their partners (Domestic and Family Violence Death Review and Advisory Board, 2018). What these numbers make explicit is that suicide and IPV are a serious problem. This is particularly the case for the Indigenous peoples in this sample. While Indigenous peoples account for less than 5% of the Queensland population, they made up 18.3% of the suicides in this sample (Australian Bureau of Statistics, 2026).
The second hypothesis was the prediction that many people who have a history of perpetrating IPV and die by suicide will have a history of mental health problems and unmet mental health needs. This was the case. The most frequent diagnosis was depression which has a strong, well-documented, association with suicide (Chesney et al., 2014; Schmutte et al., 2021). Although much less frequent, a substantial minority of people had a psychotic disorder. Treatment engagement was mixed.
Most non-Indigenous people sought help, a finding consistent with findings elsewhere concerning people who commit suicide (e.g., Windfuhr et al., 2016). Levels of treatment also varied, some had extensive general practitioner, inpatient, and outpatient treatment. The sample's treatment engagement and evident suicidal intentions demonstrate a critical divergence from the common narrative that people, particularly men, do not seek help for their mental health (this has been found elsewhere too, e.g., Kapur et al., 2022). This is an important finding, as it indicates most of the sample had identifiable and treatable mental health problems. These data suggest many people are showing suicidal intentions but not receiving appropriate, necessary care. This is consistent with a study in Queensland that found 45% of former prisoners who attended an emergency department for self-harm did not receive mental health care within 7 days, and over one third still had not received care 30 days later (Young et al., 2020), despite a heightened risk of suicide in the 7 days following self-harm (Haukka et al., 2008). The fact that people still killed themselves suggests the support they received did not meet their needs—although, of course, we are unable to know the number of people who received treatment that otherwise would have killed themselves. The picture for Indigenous peoples in this sample was far worse. While a similar number of Indigenous peoples had communicated intent to suicide previously, they were far less likely to have received a depression diagnosis and have sought mental health care, while being more likely to have an untreated mental health condition.
The third hypothesis, that many people who have a history of perpetrating IPV and die by suicide will have substance use problems and unmet substance use treatment needs, was supported. Most of the sample had previously used illegal drugs, although we are unable to tell, unless specific notes were made, whether this was problematic. However, previous alcohol problems were frequently identified. Autopsy reports identified substance use at the time of death. Alcohol was present in most decedents. For a substantial number, especially Indigenous peoples, cannabis was also present. There were high numbers of non-Indigenous people with benzodiazepines, anti-depressants, and opiates and opioids in their bodies when they died.
Causal relationships between mental health, IPV, substance use, and suicidality are difficult to determine. Psychological autopsy studies have reinforced the complexity of attributing cause to a single event, particularly for those with multiple proximal factors present, such as this group (Foster, 2011). Mental health conditions, drug and alcohol use, relationship difficulties, and a history of violence intersect. For example, O’Connor and Kirtley's (O'Connor and Kirtley, 2018) Integrated Motivational-Volitional theory suggests IPV perpetrators with underlying mental ill health are at heightened risk when confronted with events that may increase their motivation to suicide because of volitional factors. Motivational factors such as a relationship breakdown or contact with the justice system can cause a sense of defeat, humiliation, or entrapment. While volitional factors, including aggression, behavioral disinhibition or impulsivity (potentially due to drug and alcohol use), recklessness, a heightened pain threshold, and mental imagery (e.g., current/former partner feeling hurt, blamed, or guilt) shift ideation to action. To reduce suicide and violence, consideration of factors underpinning IPV, suicidal behavior, and substance use, as well as strategies to improve coping and problem-solving skills of this group, is needed (Foster, 2011; O’Connor, 2018).
IPV, relationship breakdown, and associated legal problems appear to precipitate suicide. Arguments and separation, current domestic violence orders, and the beginning of legal proceedings were commonly precursive to suicides. This was often not immediate, with few suiciding within 72 hours of an event. The first few months after a relationship breakdown, particularly for men, are a widely acknowledged period of vulnerability (De Leo & Krysinska, 2017) and problems in spousal relationships were identified in 23.2% of all Australian suicides in 2020 (Australian Bureau of Statistics, 2021). This appears to be exacerbated by involvement in legal processes. Previous research highlighted that offending typologies and phases of the justice system present varying vulnerabilities. These vulnerable periods were reflected in this study and include: after police contact, after returning to the community from police or correctional custody, and in the days either side of court appearances (King et al., 2015). These phases represent an opportunity for a multidisciplinary, multiagency approach to enhance suicide interventions and ensure violence toward self or others does not escalate.
An exploratory factor analysis helped reveal common themes. One significant factor was the presence of chronic mental health problems among individuals involved in IPV. Many of these individuals received extensive medical attention, aligning with previous research indicating higher rates of psychopathology and comorbidities among IPV offenders (Dean et al., 2024; Sariaslan et al., 2020). Further investigation is necessary to understand experiences of service providers and users, including the mental health services currently available to IPV perpetrators, outcomes of these services, and how different services interact. The stigma and the complicated nature of treating IPV offenders mean specialist treatment may be required (for a review of stigma in this population, see Tremlin & Beazley, 2024). By identifying areas for improvement and ensuring appropriate allocation of resources, the provision of support can be enhanced. It is worth noting half of the study sample had psychiatric medications in their system at the time of death. This highlights the need for primary health care providers to proactively inquire about co-occurring violence when prescribing medications, as violence may contribute to an individual's distress and suicidal thoughts or behaviors.
The study also identified a second factor, young people with a history of drug use, who were commonly Indigenous peoples. Addressing problematic drug use is a priority for both justice and health systems due to its association with offending and suicidal behaviors (Yu et al., 2019), particularly within Indigenous communities (De Leo et al., 2012). Interventions could prioritize delaying initiation of drug use and addressing the socio-acceptability of drug use, especially for self-medication. Timely and accessible treatment programs are crucial for capturing individuals during vulnerable periods and addressing the implications of drug use, including the risk of dual harm. Additionally, Indigenous community members were overrepresented in the sample, emphasizing the need for tailored, culturally appropriate prevention interventions implementable across different areas, a finding that has ramifications for policy, as discussed later (see also De Leo et al., 2012).
Indigenous status was found to be associated with less engagement with mental health care and medication use. Only a quarter of Indigenous decedents had sought help from a mental health care provider, compared to almost half of the non-Indigenous group. Medication use was also significantly lower among the Indigenous deceased. These disparities may be attributed to challenges faced by Indigenous communities in accessing care due to rural or remote locations, cultural factors, and differing perspectives on mental health. Enhancing capabilities and resources of Aboriginal Community Controlled Health Organizations can contribute to supporting vulnerable members of the community and their families. However, this requires an evidence-informed understanding of factors influencing Indigenous suicidal behaviors and help-seeking, an area that remains understudied (De Leo et al., 2012). Psychological treatments should address both IPV and suicidal behaviors when dual harm is identified as an issue. Engaging IPV offenders sustainably remains a challenge, and further qualitative research into co-occurring violence among IPV perpetrators who have attempted suicide can inform future strategies.
The third factor from the factor analysis was the presence of long-running legal disputes associated with separation. Contact with the justice system and separation were identified as periods of heightened suicide risk, warranting tailored interventions (Slade, 2019). Mapping intercept points to identify periods of contact with IPV perpetrators from various agencies can help identify opportunities for intervention and provide support to reduce the likelihood and severity of self-harm or harm to others. Legal documentation or proceedings were frequently identified as the most common proximal event preceding suicide among IPV offenders. However, as time between an incident and death decreased, incidents such as arguments/conflicts and IPV became more prevalent. This suggests that the hours and days following an IPV incident or argument/conflict are particularly vulnerable periods for individuals perpetrating IPV, especially if they have not sought mental health care. Separation was the second most observed issue, aligning with general suicide risk factors as relationship problems are commonly associated with suicide (Australian Bureau of Statistics, 2021; De Leo & Krysinska, 2017). IPV offenders may be at a heightened risk of suicide, as well as further IPV incidents, when they feel they are losing control of the relationship (Rezey, 2020).
Informing Policy
The potential for suicide in perpetrators of IPV needs to be taken seriously. Not only are perpetrators of IPV harming others, but they are also harming themselves. Many of the behaviors identified here that are associated with suicide, such as threats of suicide, alcohol and drug use, and poor mental health, are also associated with increased risk of violence to partners or former partners (e.g., Kropp & Hart, 2015). Therefore, responses to address these risks, including the underlying drivers of these risks such as trauma and negative conceptualizations of masculinity, are needed. This is especially the case for Indigenous peoples, where the numbers of suicides indicate resources should be focused. Interventions for Indigenous peoples need to be culturally informed and acknowledge the enduring trauma of Indigenous peoples while facilitating optimism about the future and breaking the cycle of abuse. Awareness of IPV and suicide risk should be embedded across sectors, including policing, emergency departments, and alcohol and other drug services. Routinely asking about these issues can help practitioners develop a more comprehensive understanding of a person's circumstances and, in turn, inform practices that reduce the risk of both IPV and suicide.
Limitations
IPV is often underreported to the police, meaning there may be additional offenders in the database not identified. Additionally, some decedents had limited available information, leading to challenges in accurate categorization. The data collection process, particularly the completion of forms by family and current or former partners during a period of bereavement, may affect the accuracy and completeness of information. Families with low mental health literacy may struggle to speculate on their relative's mental health condition. Furthermore, the study did not distinguish whether mental health care accessed by decedents was voluntary or enforced.
The potential for misclassification bias is another limitation of this study. In instances where the coroner is unable to determine intent, the cause of death may be misclassified as accidental or misadventure rather than suicide. It has been argued that coronial determinations of suicide significantly underestimate the frequency of suicide deaths in Australia (Jowett et al., 2018). Therefore, further suicides are possible for those who perpetrate IPV, particularly given high rates of engagement with illicit drug use, alcohol use, and potentially reckless behavior, which may make determining intent difficult for coroners. Further bias is possible as cases in this study required manual categorization in some instances, which can create the potential for misclassification given gaps in information available.
A final limitation is that threats of suicide in IPV seem to be frequent and can be motivated by manipulation and control, and these suicides need to be considered in the context of more general threats. Indeed, some of the suicides examined in the study appeared to be deliberate acts to manipulate a situation or convey a message. This deserves additional attention, as it may be the case that many IPV perpetrators are using threats to suicide to manipulate without actual suicidal intent. Of course, this is not the case for this sample that did suicide. Understanding the relationship between violence, threat of suicide, and suicide and the role it plays is important, as it can inform responses (Johnson et al., 2019).
Conclusion
This study provides insights into factors associated with suicide among people who have, or have allegations of, engagement in IPV. The findings underscore the need to consider IPV offenders as a heterogeneous group influenced by multiple factors with regards to the co-occurrence of IPV and suicide. IPV and suicide occur frequently, and there is potential for improvements in the delivery of IPV and suicide prevention, starting with acknowledging the problem. These findings call for a reconsideration of how co-occurring violence is addressed and provide avenues to inform future IPV and suicide prevention efforts. Together, this can reduce violence against intimate partners and self-directed violence.
Footnotes
Acknowledgments
We would like to acknowledge funding of the Queensland Suicide Register by the Queensland Mental Health Commission and Queensland Health. We also acknowledge the Department of Justice and Regulation for providing access to the Australian National Coronial Information System (NCIS).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.