
Abstract
Research demonstrates a higher prevalence of intimate partner abuse perpetrated against disabled women, than for their majority-population non-disabled peers. Compounding this disadvantage, are disability-specific barriers to help-seeking including the lack of accessible and inclusive domestic violence services. This article entails a presentation of research findings that is twofold. Findings of a survey of domestic violence services are presented, alongside findings of a mapping exercise of accessibility and inclusion features of domestic violence services (n = 45). Recommendations are made toward improving the accessibility of domestic violence services, as well as better resourcing services so that improvements can become a reality.
Introduction
A key consideration for specialist domestic violence services should be inclusion and accessibility for disabled women who are prospective service users. This is due to the high established prevalence and negative impacts of intimate partner abuse (IPA) against disabled women (Amos et al., 2023; Bonomi et al., 2018; Women's Aid, 2023). The United Nations (n.d., p. n.p.) define IPA “as a pattern of behavior in any relationship that is used to gain or maintain power and control over an intimate partner. Abuse is physical, sexual, emotional, economic or psychological actions or threats of actions that influence another person.” IPA is also sometimes referred to as domestic abuse or domestic violence. A significant body of evidence demonstrates higher rates of perpetration of IPA against disabled women than for their majority-population, non-disabled female peers (Alhusen et al., 2020; Amos et al., 2023; Anyango et al., 2023; Astbury & Walji, 2014; Garcia-Cuellar et al., 2023; Goulden et al., 2023; Jordan, 2022; Office for National Statistics, 2019). Greater risk of experiencing IPA is also leveled against disabled women above their disabled male counterparts (Anyango et al., 2023). Yet, there is poor understanding about IPA against disabled women due to a lack of research despite the high known prevalence of perpetration (Ruiz-Pérez et al., 2018).
One reason for this high prevalence is opportunistic targeting of disabled women by abusers due to the perception that they are vulnerable and will be dependent upon the abuser. Societal stereotypes may also be exploited by an abuser to shield abuse from being discovered. This includes the negative stereotype that disabled women have reduced likelihood of experiencing sexual abuse due to being less sexually attractive (Smith, 2008). Research by Aguillard et al. (2022) emphasizes that “prevailing perceptions” of disabled women such as being “dependent and helpless” are inaccurate. Aguillard et al. (2022) examined disabled women's experience of coping with interpersonal violence and evidence of their strength and resilience within this. Disabled women described how coping with a disability helped them to develop strengths that were fundamental to their resilience.
Disabled women may experience IPA that includes disability-specific forms of abuse and disability-specific barriers to coping with abuse and help-seeking (Jordan, 2022; Myall et al., 2023). Disabled women may ironically rely on their abuser for mobility support to access domestic violence services whether physically traveling to a service, using devices with internet access or making phone calls (Flynn et al., 2024). Disabled women may therefore become trapped in an abusive relationship due to barriers to independence at the intersection of disability and abuse (Johnson et al., 2022; Njelesani et al., 2021).
When trying to flee an abusive situation, disabled women may need specific practical and social supports such as childcare assistance once they have exited the relationship (Njelesani et al., 2021). Such requirements can differ based on the type of impairment (s) the woman has. The nature, prevalence, and impacts of IPA may also differ based on impairment type (Tenaw et al., 2023). The severity of disability may be a moderating factor according to Meyer et al. (2023) in the likelihood of physical and/or sexual IPA against disabled women. What appears certain is that significant complexities can arise when disability intersects with IPA. This includes how disability may make exiting an abusive relationship and engaging in help-seeking much harder for women experiencing IPA (Flynn et al., 2024). It also includes how disabled women's experiences of IPA demonstrate their development of strength, resilience, innovative coping strategies, and compassion and empathy for helping others (Aguillard et al., 2022).
The present study focusses on investigating the accessibility of domestic violence services for disabled women in the Republic of Ireland. Agencies in the Republic of Ireland that provide services for IPA come in diverse forms, although there are no dedicated agencies in the country for IPA against disabled women. A report by Burke and Dorta Cabello (2024) outlines a list of key services offered by agencies in the Republic of Ireland in relation to domestic abuse including IPA. These include stays in a safe house or refuge, psychosocial groups, transitional housing, training, therapeutic and wellness services, housing support, legal and court support, interagency coordination, planned support work, administrative calls, as well as child-related supports such as sessional childcare (Burke & Dorta Cabello, 2024, p. 17). Services rely on varied funding sources including full or partial State funding and resourcing through grants, volunteering, and charitable fund-raising (Burke & Dorta Cabello, 2024).
In the context of a significant gap in investigations about the preparedness of these services to support disabled women, findings of a mixed-method research study will be presented in this article. This study involves a national survey of the accessibility of domestic violence services (n = 34) for disabled women and a mapping exercise of accessibility and inclusion features of those services (n = 45).
Method
Study Design
It is first beneficial to specify the details of the mixed-method study design including significance and context of the study, research question, aim, and objectives. The research was conducted by an independent research team to fill a substantial gap in existing knowledge about the suitability and accessibility of specialist domestic violence services for disabled women (Ruiz-Pérez et al., 2018). The gap is significant as not only are disabled women at increased risk of IPA, but they also experience double disadvantage due to unique needs and barriers when help-seeking (Flynn et al., 2024; Jordan, 2022; Myall et al., 2023; Ruiz-Pérez et al., 2018). Thus, the lack of previous research into the accessibility and suitability of domestic violence services for disabled women in the Republic of Ireland presents a clear gap. Although the research included investigation of the subject matter of service provision, it was not commissioned or conducted as a service evaluation.
The research question for the survey and mapping exercise is, “what is the nature of accessibility of specialist domestic violence services for disabled women in the Republic of Ireland?” There are two research objectives. The first objective is to gather data on the preparedness of specialist domestic violence services in the Republic of Ireland for supporting disabled women. For this objective, a survey of services was designed as it was the best method to gather generalizable insights directly from service providers about barriers and facilitators to disability inclusivity within their services. The second objective was to determine how accessible and inclusive specialist domestic violence services appear to be for disabled women. For this objective, a mapping exercise was deemed best as the appearance of the accessibility and inclusivity of services could be determined through empirical observation.
The mapping exercise approach was an important initiative in the context of a particular barrier to help-seeking for disabled women identified by research. Namely, the impression, assumption, or understanding held by disabled women experiencing IPA that services are not inclusive or cannot meet their disability-related needs (Flynn et al., 2024). The research was conducted by an innovative, inclusive principal investigator led research team. In keeping with core Public and Patient Involvement principles (MacLachlan et al., 2024; Pettican et al., 2023), the study foregrounded the epistemic authority of experts by experience, recognizing their lived expertise as central to shaping the design and conduct of this research project. The all-female, disability inclusive team included well-regarded Irish disability advocates and activists, and experts-by-experience with visible and hidden disabilities. The team also included experienced researchers and academics situated as international subject experts in fields of disability and domestic violence and abuse (DVA). To supplement this diverse expertise, the team was supported by an advisory committee of experts from leading, relevant organizations across the country.
Finally, the research was funded by one of the country's leading DVA services. Full ethical approval for the research was granted from School of Social Work and Social Policy Research Ethics Committee at Trinity College Dublin. Data protection certification for researchers was obtained through relevant training and a data protection impact assessment was completed.
Sampling and Recruitment
Sampling and recruitment strategies differed between the survey and the mapping exercise. For the survey, the sampling frame for the study was 40 moderate to large specialist domestic violence services operating in the Republic of Ireland. Of this population, all were approached and a sample of 85% (n = 34) participated. Services were accessed using a gatekeeper, which was the domestic violence service that funded the research. Representatives were identified by each service who would be sufficiently knowledgeable to anonymously complete the survey on behalf of, and with reference to, their organization. Representatives were informed that participation was voluntary. They were also furnished with information so that informed consent could be given. The survey was administered and analyzed using Qualtrics software. Written consent was captured anonymously for participants at the outset, and IP address collection was disabled to ensure anonymity.
For the mapping exercise, the sample for the mapping exercise consisted of all organizations operating in the Republic of Ireland (n = 45) with a primary objective of addressing and combatting DVA. Organizations were identified through the Safe Ireland Directory published on the Safe Ireland website (Safe Ireland, 2025, p. n.p.). The sampling frame was a little larger than for the survey, as some moderate to large size domestic violence service divisions were included, where the main organization was not a specialist domestic violence service. These services were located across the country with a concentration of services located in the capital city due to population density. Small-scale domestic violence services, small-scale services that are not stand-alone and individual activists, advocates, and consultants were omitted from the sample.
Data Collection
Prior to data collection, a comprehensive literature review was conducted including predefined search terms, electronic database and gray literature searches, and review of the search strategy by a subject librarian and members of the advisory committee. The review search strategy included electronic database searches of Academic Search Complete; Violence & Abuse Abstracts; ProQuest Social Science Databases; EBSCOhost; and WHO Global Database. As the subject matter regarded DVA agencies in the Republic of Ireland, key contacts in the agencies assisted with gray literature searches and obtaining relevant organizational reports. Results retrieved and other search records were compiled as an audit trail. Sources were then summarized into key points in a shared document. The final literature review was written up thematically. Existing literature validated the appropriateness of a survey and mapping exercise for the research question (see for instance, World Health Organisation, 2024).
For data collection, the survey instrument was designed by the team, reviewed by the advisory committee, and pilot tested before being issued. Review of the survey also included feedback from disabled persons including individuals with learning difficulties and neurodevelopmental disability. A copy of the survey questions used can be viewed in appendix 1, which covers topics such as disability awareness, training, and capacity building for staff and service accessibility measures.
The mapping exercise as a form of desk-based research, alternatively, involved investigating DVA services using publicly available information such as through consulting organization's websites, Facebook pages, and using Google Maps. Records were then made of what predetermined inclusion and accessibility features were and were not observed. These inclusion and accessibility features were initially identified from a literature review and then were reviewed by the advisory committee. As with all components of the project, disabled women were involved directly in the process of determining inclusion and accessibility features.
Data Analysis
For the survey, data analysis was conducted using Qualtrics to create descriptive statistics focusing on frequency distributions in the form of counts and percentages. For the mapping exercise, data analysis involved simple data aggregation involving calculation of frequency distributions in the form of counts and percentages. The theoretical and conceptual approach taken to disability across both methods aligned to a social model of disability approach. Thus, disability was understood as a product of interaction between the impairment (s) the woman has, and societal, structural, and social barriers to equality (Oliver, 2013). Having established the study design and method, it is now timely to turn to findings, wherein insights about the nature of preparedness of DVA services to support disabled women are shared.
Findings
In this section, findings of the study will be presented under themes. Six themes will be shared referring to service accessibility; information accessibility; barriers to accessibility; understanding of disability; involvement of disabled women; and diversity in service provision. Mapping exercise and survey findings are presented together under these themes. For the survey, 24 out of the 34 surveys in the sample were fully completed and 10 were substantially and partially completed. Therefore, the exact number of responses per question will be reported for transparency, alongside the statistical result where relevant.
Theme One: Service Accessibility
The first theme emergent from the findings is about how accessible domestic violence services are for disabled women. This is vital to understand as disabled women are at increased risk of IPA and may have unique needs when accessing domestic violence services, such as requiring a wheelchair ramp or hoist (Flynn et al., 2024; Garcia-Cuellar et al., 2023). To understand the accessibility of participating domestic violence organizations, 14 statements pertaining to disability accessibility were presented in the survey to respondents. Findings show that most participating organizations do have information on their services that is available in either plain English format or easy-read format (69%, n = 11). Slightly fewer participating organizations have accessibility of public transport (63%, n = 10), while fewer still have wide entrances with a ramp or level access for wheelchair users (56%, n = 9). Thus, while there was a degree of accessibility demonstrated in survey findings, it was also evident that some disabled women would not be able to avail of domestic violence services due to those services being inaccessible. More detailed information on responses (n = 16) are contained in Table 1 below:
Features of Service Accessibility (Adapted from Flynn et al., 2024, p. 73).
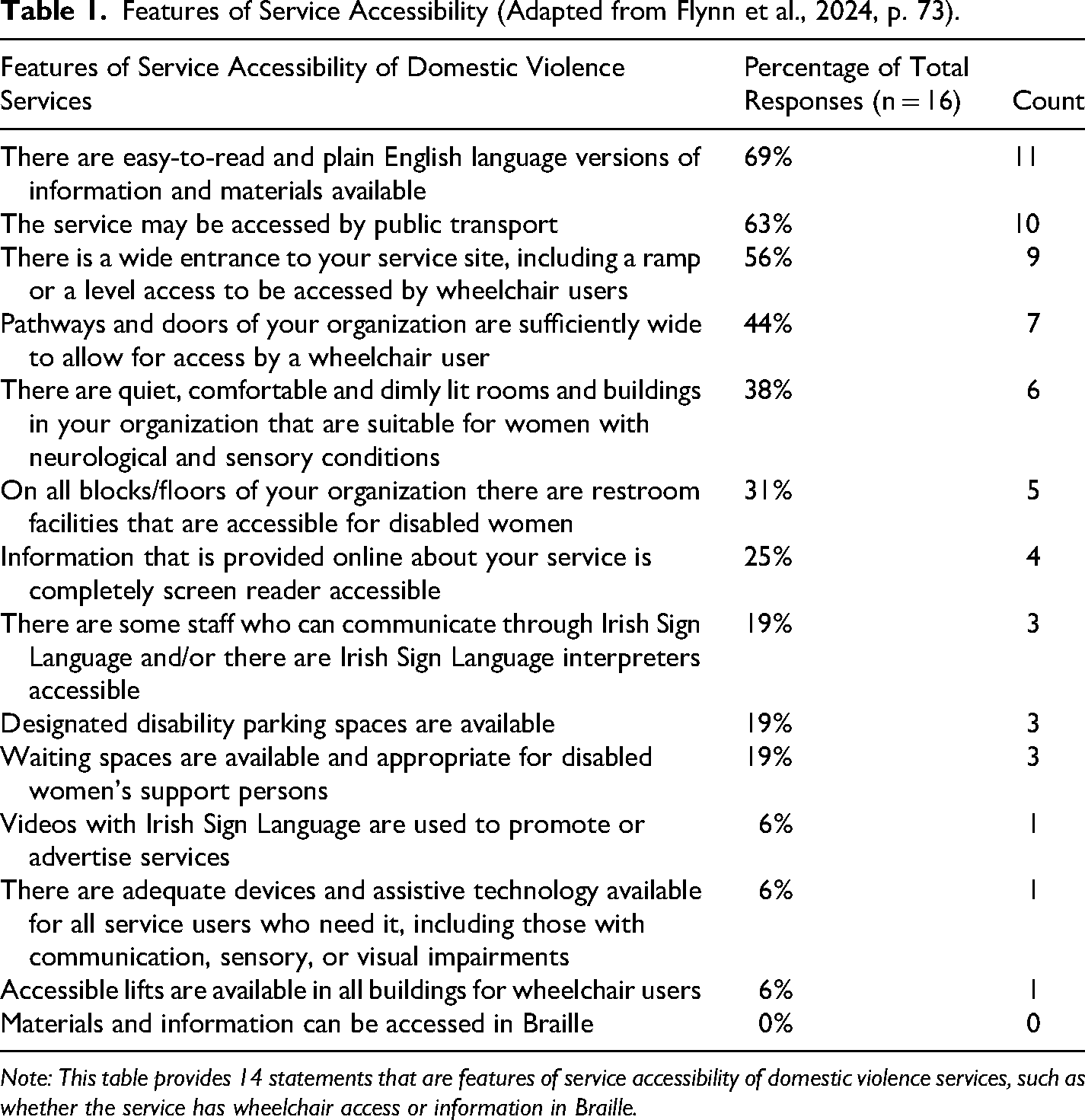
Note: This table provides 14 statements that are features of service accessibility of domestic violence services, such as whether the service has wheelchair access or information in Braille.
Building further on this picture of limited accessibility, the mapping exercise provided insights from the compilation of publicly available information that a disabled woman may see when searching for accessibility features. Fortunately, 96% (n = 43) of organizations had at least one remote access point such as web chat options, a Facebook page, or website. In 87% (n = 39) of organizations, the location and the nature of entrances to organization buildings could be viewed on Google Maps. It should be noted here that some organizations such as refuges would not be visible on Google Maps as a safety measure to prevent abusers locating victims/survivors.
Yet, the overall impression that a service would be accessible in catering to a disabled woman's needs was not formed. Only 51% (n = 23) of organizations, for instance, appeared to have wheelchair access from Google Maps, and only one organization mentioned accessibility or had any inclusive imagery. Overall, taken together, the survey and mapping exercise findings under the first theme of service accessibility demonstrate significant remaining scope to make services more accessible, as well as to make them appear more accessible, for disabled women. Table 2 below provides more detailed information on accessibility features of the organizations that were investigated.
Number and Percentage of Organizations that Appear to Have Each Accessibility Feature (adapted from Flynn et al., 2024, p. 82).
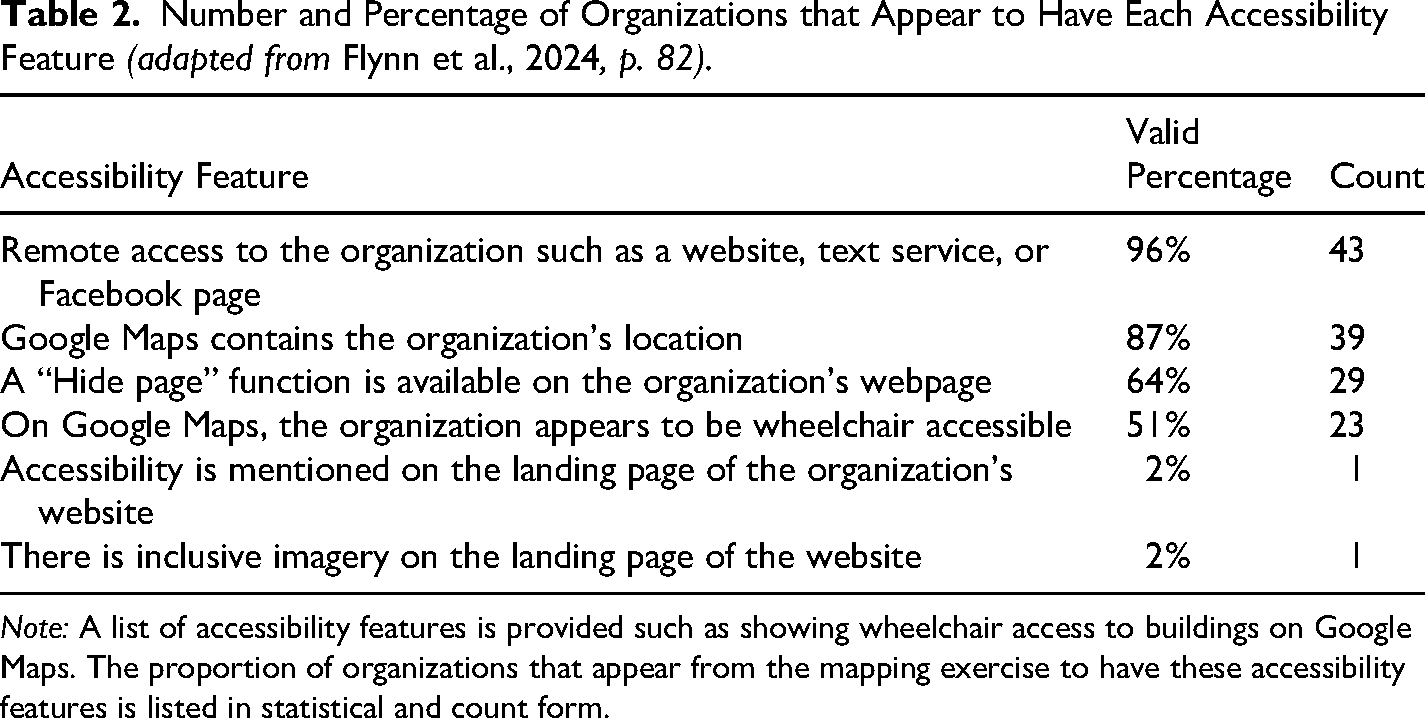
Note: A list of accessibility features is provided such as showing wheelchair access to buildings on Google Maps. The proportion of organizations that appear from the mapping exercise to have these accessibility features is listed in statistical and count form.
Theme 2: Information Accessibility
The next theme to be presented from the findings is about obtaining a more in-depth picture specifically related to information accessibility for disabled women. Information accessibility is important to understand as disabled women fleeing abuse who face communication barriers may rely on being able to access vital information like service contact details. Here survey findings show that the most reported accessibility measure was plain English versions of information and materials with 75% of the domestic violence services doing this. Thereafter, use of visuals was the next most frequent measure with approximately half of respondents doing this. Table 3 below provides further detail about information accessibility responses to this question.
Accessible Materials and Information for Women with Intellectual or Learning Disability (adapted from Flynn et al., 2024, p. 76).
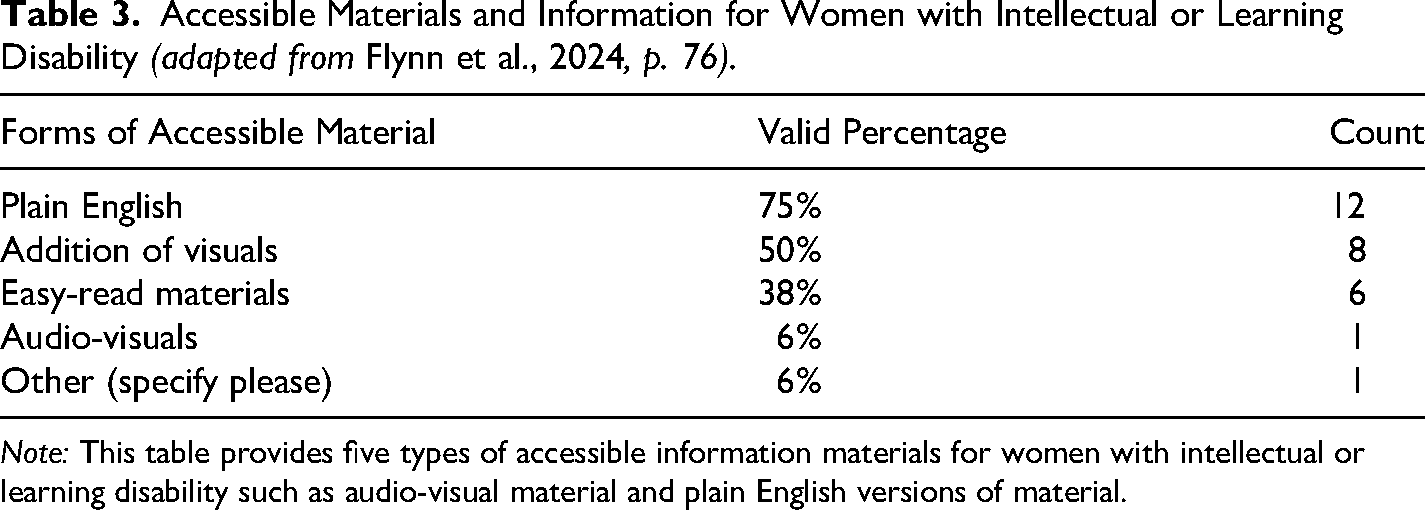
Note: This table provides five types of accessible information materials for women with intellectual or learning disability such as audio-visual material and plain English versions of material.
Building further on insights into information accessibility, the survey enquired about information accessibility specifically for hearing impaired or deaf women. Respondents were asked, for instance, if their organizations had text messaging services and all organization representatives that responded to this question (n = 11) said they had. A quarter of these representatives also said captioned videos were provided by their organizations (27%, n = 3). Table 4 below provides further information on responses around information accessibility for hearing impaired or deaf women.
Measures for Accessibility for Hearing Impaired/Deaf Women (adapted from Flynn et al., 2024, p. 77).
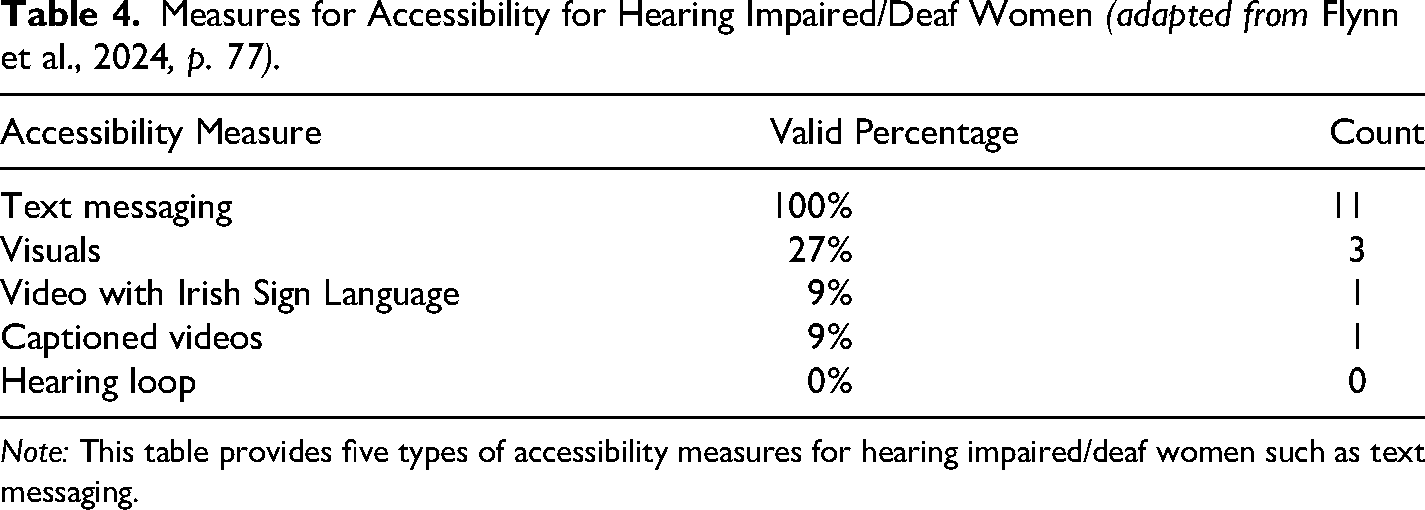
Note: This table provides five types of accessibility measures for hearing impaired/deaf women such as text messaging.
In addition to enquiring about information accessibility for hearing impaired or deaf women, the survey enquired further about the provision of easy-read format materials for disabled women. This is important as some disabled women have learning difficulties, intellectual disability, acquired brain injury (which may be a consequence of IPA) or other barriers to accessing information (Flynn et al., 2024). For the mapping exercise, principles of easy-read formatting as an accessibility measure were derived from the Foundation for People with Learning Disabilities (FPLD, 2025). These were “1. Content: Usage of short sentence, no paragraphs or word chunks”; “2. Image: Usage of images and graphics for each or most sentences”; “3. Language: Simple language with little to no abbreviations”; “4. Font size: Large font”; “5. Alignment: Text and images are uniformly aligned on either side.”; “6. Font style: Usage of one font style. No usage of fancy font, multiple styles or italics”; and “7. Design elements: Usage of minimal design elements, with few, subtle colors” (Flynn et al., 2024, p. 83; FPLD, 2025, p. n.p.). Facebook pages and websites were assessed for the degree to which they met these easy-read indicators. The organizations were then scored on a 7-point scale using this information. Only 24% (n = 11) of organizations scored between a 6 and 7 on the scale meaning the majority of organizations did not consistently provide key information in easy-read format. The results of the exercise are presented in Table 5 below:
Proportion of Organizations by Easy-Read Score (adapted from Flynn et al., 2024, p. 83).
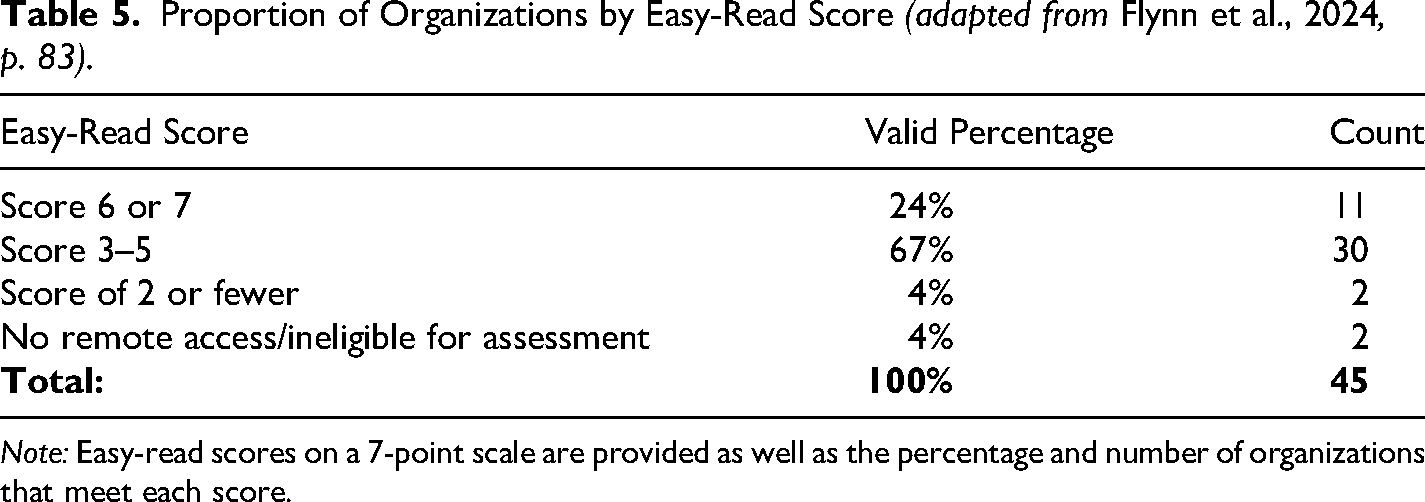
Note: Easy-read scores on a 7-point scale are provided as well as the percentage and number of organizations that meet each score.
Theme 3: Barriers to Accessibility
The next theme refers to barriers to accessibility. This represents a shift in focus toward understanding the barriers that domestic violence organizations face in making their services more accessible to disabled women. 15 organizational representatives responded to a question about this. Here, the absence of available specialist training on domestic abuse and disability as well as a deficit in resources was reported as relevant barriers for 13 of the domestic violence services. It was also clear that unmodifiable buildings were a barrier for 11 of the domestic violence services. Table 6 below provides more detail on responses to this question.
Barriers to Accessibility (adapted from Flynn et al., 2024, p. 78).
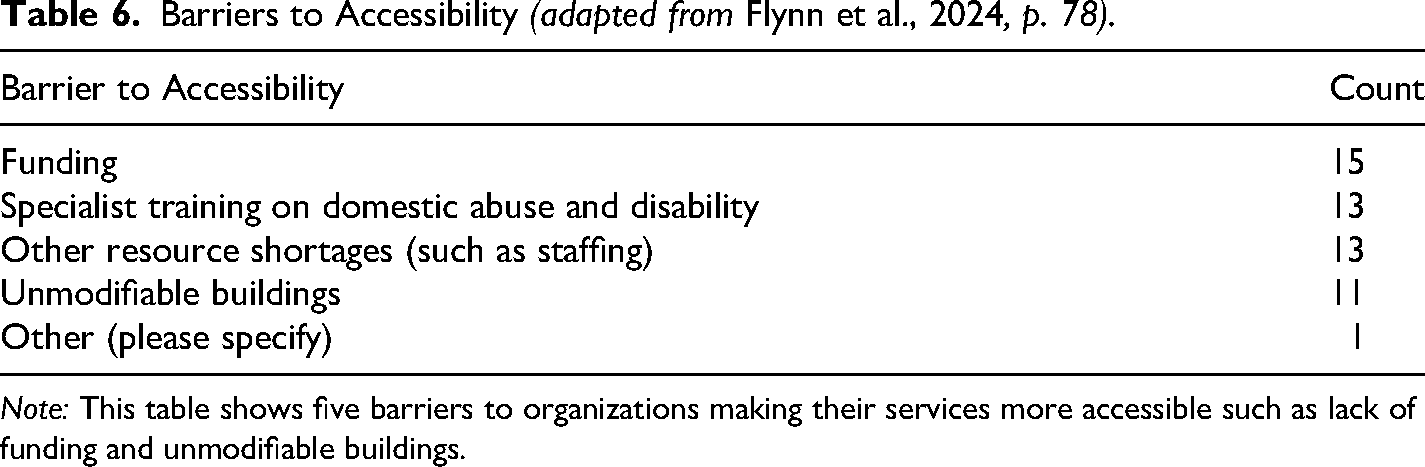
Note: This table shows five barriers to organizations making their services more accessible such as lack of funding and unmodifiable buildings.
Building on insights into barriers to accessibility, organization representatives were asked about what supports they required to improve accessibility. All respondents (n = 16) stated that specialist training from a disability organization would be helpful. 94% (n = 15) of respondents also indicated that guidance on making sensory-friendly spaces would be helpful as well as partnership with disability services. Table 7 below provides more detail on responses to potential supports to improve accessibility.
Support to Improve Accessibility (adapted from Flynn et al., 2024, p. 79).
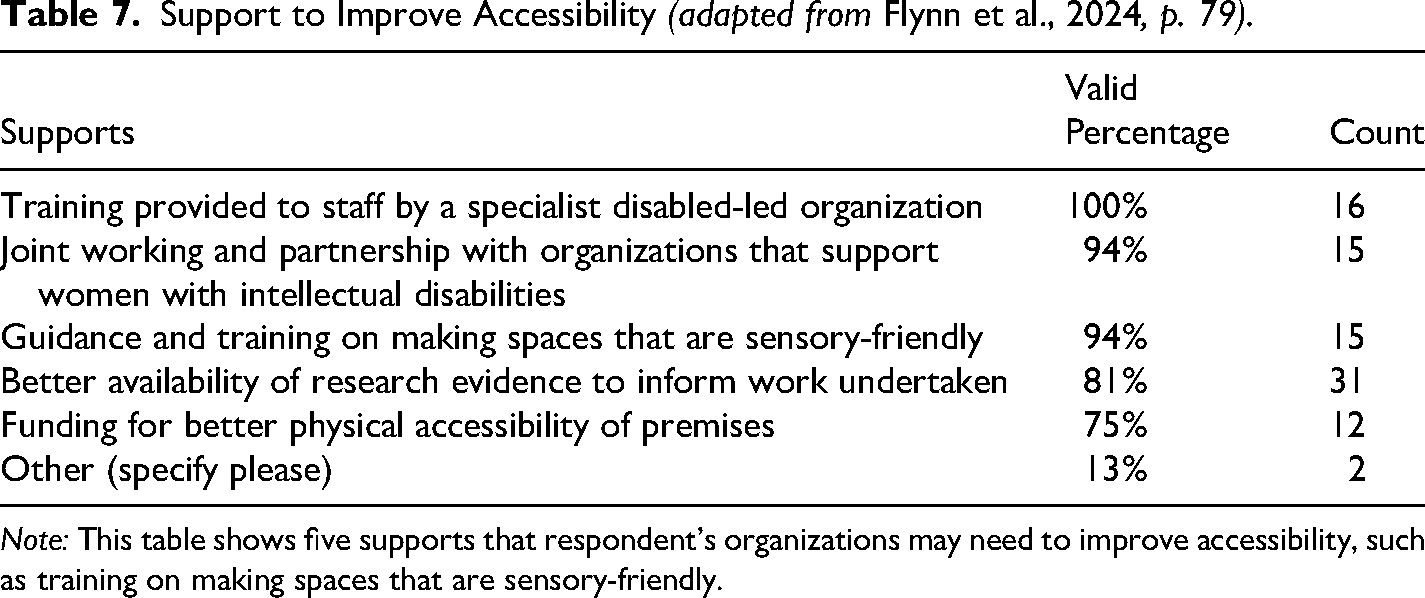
Note: This table shows five supports that respondent's organizations may need to improve accessibility, such as training on making spaces that are sensory-friendly.
Theme 4: Understanding of Disability
The next theme pertains to efforts by domestic violence organizations to understand disability, such as collecting information on the experience of disabled service users and undertaking disability training. This is important as existing research shows that disabled women may face unique and complex obstacles to help-seeking and experience unique and complex disability-specific forms of IPA (Flynn et al., 2024; Njelesani et al., 2021; Tenaw et al., 2023). In the survey, respondents were asked about training on supporting disabled women for staff. Of the 13 respondents to this next question, most indicated (n = 12) that their domestic violence service did not provide training on working with and supporting disabled women. For the one service that had training in place around supporting disabled women, it was indicated that this training pertained specifically to mental health problems like eating disorders and depression. Representatives of domestic violence services were also asked about training around understanding medical and social models of disability. In a quarter of cases, the respondents (23%, n = 3) had received training on this topic; however, most organizations had not (77%, n = 10). Thus, findings showed low levels of disability-specific training.
Understanding of disability may not, however, just arise from training. Respondents were therefore asked about collaborative working with disability services that hold expertise on disability. When asked about cross-over and collaboration in work between the representative's domestic violence organization and disability services, most respondents said this was not a feature of their organization's work (62%, n = 8). Approximately 38% (n = 5) of respondents, however, said that they had collaborated with disabled women's organizations in the past. Of these organizations, a further question was posed to determine the kinds of disabilities that the collaboration entailed. Most commonly, mental health issues were identified such as eating disorders and depression (60%, n = 3). Table 8 below provides more detailed information around responses.
Types of Disability Involved in Collaboration Work (adapted from Flynn et al., 2024, p. 75).
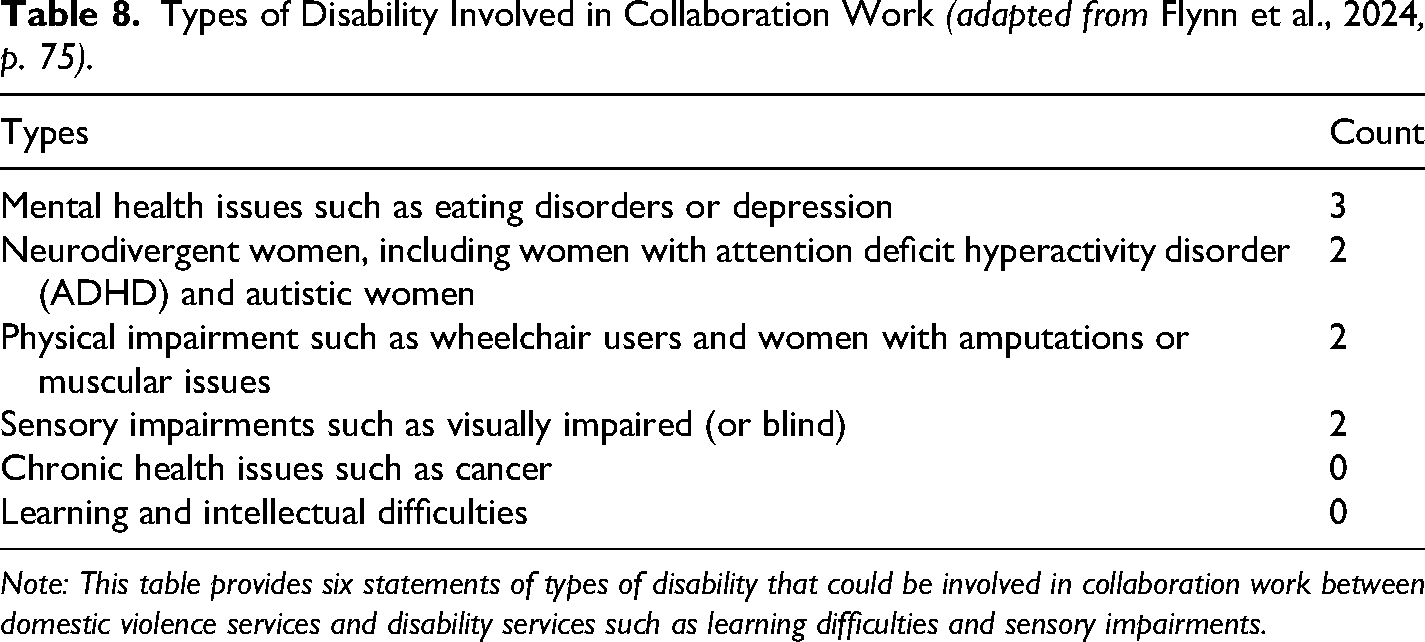
Note: This table provides six statements of types of disability that could be involved in collaboration work between domestic violence services and disability services such as learning difficulties and sensory impairments.
Toward further enquiry into the topic of understanding disability, representatives were asked about their awareness of abuse that is specific to disabled women. Fortunately, most organization representatives indicated that the organization promoted staff awareness of this form of abuse (67%, n = 10). Finally, organizational representatives were asked about whether they gathered data on disabled women who are service users. Out of the 14 services that responded to this question, six indicated that they collected some kind of data on the number of disabled women accessing their service. Within this, only two services enquired about disability with all service users. This means that the remaining services only recorded disability where it was actively disclosed by a woman. Services were then asked to specify the types of disability that they collected data on, if any. The most common data collection pertained to physical impairments (n = 6), followed by neurodivergence (n = 5), and followed by sensory impairments (n = 5).
Finally, the representatives of domestic violence organizations were asked to give percentage estimates about the number of disabled women who utilized their services over the past year (overall responses are n = 19). As the intention was to capture the subjective perception of how many service users had disability as a component of service preparedness, a standard definition of disability was intentionally not provided along with this question. 37% (n = 7) of representatives who responded to this question indicated that fewer than 10% of service users were estimated to be disabled. Approximately a quarter of respondents (n = 5) estimated that 11–20% of the overall user count for their organization would be disabled women. A further quarter (n = 5) could offer no estimate. Lastly, there were two organizations that estimated that disabled women accounted for 31–40% of their service users.
Theme 5: Involvement of Disabled Women
The fifth theme emerging from findings is about the involvement of disabled women in domestic violence organizations. This is important as international research shows that disabled women are more likely to experience IPA (Astbury & Walji, 2014; Garcia-Cuellar et al., 2023; Goulden et al., 2023; Jordan, 2022; Office for National Statistics, 2019), thus they should be involved in various ways in services that address IPA. In the survey, organizational representatives were asked if they specifically reach out to disabled women, and only 1 organization representative (7%) indicated that this was the case.
Representatives were then asked if they included disabled women in their organizational decision-making. Nearly a half and half split in responses were given to this question. Slightly more than half of the organizations (54%, n = 7) were not involving disabled women in decision-making. Less than half (46%, n = 6) were involving disabled women. To those who answered “Yes” to involving disabled women, a further question was posed, “Could you please elaborate on how disabled women are involved in decision-making about the organisation?” (Flynn et al., 2024, p. 78). Various responses were given to this, and these included involving women in developing a strategic plan, involving them through stakeholder consultation, through inclusive feedback and evaluation materials, and at board level.
Finally, organizational representatives were asked about staff members who are disabled women. They were asked if they had a presence of disabled women in their staff teams. Approximately 67% (n = 8) of representatives stated that they did not, while 33% (n = 4) of representatives stated that they did. Taken together, the findings demonstrate some involvement of disabled women in service provision and operation, with scope remaining to significantly improve this.
Theme 6: Diversity in Service Provision
The sixth and final theme refers to diversity in service provision. Here diversity refers to the provision of different kinds of support services through varied channels. This service diversity is important, as it makes services more accessible to disabled women who have diverse needs. This was investigated within the mapping exercise using publicly available information. Among the sample of services investigated, the most common form of support that was apparent was telephone or helpline support which appeared to be available for 69% (n = 31) of organizations. After this, non-counseling advice and emotional support as well as accompaniment to court and elsewhere, appeared available in 60% (n = 27) of organizations. Table 9 below provides more detail on data gathered from the investigation into available supports.
Services and the Proportion of Organizations That Appear to Provide Those Services (adapted from Flynn et al., 2024, p. 81).
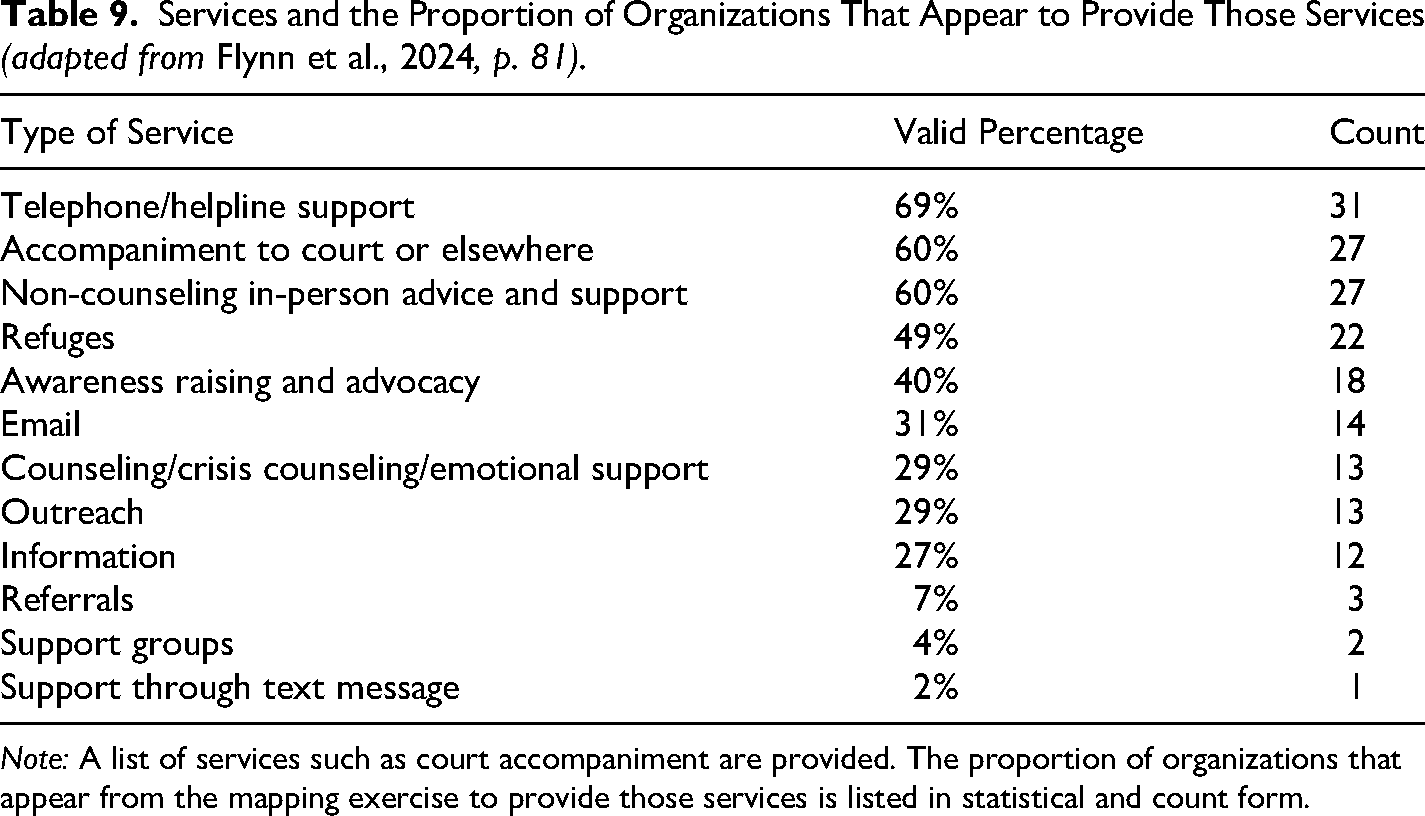
Note: A list of services such as court accompaniment are provided. The proportion of organizations that appear from the mapping exercise to provide those services is listed in statistical and count form.
Discussion
The aim of this article has been to present findings of a mixed-method study. By now, it is conclusive that diverse insights emerge from these findings on the accessibility of specialist domestic violence services for disabled women in the Republic of Ireland. From these findings, higher level implications are possible to draw out for the wider field of knowledge on disability accessibility and domestic violence services. These implications should be considered, however, within the relevant context of under-funding and under-resourcing of Irish domestic violence services in tandem with high levels of service demand.
One key focus of the findings was the accessibility of information (theme 2) for disabled women. Findings demonstrated that services did not consistently provide accessible formats of information such as plain English and easy-read information. It was also concerning from findings that no services offered accessible information in Braille. Provision of accessible information is vital in engaging with disabled women experiencing IPA according to Alhusen et al. (2020). One reason for this, illustrated in existing research by Chang et al. (2003), is that disabled women may accept and normalize abuse because of problems with accessing support and information, meaning that they stay longer in abusive situations. Another troubling aspect of information inaccessibility is that existing evidence suggests that intellectually disabled women are at increased risk of abuse but may not be able to recognize it without the correct information (Smith, 2008). These findings tally with observations made in existing research about the presence of increased challenges for disabled women accessing support above their non-disabled peers (Ruiz-Pérez et al., 2018). This includes systemic barriers that prevent disabled women exiting relationships and disclosing abuse, such as being unable to contact domestic violence services due to inaccessible information (Alhusen et al., 2020).
Findings (theme 7) also demonstrate low proactivity and rigor from services in collecting data about disabled women who access their service. This bolsters an existing lack of awareness and data around disabled women experiencing IPA (Ruiz-Pérez et al., 2018), leaving services to effectively operate in the dark. It should be acknowledged here that such data gathering is far from straight-forward but rather it is fraught with complexity (Flynn et al., 2024). There were also varied estimates given by representatives about the number of disabled women accessing their services. Most estimates lay in the range of between 10% and 20% of service users. In comparison, however, specialist domestic violence services in Wales and England have recently reported that 28.7% of victims/survivors accessing their services had disability (Women's Aid, 2023). Moreover, while research estimates vary, recent research from the Office for National Statistics in United Kingdom (2019) suggests that disabled women are beyond twice as likely to have IPA perpetrated against them than for their non-disabled peers. The study also found a staggering 1 out of 6 (17.3%) disabled women had experience of domestic abuse (17.3%). Therefore, the estimates given by services in the study not only appear conservative, but potentially indicative of a low take-up of services by disabled women in need.
This is further problematic due to existing evidence of disability-specific barriers to disabled women engaging with generic DVA services that must be overcome. Within this, fear of encountering ableist service provision where services are only designed with abled women in mind is one considerable barrier of note (Jordan, 2022). Thus, the lack of imagery of disabled women on service landing pages in all but 2% of organizations in this study is worrying (Office for National Statistics, 2019). Collaboration can, however, be a means to enhance understanding and insight about disability-related needs so that services can be made more inclusive to disabled women. Systematic review by Garcia-Cuellar et al. (2023, p. 1) finds that IPA against disabled women “involves two public health issues interacting simultaneously.” Given this complexity and convergence, it is unsurprising that findings emphasize the need for collaboration between DVA services and disability services, as well as the value of engaging directly with disabled women to gather their advice and expertise.
Another key focus of the findings was awareness within services of disability and DVA (theme 4, theme 5). Findings showed a low level of disability-specific training for DVA services’ staff as well as a lack of collaboration with disability services to create better informed and coordinated services. This is problematic as existing research shows that there are unique complexities that must be understood with IPA against disabled women. This includes disability-specific forms of abuse such as hiding medication and disability-specific name calling (Flynn et al., 2024; Brooke, Lewis and Washington, 2014). Anyango et al. (2023) also highlight the potential for disabled women to not be believed or taken seriously as a result of having disability when they do disclose. Thus, services would benefit from training staff to promote disability awareness and disability-sensitive practices.
In addition to disability-specific abuse being a significant part of IPA perpetrated against disabled women (Bonomi et al., 2018), a disabled woman may be dependent on their abuser for supports to do basic things like eat, bathe, and move (Flynn et al., 2024). It is vital therefore that disabled women can be confident in reaching out to DVA services that their disability-related needs can be met as they may no longer be able to turn to their abuser for this support. Regrettable in this context are deficits in practical accessibility highlighted by this study's findings with only one organization having “adequate devices and assistive technology” and only 44% (n = 7) having pathways and doors wide enough for a wheelchair user. Only approximately half of services appeared to have wheelchair accessible entrances. It is also important that refuges and support services actively make it known if they are accessible. Findings showed however that only one service actively attempted to reach out to disabled women. This is problematic as existing research shows that disabled women may have more restricted social networks, thus having less opportunities to disclose (Smith, 2008) and may be unaware of whether services can help them (Flynn et al., 2024).
It was positive that many services in this study could be reached by public transport as an affordable mode of travel, given that being unemployed heightens risk of IPA for disabled women (Smith, 2008), in the context of vulnerabilities to economic abuse also (Garcia-Cuellar et al., 2023). As economic abuse is a major factor within IPA perpetrated against disabled women (Garcia-Cuellar et al., 2023), it is important to recognize a disabled women's journey to safety in holistic terms. It is not only refuges as a vital but temporary solution, for instance, that should be accessible but also transitional and safe home housing services to support disabled women fleeing abuse into the long term (Flynn et al., 2024).
Remote access to support such as through telephone helplines and websites can be a crucial aid. It is regrettable therefore that findings allude to only 24% of websites having a high “Easy-read score 6 or 7,” while 4% of services appeared to have no remote access via the internet. While remote and digital access is important for inclusivity, having multiple diverse methods to access services is perhaps most constructive, in light of findings by Bonomi et al. (2018) that technology-related abuse such as control of devices can be a key feature of IPA against disabled women. The diversity of supports covered in this study, from in-person counseling to text support to court accompaniment are all important for accessibility and inclusion.
Overall, findings clearly demonstrate that organizations must improve the way they serve disabled women, while improving expertise and knowledge held on disability through research and training. This tallies with existing research that shows how disabled women are at significantly higher risk of IPA in all its major forms and experience unique barriers to help-seeking such as disability-related mistrust of services and isolation (Anyango et al., 2023). Before concluding, there are some limitations to this research that should be noted. These include an absence of the voices and experiences of disabled women on the accessibility of services. Lack of consideration of how the intersectionality of identities of disabled women such as pertaining to race, ethnicity, gender, and religion may impact findings is also a study limitation. While a good response rate was achieved for the survey, thus making findings generalizable within the context of the country, there are limits to generalizability to the international context. Findings do demonstrate relevance, however, to international research in echoing existing evidence-based observations. This includes observations that services need more resourcing and knowledge building internationally to meet women's disability-specific needs while improving disability accessibility (Namatovu et al., 2022).
Finally, recommendations arising from this research should be outlined. It is recommended that multi-annual governmental funding is ring-fenced for urgent capacity building of DVA services to meet disabled women's needs. This includes on-going funding for continuity of services toward undertaking data collection on disabled service users. This also includes funding for the delivery of disability awareness training undertaken in collaboration with disabled person led organizations. It is recommended that further research is undertaken to improve understanding of IPA against disabled women. It is also recommended that domestic violence services in the Republic of Ireland implement accessibility measures specifically identified as absent through this research. Lastly, it is recommended that collaborative initiatives are fostered between disability services and domestic violence services to ensure coordinated action and joined up thinking.
Conclusion
IPA of disabled women is a major public health concern and matter of critical importance for specialist domestic violence services. Yet, the gap in knowledge and data in this space significantly jeopardizes the capacity of domestic violence services to respond effectively to disabled women (Ruiz-Pérez et al., 2018). This article presented findings of a national survey and a mapping exercise, both of which were geared toward ascertaining the accessibility standard of domestic violence services for disabled women. While many strengths were noted around access routes to domestic violence services for disabled women, findings also show significant areas for improvement. As such, recommendations have been made toward improving the accessibility of domestic violence services, and better resourcing services so that those service improvements can become a reality.
Footnotes
Acknowledgements
The contribution of study participants, advisory committee members for the study, and anonymous peer-reviewers should be acknowledged.
The authors wish to acknowledge the important contributions of research participants, the study Advisory Group, Women's Aid for their funding support, and the anonymous peer-reviewers.
Ethics Approval Statement
Ethical approval was granted for this study from the School of Social Work and Social Policy at Trinity College Dublin.
Funding
The authors disclosed receipt of the following financial support for the research published in this article: This work was supported by the Board at Women's Aid, the Republic of Ireland [no grant number].
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.