
Abstract
Survivors of intimate partner violence face significant mental health challenges, yet few interventions explore physical activity's role in recovery. This mixed-methods study evaluated a 10-week maximal strength training program for female IPV survivors (N = 36), examining mental health and well-being outcomes, and implementation factors. Thematic analysis of interviews (n = 23) identified rebuilding agency and enhanced well-being as key benefits. Quantitative results showed moderate-to-large improvements in depression (ES = 0.6), anxiety (ES = 0.6), stress (ES = 0.7), self-esteem (ES = 0.8), and body appreciation (ES = 0.5). Findings suggest strength training provides a promising trauma-informed approach. Implementation requires trauma-informed practices and instructor training for effectiveness and sustainability.
Introduction
Intimate partner violence (IPV), encompassing physical, sexual, financial, and psychological abuse perpetrated by current or former partners, represents a severe and pervasive global health concern (World Health Organization, 2013). Approximately 27% of women aged 15–49 worldwide have experienced physical or sexual violence by intimate partners (World Health Organization, 2021). In the Australian context, these patterns persist, with an estimated 23% (2.3 million) of women over 18 having experienced physical and/or sexual violence from an intimate partner since age 15, and a comparable proportion enduring emotional abuse (Australian Bureau of Statistics, 2023). While relationship violence can be bidirectional, women disproportionately experience its primary impacts, with men predominantly identified as perpetrators (Australian Bureau of Statistics, 2023).
The consequences of IPV are far-reaching, affecting both physical and psychological health. Survivors are at increased risk of experiencing mental health issues, including post-traumatic stress disorder (PTSD), depression, anxiety, and suicidal ideation (Bacchus et al., 2018; White et al., 2024). The repeated physical and emotional abuse deteriorates self-esteem and sense of identity, with women reporting feelings of worthlessness, significantly impacting their overall mental health and quality of life (Matheson et al., 2015).
Intimate partner violence has substantial and lasting effects on survivors’ physical health. Survivors face increased risk of chronic diseases, pain, and sexually transmitted infections (Dillon et al., 2013; Stubbs & Szoeke, 2022). Additionally, women who experienced IPV are more likely to participate in risky behaviour such as drug and alcohol abuse (Stubbs & Szoeke, 2022), which may further exacerbate mental health symptoms and create additional barriers to recovery and overall well-being. The health impacts of IPV can persist long after the abuse has ended. Even after leaving abusive relationships, women may continue to experience poorer physical and mental health outcomes compared to women without IPV history (Dillon et al., 2013; Hing et al., 2021).
Psychosocial interventions are among the most commonly practised approaches to addressing the consequences of IPV. These interventions aim to empower survivors through advocacy-based approaches and target mental health impacts through clinical interventions (Trabold et al., 2020). While a 2024 meta-analysis showed that combined advocacy and clinical support can significantly reduce depression and PTSD symptoms (Micklitz et al., 2024), these interventions have demonstrated limitations. Programs consistently report modest effects, inconsistent long-term maintenance, and significant dropout rates (Micklitz et al., 2024; Trabold et al., 2020).
Physical activity interventions have emerged as a promising adjunct treatment for trauma recovery. Trauma-sensitive yoga has demonstrated efficacy in reducing PTSD symptoms and improving body awareness and self-confidence among trauma survivors, particularly through its focus on present-moment awareness, choice-making, and cultivating safety (Nguyen-Feng et al., 2019). Martial arts and boxing programs have demonstrated how structured physical activity can support recovery among sexual assault survivors through increased self-defence self-efficacy, enhanced feelings of empowerment and bodily autonomy, improved ability to manage PTSD symptoms, and access to supportive communities (Higgins et al., 2024).
While trauma-sensitive yoga and martial arts programs have demonstrated promising results in supporting survivors’ recovery, emerging research on strength-based activities presents new intervention possibilities. Resistance training has been associated with improvements in PTSD symptoms (Whitworth et al., 2017, 2019) and enhanced self-efficacy (O’Connor et al., 2010). A recent grounded theory study by Nowakowski-Sims et al. (2023) found that weightlifting contributed to reduced symptoms of depression and anxiety, improved mood, and increased mental resilience among individuals with diverse trauma histories. Participants also reported feeling more empowered and capable, both physically and mentally. Additionally, the gym environment provided a supportive community, helping participants feel connected and supported in their healing process.
Beyond mental health symptoms, IPV erodes survivors’ relationships with their bodies. Verbal abuse targeting physical appearance, combined with physical and sexual objectification, can lead to body shame and self-objectification (Davidson & Gervais, 2015). Survivors may internalise these feelings of weakness and vulnerability, diminishing their ability to appreciate and respect their bodies. The physical abuse also disrupts survivors’ sense of body ownership and control (Machorrinho et al., 2023), potentially diminishing appreciation for their body's functional capabilities.
Strength-based activities offer a pathway to address body-related impacts. Strength training offers women opportunities to experience both physical capability and bodily autonomy. Experiencing physical capability challenges cultural pressures that encourage women to view their bodies as objects, promoting the rejection of self-objectification and fostering a more positive body image (Menzel & Levine, 2011). Similarly, experiencing bodily autonomy counters feelings of lost control. The progressive development of physical strength disrupts feelings of vulnerability and weakness, which often stem from IPV. Supporting this idea, Kelly et al. (2023) found that female powerlifters reported greater appreciation for their body's functionality, rejection of societal gendered body ideals, and increased self-compassion.
Despite growing evidence supporting exercise's potential in trauma recovery, a critical research gap persists. No existing studies have specifically investigated strength training as an intervention for intimate partner violence survivors’ recovery. This study addresses this gap by examining how a maximal strength training program influences mental health and well-being among survivors of intimate partner violence. In this study, well-being was conceptualised as a multidimensional concept that goes beyond mental health symptoms. Mental health was assessed through depression, anxiety, and stress indicators, while well-being included body appreciation, functionality appreciation, and self-objectification. These body-related constructs are especially significant for IPV survivors, as abuse often erodes survivors’ sense of body control and positive body relationship.
To explore potential mechanisms of maximal strength training, we measured both physical and psychological outcomes. Physical strength was evaluated using isometric mid-thigh pull (IMTP) to provide objective evidence of strength development and to examine whether subjective experiences of increased strength aligned with measured strength gains. We also measured body composition with dual-energy X-ray absorptiometry (DXA) to determine whether improvements in body image were dependent on changes in physical appearance rather than enhanced physical ability. By exploring both quantitative outcomes and survivors lived experiences, we aim to provide a comprehensive understanding of the potential of strength training as an intervention. A secondary aim is to identify implementation factors and elements that support survivors’ engagement, ensuring the program's effectiveness and sustainability in real-world settings. Our findings will not only extend the current evidence base for physical activity interventions but also offer insights for developing trauma-informed physical activity intervention strategies that centre survivors.
Method
Study Design
This study utilised a convergent parallel mixed-methods design (QUAL + quan) to examine the impact of maximal strength training on mental health and well-being among survivors of IPV (Creswell & Creswell, 2017). Data collection involved two concurrent streams: qualitative post-intervention interviews and quantitative pre-post outcome measures. While both datasets were analysed independently, priority was given to qualitative findings to centre participants lived experiences of the program. The quantitative data enabled the assessment of objective changes in strength, body composition and mental health measures.
A pragmatic epistemological approach guided the mixed methods design (Johnson & Onwuegbuzie, 2004). This stance recognises that neither quantitative measures nor subjective experiences alone can fully capture the complex nature of survivor healing. The prioritisation of qualitative data aligns with trauma-informed principles by centring survivors’ experiences and voices while using quantitative outcomes to support their narratives (Ellsberg & Heise, 2002).
Participants
Participants were recruited through partnerships with IPV support services in Canberra, Australian Capital Territory, Australia. Eligible participants were women aged 18 years or older who had experienced IPV at any point in their lifetime. No physical activity prerequisites were required for participation.
Recruitment utilised multiple pathways. Support service staff shared study information with eligible clients during routine appointments. Information was also disseminated through recruitment flyers in service waiting areas, posts on service centre social media platforms, and inclusion in service newsletters. Interested participants could either contact the research team directly or authorise support service staff to provide their contact information to the research team. All potential participants completed screening and informed consent procedures with trained research staff prior to enrolment. By responding to recruitment materials specifically targeting IPV survivors, participants self-identified their eligibility without being required to provide documentation or detailed descriptions of their abuse experiences.
We did not assess whether IPV was current or historical. This decision reflected the trauma-informed principle of avoiding potentially re-traumatising questions about abuse. While participants recruited through support services maintained ongoing relationships with those services, all participants were provided with referral information to support services, and research staff were trained to identify signs of distress and facilitate connections to support if needed. The University of Canberra Human Ethics Committee approved the study (HREC 4796).
Program Design
The 10-week maximal strength training intervention consisted of twice-weekly, 60-min sessions. Female certified strength coaches led all sessions. The program followed a structured progressive overload principle focused on compound movements: squats, deadlifts, bench press, and overhead press.
Initial sessions (weeks 1–3) emphasised technical development and adaptation, with participants performing three sets of 8–10 repetitions at 60–70% of their predicted one-repetition maximum (1RM). During the middle phase (weeks 4–7), the intensity increased progressively as participants advanced to three sets of 6–8 repetitions at 70–80% of predicted 1RM. The final phase (weeks 8–10) focused on maximal strength development, with participants performing three sets of 3–5 repetitions at 80–90% of predicted 1RM.
Groups were capped at 8 participants per session to ensure safety and appropriate supervision. Each session included a standardised warm-up, technical instruction, and supervision of all lifts. Trainers provided individualised load adjustments based on participant capability and comfort. Participants documented their progression via training journals.
Trauma-Informed Program Delivery
The program was implemented according to trauma-informed principles, emphasising safety, participant choice, and empowerment (Darroch et al., 2024; Pebole et al., 2021). Training sessions were held in a female-only, private area that was not visible to the public view or the general gym environment. Male gym staff were instructed not to enter the training space during scheduled program sessions. The structure of each session was displayed on a whiteboard, providing transparency and predictability.
Participants controlled their level of engagement throughout the program. Alternative exercises were always available, and participants could opt out of any activity. Progression was participant-led, with coaches providing suggested weight ranges based on each participant's previous lifts. While most participants chose to engage fully and often requested additional challenges, on days when some felt vulnerable, they could participate minimally and attend for social support. Participants could withdraw from any activity or session at any time without providing an explanation. The program also emphasised consent and boundaries. Physical corrections were only made with explicit permission, such as asking, “Can I touch your back to show you where you should be feeling this lift?” The group training format was intentionally chosen to align with trauma-informed principles of peer support and connection, recognising that IPV often involves social isolation.
Data Collection
Qualitative Methods
Semi-structured interviews were conducted within two weeks of program completion. Twenty-three participants participated in the interviews. This sample size provided sufficient information power (Malterud et al., 2016) given the study's focused aims (understanding experiences of a specific 10 week strength training intervention) and sample specificity (IPV survivors who completed the program). Interviews took place in a private room at the University Health Clinic. The first author (EK), who was experienced in qualitative interviewing, conducted all interviews.
The interview guide was developed following trauma-informed principles, focusing on participants’ experiences with the program without exploring their histories of IPV. This protocol design helped ensure participants’ emotional safety while aligning with trauma-informed practices (Ellsberg & Heise, 2002). The guide was organised into three main domains: Program experiences and impact, program engagement, and program implementation factors that supported or hindered their participation. Questions progressed from broad opening queries (e.g., “What was your experience of the program?”) to more specific prompts exploring physical and psychological impacts. Follow-up probes were used to elicit deeper reflection while maintaining clear boundaries around trauma disclosure.
All interviews were audio-recorded with participant consent and transcribed verbatim by a professional transcription service.
Quantitative Methods
All baseline and post-intervention assessments were conducted at the University Health Clinic. During initial visits, participants completed demographic questionnaires and psychological measures on Qualtrics. The psychological assessments included the Depression Anxiety Stress Scales-21 (DASS-21) (Lovibond & Lovibond, 1995), the Rosenberg Self-Esteem Scale (RSES) (Rosenberg, 1965), Body Appreciation Scale-2 (BAS-2) (Tylka & Wood-Barcalow, 2015), the Functionality Appreciation Scale (FAS) (Alleva et al., 2017), and the Self-Objectification Questionnaire (SOQ) (Noll & Fredrickson, 1998).
A qualified Clinical Densitometrist performed DXA scans during the same session. Strength assessments (IMTP) were conducted separately in the university sports laboratory before the first training session and after program completion.
Measures
Psychological Measures
Depression, Anxiety and Stress
Depression Anxiety Stress Scales-21 (Lovibond & Lovibond, 1995) was used to assess psychological distress. The DASS-21 comprises three 7-item subscales measuring depression (e.g., “I couldn't seem to experience any positive feeling at all”), anxiety (e.g., “I felt scared without any good reason”), and stress (e.g., “I found it hard to wind down”). Participants rate symptom presence over the past week using a 4-point Likert scale (0 = “Never” to 3 = “Almost always”). Subscale scores range from 0–21, with higher scores indicating greater symptom severity. The DASS-21 has demonstrated good reliability and validity in non-clinical populations (Henry & Crawford, 2005)
Self-Esteem
Rosenberg Self-Esteem Scale (Rosenberg, 1965) a 10-item instrument. Participants respond to statements such as “I feel that I have a number of good qualities” and “On the whole, I am satisfied with myself” using a 4-point Likert scale (1 = “Strongly disagree” to 4 = “Strongly agree”). Total scores range from 10–40, with higher scores indicating higher self-esteem and has well-established reliability and validity across diverse populations (Robins et al., 2001).
Body Image
Body image was assessed using three measures. The 10-item BAS-2 (Tylka & Wood-Barcalow, 2015) measures positive body image (e.g., “I respect my body”). Items are rated on a 5-point scale (1 = “Never” to 5 = “Always”), with scores ranging from 1–5. Higher scores indicate greater body appreciation.
The 7-item FAS (Alleva et al., 2017) assesses appreciation for body functionality (e.g., “I appreciate my body for what it is capable of doing”). Items use a 5-point scale (1 = “Strongly disagree” to 5 = “Strongly agree”), with mean scores ranging from 1–5. Higher scores indicate greater functionality appreciation.
The SOQ (Noll & Fredrickson, 1998)measures the extent to which individuals value appearance versus functionality attributes. Participants rank 10 body attributes in order of importance to their physical self-concept: five appearance-related (e.g., physical attractiveness, weight) and five functionality-related (e.g., physical coordination, strength). Rankings for functionality items are subtracted from appearance items, yielding scores from −25 to 25. Higher scores indicate greater self-objectification.
Physical Measures
Muscular Strength
Maximal strength was measured via IMTP using a force plate (600 × 400 mm 200 Hz force-plate; Kistler 9286AA). Following a standardized warm-up, participants performed the IMTP with a fixed barbell positioned at mid-thigh height. The testing position involved slightly flexed hips and knees (approximately 145 degrees), with participants maintaining an upright torso, shoulders over the bar, and head neutral. Following three submaximal familiarisation attempts, participants performed three maximal effort pulls (3–5 s duration) with 3-min rest periods between attempts. The highest peak force value was used for analysis. The protocol has demonstrated good reliability in populations including untrained females (Drake et al., 2017).
Body Composition
Body composition was assessed using DXA (GE Lunar Prodigy) operated by a certified Clinical Densitometrist and analysed using GE Encore software (enCORE Version 17; GE Healthcare). Participants were measured in the morning following standardised conditions: 8-h fast, normal hydration, and wearing light clothing free of metal objects. Positioning was as described by Nana et al. (2012). The scan provided measurements of total body fat mass, lean mass, and bone mineral content. Scanner calibration was performed daily using a manufacturer-supplied phantom. The coefficient of variation (CV) for lean body mass was 0.7%, with a least significant change (LSC, 95% CI) of 1.9%. For fat mass, the CV was 1.3%, with an LSC (95% CI) of 3.7%.
Consistent with trauma-informed practices, body composition assessments were optional, and participants could decline or withdraw at any point. The DXA scan procedure was explained fully in advance, and participants were shown the scanner before deciding to proceed. Scans were conducted in a private room by a female Clinical Densitometrist with no other individuals present. Participants wore their own clothing and were not required to change. Any necessary positioning adjustments required explicit consent before touch. Participants could choose whether to receive their body composition results. When results were shared, they were explained with emphasis on health indicators rather than appearance or aesthetic body composition measures.
Data Analysis
Qualitative Analysis
Interview data were analysed using thematic analysis following Braun and Clarke's (2019) six-phase approach. (1) Familiarisation: Analysis began with data immersion, where two researchers independently conducted repeated readings of interview transcripts to develop deep familiarity with the content. (2) Initial Coding: Initial codes were generated inductively. The researchers met regularly to discuss emerging codes and their interpretations. (3) Searching for Themes: The initial inductive generated codes were then examined through a deductive lens focusing on themes specifically related to the project aims such as the impact on mental health and wellbeing, engagement, and implementation. This combination of inductive and deductive approaches allowed the researchers to remain grounded in participants’ experiences while addressing the objectives. (4) Reviewing Themes: Theme development involved an iterative process of reviewing, refining, and mapping relationships between themes. The research team met regularly to challenge interpretations and explore alternative explanations. When discrepancies arose, researchers returned to the original transcripts and discussed until reaching consensus, prioritising interpretations that best represented participants’ voiced experiences. (5) Defining and Naming Themes: Final themes were developed through consensus, with careful attention to selecting representative quotes that captured both the essence of each theme and participants’ voices. (6) Producing the Report: Themes were integrated with quantitative findings to provide a comprehensive understanding of the program impact.
Quantitative Statistical Analysis
Linear mixed models with a random intercept for each participant were created to model the effect of the 10-week maximal strength training program on psychological and physical outcomes. For each model, time-point (Pre-, Post-program) was included as the fixed factor, and the respective psychological or physical variable was included as the response variable. Model results are reported as unstandardised slope estimate for time-point (B), standardised effect sizes (ES), and 95% confidence intervals ([lower - upper]). Standardised effect sizes were calculated as the estimated unstandardised slope estimate divided by the square root of the sum of the random effects and residual variances. Standardised effect sizes can loosely be interpreted using Cohen's d thresholds (trivial: |ES| < 0.2, small: |ES| = 0.20–0.49, moderate: |ES| = 0.50–0.79, and large: |ES| > 0.80) (Cohen, 2013), although the main purpose of calculating standardised effect sizes was to provide comparison of effects across variables, and to provide a sense of the program's impact relative to the total variability in the response variables (which includes variability from both fixed effects and random effects along with residual error).
R (version 4.4.0) in RStudio (version 2024.04.2 + 764) was used for all analysis; the ‘lme4’ package (Bates et al., 2015) was used to conduct the linear mixed modelling; and the ‘emmeans’ package was used to facilitate standardised effect size calculations (Searle et al., 2012).
Results
Participant Characteristics
Thirty-six women who had experienced IPV completed the maximal strength training intervention and evaluation measures. Participant demographics are shown in Table 1.
Participant Characteristics.
Integrated Findings
Analysis of 23 semi-structured interviews revealed four key themes: rebuilding strength and agency, mental health and well-being, social and community connection, and program-specific elements. These themes have been integrated with quantitative findings where relevant.
Rebuilding Strength and Agency
The maximal strength training program provided a structured pathway for survivors to rebuild strength and agency. Through progressive resistance training, participants developed physical capabilities that countered their previous experiences of powerlessness. Catherine shared:
Coming from a place of complete powerlessness… I think just anything that gets you back in connection with your body and your mind, and also that gets you physically stronger so you feel more resilient, is quite empowering and powerful.
The feeling of increased physical strength gained from the program translated into practical empowerment outside the gym, particularly in challenging situations. As Joan described when discussing her court appearances:
When I stand up in court at the moment, that's the thing that is the most troubling to me and most terrifying and humiliating, but I do stand up there, and I feel my body stands a bit stronger, and I feel I’ve got a few muscles. I can stand here. My body can make me stand up, emotions and keep working. But my body is not feeble and weak.
The program structure of progression and achievement fostered self-efficacy among the participants. Physical accomplishments provided tangible evidence of capability, challenging negative self-views often internalised through abuse. Florence shared:
It was more just the strength part, and the exercise was just a focal point for me. It focused, something to focus on, something to achieve. I'm still able to achieve something. I'm not useless. I'm still worth something. It made me feel stronger.
Tuesday and Thursday became my favourite day of the week… I'm tracking my little progress on my chart… I feel like I can do anything. If I can figure this out, I can figure out other things.
Ultimately, this emphasis on personal investment and achievement helped counter feelings of worthlessness common among IPV survivors. Joan articulated this impact: I'm worth investing in and worth investing in physically. And I think I've got everything else in life telling me I'm pretty worthless… this is sort of a bit of a gain back into the cup. You know the cup feels pretty empty, but this is something that's starting to fill it up a little bit more.
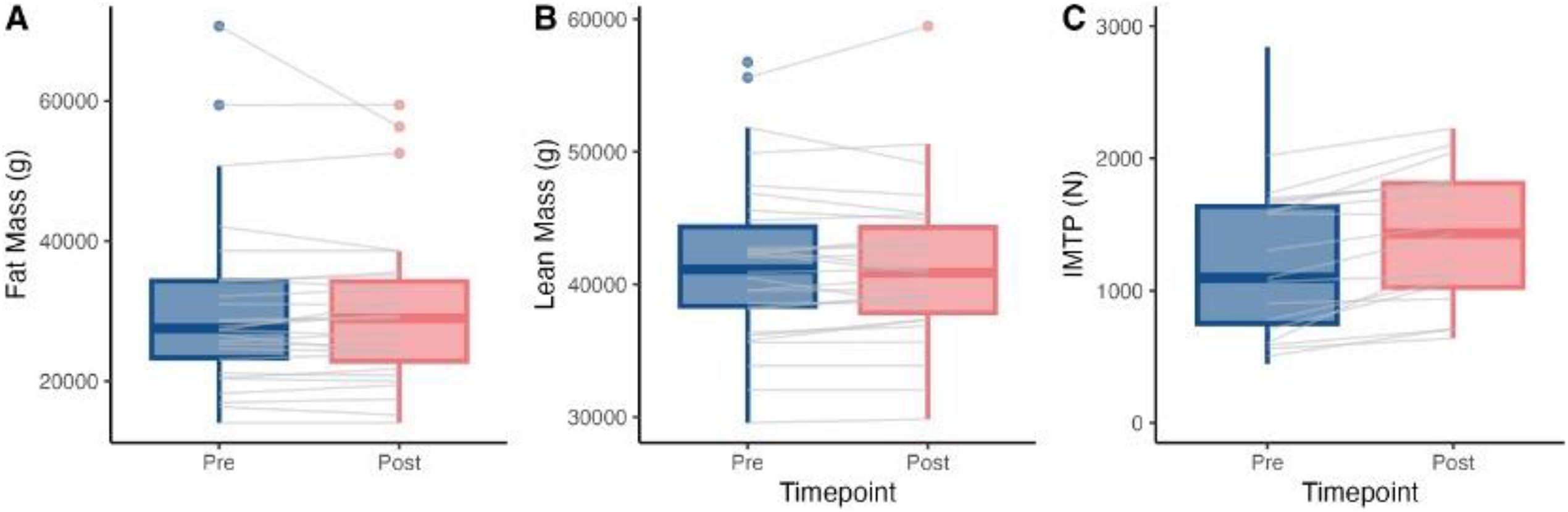
The effect of the program on physical measurements. Grey lines show the effects for individual participants. IMTP: Isometric Mid Thigh Pull.
Participants’ narratives about increased self-worth resulting from personal investment and achievement were reflected in quantitative improvements in self-esteem (B = 4.0 [2.1–5.8], ES = 0.8 [0.4–1.1], p < 0.001) (Figure 3D), which showed a moderate effect size. This finding supports the qualitative insights that developing physical strength helped rebuild participants’ sense of value and capability.
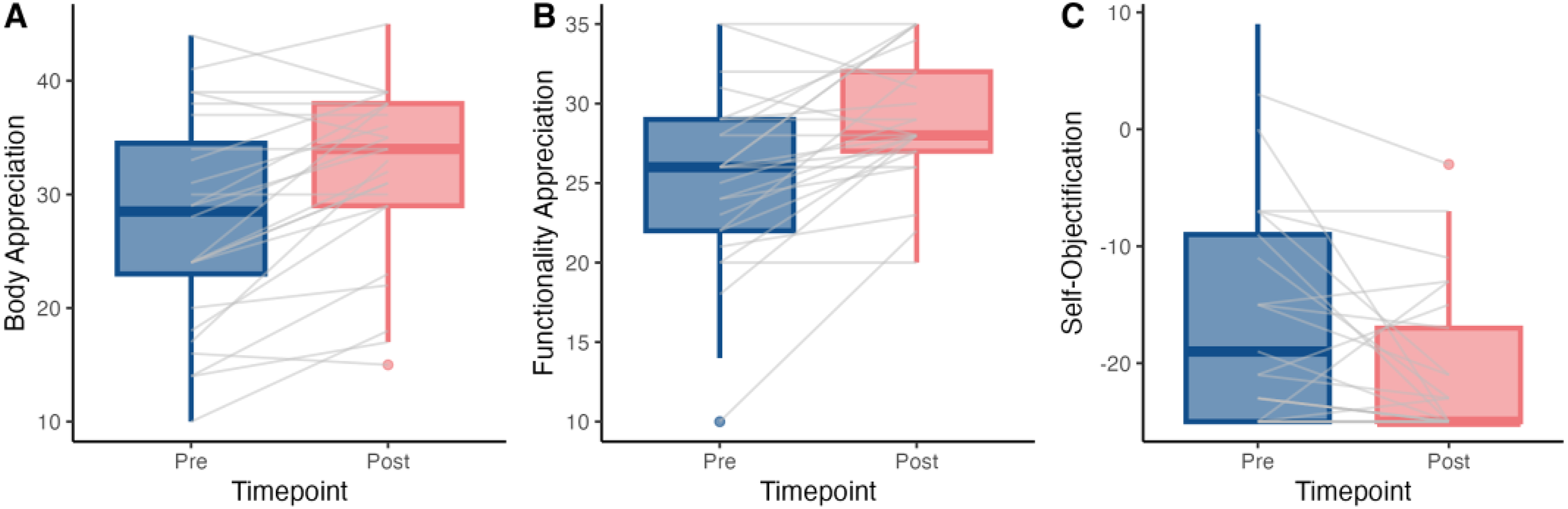
The effect of the program on body appreciation scores. Grey lines show the effects for individual participants.
The growth in physical capabilities also paralleled changes in how participants perceived and appreciated their bodies. Body appreciation (B = 4.5 [2.4–6.6], ES = 0.5 [0.3–0.8], p < 0.001) and functionality appreciation (B = 3.6 [1.8–5.3], ES = 0.7 [0.4–1.1], p < 0.001) both improved with moderate effect sizes, while self-objectification scores decreased (B = -3.8 [-6.8—−0.7], ES = 0.4 [0.1–0.8], p = 0.018) with a small effect size (Figure 2). Notably, these improvements in body perception occurred despite no significant changes in body composition, with neither lean mass (B = 110.4 [-411.4, 632.2], ES = 0.02 [-0.07, 0.10], p = 0.667), or fat mass (B = -310.1 [-1554.7, 934.4], ES = -0.03 [-0.13, 0.08], p = 0.613) showing meaningful change (Figure 1).
Mental Health and Well-Being
The strength training program generated multiple mental health benefits. Participants reported improvements in their perception of overall mental health, symptom management, and their capacity to prioritise self-care.
Participants attributed mental health improvements directly to the program's physical focus. As Catherine explained: I think it's positive because you're actually doing something with moving your body, and I think there is that concept of if you move your body it helps with the trauma, and I think it definitely does. This physical-mental connection strengthened with their physical strength, as Marie noted: I feel a lot more psychologically stronger… I think that strength almost appears to be holistic. So, if your body strength is good, then your mind is good too.
The program's structured nature helped participants manage specific mental health symptoms. Josephine described how the program provided motivation and routine: Well, I was struggling to get out of bed and so even getting out of bed to do this one thing was important to me… Then you find that once you do that you start to do other things as well. This impact on symptoms extended beyond the training sessions, as Christine shared: “By the time I drove home, I felt much calmer. Much more at ease with me, with myself.”
Beyond symptom management, participants shared that making small, incremental changes during the program helped them feel more resilient. Taylor shared:
It's a reminder, yes, we do adapt because when I was there in the bad spot, you think, ‘This just sucks, and how am I going to get out of here?’ So, it's a reminder that through physical activity, we do adapt as human beings to different environments and don’t die.
Finally, the program created a framework for participants to prioritise their own well-being, often for the first time since experiencing abuse. As Malala explained: “It has been so good for me because it's made me realise that physical health, and focusing on it, is really important. I think it's the key to the emotional and any body image things and all that.” This self-prioritisation became sustainable through the program's regular schedule, as Catherine described: “I've set aside that time to focus in on myself to do the health stuff… It was just about prioritising myself rather than just falling into the pit of despair and helplessness.”
These subjective experiences of improved mental well-being were supported by quantitative measurements. Depression (B = -6.5 [-9.7—−3.2], ES = 0.6 [0.3–0.9], p < 0.001), anxiety (B = -5.1 [-7.8—−2.5], ES = 0.6 [0.2–0.8], p = 0.001), and stress (B = -6.5 [-9.5—−3.6], ES = 0.7 [0.3–1], p < 0.001) all declined with moderate effect sizes following the strength program (Figure 3A-C). These measurable reductions in psychological distress indicators align with participants’ narratives about feeling calmer, more resilient, and better equipped to handle daily challenges after participating in the program.
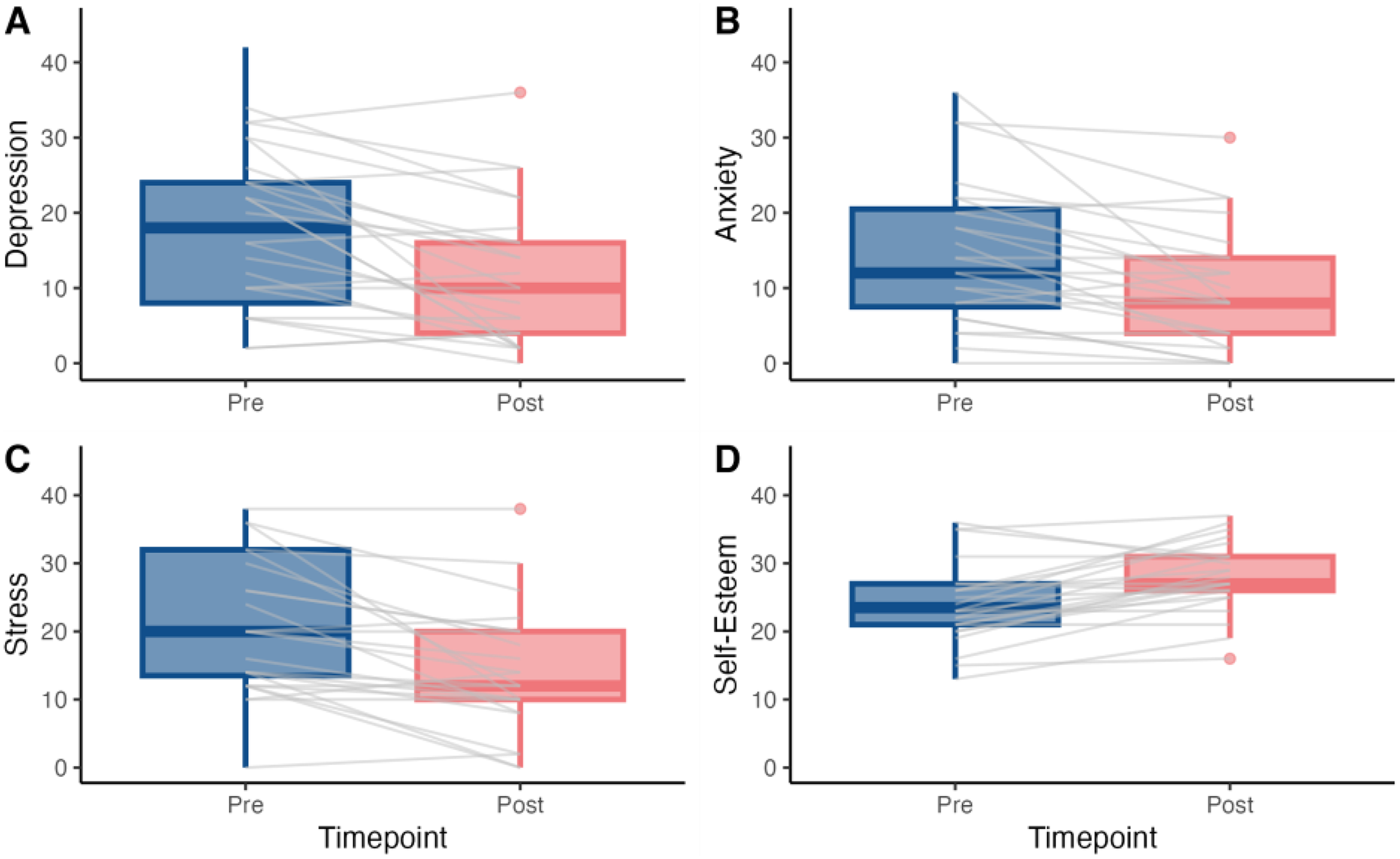
The effect of the program on mental health scores. Grey lines show the effects for individual participants.
Social Connection and Community
The program created a unique environment that facilitated meaningful social connections among participants, directly addressing the isolation often experienced by IPV survivors. Through its structured group format and strength-focused approach, the program fostered authentic relationships and community support.
The shared experience of building physical strength created natural opportunities for connection without the pressure of traditional support groups. As Hedy explained: But it's like you put us in a situation, we're doing challenging things, we're feeling powerful, we start to open up. So, it was this amazing bonus track that I don't think if you'd said to me, hey, we're doing a therapy program… I would've been hard no.
Group training sessions facilitated mutual support and celebration of achievements. Angela shared: “Really good support. And like I said, encouragement and everyone just supports each other…I was really blown away when I did my chest press and on the third go, I got to the 40 kilos and everyone's clapping and cheering.”
Program Implementation Elements
Participants attributed their positive experience in the program to the consideration of the unique needs of IPV survivors. Key components included trauma-informed delivery, skilled trainers, structured progress tracking, and free access.
The trauma-informed approach was centred on participant choice and control, creating psychological safety. As Joan explained: “I feared a little bit that it might be a place where people were going to go and tell their story…yet I felt there, there was a great freedom for those who wanted to, to do so, but there was no pressure.”
Trainer expertise emerged as crucial to program success. The trainers balanced encouragement with sensitivity to trauma. Hedy highlighted this approach: “They were both just really gentle. They never got aggressive… I really liked that they would encourage us to lift harder. I would think my limit is this… And the trainers would come over and be like, yeah, no, and make you work harder. So, they're seeing something in you that you're not seeing in yourself.”
The program's structured progress tracking provided tangible evidence of achievement, creating motivation and self-efficacy. As Taylor described: ”
You kind of go right, and you record it. So, you've got proof that yeah, you've been lifting more than when we started…it wasn't competing with other people or anything, it was just my own progression.”
Discussion
This mixed-methods study demonstrates that maximal strength training provides a novel intervention for IPV survivors’ recovery, addressing critical gaps in current support approaches. The program's effectiveness was evidenced through significant improvements across multiple domains: reduced depression, anxiety, and stress; increased self-esteem and body appreciation; and enhanced social connections. While existing DV recovery programs primarily focus on psychological and social support (Trabold et al., 2020), our findings reveal how structured physical achievement through strength training can offer additional complementary benefits to recovery from IPV.
A key finding was how maximal strength training's focus on developing physical capabilities created a powerful pathway for empowerment. This embodied approach to recovery is particularly significant as IPV systematically erodes survivors’ sense of physical and psychological power through patterns of intimidation and control (Matheson et al., 2015; Williamson, 2010). Our results demonstrate how strength training directly counters this erosion by engaging survivors in an activity that builds both physical and psychological strength. This finding aligns with research showing that women's participation in traditionally masculine activities, like strength training, can be particularly empowering as it challenges societal expectations (Kelly et al., 2023; Walters & Hefferon, 2020). This is further supported by Streetman et al.'s (2023) mixed methods study, which identified resistance training as the most empowering form of physical activity for women.
Beyond physical capabilities, our findings revealed how strength training provided a unique approach to rebuilding self-worth through progressive achievement. Participants described how objective measures of improvement (i.e., adding more weight to the bar) and documenting strength gains offered concrete evidence of their capability. Participants’ subjective experience of increased strength coincided with objective IMTP improvements indicating that the program enhanced both participants perceived sense of strength and their actual physical capability. This directly countered the erosive effects IPV has on survivors’ sense of identity and self-worth (Matheson et al., 2015; Smith-Marek et al., 2018), particularly its impacts on body image and self-objectification (Davidson & Gervais, 2015; Weaver et al., 2020). The effectiveness of this approach was evidenced by significant improvements in quantitative measures of self-esteem, body appreciation, and functionality appreciation. Qualitative data revealed how participants developed more positive relationships with their bodies by focusing on physical capabilities rather than appearance, with these benefits occurring independently of any changes in body composition.
These improvements extended beyond the gym environment into participants’ daily lives, as they applied their newfound physical confidence to various challenges, from parenting to court appearances. This transfer of strength-based confidence aligns with Nowakowski-Sims et al.'s (2023) findings that weightlifting participants reported improved confidence and self-efficacy carrying over into other aspects of their lives, demonstrating a practical mechanism through which strength training supports IPV recovery.
Intimate partner violence has well-documented impacts on psychological well-being, with survivors experiencing elevated rates of depression, anxiety, and post-traumatic stress (Bacchus et al., 2018; White et al., 2024). Our findings revealed several key benefits to mental health recovery. While research has established exercise's general benefits for anxiety, PTSD, and overall well-being (Kvam et al., 2016; Rosenbaum et al., 2015), strength training appeared to offer distinctive contributions through progressive physical achievement and structured routine. Participants reported that focusing on building physical strength directly enhanced their emotional resilience. At the same time, the regular training schedule provided an anchor point during challenges such as court appearances and single parenting. This structured support addresses a critical need, as maintaining routine is particularly valuable for managing depression and anxiety symptoms during trauma recovery (Goodman et al., 2017; Liang et al., 2025).
Physical activities that require focused attention on body movements and sensations, known as embodying activities, can be particularly beneficial for trauma recovery (Massey & Williams, 2020). Embodiment refers to experiencing the world through one's body, where according to Piran's (2017) theory, individuals connect with bodily sensations, develop agency, and resist self-objectification. For survivors, body-based interventions that direct attention to interoceptive and proprioceptive experiences can facilitate reconnection with the body to support trauma recovery (Kuhfuß et al., 2021). Maximal strength training exemplifies this type of activity, demanding focus and connection to body movements during each lift (Kelly et al., 2023). Participants reported immediate relief from intrusive thoughts and anxiety during training sessions, with these benefits extending into improved emotional regulation in daily life. The program's effectiveness in symptom management aligns with evidence that grounding attention in physical sensations can reduce rumination and help manage trauma-related symptoms (Leigh & Bailey, 2013; Massey & Williams, 2020).
The program's contribution to social recovery emerged as a key finding alongside its mental health benefits. Research demonstrates that strong social networks enhance psychological well-being and reduce depression among survivors of IPV (Beeble et al., 2009; Tan et al., 1995). This is particularly significant as IPV often involves social isolation as a control tactic. Our findings revealed that group-based maximal strength training provided a pathway for rebuilding social connections through shared physical achievement rather than shared trauma narratives. While social connection could develop in various group activities, participants specifically noted how the tangible nature of strength progression created meaningful bonds and sustained engagement. This suggests that the concrete, visible achievements unique to maximal strength training may offer distinctive social bonding opportunities.
Unlike traditional support groups that focus on processing trauma experiences (Osborn et al., 2024), the program created opportunities for authentic connection without pressure for disclosure. The structure of group training sessions facilitated natural social connections through regular contact with others who shared similar experiences, while the focus on physical achievements provided natural opportunities for interaction and mutual encouragement. This approach aligns with Nowakowski-Sims et al.'s (2023) findings that gym communities can provide critical social support for trauma survivors by creating spaces where connection develops naturally through shared activity.
Implementing maximal strength training programs for IPV survivors requires careful consideration of specific program elements to maximise participant engagement and outcomes. Our study revealed several critical factors that influenced program success, all grounded in trauma-informed principles of safety, choice, and accessibility (Darroch et al., 2024). Key facilitators included creating physically and psychologically safe training environments, providing participants control over exercise intensity and progression, ensuring appropriately trained staff who could balance technical instruction with participant-led progression, and free access to the program.
A key finding was the importance of establishing safe training environments. Female-only training spaces were essential for participants to feel secure and fully engage in the program. This aligns with Darroch et al.'s (2024) findings that women strongly preferred female-only training times and locations in trauma and violence-informed physical activity programs. Beyond the female-only space, safety was further improved through trauma-informed training approaches. The program environment avoided potentially re-traumatising practices, such as forceful commands or unexpected physical contact, which are common in traditional gym settings (Pebole et al., 2021). Instead, participants were given choice and control over their exercise selection and intensity, supporting trauma recovery by restoring autonomy often compromised through IPV. This participant-led approach contrasts with traditional gym environments, where instructors frequently use authoritative coaching styles and hands-on corrections that may be inappropriate for trauma survivors (Pebole et al., 2021). These findings extend previous work establishing safety as a prerequisite for exercise intervention efficacy with trauma-affected populations (Darroch et al., 2024), and demonstrate specific ways that strength training programs can be adapted to support survivor engagement.
A critical finding was the importance of offering the strength training program at no cost to participants. Financial barriers prevent access to exercise facilities and programs, particularly for survivors of IPV who often face economic abuse and financial instability (Johnson et al., 2022). Economic abuse, which includes behaviours that control a survivor's ability to acquire, use, and maintain economic resources, affects approximately 76–99% of service-seeking survivors (Adams et al., 2008). These controlling tactics can result in credit damage, financial dependency, and limited economic opportunities that may persist after leaving abusive relationships (Johnson et al., 2022). Our qualitative data revealed that even seemingly modest costs, such as parking fees, could make participation impossible, as participants often had to prioritise basic needs such as housing and groceries. This finding underscores how financial accessibility must be considered a core component of program design rather than an optional feature when developing exercise interventions for IPV survivors. The value of addressing these implementation barriers was evidenced by many participants’ continued engagement with the program after the formal intervention period, suggesting that when accessibility needs are met, strength training can become a sustainable recovery tool.
Limitations
Several limitations should be considered when interpreting these findings. While our sample included participants across a wide age range and diverse backgrounds, the majority were white and well-educated, potentially limiting generalisability to other populations of IPV survivors. This lack of racial and socioeconomic diversity could impact generalisability. Firstly, survivors with low socioeconomic status often face greater financial barriers to exercise programs and may harbour systemic distrust of institutional research or gyms, potentially affecting program uptake and outcomes. While our program was free to address some cost concerns, other access barriers, such as transportation and childcare, remained. Secondly, different racial and ethnic groups may have unique cultural relationships with the body, which could influence responses to strength-training interventions. For example, cultural ideals of femininity and the appropriateness of strength training for women vary across communities and may shape how survivors engage and benefit from these programs. The 10-week program duration was sufficient to demonstrate a significant impact. However, we did not include follow-up measurements to assess the longevity of the psychological and physical benefits after the program. Future research should examine program effectiveness across more diverse populations and include longitudinal follow-up to assess sustained impacts. Additionally, research exploring how strength training programs could be integrated into existing IPV services would be valuable for understanding scalability and implementation in different contexts.
Practical Implications
Our findings highlight several key elements for successfully implementing maximal strength training programs for IPV survivors. Results showed that rebuilding personal agency occurred through progressive physical achievement in female-only supportive environments, indicating programs must prioritise participant autonomy while providing appropriate technical guidance. Successful implementation requires trainers with technical expertise in strength training and an understanding of trauma-informed practices, who can balance proper instruction with participant-led progression and training environments that avoid potentially triggering practices common in traditional gym settings.
The importance of social connection through shared achievement rather than trauma narratives suggests organising training in small groups where social interaction develops naturally. Crucially, our research revealed that practical barriers, particularly cost, can prevent program access. Participants’ experiences highlight how even modest expenses could make participation impossible when managing post-separation financial challenges.
Beyond the mental health and well-being benefits observed in this study, strength training also has the potential to address the physical health comorbidities commonly experienced by IPV survivors. Research indicates that survivors face increased risk of chronic pain, cardiovascular disease, and metabolic conditions (Stubbs & Szoeke, 2022). Future research should examine how strength training programs can simultaneously support both psychological and physical health recovery in this population.
Conclusion
This mixed-methods evaluation demonstrates how maximal strength training can provide a unique and powerful pathway to support IPV survivors’ recovery through multiple interconnected mechanisms. By creating opportunities for rebuilding physical and psychological strength, the program directly addressed the erosion of personal power that characterises IPV, while progressive achievement provided tangible evidence of capability that enhanced self-worth. The structured nature of strength training, combined with its focus on physical achievement rather than trauma narratives, facilitated meaningful social connections while supporting psychological recovery. These findings suggest that when implemented with appropriate trauma-informed considerations and barriers to access removed, strength training programs could be a valuable addition to existing IPV services, offering survivors a distinct pathway for rebuilding agency, confidence, and connection through embodied achievement.
Footnotes
Ethical Considerations
This study was approved by the Ethics Committee of the University of Canberra (HREC 4796) on 17 December 2020. All participants provided written informed consent prior to enrolment in the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Australian Capital Territory (ACT) Government Mental Health and Wellbeing Innovation Grants Program, which funded the implementation of the strength training program evaluated in this study. No external funding was received for the research and evaluation activities.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.