
Abstract
Contraceptive interference alters contraceptive use, impacting not only sexual and reproductive health but also intimacy and well-being, particularly for emerging adults. Using a feminist and emotion work approach, this study analyzes semi-structured interviews with 17 women, trans and non-binary people (ages 17–23). It identifies four targeted contraceptive methods and highlights how partner-imposed constraints led to unprotected sex, fear of pregnancy or STIs, and diminished contraceptive autonomy. While some participants developed mistrust toward cis men, others reclaimed agency post-relationship. The study underscores the need for greater attention to contraceptive interference in sex education and healthcare to address its broader relational and emotional consequences.
Keywords
Introduction
Contraceptive interference, which involves disregarding a partner's contraceptive choices, remains an underexplored phenomenon in the literature. However, in a sample of 213 college women, 21.1% reported experiencing at least one instance of contraceptive interference perpetrated by a male partner (Katz and LaRose, 2019). By definition, contraceptive interference encompasses any behavior that alters or prevents the proper and desired use of contraceptive methods, such as birth control pills, intrauterine devices (IUDs), condoms, contraceptive implants, or any other methods intended to provide control over one's sexual and reproductive health (Featherstone et al., 2024).
Contraceptive interference shares certain similarities with a more extensively documented concept: reproductive coercion. However, reproductive coercion focuses on behaviors that interfere with the reproductive trajectory of a person who can become pregnant, with the intent of causing a pregnancy or controlling its outcome, either by forcing its continuation or termination (Miller et al., 2010; Moulton et al., 2021). One set of behaviors within reproductive coercion, birth control sabotage, may resemble the behaviors identified as contraceptive interference. Unlike birth control sabotage, contraceptive interference does not involve an explicit intent to control the reproductive sphere (Katz & LaRose, 2019). This concept encompasses other forms of intent, such as seeking increased sexual pleasure without a condom or asserting dominance by controlling the parameters of sexual intercourse (Ayoola et al., 2007; Davis & Logan-Greene, 2012; Grace et al., 2024; Latimer et al., 2018). Because of this conceptual overlap, the exploration of behaviors that constitute contraceptive interference remain partial.
Documented forms of contraceptive interference primarily involve behaviors that disrupt condom use, such as non-consensual condom removal (Boadle et al., 2021; Bonar et al., 2021; Davis et al., 2023) and resistance to condom use (Chen, Hammett et al., 2024; Davis et al., 2023; Wegner et al., 2017). Some authors have distinguished between behaviors that are inherently coercive and aggressive (e.g., non-consensual condom removal, threatening to harm a partner who insists on condom use) and those that are more subtle or manipulative (e.g., complaining that condoms are uncomfortable) (Davis et al., 2019). The coercive or manipulative nature of these behaviors can influence the severity of consequences experienced. Drawing from a scoping review of 37 studies, Chen and colleagues (2025) report that individuals who experience coercive condom use resistance describe a range of mental health impacts, including feeling disrespected and experiencing anxiety and depressive symptoms. They also report reduced confidence in their ability to assert themselves regarding safer sexual practices. Similarly, a scoping review of 27 studies on non-consensual condom removal identified negative sexual self-perceptions among those affected (Davis et al., 2023). Emotional impacts, such as stress, anxiety, shame, and a sense of loss of control, have also been reported among adult populations, along with apprehension about engaging with future intimate partners (Lévesque et al., 2020). Negative impacts on sexual and reproductive health are also documented, including the risks of unintended pregnancies and contracting sexually transmitted infections (STIs) (Katz & LaRose, 2019; Lévesque & Rousseau, 2021).
Contraceptive interference can also be linked to instances of sexual violence, particularly in cases of non-consensual condom removal (Bonar et al., 2019). Research on sexual violence perpetrated by intimate partners highlights various consequences for mental health (e.g., post-traumatic stress, depression), relational health (e.g., attachment difficulties, reduced relationship satisfaction), and sexual health (e.g., sexual dysfunction, decreased sexual satisfaction) (Bagwell-Gray, 2019; Hellemans et al., 2015).
Although the literature documents a range of consequences across mental health, sexual and reproductive health, and sexual well-being, these findings focus almost exclusively on behaviors that interfere with condom use. However, contraceptive interference can target a variety of contraceptive and prophylactic methods. It is relevant to examine the full scope of consequences by considering the range of contraceptive and prophylactic methods that may be targeted, including those less dependent on a partner's willingness to use them, such as IUDs and oral contraceptives.
Moreover, the available data generally concern adult populations, which limits our understanding of these situations when they are experienced by emerging adults. Emerging adulthood represent pivotal developmental periods during which individuals experience many “firsts,” establish relational boundaries, and negotiate their needs within intimate relationships (Øverlien et al., 2020). Understanding contraceptive interference in this context is crucial, as these early experiences can significantly shape future perceptions of intimacy, trust, and sexual well-being. This study therefore aims to document the various forms of contraceptive interference and explore how these behaviors affect emerging adults’ health, intimacy, and sexuality.
Based on a qualitative study with young people who experienced contraceptive interference, this study is guided by a feminist lens that recognize the gendered power imbalances in intimate relationships, alongside the concept of emotion work, which sheds light on the emotional management strategies used by young people in these contexts. Specifically, this article aims to 1) describe the reported forms of contraceptive interference, 2) document the impacts of contraceptive interference, both during and after the intimate relationship, regarding sexuality, intimacy, and health and 3) explore how emerging adults engage in emotion work in contraceptive interference contexts characterized by gendered power inequities.
Gender Power Imbalances in Emerging Adults’ Intimate Relationships
Using a feminist perspective, gendered power dynamics reflect norms that reinforce the idea of male superiority over other genders to exert control within an intimate relationship (Exner-Cortens et al., 2023). This dynamic diminishes, and in some cases eliminates, the other person's sexual agency and power in the relationship, particularly regarding contraceptive decisions (Katz and LaRose, 2019). Contraceptive interference is also associated with intimate partner violence (IPV), with established links to physical, psychological, and sexual violence (Katz et Sutherland, 2020). Some studies indicate an association between IPV and reduced contraceptive use resulting from barriers imposed by intimate partners (Decker et al., 2021; Maxwell et al., 2015). In a study conducted by Katz and Sutherland (2020) involving 146 women aged 18 to 22, participants who reported experiencing contraceptive interference also reported having been subjected to sexual violence by the same intimate partner. This suggests the importance of examining whether other forms of violence (psychological, sexual, physical, etc.) are also present, and of exploring how gendered power dynamics may operate within intimate relationships that involve contraceptive interference. Scientific literature suggests that one indicator of power inequality lies in relationship management, particularly through emotion work (Fahs et Swank, 2016; Kruse et al., 2023).
Emotion Work
The concept of emotion work, as developed by Hochschild (2003), is applied to better understand the relational context in which contraceptive interference experienced by young people occurs, as well as what constitutes or sustains it. This emotional management operates in both public and private spheres. In the private sphere, emotion work involves maintaining or preserving meaningful relationships and ensuring the well-being of others. Emotion work is cognitive when it pertains to thoughts, bodily when it involves physical engagement (e.g., breathing), and expressive when emotions are outwardly displayed (e.g., crying, laughing). It becomes active when individuals strive to regulate their emotions, either by forcing themselves to feel other emotions (evocation), suppressing emotions (e.g., “I tried to…” or “I forced myself to…”), or fully experiencing them (e.g., “I eventually cried”) (Hochschild, 2003). Emotion work involves emotionally adjusting to the other person, often at the expense of one's own boundaries. This may require forcing oneself to think certain things (e.g., “I’m sure he will be kind again, like before” or “I can change him”), or adjusting emotional reactions by downplaying the hurt experienced, often to preserve the relationship. Emotion work is significant in the context of gender-based violence because it helps explain how victims adapt emotionally to harmful situations and why they may remain in relationships where violence or coercion occurs. This is also situated within gendered socialization processes, where women are socialized to reproduce traditional gender roles and to engage in care-oriented behaviors aimed at maintaining and nurturing relationships (Davies, 2023).
This concept has been applied in other studies on gender-based violence (Fahs et Swank, 2016; Kruse et al., 2023), as emotional regulation and adjustment are particularly significant in these contexts (Tarzia, 2021). Using the concept of emotion work in this study offers insights into how young people navigate and engage in this process in the context of contraceptive interference within intimate relationships.
Methodology
Procedure
The project received ethical approval from the first author's university [University of Ottawa, Office of Research Ethics and Integrity; H-09-22-8218]. As this study is part of the first author's doctoral thesis, data generation and analysis were conducted by her. The co-authors, who are the thesis supervisors, provided theoretical and empirical guidance throughout these stages.
Participants were recruited through social media, community organizations providing specialized support services for domestic or sexual violence, and post-secondary educational institutions. The call for participation was shared via a poster outlining the following inclusion criteria: 1) being between 16 and 25 years old, 2) being or having been in an intimate relationship with the same person for three months or more, and 3) having experienced difficulties related to contraception use with that person. Since the term “contraceptive interference” remains unfamiliar, we opted for an alternative wording aimed at capturing these realities. The recruitment poster therefore presented the following question: “With this person, was it or has it been difficult to use your preferred method of contraception or to protect yourself against an unintended pregnancy?”.
During the recruitment period, 77 individuals expressed interest in participating in the study by email. A pre-interview was conducted to validate the inclusion criteria. Interested individuals were invited to answer a screening question designed to assess eligibility: “To ensure that you meet the project's inclusion criteria, could you tell me your age and briefly describe the situation you experienced in which it was difficult or impossible to use contraception with an intimate partner?” Responses generally consisted of short narratives of two to four sentences and allowed the research team to determine whether the situation referred to contraceptive interference or to other sexual health–related issues. More specifically, 31 individuals did not meet the criteria (e.g., situations related to side effects caused by contraception, difficulties accessing contraception, or referring to someone else's experience rather than their own). Among those who met the inclusion criteria, several did not respond to follow-up emails, even after reminders (n = 24). Five individuals completed the sociodemographic questionnaire prior to the individual interview but did not follow through with the interview itself. In total, 17 individuals participated in individual interviews. Almost all participants (16 out of 17) were recruited through post-secondary institutions in Montréal (Canada), whereas only one participant was recruited through an organization providing sexual and reproductive health services. Participants were interviewed between February and May 2023.
Data Generation
To generate rich data on participants’ contraceptive interference experiences, we chose to conduct individual interviews using a semi-structured interview guide. A short sociodemographic questionnaire was shared and completed online prior to the individual interview. The information and consent form was reviewed in full with participants and was required to be signed before beginning the individual interview.
To minimize the potential effects of hierarchical dynamics between the researcher conducting the individual interviews [CR] and the participants, continuous reflexivity was maintained throughout the study. This reflexivity involved taking notes on specific reflections and discussing them with the co-authors. For example, one reflection concerned self-presentation during interviews with participants. Introducing myself as a doctoral student and a sexologist during the initial interviews quickly revealed an asymmetry in positions. Many asked questions about my professional background and on the university program in sexology (contingency, student acceptance rate, etc.). I considered whether simplifying my introduction by stating only that I was conducting a study, without mentioning my professional titles (which were already listed in the consent form), might reduce this effect. I tested this approach in subsequent interviews and observed that participants were more inclined to direct their questions toward the study rather than the university program. I maintained this approach for the remaining interviews. Throughout all interviews, I specified to the participants that there was no “right way” to speak during the interviews and that they could communicate in whatever way felt most comfortable to them. I also adopted a non-judgmental and supportive attitude, and I paid particular attention to my communication style (e.g., avoiding technical terms related to the research process or the study's subject matter).
The interview guide began with an icebreaker question about the participant's motivation to participate in the project and a brief self-introduction. Following this, contraceptive interference situations were explored using an open-ended, non-directive question (e.g., “You mentioned an experience with an intimate partner via email. Could you tell me more about this situation?”). Questions about the impacts of contraceptive interference across different areas of life were then asked (e.g., “What impacts did you experience following this situation?”). Follow-up questions were included to delve into issues related to sexual and reproductive health that participants might have faced (e.g., contracting or testing for STIs, unplanned pregnancy, use of emergency oral contraception). Additional questions explored the impacts on mental health, intimate relationships, or sexuality (e.g., “In what way has this situation influenced your perception of intimate relationships?”). At the end of the interview, participants were systematically provided with a list of support resources, along with an explanation of the services offered. Additional resources could be shared depending on the participant's specific needs.
The location of the interview was chosen by the participant: 13 participants opted to participate online via Zoom, while 4 chose to participate in person at their post-secondary educational institution. All interviews were audio-recorded with the participants’ consent. Each participant received financial compensation of CAD$30. The average duration of the interviews was 53 minutes. All interviews were transcribed verbatim. After each interview, the interviewer wrote reflexive notes reflecting on the interview's content, its flow (e.g., noting interruptions, pacing, and overall impression of the interview's fluidity), the interview guide (e.g., clarity or lack thereof in the questions and necessary adjustments), the impact of the interview on the participant (e.g., using an open-ended question after the interview to gauge how the participant felt after sharing their story), and conceptual or empirical reflections related to the study's subject.
Data Analysis
The verbatim transcripts were imported into the qualitative analysis software NVivo 14 (QSR International Pty Ltd.). To document the forms of contraceptive interference, a qualitative descriptive analysis was conducted. Given the limited literature on contraceptive interference, it was deemed important, as a first step, to report its forms enacted by intimate partners in descriptive categories (Ayton, 2024). The contraceptive interference behaviors identified were categorized according to the contraceptive or prophylactic methods targeted. The intention was to classify the behaviors that corresponded to the definition of contraceptive interference adopted in this study, specifically the one proposed by Featherstone and colleagues (2024). After categorizing the reported behaviors based on the contraceptive or prophylactic methods they targeted, each behavior was analyzed to specify the ways in which it was carried out by the partner (e.g., through manipulation, deceit, or force).
For the analysis of the impacts of contraceptive interference and to ensure methodological coherence, the recent Reflexive Thematic Analysis Reporting Guidelines (RTARG) developed by Braun and Clarke (2024) were followed as closely as possible. After multiple readings of the transcripts to fully understand the participants’ individual experiences, initial inductive codes were created using the participants’ own words. Themes were then developed to organize the content and identify patterns of shared meaning in a structured and meaningful way. The themes were designed to be coherent with one another and mutually exclusive. This step was also supported by reflexive notes taken after each interview, which guided the analytical approach adopted in this article. Based on the themes, conceptual categories were created, informed by the theoretical frameworks and the reflexive notes. Citations were selected for each of the proposed conceptual categories. The reflexive exercise allowed the authors to renegotiate the proposed conceptual categories to ensure they captured the essence of the participants’ experiences. The chosen theoretical frameworks, specifically emotion work and gender-based power dynamics, were useful for identifying patterns of control that enhanced partners’ relational power, particularly around contraceptive decision-making, and in clarifying how these dynamics influenced the emotion work undertaken by participants. Accordingly, particular attention was given to the language used by participants that reflected their constrained contraceptive autonomy, which informed the development of the conceptual categories. The lens of emotion work allowed us to highlight how participants attempted to interpret or respond to situations of contraceptive interference in order to mitigate, or prevent future incidents, both during data collection and throughout the analytic process.
Results
Sociodemographic and Relational Characteristics of Participants
The participants (n = 17) were aged between 17 and 23 at the time of the individual interview. The sample consisted of fifteen cis women, one non-binary person, and one trans man. The majority of the sample (n = 11) identified as bisexual, pansexual, or questioning. Eleven participants were born in Canada, while six were born in Western Europe, Central Africa, North America (excluding Canada), or South America. Slightly more than half of the sample (n = 11) lived with their parents. Six participants reported experiencing poverty or having insufficient income to meet their basic needs. Two participants identified as religious and practicing, while three described having a spiritual practice or religious affiliation without being practicing.
A total of 21 intimate relationships marked by contraceptive interference were reported by the 17 participants. Three participants reported experiencing contraceptive interference in more than one intimate relationship. Each intimate relationship is distinguished in the identifier (e.g., the first relationship is identified as “R1” in the participant's identifier, such as P8-R1). Since our focus is on experiences of intimate relationships involving contraceptive interference, each of these relationships is treated as a separate unit in the sample. Consequently, the reported n refers to the number of intimate relationships.
Regarding relational characteristics, all perpetrators of contraceptive interference were cisgender men, except for one relationship in which the perpetrator was a non-binary person. At the time of the individual interview, only one participant was still in a relationship with the perpetrator of contraceptive interference. Ten participants had a new partner and were not experiencing contraceptive interference in this intimate relationship.
Overview of Contraceptive Interference Forms
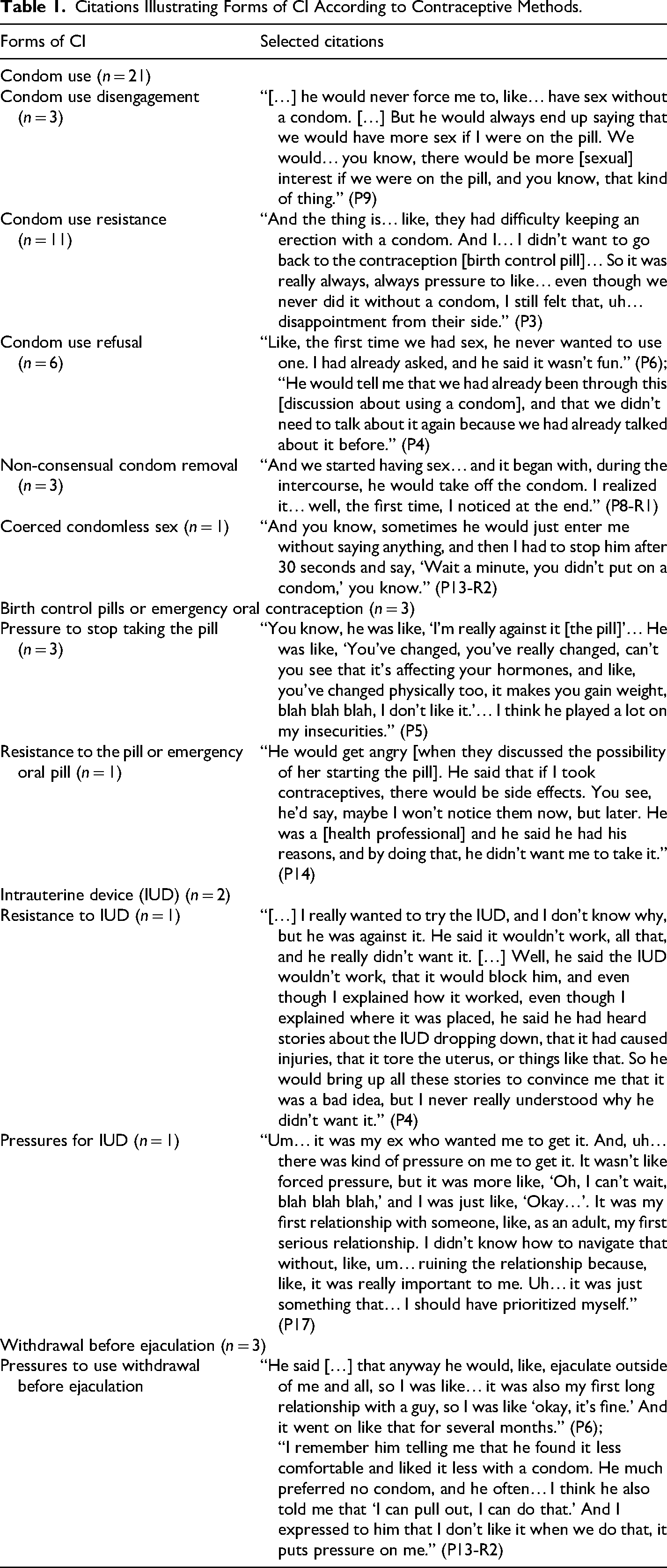
This section provides a descriptive analysis of the forms of contraceptive interference based on the different contraceptive methods targeted. Table 1 outlines the documented manifestations of contraceptive interference, illustrated by citations. Contraceptive interference impacted the use of four contraceptive methods: 1) condoms, 2) birth control pills or emergency oral contraception, 3) intrauterine devices (IUDs), and 4) withdrawal before ejaculation.
Citations Illustrating Forms of CI According to Contraceptive Methods.
Citations Illustrating Forms of CI According to Contraceptive Methods.
All participants experienced at least one instance of contraceptive interference related to condom use across all reported intimate relationships (n = 21). Five manifestations were documented. First, disengagement regarding condom use (n = 3) refers to a partner's lack of initiative in using a condom, despite a prior agreement to have protected sex. In these scenarios, the partner eventually uses a condom when requested by their partner. The second manifestation involves resistance to condom use (n = 11). In these situations, the partner explicitly resists using a condom and attempts to persuade the other not to use one. This resistance may be accompanied by reproach or behavior aimed at inducing guilt in the other person. In these cases, the sexual encounters remained protected by a condom despite the resistance. The third manifestation refers to the outright refusal to wear a condom and refusal to discuss it (n = 6). In these cases, sexual encounters were not protected by a condom. The fourth manifestation is the non-consensual removal of the condom (n = 3), where the partner removes the condom during sexual activity without the other partner's knowledge. Finally, coerced condomless sex (n = 1) refers to situations where sex with a condom was agreed upon, but the partner engaged in penetration without using a condom and without obtaining prior consent for unprotected sex. In this case, the participant had clearly expressed a desire to use a condom for protection, and one had been used in previous sexual encounters.
Birth Control Pills and Emergency Oral Contraception
Contraceptive interference can also target the use of birth control pills or emergency oral contraception. Two participants reported experiencing pressure from their intimate partners to stop using birth control pills. This pressure took the form of insults targeting their body image (e.g., comments about weight gain) and mental health (e.g., remarks about mood swings). Another participant shared that her partner prevented her from accessing birth control pills or emergency oral contraception, claiming that these methods were harmful to her health.
Intrauterine Device (IUD)
Two participants reported instances of contraceptive interference related to the use of an IUD. In the first scenario, the partner actively resisted the insertion of an IUD, claiming, despite the participant's clarifications, that it could cause injuries (n = 1). In the second scenario, verbal pressure was exerted on the participant to get an IUD so that the partner could stop using condoms, even though the participant did not wish to use this contraceptive method (n = 1).
Withdrawal Before Ejaculation
The final manifestation of contraceptive interference involves pressure to use withdrawal before ejaculation (n = 3) as a contraceptive strategy. These pressures were persistent, and participants ultimately yielded to this practice without giving consent. Although this may reflect a strategy by the partner to avoid using a condom, these situations differ from interference with condom use. In these cases, participants yield to the partner's preference, and no condom is used from the outset. However, when it is time to withdraw, the partner does not do so and ejaculates inside them, violating the agreement.
The Impacts of Contraceptive Interference
This section presents the findings from the reflexive thematic analysis and shows the diverse impacts of contraceptive interference. Four conceptual categories illustrate the participants’ experiences in the context of contraceptive interference, both during their intimate relationship with the perpetrator and after the relationship ended. The first conceptual category highlights how contraceptive interference behaviors by the intimate partner directly limited the contraceptive options available to the participants. The second category explores the impacts of restricted contraceptive autonomy on maintaining their sexual and reproductive health. The third category addresses the relational impacts, including the feeling of constantly needing to adapt to the partner and the apprehension about future intimate relationships due to the risk of experiencing contraceptive interference again. The final category focuses on the participants’ behaviors aimed at reclaiming power over their health, intimacy, and sexuality after ending the relationship marked by contraceptive interference.
Contraceptive Choices Eroded by Partner Constraints
Contraceptive interference behaviors contribute to progressively reducing the contraceptive options available to the participants. All participants reported that their partner opposed the use of condoms in one way or another. This opposition occurred repeatedly, with varying intensity across different intimate relationships. Some participants eventually felt exhausted from repeatedly requesting condom use, as their efforts often had limited or no success: “Yeah, I asked again several times. Then, at some point, I stopped asking because I knew… In the end, I didn’t ask much anymore, and when I realized… I stepped aside.” (P15). In addition to this exhaustion, some participants experienced guilt, as their request to use a condom contradicted the image they wanted to project as a sexual partner. “It's like… you don't dare tell them anymore because you feel like if you say you want to use a condom, you're ending the sexual encounter. You feel like… not that you're ending it, but that you're taking away the pleasure, taking away the excitement.” (P13-R2) “I went to see my doctor because I wanted to start taking the pill to address the discomfort this person—this guy—was experiencing. […] I actually dealt with a lot of side effects. And… like many women, I think.” (P13-R1)
Another participant shared that her partner purchased condoms that were too large, further diminishing their effectiveness, while also resisting their use. To prevent an unintended pregnancy and gain better reproductive control, she decided to start using birth control pills: “And I just wanted to take the pills because I couldn't risk having unprotected sex again and then… getting pregnant.” (P16).
However, the daily adherence required for birth control pills created a mental burden for the participants, leading to its eventual discontinuation. “And I think after… two years of using the pill, I still couldn’t manage it properly. Because the schedule… well, I’m really bad with things that are very… I had to take it at the same time every day. And I just couldn’t be that consistent […] I was putting myself through the side effects for nothing and stressing myself out for nothing.” (P10-R2) “[…] When my periods stopped, I got worried. So, I talked about it, I mentioned it to him, and as soon as he heard that, he jumped on the idea that I didn’t need contraception anymore because, anyway, I wasn’t getting my periods, so it wouldn’t make any difference, it wouldn’t change anything. And that really discouraged me. It made me even less inclined to eat, so that… that was a really bad time. Instead of being there for me, he mostly just talked about that.” (P4)
Contraceptive interference diminishes participants’ ability to exercise their contraceptive autonomy. This is reflected in being forced to use a contraceptive method other than their preferred choice, managing the mental load associated with alternative contraception, and experiencing stress, guilt, and exhaustion when requesting the use of their preferred contraceptive method.
Restricted Contraceptive Autonomy: Impacts on Sexual and Reproductive Health
Contraceptive interference, by restricting contraceptive autonomy, poses a direct threat to sexual and reproductive health. All participants reported impacts related to the fear of pregnancy, which sometimes led to the use of emergency oral contraception, and the fear of contracting an STI, which occasionally resulted in testing and medical treatment.
All participants experienced fear of pregnancy at some point in their intimate relationships: “I’m the kind of person… like… I’m so terrified of getting pregnant. I’m really, really, really scared of that.” (P3); “I don’t know how many times I did this, but I think, once or twice, I took a pregnancy test, just to be sure.” (P2). One participant recalled the anxiety of waiting for her period and the guilt she felt, believing she hadn’t been assertive enough in demanding condom use. Despite her repeated requests for protected sex, her requests were never acknowledged by her partner, who systematically refused to use a condom. This emotional labor, in which she tried to meet the other person's demands by tolerating discomfort (Fahs et Swank, 2016), is also accompanied, afterward, by a negative self-perception as she puts the blame on herself. “Well, it was really stressful, waiting each month for my period to come. It really stressed me out. And also, afterward, I remember, I would often go to the bathroom to cry because I felt really stupid for having let it happen.” (P6)
Eight participants reported fearing they had contracted an STI. Three participants underwent testing due to concerns about potential infection: “I went to get tested really often […] I thought it was STIs.” (P1). One participant received a positive STI diagnosis following testing.
The various obstacles imposed by intimate partners regarding contraceptive use exposed participants to risks of unintended pregnancies and STIs. Participants resorted to emergency oral contraception or STI testing in an effort to maintain control over their sexual and reproductive health.
Navigating Power Imbalances and (Dis)Trust in Intimate Relationships
The restriction of contraceptive autonomy by intimate partners, leading to an increased risk of STIs and unintended pregnancies, left participants feeling powerless in their intimate relationships. They felt that their needs were disregarded and, as a result, that they were not valued by their partner. “Well, I felt really alone and unheard, but mostly like I wasn’t important. Like there were so many other things that mattered way more than me. I really felt like I was his lowest priority. I was still a priority, but really low on the scale, so to speak.” (P4) “I think I felt less respected. Every time, it made me… I felt disappointed, actually, to be seen like that – more as a sexual object than someone with whom the person wanted a good, healthy, and attentive relationship. It was really more… I felt dirty. Like I was just there to physically please them. It seemed like the sexual encounter mattered more than our relationship.” (P10-R1-R2-R3)
Others mentioned that it was their first significant intimate relationship, and as such, their insecurity was also driven by the fear of causing conflict or even a breakup. “Well, I think that since I felt a bit intimidated and it was my first experiences, there was some stress for me. I really didn’t want to get into an argument. I really wanted to avoid conflict or anything like that because, on top of it, I didn’t know anything. So I was really relying on what he said.” (P10-R2)
Some participants also shared the fear they felt in response to their intimate partner's aggression and described trying to behave in ways that would avoid triggering this anger: “It didn’t really affect me to give in [to unprotected sex]. It was more about him and his reactions that affected me. And that's why I sacrificed everything because I was like, ‘I don’t want him to get mad.’” (P5). This participant weighed the implications of giving in to a sexual encounter, considering it less harmful than the risk of enduring her partner's violent reactions. This cost-benefit calculation led her to sacrifice control over her sexual and reproductive health to prevent an escalation of violence.
Eight participants reported yielding to unprotected sexual encounters without consent. This often occurred in contexts where participants felt exhausted by their partner's persistence, leading them to give in to the partner's demands to temporarily end the arguments: “I was super nervous. I was like, ‘Okay, get it over with.’ It's just… that's not how you’re supposed to feel during an intercourse with someone you love.” (P17); “Yeah, because at some point, like… with him, it was more about his pleasure than mine. So I was like, ‘Okay, let's do what you want to do.'” (P16). The partners’ behaviors imposed constraints on sexual and intimate interactions, highlighting the power imbalances within the relationship.
The impacts of contraceptive interference extend beyond the relationship, influencing participants’ perceptions and trust. Ten participants expressed apprehensions toward cisgender men, exhibiting caution in choosing subsequent partners: “After that, I was more ambivalent when meeting guys, more reserved. […] I was on guard and didn’t want anything bad to happen” (P2). Experiencing contraceptive interference led participants to view men as selfish and exploitative: “Unfortunately, as they say, men are like that, huh! If you give, they’ll take” (P7). Reflecting on two past relationships marked by contraceptive interference, one participant shared a diminished trust in men: “I’d say I trust men a lot less now, in general. I can’t believe how sneaky this kind of behavior can be, how discreet it can be” (P13-R1-R2). Another participant highlighted struggles in forming new intimate relationships and rediscovering fulfilling sexuality after the intimate relationship with their ex-partner. “I struggled with being intimate with others because, honestly, [ex-partner's name] traumatized me when it comes to intimate relationships. […] I don’t know if I’ll have sexual relationships again because I just can’t recover from what happened before.” (P11)
Reclaiming Sexuality, Intimacy and Health
While contraceptive interference significantly impacted various aspects of participants’ lives, fifteen individuals reported reclaiming their sexuality, intimacy, and health after the end of the intimate relationship marked by such behaviors. Two participants further explored their sexual orientation, considering intimate partners other than cisgender men. Another participant engaged in new sexual practices, allowing her to experience sexual pleasure with a partner for the first time: “And I was able, for the first time in two years, to regain a sense of pleasure. You know, I had never experienced that before.” (P5).
Some participants reflected on feeling increasingly confident in expressing their desires and setting sexual boundaries, as well as perceiving them as legitimate. This heightened confidence emerges in intimate contexts where they feel safe: “There are things I need to make clear, and I also need to choose sexual partners with whom I feel safe, you know. And it's okay to say no.” (P3). This confidence extends to contraceptive choices, with six participants noting that their current intimate partners acknowledged and respected their needs: “He never made me feel bad about it, never questioned it, and never even asked me to change my contraceptive method for his comfort.” (P13). Exposure to harmonious and nonviolent intimate relationships has helped participants establish new standards for navigating intimacy. This process allows them to recognize the legitimacy of their needs and boundaries as essential for maintaining their sexual and reproductive health (Bagwell-Gray, 2019).
Contraceptive interference behaviors lead participants to adopt a critical perspective on societal narratives regarding the shared responsibility for contraception. One participant observes that the lack of accountability among men regarding contraception – shaped by education, cultural, and social influences – strongly contributes to the occurrence of contraceptive interference situations. This resonates with the gendered nature of contraceptive responsibility, which is particularly disproportionate in heterosexual contexts (Alspaugh et al., 2020; Lévesque et al., 2024). “It annoys me when someone says, ‘these things happen.’ It frustrates me, and I have to say, ‘No, that's not how it's supposed to be.’ […] ‘It's YOUR life, it's YOUR body, but it's also about the safety of the other person you're sleeping with, you know? It's YOUR responsibility to wear one [condom]. You put one on even before knowing if the other person is protecting themselves in another way.'” (P13)
Discussion
This study examined the forms of contraceptive interference reported by young women, trans, and non-binary individuals within the context of an intimate relationship, as well as the consequences they described for their health, sexuality, and intimacy, both during and after the intimate relationship. Additionally, it examined how young people engaged in emotion work within intimate contexts shaped by gendered power imbalances.
The descriptive results illustrate that contraceptive interference targeted four contraceptive and prophylactic methods. All participants reported experiencing contraceptive interference related to condom use. Intimate partners adopt various behaviors to limit or prevent condom use: condom use disengagement, resistance or refusal, non-consensual condom removal, and coerced condomless sex. This is consistent with the literature on strategies for avoiding condom use, which include deception or stealthing (Davis et al., 2023; Gómez-Durán et Martin-Fumadó, 2024), resistance to condom use (Davis et al., 2023) or coerced condomless sex (Chen, Kirwan et al., 2025). The use of birth control pills or emergency contraceptives is also impacted by contraceptive interference, as partners prevent their use. Situations involving resistance to the insertion of IUDs, or conversely, pressure for its installation, are also reported. Contraceptive interference also takes the form of pressure for withdrawal before ejaculation, a fallible contraceptive method that increases participants’ anxiety. This aligns with the birth control sabotage behaviors identified by Moore and colleagues (2010), capturing behaviors aimed at preventing contraceptive use prior to sexual intercourse, such as throwing away birth control pills, destroying emergency contraception, or refusing to contribute to its cost. Behaviors occurring during sexual intercourse were also documented, including removing the vaginal ring or refusing to withdraw before ejaculation. These behaviors were reported in contexts of reproductive coercion, where the intent was to influence the other partner's reproductive trajectory. The qualitative results of the present study reveal similar behaviors, but without a clear intent to cause pregnancy. Further research is needed to better understand the multiple forms of control an intimate partner may exert to limit another person's use of contraception or prophylactic methods.
The interpretative results reveal that contraceptive interference contributes to reducing the contraceptive choices available to emerging adults. Faced with constraints imposed by their partner, some turn to other contraceptive methods that are less suitable for them, while others are subjected to unprotected sexual intercourse. This resonates with a study that shows how power imbalances in contraceptive negotiations are linked to the risk of coercion in both sexual and reproductive spheres (Decker et al., 2021). Moreover, when contraceptive autonomy is restricted by a partner, young people experience fear and anxiety about contracting an STI or becoming pregnant. This fear and anxiety emerge during sexual encounters but persist for several days afterward. As these situations occur repeatedly within the intimate relationship, many participants mention not feeling heard or considered by their partner. They feel they are constantly adjusting to the other's demands. This adjustment requires emotion work, which is even more demanding in a context marked by power imbalances (Tarzia, 2021). This adjustment, implicitly or explicitly prescribed by the partner, comes at the expense of their sexual and reproductive health and well-being (Bagwell-Gray, 2019).
A sense of misunderstanding and confusion persists among young people who struggle to understand why their partner restricts their contraceptive autonomy, even though its practice ensures safe sex for both partners. As illustrated by this quote, “As if it were a punishment for him, rather than protection for both of us” (P10), requests for safe sex are met with indifference at best, and rejected with disdain and anger at worst. As a result, young people engage in emotion work by attempting to understand their partner, forcing themselves to display empathy while suppressing the expression of their own emotions (Hochschild, 2003). This understanding is not mutual, as the partner disregards their expressed needs and boundaries. It eventually gives way to a sense of exhaustion. They try to keep the peace, recognizing that their arguments are futile, and ultimately give up on expecting their partner to respond to their needs.
These experiences, where their sexual consent and well-being were ignored, generate impacts that persist after the end of the intimate relationship. Similar to what is reported in the literature, some individuals report a fear of future intimate relationships, particularly with men, due to the apprehension of experiencing contraceptive interference or IPV again (Lévesque et al., 2020; Rousseau et al., 2025). For others, the end of the intimate relationship marked by contraceptive interference is a moment of exploration and reclamation of their sexuality, intimacy and health. Several participants share that they feel more empowered in expressing their sexual desires, their sexual and intimate boundaries, and their contraceptive preferences. These results echo the protective strategies identified in the scoping review by Chen and colleagues (2025), which describe how individuals who have experienced coerced condomless sex develop coping behaviors. Resistance strategies are reported to protect their sexual health, such as hiding their contraceptives or withholding sex unless condoms were used. This reflects a stronger assertion of sexual agency, which is also evident in the findings of our study and reveals a way of reclaiming power within a context of unequal power dynamics, where the partner shapes and constrains the couple's contraceptive decisions.
This qualitative study makes visible the ways in which these behaviors operate within gendered dynamics that disadvantage women, non-binary, and trans individuals, thereby exposing them to a range of consequences that further deepen gender inequalities. By integrating the lens of emotion work, this study also highlights the subtle but consequential ways in which emerging adults adjust, suppress, or manage their emotions to preserve the relationship, mitigate conflict, or maintain a sense of safety. These emotional strategies illuminate how coercive or manipulative behaviors, such as contraceptive interference, are navigated and identified over time.
Limitations
This study has some limitations that should be taken into consideration. First, the sample consists mainly of cisgender women pursuing post-secondary education. It is possible that the reported situations might differ for individuals who have experienced school dropout, as this social determinant of health, often associated with financial insecurity, may be linked to lower contraceptive use (Black et al., 2019). Additionally, in this study, two participants are trans and non-binary. Their interviews reveal specific forms of violence, particularly regarding the invalidation of gender identity and control over contraception, regardless of hormone use. In this sense, transphobic and heterosexist violences are present ( Zamantakis, 2020) and should be further explored in future studies on contraceptive interference.
The results demonstrate the presence of other IPV behaviors, in addition to contraceptive interference behaviors. The collected data did not allow for an in-depth exploration of these intersections in terms of the reported impacts, primarily due to the sample size. Future research should focus on the intersections between contraceptive interference and IPV, with particular attention to sexual violence, to better understand how these contexts intersect and reinforce each other.
Finally, our reflexivity as a research team undoubtedly played a role in this study. The fact that the interviewer [CR] is cisgender and white may have influenced the comfort level of trans and racialized participants in disclosing certain aspects related to their reality. Not sharing the same positionality can sometimes encourage disclosure or, conversely, discourage it (Dwyer et al., 2022). In all cases, positionality inevitably influences the interactions between the researcher and the participant during the interview (Thorpe et al., 2018; Yip, 2024). The reflective notes collected by the interviewer highlight how this awareness emerged through recognizing the influence of her personal history and her social, cultural, and environmental contexts during interactions with the participants. A respectful and safe interview environment was ensured to provide each participant with the opportunity to share what they were comfortable with. After each interview, a moment was taken to inquire how the interview had gone for the participant and how they were feeling. Some acknowledged that the experiences shared were difficult, and talking about them brought up more challenging emotions, but all emphasized that they were satisfied with having been able to share their experiences. Future research should continue to explore best practices grounded in trauma-informed approaches when working with young people disclosing IPV or sexual violence.
Implications for Practice
The results of this study show that emerging adults consulted healthcare professionals (pharmacists, nurses, doctors) when experiencing contraceptive interference, whether for STI screening, new contraceptive prescriptions, or emergency oral contraception. Training efforts for healthcare providers and professionals should be implemented to raise awareness about this specific form of violence. This would enable them to provide optimal interventions that effectively address the health needs of young people. For example, they could ask sensitive and behavior-specific questions (e.g., “Has anyone made it difficult for you to use the contraception you wanted?”). An inclusive training module addressing the sexual health realities of trans and non-binary individuals should also be offered. Our study shows that contraceptive interference affects these populations as well, who already face heightened risks of discrimination within health care settings (Rosenberg et al., 2021). Such training could also include information on contraceptive options that are available while undergoing hormone therapy, which may be particularly relevant for individuals who wish to rely on a method other than condoms.
Sex education could address the risks of contraceptive interference to sexual, reproductive, and overall well-being. It could also support the development of sexual agency by providing young people with reference points about what is reasonable and respectful to expect or request within an intimate relationship. In doing so, discussions could address emotion work and raise awareness about the moments when individuals adjust or suppress their emotions to preserve or maintain the relationship. Such content may help young people reflect on relational dynamics that compromise their boundaries, well-being, or autonomy (VanderDrift et al., 2013). However, this content should not be limited to a risk-centered approach but should also focus on sexual pleasure and comfort (Byron, 2017). Content focused on deconstructing gender norms and gendered power dynamics could be offered to encourage young people, particularly young men, to adopt a critical reflection on these concepts (Llano-Suárez et al., 2021). Young men must engage in sharing contraceptive responsibility and adopting safe sexual practices. Sex education should enable young people to have greater contraceptive autonomy, contributing to better overall health.
Conclusion
Contraceptive interference poses a direct threat to contraceptive autonomy and can occur within contexts of IPV, including sexual violence. Contraceptive interference exposes emerging adults to risks of STIs and unintended pregnancies, leading to fear and anxiety. These contexts also impact their well-being, their sexual health and their perception of future intimate relationships. The results of this study highlight the importance of further exploring contexts of contraceptive interference among emerging adults, particularly to document the barriers these behaviors pose to overall sexuality, intimacy and health.
Footnotes
Acknowledgements
The authors would like to thank all the participants who took part in this study and generously shared their stories. ChatGPT was used to assist with the linguistic revision of the manuscript.
Ethics Approval
The project received ethical approval from the university where the first author completed her doctoral studies [University of Ottawa, Office of Research Ethics and Integrity; H-09-22-8218].
Funding
The author has a doctoral grant from Fonds de Recherche du Québec – Société et Culture (FRQSC), and from Recherches Appliquées et Interdisciplinaires sur les Violences intimes, familiales et structurelles (RAIV).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article