
Abstract
The longitudinal effects of distinct intimate partner violence (IPV) types on neurocognition among South African women with HIV are unknown. Mixed linear models determined between-group (IPV exposed vs IPV unexposed) differences in domain-specific and global deficit scores (GDS) and associations with IPV types. There were no between-group differences in cognition (GDS and domain-specific) at baseline or 1-year follow-up. There were significant time*IPV type interaction effects (physical assault, sexual coercion, injury) in attention/working memory. IPV exposure was associated with a lack of cognitive improvement. IPV-screening among women with HIV is important for improved support and targeted interventions.
Introduction
In South Africa, the HIV epidemic disproportionately affects women, particularly women of a younger age (Human Sciences Research Council, 2023). Women are also disproportionately affected by an equally devastating and under-recognized epidemic of violence. Intimate partner violence (IPV), defined as any physical or sexual violence, threats of violence, and emotional or psychological abuse by an intimate partner (World Health Organization, 2021), is a global public health concern (Sardinha et al., 2022). South Africa has the highest rate of IPV among women (Gass et al., 2011), with an estimated lifetime prevalence of 24% (World Health Organization, 2019) and high rates of associated femicide (O’Regan, 2022). IPV significantly contributes to the disease burden as it is associated with various physical and mental health problems (Hansrod et al., 2015; Sardinha et al., 2022; World Health Organization, 2013), including neurocognitive impairments (Esopenko et al., 2021). For example, Daugherty et al. (2019) found significant differences in attention and executive function in women with IPV exposure compared to unexposed women, with approximately 25% of women who experienced IPV experiencing mild neurocognitive impairment and 5% severe impairment. Similarly, Williams et al. (2017) in their longitudinal study reported decreased performance on a measure of attention in female IPV victims over time. Additionally, IPV is associated with an increased risk of sexually transmitted infections (Sullivan, 2019). There is a well-documented bidirectional relationship between HIV and IPV (Sullivan, 2019; World Health Organization, 2013). Women with HIV are more likely to experience IPV than their uninfected counterparts (Iliyasu et al., 2011), with prevalence rates of 56.3% (South Africa: Matseke et al., 2016) and 64.2% (Ethiopia Alemie et al., 2023) reported among women with HIV. Disclosure of a positive HIV status can lead to either an extension of former violence or new conflict specifically associated with the disclosure (Colombini et al., 2016). Moreover, women who are in violent and unstable relationships are more likely to become infected with HIV due to decreased capacity to make decisions about their own reproductive and sexual lives (Benoit et al., 2015), reduced condom use (Gibbs et al., 2019), and coercion or forced sexual initiation (Stockman et al., 2013). Similar to IPV, HIV infection can negatively affect neurocognitive performance (Daneman & Prat, 2015). HIV-associated neurocognitive disorders (HAND) are prevalent in South African people with HIV (Joska et al., 2010; Robbins et al., 2011) and typically affect executive functions (Heaton et al., 2011), attention (Maki et al., 2015; Su et al., 2015), concentration and memory (Smail & Brew, 2018), information processing and psychomotor speed (Kanmogne et al., 2020), language (Hoare et al., 2016), verbal learning (Maki et al., 2015), and sensory perception. The syndemic nature (Closson et al., 2016; Tsai, 2018) of HIV and IPV may have profound neurocognitive sequelae, particularly among South African women who are disproportionately affected by trauma exposure (StatsSA, 2022) and HIV infection (23.5% for females vs. 12.1% for males in 2022 (UNAIDS, 2022)). However, there is a dearth of literature investigating how different IPV subtypes (e.g., injury, sexual coercion, physical assault, and psychological aggression) affect neurocognitive performance over time. We addressed this by investigating whether IPV (including sub-types) negatively impacts neurocognitive function in women with HIV over time. This is relevant for the prevention and management of women dually affected by HIV and IPV.
Using population-adjusted neurocognitive performance scores (Deist et al., 2023) for the HIV Neurobehavioral Centre's (HNRC) (HIV Neurobehavioral Research Center, 2022) International Neurobehavioral Battery (HNRC Battery), we evaluated:
Differences, if any, in global deficit scores (GDS) and domain-specific deficit scores between IPV-exposed versus IPV-unexposed women with HIV; and Associations between IPV sub-types (i.e., injury, sexual coercion, physical assault, and psychological aggression) and neurocognitive performance over one year.
Method
Sample and Procedure
A purposive convenience sample of women with HIV was directly recruited from the community and through healthcare centers for the parent study on biological endophenotypes of HIV and childhood trauma in South African women with HIV (ethics reference number: N07/07/153). Inclusion criteria were: (i) ability to read and write in English, Afrikaans, or isiXhosa at 5th grade level; (ii) no current or past diagnoses of schizophrenia, bipolar disorder, other psychotic disorders, or current seizure disorder of any cause; (iii) no current substance/alcohol use/dependence and/or psychotropic medication use; (iv) no history of central nervous system infections of neoplasms or significant head injury; and (v) a negative hepatitis B/C status. We confirmed participants’ HIV status through enzyme-linked immunosorbent assay.
Participants completed neuromedical, neurocognitive, and neuroimaging assessments at Stellenbosch University (Tygerberg campus). We collected data at baseline (n = 140; IPV-exposed n = 118, 84.3%) and 1-year follow-up (n = 73; IPV-exposed n = 58, 79.5%). At each time-point, we provided participants with refreshments and reimbursed them for transportation to and from the campus. Before data collection, participants provided written informed consent.
Measures
At baseline, participants self-reported their sociodemographic information. In addition to the main outcome measure (HNRC Battery), participants completed the Revised Conflict Tactics Scale 2 for Couples (RCTS: Straus et al., 1996) at each visit. Participants completed the measures in Afrikaans, English, or isiXhosa based on personal preference. We translated measures using forward- and back-translation techniques.
HNRC Battery
A trained research psychologist and research nurse administered the HNRC Battery to assess for HAND. The HNRC battery distinguishes between: (i) asymptomatic neurocognitive impairment; (ii) HIV-associated mild neurocognitive disorder; or (iii) HIV-associated dementia (HIV Neurobehavioral Research Centre, 2022). The HNRC Battery is widely used internationally (Cherner et al., 2007; Michael et al., 2021; the HNRC Group et al., 2018) and assesses learning, delayed recall, processing speed, attention/working memory, executive function, verbal fluency, and motor ability (Heaton et al., 2010). Where necessary, we adapted test instructions and stimuli to fit the South African cultural context (see Spies et al., 2017 for details). We computed HAND using recently generated South African norms (Deist et al., 2023). Specifically, we converted the raw scores for each neurocognitive test into scaled scores. Thereafter, we used the scaled scores to generate prediction equations using a multiple fractional polynomial (MFP) procedure. The MFP procedure (Royston & Altman, 1994) includes entering demographic variables known to account for significant variance in raw scores (including age, education, ethnicity, and neurocognitive test language) into the regression equation. Next, we used the adjusted MFP model to generate predicted test scores, after which we calculated residual scores for each participant. Thereafter, we converted the residual scores to demographically corrected T scores. We then converted the demographically corrected T scores to deficit scores as an estimate of the severity of neurocognitive impairment. The deficit scores were categorized as 0 (T score ≥ 40) = normal cognition; 1 (T score 35–39) = mild neurocognitive impairment; 2 (T score 30–34) = mild-to-moderate neurocognitive impairment; 3 (T score 25–29) = moderate neurocognitive impairment; 4 (T score 20–24) = moderate-to-severe NC impairment; and 5 (T score < 20) = severe neurocognitive impairment. We determined a GDS by averaging the deficit scores across all tests. A GDS ≥ 0.50 is indicative of poor neurocognitive performance.
Revised Conflict Tactics Scale 2 for Couples
We used the 78-item RCTS (Straus et al., 1996) to determine past-year IPV prevalence. The RCTS consists of subscales measuring injury, sexual coercion, physical assault, and psychological aggression. Scale items are considered as “less severe” or “more severe.” For example, for physical assault, items are considered “more severe” if they pose a greater risk of injury that may require medical attention as compared to “less severe” items. Importantly, “less severe” acts should not be mitigated and considered as a lesser problem to the victim or society (Hansrod et al., 2015). Subscales are also ranked on a continuum from least to most severe. Following the prevalence estimate scoring method, we calculated a dichotomous score (1 = present, 0 = not present) for each subscale to indicate whether at least one violent act from the scale had occurred in the past year. These subscale scores were then used to examine whether specific types of IPV influenced neurocognitive outcomes over time across all participants. The negotiation subscale was not included in these analyses, given that negotiation is typically understood as a positive conflict resolution strategy rather than a form of abuse. Furthermore, we calculated an RCTS total score to indicate if IPV was present overall (i.e., in one or more of the subscales) or not. The total RCTS score was used to categorize participants into two groups: IPV-exposed or IPV-unexposed. Thus, participants were classified as IPV-exposed if they were exposed to at least one form of IPV. This scoring method was previously applied to this sample and demonstrated high reliability (α=.90: Hansrod et al., 2015).
Secondary Measures
To control for the impact of other potentially traumatic events, posttraumatic stress symptoms (PTSS), and depression symptoms, participants completed the Life Events Checklist (LEC: Gray et al., 2004), the Childhood Trauma Questionnaire short form (CTQ-SF: Bernstein & Fink, 1998), the Davidson Trauma Scale (DTS: Davidson et al., 1997), and the Centre for Epidemiological Studies Depression Scale (CES-D: Radloff, 1977). These measures were described in detail in prior publications from the same cohort (see for example Deist et al., 2023; Hansrod et al., 2015; Spies et al., 2023; Spies & Seedat, 2014; Van der Watt et al., 2025). We provide a brief description of each.
The LEC (Gray et al., 2004) reliably measures exposure to potentially traumatic events to facilitate the diagnosis of posttraumatic stress disorder. It has proven reliability in the South African setting (e.g., Van der Watt et al., 2023; Ventimiglia et al., 2020). The CTQ-SF (Bernstein & Fink, 1998) is a standardized, retrospective 28-item self-report inventory measuring the severity of different types of childhood trauma including emotional abuse, physical abuse, sexual abuse, emotional neglect, and physical neglect. The CTQ-SF has proven reliability (α=.879) in the same sample population (Hansrod et al., 2015). In our sample, the Cronbach's α was .879. The DTS (Davidson et al., 1997) is a 17-item self-report measure of PTSS frequency and severity. The DTS has proven reliability (α=.885) in the same sample population (Hansrod et al., 2015). In our sample, the Cronbach's α was .981. The CES-D (Radloff, 1977) is a 20-item self-report measure of depression. The CES-D has proven reliability (α=.96) in the same sample population (Spies & Seedat, 2014). In our sample, the Cronbach's α was .964.
Analysis Plan
We analyzed the data using SPSS and Statistica. In addition to descriptive statistics, we used chi-square tests (for categorical variables) and Analysis of Variance (ANOVA: for continuous variables) to compare groups (IPV-exposed vs IPV-unexposed) on sociodemographic variables. We included variables with statistically significant group differences as potential covariates in subsequent analyses. Given the high rate of trauma exposure in the South African female population (e.g., Okafor et al., 2021; Yemeke et al., 2020), the known association between trauma exposure and neurocognitive function (e.g., Kavanaugh et al., 2017; Spies et al., 2017), and the association between PTSS and neurocognition (e.g., Jacob et al., 2019; Jak et al., 2016), we controlled for LEC, CTQ-SF, DTS, and CES-D scores. We used mixed linear models (MLM, Kenward-Rogers type III) to determine neurocognitive profiles over time (using the GDS and domain-specific deficits scores, respectively). Additional covariates included age, education, and home language. MLM allows for the use of all data points and the inclusion of incomplete cases, increasing the analysable sample size. We conducted LSD post hoc analyses to determine between-group and within-group differences at the different time points. We corrected for multiple comparisons throughout using Fisher LSD within each MLM. We used Eta-square to determine effect size. Statistical significance was set at p = .05.
Results
At baseline, there was a significant between-group difference in age (F(1) = 6.95, p < .01, η2 = 0.05). IPV-exposed participants were younger (mean = 32.43 years, SD = 6.54 years) compared to IPV-unexposed participants (mean = 36.50 years, SD = 7.21 years). There were significant between-group differences (see Table 1) in education (p = .01, Cramer's V = 0.30) and home language (p = .05, Cramer's V = 0.23) at 1-year follow-up.
Baseline and 1-Year Follow-up Sample Characteristics and Between-Group Differences.
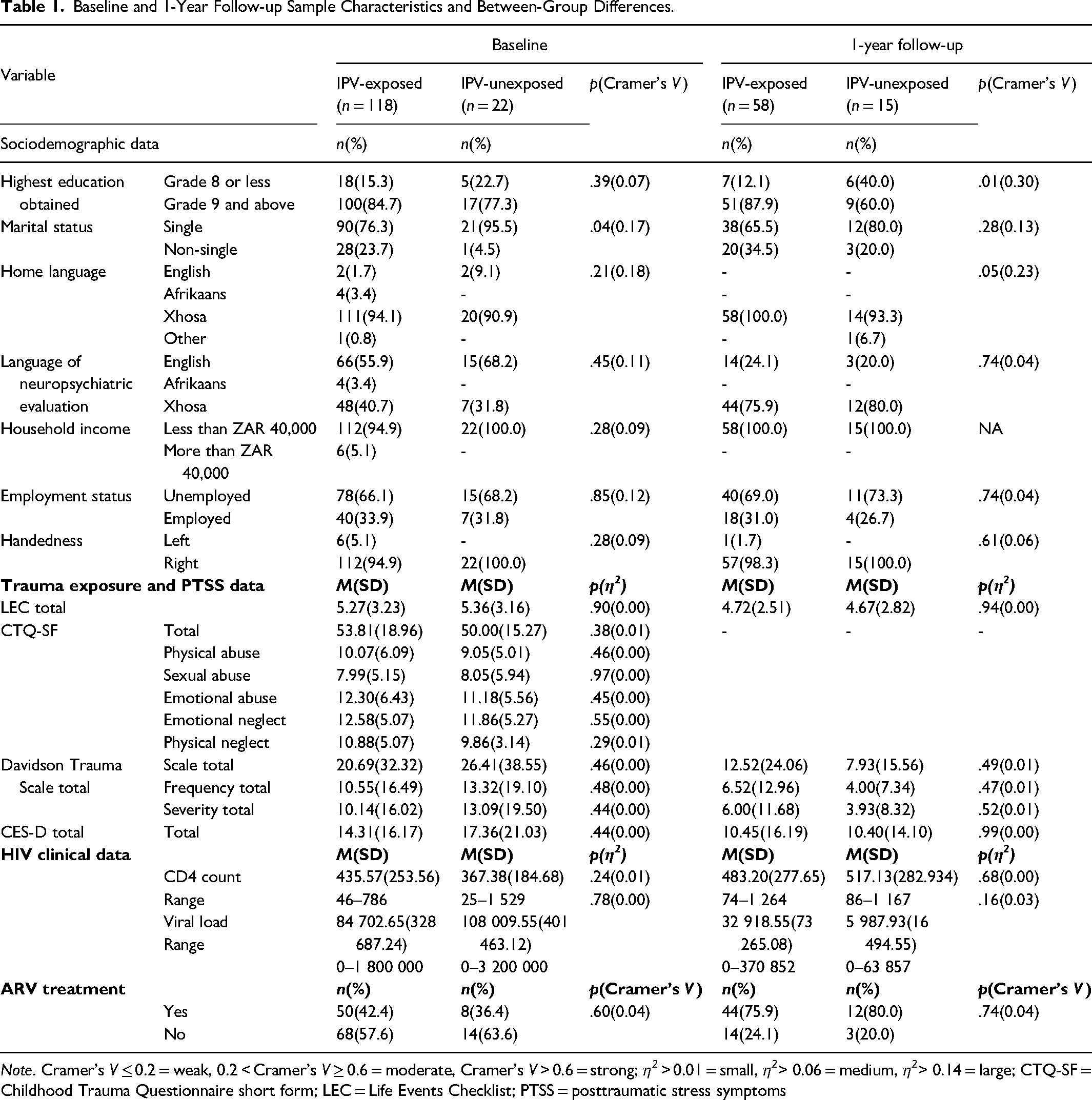
Note. Cramer's V ≤ 0.2 = weak, 0.2 < Cramer's V ≥ 0.6 = moderate, Cramer's V > 0.6 = strong; η2 > 0.01 = small, η2> 0.06 = medium, η2> 0.14 = large; CTQ-SF = Childhood Trauma Questionnaire short form; LEC = Life Events Checklist; PTSS = posttraumatic stress symptoms
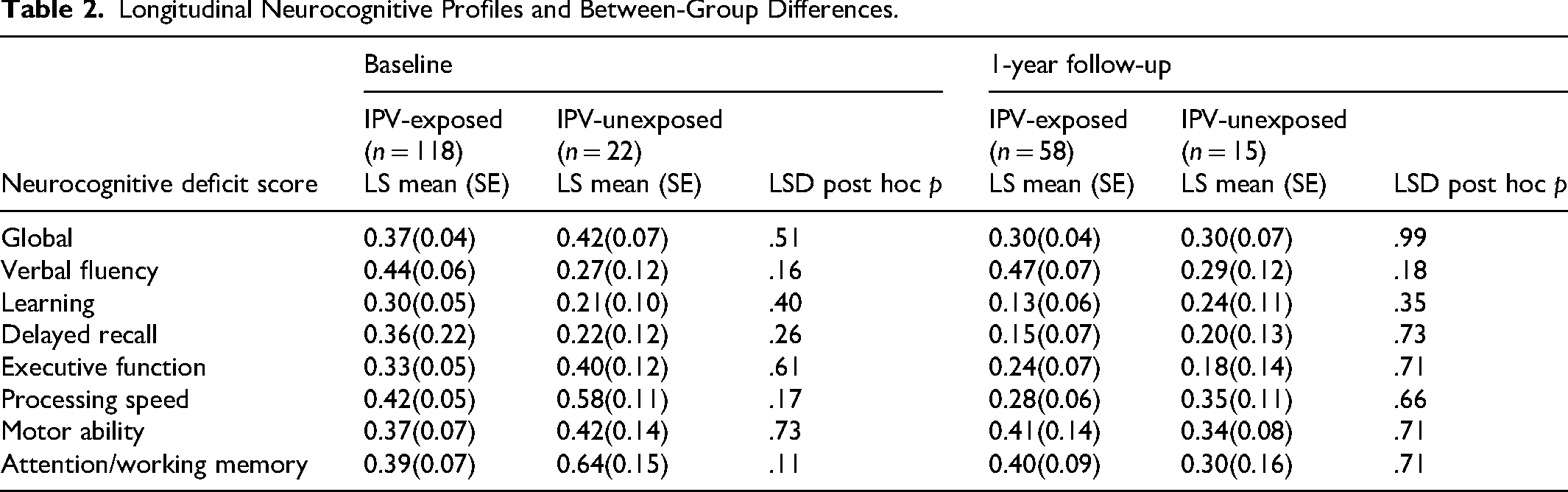
There were no between-group differences in GDS or domain-specific deficit scores at baseline or 1-year follow-up (see Table 2). However, there was a trend towards a between-group difference in attention/working memory deficit scores, with IPV-unexposed participants performing poorer compared to IPV-exposed participants. Further analysis indicated a trend towards a time*group interaction effect (F(1,111) = 3.20, p = .08) within the attention/working memory domain (see Figure 1). Attention/working memory slightly improved over time for IPV-unexposed participants (p = .07) but remained unchanged for IPV-exposed participants (p = .71).
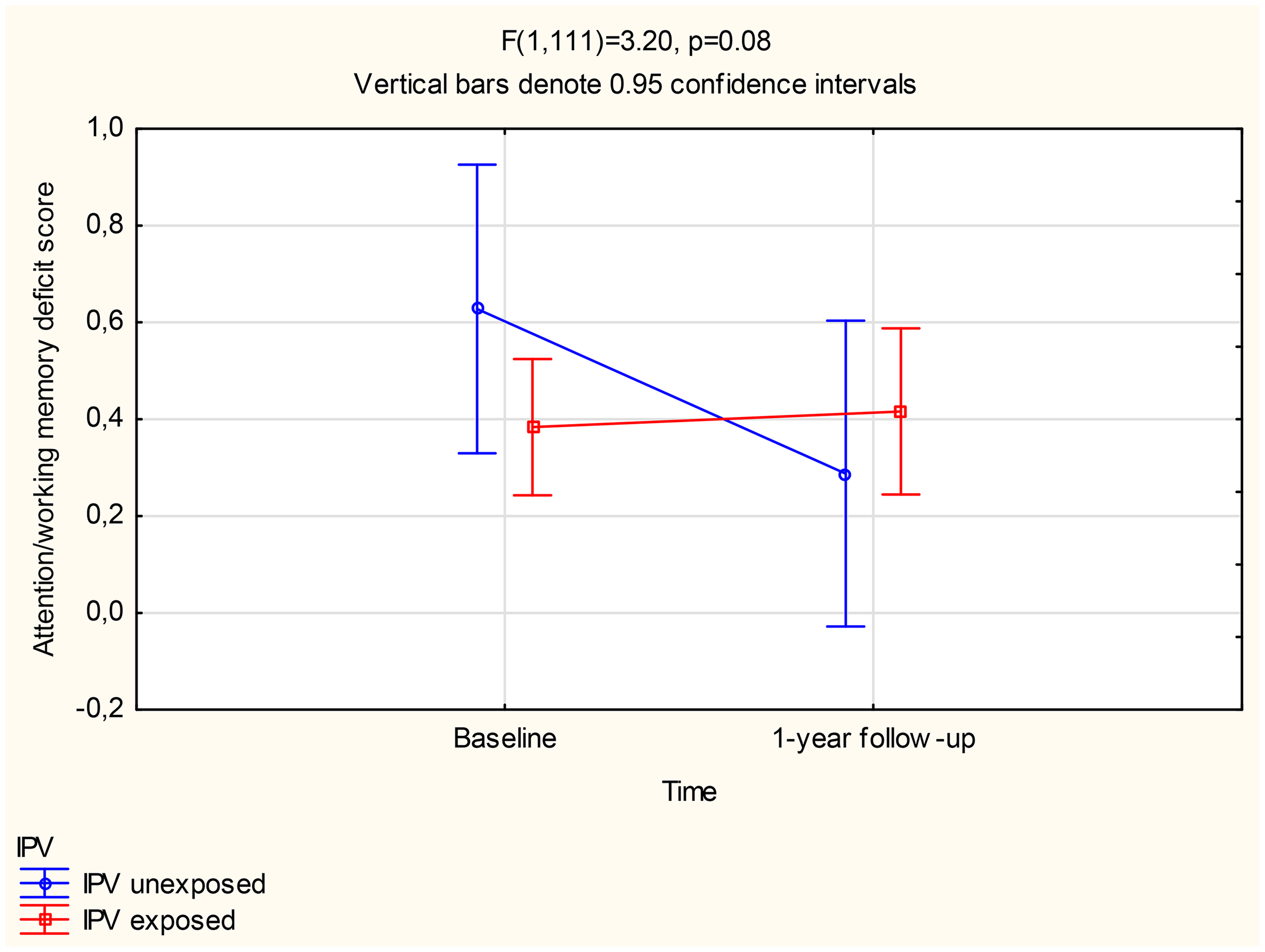
Between-group difference in longitudinal attention/working memory deficit scores.
Longitudinal Neurocognitive Profiles and Between-Group Differences.
Types of IPV Exposure and Neurocognition
Table 3 presents the prevalence of the distinct types of IPV exposure at baseline and 1-year follow-up. Following a generalized estimating equation (GEE), we found significant proportionate decreases in physical assault (p < .01) and sexual coercion (p = .03) over time.
Type of IPV Exposure at Baseline and 1-Year Follow-up.
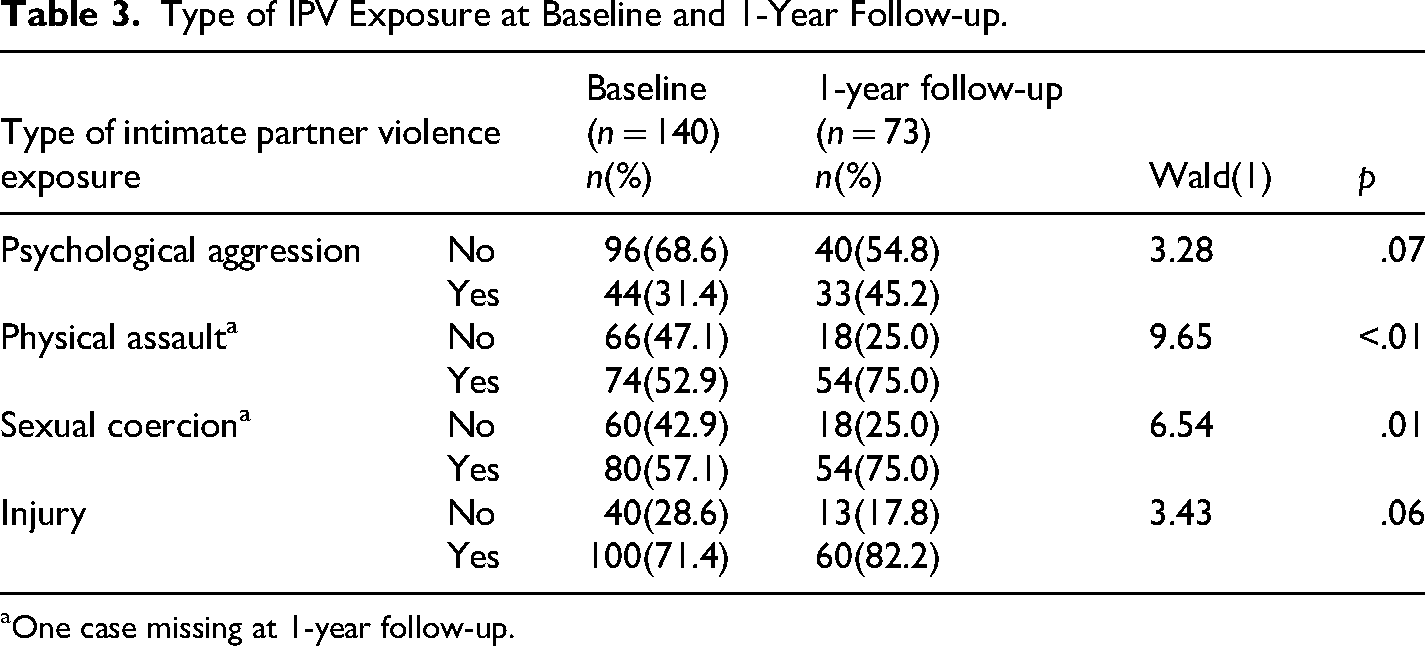
One case missing at 1-year follow-up.
There were no significant time*IPV type interaction effects when considering GDS (see Supplementary Table A); however, there was a trend toward a significant time*IPV type interaction effect for physical assault (F(1,88) = 3.67, p = .06, η2 = 0.04; see Figure 2). Post hoc analysis indicated a significant difference in GDS at 1-year follow-up (p = .04), with physical assault exposure associated with higher GDS (i.e., poorer performance). Over one year, there was a significant decrease in GDS (i.e., improved performance, p < .01) in participants not exposed to physical assault. In contrast, GDS remained unchanged (p = .69) in participants exposed to physical assault. Physical assault exposed participants’ baseline GDS was significantly higher (i.e., poorer performance) compared to the 1-year follow-up GDS of physical assault unexposed participants (p = .02).
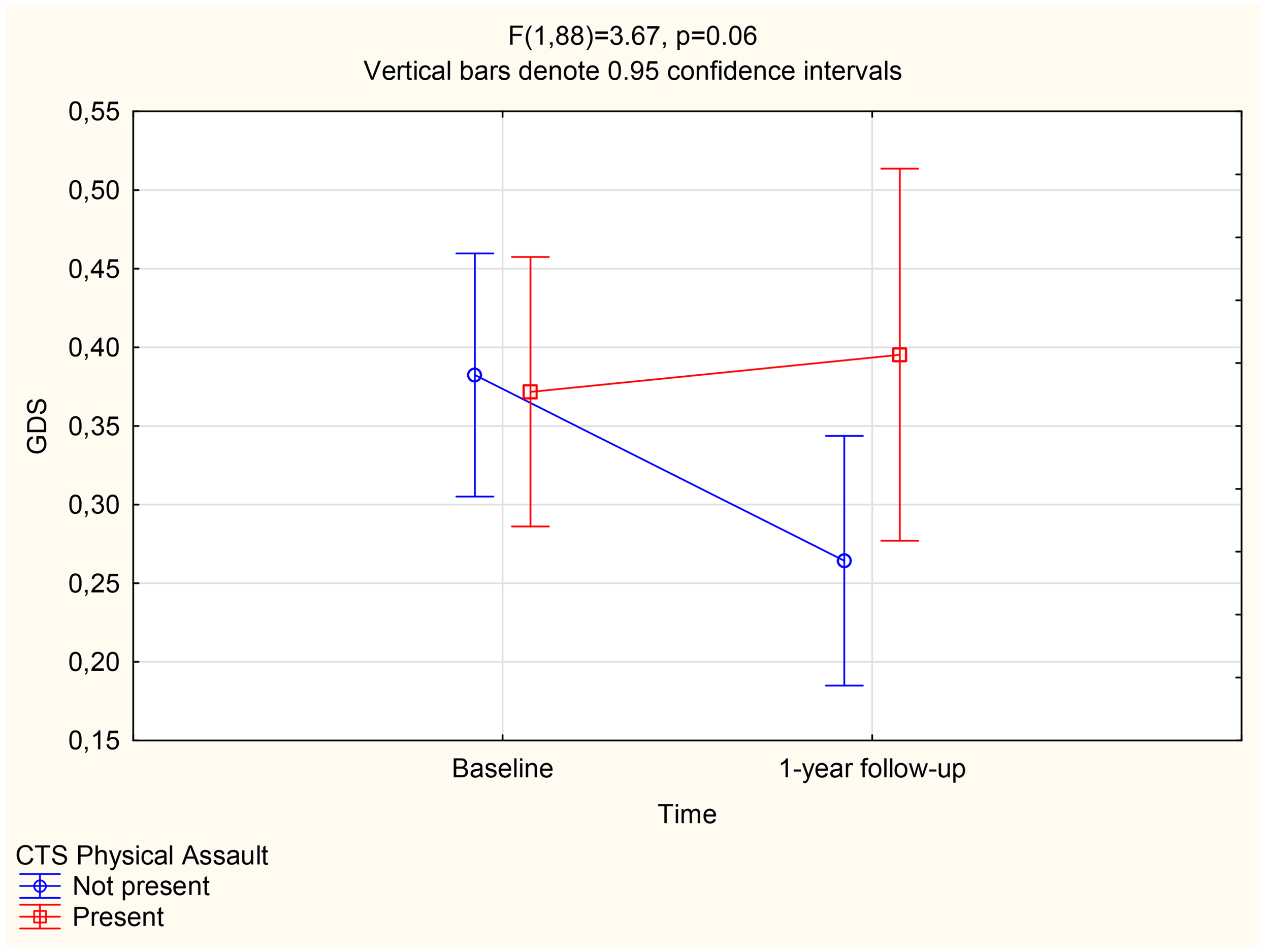
Between-group difference (physical assault exposure) in GDS over time.
Types of IPV Exposure and Attention/Working Memory
Given the above findings regarding attention/working memory and physical assault exposure, we conducted an MLM to determine if there was a significant time*IPV type interaction effect within the attention/working memory domain (see Supplementary Figure A). Results indicated a significant interaction effect (F(1,11) = 6.50, p = .01). Over 1 year, there was a strong trend toward a significant decrease in attention/working memory deficit scores (i.e., improved performance; p = .06) in participants not exposed to physical assault. In contrast, attention/working memory deficit scores slightly increased (i.e., poorer performance; p = .06) in participants exposed to physical assault. Further analysis of the attention/working memory domain and IPV type showed a significant time*IPV type interaction effect for sexual coercion (F(1,87) = 5.37, p = .02, η2 = 0.07) and injury (F(1,113) = 4.31, p = .02, η2 = 0.05), respectively (see Supplementary Figures B and C). Based on post hoc analysis, sexual coercion unexposed participants’ deficit scores slightly decreased (i.e., improved performance; p = .10) over time, while sexual coercion exposed participants’ deficit scores marginally increased (i.e., poorer performance; p = .09). Lastly, injury unexposed participants’ deficit scores slightly decreased (i.e., improved performance; p = .18) over time, while injury exposed participants’ deficit scores marginally increased (i.e., poorer performance; p = .08).
Discussion
In our sample of women with HIV, there was no significant between-group difference in GDS of IPV-exposed and IPV-unexposed participants at baseline or 1-year follow-up, yet we noted a trend for between-group differences in attention/working memory deficit scores. Analyses considering the different IPV types within the attention/working memory domain revealed significant time*IPV type interaction effects for physical assault, sexual coercion, and injury, respectively.
The Effect of IPV Exposure on Global and Domain-Specific Cognition
Given that both HIV (e.g., Daneman & Prat, 2015) and IPV (e.g., Clark, 2019; Esopenko et al., 2021) are associated with poorer cognition, we expected that IPV-exposed women with HIV would have significantly higher GDS (i.e., poorer performance) compared to IPV-unexposed women with HIV. However, our results revealed no significant difference in the present sample. Similarly, previous research in the same population examining longitudinal neurocognitive outcomes among women with and without HIV reported no significant differences in GDS, but did identify significant differences in domain-specific deficits, particularly in learning and attention/working memory (Van der Watt et al., 2025). These findings underscore the importance of considering the sensitivity and discriminative power of composite measures like the GDS compared to evaluating individual tests or specific cognitive domains separately (see also Van der Watt et al., 2025). Additionally, the results may be influenced by the application of the recently developed South African norms for the HNRC Battery (Deist et al., 2023), which were also used by Van der Watt et al. (2025). The importance of country- and population-specific norms in neurocognitive assessment cannot be overemphasized (Kiselica et al., 2024; Raudeberg et al., 2021; Villalobos et al., 2023).
However, consistent with Van der Watt et al. (2025), who observed significant differences in domain-specific deficit scores, including learning and attention/working memory, we also identified a trend toward between-group differences in the attention/working memory domain. This is in line with previous research linking specific neurocognitive domains to IPV perpetration (Chiu et al., 2022), where poorer working memory was significantly associated with greater aggression during conflict discussions among couples (Godfrey et al., 2020). Similarly, female victims of psychological IPV have demonstrated deficits in attention and decision-making (Daugherty et al., 2019). Collectively, these findings emphasize the importance of considering the sensitivity and discriminative capacity of composite measures like the GDS, in addition to evaluating individual tests or cognitive domains separately (see also Van der Watt et al., 2025).
Surprisingly, IPV-unexposed participants had higher baseline attention/working memory deficit scores (i.e., poorer performance), compared to IPV-exposed participants. This contradicts findings that IPV is associated with memory loss (Potter et al., 2021; Zieman et al., 2017). Yet, the time*IPV interaction effect indicated that IPV-unexposed women's attention/working memory deficit scores declined over time (i.e., improved performance), while the IPV-exposed women's deficit scores remained the same. This suggests that IPV exposure is a barrier to improvements in attention/working memory time (likely driven by antiretroviral use (e.g., Spies et al., 2017; Van der Watt et al., 2025)) among women with HIV. Future research incorporating objective measures of antiretroviral therapy adherence is needed to better understand its influence on the longitudinal neurocognitive functioning of women with HIV who have also been exposed to IPV.
Type of IPV Exposure and Neurocognition
Physical assault exposed participants’ GDS was significantly higher (i.e., poorer performance) compared to physical assault unexposed participants’ GDS at 1-year follow-up. Physical assault unexposed participants’ GDS significantly declined over time (i.e., improved performance), while the GDS of physical assault exposed participants remained unchanged. This supports findings from a multicountry study that specific types of IPV differentially affect health outcomes among female IPV victims (Potter et al., 2021).
Regarding physical assault as an IPV subtype, there is the possibility of traumatic brain injury (TBI: Haag et al., 2022) as measured by RCTS items (i.e., “beat up,” “choked,” and “slammed against wall”: Straus et al., 1996). Research indicates poorer executive functions in women with IPV-related TBI, compared to IPV-related sexual assault victims (Raskin et al., 2024). Yet, one would expect similar findings of higher GDS (i.e., poorer performance) for the injury subscale (as it may also indicate TBI)—which was not the case for GDS in our cohort. Additional item-specific analyses within a larger sample that also incorporates TBI data may help to clarify our findings.
Types of IPV Exposure and Attention/Working Memory
We found significant time*IPV type interaction effects within the attention/working memory domain for physical assault, sexual coercion, and injury, respectively. For all these IPV types, attention/working memory deficit scores remained the same over time for exposed women, while deficit scores decreased (i.e., improved performance) for unexposed women. This suggests that physical assault, sexual coercion, and injury, respectively, are significant barriers to improvements in attention/working memory performance over time among women with HIV. In accordance with the above, the findings of physical assault exposure may be related to potential TBI. Research indicates poorer memory in women who experienced IPV-related TBI, compared to women who experienced IPV-related sexual assault (Raskin et al., 2024). Specifically, the presence of ‘chocking’ was associated with poorer Hopkins Verbal Learning Test (HVLT: Brandt, 1991) recall performance (Raskin et al., 2024). Yet, it is important to note that Raskin et al. (2024) excluded sexual assault victims who experienced a blow to the head or strangulation. This is not necessarily the case in our cohort. Further analyses controlling for specific items (such as “choked”) within a larger sample are necessary to determine if sexual coercion exposure without the possibility of TBI will remain significantly associated with poorer attention/working memory over time.
The slight increase in attention/working memory deficit scores (i.e., poorer performance) over time among women exposed to physical assault, sexual coercion, and injury suggests that all IPV types (except for psychological aggression) as measured by the RCTS pose a risk for poorer longitudinal attention/working memory among women with HIV. Research supports the association between IPV victimization and poorer attention (Daugherty et al., 2019).
Notably, the dichotomous scoring approach of the RCTS assesses IPV exposure without distinguishing between victimization and perpetration (see Straus et al., 1996 for scoring instructions). Evidence suggests that male IPV perpetrators often display cognitive deficits, particularly in attention and memory domains (Romero-Martinez et al., 2021). Specifically, violent IPV perpetrators perform worse than nonviolent controls on measures of attention, sustained attention, and working memory. A recent meta-analysis further confirmed that IPV perpetrators exhibit poorer neuropsychological functioning—including working memory, attention switching, cognitive flexibility, planning, and phonemic fluency—compared to nonviolent men (Romero-Martinez et al., 2024). Consequently, it is not possible to determine whether the observed effects in the attention/working memory domain in our sample were driven by victimization, perpetration, or both, as our sample likely included individuals who were perpetrators of IPV. Indeed, South African studies commented on the underreported prevalence of male victims of domestic abuse, their silence (Barkhuizen, 2015; Kgatle & Mafa, 2021; Modau, 2016; Tshoane et al., 2024), and the inadequacies of the criminal justice system in protecting them (Tshoane et al., 2023). Victims of violence are also more likely to become perpetrators of violence (e.g., Kurniawan et al., 2019). While we found no difference in LEC among IPV-exposed and unexposed women within our sample, we did not isolate the physical and sexual assault items of the LEC. Combined, this warrants further analyses within a larger sample, which considers the IPV status (i.e., perpetrator or victim) to fully understand our findings regarding attention/working memory and the potential circular effect.
Implications
Prior research among the same cohort of women with HIV found a significant decrease in GDS (i.e., improved performance) over one year after controlling for childhood adverse events, lifetime trauma exposure, and PTSS (Van der Watt et al., 2025). The authors hypothesized that this may be due to the increased antiretroviral use (between baseline and 1-year follow-up), which possibly facilitated improved cognitive function (Cross et al., 2013; Nakasujja et al., 2010; Sacktor et al., 2006). Yet, among our sample with comparable antiretroviral use, IPV-related physical assault exposure hindered longitudinal cognitive improvement. This highlights how different IPV profiles may differentially impact health over time and should be considered when developing interventions (Potter et al., 2021). For instance, our findings showed that both injury and sexual coercion were associated with a decline in attention/working memory over time; however, the effect of sexual coercion was of medium magnitude, whereas the effect of injury was small. Further research is needed to clarify the mechanisms through which different forms of IPV uniquely affect attention/working memory. The high prevalence of IPV in our sample (ranging from 79.45% to 84.29%) reinforces the need for healthcare professionals to screen for IPV among women with HIV (Hansrod et al., 2015). These rates exceed previous estimates reported for South African women with HIV (56.3%: Matseke et al., 2016), highlighting the urgency of training HIV care providers in comprehensive trauma screening, linking at-risk women to appropriate services and interventions (Yemeke et al., 2020), and delivering trauma-informed care (Brown & Adeagbo, 2022). Women with HIV who have experienced IPV should receive additional counseling and ongoing support to reduce the impact of IPV as a barrier to longitudinal neurocognitive improvement. Interventions should particularly target women exposed to IPV-related physical assault, as all forms of IPV (including physical assault, sexual coercion, and injury) except psychological aggression were found to specifically hinder attention and working memory improvement over time. Therefore, healthcare professionals should monitor changes in attention and working memory in women with HIV, as such changes may indicate IPV exposure. These findings further emphasize the importance of broader implementation of IPV screening in HIV care settings and the integration of trauma-focused interventions into HIV treatment (Yemeke et al., 2020). Lastly, our findings highlight the importance of educating women with HIV about IPV. This includes working toward greater gender equality within South Africa to reduce the prevalence of IPV (Falb et al., 2015).
Limitations, Future Recommendations, and Strengths
The small sample, especially at 1-year follow-up, limits the statistical power of our findings, despite the strength of the longitudinal design. However, MLM allowed us to use all data points and to include incomplete cases, increasing the analyzable sample size. Nonetheless, we encourage future research with a larger sample.
The exclusion of women using psychotropic medication at study entry in the parent study may have unintentionally introduced selection bias. Women exposed to IPV often present with symptoms of depression (e.g., Woolhouse et al., 2019) and anxiety (Chandan et al., 2020), conditions that are frequently managed with psychotropic medication. Consequently, those experiencing more severe mental health effects of IPV may have been underrepresented, and exclusion of these women may have resulted in an attenuation of observed associations with cognitive outcomes.
We acknowledge that the difference in sample size between IPV-exposed and IPV-unexposed participants may have affected the assumption of equal variances and the possibility of a Type 1 error (Parra-Frutos, 2013). However, dichotomous scoring was previously proven to be reliable within the same cohort (Hansrod et al., 2015) and another multi-country IPV study (Potter et al., 2021). Also, the prevalence scoring method allowed for the direct comparison of IPV-exposed versus IPV-unexposed HAND data and served as an accurate representation (and reminder) of the high IPV exposure rates among South African women in general (24%: World Health Organization, 2019) and South African women with HIV (56%: Matseke et al., 2016). Nevertheless, we recommend future research with more balanced sample distributions and/or the use of IPV as a continuous variable to validate our findings. Applying the chronicity scoring method (Straus et al., 1996) could further clarify the effects of cumulative IPV and polyvictimization, which may differentially influence longitudinal neurocognitive functioning.
IPV is a multifaceted and complex phenomenon which is not necessarily accurately captured by the use of a single measure such as the RCTS (Hansrod et al., 2015). The RCTS does not consider the context, meaning, and motives behind IPV. Further, the dichotomous scoring method does not differentiate between victims and perpetrators. This limits our interpretation of the findings and precludes us from drawing definitive conclusions. Thus, research using the RCTS can benefit from supplemental interviews to provide contextual information (Chapman & Gillespie, 2019) which must be considered to minimize the possibility of inflating IPV rates (Lehrner & Allen, 2014). Future research should consider using multiple IPV measures, including qualitative interviews, to provide better contextual information.
The use of self-report demographic, trauma, and IPV exposure measures possibly contributed to social desirability bias. While objective measures such as medical and social service records may reduce social desirability bias, South African women are reluctant to officially report IPV, given experiences of insufficient support by public services (TEARS, 2022) and the normalization of abuse in South Africa (Gordon, 2016). This highlights the importance of using multiple sources of information to determine IPV prevalence.
Lastly, our sample was mostly Xhosa-speaking (with only one participant reporting a different home language at 1-year follow-up), limiting the generalizability of our findings to women with a different home language. While we did control for home language in all analyses, future research should include women with different home languages to reflect the South African population (Statista, 2024).
Despite the above limitations, our research provides valuable insights into the progression of HAND and the effect of IPV on this progression. Specifically, we added to the work of Potter et al. (2021) in providing a basis from which to better understand how different IPV types may impact women's health, with a specific focus on women with HIV. Our findings are further strengthened by the use of longitudinal data as opposed to the cross-sectional data of Potter et al. (2021). Lastly, our research aligns with the 5th Goal (Gender Equality and Women and Girls’ Empowerment) of the Sustainable Development Goals (United Nations, n.d.), which is especially important within the South African context, where women are disproportionately affected by IPV exposure (O’Regan, 2022) and HIV (UNAIDS, 2022).
Conclusion
Among our sample of women with HIV, IPV-related physical assault exposure was a barrier to longitudinal neurocognitive improvement. Further IPV-related physical assault, sexual coercion, and injury were barriers to longitudinal attention/working memory improvement. Our findings highlight the importance of screening for IPV and IPV subtypes among women with HIV for improved support and targeted interventions focusing on improving attention/working memory. We encourage the continued effort towards educating people about IPV and gender equality within South Africa to decrease the prevalence of IPV.
Supplemental Material
sj-docx-1-vaw-10.1177_10778012251397969 - Supplemental material for Longitudinal Neurocognitive Performance in South African Women With HIV and Domestic Violence
Supplemental material, sj-docx-1-vaw-10.1177_10778012251397969 for Longitudinal Neurocognitive Performance in South African Women With HIV and Domestic Violence by A. S. J. Van der Watt, G. Spies and S. Seedat in Violence Against Women
Footnotes
Acknowledgments
We thank the women who participated in this study. We thank Professor Martin Kidd for assisting with the statistical analyses and norming of the neurocognitive data.
Funding
AvdW received funding from the National Institutes of Health Pittsburgh & Stellenbosch Universities HIV-Associated Cardio-Metabolic, Chronic Kidney and Neuropsychiatry Diseases Research Training Fellowship Programme to write this manuscript. Additional research support was provided by a CFAR grant awarded to S Seedat [P30-AI036214] and the HIV Neurobehavioral Research Center (HNRC; National Institutes of Health [grant number P30-MH62512]). This work is supported by the South African PTSD Research Programme of Excellence and the South African Medical Research Council/Stellenbosch University Genomics of Brain Disorders Research Unit.
Authors’ Contributions
SS contributed to study conception and writing the manuscript. GS contributed to study conception, recruitment, data collection and management, and writing the manuscript. AvdW contributed to data cleaning, data analysis, and manuscript writing.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.