
Abstract
Intimate partner violence is highly prevalent worldwide. Previous research has linked partner violence with reduced contraceptive use, but little is known about the role of non-physical violence in non-Western contexts. Using data from the 2015–16 India Demographic and Health Survey, this study investigates how unequal gender dynamics, marital violence, and coercive control influence unmet need for contraception. Findings suggest that coercive control may play an important role in shaping women's contraceptive use and reproductive autonomy. Health practitioners and advocates should consider coercive control by spouses as a meaningful barrier to contraceptive uptake when women wish to space or limit pregnancies.
Background
In recent years, intimate partner violence has gained attention as a cause for concern for policymakers and scholars alike, in part because of the well-established relationship between intimate partner violence (IPV) and adverse physical and mental health outcomes. Globally, over 25% of women report experiencing physical or sexual violence by an intimate partner over their lifetimes (WHO, 2024). Previous research has identified a relationship between IPV and reproductive outcomes and decisions (Maxwell et al., 2015; Miller et al., 2010; Paul & Mondal, 2022). Reproductive health problems, including urinary tract infections, unplanned or unwanted pregnancies, and chronic pelvic pain, are among the most common long-term health consequences among women survivors of IPV (Campbell, 2002). Cultural norms related to marital dynamics and intimate partner violence influence victims’ perceptions of the violence and their willingness or ability to seek assistance or act to subvert IPV. This study contributes to existing knowledge of the effects of intimate partner violence by assessing how different types of violence, including non-physical abuse tactics classified as coercive controlling behaviors, influence reproductive autonomy among Indian women by contributing to women's likelihood of experiencing an unmet need for contraception.
India is a relevant case study for the relationship between intimate partner violence and reproductive autonomy for several reasons. First, significant gaps in men's and women's status persist. Women in India are 76% as likely as men to enroll in college, but only 36% as likely to participate in the workforce (World Bank, 2012); fewer than 1 in 5 Indian women are formally employed (International Labour Organization, 2022). Traditional Indian society boasts of a system of joint family, the subordination of women to men within the household, patriarchy, and hierarchy (Ahmed-Ghose, 2004; Derne, 1994; Sabri & Young, 2022; Tichy et al., 2009), and entrenched gender ideologies have reinforced the importance of homemaking and childbearing as priorities for Indian women (Anukriti et al., 2022; Dube, 1988). Second, IPV is common in India, impacting up to 40% of women in the country (Garg et al., 2021). Third, marriage is nearly universal in India, but divorce is extremely rare (Biswas, 2016). Consequently, women are less likely to feel able to exit their marriages if they become violent or their autonomy becomes undermined by their husbands. Social pressures in favor of both marriage and childbearing may create barriers for women to actualize upon their own fertility preferences or leave their husbands if they feel threatened.
Finally, unmet need for contraception—defined as contraceptive non-use when a woman who is of childbearing age and capable of conceiving does not want to become pregnant in the next 2 years—is relatively high in India and remained around 20% for Indian women in the 10 years prior to the collection of the data used in this study (WHO, 2015). Despite recent declines in unmet need for contraception (Sedgh et al., 2016), there remains considerable prevalence, particularly among younger women. Providers in India routinely counsel women to space births 2–3 years apart, and many women express a desire to follow this advice (Chor et al., 2012; Smith et al., 2017). However, contraception for spacing is not always used, due to a lack of knowledge about different methods, opposition from husbands, and concerns about side effects (Sedgh & Hussain, 2014; Smith et al., 2017). Several persistent myths about the consequences of modern contraceptives have deterred many women from adopting short-term reversible methods of contraception (Mohanty et al. 2020). Moreover, women who do not want additional children report feeling pressured by husbands and family members, creating barriers to contraceptive use for the purposes of limiting fertility (Smith et al., 2017). A distinguishing characteristic of the contraceptive landscape in India is the high prevalence of female sterilization; among women reporting both a need for contraception and use of any method, approximately 76% identified sterilization as their method of choice (Ewerling et al., 2021). Due to its permanence, sterilization differs significantly from many other contraceptive methods, which are short-term and reversible, and able to be used for spacing pregnancies. For this reason, barriers to the uptake of contraception earlier in the reproductive life course are of particular concern in the Indian context.
This study contributes to the empirical and theoretical understanding of the relationship between IPV and reproductive autonomy in two ways. First, it examines the prevalence of coercive control and limits to personal autonomy in a nationally representative sample of Indian women, and identifies patterns of victimization across aspects of violence and gendered disadvantage. Second, it adds to our theoretical understanding of the consequences of IPV by expanding analysis of the relationship between marital violence and reproductive decision-making to include non-physical aspects of abuse, including coercive control. Physical violence and sexual violence are considered alongside these “non-violent” tactics, building on and responding to existing literature on spousal abuse and contraception. Abuse tactics beyond physical and sexual violence are understudied with regard to reproductive health and reproductive autonomy, particularly in non-Western contexts; this study aims to address this gap by considering the unique role of coercive control and how it co-occurs with other forms of violence.
Gendered Power Dynamics and Marital Violence in the Indian Context
A growing body of literature has emerged examining the prevalence and consequences of marital violence in India. Large multisite studies in India indicate that marital violence against women is prevalent across castes, regions, religious groups, education levels, and socioeconomic status (Bhat & Ullman, 2013; Garg et al., 2021; International Institute for Population Sciences (IIPS) & Macro International, 2007). Because marriage is so universal in India, it is expected that all women will marry, and almost all IPV in India occurs in the context of marriage. In addition, arranged marriage remains a common practice in India (Allendorf & Pandian, 2016). Arranged marriage without the consent of both partners may add to the risk of marital violence victimization among Indian women (Sabri et al., 2014). This, combined with patriarchal and patrilocal norms, creates unique risk factors for women in India, who often have little recourse from these marriages. Arranged marriages contribute to a higher prevalence of educational hypogamy in Indian marriages than is seen in Western contexts; in particular, Lin and colleagues (2020) find that Indian women are more likely to marry men who have less education than they do, but who come from more privileged families. When a woman's education or employment places her at an advantage, men may correct for this perceived threat to their dominance using violence (Weitzman, 2014).
Gendered marital dynamics, which may influence women's health and reproductive control, are not limited to marital violence. Broader patterns of gender norms and gendered power dynamics contribute to limits to women's autonomy both within and beyond the immediate household. Basu (1992) defined autonomy as women's ability and freedom to act independently: for example, to go places (such as a clinic or market), or make decisions related to health or household purchases, without needing permission. Gender norms limit women's activities outside the home in many parts of India, particularly in rural areas (Anukriti et al., 2022). These norms result in relatively high levels of social isolation (Kandpal & Baylis, 2019), and low access to spaces where health-related decisions are made, such as clinics and pharmacies, without a husband or other relative present. Women in India also have comparatively fewer resources than men. Nearly 20% of Indian women do not have access to a bank account, and many Indian women's bank accounts are inactive (Kumar, 2022). While financial inclusion advocates have argued that mobile banking has the potential to increase women's financial inclusion in many developing contexts, India has one of the largest gender gaps in mobile phone access in the world (GSMA, 2020). A lack of mobile phone access results in the loss of access to mobile banking, reduced contact with social ties, and lower access to information and health services (Mohan et al., 2020). As a result, more general gender inequalities may contribute to women's general and reproductive health and autonomy.
These entrenched gender ideologies also give rise to widespread beliefs about the roles of husbands and wives, and the acceptability of marital violence. Studies show that 42% of Indian men and 48% percent of Indian women express that wife beating is acceptable under some circumstances (Dasgupta 2019; Pradhan & De 2024); Because patriarchal gender ideologies are often associated with coercive control (Stark, 2007), it is possible that coercive controlling behaviors are prevalent and impactful in Indian marriages, including with regard to reproductive autonomy.
Conceptualizations and Typologies of Intimate Partner Violence
Conceptually, intimate partner violence is a complex set of dynamics that may include a variety of physical and non-physical tactics. Johnson (1995, 2001 ) argues that the umbrella term “intimate partner violence” is often used to describe two different (though related) phenomena: situational couple violence (SCV), and intimate terror violence. Johnson's typology bridges the seemingly contradictory approaches of family violence theory, which views IPV as matter of conflict arising from common family stresses (Straus et al., 1980; Straus & Smith, 1990), and feminist theory, which conceptualizes IPV as a matter of control, rooted in patriarchal norms which center male dominance in heterosexual relationships (Dobash & Dobash, 1979; Stark & Flitcraft, 1996; Stets, 1988). Johnson (1995) describes intimate terror violence as violence embedded in a broader pattern of controlling behaviors. Situational couple violence, in contrast, refers to violence occurring absent this broader pattern of control. These two types of violence are not differentiated by the number or severity of violent tactics; Johnson and Leone (2005) demonstrate that there are cases of severe violence that do not include coercive control. At the same time, perpetrators of intimate terrorism may not use physical aggression frequently, or may not employ severe violence to exert control, instead employing a range of non-violent tactics, including emotional abuse, isolation, economic abuse, threats, and intimidation. Other scholars working in the feminist tradition have written about these strategies as well (Lloyd & Emery, 2000; Stark & Flitcraft, 1996), highlighting how abusers utilize nonviolent tactics to maintain control over their partners. Some evidence suggests that victims of both violent and nonviolent coercive controlling relationships exhibit similar levels of fear (Crossman et al., 2016), underscoring the consequences of coercive control for victims.
Using this framework, researchers in the United States and Canada have identified differential consequences of intimate terror violence and situational couple violence. Johnson and Leone (2005) find that post-traumatic stress disorder symptomology is more prevalent and more severe for survivors of intimate terror. Some studies also find that intimate terror victims are more likely to seek formal support, such as help from the police or nongovernmental organizations, than survivors of SCV, but are less likely to engage in informal support-seeking through their personal networks (Ansara & Hindin, 2010; Leone et al., 2007), possibly as a result of intimate terror victims’ increased discomfort and awareness of their need for help (Johnson & Leone, 2005). Research using this framework to examine intimate partner violence in non-Western contexts is limited, but growing. Studies examining IPV and many outcomes, including health outcomes, in developing countries often focus primarily on physical violence, without differentiating between relationships in which coercive control tactics are used and those in which they are not. The evidence from the United States and Canada suggests that this distinction is significant and that coercive control and restrictions placed on personal autonomy are likely to have separate or additional consequences for those who are experiencing other forms of IPV. Studies that do examine coercive control in non-Western contexts have identified differential patterns of abuse consistent with Johnson's typology, including clustering of coercive control with other forms of abuse, physical abuse without coercive control, and experiences of coercive control without reports of other forms of IPV (Decker et al., 2021; Jaramillo-Sierra & Carvajal-Villalobos, 2021; Kanougiya et al., 2021).
Intimate Partner Violence and Reproductive Control
Although IPV has been linked to many adverse health outcomes, including acute injuries, chronic health conditions (Black, 2011; Weitzman & Goosby, 2021) and mental health troubles, reproductive health problems remain among the most prevalent health consequences of IPV for women (Campbell, 2002). Reproductive coercion, defined as “behavior that interferes with contraception use and pregnancy in ways that reduce female control over reproductive decisions, including pregnancy coercion and contraceptive sabotage” (American College of Obstetrics & Gynecology, 2013), is associated with IPV and may co-occur with other forms of IPV, including sexual violence, physical violence, and coercive control. Women who experience IPV are twice as likely to have a male partner refuse to use contraception (Dasgupta et al., 2015; Garcia-Moreno et al., 2006) or engage in condom or contraceptive sabotage (Wood et al., 2020). IPV and reproductive coercion are associated with numerous adverse reproductive health outcomes, including unintended pregnancies (Miller et al., 2010; Pallitto et al., 2013), induced abortions (Stephenson et al., 2016; Thakuri et al., 2020), and elevated risks of miscarriage, stillbirth, and infant mortality (Afiaz et al. 2020; Okenwa et al., 2011; Pastor-Moreno et al., 2020).
A significant body of work examining the relationship between intimate partner violence and reproductive autonomy in South Asia has focused on the association between violence and the utilization of modern contraceptive methods (Dalal et al., 2012; Forrest et al., 2017; Paul & Mondal, 2022). Investigating the relationship between IPV and contraceptive behaviors in Pakistan, Zakar and colleagues (2012) find that women who experienced severe physical abuse are less likely to have their husbands’ support in using contraception, and are more likely to experience unplanned pregnancies and poor prenatal care. In a cross-national study using data from Bangladesh, India, and Nepal, Raj and McDougal (2015) find that IPV is associated with higher rates of contraceptive failure. Some evidence suggests that reproductive coercion in India occurs more often in the context of physical and sexual spousal violence (Silverman & Raj, 2014).
Despite this growing body of literature, the relationship between IPV and contraception remains inconclusive. Existing research found a varying degree of effects of IPV on contraceptive usage; some studies have found a significant, positive association between IPV and the likelihood of using contraception (Chen et al., 2020; Dalal et al., 2012), while others have found a reduced likelihood of contraceptive usage (Bishwajit & Yaya, 2018; Stephenson et al., 2008), or a null finding (Tiruye et al., 2020), depending on how IPV was operationalized. In studies conducted in India (Raman et al., 2016; Tiwari et al., 2018) and sub-Saharan Africa (Kibira et al., 2020), women reported that they lacked autonomy with regard to reproductive decisions or experienced conflict with their partners over contraceptive use; some conveyed that threats of physical violence led them to abstain from using modern contraceptives. A recent study found that Indian women who experience coercive control by their husbands are less likely to use modern contraceptive methods, compared to no method or traditional methods, and are more likely to undergo female sterilization (Paul & Mondal, 2022). Female sterilization is broadly the most common method of contraception used in India (Ewerling et al., 2021), in part due to now-defunct campaigns promoting it to limit population growth (Gupta 2017). The high prevalence of sterilization is due in part to misconceptions about temporary, reversible contraceptive methods (Mohanty et al., 2020), opposition from family members (Singh et al., 2021), and barriers to access and continuation of modern methods. Female sterilization is particularly common in rural areas and is especially prevalent among poorer and less educated women (Singh et al., 2021). Women in violent and controlling relationships may be more likely to opt for sterilization due to a lack of knowledge of or access to other forms of contraception, or because sterilization is uniquely immune to interference by an abuser (Paul & Mondal, 2022).
Conversely, some research suggests that women who experience partner violence may be more likely to use contraception, particularly forms of contraception that they themselves can control, rather than condoms. Two recent studies of women's contraceptive usage in India found that women who experienced IPV were more likely to report using “woman-controlled” spacing methods to prevent unwanted pregnancies, such as IUDs, rather than relying on condoms (Chen et al., 2020; Tomar et al., 2020). Reed et al. (2016) also note that women who experience IPV are more likely to report contraceptive usage that their husbands are not aware of, indicating that they may use contraception to undermine control exerted by abusive partners.
While a number of studies have examined the relationship between IPV and contraception usage, this study specifically examines the relationship between IPV and unmet need for contraception. By focusing on unmet need, this study aims to identify how different facets of IPV and gender inequality, including physical violence, sexual violence, coercive control, and limits to personal autonomy, influence Indian women's ability to control their fertility when they wish to prevent pregnancy.
Data and Methods
This study uses data from the 2015–2016 India Demographic and Health Survey (DHS). The DHS is a nationally representative, cross-sectional household-based survey of men and women between the ages of 15 and 49. The survey is administered by a trained interviewer in a one-on-one setting with individual adults in the household. The 2015–16 India DHS includes an extensive domestic violence module, which asks about different types of violence, control tactics, a woman's fear of her husband/partner, injuries caused by the violence, and help-seeking behavior. The domestic violence module was randomly given to one woman in each of the selected households; a total of 83,397 women were selected to complete the domestic violence module. Of those, 79,729 completed the domestic violence questions as part of their interview. The sample was further restricted to married women, as almost all childbearing and reproductive decisions in India are made within the context of marriage. A relatively small number of observations (<10%) were eliminated due to missing data on a key independent variable (coercive control) or dependent variable (unmet need), yielding an analytic sample of 64,395 observations.
Unmet need for contraception was operationalized using a variable for unmet need in the DHS, and was dummy coded with 1 indicating unmet need for spacing or unmet need for limiting, and 0 indicating no unmet need for contraception. Just over 13% of the sample were classified as currently experiencing unmet need for contraception, with a majority (n = 5489) stating that they want no more children and a sizeable minority (n = 2720) indicating that they want more children but do not want them in the next two years. The DHS draws on 15 survey questions to determine unmet need for contraception. First, respondents are categorized by whether or not they are using any method of contraception, either traditional or modern. Among nonusers, women who are pregnant or experiencing postpartum amenorrhea are classified as having unmet need if they report that their current or recent pregnancy was unintended. Women who are not using contraception and who are neither pregnant nor experiencing postpartum amenorrhea are further classified by whether they have the capacity to become pregnant (i.e., if they are fertile or infertile); fertile women in this group are then categorized as having an unmet need for contraception.
Physical violence: Six measures of physical violence were used to create the scaled physical violence score (α = .82). Items included in the physical violence scale match those included in the revised Conflict Tactics Scale (CTS2; Straus et al., 1996). Physical violence questions were asked with a frequency indicator: if a respondent replied that her husband/partner had perpetrated the type of violence in question, the respondent was then asked if their partner had perpetrated the violence (1) not in the last twelve months, (2) sometimes, or (3) often. Each question was coded on a scale of 0 to 3, and the scores of each question were summed to create a composite score for physical violence.
Coercive Control: Nine items were used to operationalize controlling behavior (α = .75). Measures of controlling behavior match items in the Psychological Maltreatment of Women Survey (Tolman, 1989) used in previous research to operationalize intimate terror violence (Johnson and Leone, 2005): (1) does your husband/partner get jealous when you talk to other men? (2) Does your husband/partner accuse you of being unfaithful? (3) Does your husband/partner not permit you to meet with female friends? (4) Does your husband/partner try to limit your contact with your family? (5) Does your husband/partner insist on knowing where you are? And (6) Does your partner trust you with money? These questions were answered as a binary (yes/no). The other three items capture emotionally abusive elements of coercive control: (1) Have you ever been humiliated by your husband/partner? (2) Have you ever been insulted or made to feel bad by your husband/partner? And (3) Have you ever been threatened with harm by your husband/partner? These items were asked in terms of frequency: never, not in the last 12 months, sometimes, or often. To keep coding consistent with the previous six items and not place additional weight on these items in the scale, responses were recoded as binaries with 0 for “never/not in past year” and 1 for “sometimes/often.” All nine items were then summed into a scale ranging from 0 to 9.
Sexual Violence: Sexual violence is captured using three items from the DHS: (1) Have you ever been physically forced into unwanted sex by your husband/partner? (2) Have you ever been forced into other unwanted sexual acts by your husband/partner? And (3) Have you ever been physically forced to perform sexual acts you didn’t want to? For each item, respondents reported if they had experienced the form of sexual violence “never,” “sometimes,” “often,” or “yes, but not in the past 12 months.” These items were assigned values from 0 (never/not in past year) to 2 (often) and summed to create a composite sexual violence score ranging from 0 to 6.
Movement Restrictions: Drawing on the literature on women's limitations in freedom of movement, a movement restriction score was calculated using three items from the DHS (α = .88). Respondents were asked if they were allowed to go to the market or the clinic, or to leave town (1) alone, (2) with someone else only, or (3) not at all. Responses were coded such that being permitted to travel without accompaniment was assigned a score of 0, being permitted to travel with someone else was assigned a score of 1, and not being permitted to travel to a given location was assigned a score of 2. Responses to these questions were summed in a scale ranging from 0 to 6.
Financial Autonomy: Three binary items were used to capture women's financial autonomy. These included (1) whether the woman was working outside the home, (2) whether the woman had a bank account she used, and (3) whether she had her own money that she alone could decide how to spend. These items did not work as a scale and were included in the model as individual measures.
Consistent with prior literature (Hardesty et al., 2015), K-means cluster analysis was used to identify a cut point to distinguish between high and low control cases. Cluster analysis is appropriate in modeling coercive control under Stark's (2007) and Johnson's (1995, 2001) conceptualization of coercive control as a constellation or collection of controlling behaviors within a relationship. Most studies that have used cluster analysis identify two-cluster solutions, encompassing relationships with high control and relationships with little to no controlling behavior (Hardesty et al. 2015; Leone 2011; Ornstein & Rickne, 2013). K-means cluster analysis indicated that a control score of 2 or higher constituted the “high control” group (n = 19,363). Cluster analysis was also used to identify a cut point to distinguish between high autonomy and low autonomy cases, with low autonomy cases having higher restricted autonomy scores. A cut point of 2 was identified.
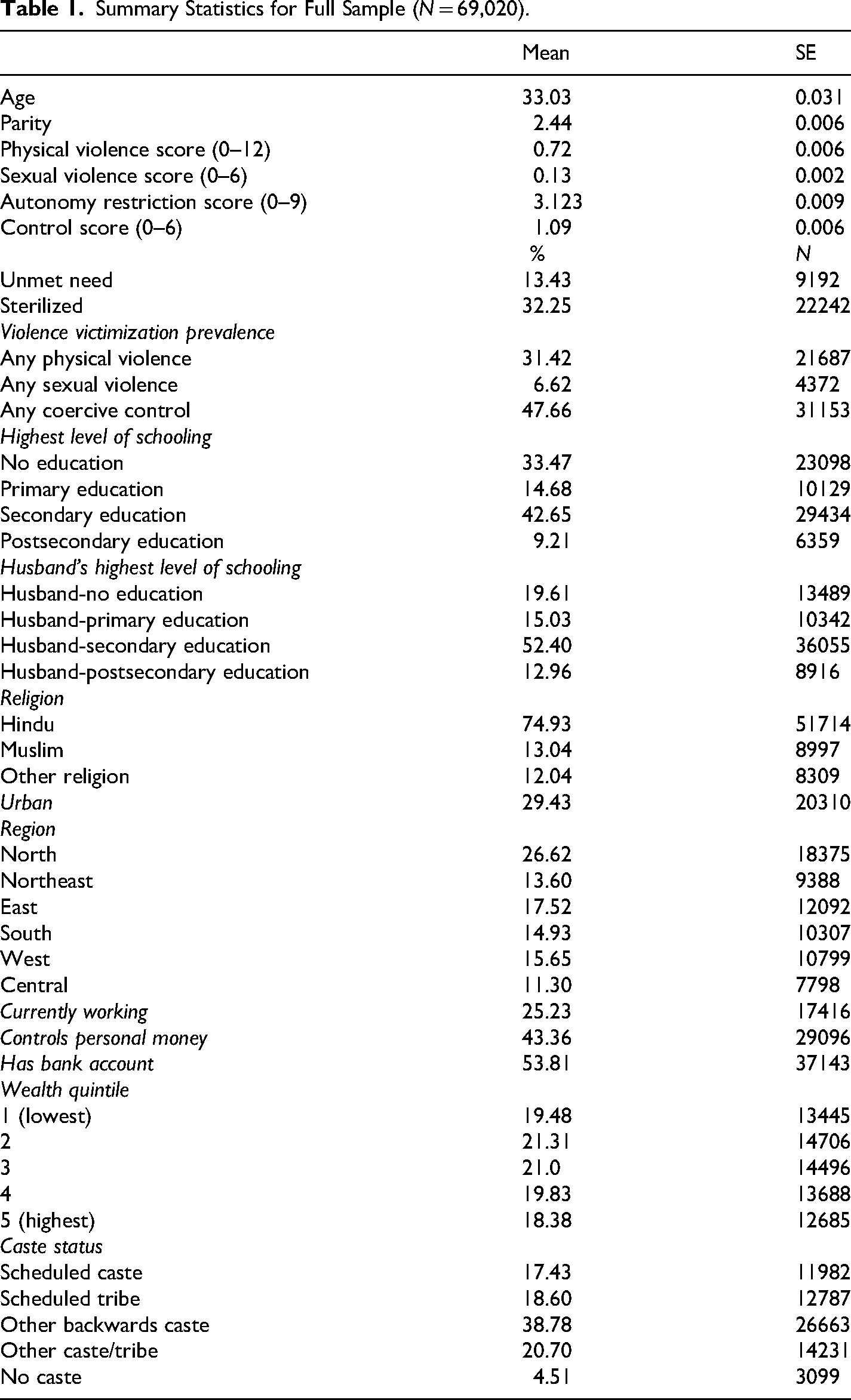
Covariates: Predictive models include several covariates representing key predictors of fertility behavior among Indian women and families. Covariates include the respondent's age, parity, highest level of education, husband/partner's highest level of education, urbanicity (urban/non-urban), employment status (working outside the home/not), religious affiliation, region of residence, and wealth quintile. Caste status was recorded using two measures from the DHS, the first of which asks if the respondent belongs to a caste/tribe and the second of which categorizes those who answered in the affirmative as belonging to a scheduled caste (historically marginalized lower-caste groups), scheduled tribe (indigenous communities or tribes), other backwards class (other socially disadvantaged groups not included in the previous categories), and “other caste” (individuals belonging to a caste/tribe that is not included in the other categories). Summary statistics can be found in Table 1, below. Descriptive statistics by contraceptive need can be found in Table 2.
Summary Statistics for Full Sample (N = 69,020).
Descriptive Statistics by Unmet Need for Contraception.
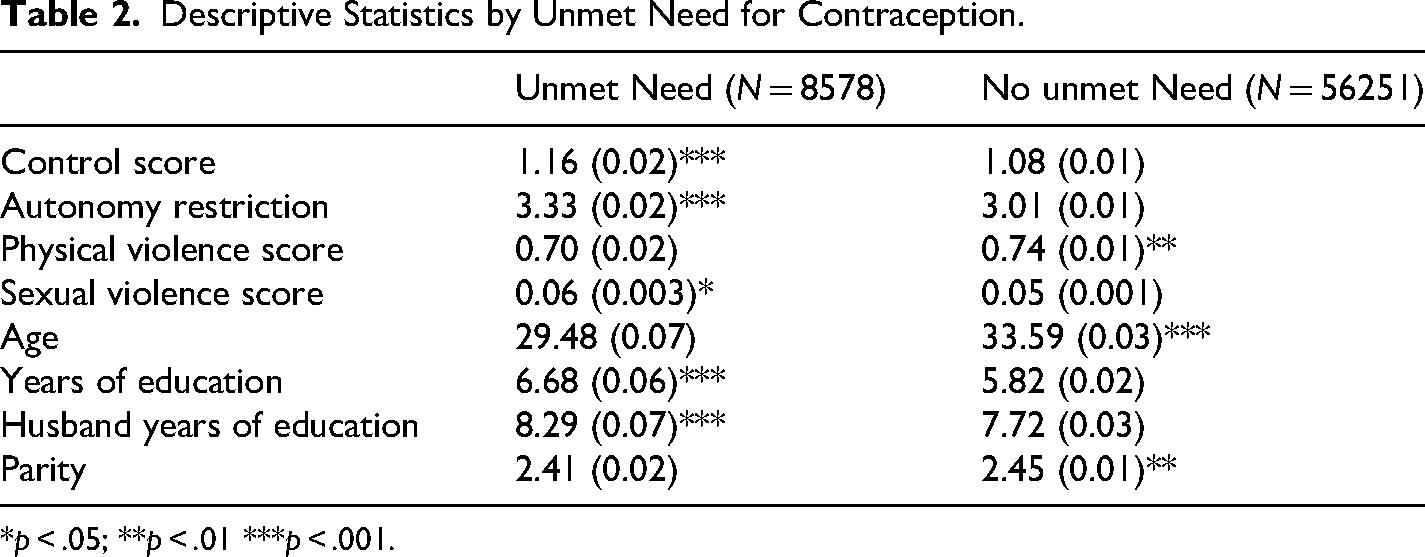
*p < .05; **p < .01 ***p < .001.
The mean age of respondents in the sample was approximately 33 years, and the mean parity was 2.44 children. 13.42% of women in the sample reported an unmet need for contraception for either spacing or limiting births. Spousal violence was commonly experienced by respondents, with 31.42% having ever experienced physical violence by their spouse/partner, 6.62% having experienced sexual violence by their spouse/partner, and 47.6% having reported at least one controlling behavior by their spouse. The mean physical violence score was 0.72, and the mean sexual violence score was 0.13. The mean control score was 1.09, reflecting the fact that the majority of women in the sample were not in highly controlling relationships. Completion of secondary school was the modal category for educational attainment for both women and their partners in the sample. Approximately one quarter of women in the sample were currently working outside the home. Roughly 75% of respondents identified as Hindu, 13% as Muslim, and 12% as members of other religious groups. Approximately three-quarters of respondents were recorded as belonging to a scheduled caste, scheduled tribe, or other backwards class.
There are distinct differences between the women who report experiencing an unmet need for contraception and those who do not. Women experiencing unmet need are, on average, younger, with younger husbands. They are also in more controlling relationships, with greater restrictions imposed upon their personal autonomy. As women in India are more likely to utilize sterilization once they have achieved their desired family size, it follows that older couples are less likely to experience an unmet need for contraception. Women without unmet need experience slightly more physical violence, which is in line with existing theorizing that women use contraception to subvert violence, or that men react to contraceptive usage with violence.
Analytic Approach
Analyses were performed using Stata 18. Descriptive analyses used t-tests and chi-square tests to identify statistically significant differences between groups. Predictive associations between violence, covariates, and unmet need for contraception were modeled using logistic regression. DHS-provided survey weights were applied to account for the two-stage clustered stratified sampling method utilized during data collection, including stratification by region and urbanicity.
Results
Descriptive Results
Initial analyses identified patterns of intimate partner violence occurring in Indian marriages based on the types of tactics used and the degree to which those tactics are used. Descriptive findings demonstrate that physical violence, coercive control, and limits to autonomy frequently co-occur in relationships, with individuals experiencing higher levels of control also experiencing higher levels of restricted autonomy and physical violence. Descriptive statistics by relationship type, as determined through the cluster analyses, can be found in Table 3. The “high control” group (N = 22131) accounted for 33.9% of the sample. The low free movement group (N = 32513) made up 47.1% of the sample. Approximately 17.5% of the sample fell into both the high control and low free movement categories.
Descriptive Statistics by Control and Movement Freedom Groups.
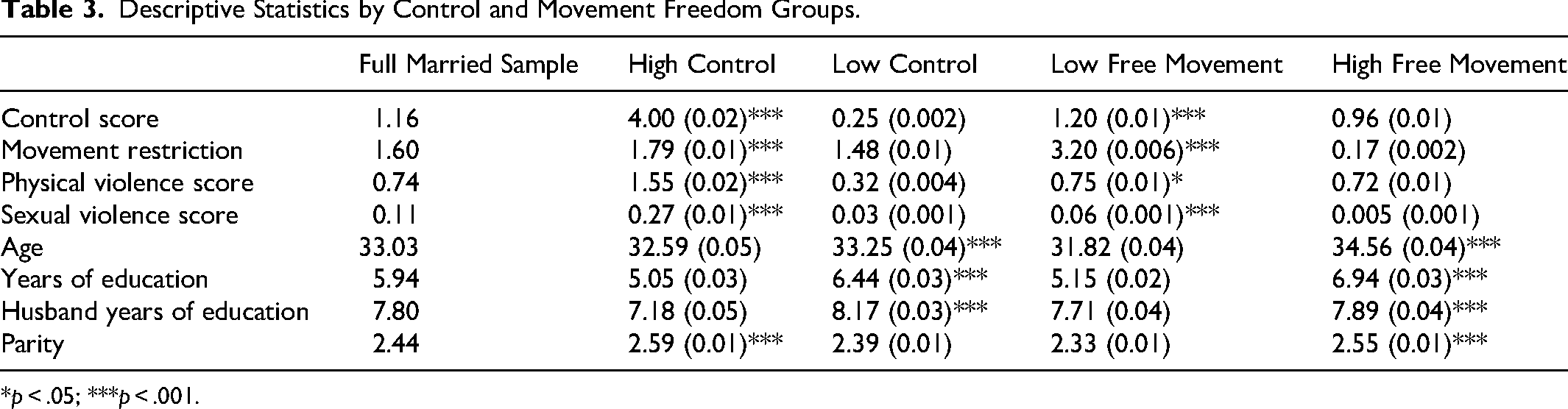
*p < .05; ***p < .001.
The high control and low control groups reflect qualitatively different experiences of women in India. Respondents experiencing high levels of controlling behavior from their husbands are, on average, younger and less educated, with husbands who have completed fewer years of education. They also experience, on average, significantly greater levels of physical violence and sexual violence, and significantly more limits to their personal autonomy, such as being unable to leave the home unaccompanied or not having access to financial resources.
Similarly, women who fall into the low autonomy group are younger and less educated, with a higher mean coercive control score. They experience, on average, slightly more physical and sexual violence than those in the higher autonomy group. The largest distinction between the low and high autonomy groups is their autonomy restriction scores, with the low autonomy group having a mean autonomy restriction score over four times higher than that of the other group.
The key differentiating factor in these types of relationships is the presence of high levels of controlling behavior. With the exception of the “high free movement” group, almost all women in the sample experienced some limits to personal autonomy; however, as seen in Figure 1 (above), the “high control” group also experienced significantly greater mean scores for across all types of violence and restriction, surpassed only on the movement restriction score by the “low free movement” group. The “low free movement” group also experienced comparatively higher levels of physical violence and coercive control compared to the “high free movement” and “low control” groups.
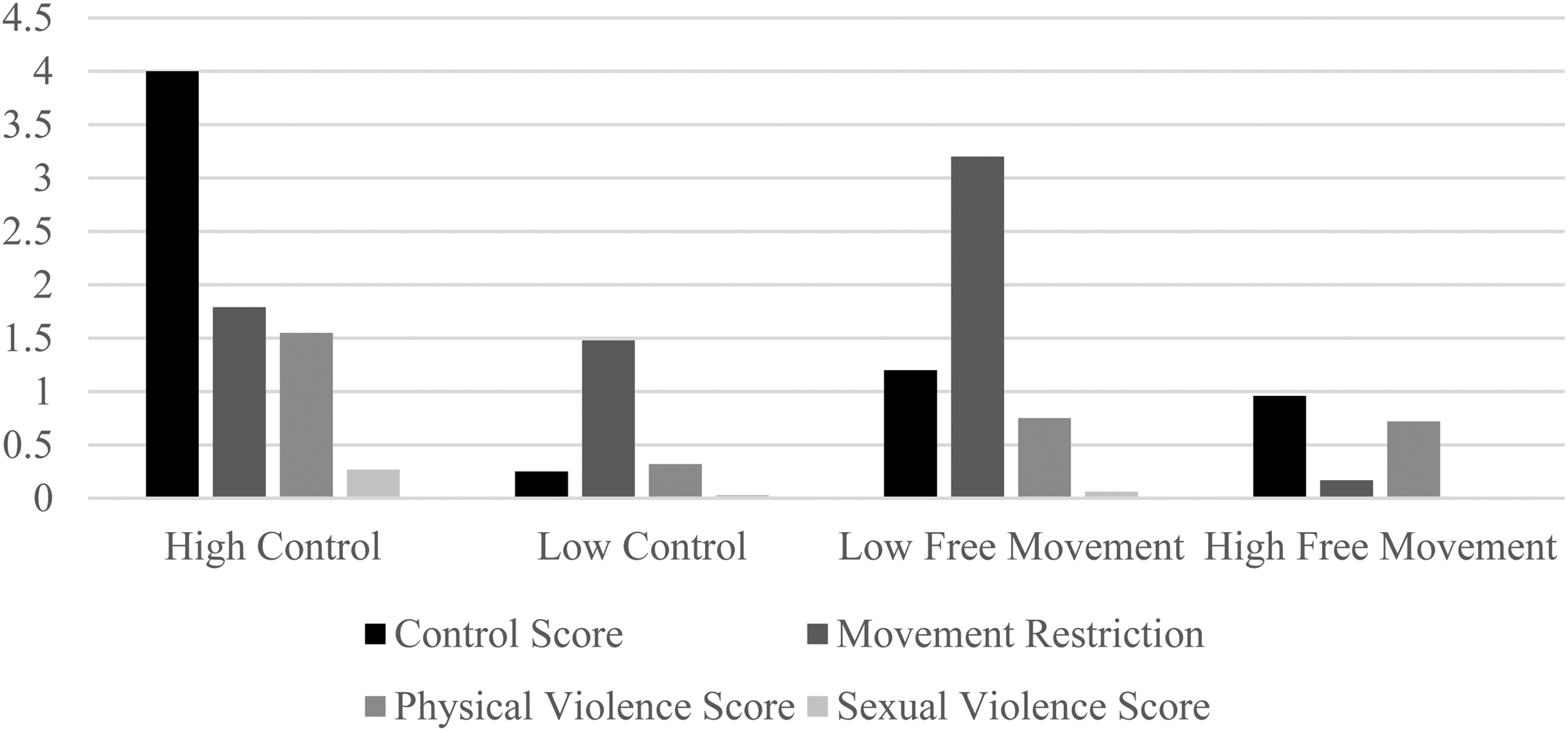
Violence Scores by Relationship Type.
Within the full analytic sample, the most common control item was jealousy, followed by distrust with money. No more than 25% of the full sample experienced any one control issue. Within the high control group, the most common control item was distrust with money, followed by a husband restricting the respondent from visiting with female friends, and the husband exhibiting jealous behavior. No less than 20% of the high control sample experienced any one controlling behavior item, although less than 20% reported being threatened or insulted by their husband/partner. As seen in Figure 1 and Table 3, members of the high control group experienced, on average, four of the included coercive control items.
Logistic Regression Results
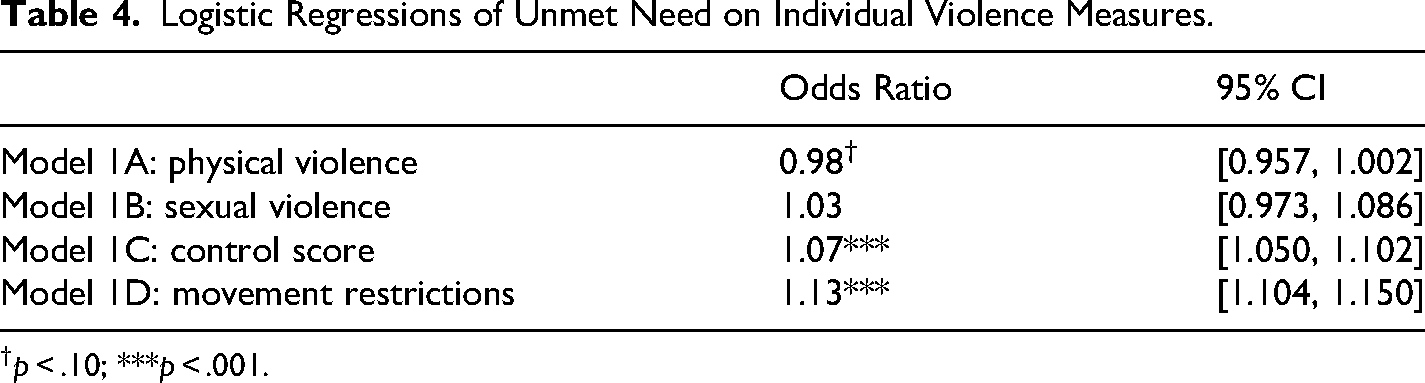
Logistic regression analyses were used to assess the relationship between aspects of intimate partner violence and unmet need for contraception. As seen in Table 4, Models 1A‒1D test the bivariate relationship between each aspect of violence and unmet need for contraception, with no controls.
As seen in Table 3, the association between physical violence and unmet need for contraception was only marginally significant (OR = 0.98, p < .10). Sexual violence had no significant association with an unmet need for contraception (OR = 1.03, p > .10). Both control (OR = 1.07, p < .001) and movement restrictions (OR = 1.13, p < .001) were found to significantly predict higher odds of experiencing unmet need.
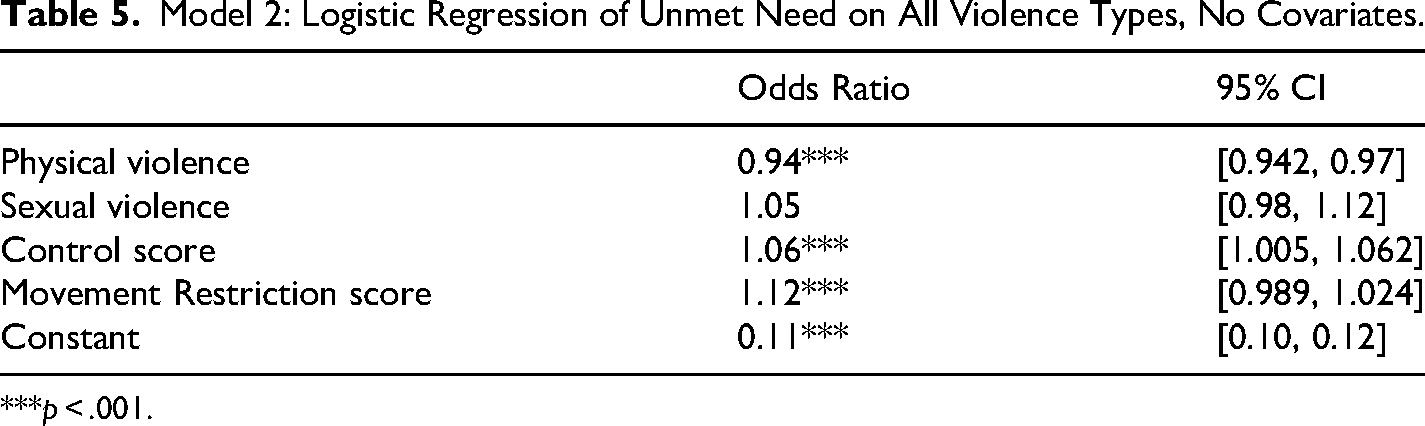
Table 5 shows the unadjusted model predicting unmet need using all four violence variables without covariates, Model 2. In this model, physical violence becomes significant, but in the direction of lowered odds of unmet need (OR = 0.95, p < .001); however, the effect size is relatively small, particularly when compared to the effects of control and movement restrictions, with which physical violence frequently co-occurs. The sexual violence score is not statistically significant (OR = 1.05, p > .10). When accounting for the other types of violence, movement restrictions (OR = 1.12, p < .001) and coercive control (OR = 1.08, p < .001) are found to significantly increase the odds of experiencing unmet need for contraception for each additional point on the scale.
Logistic Regressions of Unmet Need on Individual Violence Measures.
p < .10; ***p < .001.
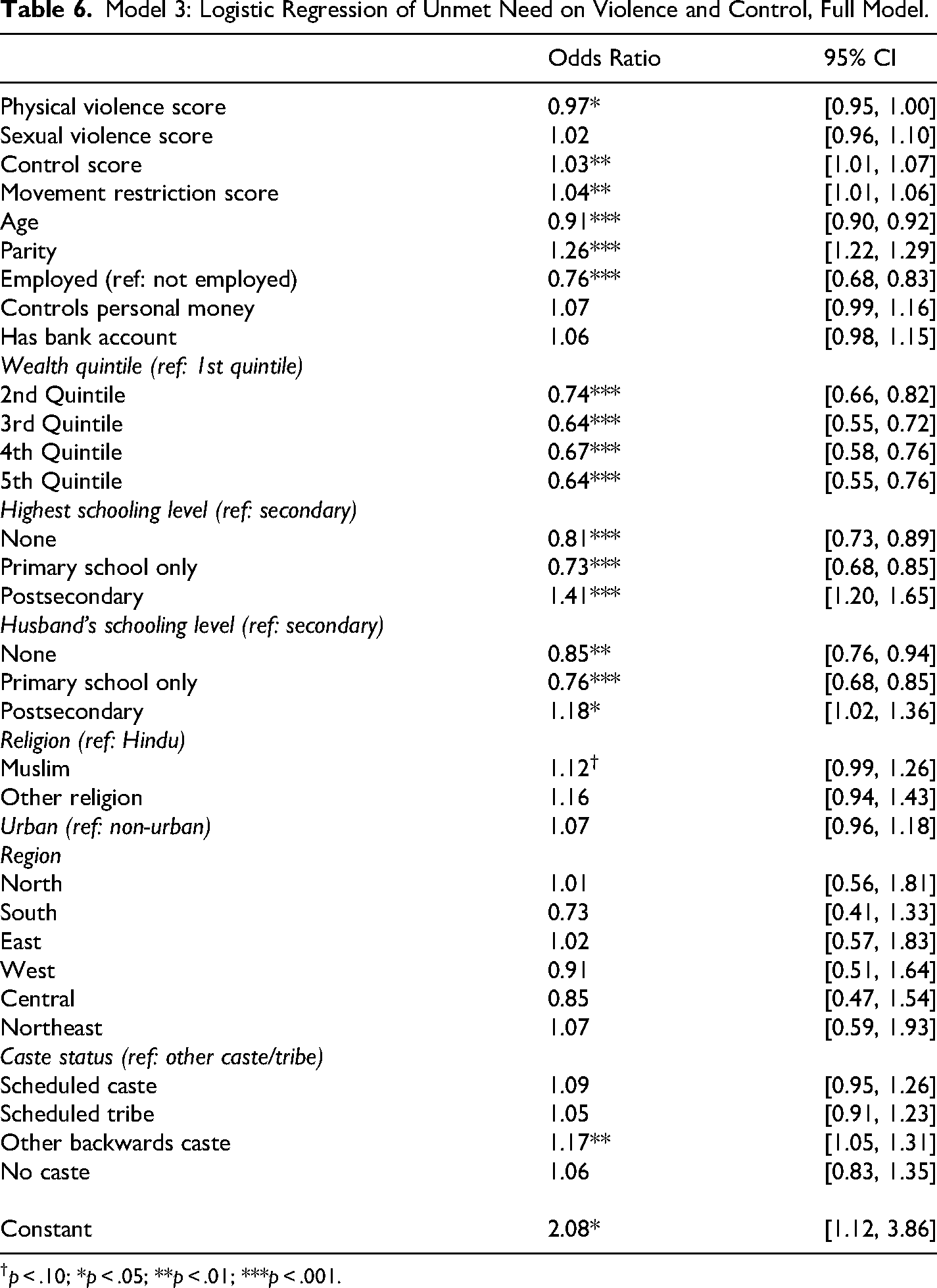
Table 6 contains the full model, including all four forms of intimate partner violence and autonomy limitations. This model also includes a range of variables commonly associated with intimate partner violence and unmet need for contraception. Results are displayed as adjusted odds ratios.
Model 2: Logistic Regression of Unmet Need on All Violence Types, No Covariates.
***p < .001.
Model 3: Logistic Regression of Unmet Need on Violence and Control, Full Model.
p < .10; *p < .05; **p < .01; ***p < .001.
Table 6 displays the results of Model 3, the full model inclusive of covariates. In Model 3, net of other factors, physical violence significantly predicts lower odds of unmet need for contraception (OR = 0.97, p < .05). In contrast, sexual violence (OR = 1.04, p > .10) is not found to be a significant predictor of unmet need. However, this model also finds that coercive control remains statistically significant net of other factors, though its effect size is reduced (OR = 1.03, p < .01). Because women in the high control group experience, on average, three control tactics, the cumulative effect is significant with regard to risk of experiencing unmet need among this group. Net of controls, restrictions on personal movement also remain a significant predictor of unmet need, but with a substantially smaller effect size (OR = 1.04, p < .01). A woman working outside the home was associated with significantly reduced odds of having unmet need for contraception (OR = 0.76, p < .001); however, the other measures of financial autonomy—having control of personal money and having a bank account—were not statistically significant.
Model 3 also identifies age and parity as significant predictors of unmet need for contraception. Age is highly significant (OR = 0.91, p < .001), with older women experiencing comparatively lower odds of experiencing unmet need. This may be due to an increased likelihood of having completed parity. Parity is also an important predictor (OR = 1.26, p < .001): women who have more children are much more likely to report unmet need for contraception, suggesting that they have potentially achieved their desired parity or are more inclined to delay any additional births.
Women with higher levels of education are more likely to experience unmet need for contraception, possibly due to differences in fertility preferences. Relative to Hindu women, Muslim women had higher odds of experiencing unmet need, but this association was only marginally significant (OR = 1.10, p < .10). Consistent with existing literature on social class and family formation behavior, the likelihood of experiencing unmet need decreases significantly as one move from the lowest to the highest wealth quintiles. No significant differences were found with regard to geographic region or urbanicity. Women belonging to “Other backwards classes” had significantly higher odds of unmet need (OR = 1.17, p < .01), compared to women in other castes.
As a sensitivity check, a second set of analyses was performed using only data from unsterilized respondents (N = 43,160). Results are largely consistent with those found in Models 2 and 3, albeit with reduced effect sizes and significance levels for both coercive control (OR = 1.03, p < .05) and movement restrictions (OR = 1.03, p < .05). Most notably, physical violence was no longer statistically significant when the sample was restricted to unsterilized women. Women's employment had a lower effect size (OR = 0.87, p < .01), and having a bank account became marginally significant (OR = 1.07, p < .10) in this model. In contrast to the full sample model, this model identified Muslim women as having lower relative odds of unmet need (OR = 0.85, p < .01) relative to Hindu women. The full results can be found in Table S7 in the supplemental materials.
Additional sensitivity checks were performed to look for potential moderation. Models were fit to identify whether physical violence was significant in the context of high control or low autonomy; the same check was performed for sexual violence. No significant results were found to suggest that any form of violence becomes significant or more significant in the context of high control or low autonomy, such that evidence of moderation effects by coercive control or autonomy restrictions was not found. The results of these models can be viewed upon request.
Discussion
This study reflects that intimate partner violence is a complex experience, and different aspects of violent relationships impact women in different ways. Prior studies examining the relationship between intimate partner violence and unmet need for contraception focused on the impact of physical and/or sexual violence. This paper adds to our theoretical and empirical understanding by demonstrating that, even when accounting for physical and sexual violence, coercive control and restrictions imposed on personal movement are significantly associated with an increase in women's risk of experiencing unmet need for contraception.
This study does not discount the relevance of physical violence in predicting unmet need for contraception. The full sample model with covariates finds that physical violence is associated with reduced odds of having an unmet need; this may support the hypothesis that women in violent relationships take steps to limit their fertility as a way to undermine their partners’ control. Alternatively, this may reflect the fact that physical violence may be a response by husbands to wives’ contraceptive use.
The presence of control issues in intimate relationships, particularly within violent relationships, is not uncommon. As discussed, approximately one-third of the sample falls into the “high control” category, experiencing, on average, four control tactics by their partners. Findings in this study are consistent with an intimate terrorism model of intimate partner violence, in which one partner uses controlling behavior to exert power over the other, including over their reproductive decisions. While men may use physical violence to exert control over their wives, they may also employ nonviolent tactics, such as limiting access to social support networks or engaging in jealous behaviors, which may frighten wives, in order to maintain power within their marriages. Although the DHS does not ask about reproductive control behaviors, such as condom refusal or engagement in contraceptive sabotage, it is possible that such behaviors are also practiced by coercive controlling abusers; future research should examine this possibility more explicitly.
Women's desires to space or limit pregnancies may be of particular concern in situations in which their husbands want more children (Forrest et al., 2017). A desire not to have children, or to have fewer children, may be interpreted as a threat to men's dominance in the family, or at the very least, a challenge to an expected power dynamic. This may in turn be associated with additional violence, as men with particularly entrenched patriarchal gender ideologies may be more likely to respond to perceived challenges to their authority with physical aggression and/or control tactics. At the same time, living with a violent partner may lead some women to desire smaller families, particularly in light of increases in physical violence during pregnancy in many abusive marriages (Mahapatro et al., 2011). Women may express an unmet need for contraception due to a desire to limit future pregnancies in response to abuse, a theoretical complication worthy of exploration. Because the Demographic and Health Survey is cross-sectional, this study could not examine whether disagreements over family planning preceded intimate partner violence, or whether women's fertility preferences may shift in response to living with a violent husband.
Controlling behaviors from husbands are not the only non-violent tactics that influence women's reproductive autonomy. Limits to personal autonomy also play a role in a woman's ability to enact her reproductive preferences, particularly with regard to freedom of movement. While autonomy restrictions are a component of violent relationships, Figure 1 illustrates that women in relationships where they experience significant limits to freedom of movement may not necessarily experience high levels of physical violence. The mechanisms driving the relationship between autonomy and unmet need for contraception may therefore be different. However, the fact that women in high control, intimate terror relationships experience elevated levels of autonomy restriction, and the fact that limited freedom of movement independently influences the risk of experiencing unmet need, suggests that limits to women's autonomy may be used by abusers to maintain control. These are tactics which can be imposed and enforced not only by spouses, but by in-laws as well, which may be of particular importance in the patrilocal context of Indian society.
While this study models unmet need for contraception as it is reported by individual women, unmet need is best understood as a population-level indicator. India has maintained high levels of unmet need for contraception, which has historically co-occurred along with a high prevalence of intimate partner violence. While new laws enacted in the past few decades have sought to decrease violence against wives in India, beginning with the 2005 Protection of Women from Domestic Violence Act, enforcement of domestic violence laws is challenging across legal contexts. Marriage is considered a private matter, and women report that they feel deterred from reporting violence to the police or seeking help from community organizations (Ragavan et al., 2015; Shirwadkar 2009). Even when abusers are prosecuted for acts of physical or sexual violence, coercive control is much more difficult to ban or protect against; numerous countries around the world have debated various approaches to dealing with the problem of so-called non-violent abuse (Cross, 2022), and many women remain without legal recourse for non-violent controlling behaviors. An important implication of the current study is that these non-violent aspects of abuse remain common and consequential for India's women, and that addressing high levels of unmet need for contraception may require interventions that address coercive control and restrictions placed on women's freedom of movement.
This study has several limitations. As previously mentioned, because it is cross-sectional in nature, the DHS cannot be used to track how changes in relationship dynamics and contraceptive needs may interact over time as couples have children, experience changes in fertility desires, and move towards a desired parity. Older women within the sample experience less coercive control, but more physical violence, and are less likely to experience unmet need for contraception, having undergone sterilization after achieving a desired number of children. Second, because some women selected for the intimate partner violence module were unable to complete it due to privacy concerns, and because some women who participated in the module did not answer questions about coercive control, it is possible that the implications of controlling behavior are underestimated in this study. Third, the use of scales in these analyses may obfuscate the roles of specific elements in predicting unmet need for contraception.
Despite these limitations, this study provides evidence that coercive control and limits to personal autonomy play unique roles in shaping women's risk of experiencing unmet need for contraception in India, even when controlling for physical violence. Researchers concerned with how couple dynamics influence reproductive decision-making and reproductive autonomy should consider how these non-violent aspects of violent relationships contribute to women's outcomes. Future research should examine how coercive control manifests itself in other contexts, and how the use of coercive control and imposed restrictions on women's autonomy shape reproductive and other health behaviors and outcomes.
Supplemental Material
sj-docx-1-vaw-10.1177_10778012251384630 - Supplemental material for Marital Dynamics, Physical and Non-Physical Violence, and Indian Women's Reproductive Control
Supplemental material, sj-docx-1-vaw-10.1177_10778012251384630 for Marital Dynamics, Physical and Non-Physical Violence, and Indian Women's Reproductive Control by Randi Saunders in Violence Against Women
Footnotes
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (grant number P2CHD042849).
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biography
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.