
Abstract
This qualitative research amplifies the voices of Jewish and Arab women in Israel, illuminating their experiences with obstetric violence, its consequences, and coping strategies. The premise of this study is the feminist approach that aims to eradicate phenomena related to gender and patriarchal structures affecting women, their bodies, and their health. The research was based on the qualitative-constructivist methodology, by means of thematic analysis of 20 in-depth semistructured interviews. Two main themes emerged: first, consequences (e.g., physical, emotional, spousal relationships, and mistrust) and second, women's coping strategies (e.g., repression, avoidance, garnering inner strengths, resilience, and relying on external help).
Keywords
Obstetric violence (OV) is a global problem, typically a form of gender violence that exists within a wider discourse of structured violence and includes inequality, a patriarchal approach, discrimination, and lack of access to equality and women's human rights (Šimonović, 2019). It is more commonly encountered by women of minority groups particularly during hospital births, and among individuals facing social, economic, or health-related challenges (Perrote et al., 2020; Vedam, 2019).
OV refers to abuse, dehumanized care, disrespect, and mistreatment of women (Bohren et al., 2015). OV might occur through the full continuum of fertility treatments to childbearing, and it is a sex specific form of violence against women and a violation of human rights (Garcia, 2020).
Among expressions of disrespect and abuse toward women, one can note deliberate physical violence, unintentional passive violence (such as neglect due to understaffing or overload), verbal violence, and inadequate health system conditions that harm privacy and confidentiality (Bohren et al., 2015).
It is worth mentioning that raising the awareness of the term “OV,” which involves both structural and interpersonal gender-based abuse, means contributing to the ongoing awareness of violence against women rather than blaming health care providers (Mena-Tudela et al., 2023).
Whereas the research literature focuses mainly on attempts to understand the roots of the problem, few studies have assessed the implications of OV to women's and their children's health, and how they cope (Hill & Castañed, 2022; Silveira et al., 2019).
Consequences of OV
The literature indicates a direct relationship between women's perception of OV as traumatic and the severity of long- and short-term emotional, physical, interpersonal, and social consequences.
On the emotional level, women who had experienced OV reported feelings of oppression, denial of self, and emotional infantilization (Shabot, 2016), loss of self-confidence in their ability to care for their child (Perrotte et al., 2020), depression and tension in their spousal and family relationships (Acharya et al., 2021), negative feelings toward their child (a sense of detachment, inability to feel affection or love), and even alienation (Nicholls & Ayers, 2007). The mother's negative feelings toward her newborn are often transferred to other children in the family and are manifested in an attempt to minimize physical contact with them (Beck, 2015; Elmir et al., 2010; Nicholls & Ayers, 2007).
Also, it has been observed that the rate of posttraumatic stress disorder (PTSD) following childbirth, was found to be related to the increase of OV. For instance, cross-sectional research conducted in Spain, encompassing postpartum women whose deliveries had occurred within the preceding 12 months, demonstrated that the emergence of PTSD was correlated with cases of professional noncompliance with the birth plan and a lack of respect. Furthermore, verbal and psychoaffective OV exhibited associations with the onset of PTSD, and verbal abuse was identified as the most influential factor in predisposing individuals to the development of this disorder (Martinez-Vázquez et al., 2022).
Research carried out in Brazil revealed that individuals undergoing OV exhibited a higher propensity to disclose postpartum depression (PPD) 3 months after childbirth compared to their counterparts (Silveira et al., 2019).
The incidence of perceived OV within a cohort of Italian women was notably elevated, particularly among younger and less educated participants, individuals who had not participated in a prenatal childbirth preparedness course, and those who underwent natural childbirth. Moreover, the study identified that the occurrence of abuse and violence during childbirth heightened the probability of subsequently reported adverse mental health outcomes (Scandurra et al., 2021).
In a study of the consequences of OV in the United States, Beck (2015) pointed to another significant phenomenon—ambivalence about motherhood, which manifested in harsh feelings of mechanism, detachment, faked feelings, anger, and shame.
Since society perceives shame and pain as inherent to the birth-giving experience, many women do not receive recognition from their close community and thus feel silenced and barred from sharing their feelings and the consequences of OV (Shabot & Korem, 2018). When a woman becomes a mother, the gendered shame that she had previously felt is connected to her role as a mother. This sense of maternal shame, according to Shabot and Korem (2018), prevents many women from receiving recognition of the harsh experiences and emotional consequences of OV.
On the physical level, violence and OV are directly related to traumatic deliveries as perceived by women (Fernández, 2013). The physical trauma is manifested in women's reports of injuries, inflammations, and pain (Acharya et al., 2021).
On the behavioral level, research has indicated that many women feel trapped for years in the experiences and memories of their traumatic delivery and OV (Ayers, 2004; Van der Pijl et al., 2020). This affected their behavior patterns including flashbacks that affected their reality and day-to-day functioning (Ayers, 2007).
Women's traumatic experiences of OV have a detrimental effect on their spousal relationship, especially when their partner did not comprehend the scope of the injury or was not considerate enough of their needs. Studies have shown that many women were angry with their partners for not supporting them enough, or not preventing the violence in the delivery room (Henriksen et al., 2017). Another complex coping for women was sexual intimacy, which served as a constant reminder of the OV, and often led to avoidance of sexual intimacy (Morris et al., 2023). The fear of becoming pregnant again was also described as a significant factor (Shorey et al., 2018).
From the social aspect, women reported that the stress of the traumatic delivery increased their sense of social isolation. Women's traumatic childbirth experiences were linked to not enjoying motherhood. Therefore, women felt lonely when they met other women who had not experienced birth trauma, and were enjoying their motherhood. In addition, they found it hard to share the OV trauma with other mothers or friends and felt there was no channel to communicate their experiences (Moyzakitis, 2004).
Following incidences of OV from medical teams, many women's trust in the institutional healthcare system was significantly damaged and affected their decision to choose a biomedical framework for their next delivery. When women wanted to get pregnant again, they found it hard to trust midwives, counselors, and other medical staff in the hospital, who would treat them in their next pregnancy and childbirth (Fenech & Thomson, 2014; Greenfield et al., 2022). Many women mentioned that they would choose public delivery rooms as their last resort, and others stated that they would prefer traditional home births (with a doula or other community practices) and without medical interference—to avoid any reencounter with the medical system that was perceived as abusive (Bohren et al., 2015; Espinoza-Reyes & Solís, 2020).
Coping Strategies With the Consequences of OV
The literature relating to women's coping with OV is still sparse. The few studies that have addressed this issue describe varied practices—from knowledge and awareness of childbirth processes to locating support systems in the family and on social networks. Espinoza-Reyes and Solís (2020) emphasized that the fact that women were victims of OV did not mean that they remained passive or accepting or reproduced hegemonic obstetrical practices. Rather, they have the ability to resist and undermine these practices. Women's individual agency allows them to deal with OV through use of various creative resistance tactics. For example, to reduce the high levels of stress they were feeling, women tried to embrace positive thoughts that focused on their newborn and avoided thinking about the traumatic events. Others, on the contrary, chose to dwell on past events as a way to deal with the pain (Allen, 1998). Concrete actions were also taken. They searched for information about the traumatic experience from their partners and midwives, looked for support sources, and returned to their previous job, which they knew would distract them from stress and thoughts (Allen, 1998). To cope with the implications of obstetric abuse to their relationship with their infant, women invested a great deal of emotional and mental efforts to reinforce the bond between them, and to overcome the sense of detachment (Elmir et al., 2010). Another tactic involves discussions with physicians to coordinate expectations regarding childbirth at the early stages of pregnancy, and to establish trust and closeness. They viewed their medical file from the previous delivery to analyze it and reach decisions about the future birth, and to maximize and regain control (Greenfield et al., 2022).
Formal support systems (women's partners) and informal support systems (social media) play a crucial role in women's ability to cope with the harsh experiences of obstetric abuse. It has been shown that spousal support and early breastfeeding of the infant are two protective factors against the development of PTSD that is rooted in OV (Martinez-Vázquez et al., 2021). Regarding informal support systems, in recent years, women have been sharing their intimate childbirth experiences on social media, including reports of OV. In Israel, reports have appeared on Facebook pages such as “active childbirth,” “natural childbirth,” and “homebirth.” Although the difficult stories were usually posted in closed groups, and most did not reach the mainstream media, they still provided support to mistreated women, or warned about medical teams that could potentially be abusive (Leinhart, 2019). Social networks also served as a safe space for abused women, as revealed in a study by Espinoza-Reyes and Solís (2020), who noted the resistance strategies on social media of women who had suffered OV in Mexico—designated support groups for women to tell their stories in a safe environment.
Maternal Healthcare in Israel Within a Multicultural Society
Israel records a high annual childbirth rate, surpassing all organization for economic cooperation and development nations. The majority of these births occur in the country's 27 public or semiprivate hospitals. While national healthcare laws guarantee comprehensive birth-related care, women can choose their labor hospital but lack familiarity with staff and have limited options for specific health providers. Despite proven benefits, there is no comprehensive system for consistent care from the same healthcare providers throughout the entire birthing process, except for home births. The Ministry of Health (MoH) strictly regulates out-of-hospital births, imposing guidelines for home births, banning freestanding birth centers, and providing no financial support or insurance for home birth midwives (Leinhart, 2019).
The Israeli healthcare system adeptly plans and delivers care and support services within a multicultural society (Halperin et al., 2015). In this study, the authors focused on Israeli women from two different culture societies: Jews and Arabs.
According to the Israeli Central Bureau of Statistics (CBS) data (published on January 3, 2024), Israel's population was estimated at 9,842,000 residents: 7,208,000 Jews (73.2% of the total population), 2,080,000 Arabs (21.1%), and 554,000 others (5.7%) (Central Bureau of Statistics, 2024).
Both Israeli Jewish and Arab women hold Israeli citizenship, residency, and access to the national medical system. Maternity ward staff, particularly in the North, comprises a blend of Arab and Jewish midwives and doctors, ensuring equitable treatment (Halperin et al., 2015). However, there are studies indicating that despite uniform healthcare coverage, ethnic inequalities in health persist between Arab and Jewish populations (Daoud et al., 2018). Regarding maternal care, Arab Israeli women use fewer perinatal resources and report more birth trauma than Jewish Israeli women (Halperin et al., 2014).
In light of the above literature, and the sparsity of studies that have investigated the consequences of OV and women's coping strategies, the present study aimed to expand the knowledge on this issue. Also, this qualitative research aimed to give voice to Jewish and Arab women in Israel, who had suffered OV, to learn about its consequences to them over time, and to learn how they coped on various levels from a personal perspective—a subject that has not been studied in Israel so far. This study is rooted in the feminist approach that aims to raise awareness and to eradicate phenomena related to cultural, patriarchal, and gender-related structures (Sharma, 2019). Gender structures consist of gender inequality that discriminates against women's activities, experiences, choices, and values (Mayra, 2021).
Methodology
Based on Strauss and Corbin’s (1990) grounded theory design, this study employed a constructivist-qualitative methodology in an attempt to understand the meanings that women affected by OV attributed to their experiences, and their perceptions and explanations of this violence. This approach clarifies the interviewees’ reference framework, and how it is experienced by understanding their world from their perspective (Taylor & Bogdan, 1998). Grounded theory allows researchers to focus on the significance that the interviewees attribute to their own experiences, and to present a consolidated analysis that is as close as possible to these experiences (Charmaz, 2006). This approach is suitable to the theme and goals of the current study.
Participants
Twenty semistructured in-depth interviews were conducted with 10 Arab women and 10 Jewish women in Israel, who had given birth during the previous 7 years. Semistructured in-depth interviews are characterized by flexibility and dynamism (Taylor & Bogdan, 1998), aimed at learning about situations that cannot be observed directly (Creswell, 1998).
We used a purposeful sampling method (Bryman, 1988), which is characterized by a focused effort to achieve variance among the interviewees; accordingly, the ages of the participants (25–50; M = 35.5), education (at least a Bachelor's degree), religion (10 Jewish, five Muslim, and five Christian), employment, residence area, and number of children (1–3). See Table 1 for full demographic details.
Background Characteristics of the Participants.
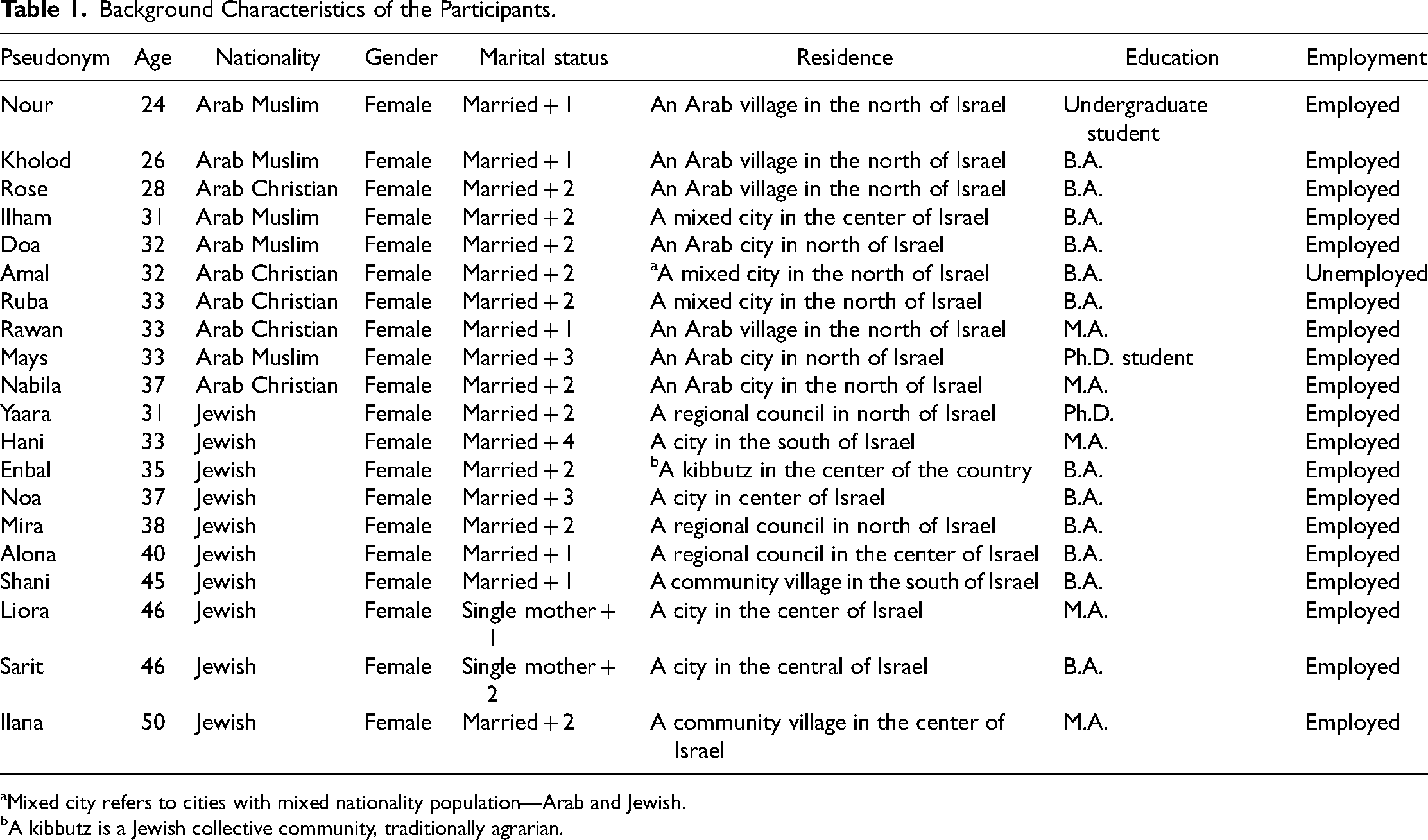
Mixed city refers to cities with mixed nationality population—Arab and Jewish.
A kibbutz is a Jewish collective community, traditionally agrarian.
Procedure
Data Collection
A message posted on various social media in Hebrew and Arabic was sent out to recruit participants. Thirty women responded, expressed their willingness to participate, and said that it was important to them to share their experiences. Initial contact was made by telephone including a detailed explanation about the study. An explanatory page about the research and its goals was also sent. The final 20 participants were chosen based on their willingness to participate in the research, after openly agreeing to be interviewed and tell their story, sampled through convenience sampling. An informed consent form was signed by all the respondents.
The interviews were conducted in the participants’ native language, whether Arabic or Hebrew, by a research assistant who is a social worker and speaks both languages. The interviews were held between August and October 2020 and were recorded and transcribed. Due to coronavirus disease 2019 restrictions, 17 of the interviews were held on Zoom. Each interview lasted between 1 h and 2 h, and the respondents were assured anonymity and full confidentiality. Pseudonyms were used for all participants.
The questions that the participants answered allowed them to openly relate to their pregnancy and childbirth experiences, the consequences of the abuse on various levels, and how they coped—all from their personal perspective.
The interviews included background and sociodemographic questions (age, ethnicity, marital status, etc.) and open-ended questions such as: (a) Tell us about your pregnancy and birth experience. Please elaborate on the follow-up, treatment, and birth experience vis-à-vis the medical staff. (b) How would you define your experience of abuse during pregnancy and childbirth? (c) How did the abuse you experienced affect you on various levels—emotional, physical, functional, cognitive, or other? (d) How did you deal with the abuse? Did you share this experience? Did you seek help? (e) What helped you cope with this experience? (f) What are your recommendations for women and healthcare professionals?
The research was approved by the college's ethics committee on July 16, 2020 (research number: 2020-60, L/SW).
Data Analysis and Trustworthiness
The data were coded after all the interviews had been completed. Through data analysis of the interviews, content and meaning of patterns were constructed. Content similarities and differences were identified, as well as patterns, themes, and continuity, following the six analysis stages specified by Braun and Clarke (2006): familiarizing with the data (transcription and active reading); generating initial codes (organizing codes into meaningful groups); extracting themes (sorting codes into potential themes); reviewing themes (rereading themes and examining coherence and validity of the encoded data); defining and naming themes (extracting the essence of the story in each theme); producing the report (findings, citations, and the meaning of the themes).
The analysis was conducted by both authors. First, the author who is fluent in both Arabic and Hebrew read all the interviews, and the author who speaks only Hebrew reviewed the Hebrew interviews. Next, after the key themes and appropriate citations were extracted and agreed upon, they were translated into English.
The respondents of this study differed demographically (age, residency, etc.), but after analyzing the first 10 interviews, we found that repeated themes were extracted. At this stage, we had identified two themes, some of which included subthemes. After analyzing 15 interviews, it was obvious that the women's descriptions, experiences, and interpretations reinforced the two themes. At the twentieth interview, we stopped the analysis in view of the repetition of the content and interpretations—which signified saturation of the research topic. The authors made an effort to adhere to the standards suggested by Franklin and Balan (2005)—credibility, transferability, dependability, and conformability.
The two main themes that emerged from the data analysis concern the consequences of OV to the women who were subjected to it, and their coping strategies on various levels.
The Researchers’ Premise
As researchers and professionals in the fields of nursing and social work, who espouse the feminism critical theory, we have based this study on the premise of that perception. The research is the outcome the two researchers sharing their personal experiences of OV with each other. Researchers’ personal revelations have advantages and shortcomings. In this case, the advantage is close acquaintance with and understanding of the research population, and accessibility to the field (Patton, 1990). The shortcoming is that there might be preconceptions and a judgmental attitude toward the researched phenomenon (Shkedi, 2011). During data analysis and processing, the researchers discussed their evaluation of the findings and data processing, and somewhat managed to reach an inside/outside stance (Hesse-Biber & Piatelli, 2007). The reflection process, their awareness of their different ethnicity, and their personal identification with the subject, alongside their determination to raise the issue to the consciousness of healthcare professionals and policymakers in Israel—allowed adhering to the ethical and research standards required in qualitative research (Franklin & Balan, 2005).
Results
The women who participated in the present study reported various types of OV including verbal violence, objectification, treating the woman as invisible, and performing invasive examinations without informed consent. The focus was on the consequences and coping strategies as the women perceived and described them. The first theme—consequences—includes physical and emotional consequences, damaged spousal relationships, and mistrust of the healthcare system and service providers. The second theme—coping strategies—includes repression and avoidance as a way of dealing with the pain and trauma; garnering inner strengths, resilience, knowledge, and awareness of the childbirth process; relying on external support; sharing on social media and with other women who had experienced OV; and reaching out to therapists/legal aid/public complaints.
Consequences
Physical Consequences
Women described pain that did not subside for a long time after delivery, which stemmed from invasive examinations, an episiotomy procedure, and stiches in the perineal area, usually performed without the woman's consent. These pains affected the woman's ability to function physically, have sex for months after, a weakened pelvic floor, urinary incontinence, increased fatigue, and difficulties caring for the newborn child. They also shared that low availability of clinic appointments delayed their recovery, for instance for removing caesarean stitches. All these affected not only their day-to-day functioning but their body image as well. It affected me very badly. First of all, it hurt a lot. I remember myself six months later with pain from the scar… They [the medical staff] did me some harm there… (Mira) There was a lot of pain, ……I couldn’t sit or go to the bathroom, I couldn’t hold myself. This was after stitches …. I can’t stand near the sink for more than half an hour, and I still feel the laceration exactly… I’m telling you this after nine years… I still feel there's something missing in my body, and what was done to my body at birth, it's like there's something which isn’t perfect. I keep telling my husband… something happened to my body… (Mays)
Emotional Consequences
Following childbirth and the violence they had experienced, the women's physical and emotional condition often prevented forming the initial relationship with and care for their infant. Women stated that the medical teams’ top priority was to perform postdelivery examinations, instead of being available for support to help the woman's relationship with her child.
Shani described how she could not sit or walk after the Caesarean section and was in recovery. She badly wanted to see her baby and touch it, but the medical staff did not cooperate because they were busy with other things and could not fetch the baby. That kept her awake, and she was sad and troubled all night. Naturally, I couldn’t walk or sit. I managed to eat a little, and then they took me to the department. When I asked where my baby was, they said he was in the nursery. I said I wanted to see him, and they said I couldn’t because I had had epidural anesthesia. I asked when I could see him; they said “in the morning, recover, we have other things to do”… I couldn’t sleep all night, I was sad… (Shani)
Moreover, the staff often stood in the way, because they denied the mother's holding or breastfeeding the newborn, and even answered aggressively or impatiently when they were asked for help. This situation created a sense of vulnerability and isolation. One night, I tried to breastfeed her, but had a hard time because my nipples were sore and hurting… At some stage, I cried, which is natural and hormonal, and I was in pain and couldn’t breastfeed my daughter… The nurse started shouting at me, “Stop crying, you’re passing it on to the baby”… Obviously, that only added to the difficulty… (Hani)
Some of the participants described their immediate emotions as falling in love with their infant and euphoria, yet perceived the situation as fraught with fear, chaos, relief that the delivery was over, and a flurry of emotions that harmed the initial relationship with the baby. Women reported a variety of emotions that stemmed from the traumatic experience and how the medical staff had treated them and their body including sadness, depression, constant crying, anger, guilt, anxiety, and overprotectiveness of the infant. I recently had psychotherapy… I think that after my second childbirth, I suffered from postpartum depression… for a year after… I realized something was wrong, I can’t say exactly what… [and she went on to describe the medical staff's attitude, and how uncomfortable and vulnerable it had made her feel]. (Inbal) …I keep remembering this childbirth, and I would cry for a long time. In the beginning, people used to ask me “how was your delivery”… and, you know, I had tears and I would be really upset… The difficultly of the childbirth accompanied me for a long time…I know I will get over it, but I don’t know when, and I don’t know how long it will take… (Rawan)
Consequences to the Spousal Relationship
Women reported that the abusive delivery experience deeply affected their spousal relationship: anxiety and fear of becoming pregnant again, distancing herself and avoiding sexual intimacy, severe pain during sex due to damage caused during childbirth, and oversensitivity. The experience was traumatic to any extent… I preferred that my husband stays in a room and I stay in a different room, so a pregnancy can’t happen… (Nabila) A bad outcome that happened was that I started having painful sex. (Doa)
Mistrust of the Healthcare System and Service Providers
Trust in the healthcare system and medical staff is significant to women's sense of security. However, not all the women felt that the system was on their side, but that it operated from other considerations and interests, and to avoid lawsuits. Others shared that they were disappointed, lost trust, and even avoided getting treatment because they did not rely on the healthcare system and service providers. Some reported surgery and examinations during or after childbirth, which they were not sure were needed, and put them and their newborn at unnecessary risk, and that the staff did not listen to their needs. Liora expressed her anger and mistrust of high-level policymakers in the MoH: I can’t be angry at the staff, but I am angry at those at the top, who have no idea what is happening in the field… All the programs and resources are invested where they shouldn’t be, and that's what I’m angry about… I’m sure that if they went out into the field, the healthcare system would be completely different. (Liora)
Nabila told us that before her second delivery, and in light of her first abusive delivery and mistrust of the healthcare system, she sought referrals to various hospitals, in an attempt to find a hospital that was not run like a factory, where she could give birth without experiencing a sense of neglect like the previous delivery and knowing that she would not accept instructions blindly. I didn’t want a hospital that works like a factory… I chose another hospital, one that is not crowded and was recommended by my sister who gave birth there… I don’t have this blind trust in them [medical staff] anymore because we’re all humans. All of them might have their own interests… (Nabila)
Coping Strategies
Repression and Avoidance as a Way of Dealing With the Pain and Trauma
Many women shared that they were aware that they had repressed the traumatic experience of obstetric abuse as a means of coping. Some reported that they had ignored the experience for years by disengaging from themselves, and had only related to the negative experience years later. Although some were referred to psychological or psychiatric treatment following the trauma, they did not apply for help. Others, who had attended therapy, said that they did not feel that the therapy had helped them to deal with the OV they had endured. I really didn’t feel the need… I really felt that the past [the abusive treatment by the medical staff] was in the past, and I was looking ahead to the future. (Sarit) I don’t believe in psychologists, and I didn’t see fit to go… for me it was just a waste of money, and I preferred to invest money in important things… You can say that I detached myself during that period [after the abusive childbirth experience] … I just disengaged from myself and forgot that I was a human being that needed to look after herself too. I invested all my energy in my child. Now that she is older and more independent, I’m slowly beginning to take care of myself… after seven years… (Liora)
Garnering Inner Strengths, Resilience, Knowledge, and Awareness of the Childbirth Process
The women who mentioned their resilience as a coping strategy mainly shared that they came to the second childbirth with a great deal of knowledge and awareness about the process; that is to say, they garnered their inner strengths to cope with the trauma and prevent its recurrence. One of the women noted that her resilience and inner strength helped her deal with the negative experience and tell her story of obstetric abuse without developing a complex. I told it [the abusive treatment during childbirth] like everyone tells their childbirth story. People were very surprised… A work colleague asked me if I had given birth in the desert, and how I didn’t wise up… for me, it was something I had experienced, and thank God I have the resilience to get through it without needing more… (Sarit)
Sarit's interview was used also to illustrate the previous coping mechanism of repression and avoidance; however, while it seems that she had repressed the abuse, she also felt that her resilience was the thing that helped her get through that bad experience.
Women also shared that at their second delivery they were much more aware of their rights and what they could ask for, such as changing the midwife, refusing examinations if they felt unsuitable or painful, or asking about the aim and necessity of certain procedures. They felt that knowledge and awareness of the process made them calmer and more prepared, they knew what to ask for and what to refuse. Knowledge is power, and a resource in which they are aware of their rights, and able to implement their rights and prevent an additional abusive experience. I imagine my next childbirth… I don’t know if it will work out, but I will try to contact the staff and sit with them way before, and explain who am I and what I want, although I don’t really know if this is possible. I don’t know if it has an effect because I can imagine they sit with others and listen to them every day. I learned that I should always be prepared for an emergency and ask for help. (Amal)
Relying on External Support—Family, Friends, and Other Women Who Had Not Necessarily Experienced OV
Many women mentioned relying on family members and other women friends for support through the experience of OV and their subsequent feelings. I’m lucky that my mom is a social worker, so we would talk a lot about emotions… There was a lot of truthfulness and support from my husband. The shower in the first week was at my mom's (she bathed the baby), the second week in my mother-in-law's house (she lives a floor upstairs), the third week my husband bathed the baby, and then I started doing it… These things really helped. (Rawan)
Sharing on Social Media and With Other Women Who Had Experienced OV
Some women reported that they had shared their experience on social media, which provided a space for legitimization and understanding of the obstetric abuse experience they had endured. Other women chose to share with other women through lectures they gave in the community to raise awareness of the problem. Participation in research is another way that women mentioned to promote awareness, to prevent similar negative experiences for other women, and to disseminate knowledge about their rights and how to reduce the problem. My mother is generally a person who does not reveal feelings, but I think she understood me and was with me afterwards… She saw how much I suffered [from the childbirth and how I was treated]. She saw I couldn’t sit for a month, I think… She was with me all the time, she saw how I suffered, and she supported me. But, even my mother, I think, didn’t understand in depth… It was definitely different in her time, something that was not discussed at all, and everything was “fine” and “legitimate”… I think that friends my age really understood the problem, but I mainly shared on social media, Facebook… And then I saw that many women had gone through similar things… and I even read about worse cases, so I told myself, “Okay, this is really common!” So, when you asked me if I wanted to participate in this interview, I said yes. It's important to promote awareness of this issue, maybe prevent it… and other women should know their rights. (Mira)
Reaching Out to Therapists/Legal Aid/Public Complaints
The women who had suffered OV shared their thoughts whether to file complaints about the medical staff. Some said that they wanted to complain but did not do so for a variety of reasons—lack of mental strength, unwillingness to get stuck in court, or busy being a mother and looking after a baby. One woman shared that despite the desire to complain about the negative and abusive experience she had endured, her family physician convinced her not to complain. In another case, one woman told us that in a meeting with the hospital administration and medical staff, she was treated like a liar, and there was no willingness to listen and contain her negative experience. She decided not to sue the hospital because she felt she stood no chance. In other cases, women complained, received an apology, but nothing more. The outcome for most women was not to return to the same hospital, or thoughts about having chosen a different hospital to begin with. I looked into the legal aspect because it was very important for me that no other woman goes through what I went through, and if I did nothing… I felt a sense of responsibility that if I stayed quiet this would happen again. I don’t know, just be careful, be more responsible. I don’t want this to happen to someone else. (Nabila) I don’t think they take the complaints seriously unless you file a complaint through a lawyer. I don’t know… I didn’t even receive a response to my complaint. (Rose)
Table 2 summarizes the types of consequences and women's coping strategies.
Summary of OV Consequences and Women's Coping Strategies.
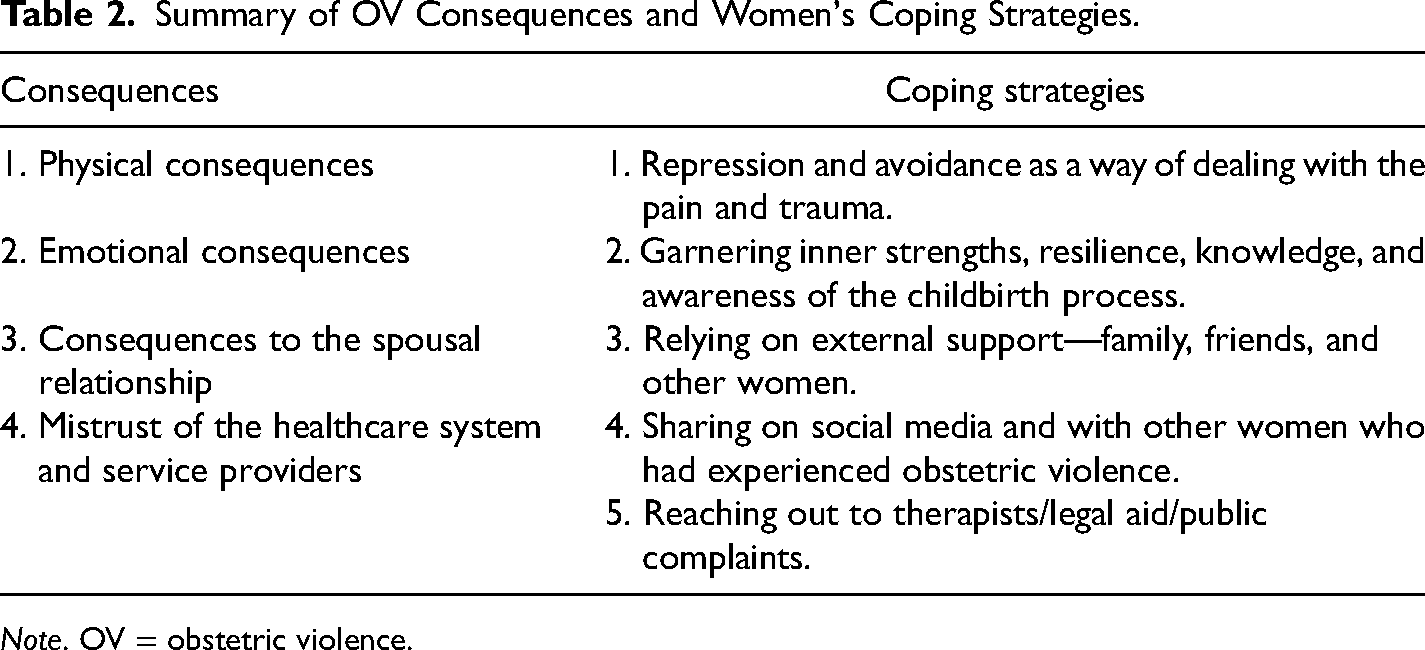
Note. OV = obstetric violence.
Discussion
The aim of this study was to give a voice to the insights of Arab and Jewish women in Israel, who had experienced OV, about the consequences of the abusive experience and their coping strategics from their own perspective. Another goal was to expand the research knowledge on an issue that, as far as we know, has not been studied among Arab and Jewish women in Israel.
The main points of view of this research were as follows:
OV is essentially gender-related, and the women who had suffered OV are in a position to precisely clarify their experience, through emphasis on their unique status as women, and thus to raise the awareness of medical personnel to the consequences of OV—to both the women and their immediate environment. Additionally, to remind healthcare personnel of their obligation to provide humane and respectful treatment, and of their responsibility to eradicate the phenomenon, while relating to the unique gender-related elements of pregnancy and childbirth (Briceño Morales et al., 2018). To support the women who suffered OV through sharing that could help them deal with the consequences of the abuse.
This study adds to the sparse literature and gives a unique insight on the Israeli context of how the experiences of violence negatively affect women in a wide spectrum of their lives, even years later. Furthermore, it gave a voice to the interviewed women and their recommendations about how to cope with the consequences of OV, and to empower women's ability to make their own choices.
The research population in this study included an equal number of Arab (minority) and Jewish (majority) women. However, the Arab women did not represent the socioeconomic characteristics of Arab society in general. Unlike previous research, which found considerable perceived gaps in aspects of education, employment, and health (Chernichovsky et al., 2017; Daoud et al., 2018), the participants in this study are educated and have higher socioeconomic status. Notably, when examining the education situation between the two groups in Israel, the gap narrows when it comes to women. According to the CBS 2023 statistical report, the rate of women with academic education (all degrees) was 60.3% and among Arab women—an exceptionally high 69.2%. The rate was even higher with Master's degrees (75.6%). For every one male Arab student, there were three female students (Central Bureau of Statistics, 2023). These data indicate an increasing trend of Arab women's participation in higher education in Israel, which could lead to a change in their status and place in society.
At the same time, patriarchal norms persist prominently within significant segments of Arab society. However, as a society undergoing transition, women consistently question and challenge these norms. The increasing involvement of women in the labor market and higher education over the past two decades suggests that their endeavor for self-fulfillment may be yielding positive outcomes (Hadad Haj-Yahya et al., 2018). This is probably one of the reasons why women with these characteristics also expressed their willingness to participate in this study, seeing themselves as an agency of social change.
The first theme dealt with the consequences of OV on a number of levels: physical; emotional; spousal relationships; and trust of the healthcare system. As was found in previous studies (Acharya et al., 2021; Greenfield et al., 2021), women reported ongoing physical pain long after the abuse, which in their perception was a direct result of the mistreatment—unnecessary invasive procedures (such as episiotomy), and lack of proper response to their pain due to understaffing and unavailability of postpartum medical aid.
The current study underscores that women participating in the research articulated that the experience of physical pain impeded their daily functioning, encompassing tasks such as caring for their newborn and engaging in sexual relationships. This assertion is substantiated by earlier studies (Acharya et al., 2021; Morris et al., 2023).
When women who were mistreated by the medical staff experience the childbirth as traumatic, they mention the emotional pain that accompanies the physical pain. In this study, women described the feelings of sadness, depression, anger, guilt, and anxiety that overshadowed the sense of euphoria and falling in love with their newborn and affected their maternal connection with the infant. PPD was mentioned (De-Souza et al., 2017; Martinez-Vázquez et al., 2022; Silveira et al., 2019), as were ambivalent feelings about their functioning as a mother expressed in anger and guilt (Beck, 2015). Some participants added that they felt very lonely during a period when they themselves needed time to recuperate and heal from the difficult delivery and the staff's attitude. This finding is also supported in the literature (Acharya et al., 2021; Fenech & Thomson, 2014; Smith-Oka et al., 2022).
Studies have shown that belonging to a minority group is a risk factor for PPD. In Israel, a study that compared the prevalence of and risk factors for PPD among Jewish and Arab women in Israel found that prevalence among Arab women was significantly higher compared to Jewish women (20.8% vs. 7%, respectively) (Shwartz et al., 2019). However, among Arab women the predominant risk factors for PPD were chronic stress, insufficient social support, and unintended pregnancy. Conversely, within the cohort of Jewish women, the identified risk factors for PPD encompassed chronic stress, a lower educational attainment, and instances of intimate partner violence (IPV). Previous research (Daoud et al., 2017) has indicated the relationship between IPV and belonging to a minority group, including Arab women in Israel, and explained that IPV in their study was not found to be a risk factor for PPD among Arab women because more Arab than Jewish women have “normalized IPV” and perceive acts of partner violence as part of their lives (Daoud et al., 2017).
In this context, an additional facet delineated in the literature posits that OV bears a certain resemblance to IPV. This form of maltreatment manifests through instances of physical, psychological, and sexual violence, as well as control over the woman's behavior. Consequently, women subjected to such occurrences exhibit a heightened vulnerability to physical injuries, engage in suicide attempts, and experience an elevated incidence of PPD (Daoud et al., 2020).
Alongside the physical and emotional effects, women reported damage to their spousal relationship, which included avoidance of sex due to physical discomfort, anxiety about another pregnancy, and over-sensitivity. This supports previous research, which also found that sexual intimacy was occasionally a reminder of the OV experience (Acharya et al., 2021; Ayers et al., 2006; Elmir et al., 2010).
An additional result of OV is loss of trust in the medical system and service providers. In most cases, the mistrust is not directed at the specific caregivers, but at the healthcare system in general for its misunderstanding of the woman's body and needs. This is an important point because the mistrust, as described by the participants, has two key outcomes—fear of having another child, and refraining from necessary treatment as was seen in previous studies (Faheem, 2022; Fenech & Thomson, 2014; Greenfield et al., 2022; Shorey et al., 2018). This situation could go on for years without receiving any help that fits their needs during pregnancy and childbirth. These findings underline the immediate and long-term consequences of OV, and the importance of creating future interventions that conform with women's needs.
In the present study, following their experience of OV, women perceived the hospitals as operating mainly in their own interests, which did not necessarily coincide with the women's needs. Notably, unlike previous studies that found that minority groups had less trust in the healthcare system (Cantarero-Arévalo et al., 2014; Schwei et al., 2014), research that compared the level of trust in the Israeli healthcare among minority groups (including Arabs) with the Jewish population) excluding Jewish immigrants, also a minority group) found that the level of trust among the Arab population was higher (Pinchas-Mizrachi et al., 2020). The explanation lay in the demographic characteristics of the Arab population that participated in the study; namely, older, less educated, and more religious Arabs tend to trust the healthcare system more, indicating an expectation for a traditional patient–caregiver relationship within this demographic (Pinchas-Mizrachi et al., 2020). However, the Arab women in the current study, who mentioned mistrust of the healthcare system, had a higher socioeconomic status and were consequently aware of their right to receive quality treatment that suited their needs and, therefore, did not have blind trust in the healthcare system, very much like their Jewish counterparts.
The second theme focused on women's various coping strategies with the consequences of OV. There is a lacuna in the literature that investigated this issue from the perspective of Jewish and Arab women in Israel, and in the world in general. In the present study, a number of coping strategies were described. First, repression and avoidance as a way to deal with the pain and trauma. Some women reported that the repression was a form of disengagement from their negative experience, and that it took years before they could think about and analyze the events. Emotional detachment from the experience in fact caused detachment from the self, mainly as a way to focus exclusively on the child. Sachdeva et al.’s (2022) literature review emphasized the postpartum confrontation with obstetric trauma. It should be noted that the traumatic experience is linked to women's feelings that they are neither heard nor seen during the childbirth process (Pop-Jordanova, 2022). Furthermore, some women tend to minimize or “forget” the abuse (even when there it is clearly evident) as a protection mechanism against the traumatic memory (Briceño Morales et al., 2018).
Another form of coping is resilience and accumulating inner strengths, knowledge and awareness of the delivery process. Resilience relates to a woman's ability to cope during ongoing stress, in terms of how she sees the world and how she lives in it (Ford-Gilboe et al., 2009). This reaction is personal, dynamic, and context-related (Alves et al., 2021). In the present study, women expressed their resilience through acquiring knowledge and awareness of the childbirth process. They stated that, through their resilience and knowledge, they regained control which allowed them to tell their story without reliving the trauma. Also, resilience allowed them to be better prepared for the next delivery, aware of their rights, and in control of the process. The literature on women's resilience focused primarily on growth after experiencing IPV (Brosi et al., 2020), or ongoing stress during the fertility and childbearing period (Alves et al., 2021), but not on OV. However, previous studies mentioned that some women chose to cope by means of expanding knowledge and taking back control (Allen, 1998; Greenfield et al., 2022). Notably, regaining control expresses the understanding and acknowledgement that women control their bodies and choices, which creates a positive experience that respects the woman's body and her decisions concerning the reproduction process through gender awareness of her unique needs (Šimonović, 2019).
Many women in this study mentioned their reliance on their family's and friends’ daily support, which also served as a channel that allowed them to tell their stories and feelings concerning the mistreatment they had experienced to a sympathetic ear. It is evident, also in the literature, that they needed empathy and support from their life partner, family and close friends to deal with the OV experience (Allen, 1998; Ayers et al., 2006; Nicolls & Ayers, 2007). As emphasized by Shabot (2021), women do not give birth alone, so that coping with OV requires attention to the woman's interpersonal relationships, characteristics of her community, and support, acknowledgement and help from those around her.
This finding illuminates the degree to which the woman's family and close friends are a crucial source of support for women in the collectivist Arab society (Meler, 2017). Jewish women also emphasized the importance of the family as an anchor during their experience, despite their more individualistic society (Ben David & Khatib, 2021).
Social media and discussions with other women were described by the participants as an active strategy to protest OV, and raise it to public consciousness, especially for the benefit of other women. In this study, all the women were educated, and cognizant of the influence of social networks, and relied on sharing to make people aware of and protest against OV. Women also mentioned that exposing their story allowed them to receive support and empathy from other women. Social networks are perceived as a safe space for women, where they can share their intimate stories about childbirth; a space that provides a platform for shared coping, discussing the problem and how it might be eradicated (Espinoza-Reyes & Solís, 2020; Leinhart, 2019).
Another form of active coping, which expresses women's desire to raise awareness of OV as abusive, and to obtain recognition from the healthcare system itself, was to reach out to legal and public complaints agencies. Some chose to file complaints against medical staff members, sue the hospital, or approach higher officials in the healthcare system. It seems that this was not necessarily effective, because they encountered barriers in the institutions’ ability to contain their experience, and in some cases were even labeled liars. It seems that the judicial system is usually unaware of the gender-related elements, finds it hard to understand the physical and emotional cost of mistreatment during childbirth, and is unwilling to award damages except in cases of death or disfigurement (Kukura, 2017). Moreover, the gender and social power structures do not facilitate women's access to the legal arena (Sommerfeld, 2022). On the issue of health institutions’ reactions, it seems that the denial of OV as a phenomenon is based on the perception that the mistreatment is specific rather than general, or on gaps in the staff's understanding of the woman's experience as OV because everything was done to facilitate a successful birth (Martínez-Galiano et al., 2023; Oliveira & Penna, 2017).
Unlike previous studies that indicated differences between women of different ethnicities in the perception of OV (Bohren et al., 2015), the present study found no differences between the two groups—Arab minority women and Jewish women.
This reinforces the argument that OV is gender-related by nature (Šimonović, 2019), and that gender-sensitivity is required to deal with it and its short- and long-term consequences.
Limitations
The participants of this research were targeted rather than random; that is, some population groups are not represented in the sample, and it is possible that enlarging the pool of respondents could have contributed additional insights. Additionally, Arab and Jewish women from low socioeconomic and low education groups were not interviewed. We presume that the women who consented to be interviewed—higher income and education women—also have high self-awareness and robust mental resources.
Contribution
This qualitative study has expanded the knowledge concerning OV as a process that takes place not only on a continuum from fertility treatments to childbirth experiences but years later, among two different cultures in Israel, Jewish and Arab women, and has examined this issue within gender contexts. The study can be a basis for expanding knowledge and research in OV and exploring other issues and populations that were not addressed.
As far as we know, this is a first study in Israel that describes the effects of OV on women and how they coped with it, as seen from their own perspective. Many women noted that the goal of their participation in the study was to raise awareness to the unique gender-related aspects, and make their knowledge available to healthcare professionals, while acknowledging the challenges and barriers they must face. Sharing, for them, is part of the healing process. Their voices are heard and valued, and space is given to creating a change in the attitudes of the healthcare system and medical professionals of the woman's body, needs, wishes, and knowledge of her own body during the pregnancy and childbirth process.
Conclusions
This study sheds light on and expands the missing knowledge concerning OV among Jewish and Arab women in Israel, their perceptions of the consequences, and their coping strategies with the OV they had experienced in the Israeli healthcare system. The findings point to the importance of raising awareness from a feminist perspective, which emphasizes the importance of knowledge as presented by the women themselves and in their own words. This approach reflects the unique effect of gender-related and ethnicity aspects on the implications of the OV experience to them and their coping strategies. The present study can serve as a body of knowledge for healthcare professionals, who come in contact with women of varied ethnic societies that live together in the same country. Also, policymakers can learn the importance of a gender-sensitive approach to reducing the problem of OV, which usually occurs through medical staff's lack of awareness.
Footnotes
Approval of Ethics Committees
Approval from the ethics committee of Ruppin Academic Centre was obtained on July 16, 2020 (research number: 2020-60, L/SW).
Acknowledgments
We extend our deepest gratitude to the women who participated in this research, generously sharing their experiences and insights.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.