
Abstract
The present study investigated social identification with “survivors” versus “victims” following sexual violence and the degree to which this predicted posttraumatic growth versus posttraumatic stress. Participants (N = 290) were adult women who had experienced sexual violence. As predicted, cumulative sexual trauma was positively associated with symptoms of both posttraumatic stress and posttraumatic growth. Further, people who had experienced more cumulative sexual trauma were more likely to identify with victims, which in turn predicted posttraumatic stress. Similarly, people who had experienced more cumulative sexual trauma were also more likely to identify with survivors, and this in turn predicted posttraumatic growth.
The psychological ramifications of sexual violence are well-documented: sexual violence places people at a high risk for mental illness, including posttraumatic stress disorder (PTSD), depression, and anxiety disorders (Forbes et al., 2013; Landrine et al., 1995; Ullman & Relyea, 2016). Increasing evidence points to a cumulative effect of trauma on mental health, where repeated or more severe traumas compound these detrimental effects on psychological well-being (Cloitre et al., 2009; Van der Kolk et al., 2005). While it is well-documented that the majority of people will be resilient in the wake of a traumatic event (Bonanno, 2004), a sizeable minority of people will experience detriments to well-being that constitute clinically significant distress. PTSD is the primary mental health condition associated with experiencing trauma, and is characterized by prominent intrusive symptoms (such as recurrent memories or flashbacks of the trauma), heightened arousal, disruptions in emotion regulation, and avoidance of reminders of the traumatic event (APA, 2013). Although the majority of people who experience traumatic events will not go on to develop PTSD, sexual violence exposure is more strongly linked to PTSD incidence than any other type of trauma (Creamer et al., 2001; Forbes et al., 2013; Kessler et al., 1995). Further, experiencing sexual violence is itself a risk factor for future revictimization, compounding the risk that a person will develop PTSD (Classen et al., 2005; Ellis et al., 1982).
While these devastating impacts of traumatic experiences are well-established, there is evidence that many trauma survivors also report posttraumatic growth, a phenomenon where people experience positive psychological changes following a trauma. These positive changes typically include fundamental shifts in an individual's sense of meaning in life, enhanced interpersonal relationships, and an increased understanding of one's values (Tedeschi & Calhoun, 2004). Notably, posttraumatic growth is more than simply resilience or “bouncing back” after trauma, and instead constitutes a shift towards enhanced psychological functioning compared to one's pretrauma state (Tedeschi & Calhoun, 1996). Whereas prior research has focused on the individual psychological factors that determine posttrauma mental health, more recently social factors have also been found to play a substantial role (Muldoon et al., 2019).
The Social Identity Approach (SIA)
Experiences of sexual violence are profoundly isolating events, and it is therefore unsurprising that the psychological sequelae of these experiences are often viewed through an individualistic lens, where coping skills, personality, and prior psychopathology have been considered to be the primary predictors of posttrauma mental health. Yet an increasing body of evidence points to the need for a social psychological understanding of responses to trauma. The social environment dictates the type of traumas that people are likely to experience and the resources that they will have to respond to this experience (Muldoon et al., 2019, 2021). Therefore, experiences of trauma cannot be fully understood through an individualistic lens, but rather, these individual factors need to be considered in a broader social context. The SIA provides a theoretical framework for understanding how and why trauma experiences may lead to diverging pathways in terms of individual mental health.
The SIA is based on the premise that one's social identities (i.e., one's sense of self, based on their group memberships) substantially affect both physical and psychological health (Haslam et al., 2018; Jetten et al., 2012). Belonging to groups not only provides connection to others, but is also an important source of self-esteem and meaning in life (Greenaway et al., 2016). This power of groups to promote well-being is known as the social cure effect (Jetten et al., 2012, 2017), and is the basis for a psychological intervention that has demonstrated effectiveness in reducing loneliness and social anxiety and improving social connectedness, Groups 4 Health (Haslam et al., 2016, 2019). Groups themselves are not always beneficial, however, and some group memberships may do more harm than good. In contrast to the social cure effect, certain group memberships may be damaging to well-being, constituting a social curse effect (Kellezi & Reicher, 2011). More specifically, being part of groups that are stigmatized or discriminated against is detrimental to one's sense of self-worth, particularly when one cannot easily (or does not wish to) leave the group (Wakefield et al., 2019). For example, many women strongly identify with their gender identity and do not desire to change it, yet being a woman puts people at risk of sexism, discrimination, and sexual violence. Perceiving discrimination as being due to one's group memberships, such as when women attribute negative treatment as sexism, can be harmful to one's identity and sense of self-esteem. In response to such treatment, people may in turn increase their identification (and thus their sense of belonging) with the stigmatized group, as a source of psychological protection against the negative effects of discrimination, known as the rejection-identification model (Branscombe et al., 1999, 2011).
Traumatic experiences are inextricably tied to social identities. Simply belonging to particular groups puts people at differential risk of trauma exposure and also influences the resources that one can draw on to recover from a potentially traumatic event. For instance, during wartime, women face a disproportionate risk of sexual violence compared to men, where rape is used as a form of social and political control that reinforces traditional gender stereotypes (Milillo, 2006). In patriarchal societies, the social and psychological aftereffects of these crimes are exacerbated, where the resulting shame and “dishonor” isolates women from their communities and families, thereby preventing them from accessing social and economic resources that may help them to recover (Milillo, 2006). As such, identity as a woman can interact with other important social identities (e.g., cultural identity) to increase both the likelihood of experiencing a trauma and the resources that can be drawn upon in the aftermath.
While group membership alone may be sufficient to increase the risk of exposure to potentially traumatic events, subjective identification with one's group memberships may impact how a traumatic event is perceived. Traumatic experiences are more likely to cause substantial psychological harm (e.g., posttraumatic stress) when they call into question a group membership that is subjectively valued (a social identity; Muldoon et al., 2019). For example, sexual violence may have particularly adverse psychological consequences in more patriarchal societies, as it undermines values of sexual purity that are strongly tied to one's identity as a woman (Kellezi & Reicher, 2011). Conversely, posttraumatic growth responses are more likely when one's social identity is extended with the creation of a new (positive) social identity, or when one reconnects with a preexisting valued identity (Muldoon et al., 2019). Evidence illustrating this comes from survivors of violence and abuse in South Africa. After abuse and/or violence, people who identified with antiviolence activists were more likely to experience posttraumatic growth (Haslam et al., 2022).
Sexual Violence through a Social Identity Lens
Despite these promising findings, the SIA has only recently been applied to trauma and there is a paucity of research examining sexual trauma using this model. Along with drawing attention to the pervasiveness of sexual violence, the #MeToo movement has shed light on the use of survivor and victim terminology to label people who have experienced sexual violence. While the term “victim” was historically used (i.e., victim of crime; Van Dijk, 2009), the term survivor has gained traction in recent years, in reaction to the connotations of passivity and lack of agency associated with “victim” (MeToo Movement, 2022). This shift is supported by research: whether someone is portrayed as a survivor or a victim leads others to make different attributions of blame (Schwark & Bohner, 2019) and to differences in judgments of the severity of the assault experience (Papendick & Bohner, 2017). Researchers themselves are not immune to these biases: A meta-analysis of research on “rape victims” versus on “rape survivors” found that researchers who used the term “victims” predominantly investigated the negative mental and physical health consequences associated with the trauma experience (Hockett & Saucier, 2015). Conversely, researchers who used the term “rape survivors” were more likely to investigate outcomes such as resilience and posttraumatic growth, alongside the negative psychological consequences (Hockett & Saucier, 2015). The authors concluded that framing participants as “victims” predisposed researchers towards a narrower and more negative conceptualization of their participants, as opposed to those who used the term “survivors,” which predisposed researchers towards viewing their participants more holistically.
These early findings are promising, yet focus predominantly on others’ perceptions of victims and survivors. Although there is little research investigating the impacts of these labels on the victim/survivors’ own self-perception, some early research indicates that people who have experienced sexual assault may have preferences for a particular label (i.e., survivor or victim), or indeed may reject these labels altogether (Williamson, 2024; Williamson & Serna, 2018). Rejection of victim/survivor labels has also been found in research with people who have experienced childhood sexual abuse (Hunter, 2010), with some researchers arguing that such labels are reductive and ignorant to the broader social and political frameworks under which sexual violence occurs, over-emphasizing the role of the individual in both experiencing and healing from victimization (Ovenden, 2012; Spry, 1995). Here, social identity research can fill the gap of understanding the factors that influence self-perceptions as a victim or survivor (or both/neither).
It is clear from social identity research that identifying with labels that denote a shared group identity has implications for how people perceive and respond to their experiences (e.g., Haslam et al., 2012; Levine & Reicher, 1996). Findings from qualitative research indicate that perception of oneself as a victim or survivor may be associated with differences in mental health outcomes. Thompson's (2000) seminal work interviewing individuals who had experienced rape found that the majority of participants identified with both labels, however, identification with each term varied across time. In order to construct a positive self-image, participants described the need to adopt a survivor identity, as this evoked a sense of having recovered and regained control. Yet participants also reported the importance of assuming a victim identity when disclosing their trauma experiences, in order to be taken seriously. Victim identities also helped people to shift blame for the event from themselves to the perpetrators. However, these identities were also associated with negative effects: participants felt that survivor identities minimized the significance of the event and prevented them from eliciting care and support from others, whereas victim identities diminished feelings of autonomy (Thompson, 2000). Both identities therefore were seen to have distinct merits and drawbacks.
Similar results were found in qualitative research with victim/survivors who experienced sexual violence during the Bosnian war (Skjelsbaek, 2006). Here, women who interpreted their experience in terms of their gender identity (i.e., saw their rape as an attack on them as women), were more likely to endorse a victim identity. These women were also more likely to blame themselves for the event and were less likely to have disclosed the violence. Therefore, victim identification was associated with isolation from community supports and poor mental health outcomes (Skjelsbaek, 2006). Conversely, women who interpreted their experience in terms of their ethnic identity (i.e., interpreted their rape as a crime against them as Bosnians) endorsed survivor identities, which connected them to other war survivors, including those who had had different experiences of victimization (e.g., men who were injured during the war). Further, this interpretation of their experience allowed these women to uphold and protect a valued social identity, that of being a woman, and also that of their valued ethnic identity (Skjelsbaek, 2006). This interpretation of their trauma experience appeared to yield more positive mental health trajectories.
More recent quantitative research suggests that the relationship between survivor/victim self-labeling and emotional experiences is complex: for example, Boyle and Clay-Warner (2018) found that self-labeling as a victim was positively associated with shame and posttraumatic stress symptoms, whereas self-labeling as a survivor was associated with anger and fear. In contrast, research by Williamson and Serna (2018) found that self-labeling as a victim/survivor following sexual assault was not associated with differences in self-compassion or self-blame. It is clear from these findings that the relationship between self-labeling as a victim/survivor and mental health outcomes is more complex than simply one term being better than the other. One possible reason for this is that self-labeling as a victim/survivor is distinct from self-categorization and social identification processes. Compared to merely self-labeling, social identification is a more nuanced process of identifying with a collective of others, where one takes on board the norms, beliefs, and values that one associates with that particular group. Thus social identification with victims and/or survivors is broader than simply preferring one label over another; it involves recognition of the properties inherent to the group and an evaluation of oneself as fitting in with those properties (Turner & Onorato, 1999). Social identification with a group also facilitates distinct processes within and between groups: for example, it highlights similarities and differences between groups and enables processes of social influence from other in-group members (Tajfel & Turner, 2004). Endorsing a label is therefore necessary but insufficient for social identification to occur.
The SIA has only recently been applied to sexual violence, with emerging evidence that these processes are in fact associated with differences in posttrauma mental health. For example, in a sample of university student sexual assault victim/survivors, victim identification, or combined victim and survivor identification, was associated with higher levels of depression and lower self-esteem, compared to survivor-only identification (Boyle & Rogers, 2020). Further, thematic analysis with publicly available narratives of women who have experienced sexual violence suggests that some victim/survivors may subsequently engage in a process of identity redefinition and advocacy in order to improve outcomes and experiences for the collective (Muldoon et al., 2021). This early research provides further support to suggest that mental health trajectories following sexual assault experiences are linked to social identity processes.
The Present Study
The literature to date suggests that the terms “survivor” and “victim” constitute social identities which influence both one's own and others’ perceptions of a sexual assault experience. Although there are promising findings suggesting that survivors and victims are perceived differently by others, there is very little research examining the impacts of social identification with survivors/victims on mental health. There are at least four reasons why research is needed that examines sexual violence through a social identity lens. First, there is strong evidence suggesting sexual violence is an intergroup rather than interpersonal phenomenon, motivated by hostility towards an out-group (e.g., women; Hitlan et al., 2009). Second, advocacy movements such as #MeToo seek to mobilize survivors (and allies) as a group toward collective action to eradicate sexual violence (MeToo Movement, 2022). This broadens the perception of individuals who have experienced sexual violence as belonging to a discrete community with similar others. Third, prior social identity research has provided evidence for the role of social identities in impacting psychological responses to traumatic experiences (e.g., Muldoon et al., 2019, 2021), therefore it is likely that social identification plays a similar role in experiences of sexual violence, given that these experiences have a higher incidence of resulting in PTSD. Finally, research on others’ perceptions of survivors and victims highlights public perceptions of these labels as separate, group-based identities that are associated with different interpretations of sexual trauma, which once again suggests that social identity processes are likely to impact one's own perception of a sexual trauma experience. Taken together, this emphasizes the need for quantitative research that examines the effects of identifying as a survivor or a victim, using the SIA.
The present study investigated the impact of social identification with survivors and victims on mental health outcomes following experiences of sexual violence. In line with prior research on the effects of trauma (Cloitre et al., 2009; Van der Kolk et al., 2005), we expected that sexual trauma would have a cumulative effect, such that more severe and more frequent experiences would be associated with higher levels of posttraumatic stress and posttraumatic growth. However, the main aim of this study was to investigate whether survivor and victim identification intervened in this relationship to predict different psychological sequelae. Given that the term “victim” has been associated with passivity and weakness, we predicted that stronger identification with victims would be linked with higher levels of posttraumatic stress, such that:
In contrast, we predicted that the connotations associated with being a “survivor,” including those of empowerment and agency, would be linked with posttraumatic growth. Specifically, we hypothesized the following:
Method
Participants
An a priori power analysis indicated that 250 participants would be sufficient to detect an effect size of 0.2 (a small effect; Cohen, 1988). Participants were 290 Australian adult women ranging in age from 18 to 81 years (M = 31.23, SD = 12.30). All participants self-identified as having experienced a form of sexual trauma (see Procedure for details). Participants were majority White (77.59%), heterosexual (62.14%), with an education level of Bachelor’s degree or below (79.64%). Full demographic details of participants are listed in Table 1.
Descriptive Statistics for Key Variables.
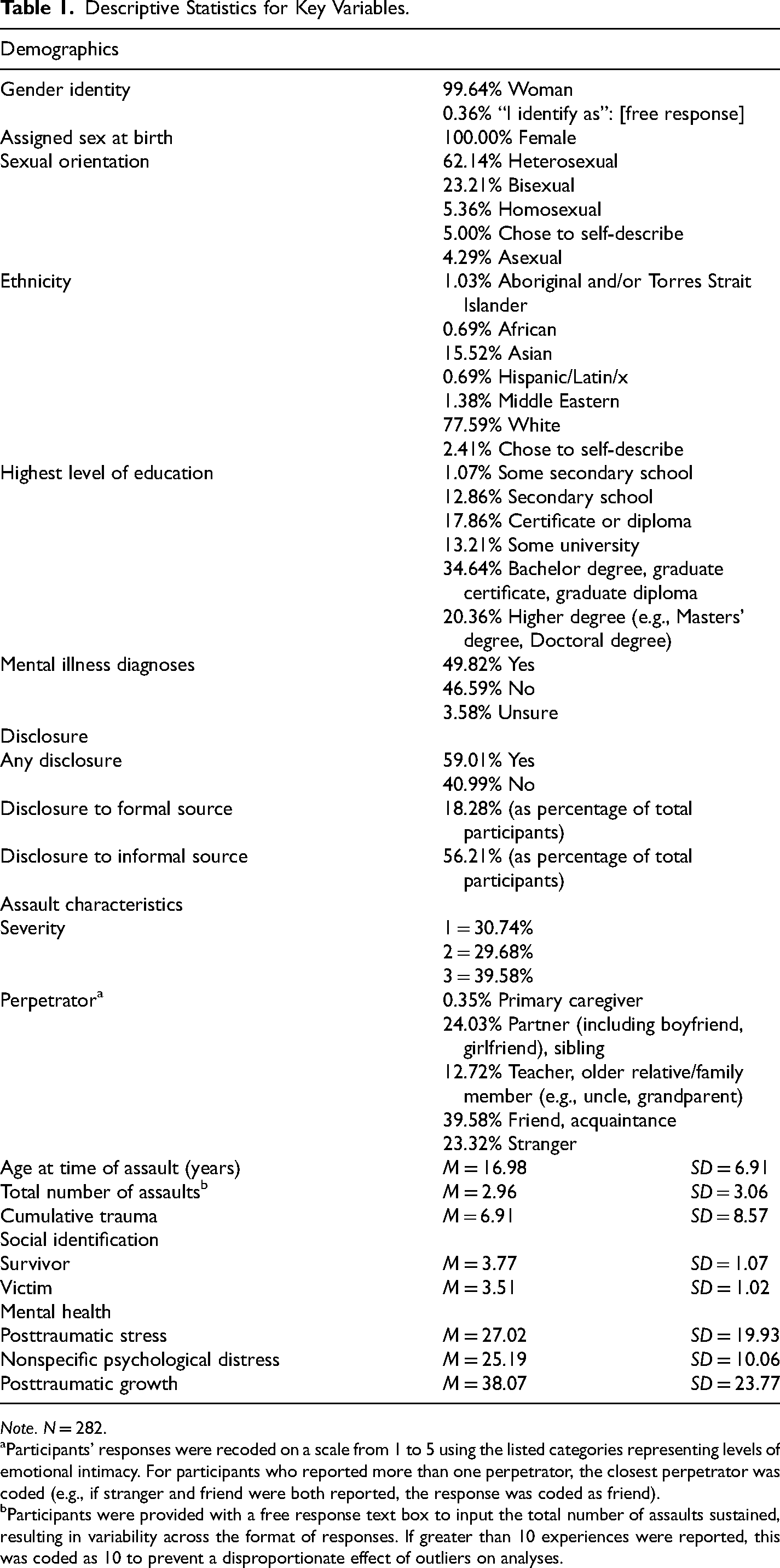
Note. N = 282.
Participants’ responses were recoded on a scale from 1 to 5 using the listed categories representing levels of emotional intimacy. For participants who reported more than one perpetrator, the closest perpetrator was coded (e.g., if stranger and friend were both reported, the response was coded as friend).
Participants were provided with a free response text box to input the total number of assaults sustained, resulting in variability across the format of responses. If greater than 10 experiences were reported, this was coded as 10 to prevent a disproportionate effect of outliers on analyses.
Procedure
The ethical aspects of this research were approved by The Australian National University Human Research Ethics Committee. Participants were invited to take part in a survey called Identity and Wellbeing After Trauma Experiences. This survey was advertised online to female-identifying people via Prolific, an academic research recruitment platform, and preregistered at the following link: https://aspredicted.org/blind.php?x = 7VR_3RF
Upon providing consent participants were screened for eligibility using the Trauma History Questionnaire (THQ; Hooper et al., 2011), which assesses for exposure to 24 different types of trauma, including crime-related events, general disaster and trauma, and physical and sexual experiences. All items correspond to Criterion A traumas in the DSM-5 (American Psychiatric Association, 2013). Participants were eligible to participate if they had experienced a sexual trauma, as indicated by answering “yes” to any of the following items (listed in decreasing order of severity
1
):
Has anyone ever made you have intercourse or oral or anal sex against your will? (3) Has anyone ever touched private parts of your body, or made you touch theirs, under force or threat? (2) Other than incidents mentioned [above], have there been any other situations in which another person tried to force you to have an unwanted sexual contact? (1)
A control variable, total trauma exposure, was created by summing the number of items across the entire questionnaire to which participants responded “yes.”
Eligible participants completed follow-up questions regarding the nature of their sexual trauma experience(s), followed by questions about their experience of disclosing the trauma, social identification with survivors and victims, measures of posttraumatic stress and posttraumatic growth, and demographic information.
Measures
Assault Characteristics.
Given the sensitive nature of the subject material, participants were only asked follow-up questions regarding their most severe experience of sexual violence. Participants indicated their age(s) at the time of the experience, the number of times they experienced this (frequency), and their relationship to the perpetrator. Frequency and severity of sexual trauma experiences were multiplied to create a combined score, cumulative sexual trauma, such that people who had experienced more frequent and/or more severe sexual trauma events had higher scores on cumulative sexual trauma.
Disclosure Experiences.
Participants were asked if they ever told anyone about their experience of sexual violence. Participants who indicated having disclosed were asked to identify who they had told from a list of sources, using an adapted version of the General Help-Seeking Questionnaire (Wilson et al., 2005). The sources listed in this questionnaire were a priori divided into formal sources (healthcare, legal, and professional supports) and informal sources (family and friends). As with the assault characteristics questions, participants were only asked about their disclosure experiences for their most severe assault.
Social Identification.
To measure social identification with survivors and victims, participants completed the Multicomponent Measure of In-group Identification (Leach et al., 2008). Eleven of the original 14 items in this scale were retained for use; three of the four items from the satisfaction subscale were deemed inappropriate for the context: It is pleasant to be a victim; I am glad to be a victim; Being a victim gives me a good feeling. The scale uses a 7-point Likert format (1 = Strongly Disagree to 7 = Strongly Agree). The scale was completed twice, once using the term “victim” and once with “survivor.”
Mental Health.
Participants reported frequency of PTSD symptoms over the last month using the Post-traumatic Stress Disorder Checklist for DSM-5 (PCL5; Blevins et al., 2015), a 20-item Likert scale (1 = Not at All to 5 = Extremely). Participants also completed the Post-Traumatic Growth Inventory (PTGI), a 21-item Likert scale measuring endorsement of posttraumatic growth symptoms resulting from the trauma experience (1 = Not at All to 6 = A Very Great Degree; PTGI; Tedeschi & Calhoun, 1996). Participants were also asked to provide any current or historical diagnoses of mental illness.
Demographics.
Participants were asked to provide the following demographic characteristics: gender identity, sex assigned at birth, sexual orientation, age, ethnicity, and education level.
Data Analysis
Analyses were conducted in SPSS (version 25.0.0.1). Correlations between key dependent variables (victim identification, survivor identification, posttraumatic growth, and posttraumatic stress) were assessed. To test the hypotheses, PROCESS version 3.5 (Model 4 using 5000 bootstrapped samples; Hayes, 2017) was used to test two mediation models using the hypothesized predictor (cumulative trauma), mediators (victim identification and survivor identification), and dependent variables (posttraumatic stress and posttraumatic growth). All models included the following covariates: current age, highest attained education level, total types of trauma endorsed (i.e., to control for degree of exposure to nonsexual forms of trauma), and ethnicity (coded as 0 = Ethnic Minority, 1 = Ethnic Majority/White). 2
Results
Descriptive Statistics
Demographic information and descriptive statistics for each of the key variables (assault characteristics, social identification, mental health outcomes) are provided in Table 1. The most common experience of sexual trauma reported was rape (Has anyone ever made you have intercourse or oral or anal sex against your will?), reported by 112 participants (39.6%). The most common perpetrator was listed as a friend or acquaintance, reported by 112 participants (39.6%). The majority of participants reported at least one disclosure (59.01%).
Correlations between key dependent variables are presented in Table 2. Social identification scores for survivors and victims had a significant strong positive correlation with one another (r = .781) Survivor identification had a significant weak positive correlation with both posttraumatic stress (r = .201) and posttraumatic growth (r = .334). Similarly, victim identification had a significant weak positive correlation with both posttraumatic stress (r = .259) and posttraumatic growth (r = .230).
Correlation Matrix of Key Dependent Variables Using Pearson's r.
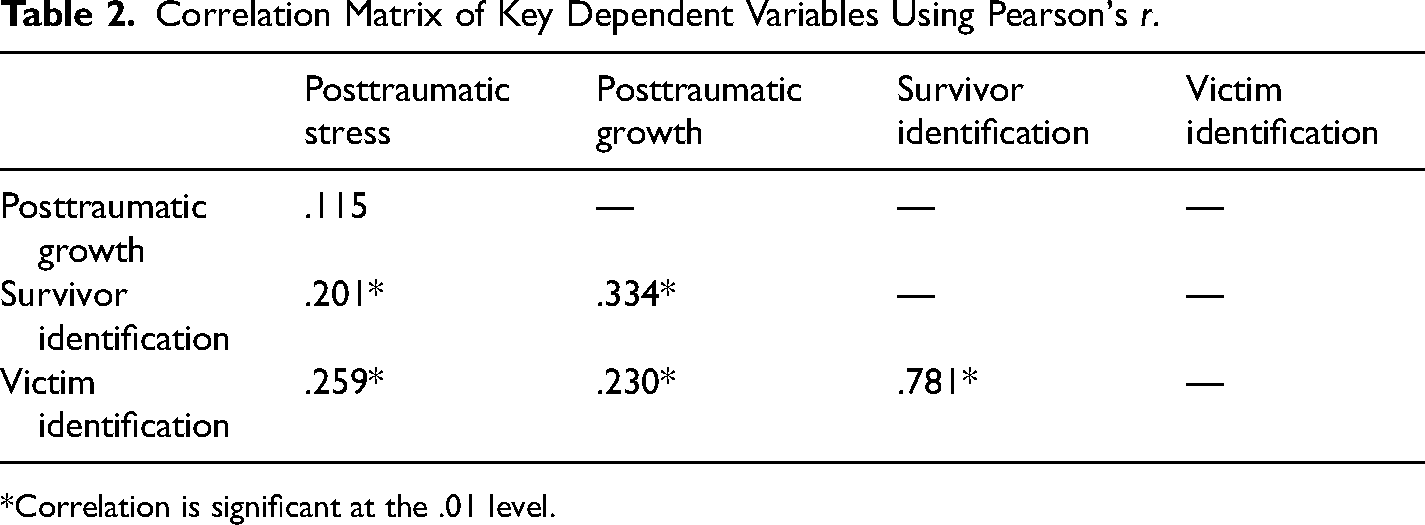
*Correlation is significant at the .01 level.
The Effect of Victim Identification on Posttraumatic Stress
Cumulative sexual trauma positively and significantly predicted victim identification (β = .19, p = .002) and survivor identification (β = .16, p = .009). However, only victim identification in turn significantly and positively predicted posttraumatic stress (β = .22, p = .009). Consistent with H1, the indirect effect of victim identification was positive and significant (β = .04, 95% CI [.004, .10]), see Figure 1. This was such that individuals with more cumulative sexual trauma were more likely to identify with victims, which in turn predicted greater posttraumatic stress. The indirect effect via survivor identification (β = −.01, 95% CI [−.04, .02]) was nonsignificant.
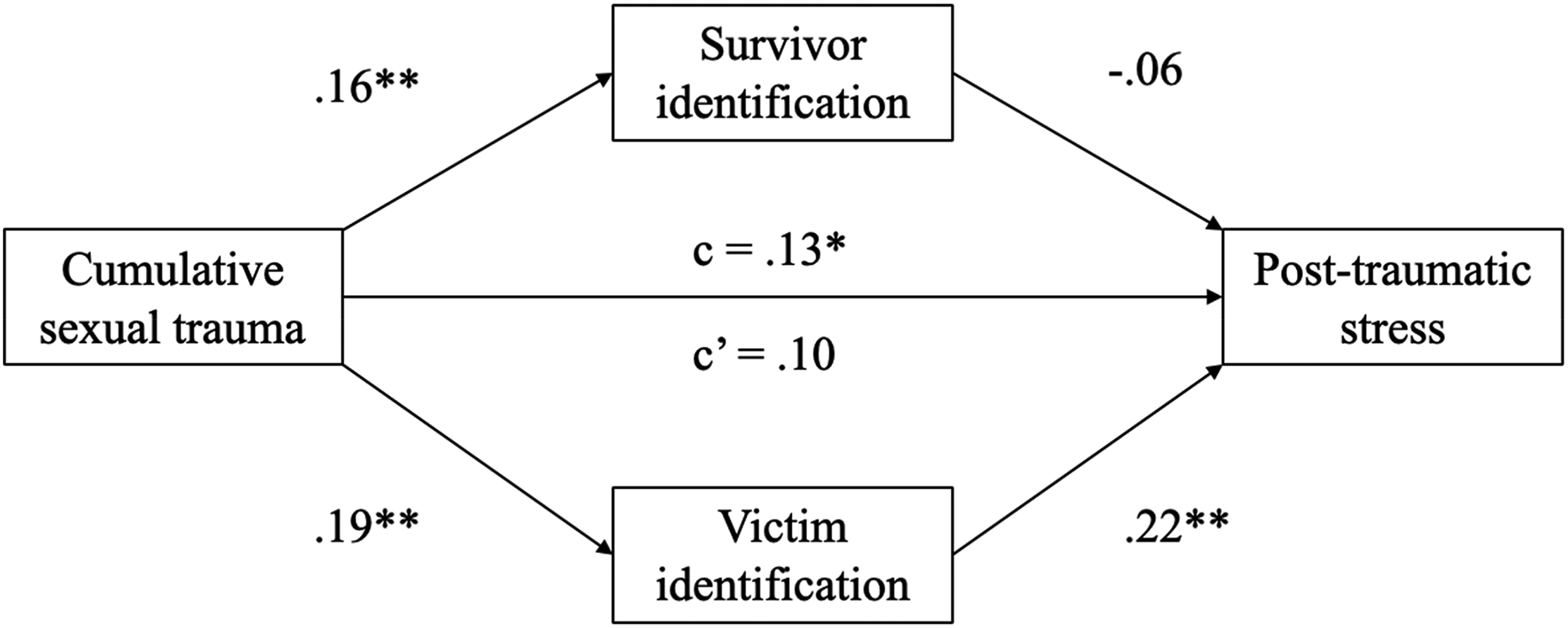
Path diagram depicting the indirect effect of victim identification on posttraumatic stress.
The Effect of Survivor Identification on Posttraumatic Growth
Cumulative sexual trauma positively and significantly predicted victim identification (β = .19, p = .002) and survivor identification (β = .16, p = .009). However, only survivor identification in turn significantly and positively predicted posttraumatic growth (β = .39, p < .001). Consistent with H2, the indirect effect of survivor identification was positive and significant (β = .06, 95% CI [.008, .13]), see Figure 2. This was such that individuals with more cumulative sexual trauma were more likely to identify with survivors, and this in turn predicted greater posttraumatic growth. The indirect effect via victim identification (β = −.02, 95% CI [−.07, .02]) was nonsignificant.
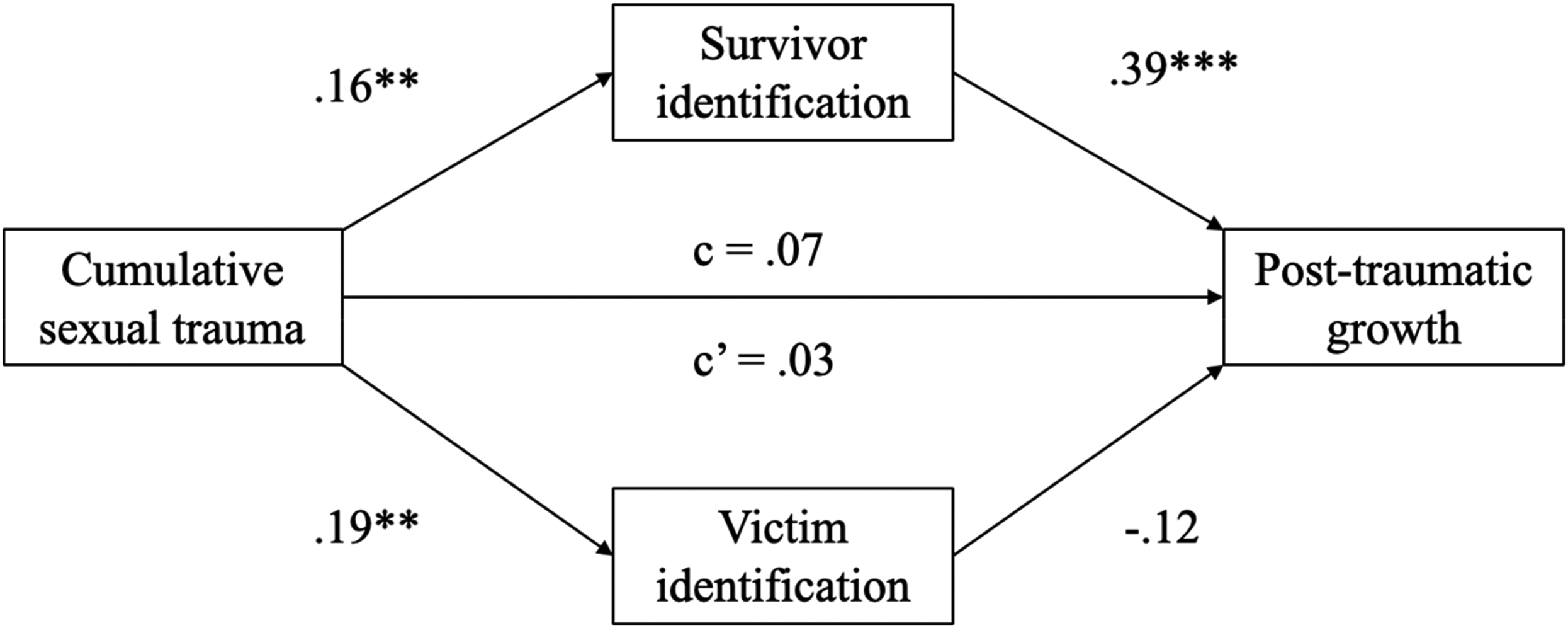
Path diagram depicting the indirect effect of survivor identification on post-traumatic growth.
Discussion
Results of the current study found support for a cumulative effect of sexual trauma on both posttraumatic stress and posttraumatic growth, with more frequent and more severe sexual trauma experiences predicting higher levels of both posttraumatic stress and growth. This finding is consistent with prior research on the cumulative effects of trauma (Van der Kolk et al., 2005). However, for the first time, we found evidence that these distinct pathways were partially accounted for by the social identities that are associated with traumatic experiences. Supporting H1, mediation analyses found that greater cumulative trauma predicted increased victim identification, which in turn predicted posttraumatic stress. At the same time, greater cumulative trauma also predicted increased survivor identification, which in turn predicted posttraumatic growth, supporting H2. Interestingly, in the mediation models containing both kinds of social identities, victim identification did not predict posttraumatic growth, and likewise survivor identification did not predict posttraumatic stress. Therefore, despite being highly positively correlated, it appears that victim identification is uniquely associated with posttraumatic stress (and not growth), while survivor identification is uniquely linked to posttraumatic growth (and not stress).
Taken together, these results speak to the value of exploring trauma trajectories through a social identity lens. Specifically, the findings suggest that victim identification may yield social curse effects, accounting for some of the harmful psychological effects of prolonged or severe trauma. In contrast, survivor identification may yield social cure effects by promoting posttraumatic growth. Identification with others who have overcome similar types of traumas may facilitate positive mental health outcomes that go beyond merely resilience and recovery. Notably, our results found the indirect effects of victim and survivor identification on posttraumatic stress and posttraumatic growth persisted despite controlling for the total amount of (nonsexual) trauma experienced. That is, the effects of victim and survivor identities in this study were specific to sexual trauma. One possibility is that the #MeToo movement has influenced the development of these terms as group memberships and identities, rather than simply labels. #MeToo has not only increased awareness of the prevalence of sexual violence, but has actively promoted a view of survivors as agentic and as a community. It is possible that identification with survivors encourages people to view themselves as capable of healing from their trauma, whereas identification with victims inhibits the possibility of recovery. Further, identifying with survivors may provide access to community of people with similar experiences of trauma. This may lead to enhanced social relationships, which is a key facet of posttraumatic growth. Also possible is that the #MeToo movement has emphasized the use of survivor terminology to such a degree that negative connotations associated with the term “victim” have become increasingly salient.
The strong correlations between survivor and victim identities also suggest that these identities are not separate but intertwined, and replicates prior work (Boyle & Clay-Warner, 2018). It is likely that many people who have had experiences of sexual violence endorse both identities to some extent, as was the case for participants in Thompson's (2000) study. Novel to this study, however, we found that a social identity lens can help us to understand the distinct effects of these intertwined ways of self-defining following sexual trauma.
Implications
One of the key implications of these findings is that identification with survivors or victims of sexual violence is likely to have real consequences for subsequent mental health. Emphasizing a survivor narrative therefore becomes all the more crucial for encouraging positive mental health outcomes. A SIA to sexual trauma could prove useful in informing strategies for recovery from sexual violence. Identifying as a survivor is associated with a trajectory of growth, while identifying with victims is linked to psychological distress. This suggests that survivor terminology (as opposed to victim terminology) is likely to be less harmful in discourse regarding sexual violence, including in media, criminal/legal, and health settings.
The shift in conceptualization of sexual violence over time from a purely interpersonal issue to a broader social concern has been mirrored in organizational structure and policy, and the current findings both reflect this and could be used to support further structural change. Where “crisis response” was once the sole focus of antiviolence efforts, organizations today understand the need for a broader approach that spans a greater duration, with consequences persisting beyond the immediate event (Lee et al., 2024). Use of survivor terminology (as opposed to victim) supports this perspective by encouraging not only a more holistic but also a less “static” identity following sexual violence, thereby acknowledging the temporal complexity of this issue. The current findings support the use of survivor-based language in organizations and public policy to facilitate more positive and empowering outcomes for individuals and communities.
Further, it is possible that survivor identities could also be harnessed as a psychological resource to promote recovery from sexual violence. Social identities are not fixed, but dynamic and malleable, and are therefore effective targets for intervention. Indeed, psychotherapy interventions that utilize social identity models have been shown to effectively reduce depression and promote long-term positive mental health outcomes (Haslam et al., 2016, 2019). Our findings thus point to the potential utility of mental health interventions for sexual trauma survivors that are based on social identity principles.
Strengths and Limitations
The strengths of the current project include preregistration, a priori power analysis, and the use of a large sample who all reported experiencing sexual trauma. Despite online recruitment, we were able to access a vulnerable population that had experienced significant trauma. Beyond the current study, the success of our methodology indicates that online recruitment tools may be a fruitful avenue for accessing vulnerable populations. Further, our sample also included a diverse range of participants across ethnicity and sexual orientation status. This is of considerable importance given that people of marginalized ethnicities and sexualities may be more at risk of experiencing sexual violence (Balsam et al., 2005; Black et al., 2011), and enables us to be more confident in generalizing our results to a wider population.
Further, the use of a multicomponent social identification scale to measure identification with survivors and victims helps increase our confidence that even partial identification as a survivor or victim is likely to impact mental health. It is likely that our sample included a subgroup of victim–survivors who reject labeling themselves as such (i.e., as seen in work by Williamson & Serna, 2017), yet even with inclusion of these participants in our analyses, we still found support for our hypotheses. Using a multicomponent and continuous measure of identification (rather than simply asking participants about their labeling preferences) therefore provides us with a more nuanced understanding of how social identification processes are linked to mental health symptoms, perhaps over and above that of simply labeling effects alone.
This study was also the first to investigate survivor and victim identities through a social identity lens, and the findings support the utility of conceptualizing survivor and victim identities using this framework. However, the use of a correlational design precludes attributing causation to any of the findings discussed, and is a limitation of the project. Additionally, we use the term “cumulative sexual trauma” to describe the experiences of our sample, in line with current evidence which suggests that the effects of trauma are not merely additive, but increasingly detrimental with repeated exposure. However, our study is cross-sectional in design, and our analysis is based on participants’ most severe experience of violence, meaning that our findings are unable to fully capture the longitudinally unfolding effects of ongoing experiences of trauma. Nevertheless, our finding that cumulative trauma predicted higher levels of posttraumatic stress replicates prior research (e.g., Cloitre et al., 2009; Van der Kolk et al., 2005). Therefore, what remains unclear is at what point along one's recovery trajectory that survivor and victim identities develop. Although we have theorized here that identification with survivors and victims leads to mental health impacts, another possibility is that the mental health consequences of sexual violence affect social identification with survivors and victims.
Future Directions
Although the current findings are promising and speak to the role of social cure and social curse processes in recovery from trauma, more research is needed to understand how survivor and victim identities develop. Our results indicated that there is an association between the cumulative effects of sexual trauma and these social identities, which are then associated with different mental health outcomes. However, longitudinal research could be beneficial to uncover how such identities change over time, which may also clarify causal pathways between mental health outcomes and identification.
While survivor and victim terminology dominates the discussion around sexual violence, it is also possible that neither term is preferable. Both terms risk reducing a person's conceptualization of themselves to their trauma experience alone. To our knowledge, there is no current research investigating victim/survivors’ terminology preferences, which is a significant gap in this literature. Along this same vein, there is also a need for research that emphasizes intersectionality, and examines how survivor and victim identities interact with other identities, such as ethnic and racial identities, sexual orientation, and gender. It is possible that the normative content of one's other valued identities may lead to differences in mental health symptoms associated with survivor and victim identification. For example, identities that emphasize norms of traditional femininity and purity may contradict the norms and content associated with survivor identification. It is possible that holding an identity which values purity and subservience may prevent identification with survivors, or may hinder on one's ability to engage meaningfully with a survivor identity. As such, there is a need for research which examines the contexts in which survivor and victim identification is helpful and harmful.
In sum, our research illustrates that trauma and identity are inextricably linked. Cumulative sexual trauma fundamentally alters one's sense of self; it is not just a violation of bodily autonomy, but a violation of one's core being. Therefore, research exploring identity processes is crucial to understanding how one recovers from such events. More pressingly, we have a responsibility to care for and support sexual trauma survivors. These survivors should not have to bear the burden alone and our research suggests that indeed, we can use the power of social groups to promote recovery and well-being among people who have experienced these unspeakable acts.
Footnotes
Authors’ Note
We would like to acknowledge the following contributors to this project: funding contributions from the Australian Government Research Training Program and the National Health and Medical Research Council (NHMRC) Emerging Leadership Fellowship #1173270; mentorship from Michelle K. Ryan (Global Institute for Women's Leadership, The Australian National University). Additionally, we would like to thank the participants of this research for their courage and vulnerability in sharing their experiences with us.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.