
Abstract
A partner's reproductive coercion and abuse (RCA) can significantly undermine women's physical health and psychological wellbeing. Yet little research has explored how RCA affects experiences of mothering and relationships with children. Based on an analysis of interviews with 30 Australian mothers, we found that RCA affected mothering in complex ways. Many struggled with feeling detached, resentful, and guilty toward their children, while some found mothering an emotionally and morally restorative experience after the RCA. All felt compelled to conceal their abuse from their children and others. The findings have implications for how healthcare practitioners can support mothers in the aftermath of RCA.
Pregnancy and becoming a parent are major life transitions. Although mothering is culturally idealized as a fulfilling experience for women (Douglas & Michaels, 2005; Hays, 1996), the reality does not always match the ideal. This may particularly be the case for women if a partner has forced them to bear a child or made them end a pregnancy. This study explores the impact of a partner's reproductive coercion and abuse (RCA) on experiences of mothering.
RCA refers to deliberate attempts to control, dictate, or interfere with a person's reproductive choices (Miller et al., 2010; Tarzia & Hegarty, 2021). It includes coercive behavior to cause or continue a pregnancy (such as rape or threats to make a woman continue a pregnancy, or sabotaging or controlling access to contraception), as well as behavior to prevent a pregnancy (such as coercing a woman to have an abortion or to use birth control, or using violence to cause a miscarriage) (Grace & Anderson, 2018; Tarzia & Hegarty, 2021). RCA is typically perpetrated by an intimate partner and is associated with other forms of intimate partner violence (IPV) (Grace & Anderson, 2018). Perpetrators are motivated by a range of factors, including self-interest and a sense of entitlement to control their partners, and a desire to dominate and entrap them in the relationship (Tarzia & McKenzie, 2024).
Research has identified that RCA is commonly experienced by women, though evidence about its prevalence is still emerging. Prevalence estimates of RCA range from 8% to 30% of women, depending on the setting and population studied (Rowlands & Walker, 2019) and how RCA is defined and measured (Tarzia & Hegarty, 2021). For example, a review of counseling data from 5,107 clients of two Australian sexual and reproductive health counseling services found that 15.4% had experienced RCA (Sheeran et al., 2022). Similar proportions disclosed experiences of coercion to promote pregnancy (6%) and coercion to prevent or end a pregnancy (7.5%), with 1.9% of clients experiencing both.
Research on the Impacts of RCA
RCA can have serious long-term consequences for women's lives and wellbeing. Along with having unplanned or unwanted pregnancies and pregnancy terminations (Grace & Anderson, 2018), the impacts include rapid, repeated pregnancies (Cha et al., 2016), poor mental health (Alexander et al., 2016; McCauley et al., 2014; Price et al., 2019; Tarzia et al., 2018), as well as consequences for the victim/survivor's physical health, such as sexually transmitted infections (Capasso et al., 2019; Kazmerski et al., 2015). RCA may also affect children's health, with emerging evidence suggesting babies are more likely to have a low birth weight if they are born after RCA (Fay & Yee, 2020). This may be due to the impacts of the abuse on maternal stress levels and use of alcohol, cigarettes or other substances, and/or a lack of access to antenatal care during pregnancy (Fay & Yee, 2020; Park et al., 2016).
A partner's abuse and control of reproduction may also have consequences for women's experiences of mothering and relationships with their children. Researchers have established that other forms of prior trauma, such as childhood sexual abuse or cumulative trauma experienced by women from refugee or Aboriginal communities, can make birth and mothering challenging (Berman et al., 2014). Research has also identified that abuse by a partner that occurs during pregnancy and after birth can affect mothering experiences, not only because it can undermine women's physical and mental health, but also because perpetrators may deliberately sabotage women's relationships with their children (Buchanan, 2017; Chiesa et al., 2018; Katz, 2019; McIntosh et al., 2021; Sousa et al., 2022)
Other Research on Impacts of Unwanted Pregnancy and Pregnancy Loss
More broadly, a considerable body of evidence shows that an unwanted pregnancy or pregnancy loss due to other factors (such as miscarriage, contraceptive failure, or denial of access to abortion services) can have detrimental consequences for maternal wellbeing and parenting. For instance, the loss of a wanted pregnancy can cause distress and grief (Grauerholz et al., 2021; Herbert et al., 2022), which can make it harder for women to engage with a subsequent pregnancy, particularly if their grief is not acknowledged by their family, friends, or health professionals (Garrod & Pascal, 2018). In relation to unwanted or unintended pregnancy, researchers have identified associations with post-partum depression (Qiu et al., 2020), problems emotionally bonding with the baby (Foster et al., 2018; Shreffler et al., 2021), and increased parenting stress and conflict in mother–adolescent relationships (Nelson & O'Brien, 2012). When an unwanted pregnancy is the result of rape in the context of war (Kantengwa, 2014; Woolner et al., 2019), or rape by a family member or a stranger (Thomson Salo, 2010), women report feeling ambivalent and disconnected to their child and struggling with decisions about telling the child about the circumstances of their conception. However, some women also say that motherhood gave them a reason to live in the aftermath of rape and war-related trauma (Kantengwa, 2014).
Study Aim
Reproductive abuse and control by a partner are also traumatic experiences, though how they affect mothering and relationships with children is poorly understood. Without understanding those impacts, we are unable to develop effective interventions to support women to address the consequences of RCA for their parenting and connections with their children. To address this gap, we sought to answer the question: How does RCA affect women's experiences of mothering and their relationships with their children?
Methods
Our research was conducted in the state of Victoria, Australia, although we recruited participants from across Australia. We interviewed 30 mothers for this study. Most were recruited through advertisements on social media. Our advertisement asked: “Has a partner or family member ever forced you to get pregnant, stay pregnant, or end a pregnancy? If so, we invite you to take part in a confidential interview about how these experiences have impacted on your relationship with your children.” Forty-two people expressed interest via an online form, and we contacted all of them, resulting in 26 interviews. We recruited the remaining four participants via an online survey that we were undertaking for a separate study on women's experiences of psychological abuse (including RCA). We contacted survey participants who had expressed interest in further research and had experienced RCA.
The authors LT and MM held in-depth interviews (Guest et al., 2013) between September 2021 and July 2022, using telephone or online video conferencing. The interviews were between 23 min and 2 hr in duration. We asked participants to tell their story about how their experiences of being forced to become pregnant or to end a pregnancy had impacted on their relationship with their child/ren. We asked participants to begin by talking about what happened in their relationship with regard to pregnancy, then used probes to explore their experiences of mothering after RCA. An in-depth interview approach suited the purposes of this exploratory study, as it enabled participants to identify the issues that they felt were important and explain them in their own words (Guest et al., 2013). We audio recorded the interviews and had them transcribed verbatim by a professional transcription service.
For the data analysis, we first imported the interview transcripts into the qualitative data coding program NVivo R1 (2020). Using a reflexive thematic approach (Braun & Clarke, 2019), we first coded the data descriptively, then developed interpretive codes, which we then categorized into overarching themes about impacts on mothering. We took an inductive approach to coding and repeatedly returned to the transcripts to check how our emerging interpretations connected with the data. The three authors met several times as a team to discuss the preliminary themes. Consistent with a reflexive analytic approach, we recognize that the themes we developed reflect our subjective engagement with the data, rather than being “discovered” through our analysis (Braun & Clarke, 2019). Considering this, we acknowledge that our interpretations of the data were informed by a feminist lens, including an understanding that both RCA and mothering are experiences that are shaped by gendered discourses constructed within a patriarchal social context. Our interpretive lens is influenced by our professional backgrounds and education in social work (MM and CH) and sociology (LT), as well as our shared commitment to the right to safe and legal access to abortion services.
The safety of participants and the potential for the topic to cause distress were key ethical considerations. Consistent with a trauma-informed approach (Campbell et al., 2019), we used safe methods of communication with participants (such as by referring to the study as a “women's health study” in emails, in case they were intercepted by a participant's abusive partner), and during interviews, we validated participants’ experiences and strengths. Many participants said they found that talking about their experiences was cathartic. For many, it was the first time they had shared these experiences and they wanted to help to raise awareness of the impacts of RCA. The study received ethics approval from the University of Melbourne Human Research Ethics Committee (HREC # 2021-2174219765-3).
Participants
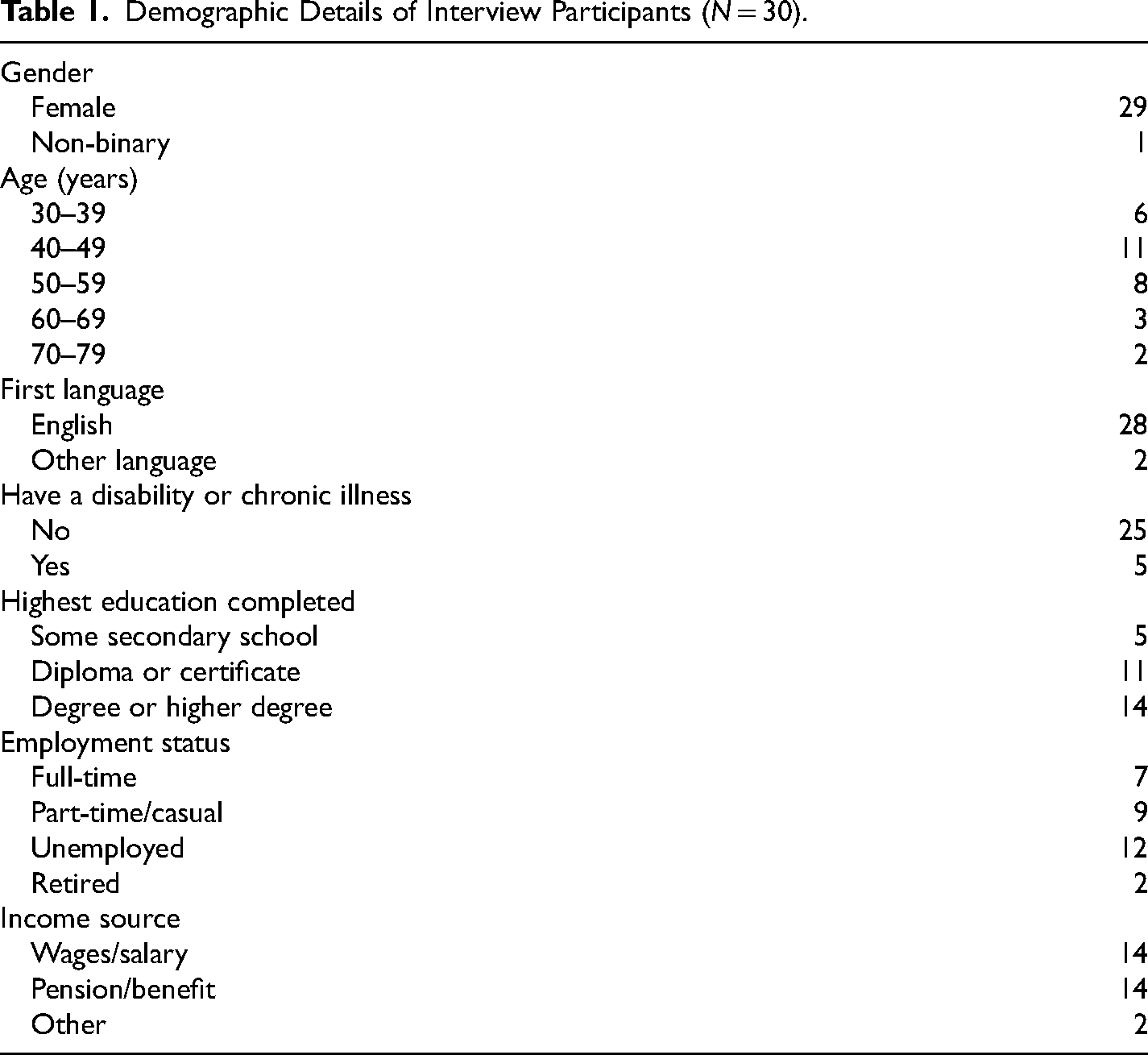
There were 30 participants in the interviews. They lived in states and territories across Australia, with over a third of the sample living in Victoria. Their ages ranged between 32 and 79 years, with most aged in their 40 s or 50 s. For some participants, the RCA experiences they described had occurred approximately 40 years prior to the interview, while for others the experiences had been in the past 5 years. Most lived with their children and did not have a current partner. All but two said English was their first language. None identified as Aboriginal or Torres Strait Islander. Further details are provided in Table 1.
Demographic Details of Interview Participants (N = 30).
Findings
Participants described experiencing a range of forms of RCA. Eighteen were subjected to pregnancy-promoting behavior, 14 were subjected to pregnancy-preventing behavior (including three who described attempts to force them to miscarry), and five experienced behavior from their partner at different times that was aimed at both promoting and preventing pregnancy. Many of the 30 participants said that their partner had shown signs of controlling behavior before the RCA. All described emotional, physical, and/or sexual violence continuing after the RCA, including their partner deliberately undermining their relationships with their children and/or being directly abusive toward their children. Although some said the impacts of those behaviors overlapped with the impacts of RCA, most were able to identify specific consequences for their mothering as a result of the RCA.
Based on our analysis of their interviews, we developed three themes about mothering experiences after being subjected to RCA: (1) “It's a struggle for me to mother”: detachment, resentment, and guilt; (2) “It healed a lot of pain for me”: restoration, redemption, and protectiveness; and (3) “I don’t ever, ever want them to know”: covering up and carrying the blame. The themes were linked with both pregnancy-promoting and pregnancy-preventing forms of RCA. Often all three themes were evident in a single interview, which reflected the conflicted feelings participants experienced in mothering after RCA.
“It's a Struggle for me to Mother”: Disconnection, Resentment, and Guilt
A strong theme from the interviews was about mothering being a torment of disconnection, resentment and guilt. More than half of the participants spoke of struggling with these interconnected emotions, particularly those who had been made to bear a child, as well as some who had been made to terminate a pregnancy.
Participants’ conflicted emotions often began early with feelings of estrangement and alienation from the baby during pregnancy. One remarked that her pregnancy felt like “some foreign thing was growing on me” (participant 22). Another said: “I always thought I would want to find out the gender … [but] I just didn't want to know anything about the baby at all” (participant 5). An emotional numbness often continued after the baby was born. For instance, one woman commented: “When I gave birth to her, I just felt nothing. [People say] you love them straightaway. I’m like, no, I didn’t. I was just like, okay, this is what I have to do” (participant 17).
What was confronting for those who had been forced to conceive or carry a pregnancy was that their child's existence was a living reminder of the abuse they had endured. This made it challenging to feel love for their child. One said: “I still resented the fact that I had this baby. I looked at him, and I remember thinking, I should really love this baby, and I don’t. It just embodied everything that [my partner] made me go through the last nine, 10 months” (participant 22). Like others, she also found it emotionally difficult to breastfeed: “[My child] was bottle-fed straight from the get-go … I just didn't want to [breastfeed] …I had such a disconnection from him that I just didn't feel comfortable feeding him.” Feelings of detachment and discomfort were typically intertwined with intense guilt and a deep resentment about the position their partner had put them in in relation to their child. The anguish of these interconnected emotions was illustrated in the following quote from another participant: “I just hated every second of the pregnancy, and then hated myself for hating every second of it. Then hated my husband for putting me in this position” (participant 7).
Many of the mothers wrestled with an inner turmoil throughout their child's early years. For instance, one participant's partner had threatened her to ensure she continued her pregnancy, and after her child was born, she suffered postnatal depression. Her struggle to voice her feelings during her interview demonstrates the deep discomfort and guilt she felt about the thoughts she had about her child: It's really hard to say - I'm struggling, you know, to let the words out of my mouth, but I couldn't help thinking that when times were really tough I would think things like, “I only had you because I had to” or “I only had you because I was made to” … [because of my feelings] I feel like I've been sort of robbed of those first [years of childhood] … it's all … a blur and I sort of missed a lot. (Participant 3)
The troubling feelings had lingered even after participants had separated from the perpetrator. This was particularly the case when women were reminded of him through their child's appearance or behavior. Mothers also felt the need to shield their child from being affected by their own emotional responses, as illustrated by the following quote: “Sometimes I would look at [my child] and some of his mannerisms do remind me of his dad, so I find that confronting … because it's like, what do I do with those feelings. I don’t want that to impact my parenting” (participant 8).
A struggle to bond with their baby and to enjoy mothering not only affected participants who had been made to carry a pregnancy, but also those who had been forced to terminate one. For example, one said: One of the very few things that hurts me now is the fact that I was a mother in such terrible circumstances that I wasn’t as present as I should have been. The termination was probably just another layer of that, it detaches you … from the beautiful experience of being a mother. I suppose because it's all been tainted by such a horrible background. (Participant 10)
As evident in the above quote, many participants conveyed a deep regret and anguish that they had not been able to be the mother they had wanted to be. Participants consistently expressed that although they did the right things in responding to their children's basic needs, they felt “wrong” in their emotional responses. For example, one woman described counting down the milestones to her child's independence: [I was] wanting to get this childhood over with … I was just wishing her life away … Every birthday [my child has] it's like, well thank God. That's another year over … You know, it's terrible … Just this constantly celebrating in the wrong kind of way, which is really horrible. (Participant 3)
Due to their conflicted feelings, often mothering only felt like a burden of hard work and responsibility rather than a source of pleasure. Participants described it feeling like “just a job” or a “duty,” or that they were just “going through the motions.” They not only suggested they had not been the mother they had wanted to be, but also that they had not been able to lead the life they had wanted to lead. For instance, one woman said her husband had constantly monitored her and prevented her from attending medical appointments to ensure she finished the pregnancy. As a result of his actions, she was no longer the person she once was. Instead, she said she had been left a single parent and “a tense, worried mum”: My life is stuck. I can't move forward … I was such a good person, such a high achiever and positive person. I became nothing … I lost my career … I am limiting myself to take care of the child alone … This life has been robbed out of me only because I had that baby. (Participant 12)
Being made to have an unwanted child also left participants carrying a considerable financial load. One commented on the expense of childcare, saying: “To pull yourself out of, basically poverty, is nearly impossible. So you do end up resenting the children a little bit, because you have to sacrifice so much while the other party hasn’t sacrificed or lost anything” (participant 11).
Given the intensive demands of mothering, some said they had secretly dreamed they could be relieved of their burdens. One participant described suffering major depression after being coerced by an abusive partner to bear a child. Although it was very difficult to admit, the participant said that at times they had “intrusive thoughts” about their child dying: This is really hard to say out aloud, but like, [at times I was] wishing my child was dead. Not to the point where I would actually … I feel the need to immediately say that I love my child, so much, but I also went through a period of like, fantasizing … instead of worrying that something would happen to [my child], like … “Oh no what if he gets hit by a car” or something, actually being like, “Oh … that would be a relief. I want out”. (Participant 6)
Such intrusive thoughts were confronting and triggered intense feelings of guilt. For example, another woman (participant 5) said that although she “did all the right things” to keep her baby healthy during her pregnancy, she “just would wish in my heart that I would lose the baby.” But she also felt terrible about thinking that way: “I felt so guilty and so bad that I had had those thoughts about the pregnancy.”
As the quote above illustrates, a frequent worry was that they were “bad” as a mother because they did not feel as they should. Many commented that women were expected to be overjoyed about becoming a mother and should be intensely engaged with their children; for example, they said mothers were supposed to be “so excited for the pregnancy and never complain about anything” (participant 5), should “love [the baby] straightaway” (participant 17), be “ecstatic” when their child took their first steps (participant 3), and should enjoy “lovely connecting sessions” doing arts and crafts with their children (participant 22). However, when their emotional responses fell short of those idealized expectations, participants often blamed themselves. For example, one woman who was forced to bear a child said: It is still a struggle for me to mother … It's so much more thought and guilt … I find it so much harder to be that fun … mother who's so engaged … it's more of a duty, sometimes. Or just thinking, I'm just going to fail at everything, or I missed something at [my child's] school, oh, God, I'm a bad mum. (Participant 22)
The conflicted emotions that participants harbored increased the stress of managing children's behavior. For example, one conceived her daughter after her partner forced her into sex. She said: Even now I think I find her my most challenging [of my children] and I get frustrated with her a lot more easily. With the normal stuff … the tantrums and refusing to eat food … my tolerance level for hers is a lot lower and I think it's probably borne out of resentment that I’m dealing with all of this stuff when I didn’t want to be. (Participant 11)
Many feared that their unhappiness “seeped out” and could be felt by their children. To protect their children, they went to great lengths to suppress or shift their feelings. For example, the participant quoted previously said: I got to a certain stage where I kind of mentally made the decision that I needed to force myself to change my mindset, basically. Because if I didn’t it would probably carry through onto the baby and I didn’t want to do that to a child that had no choice or say in the matter either. (Participant 11)
Others spoke of “overcompensating” for their disconnection by organizing huge, themed parties for their child's birthday, or intensively managing their mental health so they could meet their child's needs. One said: “I do a lot of trauma-informed yoga and therapy, so I’m like hopefully if I keep doing this I can keep showing up and showing up and showing up, you know, in better ways, so that I can be the parent that I want to be” (Participant 6).
“It Healed a Lot of Pain for Me”: Restoration, Redemption and Protectiveness
A second theme from the analysis was that mothering after RCA was an emotionally restorative and redemptive experience, which also prompted strong feelings of protectiveness toward their children. This theme was particularly evident in interviews with participants who had been made to end a pregnancy, as well as in some interviews with those who had been forced to bear a child, though they had different reasons for finding mothering restorative.
For mothers whose partners continued to subject them to abuse after forcing them to have a child, mothering provided a much-needed source of joy and meaning amid their traumatic experiences. For example, one participant's partner had impregnated her by ignoring their agreed contraception method and then continued to abuse her after the birth. She said that although she initially resented the pregnancy, her feelings changed when her baby was born: “My whole life was chaos but … this beautiful little baby was my oasis” (participant 7). Similarly, another woman, who fell pregnant after her partner had secretly removed a condom, said her child was “the best thing ever … [and] the only thing I don’t regret about my relationship” (participant 9). Being able to mother a child also provided a sense of purpose. One said that although her child was born as the result of rape, her child “kind of saved me… [and] gave me a reason to live” in the context of her partner's ongoing violence (participant 25). Children also provided a reason to leave; as one woman explained, it was “easier” for her to separate from her partner because: “Once I actually had the baby … I felt like I was no longer the top priority” (Participant 5).
For those who had endured the grief and guilt of being forced to abort a wanted pregnancy, having a subsequent child was often an emotionally restorative experience. For instance, one woman said: “all I’d ever wanted was to be a mum,” but she been forced to abort two pregnancies after her partner threatened to kill the baby if she didn’t. She said the forced abortions left her feeling “terrible” and “broken.” However, being able to nurture and “cherish” the children she subsequently had made her feel immensely grateful: “I would think about the terminations and think about how precious life is” (participant 4). Being able to mother also appeared to enable participants to redeem a wrong that they perceived themselves to be implicated in. A deep sense of culpability for the loss of a previous child prompted many to devote themselves to parenting their existing or subsequent children. For example, one woman's partner had pressured her into an abortion. She said that the fact she had terminated a healthy, wanted pregnancy “was very much on my mind during my future pregnancies. I felt like I'd killed a baby … that's hard to live with” (participant 19). When asked if the termination had affected how she parented her subsequent children, she replied: “Oh gosh yeah. They are so precious to me that my whole life revolved around my children.” Similarly, another woman (participant 1) suggested mothering had helped her to “make up” for a previous termination. Her partner had made her abort her pregnancy by threatening to push her down some stairs if she didn’t. She said she had always felt a deep regret and guilt for not standing up to him. However, she said that when she later had a baby with a new partner, devoting herself to her child's needs had helped her to atone and heal the loss: I give everything to [my child], absolutely everything. In fact, people will say she's spoiled because she does so many different activities and she's living a great life. My mum thinks “Oh what about time for yourself?” I’m like well I don’t really care about myself, it's her, life is about her, not me … If [my child is] happy, I’m happy, and so because of that loss of that pregnancy, I’m making up for it with her… just being able to replace that lost baby … it healed a lot of pain for me.
Guilt and a belief that they should somehow be punished for terminating a pregnancy also caused participants to feel intense worry about losing their subsequent children and an overwhelming need to protect them. For example, the woman quoted previously said she found her pregnancy “extremely stressful, because … I felt guilty because of what I’d done before, and I thought that it was karma for me to lose this one.” She also said she used to get extremely anxious when her child was unwell and was “the biggest helicopter parent around…I would be so worried about everything” (participant 1). Similarly, another woman (participant 2) described how she had strongly wanted to keep her pregnancy, but her partner had threatened her that if she didn’t abort it, he would take her other two children away from her. She said: I’ve never, ever forgiven myself for what happened … It went totally against my beliefs, my values … [the child I lost through the forced abortion is] always in my thoughts and thinking what it would’ve looked like, how it would’ve got on with [my other kids]. I think there were times I just felt really - just really concerned about keeping [my kids] safe. It's a bit hard to explain, but not that [my abusive partner] was going to do anything to them. It just made them more precious, I guess. In that I didn’t want to lose either of them as well.
“I Don’t Ever, Ever Want Them to Know”: Covering Up and Carrying the Blame
The third theme from our analysis was having to carry the blame and conceal their experiences from their children and others. This theme was evident in interviews with participants who had been forced into a pregnancy, as well with those made to terminate a pregnancy.
A major reason that participants did not want their children to know about the abuse they had endured was a fear that the knowledge may harm their children. Those who had a pregnancy as a result of rape were adamant that their child must never find out about their origins. Participants said they felt it would be “horrible” or “really awful” for the child to know and might damage the child's sense of self; as one said: “[My child] doesn’t deserve that. To think that he was a mistake or to have the true understanding of how he came into existence” (Participant 8).
Participants also worried that their children may see them as a heartless mother who did not love really them. For example, one woman said she felt like she was not only keeping her experiences of RCA secret to protect her children, but also to protect herself: If [my son] found out that I didn’t want him and aborted the first [child] … it would just be awful for him. I feel guilty, and I feel irresponsible that I haven’t been a very good role model for [my daughters] … I don’t want them to even know what happened. I don’t know why, maybe that's my shame, maybe it's embarrassment on my part I’m not sure, but I feel like it's a protection for them. Whether it's actually not, whether it's actually protection for me and not them, I don’t know. I feel very strongly that I don’t want them ever to know. (Participant 7)
Another woman feared that her children's view of her had changed after she tried to talk to them about her experiences of being made to abort a twin pregnancy. She said: “It really has impacted on [my children] because they’re like, “Do you really love us? Do you really care for us? … Well, how could you be a good mum if you could get rid of our brother and sister like that?” Yeah, it's not an easy topic to have with them” (participant 13).
A further reason for keeping RCA a secret was to protect the child's relationship with their father. However, concealing it also meant mothers could never explain to their children the difficulties they had faced in parenting them. For example, one woman said that because her partner had forced her to become pregnant, she had found it hard to enjoy her son's early years. To protect her son and his relationship with his father, she felt that she would never be able to tell her son about the abuse she had faced and the immense stress it had caused her in parenting him. However, at the same time, she deeply resented the injustice of having to conceal it, as it enabled her ex-partner to “play himself off as this perfect dad” (participant 8). Another participant felt that she had been emotionally “missing” as a mother because having a child had not been her choice. She said she had worked hard to ensure her daughter was never aware of her detached feelings. However, at the same time, she regretted that she could never have an honest conversation with her child about how the circumstances of her conception had affected her mothering: “So, then I've got this secret from [my child], because I never want her to know … I want to protect her from that. It's one of many secrets, family secrets, that I can try and keep from [my child] which is not great, but I just have to accept that” (Participant 3).
Social taboos around speaking about maternal unhappiness or abortion experiences also had a silencing effect. For instance, one participant said: I feel terrible saying this now, which is why I don't tell a lot of people, but I just didn't connect with my pregnancy at all … Is guilt the right word? Maybe it's more shame … because … there's this expectation of mothers that we have to be so excited for the pregnancy and so excited for the baby and you can never complain about anything … I feel more like it's a taboo to talk about. (Participant 5)
However, being unable to share their RCA experiences and their impacts meant participants’ trauma went unacknowledged by others, which added to their poor mental health. This was the case for one woman, whose husband and family had threatened to deport her if she didn’t terminate her pregnancy. Afterward she suffered intense distress, grief and guilt, even though she supported women's rights to abortion in general. However, she had to conceal her anguish because abortion was “taboo” to talk about. She subsequently fell pregnant and this time she managed to keep the baby. However, she said: I had a nervous breakdown a few years after the abortion. I would walk about with a little baby doll, but not yet acknowledging that that was a problem … Then I sort of went to pieces … I was in hospital and everything … it was that suppression of … all the emotions… Not only you are left with your emotions on your own, but you have to hide them. (Participant 27)
Discussion
The findings of this in-depth study demonstrate the complexity of mothering after RCA. Research to date has identified that IPV during pregnancy and parenting can undermine maternal wellbeing and relationships with children (Buchanan & Humphreys, 2021; Dekel & Abrahams, 2023; Katz, 2019), yet our study shows that the damaging impacts can begin earlier, through a partner's control around conception. Based on interviews with 30 participants, we found that being made to end a pregnancy or bear a child can create intense psychological turmoil that increases the stress of parenting and compromises mother–child relationships. Both pregnancy-promoting and pregnancy-preventing forms of RCA had implications for mothering, with no clearly predictable pattern for how the different forms of abuse affected participants. The struggles they faced in emotionally bonding with their child/ren and the resentment and guilt this caused were similar to those described by women who have had a child due to wartime rape (Denov et al., 2018; Woolner et al., 2019), as well as women who lost a pregnancy due to medical reasons (Garrod & Pascal, 2018). However, participants in our study faced the additional complexity of being tied (often through having a child) to a partner who continued to abuse them.
Based on our findings, we argue that in mothering after RCA, victim/survivors not only endure emotional trauma and the loss of their autonomy, but they also suffer a form of moral injury. A moral injury is a particular psychological anguish that a person feels when they have been forced to take part in what they perceive to be a wrong or harmful act (Jinkerson, 2016). The concept has been used to understand military trauma (Sherman, 2020) and has recently been applied to the experience of IPV (Salzberger, 2021). Salzberger (2021) has argued that victim/survivors of IPV endure a moral injury when the perpetrator has forced them to witness or take part in harmful acts, such as the neglect or abuse of a child, harm to family pets, or cutting their ties to their friends or family. The victim/survivor must then live with the consequences of the acts and the guilt, regret and trauma of witnessing and/or being implicated in them.
Many of the participants in our study described a similar anguish. In effect, their partner's reproductive abuse put them in a position where they felt emotionally and morally compromised as mothers, while their partner was largely unaffected by the harm he had caused. For many, being forced to bear an unwanted child meant their emotional capacity to bond with their child/ren was severely undermined. As a result, they struggled with a combination of resentment, regret and guilt that they had been made to act in ways that contradicted their own wishes, values and beliefs about how they wanted to mother. Not only did participants feel personally wronged, but they also harbored intense worries that they had wronged their children by not feeling the love for them that they wanted to feel. Additionally, for many, terminating a healthy and wanted pregnancy felt like a wrongful act, even though they had not done so by choice (and even when they supported abortion rights for women in general). They were often left with lingering feelings of grief and guilt, as well as a nagging anxiety that they may lose their subsequent children because they believed they deserved to be punished somehow for having previously ended a pregnancy.
As Salzberger (2021) has argued, the effects of the moral injury of IPV can remain long after an abusive relationship has ended. This was evident for participants in our study, who often endured years of anguish about their mothering and felt they could never be honest with their children about how their traumatic RCA experiences had affected their parenting. Having to keep the abuse secret intensified the resentment and sense of injustice experienced by those women, as it allowed the perpetrator to maintain an image of a “perfect dad.”
Our findings also suggest that idealized cultural expectations of motherhood can intensify the moral harms women suffer after the RCA. Culturally, mothering is constructed as an important signifier of women's value and moral character (May, 2008). Dominant cultural discourses suggest that a good mother must be vigilantly and selflessly devoted to her child's wellbeing and development, while such high expectations are not associated with fathering (Collins, 2020; Hays, 1996; Johnston & Swanson, 2003; Sutherland, 2010). A woman is not only meet impossible standards of maternal behavior but to also feel the “appropriate” maternal emotions. As the comments of participants in our study demonstrated, the “feeling rules” for motherhood frame the experience in idealized terms (Donath, 2015); mothers are expected to feel overjoyed at becoming pregnant, to instinctively and immediately bond with their baby, and to see mothering as their primary source of pleasure and fulfillment (Johnston & Swanson, 2003; Røseth & Bongaardt, 2019). At the same time, feeling unhappiness or regret about being a mother is constructed as a personal failing, rather than being connected to the circumstances in which mothering occurs (Lundquist, 2008; Mauthner, 2010; Røseth & Bongaardt, 2019). These discourses about mothering also shape perceptions of women who terminate a pregnancy, who may be stigmatized as selfish and unfeminine for prioritizing their own needs (Adair & Lozano, 2022; Astbury-Ward et al., 2012; Doran & Hornibrook, 2016). Our findings suggest that these social expectations amplify the moral injury of reproductive abuse, because they not only add to the guilt women suffer for not feeling or acting as a “good mother” should, but they also mean it is taboo for women to speak about their distress and the traumatic experiences that have caused it. Without any way to share their emotional burdens, mothers suffer the injustice of having to conceal their abuse, carry the guilt, and manage the consequences alone.
Paradoxically, our findings also suggest that being able to be a mother after the trauma of RCA can be an emotionally and morally restorative and rewarding experience. Similar findings have been identified in studies on pregnancy as a result of war-time rape; some women in those studies say that mothering provided them a sense of purpose and meaning (Denov et al., 2018; Kantengwa, 2014; Thomson Salo, 2010; Woolner et al., 2019). For some participants in our study, mothering was not only emotionally healing, but also appeared to provide a sense of redemption after the moral injury of RCA. This was evident when participants described feeling that they were able to make up for their perceived wrong doings (and/or wrong feelings) by devoting themselves to caring for their children. That mothers may perceive a need to redeem themselves after being subjected to RCA highlights the complex consequences of RCA and the moral anguish that can be caused by being implicated in actions that were forced upon them.
Implications
Mothers who have experienced RCA may have contact with a range of services, including reproductive, antenatal and postnatal, maternal and child health, and parenting support services. Those who have experienced RCA may be particularly likely to seek professional support for peri- or post-natal depression, as it is associated with both unwanted pregnancy (Barton et al., 2017; Muskens et al., 2022; Qiu et al., 2020) and with IPV (Zhang et al., 2019). In all those services, practitioners can potentially play a critical role. Firstly, practitioners can help to prevent the harmful sequelae of RCA on mothering by supporting women's reproductive autonomy and safe access to contraception, abortion, and pregnancy care. Secondly, practitioners are in an important position to offer emotional support to women who are struggling with the impacts of RCA for their mothering, including the psychological consequences of being implicated in acts that they did not choose. However, our findings indicate that mothers may find it difficult to directly discuss the RCA or its consequences. Research with health care practitioners who have worked with mothers of children born after sexual violence (including rape associated with war, sex trafficking and/or IPV) has also found that although mothers might seek help for their mental health or to manage children's behavior, they tend to be reluctant to talk about the impacts of traumatic reproductive experiences (Meuleman & van Ee, 2021; van Ee & Blokland, 2019; van Ee & Kleber, 2013). Therefore, to encourage disclosure, practitioners need to take a proactive approach and directly ask about their mothering experiences and their history of reproductive experiences with their partner (van Ee & Blokland, 2019). Additionally, our findings indicate that explicitly acknowledging the pressure of living up to idealized social expectations of motherhood may also help women to feel comfortable to share their struggles with mothering.
Our findings also indicate that it is critical for practitioners to create a space for victim/survivors to explore and understand the emotional and moral complexities of mothering after RCA. As Salzburger (2021) has argued, supporting a victim/survivor of IPV may include identifying strategies that help them to make peace with themselves and repair the moral injuries they may have suffered. For mothers who have been subjected to RCA, this may involve exploring how they can live with and address maternal guilt, regret, and resentment. It is also important for practitioners to identify and validate the caring and protective responses victim/survivors have provided for their child/ren, despite the complicated emotions that may emerge after RCA. Additionally, some of the strategies identified by practitioners who have supported women with children born after sexual violence in other contexts (van Ee & Blokland, 2019) may be valuable, such as interventions for mothers and children together (for example, play-based therapies). However, further research with victim/survivors is needed to understand how professionals can best support them to address the complex impacts and injuries of RCA.
Study Strengths and Limitations
A strength of our study was the use of in-depth interviewing techniques, which supported participants to share rich and detailed data about experiences of mothering. The broad range of participant ages (from those aged in their 30 s to those in their 70 s) was also a strength. It meant we were able to capture experiences of parenting children over a considerable period of time. However, we also acknowledge that when RCA occurred a long time ago, it might have been more difficult for participants to recall how it had affected their mothering. Additionally, almost all participants spoke English as their first language; a sample with greater diversity in terms of language and cultural background may provide different data about the impacts of RCA on mothering, due to potential differences regarding ideas about reproductive rights, mothering and women's roles in families.
Conclusion
Through a detailed analysis of interviews with 30 mothers, our study has shed light on the complex ways in which mothering can be affected by RCA. Our findings highlight the emotional, relational, and moral harms that mothers may endure, as well as the efforts they make to protect and care for their children, despite the abuse they have suffered. The study also identifies that a desire to protect their children and a social taboo around talking about maternal unhappiness may make it difficult for mothers to disclose their struggles to others. Our findings have important implications for how healthcare practitioners can assist mothers to share and understand the harms caused by RCA.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Oak Foundation (![]() ) through the Safer Families Centre. The funding body played no role in study design, data collection, analysis, or preparation of the manuscript. The authors wish to acknowledge and thank the participants in the study who generously shared their experiences in the hope of increasing community understandings of the impacts of reproductive coercion and abuse on mothering.
) through the Safer Families Centre. The funding body played no role in study design, data collection, analysis, or preparation of the manuscript. The authors wish to acknowledge and thank the participants in the study who generously shared their experiences in the hope of increasing community understandings of the impacts of reproductive coercion and abuse on mothering.