
Abstract
Depression and intimate partner violence (IPV) are highly related. However, it is unclear what drives this relationship: the form of violence (psychological, physical, or sexual) or its severity. In this study, we first identify patterns of combined forms and severity of violence and then estimate the effects of IPV on depression. We use the DHS and focus on Peru, a country with high IPV rates. Five classes of IPV were identified. The more intense the IPV class, the higher the effect on recent depression. However, the effect on depression tends to be smaller when levels of depression are higher.
Introduction
According to the World Health Organization (2013), 35% of women have experienced physical or sexual violence from their current or former partners at some point in their lives. This highlights the significance of addressing the issue in the context of global public health, as emphasized by Ribeiro et al. (2008).
The effects of intimate partner violence (IPV) have been extensively studied and documented in various research studies (A. E. Bonomi et al., 2009; Campbell et al., 2002; Devries et al., 2013). Depression is one of the most common mental health consequences faced by female survivors of IPV and is reported to affect between 21% and 83% of them in different countries, according to Golding's (1999) meta-analysis. It is important to focus on depression as one of the mental health consequences of IPV, as this form of violence can lead to a range of mental health disabilities (Ribeiro et al., 2008) significantly affecting the lives of women (Ackard et al., 2007; Madruga et al., 2017; T. A. Roberts et al., 2003).
Most studies examining the relationship between IPV and depression have found evidence of a statistical association. This evidence ranges from meta-analyses (Bacchus et al., 2018; Devries et al., 2013; Golding, 1999; Stith et al., 2004) and systematic reviews (World Health Organization, 2013) to longitudinal studies (Armour & Sleath, 2014; Devries et al., 2013; Holmes et al., 2017; Loxton et al., 2017). The relationship between IPV and depression is still a topic of debate, with mixed results regarding which approach, the form of violence or its severity, has a greater impact on the strength of this relationship. Psychological, physical, and sexual violence are considered different forms of violence, while severity of violence is understood as a scale from less to more burdensome aggressions, as defined by the Conflict Tactics Scale. Johnson and Leone's (2005) research indicates that the link between IPV and depression is complex and varies among different groups of survivors, as categorized by IPV typology. This study follows their lead to address the heterogeneity of IPV and its correlation with depression.
Our goal is to build a typology for IPV and then determine how belonging to each class of IPV affects recent depression (within the last 14 days) in survivors. We focus on Peru, which has one of the highest and most consistent rates of physical and sexual IPV in Latin America (30.7%), second only to Ecuador (35.5%) and Colombia (33.3%) (Bott et al., 2012, 2019; Instituto Nacional de Estadística e Informática, 2018). However, most studies on IPV and depression come from Global North countries where IPV prevalence is lower (World Health Organization, 2013). As far as we know, this study is one of the few that examines IPV and depression in a Latin American context and utilizes appropriate methods for creating an IPV typology (latent class analysis) and a quasi-experimental method for determining the relationship between IPV typology and depression (Marginal Mean Weighting through Stratification).
The Relationship Between Intimate Partner Violence and Depression
Depression, Forms of Violence and Severity
Studies have shown that there is a relationship between IPV and depression. However, there is still some uncertainty regarding which type of violence (psychological, physical, or sexual) is associated with depression. While some studies indicate that physical violence triggers depression (Nixon et al., 2004), others suggest that psychological violence, such as dominance-isolation (Hazen et al., 2008), or specific forms of psychological violence (Coker et al., 2005; Ruiz-Pérez & Plazaola-Castaño, 2005) can be the cause. Moreover, compared to psychological violence, some authors argue that physical violence, especially sexual violence, has a more significant impact on depression (Ruiz-Pérez & Plazaola-Castaño, 2005). As these results suggest, there is a pending task for clarifying how different forms of IPV relate to depression.
The contradictory results regarding IPV originate from two different approaches: (a) assuming that the various forms of violence (psychological, physical, and sexual) are independent of their severity, which oversimplifies the complex nature of IPV; or (b) assuming that these forms of violence co-occur, which leads to a flawed generalization of the experience of IPV. These approaches are operationalized using variables to measure the type of violence and its severity. It is important to note that methodological limitations such as cross-sectional data or poorly designed questionnaires may also influence these choices.
Assuming these practical choices—independence or co-occurrence—blurs the actual relationship between IPV and depression, a reason that pushed several scholars to examine this relationship from a different angle, that of IPV severity (Ruiz-Pérez & Plazaola-Castaño, 2005; Terrazas-Carrillo et al., 2016). The severity approach in understanding IPV has been referred to as a dose–response relationship by researchers such as Golding (1999), as severe violence can cause more depression in survivors. However, this approach only considers the level of severity of the violence experienced, disregarding the types of violent acts committed. For instance, two survivors subjected to severe violence could exhibit different levels of depression depending on whether the abuse was mainly psychological or physical. While the severity paradigm has its merits, it is necessary to conduct research that delves into how the combination of the forms of violence and severity of violence can provide a more accurate representation of the IPV experience. This is crucial in enhancing our understanding of the relationship between violence and depression.
These issues underscore the importance of recognizing that both approaches may be integrated to produce different experiences of IPV, which may affect the strength of the relationship between IPV and depression. In this task, it is advisable to follow the literature on IPV typology.
IPV Typology and Depression
Johnson's work (1995, 1999) contributed to our understanding of IPV by analyzing power and control at the dyadic level. Johnson's research revealed that IPV is not a homogeneous phenomenon but a heterogeneous one, exhibiting different patterns of violence where subgroups of survivors share common IPV experiences. These subgroups may have a varying relationship with critical variables such as help-seeking or depression (Johnson & Leone, 2005). Johnson's IPV typology identified two subgroups of survivors, which suggested the need to combine different approaches in future research. The first subgroup, called situational couple violence, involves low-severity violence based on abuse in the absence of controlling behaviors. The second subgroup, intimate terrorism, is based on coercive controlling violence that displays more severe and frequent aggressions that escalate over time.
Johnson's proposed typology for IPV has been a topic of controversy. While he presented it as a solution to the discussion on gender symmetry in IPV, he did not resolve the debate (Conroy et al., 2022; Hardesty & Ogolsky, 2020). Johnson's typology has received criticism for presenting IPV types as sharply defined groups when they actually reflect a continuum (Alexander & Johnson, 2023). Moreover, the typology fails to account for the possibility of individuals changing from one type to another and overlooks the various motivations behind the aggressions (e.g., instrumental, hostile) (Capaldi & Kim, 2007). Additionally, using labels stemming from IPV typologies has been problematic in judicial contexts. For example, the label “situational couple violence” has been used to downplay abuse claims in custody cases (Meier, 2015).
Johnson's work regarding IPV typology has been validated in different settings (Ansara & Hindin, 2010; Carbone-López et al., 2006; Clark et al., 2019; Gupta et al., 2018). More importantly for our purposes, the IPV typology has shown that different patterns of IPV relate differently to depression, questioning the unidimensional relationship between IPV and depression commonly reported (Bauer et al., 2013; Fedovskiy et al., 2008; Gerber et al., 2008; Hazen et al., 2008; Mittal et al., 2018; Ruiz-Pérez & Plazaola-Castaño, 2005). This suggests that different patterns of IPV relate differently to depression. According to Johnson and Leone (2005), studies not following the IPV typology approach may blur the strength of the relationship between IPV and depression, producing even more biased results when using convenience samples (shelters, courts, health care organizations, community health care systems, etc.). While we do not claim that studies that omit the IPV typology paradigm are incorrect, we emphasize that it is challenging to disentangle mixed results from the homogenization of experiences of IPV.
Johnson and Leone (2005) extended the IPV typology framework to examine how the two types of Johnson's typology, situational couple violence and intimate terrorism, affect the mental health of survivors. They found that each type of IPV has a distinct association with depression, which can be attributed to the unique interpersonal dynamics in the relationship, as well as the diverse psychological and social factors that underlie them. These findings are significant for future research as they highlight the importance of considering the heterogeneity of survivors in IPV studies.
As far as we are aware, after the publication of Johnson and Leone's work in 2005, only three studies have investigated the link between IPV and depression by using a previously identified IPV typology (Armour & Sleath, 2014; Carbone-López et al., 2006; Clark et al., 2019). Although these studies have contributed to our understanding, there is still a gap in the literature: the need to explore the relationship between IPV typology and depression using better methods. Moreover, studying this gap in a non-Global North country with a high prevalence of IPV can provide additional insights into the relationship between IPV and depression. In detail, all these three studies combine the form and severity approach as they use yes/no questions to identify if women were (or not) survivors of different acts of IPV that can be ordered in terms of how severe they are (e.g., following the Conflict Tactics Scale). Carbone-López et al. (2006) used latent class analysis on the same data as Johnson and Leone (M. P. Johnson & Leone, 2005) (National Survey on Violence Against Women) and found three classes based on yes/no measures of physical violence, sexual assault, and stalking. Clark et al. (2019) also used the same approach for psychological, physical, and sexual measures of IPV in Nepal, and they found four classes of IPV. Armour and Sleath (2014) used latent profile analysis for a small convenience sample of 318 university students in Northern Ireland. They combined patterns of IPV with parental and global victimization.
Despite several studies on the relationship between IPV typology and depression, a more thoughtful understanding of the relationship between the two is still pending. While most studies indicate that depression tends to be higher when more forms of violence coexist and become severe, only Carbone-López et al. (2006) explored the relationship between IPV and depression by class of IPV. However, it is essential to apply appropriate methods to evaluate the relationship between IPV classes and depression. For example, Armour and Sleath (2014) compared the average depression levels among classes of IPV, while Clark et al. (2019) were more interested in subnational variations in the relationship between IPV and depression, for which they used multilevel modeling. Carbone-López et al. (2006) used multivariable logistic regression models to assess the effect of belonging to an IPV class on depression, controlling for several demographic factors. However, some of their methodological choices are unclear, such as the comparison group and handling confounding variables, leaving room for further research. Johnson and Leone (2005) built their IPV typology using cluster analysis. They then transformed them into dummy variables included in subsequent estimations (logistic regression) to identify the association between IPV and depression. However, such an approach will likely result in selection bias, and comparisons of depression effects within the IPV typology are limited. Therefore, research on IPV and depression would benefit from testing the combination of the form and severity paradigm under more appropriate methods to unveil a better examination of how IPV affects depression along different patterns of an IPV typology.
Current Research
The objective of this study is to construct an IPV typology (based on the form and severity of violence approaches) to subsequently estimate the relationship between IPV and recent depression (in the past 14 days). The study is focused on Peru and uses a household survey (Demographic Health Survey), which is representative at the subnational level. The first hypothesis is that by identifying an IPV typology, it will be possible to discern between different forms and severity levels of violence that survivors experience. The second hypothesis is that the link between IPV and depression relies on specific characteristics that are better captured by combining the forms of violence and severity paradigms. Therefore, we suspect that the association of each class of the IPV typology with depression is scaled, with a weaker association with depression in women in the less intense classes and a stronger association in the most severe ones.
Methodology
Data
We pooled 6 years of the Demographic Health Survey (DHS) in Peru, specifically from 2013 to 2018. This household survey randomly selects women between 15 and 49 years old within selected households for the module on IPV committed by their current or last partner. These questions pertain to different forms of IPV that closely follow the Conflict Tactic Scales-2 (CTS-2). We focused on the urban sample of the DHS, which accounted for 59% of the total sample, as women in rural areas face different risk factors (Agüero, 2018) and constraints that may lead to a different typology of IPV such as reinforced gender stereotypes, deeply rooted justification of violence, distance to State services, and linguistic barriers (Benavides et al., 2015). This resulted in eliminating 11,258 observations (rural women or missing observations) and leaving 16,064 observations.
The sample consisted of all women in the urban area who were asked about depression, regardless of whether or not they experienced IPV. To identify the IPV typology, we did not include sexual violence as the DHS only includes two questions that are insufficient to reflect the diversity of sexual violence acts and would produce an inconsistent typology. We identified an IPV typology using a sample of 6,615 women who had experienced IPV at some point in their lives. The sample used to estimate the impact of IPV on depression is larger (16,064), as it needed to include an additional comparison group of nonsurvivors. The nonresponse rate in the DHS was low (2.9%) and similar to other countries where this survey was conducted (Inner City Found, 2012). After exclusions, the sample maintained its original characteristics (Table 1). Descriptively, most women in the sample cohabited (66%) and had attained high school education (45%). The average age of the women was 33, while their partners’ average age was 36. The women made most of the decisions in the household, including health care, big purchases, visiting relatives, and daily food purchases. Violence was common in their households, with almost half of them (46%) having a father who was violent against their mothers.
Total and Final Sample.
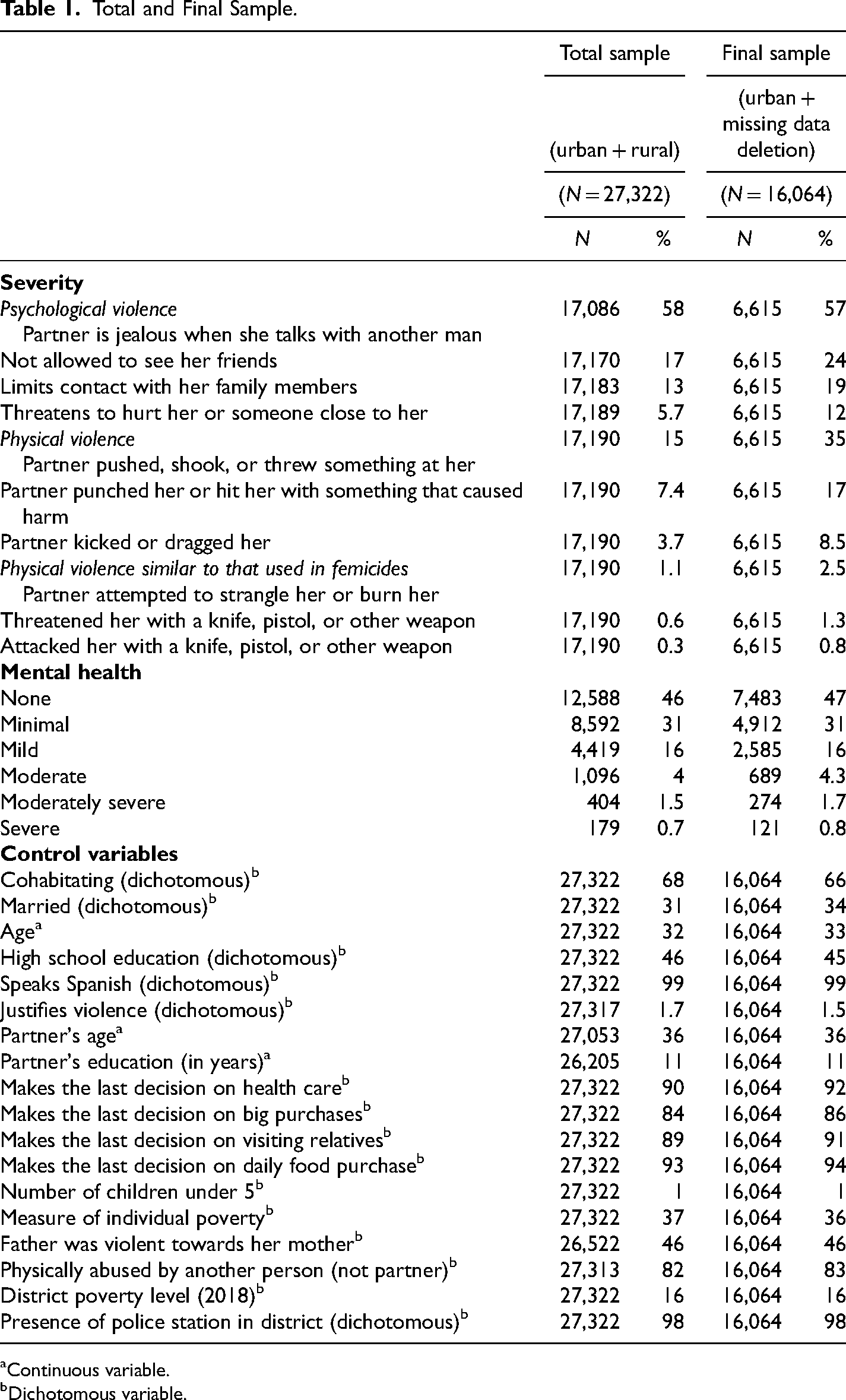
Continuous variable.
Dichotomous variable.
Material and Methods
The construction of the IPV typology
In order to identify the different types of IPV, we used latent class analysis (LCA). This technique helps identify similar patterns among people by creating groups (classes) that are mutually exclusive and homogenous. We applied this method to the context of Peru, using a range of one to six classes of IPV based on previous studies (Graham-Kevan & Archer, 2003; Johnson, 1999; Piispa, 2002) and following the process described by Masyn (2013). In line with prior works (Macmillan & Kruttschnitt, 2005; Percy & Iwaniec, 2007; Siller et al., 2020; Tsuyuki et al., 2020), we chose the optimal model based on different goodness of fit indicators (log-likelihood, Akaike information criterion—AIC, Bayesian information criterion—BIC, adjusted IAC, adjusted BIC, entropy, and Vuong–Lo–Mendell–Rubin adjusted likelihood ratio test. Smaller values indicate a better solution in the information criterion family of indicators. We chose the model with the smallest value, which indicates a better solution in the information criterion family of indicators. We followed the BIC. Nylund et al. (2007) show that when the sample size is large enough (greater than 1,000 observations) and the model to be estimated is not complex (it does not contain continuous variables), BIC is preferred to bootstrap likelihood ratio test (BLRT) as the former adequately identifies the number of classes (this was our case). We assigned each observation to a class based on posterior probabilities for class membership. To assess class separation, we evaluated the entropy values (higher than 0.80 indicates class separation). We also used multinomial logit models to assess class homogeneity, with odds ratios greater than 0.7 or less than 0.3 meaning good class separation. We used these methods to identify the different types of IPV in our study accurately.
LCA was used to categorize women based on a set of indicators that were linked to the types and severity of violence experienced by them. We considered both psychological and physical violence and their respective severity levels (which referred to the accumulation of different types of violence regardless of their form). We followed the approach proposed by Ansara and Hindin (2010) and used four dichotomous variables to measure psychological IPV (with a Cronbach's alpha of .710) and six to measure physical IPV (with a Cronbach's alpha of .664). All of these variables are related to lifetime IPV with the current or last partner. Since the Peruvian DHS closely follows the CTS-2, we adopted its implicit severity scale, which ranks jealousy as the least severe form of violence (57%), while attacks with a weapon are the most severe (1.48%).
The effect of IPV on depression
In order to estimate the effect of IPV on depression within each class, we used Generalized Propensity Score Matching. This technique helped us balance the different groups (“treatments”) based on marginal mean weighting through stratification (MMWS). To classify IPV survivors, we used the posterior probabilities of the LCA model. We then used an adjustment method based on the generalized propensity score for multiple groups (MMWS) proposed by Huang et al. (2005). This method adjusts for estimates while employing inverse probability of treatment weight (IPTW) and clustering on the probability of belonging to each class obtained from multinomial logit models (propensity score). We opted for MMWS instead of using the IPTW directly because the former presents less bias and greater efficiency even in the presence of specification errors in the generalized propensity score model (Hong, 2012; Huang et al., 2005). Using this technique allowed for reducing selection bias risk. The reduced bias in this method is based on two assumptions that have been fulfilled in our case: ignorability, which signals that all relevant covariates have been included in the propensity score estimate (Ho et al., 2007; Stuart, 2010); and that of overlap of the propensity scores, which requires a considerable number of observations.
We used age, relationship to the aggressor (married, cohabitating), education, language, victim-justification of violence, partner's age, and education (in years), decision-making in the home, number of children under 5 years old, as well as history of violent father and violence by a nonpartner as covariates for the generalized propensity score estimates. We also included district-level characteristics to control for local differences associated with violence risk: the percentage of people under the economic poverty line (National Census from 2007) and the presence of a police station in the respondent's district (Census of Police Stations). The choice of these covariates followed the iterative balancing strategy of Rosenbaum and Rubin (1984).
The model was adjusted until a good balance was found and the propensity scores were obtained. Observations were then ordered, stratified, and maintained within the common support to obtain balance within each group. Then, the marginal mean weight was calculated for each observation, and finally, linear regression was performed with depression as a dependent variable. The independent variables were membership (dummy variables) for each IPV class, while nonsurvivors were kept as the base category. Every observation was weighted with the inverse of the marginal mean weight, and the results were reported as an average effect. It is important to note that our results do not imply causation.
Furthermore, depression was measured based on the Patient Health Questionnaire (PHQ-9) (Kroenke et al., 2001), which follows the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) in measuring the severity of depression. The questionnaire consists of nine items related to the presence and duration of depression over the past 14 days, which is referred to as recent depression. For instance, it includes questions like “In the past 14 days, have you had little desire or interest in doing things?.” There are four possible answers, and each answer is assigned a score ranging from 0 to 3 based on the duration and intensity of the symptom. Recent depression was calculated by adding the scores of the nine items and ranges from 0 to 27. Depression was classified as nonexistent (score 0), minimal (score 1–4), mild (5–9), moderate (10–14), moderately severe (15–19), and severe (20–27) based on the defined cut-offs (Kroenke et al., 2001). In our sample, 46.6% had no depression, 30.6% had minimal depression, 16.1% had mild depression, 4.3% had moderate depression, 1.7% had moderately severe depression, and 0.8% had severe depression.
Results
IPV Typology
Table 2 presents the indicators of goodness of fit to select the best solution. In our case, we used a large sample and a noncomplex model, and the BIC performed better than other goodness-of-fit measures. Therefore, we chose the five-class solution. The entropy level of 0.79 is higher than the standard threshold of 0.60, indicating that the classes are well-separated. Table 3 confirms class homogeneity, which shows that individuals are similar within each class, with most estimates being smaller than 0.3 and larger than 0.7.
Model Fit Statistics According to Number of Classes for the IPV Typology.
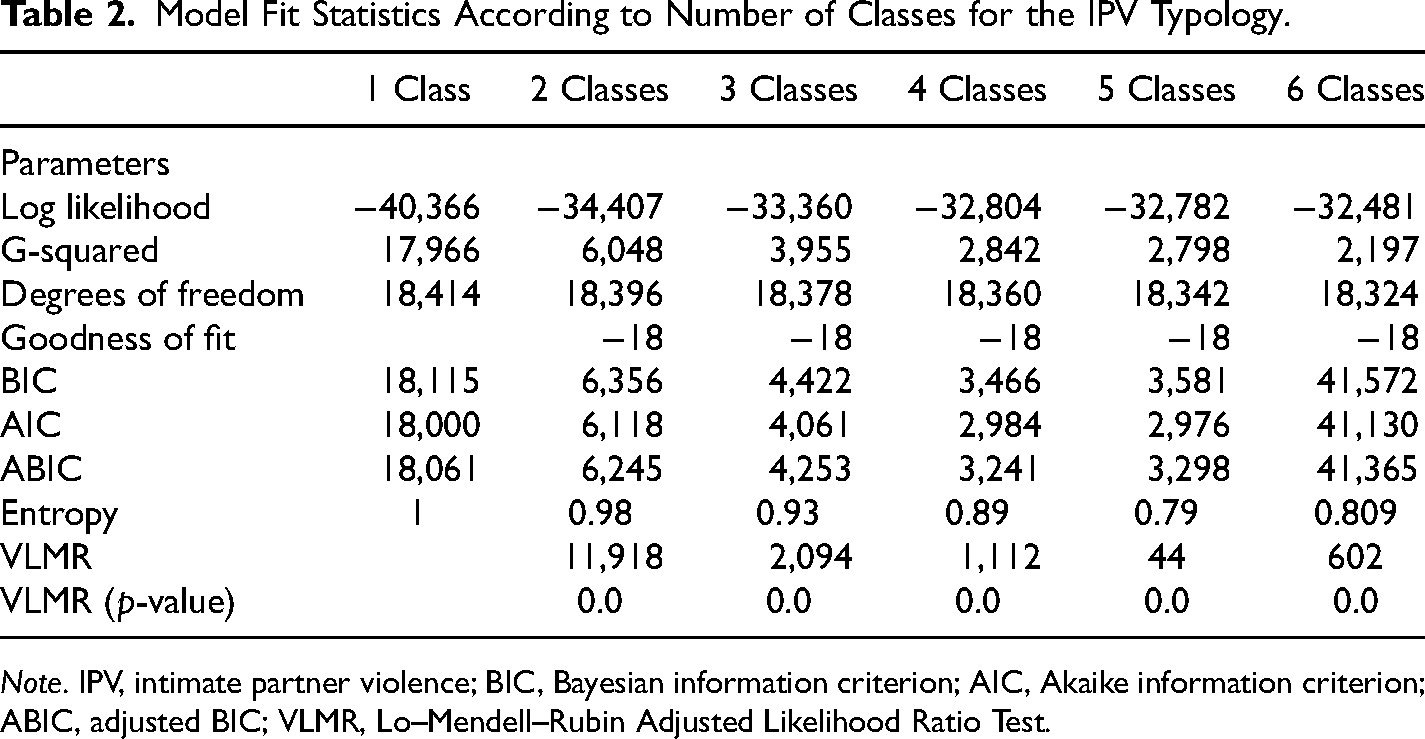
Note. IPV, intimate partner violence; BIC, Bayesian information criterion; AIC, Akaike information criterion; ABIC, adjusted BIC; VLMR, Lo–Mendell–Rubin Adjusted Likelihood Ratio Test.
Evaluation of Class Separation Among Classes in the IPV Typology.
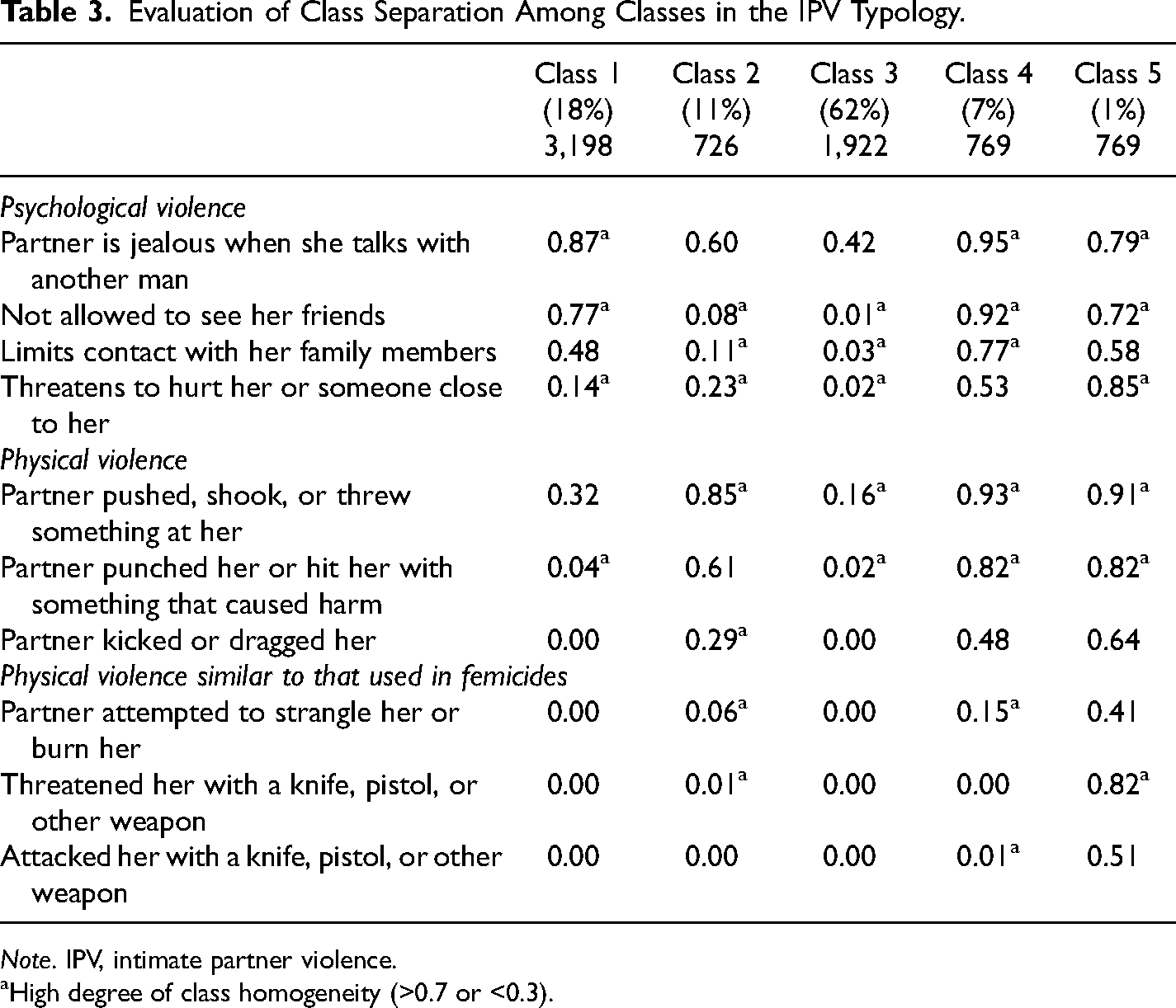
Note. IPV, intimate partner violence.
High degree of class homogeneity (>0.7 or <0.3).
Table 4 presents the prevalence of each variable used to build the IPV typology. The five classes are characterized by a combination of the most common forms of violence and the severity of IPV. Class 1, which represents 62% of the sample, is the least intense and most frequent. This class is defined by the combination of one form of psychological violence (partner is jealous when she talks with another man) and one of physical violence (partner pushed, shook, or threw something at her), with a prevalence of 42% and 16%, respectively. Other forms of violence are less common (<3%). In Class 2, which represents 18% of the sample, the severity of psychological violence increases. Not only is jealousy more common (87%) but also isolation tactics such as not allowing women to see their friends (77%) or family (48%). A substitution effect seems to be reflected when we pass to Class 3 (11% of the sample). In this case, the frequency of the different acts of psychological violence decreases, but the acts related to physical violence increase in number and intensity. For example, 85% of women had a partner who pushed, shook, or threw something at them, 61% were punched or hit with something that caused harm, and 29% were kicked or dragged by their partners. The change for Class 4 (7% of the sample) is an increase in the number of aggressions and their intensity. All forms of psychological aggression are widespread, and physical violence is more diverse. In Class 5 (1% of the sample), there is an increase in the number and frequency of psychological and physical violence aggressions, including near-to-lethal aggressions for the first time in the IPV typology. For instance, 41% of women experienced attempts by their partner to strangle or burn them, 82% faced threats with a knife, pistol, or another weapon, and 51% were attacked with a knife, pistol, or another weapon.
Prevalence of Indicator Variables in Each IPV Class (%).
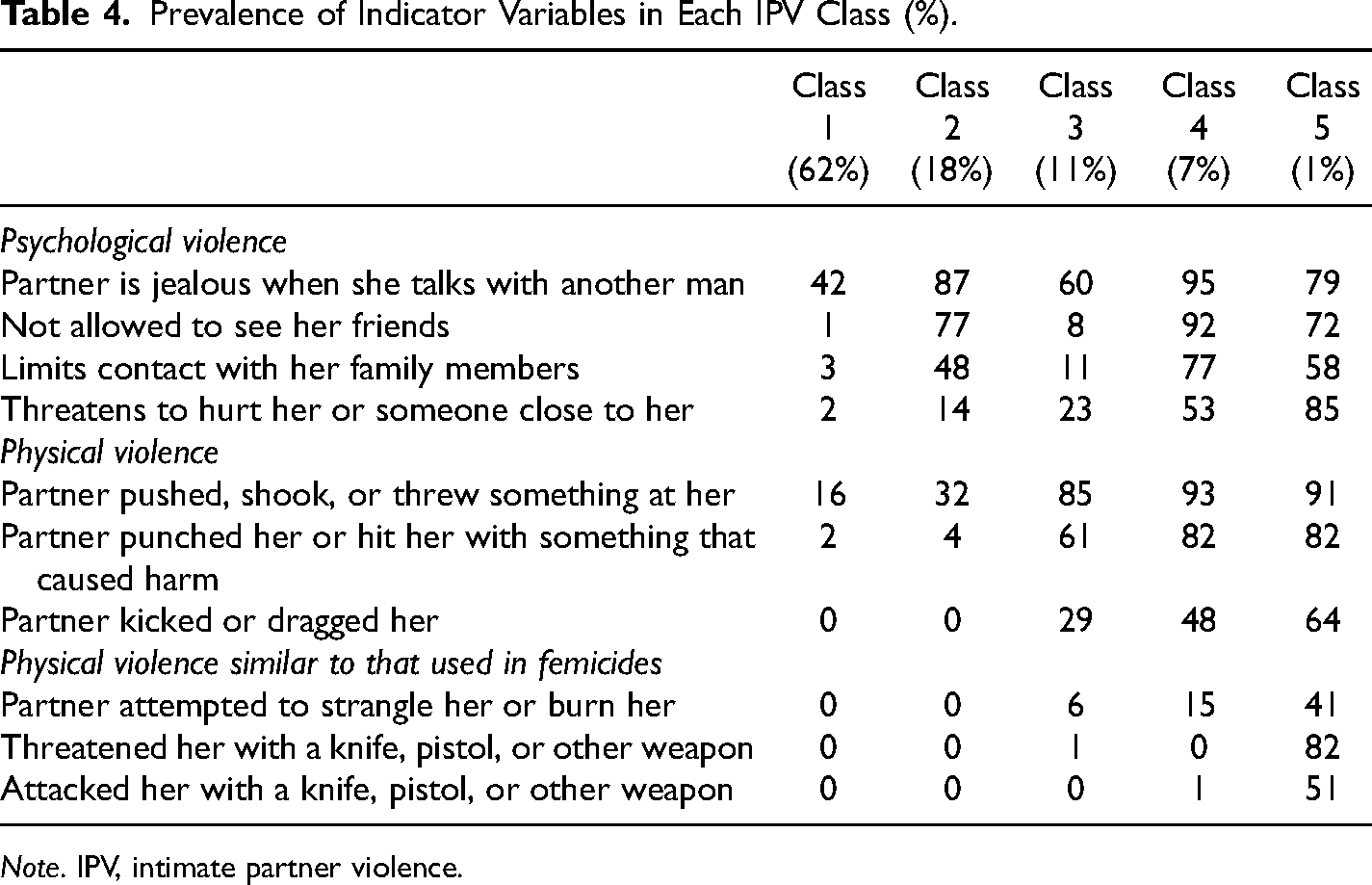
Note. IPV, intimate partner violence.
The Relationship Between IPV and Recent Depression
The average levels of recent depression for each IPV class are presented in Table 5. The table shows that as the intensity of IPV increases (from Classes 1 to 5), severe depression tends to be more common, but not always linearly. Among nonsurvivors, 59.5% have no depression at all, and 28.1% have minimal levels of depression. Most survivors present minimum levels of depression (ranging from 26.2% to 36.0%). However, the two most intense classes show that most survivors face mild depression (35.3% and 36.3%, respectively).
Average Depression by IPV Class (%).
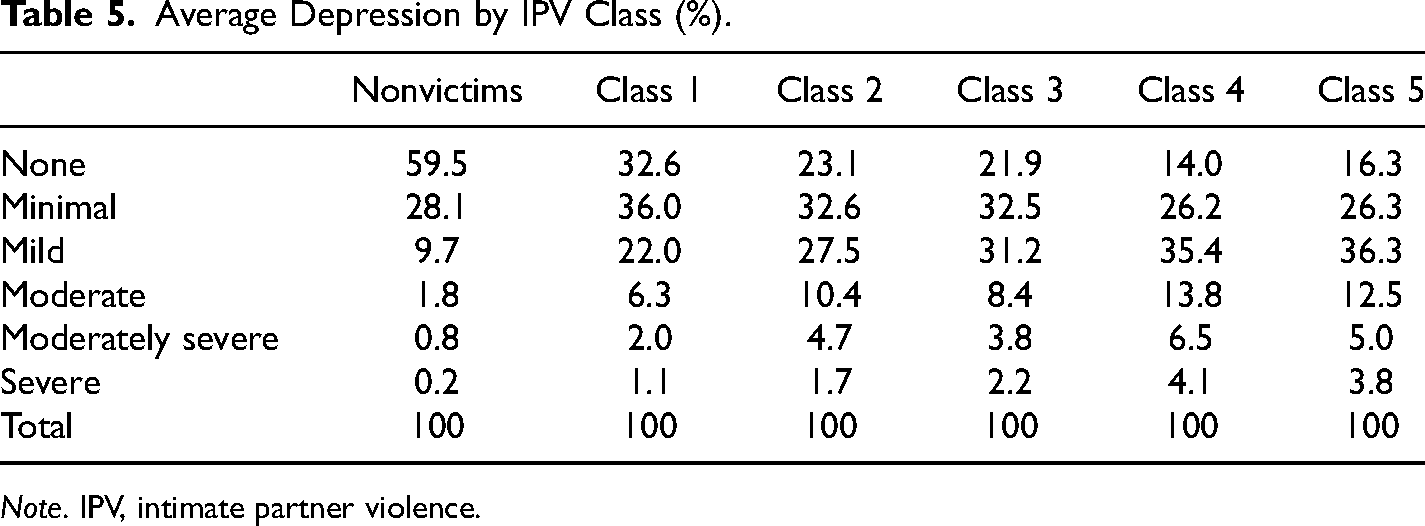
Note. IPV, intimate partner violence.
Table 6 presents the results of the effect of belonging to an IPV class on recent depression compared to not having experienced violence. The results show that IPV has a significantly higher effect on recent depression across all classes compared to nonsurvivors. The comparison across classes demonstrates that the association of IPV with depression increases as the class experiences an increase in forms of violence and severity. Within each class, the effect of IPV tends to be smaller as depression severity increases from minimal to severe.
Effects of Belonging to Each IPV Class on Recent Depression.
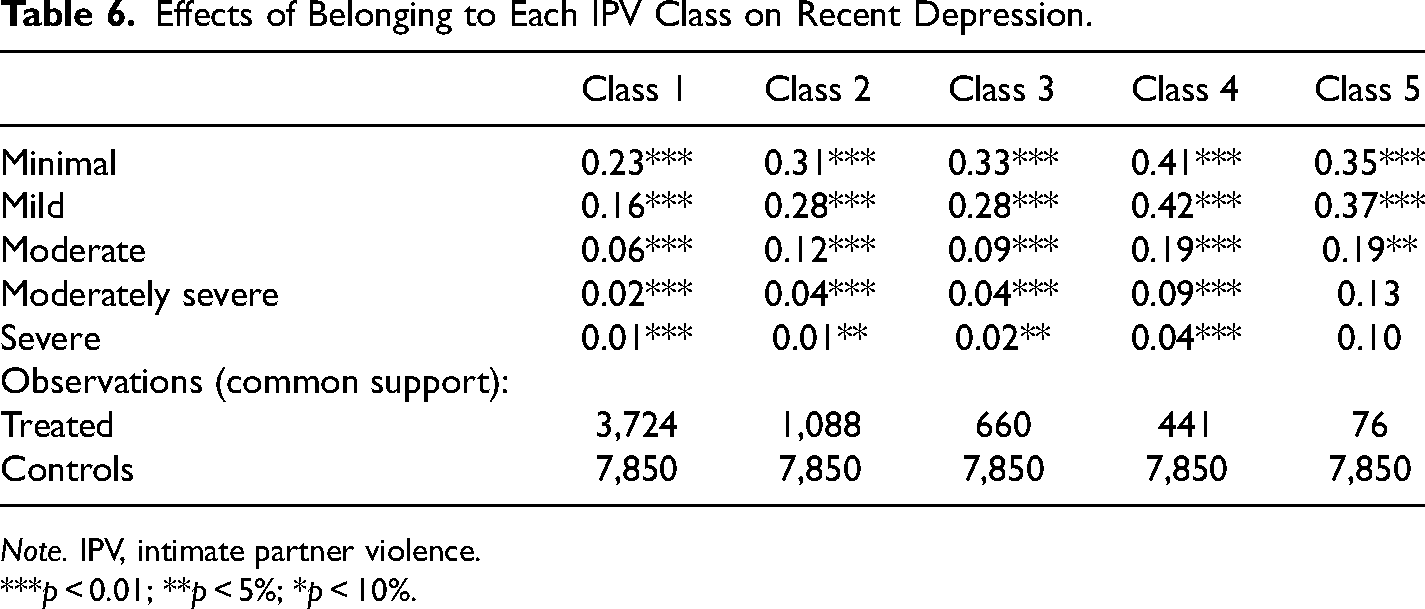
Note. IPV, intimate partner violence.
***p < 0.01; **p < 5%; *p < 10%.
For example, across the first three classes (columns 2–4), the probability that a woman experiencing IPV presents recent minimal depression is 23 percentage points (pp), 31 pp, and 33 pp higher than nonsurvivors. On the other hand, the effect of IPV on recent severe depression is 1 pp, 1 pp, and 2 pp, respectively. The relationship is slightly different for Classes 4 and 5, for which the largest coefficients are on mild depression symptoms (42 pp and 35 pp compared to nonsurvivors). However, it still gets smaller as depression severity increases.
Discussion
This study aimed to construct an IPV typology (based on the forms of violence and its severity) for the Peruvian context and subsequently estimate the effect of belonging to each class on recent depression (past 14 days). As far as we know, it is one of the few studies on IPV typology and depression in Latin America.
In line with prior results, our findings suggest that instead of treating IPV as a homogeneous phenomenon, it is better to consider it heterogeneous. We identified five IPV classes based on the combination of forms of violence (psychological and physical) and their severity (number of aggressions in each form). The differences across our classes of IPV seem substantial, qualitatively speaking. For instance, Class 1, the least severe class, differs from Class 2, the next class, by including isolating behaviors, which suggests an aggressive escalation in the perpetrator's control strategies. Comparing the second and third classes shows a significant increase in the frequency of physical aggression. Lastly, comparing classes to the most severe one (Class 5) stresses the salience of the intensity of physical violence, as well as the physical aggressions (burns, strangulation, and use of weapons) that are common in femicides.
Our resulting typology follows previous findings. Classes 1 and 5 in our IPV typology are similar to Johnson's situational couple violence and intimate terrorism (Johnson, 1995, 1999), respectively. These groups have also been validated in later studies (Cale et al., 2017; Graham-Kevan & Archer, 2003; Piispa, 2002). Moreover, our results suggest that there is a significant variation in the intensity and use of psychological abuse and physical violence. In line with prior studies (M. Johnson, 1999; Leone et al., 2004), this variation indicates that the combination of forms of violence is used to exert general control over one's partner.
Our results extend this literature by signaling four critical features in the IPV typology. Firstly, the combination of forms of violence. Psychological and physical violence combine to produce different classes of women survivors of IPV, which suggests that facing IPV is better captured by distinguishing experiences of violence. Secondly, the increase in the number of aggressions for each class builds the idea of a scaled intensity of violence. Passing from Class 1 to Class 5 implied that the number of aggressions increased, which is an interpretation of how severity also becomes a more salient trait of experiencing IPV. Thirdly, there is a substitution effect between psychological and physical violence. Even though the previous point suggests a linear relationship between class and IPV (the higher the class, the more severe the violence), this association is not uniform. The differences between Class 2 and Class 3 were characterized by less psychological violence but more physical, which may suggest perpetrators’ tactics to control their partner, different types of perpetrators, strategic use of violence, or other meanings that future research should address. Fourthly, the most intense class includes aggressions similar to femicides. Our results recognize that psychological and physical violence combine at different levels to reflect experiences of IPV across the classes in our typology. Future cross-country research will help assess the stability of typologies in different cultural settings.
We found that the IPV classes are related to recent depression. The association between a higher intensity of IPV and depression along the classes of IPV suggests that what matters is not necessarily the form of violence (psychological or physical) or its severity but their combination. For most women who experience IPV, violence may be intermittent, with long periods of no physical violence, in which moments of tension are probably interspersed with moments of peace. This notion of interrupted violence is similar to that of Roberts and Roberts (2005) in their study of IPV typologies. It would be helpful to extend this finding and examine the triggers of violence as well as the process and rhythm of tension accumulation in couples, given these interspersed acts of violence.
Our study on IPV allowed us to develop a typology that identifies various classes of IPV and their association with depression. We found that belonging to any class of IPV is related to depression, with a stronger impact as the class increases in intensity. Within each class, the effects tend to be smaller as depression severity increases.
Having uncovered an IPV typology, our findings also highlight that belonging to any IPV class is related to depression; these effects tend to be stronger as the class increases in intensity, and within each class, the effects tend to be smaller as depression severity increases.
By building an IPV typology and using quasi-experimental methods, our results foster three interpretations that may help to clarify the mixed results in the literature on IPV and depression. Firstly, as physical violence intensifies, the association between IPV and recent depression gets larger. This indicates that physical violence plays a significant role in depression and may explain why physical violence has a more substantial impact on depression than psychological violence (Coker et al., 2005; Hazen et al., 2008). However, psychological violence is also significant as it is somatized (Hazen et al., 2008) and lasts longer over time (Loxton et al., 2017; Loxton & Schofield, 2006), even after the relationship has ended (Kernic et al., 2003). Psychological violence interacts with physical violence, which produces the results mentioned above.
Secondly, the most intense class (Class 5) of IPV is linked to an increased association with depression due to the severity of physical violence and the risk of death. Here, 25% of survivors have experienced violent acts similar to most femicides in Peru (Defensoría del Pueblo, 2015). Women who experience intense violence have a lower probability that their individual and community resources can absorb the effects of violence on depression, with a higher likelihood of perceiving that their life outcomes are uncontrollable (Coker et al., 2005). Thus, severe violence is a physical phenomenon produced by aggression and a social one framed within larger ecological relationships.
Thirdly, the probability of experiencing depression likely interacts with interruptions to physical violence. Long periods between violent acts could bring the survivor to normalize sporadic violence and become comfortable with the idea of long, peaceful periods between explosions of violence. Nevertheless, the inverse may be true. In relationships with frequent and severe aggressors, the presence of fear, entrapment, and the feeling of not being able to escape has been highlighted (Devries et al., 2013), which exposes the survivors to continuous depression, reducing their sensitivity to new depressive stressors (La Flair et al., 2012). Returning to the case of intermittent IPV, it is possible that these acts of violence catch the survivor unaware, and with fewer psychological (coping mechanisms) and social (networks) resources to react in the face of violence and to deploy useful strategies to prevent the violence or leave the relationship.
Our findings have implications for addressing services for IPV survivors and perpetrators. Early detection of IPV is crucial as depression has short- and long-term consequences. Screening tools combined with depression diagnosis can help address health consequences, design safety planning, and promote reporting of cases to the criminal justice system. As depression can make survivors’ decision-making processes more complex, bystanders’ programs would enhance the possibility of detecting violence and avoiding escalation (Coker et al., 2005). Therefore, solutions must consider the heterogeneity of survivors rather than their universality.
Though we use data on survivors, our results suggest some prevention and intervention implications for perpetrators. Assuming that perpetrators’ motivations and use of violence differ across the classes of IPV typology, batterer intervention programs can vary in effectiveness. Solutions must also be diverse. For instance, incorporating trauma or substance abuse components into these programs is more effective, which can reduce violence and indirectly alleviate depression in IPV survivors (Karakurt et al., 2016). Mixed results in gender-role-based batterer interventions may also be explained by perpetrators’ different motivations and uses of violence. This creates the need to consider, for example, other effective approaches ranging from providing behavioral, communicational, and conflict-solving tools for couples (Braithwaite & Fincham, 2014) to promoting emotional- and behavioral-skills enhancement programs (acceptance and commitment therapy) for perpetrators (Zarling et al., 2015). According to a comprehensive review by Crane and Easton (2018), addressing the heterogeneity of perpetrators would benefit from programs that incorporate risk assessment tools to identify appropriate treatments and develop strategic uses of integrated treatment models.
This study is not free of limitations. Our results are produced by a quasi-experimental method for cross-sectional data; hence, causality cannot be established. It would have been ideal to control for baseline levels of depression. However, our data did not include a panel of respondents or retrospective questions. These would have been useful to control for cases where depression precedes IPV or behavioral responses that anticipate aggression. As sexual violence questions in our data were not appropriate to capture this phenomenon, a larger span of these aggressions could help deepen their relationship with depression. Regarding the variables used, our study is limited to how the DHS formulates psychological and physical violence questions that may hide specific violence manifestations. Our severity measure was based on the implicit severity scale of the CTS-2, which ignores the varying and possible nonlinear harm each act may inflict. In addition, the CTS-2 lacks context when exploring IPV (Jones et al., 2018) and assumes a hierarchy of conflicts that may not always hold. The IPV typology literature would benefit from comparing results using alternative measures. On the methodological side, although we followed clear rules for assigning women to each class in our typology based on the posterior probability, our results could be sensitive as they ignore the error in assigning subjects to classes (Masyn, 2013). Finally, it is important to note that our IPV types are mutually exclusive categories and do not recognize the possible continuity within and across different types.
Although there are some limitations, the current study has helped us to understand the connection between IPV heterogeneity and depression beyond the approach of forms and severity of violence. Our findings have enabled us to contribute to the literature in three ways. Firstly, depression can be extensive and varied across different classes of an IPV typology, which will improve our theoretical approaches to this subject. Secondly, by using appropriate techniques to identify our IPV typology and capturing its relationship with recent depression, we have advanced our understanding of the mixed results in the existing literature. Finally, while our results align with the literature in high-income countries, we need to consider if cultural differences can explain our findings. For instance, previous research in Peru has suggested a link between violence and its justification in women, as well as sexism in aggressors (Hernández & Morales, 2019) in a context of precariousness that, when combined, could exacerbate previously identified risk factors.
Finally, given that using IPV typologies improves our capacity for problematizing and proposing effective solutions, our results suggest important clues for public policy. Public policy and services for IPV survivors, such as public safety planning and survivor interviews, should be customized to suit the various needs of different survivors. Health care establishments should also consider universal screening to identify and differentiate women based on different IPV classes. However, screening alone is insufficient if there is no adequate health care system or medical personnel to improve diagnosis (Duxbury, 2006). Specialized training for medical personnel can improve their abilities to identify, respond to, and authenticate violence in women and should also be tailored to aid in identifying different classes of survivors (Danley et al., 2004; Feder et al., 2011). It is important to note that improving services does not solve the ethical dilemma of detecting violence and later reporting it or leaving it in the hands of the survivors as much as is legally possible (Duxbury, 2006; Feder et al., 2011). Therefore, the criminal justice system should consider the different needs and risks that each woman experiences based on her specific situation. Health professionals should also deepen their understanding of the complex nature of violence and avoid negative behaviors by being nonjudgmental, nondirective, and individually tailored in their care (Feder et al., 2011), aspects that could be addressed using coordinated public interventions.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.