
Abstract
Outreach is an important approach to improve health and social care for women experiencing street involvement (SI) or gender-based violence (GBV). Few studies have examined outreach approaches that incorporate SI and GBV. Drawing on feminist theories and principles of community-based research, we detail an inclusive co-design approach for an outreach intervention considering these interrelated contexts. Women with lived experience, researchers, and service leaders drew on research and experiential knowledge to define outreach engagement principles: tackling GBV, personhood and relational engagement, trauma-informed engagement, and harm reduction engagement. The resulting intervention integrates these principles to enable building and sustaining relationships to facilitate care.
Keywords
Background
Women who experience street involvement (SI) are regularly at the severe end of the spectrum for gender-based violence (GBV) severity, duration, and type (Boyd et al., 2018; Oppal, 2012; Parker & Leviten-Reid, 2022). They are also more likely to be killed and continue to experience violence throughout their lives when compared to other groups of women (Davies et al., 2015; Oppal, 2012). SI is a broad concept that infers significant structural disadvantage including poverty, precarious housing, an inequitable burden of mental and physical health challenges, and problems receiving health and social care that aligns with people's needs (Bungay, 2013). SI may similarly include high degrees of public visibility, problematic drug use, minimal connections to social support, and criminalization associated with survival strategies such as stealing, sex work, and drug dealing (Bungay et al., 2010; Higgitt et al., 2003).
The interrelationships between GBV and SI contribute to catastrophic health and social inequities for women, for instance, poverty, homelessness, isolation, depression, posttraumatic stress disorder, traumatic brain injury, and premature death (Boyd et al., 2018; Hayashi et al., 2016; O'Connor et al., 2022; Stubbs et al., 2022; Wallstam et al., 2017). Despite these pressing problems, women encounter considerable challenges in receiving appropriate and timely health and social care (Bungay, 2013; Kneck et al., 2021; Maulsby et al., 2015). Siloed care models that overlook complexity and compartmentalize women's health and social concerns, lack of care providers, and ongoing violence (e.g., controlling partners) are notable barriers to women's engagement in care (The Women's Coalition, 2014; Vancouver Coastal Health, 2016). Additionally, stigma and discrimination within care provision (e.g., labeled as “drug seeking”) contribute to disrespectful, unsafe clinical encounters and mistrust in care, thereby exacerbating barriers to care. Paternalistic ideologies of deviance and/or those that infantilize women as victims requiring rescuing and who are unable to enact agency reportedly underpin discrimination and contribute to negative social judgment in care encounters (Bungay, 2013; Maulsby et al., 2015). Consequently, women may be reluctant or unable to engage in care until a crisis occurs, rendering high rates of Emergency Department utilization and mortality (Kneck et al., 2021).
Outreach is a commonly employed strategy used by nurses, social workers, and other allied service providers to support women experiencing SI or GBV to engage with care (Jiao et al., 2022). Within a street-involved context, outreach is consistently contrasted with traditional site-based services, occurring in community settings where people spend their time such as parks, drop-in centers, and on the street (Sarradon-Eck et al., 2014; Small et al., 2012). It is described as a flexible and accessible option to engage with people who may be mistrustful of care providers and experience other related barriers (Maulsby et al., 2015; Rowe et al., 2016). Street-involved outreach services regularly include harm reduction supply distribution, health promotion education, crisis intervention, and linkages to emergency shelter, mental health care, and emergency first aid (Jiao et al., 2022; Rowe et al., 2016; Wagner et al., 2020). Outreach has been shown to be effective in building relationships between people experiencing SI and service providers with documented benefits of improved access to housing and reduced drug-related harms (Guo & Slesnick, 2017; Small et al., 2012; Wagner et al., 2020).
GBV-specific outreach interventions have primarily emphasized women experiencing intimate partner violence (IPV). Unlike street-involved outreach, IPV-related outreach commonly occurs in the home, relying on “population” lists generated from emergency shelters, the criminal justice system, and community health centers to determine “who” to target (e.g., McGinn et al., 2019; Murphy et al., 2023; Rodgers et al., 2017; Stover et al., 2009). Advocacy, emotional support, safety planning, and ensuring women's attendance at criminal court proceedings involving a violent partner are activities reported in IPV-specific outreach (Stover et al., 2009). Growing evidence illustrates the beneficial effects of reduced psychological distress symptoms, reduced violence, and improved physical and emotional functioning (Lhussier et al., 2016 Rodgers et al., 2017). While evidence of outreach effects has demonstrated promising results, minimal attention has been paid to designing and testing outreach interventions among women experiencing both GBV and SI. Given the well-substantiated GBV crisis among women experiencing SI (Kneck et al., 2021), there is an urgent need to develop outreach interventions that simultaneously consider the interrelationships between GBV and SI, the root causes, and related affects.
Purpose
In this article, we describe how, through a community–academic partnership, we co-designed a strengths-based, women-led, outreach intervention aimed at enhancing health and social care among women experiencing GBV and SI in an urban setting. We specifically illustrate how we took up principles of community-based participatory research (CBPR), intersectional feminist perspectives on gender equity and violence, and grassroots activism to determine our co-creation processes. We also detail how we drew upon our collaborations to identify the equity-oriented, strengths-based intervention principles that ultimately informed the core elements of an outreach intervention later tested in pilot research (see Bungay et al., 2021).
Study Setting
To situate our study, we first describe the community environment in which our project occurred. The materials used in this discussion were drawn from a multistage, CBPR pilot study known as the STRENGTH Project that occurred between 2017 and 2020. The larger project aimed to assess the acceptability and feasibility of an outreach intervention to build trust, sustain relationships between an outreach team and women experiencing SI and GBV, and enhance women's navigation within health and social care. We use the terms woman/women as inclusive of anyone who identifies as a woman. The research occurred in the ancestral and unceded territories of the xʷməθkʷəy̓əm (Musqueam), Skwxwú7mesh (Squamish) and Səl̓ílwətaɬ (Tsleil-Waututh) in what is commonly referred to as the downtown eastside (DTES) neighborhood of Vancouver, Canada. The DTES is approximately 4 km2, east of the city center and accounts for 3% of the City's population (Provincial Health Services Authority [PHSA], 2020). There are an estimated 19,960 residents in the community, 42.1% of which are female. Almost 10% of the residents identify as Indigenous, 1 compared to 2% across the city as a whole (City of Vancouver, 2020). It is well known that Indigenous people disproportionately experience violence as a direct result of colonial, racist structures, including the Indian Act, the Sixties Scoop, and residential schools (National Inquiry into Missing and Murdered Indigenous Women and Girls [NNMMIWG], 2019).
The DTES is among the poorest communities in Canada. Over 79% of people rent their current dwelling (PHSA, 2020); one in 18 residents is homeless; and food and income insecurity are severe (Wallstam et al., 2017). This community is also deeply affected by the toxic drug supply crisis. In January 2022, British Columbia reported 207 unregulated drug toxicity deaths, which is the equivalent of 6.7 deaths per day (Ministry of Public Safety and Solicitor General, 2022). While reporting processes make accurate numbers difficult, it is assumed approximately 67 of these deaths occurred in this small neighborhood.
Women face a disproportionate burden of violence associated with historical and ongoing gendered and racialized violence (Boyd et al., 2018; Oppal, 2012; The Women’s Coalition, 2014). In 2012, 16% of sexual assaults reported in the City of Vancouver occurred in this small neighborhood (City of Vancouver, 2013). Women within the DTES are among those who have been murdered or gone missing within British Columbia since the 1970s; a direct result of serial killers targeting women experiencing severe marginalization and SI and a lack of societal response to the intentional targeting of women in these crimes (Oppal, 2012). While there is a plethora of public and not-for-profit services attending to primary care and basic needs (e.g., low-cost meals, bathrooms, showers), women continue to experience gendered barriers to care (Vancouver Coastal Health, 2016). Gendered violence, exploitation, and abuse are common in co-ed services and women-specific services are often inaccessible or unable to meet women's needs, particularly concerning mental health and trauma care (Vancouver Coastal Health, 2016; Wallstam et al., 2017).
Perspectives on Community-Based, Participatory Research
Before detailing the methods used in our co-design process, it is important to situate our work and the rationale for adopting a CBPR approach. Extant evidence indicates that health and social care interventions that embrace a community engagement approach in design and implementation can have a more positive effect on a range of health outcomes across varying health and social concerns (O’Mara-Eves et al., 2015). CBPR is recognized as an important and respectful research approach for community engagement, particularly with communities grappling with structural disadvantage and related health and social inequities (Belone et al., 2016; Wallerstein et al., 2018). CBPR involves a commitment to addressing community-identified priorities, research that attends to the sociohistorical context of the community and its members, and shared decision making throughout the research endeavor (Wallerstein et al., 2018). CBPR approaches attend to power and safeguards that the processes by which research questions are generated and how the research is carried out serve to advance equity, inclusion, and social justice among community members (Bell & Reed, 2021; Culbong et al., 2022; Wallerstein et al., 2018). Considering the documented benefits of outreach and the urgent need to address barriers to care among women experiencing GBV and SI in ways that are safe, appropriate, and feasible, CBPR approaches offer great potential for enhancing intervention feasibility and acceptability that may ultimately enhance women's health and well-being.
Co-Design Methods and Process
The co-design process occurred iteratively and was informed by an established partnership between the executive director (LD) of the Inner-city Women's Initiatives Society a not-for-profit women's service organization and VB; a researcher specializing in GBV and women's health. In keeping with the principles of CBPR (Belone et al., 2016; Wallerstein et al., 2018), we sought to respond to the well-established need for the intervention that had been identified in earlier community-led research and consultations with women living in the DTES concerning safety and health and social care (see Bungay, et al., 2010; Vancouver Coastal Health, 2016; Women's Coalition, 2014). We also adhered to the CBPR principles of meaningful inclusion and the valuing of multiple sources of knowledge (Culbong et al., 2022) and drew upon our shared commitment to an outreach intervention that considered intersectional feminist perspectives on gender equity and violence. As detailed in Figure 1, these principles and commitments enabled us to come together to determine the steps in our process that facilitated the inclusion of people with a range of perspectives and multiple and varied sources of knowledge. In the subsequent discussion, we detail how we engaged with CBPR principles to create the team that would undertake this work and the iterative processes of knowledge development and sharing that ultimately led to the co-design framework presented in Figure 1.
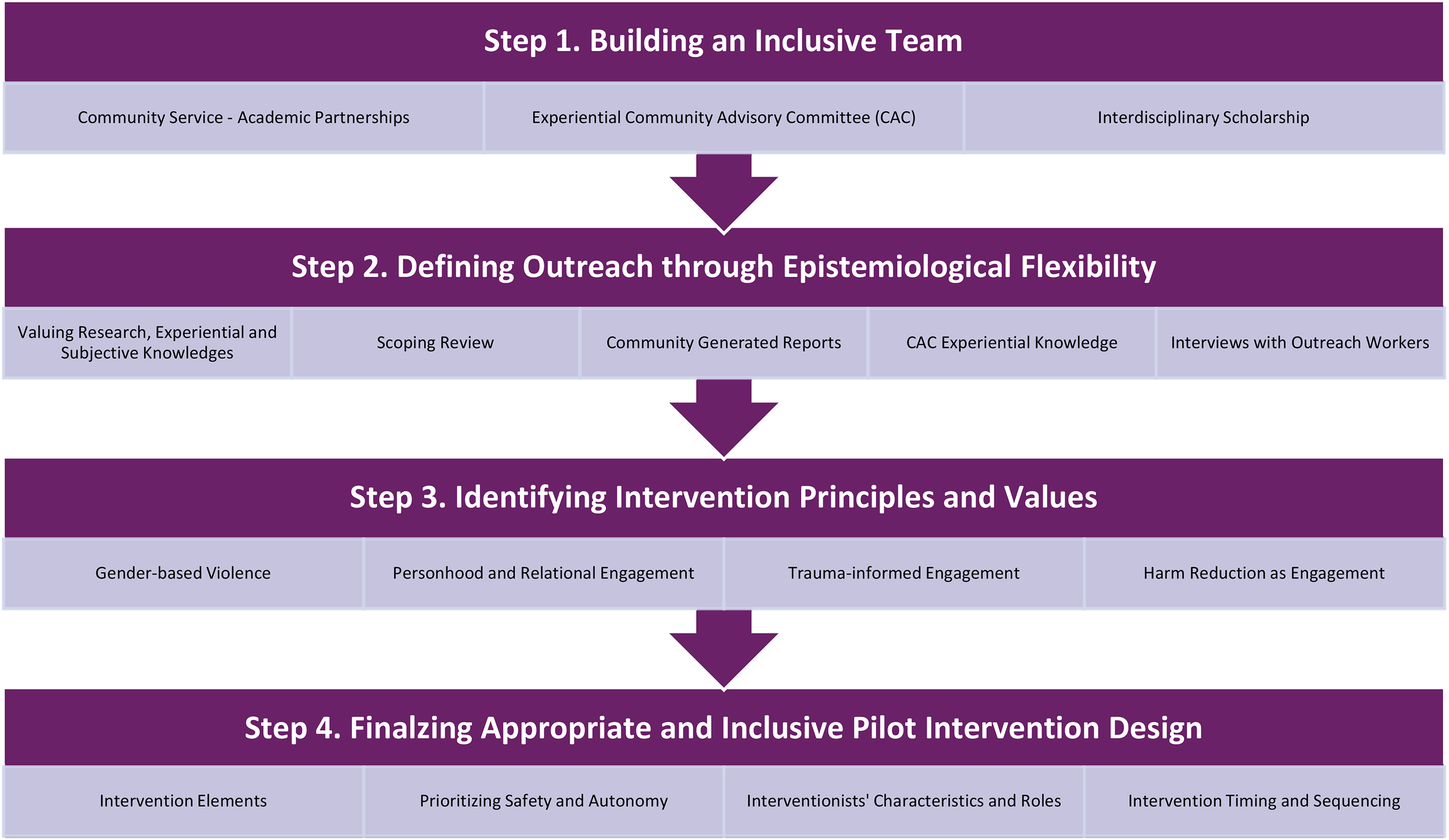
The co-created design process/framework.
Step 1. Building the Team
Identifying the range of perspectives and experiences necessary to inform the co-design process and recruiting study team members was an essential first step to ensure our project was inclusive of the range of experiences and knowledges necessary for this work. VB and LD collaboratively identified three partnering organizations in health and social care, legal advocacy, and family welfare they deemed critical to inform an outreach intervention that could provide a comprehensive and integrated approach to women's health and social care needs. Meetings were held with each organization and three leaders/staff agreed to join the research team. Memoranda of Understanding was created between the research and community organizations to solidify our responsibilities and commitments to one another and the work.
CBPR also seeks to redress the marginalization and exclusion of community members in the design and implementation of research (Culbong et al., 2022; Switzer et al., 2019). Therefore, a community advisory committee (CAC) was created to facilitate authentic engagement with women who have expert knowledge of the everyday realities of women in their community. Four women with shared lived experience of GBV and SI who lived in the community were invited to participate. All women had preexisting relationships with the community lead. To foster CAC safety, address barriers to engagement, and build trust between researchers and community members (Bell & Reed, 2021), the CAC also included a service leader and one support worker known to CAC members who facilitated members’ participation and well-being throughout the study. They specifically provided mentorship and transportation and engaged in regular wellness checks and ongoing support for health and social care.
We collaboratively developed CAC Terms of Reference concerning contributions, membership, compensation, and engagement activities. The CAC met 44 times and decisions were documented in meeting minutes that served as a data source for the project. CAC members received financial compensation to attend meetings, review materials, and develop and participate in outreach worker orientations. To complete the team, three additional health and social science researchers with programs of research in mental health, addictions, GBV, and improving care access for women experiencing SI were recruited to help inform instrumentation and analytic approaches for pilot testing.
Step 2. Defining Outreach: The Need for Epistemological Flexibility
One of the teams’ first tasks was to define outreach. We intentionally grappled with epistemological ideas about knowledge, noting the importance of recognizing, valuing, and integrating our team members’ varied knowledge bases including research, subjective, and experiential knowledge (Bell & Reed, 2021; Culbong et al., 2022). We applied an iterative approach, moving back and forth between various knowledge sources to achieve our aims.
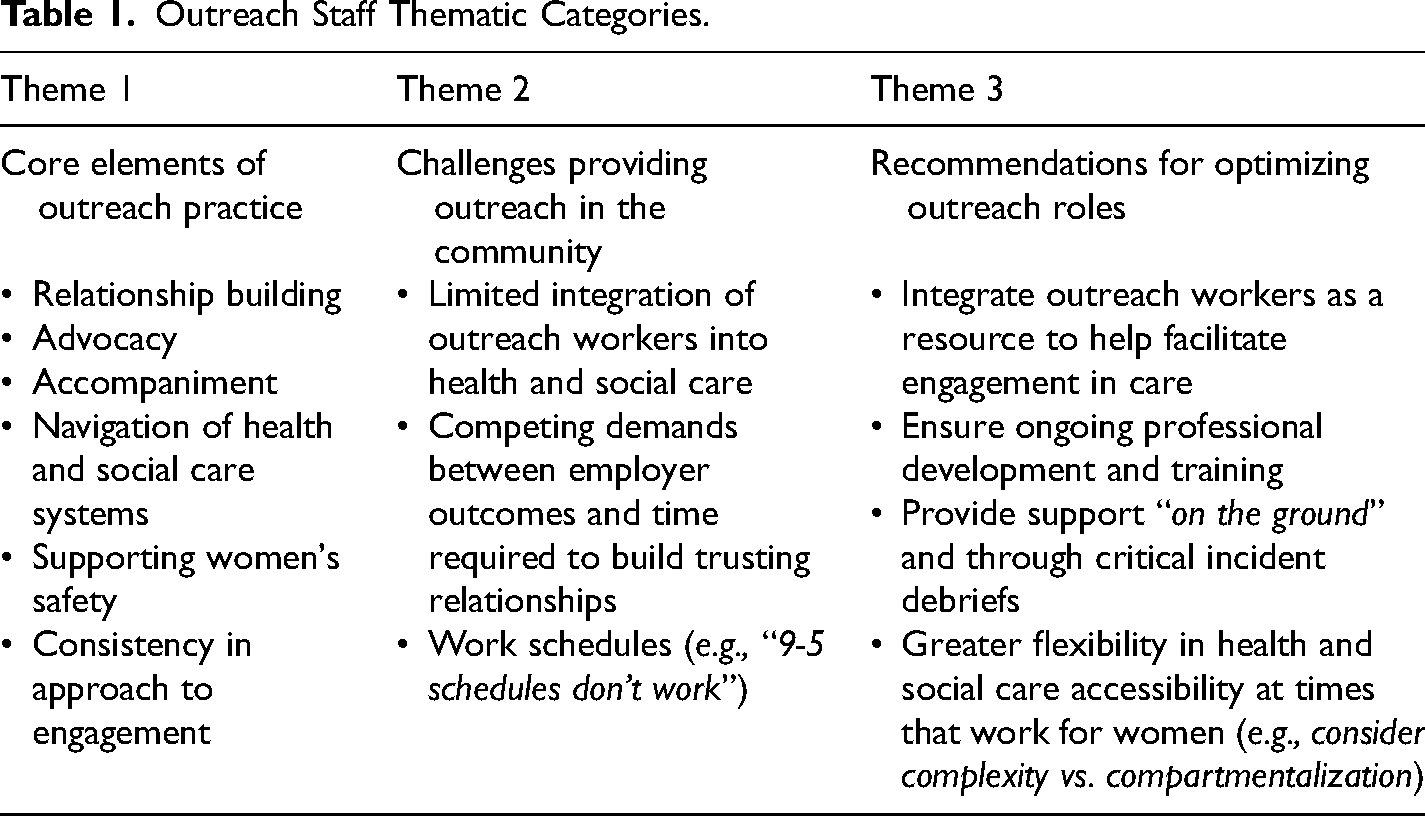
Research knowledge about GBV, women's health, and outreach practice was synthesized and discussed among the team. To aid this discussion, we undertook a systematic scoping review of research literature concerned with outreach implementation and measurement in community contexts to identify research-informed best practices for relationship building, providing support, crisis intervention, and fostering self-efficacy in health and social care navigation (see Jiao et al., 2022). We then compared and contrasted our findings with the experiential knowledge of the CAC. Community-generated research reports about GBV and evidence-informed strategies to enhance women's safety in their homes, communities, and clinical care encounters were also reviewed (e.g., Women's Coalition, 2014). These community reports and the CAC's engagement centered on women's experiences and strengths-based approaches to safety (Bell & Reed, 2021). As we engaged with these materials we identified the need for additional knowledge about community outreach delivery models from the perspectives of those delivering such services. We purposefully recruited and conducted 1-1 interviews with eight outreach workers from six organizations providing outreach to women experiencing SI. The participants’ outreach work experience ranged between 2.5 and 12 years and their respective organizations adhered to a compartmentalized approach to women's concerns focusing on homelessness, postincarceration transition, mental health, and addictions. Interview questions centered on understanding the nature of their work, their experiences of working with women in the community including their perspectives on building and sustaining relationships, and some of the barriers and challenges they faced in undertaking their work (Table 1).
Outreach Staff Thematic Categories.
Drawing on the synthesis of various data sources and our dialogues, we finalized an operational definition of outreach to guide the intervention. Outreach was defined as activities to locate and make connections with women within their local community to build trust in ways that would support sustained relationships over time. Outreach activities included unconditional episodic, short-term support (e.g., food, harm reduction supplies, assistance finding shelter) and ongoing engagement with women to create linkages with, and facilitate receipt of, health and social care commensurate with their self-identified needs. Our program specifically focused on tackling barriers in service access and receipt; building from and enhancing women's strengths and capacities to foster their health and well-being over time; and providing ongoing assistance as new needs arose.
Step 3. Identifying Core Principles and Values
In building our shared understanding of outreach, we further identified the need to articulate the core assumptions underpinning our design to ensure a safe, accessible, and culturally appropriate 2 outreach intervention. Our understandings of GBV, trauma, equity, and inclusion were particularly important as was our aim to challenge ideologies of deviance and infantilization. We agreed on four core principles, detailed below.
Principle 1. Tackling gender-based violence
We defined gender as a social process concerned with the complex ways in which social differences between individuals and/or groups based on “sex” characteristics and expression acquire meaning and become structural factors in the organization of everyday life (Smith, 1999). Gender is relational and extends beyond the social properties of an individual person or interpersonal relations to include the broader structural relations of power of which we are part (Smith, 1999). GBV is situated in structural relations of power and includes harmful acts, practices, and policies directed at an individual based on their gender (Young, 1990). GBV disproportionately affects women, girls, and people who do not adhere to patriarchal ideologies about what constitutes “masculine” and “feminine.” Patriarchal ideologies regularly dichotomize and essentialize so-called male and female, privileging the masculine and normalizing “femaleness” as a subordinate position in society. Such ideologies are at the root of GBV (Smith, 1999; Young, 1990). GBV includes acts of violence (e.g., physical, sexual, psychological, material) committed by one person against another. Although most often used to describe interpersonal acts of violence, GBV is simultaneously structural. GBV is a social practice, whereby relations of power construct situations in which interpersonal violence not only occurs but is often normalized as a regular part of life (Young, 1990). Liberal ideologies of egalitarianism and individualism further advance the structural features of GBV by enabling marginalizing discourses of blame and responsibility among women affected by violence (Young, 1990). Thus, women's experiences of GBV and intersecting health and social inequities are reinforced by the structural processes built into the fabric of our society (Varcoe et al., 2017). Considering the structural context of GBV in health and social care directs our attention to the social processes whereby institutions such as law, policy, health care, and social services adhere to, and perpetuate patriarchal ideologies within their organizations and practices (Hill Collins, 2019; Varcoe et al., 2017) including how social and health services (and other social institutions) identify and respond to women's concerns (Krieger, 2003).
Our understanding of GBV also includes the multiple and intersecting systems of oppression that influence women's lives and the problems that arise as a result. While gender is prominent in our project, we drew heavily on intersectionality scholarship (Hill Collins, 2019) to understand how sociostructural relations of power contribute to and perpetuate GBV. We specifically identified that gender and GBV are inextricably tied to other axes of power and privilege including race, social class, colonial histories, sexuality, (dis)ability, and age (Hill Collins, 2019). Thus, we aimed to co-design an outreach intervention that considered how patriarchal and colonizing ideologies and practices influence women's health and social care; how such institutions identify and respond to their concerns; and how outreach can mitigate against and not perpetuate the harms enacted through such processes.
Principle 2. Personhood and relational engagement
Because we viewed outreach as an active and relational process, it was vital we articulate our views on personhood and relational engagement. We employed a complex view of personhood that encompasses the “whole” person versus a limited view of women restricted solely to the problems to be addressed that have permeated street-involved outreach interventions (Betron et al., 2021; Bungay et al., 2010; Greer et al., 2020; Tuck, 2009). Personhood encompasses the strengths and capacities of women and outreach workers, their knowledge, experience, and the challenges they face (Tuck, 2009). Building upon this holistic view, we drew from tenets of relational practice to help frame our understanding of relational engagement. We noted that each person (i.e., outreach worker, woman) and their actions are shaped by multiple influences including situations, emotions, context, experience, and relations with others (Doane & Varcoe, 2015). We also acknowledged that these histories and contexts can be prohibitive or supportive in building relationships (Doane & Varcoe, 2015). However, to fully grapple with our assumptions about personhood and the interconnectedness and complexity of relationships (Jaramillo & Carreon, 2014), we additionally considered the values necessary to guide outreach workers’ actions. These values included respect, reciprocity, and the right to self-determination.
Reciprocity refers to an ethical value system based on giving and receiving, not in terms of material goods, but as a set of relational practices that requires each actor (or group) to make an equivalent response in a respectful and mutually beneficial way (Jaramillo & Carreon, 2014). Similar to our approach to epistemological flexibility, reciprocity requires mutual recognition that each person has value, worth, and knowledge within the relationship, and it is through this recognition that respect and reciprocity can be enacted. Self-determination builds on the worth and value of persons to recognize their inherent rights and capabilities to make their own choices (Tuck, 2009). Within an outreach context, self-determination was equated with women-led engagement, in which the goals and priorities concerned women's health and social well-being, and their readiness to engage with these priorities was determined by the women for whom outreach was intended. We aimed to ensure that outreach was enacted to privilege women's strengths and resilience within the complex structural context that contributes to inequities in care. Ultimately these perspectives concerning personhood and relational engagement supported the design of an intervention whereby women's and outreach team members’ strengths and capabilities are respected and when shared, created opportunities for sustained relationships, identification of women's goals and aspirations, and plans for engaging with health and social care services necessary to attain these goals.
Principle 3. Trauma-informed engagement
Our focus on GBV as a factor shaping women's expereinces and our understandings of personhood and relational engagement, necessitated we tackle how these principles intersected within a street-involved context. We reviewed materials concerning trauma-informed care (TIC) and trauma and violence-informed care (TVIC) (Elliott et al., 2005; Nathoo et al., 2018; Ponic et al., 2016; Wathen & Varcoe, 2019) to help shape our understandings. These perspectives reinforced the importance of integrating an understanding of trauma, related causes, and consequences into intervention design. We defined trauma as the experiences and responses associated with violent events and therefore the direct result of structural and interpersonal GBV on women's lives (Elliott et al., 2005; Young, 1990). We also acknowledged that trauma (e.g., discrimination, sexual assault) can impact women's psychological and physical functioning, for instance, PTSD, depression, and disability (Campbell, 2002). We further acknowledged that trauma is situated within the intersectional causes associated with sexism, racism, classism, and (dis)ableism that permeate women's lives and do not rest solely at the level of the individual (Wathen & Varcoe, 2019; Young, 1990).
We then wrestled with how we might integrate other principles of TIC/TVIC approaches into our outreach intervention design. We recognized that such approaches are inherently aimed at providing direction to clinicians and organizations to provide health and social care in a safe, nonretraumatizing way (e.g., EQUIP Health Care, n.d.a.). Within TIC/TVIC for instance, safety in a care encounter has been described as including freedom from discrimination, creating opportunities for choice, and using strengths-based ways to provide care (Wathen & Varcoe, 2019). These perspectives also acknowledge that service providers may have trauma histories and therefore vicarious trauma for staff should be considered (Darroch et al., 2024). While recognizing the importance of the central tenets of TIC/TVIC, we struggled with how to implement these concepts in an intervention design that simultaneously adhered to our holistic conceptualization of personhood and the relational values of reciprocity and rights to self-determination. Our team specifically queried about the potential—albeit unintentionally—of TIC/TVIC approaches to perpetuate a limited view of women as damaged versus a view of the “whole” person (Tuck, 2009). The CAC and community partners also questioned the potential impact of TIC/TVIC methods that position the service provider as responsible for safety. They specifically questioned the focus on providers’ responsibility to “offer choice” or “provide clear expectations” (Wathen & Varcoe, 2019, p. 5) as potentially reinforcing the implicit, unidirectional, and paternalistic power hierarchies that can diminish the reciprocity and respect for self-determination necessary for safe and respectful engagements between outreach workers and women. While recognizing that any service has a particular scope, the framing of outreach workers as “establishing expectations” for a woman risks negating a relational approach to personhood and reinforcing infantilizing practices. There were also concerns that oversights in self-determination could reinforce biased assumptions about what constitutes trauma, thereby overlooking the significance of understanding how people respond to traumatic events and what they perceive as trauma can be highly individual. The CAC members identified that threats of interpersonal violence were daily features of women's lives as was the structural violence associated with stigma and discrimination. However, it was important that our approach to trauma-informed engagement both recognize the ongoing violence and the complexity and variation in how women think about and take up violence in their lives.
We also wanted to avoid perpetuating a transactional approach to outreach, whereby outreach service was constructed as doing something for a woman versus with and in partnership. The CAC specifically noted that without building a relationship of trust and reciprocity whereby expectations were constantly evolving in terms of how women and the outreach team worked together, the intervention would fail to achieve its aims of building upon women's strengths and advancing self-efficacy to navigate health and social care in increasingly autonomous ways. The CAC members further noted that both outreach workers and women need to communicate about respectful approaches to engagement including how they each expected to be treated. Communication was viewed as integral to how women and outreach workers collaboratively set parameters for their interactions in a relational manner. Additionally, the element of time was viewed as “missing” in much of the discussions about TIC/TVIC we reviewed; noting that sufficient time was necessary to build trust to allow for such communication, which could further enhance safety within an encounter.
To help address these tensions in developing our approach to trauma-informed engagement, we drew on the work of scholar Tuck (2009) to remain oriented to the value, worth, and strengths of women and the relational nature of the intervention. In her work “Suspending Damage: A Letter to Communities,” Tuck (2009) illustrates how research often perpetuates, albeit perhaps unintentionally, the ideologies of a damaged victim who reinforces “a one-dimensional notion of these people as depleted, ruined, and hopeless” (p. 409); operating through a “theory of change that establishes harm to achieve reparation” (p. 413). Thus, while we acknowledged the importance of the tenets of TIC/TVIC (e.g., need to understand trauma and its causes and consequences; foster safety in engagements), we viewed safety and expectations as elements that were defined collaboratively and continuously negotiated over time recognizing that women have the right to determine their own concept of safety.
Principle 4. Harm reduction as engagement
Substance use among women who are street involved is often inextricably linked to historical and ongoing GBV and trauma (Garami et al., 2019). We therefore, saw the need to articulate our position on harm reduction as a principle and a practice that could inform our approach to engagement with women using unregulated (i.e., nonprescribed opioids, cocaine, methamphetamine) and regulated (i.e., alcohol) substances. We drew on research and our experiential knowledge to explore varied perspectives about harm reduction that supported us in considering our commitment to relational approaches to engagement.
First, we worked to conceptualize what we meant by substance use–related harm. We agreed that substance use–related harm is a complex process that reflects the interplay between structural features of society (e.g., criminalization, poverty, discrimination, drug toxicity, GBV) and people's drug use practices (Jiao, 2019). We also recognized that understanding harms and strategies for harm reduction required an understanding of the various substances used, their mechanism of action, and the impact of drug withdrawal on women's overall well-being. We further identified the importance of understanding the specific discrimination experienced among women who use unregulated drugs, particularly in the context of health and social care. As demonstrated in earlier research and verified among our CAC team, women experiencing SI, are often dismissed as “drug seeking” when attending to health care (Lloyd, 2010), and as such may have their actual health concerns negated during clinical care encounters (Bungay, 2013; Bungay et al., 2010). Such experiences contribute to mistrust in care provision, unmet care needs, and worsening health inequities for women, and we needed to consider how to avoid perpetuating discrimination in our work.
We therefore conceptualized harm reduction as a relational practice—an approach to engagement that communicates respect and a nonjudgmental approach to women's use of substances (Foy, 2017; Jiao, 2019). Harm reduction includes technical aspects such as drug-using equipment (e.g., syringes, pipes, sterile water), pharmacology (e.g., opiate substitution), and education concerning use (Jiao, 2019). Harm reduction also includes attention to the sociostructural context of people's lives that influence both susceptibility to harm and capacity to prevent and respond to substance use–related harms (Jiao, 2019). The intersecting effects of GBV and related inequities for women's safety in the context of substance use are well documented. Poverty, precarious housing, control by intimate partners, criminalization, and consequential drug toxicity negatively affect women's abilities to use in safe spaces, free of violence, and exploitation by others (Boyd et al., 2018; Rance et al., 2018). Taken together, technical aspects serve as tools for engagement affording outreach workers the opportunity to offer support with women to meet a self-identified need concerning their use; simultaneously communicating respect and creating opportunities for relationship building (Foy, 2017).
Step 4: Finalizing the Outreach Intervention
Building upon our outreach definition and guiding principles our next step was to design the outreach intervention, specifically, the elements, implementation approach, and the interventionists’ characteristics and roles. To sustain our inclusive approach and to foster intervention acceptability and appropriateness, we decided that the outreach interventionists would include experiential community health workers (CHWs) and nonexperiential interventionist outreach workers (IOWs) (Austin et al., 2023; Greer et al., 2020; World Health Organization [WHO], 2018). CHWs were self-identifying women with expert knowledge about the community who also share distinct social locations and life experiences with the women we sought to engage (Saboori et al., 2022; WHO, 2018). The CHWs were women with lived experience of SI and GBV and had previous CHW experience. IOWs were also self-identifying women with additional training and education in health and social sciences and service delivery. IOWs would have expertise in undertaking health and social assessments and navigation and facilitation of health and social care through strengths-based and trauma-informed approaches to engagement.
While we recognized the importance of CHWs to facilitate connections with health and social care services among women underserved by such (Betron et al., 2021; Greer et al., 2020; Saboori et al., 2022; WHO, 2018), our literature review and expert knowledge reinforced our concern of the potential for harm among CHWs. Previous research, for instance, demonstrated that CHWs in street-involved settings report significant emotional distress associated with unrealistic responsibilities and poor supports while working (Greer et al., 2020). To prevent harm, we established that the CHWs would work in partnership with IOWs, sharing expertise while also receiving mentorship and support for their own professional development (WHO, 2018). Before engaging in outreach, the CHWs and IOWs would undergo intensive training in professional boundaries, self-care, trauma-informed engagement, mental health first aid, and crisis intervention. Bi-weekly meetings with the outreach team facilitated by the research manager would further enable the team to explore successes and challenges, provide safe debriefing, and allow for the identification of professional development activities commensurate with team members’ collective and individual needs (WHO, 2018). During this time, the CAC further noted that the project required an appropriate identity that could communicate our central values, particularly the importance of women's rights to self-determination, our commitment to recognizing and building upon women's strengths, and our relational approach to engagement. The CAC met to brainstorm a project title, arriving at STRENGTH (sisters together reaching every new goal toward healing). With the support of the community leaders and research team members, the CAC hired a local Indigenous artist to create a logo that identified the aims of this project in a respectful and strengths-based manner.
Next, we worked to finalize the intervention elements, activities, and related timing and sequencing. We knew we needed a design that would permit sufficient time for the interventionist team to build credibility as a safe, trustworthy, and appropriate “service” among women. They also needed time to work in partnership with women to address the complexity of women's needs (Rodgers et al., 2017). We, therefore determined that the intervention would be delivered over an 18-month period and include two interrelated relational elements.
Element one: Making contact
During the first three months, the interventionists would focus on making contact, defined as the activities necessary to build awareness and credibility of the intervention study among women in the community. The CHWs and IOWs would work in pairs to engage in foot outreach on the street, in alleys, and at drop-in services, shelters, and housing facilities; established practices for outreach in street-involved settings (Rowe et al., 2016; Slesnick et al., 2017; Small et al., 2012). Logo decals were to be attached to their backpacks and the teams would carry information cards detailing the project aims and contact information for further engagement. The CAC specifically noted the importance of consistency to enable women to gain familiarity with the teams. Accordingly, outreach would include day and evening hours with a rotation of locales determined by the CAC and CHWs. Drawing on the CHWs’ and CACs’ expertise concerning women's material, psychological, and physical safety and our principle of trauma-informed engagement, we developed guidelines about approaching women during making contact activities. For instance, women would not be approached if they were working (e.g., sex work), in the process of using substances (e.g., injecting or smoking), or in some instances, with another person or group. Approaches in these circumstances could be considered intrusive, disrupt income potential, and threaten women's safety if they were with a controlling partner. Because the CHWs would likely be known to many women, it was also imperative to develop guidelines related to their leadership. We identified that the CHWs could approach women they knew if they deemed it safe, and, with a woman's permission, do introductions to the IOWs.
To aid in credibility and trustworthiness as a nonjudgmental resource and respond to women's episodic needs, the teams would be able to offer harm reduction, food, and hygiene supplies (Austin et al., 2023). They would also provide referrals and accompaniments for emergency shelter or health care as needed or other safety-specific concerns that women might identify (e.g., need for accompaniment away from a potentially unsafe situation). Women would not be required to provide any personal details to receive these supports, reinforcing the unconditional, trustworthiness and women-led nature of the engagement. We proposed relationships with women would grow over time, and as such, we would begin recruiting to element two—making linkages.
Element two: Making linkages
Making linkages included the relational processes necessary to sustain participants’ engagement and enable women and IOWs to collaboratively work on short-, medium-, and long-term goals necessary to advance women's safety, health, and well-being. To determine women's goals and support needs (e.g., accompaniment, referral), outreach team members would work in partnership with women to assess strengths and self-identified priorities; guided by an assessment tool developed collaboratively between researchers, service leaders, and the CAC. The guide would allow a woman and IOW to explore her health and emotional status, housing and financial security, safety at home and in community, and health and social care needs (e.g., primary care, legal assistance). Unlike intake processes that regularly occur in a formal clinical setting, these assessments would be women-led and completed at a location and pace that worked for the participant. The CAC further noted that confidentiality was a paramount concern among women including the CHWs. Thus, engagement with the CHW for these activities necessitated that we avoid placing CHWs or participants in an uncomfortable situation. Women could decide their preference for the CHW to be included in these discussions and the CHW would have the option to decline an engagement.
Considering the complexity of the interrelationship between GBV and SI (Boyd et al., 2018; Bungay et al., 2010), we acknowledged that urgent, immediate needs could arise (e.g., recent assault, loss of safe place to sleep), particularly those threatening women's safety, and would need to be prioritized. If this occurred, the outreach teams would assist as appropriate, follow up, and continue the assessment at another time. Upon assessment completion, the IOW and woman would review the assessment, establish priorities, and develop a strengths-based plan to achieve the priorities. A nonpunitive, relational trauma-informed approach for missed connections, lateness, or challenges in focus during engagements would be applied. We viewed humility as an outreach skill, noting that everyone has times in their lives when they cannot make an appointment or fully engage (Foy, 2017). IOW would follow up with women for any missed connections to provide a check-in to assess for, provide episodic or crisis support, and determine an appropriate time for the next meeting.
When considering goal setting and planning, we sought to integrate an incremental approach. Achieving a small success (e.g., obtaining lost identification; applying for shelter) can create opportunities for engaging with other, more complex priorities such as attending to primary health care, obtaining more permanent housing, and engaging with legal assistance associated with having been assaulted (Darroch et al., 2024; Foy, 2017; Rodgers et al., 2017). The CAC specifically noted the potential for positive self-regard and self-confidence with incremental success and we therefore integrated quarterly check-ins for all enrolled participants to review accomplishments. Drawing on our project aims and intervention design, we identified sustained engagement, priority attainment, and increased autonomy in navigating health and social care as core outcome indicators to be explored in the next phase of our project which involved the implementation of the pilot study.
Summary and Conclusions
The co-design process undertaken in the STRENGTH demonstrates that CBPR approaches are appropriate and feasible to meaningfully and inclusively co-design research interventions that consider the structural and interpersonal contexts in which GBV and SI occur. Through our shared commitment to tackle inequities in health and social care and disrupt damaging ideologies of deviance and infantilization, we were able to co-create an outreach intervention, whose cultural appropriateness and acceptability were later pilot tested in our local urban context (see Bungay et al., 2021). While the need for CBPR approaches is well recognized and the methodological expertise is growing, further scholarship regarding strategies to train and build capacity among researchers and communities to implement CBPR methodology is warranted (Bell & Reed, 2021; Belone et al., 2016; Culbong et al., 2022; Switzer et al., 2019). Transparency and sharing about the real-world application of CBPR approaches can help to address such gaps (Darroch et al., 2024). As noted by Culbong et al. (2022), the examination and reflection of community–academic partnerships allow us to explore what is possible and what can be achieved, thereby strengthening opportunities for community leadership, empowerment, and inclusion in the research process.
Our work builds on these calls for greater reflection and transparency by elaborating on how principles of CBPR were enacted within an interrelated GBV and street-involved context and how communities and researchers might structure inclusive partnerships and co-design processes for intervention studies. Specifically, this article focuses on one element of a larger co-design process, namely determining how current perspectives about outreach practice, GBV, and SI (e.g., TIC/TVIC, harm reduction, relational engagement) can be interrogated, refined, and applied by integrating varied epistemological orientations among diverse groups of people. Explicitly creating a shared understanding of the underlying social justice aims associated with CBPR approaches (i.e., disrupting dominant damaging ideologies; enhancing health and social care; respecting rights to self-determination) and core principles and values necessary to enact these aims through research was critical to the co-design process. It is vital that people engaging in CBPR explicitly articulate their guiding principles and values including how such principles are operationalized to achieve goals of disrupting the status quo and advancing equity and inclusion in the community (Bell & Reed, 2021; Belone et al., 2016).
Additionally, as noted by numerous scholars (e.g., Austin et al., 2023; Boyd et al., 2018; Bungay et al., 2010), interventions specifically aimed at enhancing health and well-being among women experiencing GBV and/or SI, require attention to the local context of the intervention setting. Our work further illustrates that such assessments include both the individual and structural features of experiences that exacerbate violence against women and barriers to care. Attending to structural features such as discrimination in care encounters and unmet care needs due to compartmentalization of women's health and social concerns, creates opportunity for interventions that can reduce mistrust in care and attend to the complexity of women's lives thereby creating possibilities for enhanced health and well-being among women. It also enhances the ability of CBPR approaches to engage with and respond to community-identified priorities within the co-design process (Bell & Reed, 2021; Culbong et al., 2022; Wallerstein et al., 2018). Community-identified priorities rarely emphasize individual behavior, but as our work illustrates, such priorities are embedded in the structural features of everyday life that contribute to structural disadvantage, which in our project is inclusive of GBV.
Grappling with community priorities and attending to structural features of the local context, also communicates trust and respect for experiential knowledge, essential elements of effective community–academic partnerships (Belone et al., 2016). Our project strengthens the evidence that flexible, iterative, and practical approaches in co-design and research implementation enhances effective CBPR (Bell & Reed, 2021; Belone et al., 2016; Switzer et al., 2019). We demonstrated the importance of continuous feedback loops, enactment of respect and reciprocity, and overcoming barriers to engagement (e.g., financial and service navigation support) for developing and sustaining trust in the process and among the team. Transparency in our decision-making processes further enabled trust, all of which were enhanced by engaging with creating and attending to our memorandum of understanding terms of reference.
While it is likely that our learnings may be useful for CBPR approaches to any community experiencing historical (and ongoing) structural disadvantage, each project will attend to the local context in which the work is situated. Additionally, inclusive approaches to epistemological plurality support reciprocity and respect necessary for trust and meaningful engagement among the team (Bell & Reed, 2021). In documenting our process, we hope that other community–academic partnerships find value in learning about our experiences and that we are able to contribute to the scholarship of CBPR methodology and the substantive field of outreach that better integrates the complex interrelationships between SI and GBV, thereby enhancing women's health and well-being and their engagement with care.
Footnotes
Acknowledgements
We would like to extend our deep thank you to community experts Jade (in memorial), Sandra, and Chase for their input into the implementation of this work as well as all of the women who gave their time as research participants. Dr. Bungay is funded in part by the Canada Research Chair Program. Ethics Certificate Numbers: H18-00069.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Social Science & Humanities Research Council of Canada (grant number 890-2016-001) and the Vancouver Foundation (grant number UNR16-0443).