
Abstract
The COVID-19 pandemic increased women's vulnerability to intimate partner and sexual violence (IPV/SV), as well as challenging organizations’ ability to respond. This research is based on a 2021 nationwide survey about the impacts of COVID-19 on IPV/SV services across Canada. Nationwide, organizations adopted several measures to reduce the risk of COVID-19 transmission, including scaling back services, reducing or stopping their volunteers, and reducing the number of in-shelter clients. Organizations detailed several financial challenges including increased costs and cancelation of fundraising events. Organizations also reported many staffing challenges, from increased workloads to staff leaves of absence due to childcare responsibilities, mental health reasons, or contracting COVID-19. Policies ensuring adequate financial support to IPV/SV services in nonemergency times could help minimize disruption to service delivery during crisis situations.
Introduction
Intimate partner violence (IPV) and sexual violence (SV) are recognized as two major global public health and human rights issues affecting an estimated one-third of women worldwide (World Health Organization, 2021). Crisis situations, such as the recent COVID-19 pandemic, can have serious ramifications for women's1 risk of IPV and SV, and for service organizations’ ability to respond (Fraser, 2020). Within the context of COVID-19, lockdown measures such as the closure of schools and daycares, as well as job losses due to a changing economic landscape, can increase stress within the home, potentially increasing the likelihood of violence. Lockdown measures also mean that women may be trapped at home with their abusers and have a harder time accessing support safely and privately (Evans et al., 2021).
The Canadian Context
Within Canada, an estimated 11 million people aged 15 and over have experienced IPV at least once in their lives, with women and girls being disproportionately affected (Women and Gender Equality Canada, 2022a), and nearly five million women aged 15 and over report having experienced SV (Statistics Canada, 2019). In addition to the numerous physical and mental health consequences of IPV and SV, these forms of violence pose a tremendous financial burden on Canadian society. Approximately $7.4 billion and $4.8 billion are spent annually to address the consequences of IPV and SV, respectively, including medical care, counseling, loss of employment, legal aid, funerals, as well as the intangible costs of pain and suffering (Department of Justice, 2009; Zhang et al., 2012).
Under Canada's federal system of government, addressing IPV/SV is a concerted effort between federal and provincial/territorial governments. The federal government leads the development of national action plans, including the most recent 10-year National Action Plan to End Gender-based Violence launched in 2022 (Women and Gender Equality Canada, 2022b), and provides funding to the 13 provincial/territorial governments. In 2021, the federal government committed nearly $600 million, distributed over 5 years, to support provincial/territorial governments in implementing this National Action Plan (Prime Minister of Canada, 2021). Provincial/territorial governments then use this funding to implement and maintain IPV/SV services including women's shelters, crisis lines, and sexual assault centers (Women and Gender Equality Canada, 2022b). The operation of such services is therefore directly dependent on and influenced by federal priorities. For instance, the previous conservative administration (2006–2015) reduced funding by nearly 40% to its federal agency responsible for advancing gender equality; Status of Women Canada (now Women and Gender Equality). These budget cuts directly resulted in the closure of many women's organizations, including IPV/SV services across the country (Canadian Women's Foundation, 2020; Knight & Rodgers, 2012).
Similarly, public health responses to COVID-19 in Canada were shaped by its decentralized structure. In Canada, the management and delivery of healthcare is a provincial/territorial jurisdiction, while the federal government is responsible for setting national standards and allocating funding to provincial/territorial governments (Government of Canada, 2023). In the context of COVID-19, the federal government was responsible for international travel restrictions, healthcare funding to each province/territory, emergency financial support to individuals, businesses, and communities, as well as vaccine procurement (Cameron-Blake et al., 2021). On the other hand, provincial/territorial governments were responsible for implementing containment measures such as the closure of schools, face mask mandates, and restrictions on gathering sizes (Cameron-Blake et al., 2021). While there were several similarities across provinces and territories, there was also variation in both the types and stringency of measures enacted, as well as the timing of when such measures were implemented. For example, Quebec was the only province to implement a curfew at any point in time during the COVID-19 pandemic. Certain provinces and territories (e.g., Quebec, Ontario, New Brunswick, Nova Scotia, and Nunavut) issued stay-at-home requirements, whereas others (e.g., Saskatchewan, Alberta, and Yukon) issued recommendations or advisories.
IPV/SV in Crisis Situations
Crisis situations, including natural disasters, economic downturns, and public health emergencies, may increase gender-based violence (Canadian Women's Foundation, 2018; Fraser, 2020). Researchers examining rates of physical and sexual violence among internally displaced women in Mississippi due to Hurricane Katrina found that violence against women increased posthurricane and rates remained elevated 2 years later (Anastario et al., 2009). Similar findings have been reported in the aftermath of hurricanes in Florida and the Fort McMurray wildfires in Canada (Gearhart et al., 2018; Zoledziowski, 2020). Women's shelters and police in Canadian provinces have also reported increased calls and requests for help following previous economic downturns and increased unemployment (Bartlett, 2016; Lagerquist, 2016). Prior to the COVID-19 pandemic, the Ebola outbreak in Sierra Leone and the Democratic Republic of Congo was associated with an increase in IPV/SV (Fraser, 2020).
This increase in reports of IPV/SV during crisis situations may have important implications for service providers. First, increased demand may stretch an organization's already limited resources. Globally, even in noncrisis times, IPV/SV shelters often struggle to meet demand and operate at maximum capacity, turning away hundreds of women each year (e.g., Lyon et al., 2008; Swiss Info, 2019; Vetten & Lopes, 2020; Women's Shelters Canada, 2019a). Second, crisis situations may lead to budget crunches at the municipal and federal level, as governments focus resources on addressing the immediate impacts of the event (e.g., preventing new infections and deaths from infection) while other social issues and related services, such as IPV/SV, may be deprioritized during the event (Fraser, 2020; Renzetti, 2009). Finally, organizations may face unexpected, additional costs. A survey of North American IPV shelters on disaster preparedness found that shelters were ill-equipped for a crisis, with less than half having a stockpile of emergency supplies (Enarson, 1999). In the wake of COVID-19, IPV/SV services may have faced increased costs due to purchasing personal protective equipment (PPE) and technological equipment to support telework and transitioning services to a virtual model.
To date, most studies of COVID-19 and IPV/SV have focused on characterizing the experiences of survivors and on determining whether the incidence of violence increased (e.g., Gregory & Williamson, 2021; Kourti et al., 2021; Lyons & Brewer, 2021). Few studies have considered the experiences of organizations that provide services to persons experiencing IPV/SV. Understanding how these organizations have fared during the pandemic is important because it affects their ability to provide support to survivors and to respond to sudden fluctuations in demand.
COVID-19 transformed the work landscape in Canada and abroad, from sudden and unplanned transitions to telework and mass layoffs and furloughs (Clarke & Fields, 2022; Eurostat, 2020; OECD, 2021). These changes could have significant consequences both for survivors trying to access IPV/SV organizations and for those same organizations trying to provide critical, potentially lifesaving, frontline support. In their qualitative study, Burd et al. (2023) explored the experiences of staff from violence against women organizations in the province of Ontario during the first year of COVID-19 and identified the many personal and emotional impacts the pandemic had on them. Staff expressed worry about survivors trapped at home with their abusers, guilt over reducing the number of beds available in shelters due to containment measures, the toll from doing trauma work within one's own home, concerns about their job security, and difficulties in engaging in self-care strategies due to lockdown measures. A nationwide survey of 376 staff and volunteers from IPV/SV services across Canada in the early months of the pandemic identified similar challenges (Trudell & Whitmore, 2020). Nearly every single participant reported that their organization introduced some sort of change to their policies and procedures in response to COVID-19, including implementing PPE, working from home, transitioning in-person services to online, reducing the number of spaces available in shelters, and canceling certain projects or activities. These numerous adaptations occurred as staff were observing greater needs and challenges among their clients; 82% of participants noted increases in both prevalence and severity of violence and 34% observed worsened mental health among clients. Staff and volunteers were also affected: 90% of respondents reported increased difficulty in their ability to do their jobs; 81% reported increased work-related stress, and approximately 25% of directors had to make the complicated decision to lay-off staff or cut hours. Our own research team conducted interviews with 17 IPV/SV service providers from 15 organizations across Canada within the first 6 months of the pandemic (Michaelsen et al., 2022). They described the many changes their organizations had to implement in response to the pandemic, including moving shelter operations to a hotel, introducing a quarantine period for incoming shelter clients, offering services virtually, canceling fundraisers, and having to pause some activities to focus on COVID-related tasks. These changes affected their workload, finances, and the extent to which they could support clients. Similar studies conducted in United States and Europe at the onset of COVID-19 corroborate these findings (e.g., Bergman et al., 2022; van Gelder et al., 2021; Wood et al., 2020).
While these studies offer important insights, they were conducted within the first few months of the COVID-19 pandemic, which the World Health Organization only declared over in May of 2023 (Wood et al., 2023). Understanding the longer-term impacts of COVID-19 on IPV/SV organizations, including whether the challenges experienced at the onset of the pandemic still held true more than a year later, is critical in order to accurately assess the needs of the IPV/SV sector and ensure organizations are able to meet demand. Building on our prior research exploring the pandemic-related experience of 15 IPV/SV organizations in Canada, the aims of this study were (a) to determine whether the challenges that those organizations reported were generalizable to a broader sample of IPV/SV organizations across Canada and to (b) to examine whether the pandemic-related challenges that IPV/SV organizations in Canada experienced at the start of the pandemic were still of concern to these organizations 18 months later.
Method
We surveyed organizations across Canada that provide services for survivors of IPV/SV. The design, content, and implementation of the survey were informed by the aforementioned qualitative study (Michaelsen et al., 2022). The challenges highlighted by interviewees guided the development of the survey questionnaire used in this study. Interviewees also provided advice on how to best engage with other IPV/SV organizations via a survey, which informed our decision to create a web-based survey and limit the time required to complete it. Aware that IPV/SV organizations may be overloaded due to the pandemic, our goal was to make the survey as concise as possible.
The survey was conducted in October and November 2021 using LimeSurvey (Limesurvey GmbH, n.d.). Questions focused on organizational characteristics, experiences during the first month of the pandemic (March–April 2020) and at the time of survey completion, changes in the scope or delivery of services due to the pandemic, challenges faced, and emergency funding received. Questions had fixed responses, including rating scales and multiple choice. Participants were able to skip questions that they were unable or did not want to answer. The complete questionnaire is available as Additional File 1.
We created a list of organizations that provide services to survivors of IPV/SV across Canada by searching online resources such as Shelter Safe (https://sheltersafe.ca/) and the websites of provincial umbrella associations (e.g., Ontario Coalition of Rape Crisis Centers [OCRCC, 2022]). We identified a total of 357 organizations and sent a link to the online survey to each of them by e-mail in late October 2021. The e-mail explained the purpose of the survey and invited one management staff member per organization to participate. We also contacted provincial umbrella organizations and asked for their assistance in sharing the survey with their members. We followed up with each organization with a phone call in November to confirm whether they had received the survey link and to correct their e-mail address if necessary. We sent a reminder e-mail one week before the survey deadline (November 30th). Of the 357 organizations we identified, only three were unreachable because the phone numbers listed were out of service and the email addresses were nonfunctional. These three were removed from our database, leaving a total of 354 organizations.
All respondents provided informed consent. This research was approved by the Comité d'éthique de la recherche en sciences et en santé at the Université de Montreal and the McGill University Research Ethics Board.
Response Rate
We received a total of 180 responses to our survey. We omitted six responses that were ineligible because the organization did not provide services for IPV/SV. We also omitted seven duplicate responses. Duplicate responses were generated when a respondent closed the online survey before completing it and then attempted to return to the survey later on to answer additional questions. We merged these responses when we were confident that they were from the same organization, for example, the organization was located in the same town and provided identical responses to early questions in the survey. Following these omissions, a total of 167 organizations were included in our analysis, for a response rate of 47% (167/354).
Forty of the 167 organizations that responded did not complete the entire survey but their partial responses were included in analyses. Of these 40 incomplete responses, 19 (47.5%) were incomplete due to item nonresponse (i.e., an organization completed the survey but did not answer selected questions) and 21 (52.5%) were incomplete because participants exited the survey at some point before the end, leaving all remaining questions unanswered. There was no evidence that the probability of survey completion differed by geographic region or by rural/urban location.
Analyses
Survey responses were exported from LimeSurvey into SPSS 27 for data cleaning and analysis. All analyses were descriptive: we calculated proportions and differences between proportions with corresponding 95% confidence intervals. Results are presented for the entire sample and by region. Some provinces and territories in Canada have very few IPV/SV organizations and so the number of survey responses from these areas was very small. We grouped responses from the Atlantic Provinces (New Brunswick, Nova Scotia, Prince Edward Island, Newfoundland, and Labrador), the Prairies (Manitoba, Saskatchewan, and Alberta), and the Northern Territories together (Nunavut, Northwest Territories, and Yukon) to prevent individual organizations from being identifiable.
Results
Characteristics of Participating Organizations
Organizations from every province and territory in Canada participated in this study. The largest proportion were in Quebec (n = 50, 30%), 20% were in Ontario (n = 34), 20% in the Prairies (n = 34), and the remainder in British Columbia (n = 28, 17%), the Atlantic Provinces (n = 14, 8%), and the Northern Territories (n = 6, 4%). One organization did not report where they were located. Over half of the organizations were in urban/periurban areas (57%, n = 96); the remainder were in rural areas (43%, n = 71).
Respondents were asked to indicate the types of violence their organizations’ services addressed. Almost all organizations provided support for IPV (n = 164, 98%) and 58% (n = 97) for SV. Many also provided support for persons experiencing other types of violence, including family violence, elder abuse, and human trafficking. Specific services provided by the organizations included shelter/transitional housing (n = 156, 93%), a 24/7 telephone crisis line (n = 155, 93%), counseling, and/or psychosocial support (n = 133, 80%), and 24/7 text or email support (n = 72, 43%).
Organizational Challenges
Respondents were asked about the challenges they faced during the first month of the pandemic and at the time of survey completion. Nearly all organizations experienced pandemic-related challenges during the first month. At that time, the majority of organizations reported they did not have sufficient PPE (n = 107, 69%, 95% CI [61%, 76%]), technical resources to work from home (n = 108, 70%, [62%, 76%]), physical space to permit social distancing (n = 104, 67%, [59%, 74%]), or human resources (i.e., staff) for the increased workload due to COVID-19 (n = 94, 61%, [53%, 68%]). Half of organizations reported insufficient financial resources to address COVID-related expenses (n = 77, 50%, [42%, 58%]). Eight organizations reported experiencing no challenges during the first month of COVID-19.
By November 2021, only 1% (n = 2) of organizations had insufficient PPE (prevalence difference [PD]: −0.68, 95% CI [−0.75, −0.60]), only 8% (n = 12) had insufficient technical resources (PD: −0.62, [−0.70, −0.53]), and only 10% (n = 16) had insufficient financial resources for COVID-related expenses (PD: −0.39, [−0.48, −0.30]). However, two important challenges persisted 18 months into the pandemic: 50% (n = 76) of organizations were still struggling with staff shortages (PD: −0.11, [−0.22, 0.00]) and 49% (n = 75) still lacked sufficient physical space for distancing (PD: −0.18, [−0.29, −0.7]).
Actions Undertaken by Organizations in Response to COVID-19
Nationwide, nearly all organizations reported adapting their services according to public health guidelines, such as: wearing PPE (n = 143, 98%, 95% CI [94%, 99%]), implementing physical distancing measures (n = 139, 95%, [90%, 98%]), increasing sanitization of premises (n = 144, 99%, [95%, 100%]), and moving services online (n = 111, 76%, [68%, 82%]).
The pandemic restricted the scope of services that many organizations were able to provide. Half of the organizations scaled back their services (n = 73, 50%, 95% CI [42%, 58%]) and one in four reported that they temporarily stopped providing services altogether (n = 36, 25%, [18%, 32%]). Approximately three-fourths of organizations reduced the number of in-shelter clients they accepted (n = 106, 73%, [65%, 79%]) and 66% reduced or stopped volunteers from coming in (n = 96, 66%, [58%, 73%]). More than three-quarters of organizations stopped accepting material donations (n = 113, 77%, [70%, 84%]).
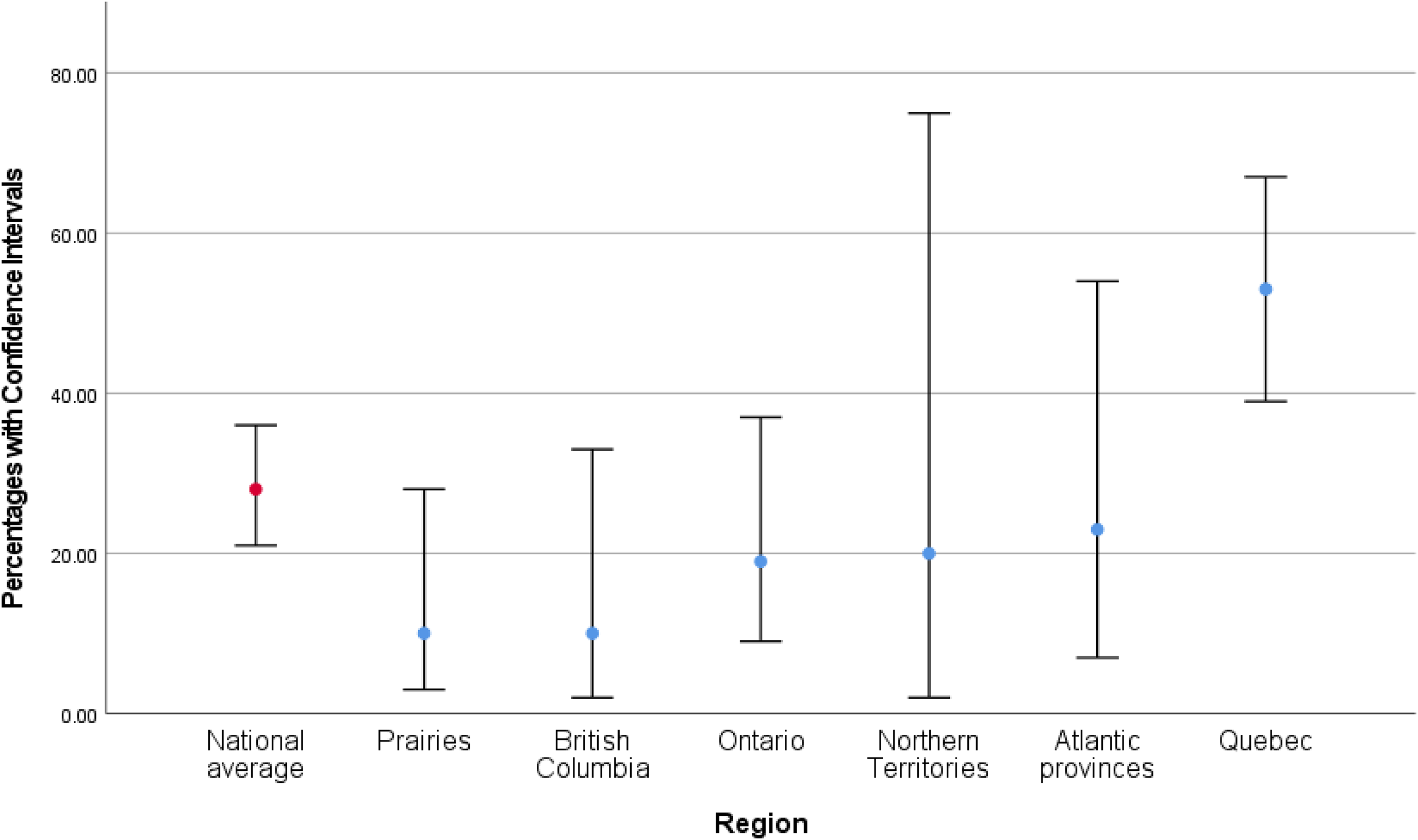
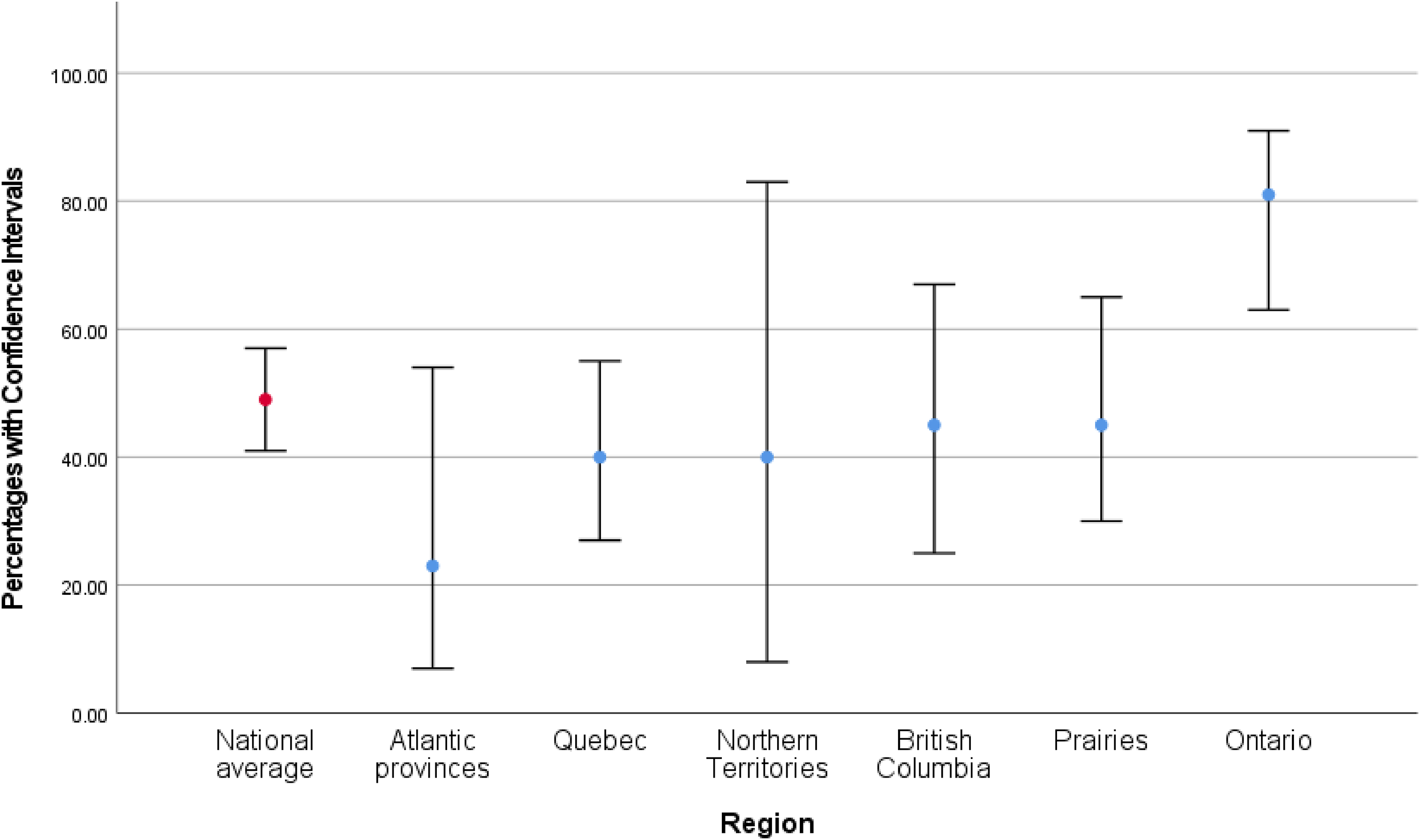
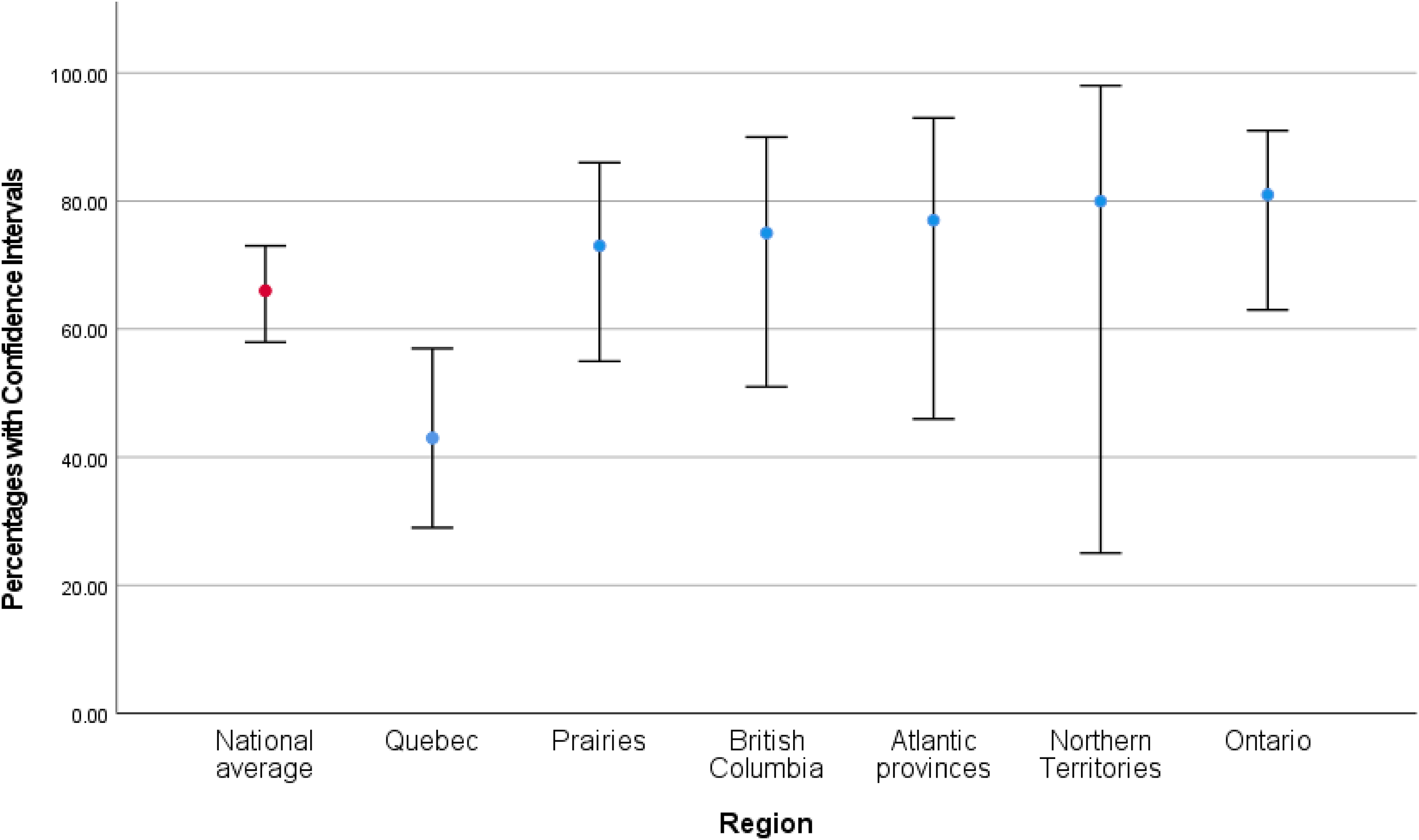
We found little evidence of regional differences in these service restrictions, as shown in Figures 1–3. This may be because regional estimates are imprecise due to small sample sizes. However, compared to the national average, organizations in Quebec were 16 percentage points less likely to temporarily stop services (PD: −0.16, 95% CI [−0.27, −0.06]), 13 percentage points less likely to reduce the number of shelter spaces for clients (PD: −0.13, [−0.29, 0.03]), and 21 percentage points less likely to reduce number of volunteers (PD: −0.21, [−0.37, −0.05]).
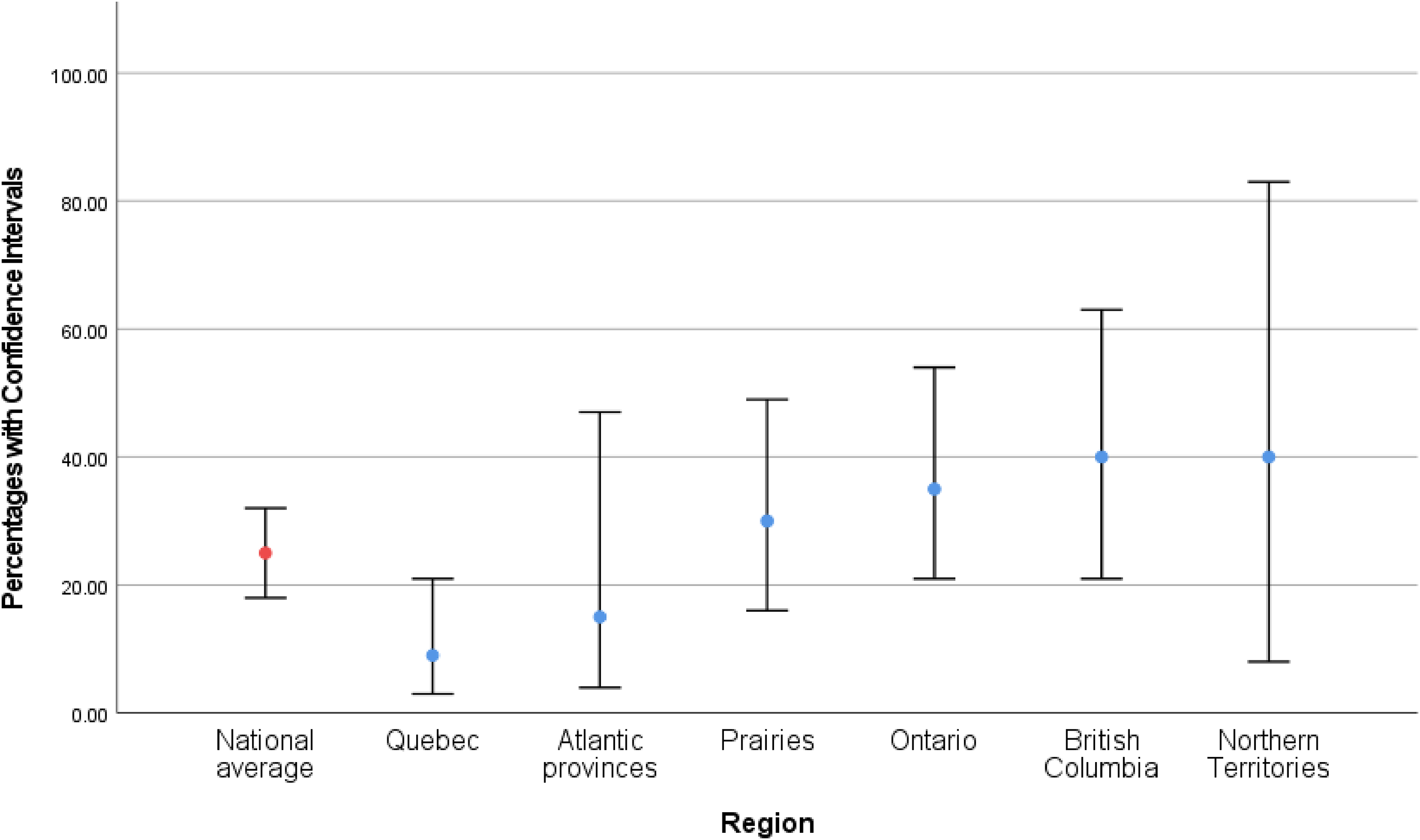
Percentage of organizations that temporarily stopped services, by Canadian region.
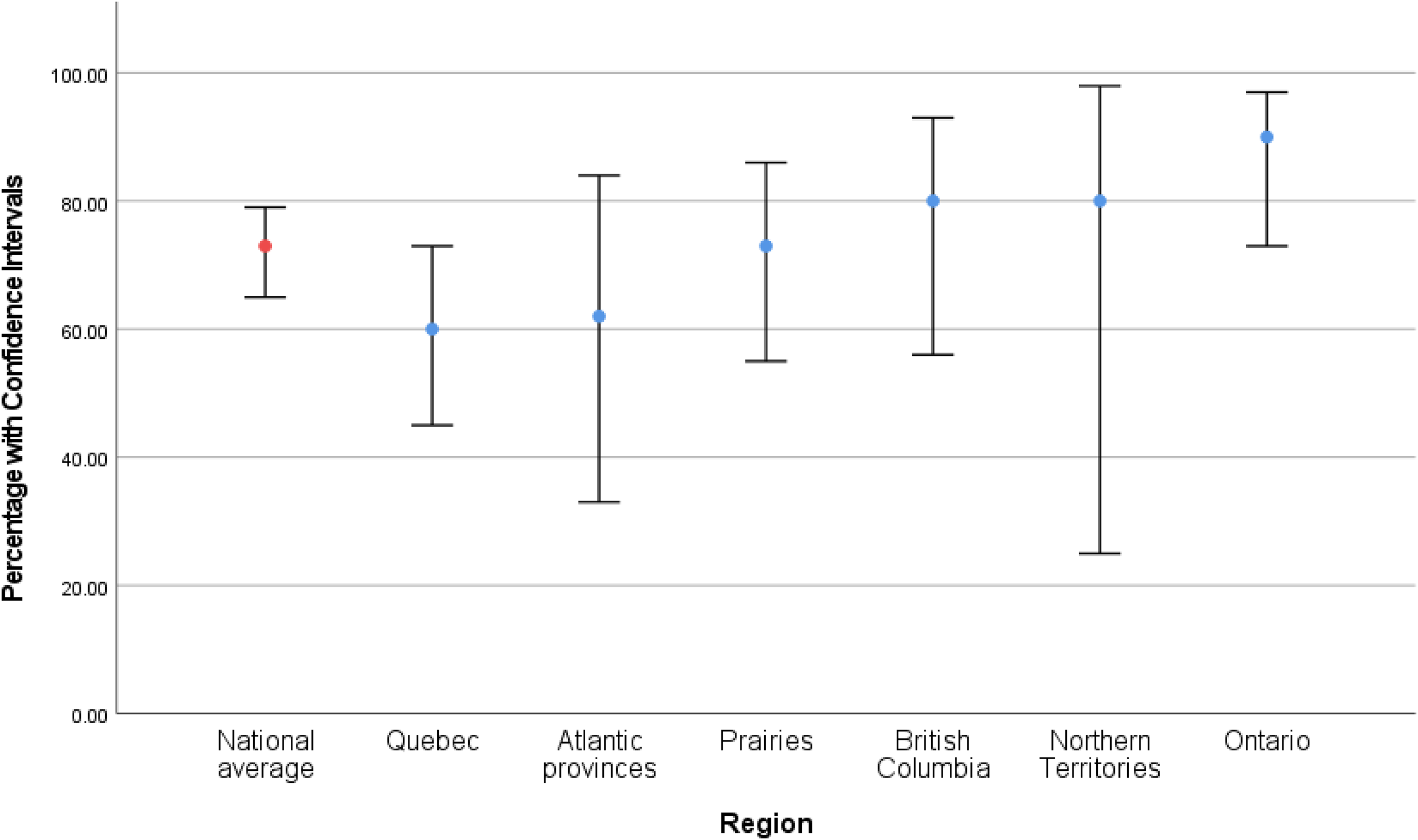
Percentage of organizations that reduced in-shelter clients, by Canadian region.
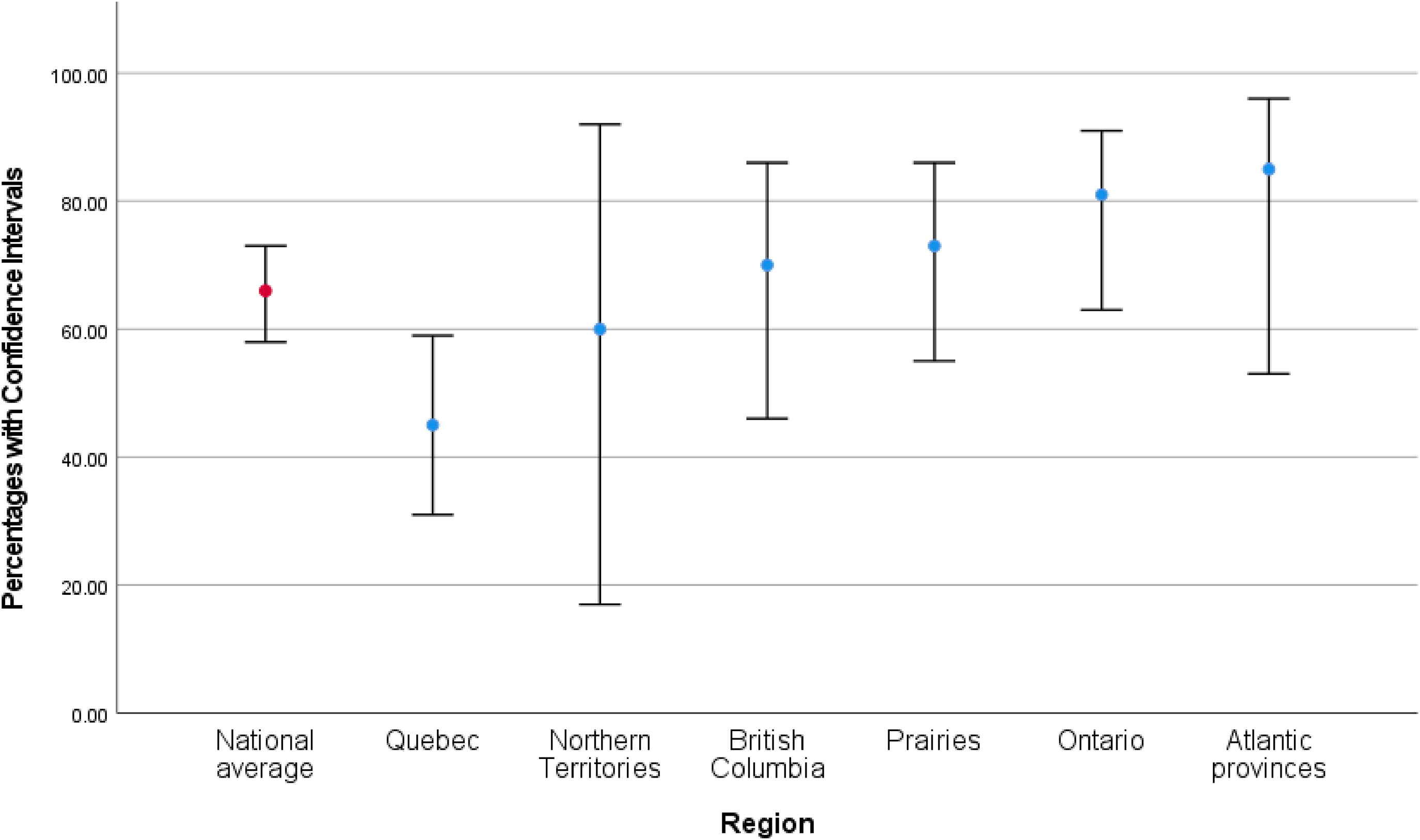
Percentage of organizations that reduced or stopped volunteers, by Canadian region.
Financial Challenges Faced by Organizations
Most organizations across the country faced financial challenges because of the pandemic including increased costs (n = 111, 76%, 95% CI [68%, 82%]), increased wages for staff working during the pandemic (n = 90, 62%, [53%, 69%]) and cancelation of fundraising events (n = 100, 68%, [60%, 76%]). Nine organizations reported no financial challenges. We found no indication that these estimates varied by region.
Emergency Funding From Governmental Sources
A total of 146 organizations responded to questions about the receipt of emergency funding. Of those, nearly all (n = 139, 95%) received emergency funding from either federal, provincial/territorial, or municipal governments. Federal and provincial/territorial governments were the most common sources of emergency funding: 84% of organizations (n = 122, 95% CI [77%, 90%]) received federal funding, 69% of organizations (n = 101, [62%, 77%]) received provincial/territorial funding, and 15% (n = 22, [9%, 21%]) reported receiving funding assistance from their municipal government.
Donations From Nongovernmental Sources
We asked organizations whether there had been a change in the number of monetary donations received from nongovernmental sources since the onset of COVID-19. A total of 145 organizations responded to these questions: roughly one-third of organizations (n = 53, 37%, 95% CI [29%, 45%]) reported receiving a higher number of monetary donations, approximately one-quarter reported receiving a lower number (n = 40, 28%, [21%, 36%]), 19% reported no change in the number of donations (n = 28, [14%, 27%]) and the remainder were unsure (n = 24, 17%, [11%, 24%]).
We also asked organizations whether donations from nongovernmental sources represented a larger or smaller proportion of their overall income in 2020 compared to 2019. Around one-quarter of organizations stated that they comprised a higher percentage of their income (n = 40, 28%, 95% CI [21%, 36%]) and another third that they comprised a lower percentage (n = 43, 30%, [23%, 38%]) compared to the year prior to the pandemic. Twenty-eight organizations (19%, [14%, 27%]) stated there was no change in this proportion and 34 organizations (23%, [17%, 31%]) were unsure.
Organizations in Quebec were 25 percentage points more likely to report an increase in the number of monetary donations from nongovernmental sources compared to the national average (PD: 0.25, 95% CI [0.09, 0.41]) (Figure 4) and 25 percentage points more likely than the national average to report that monetary donations accounted for a higher proportion of their overall income compared to 2019 (PD: 0.25, [0.09, 0.41]; Figure 5).
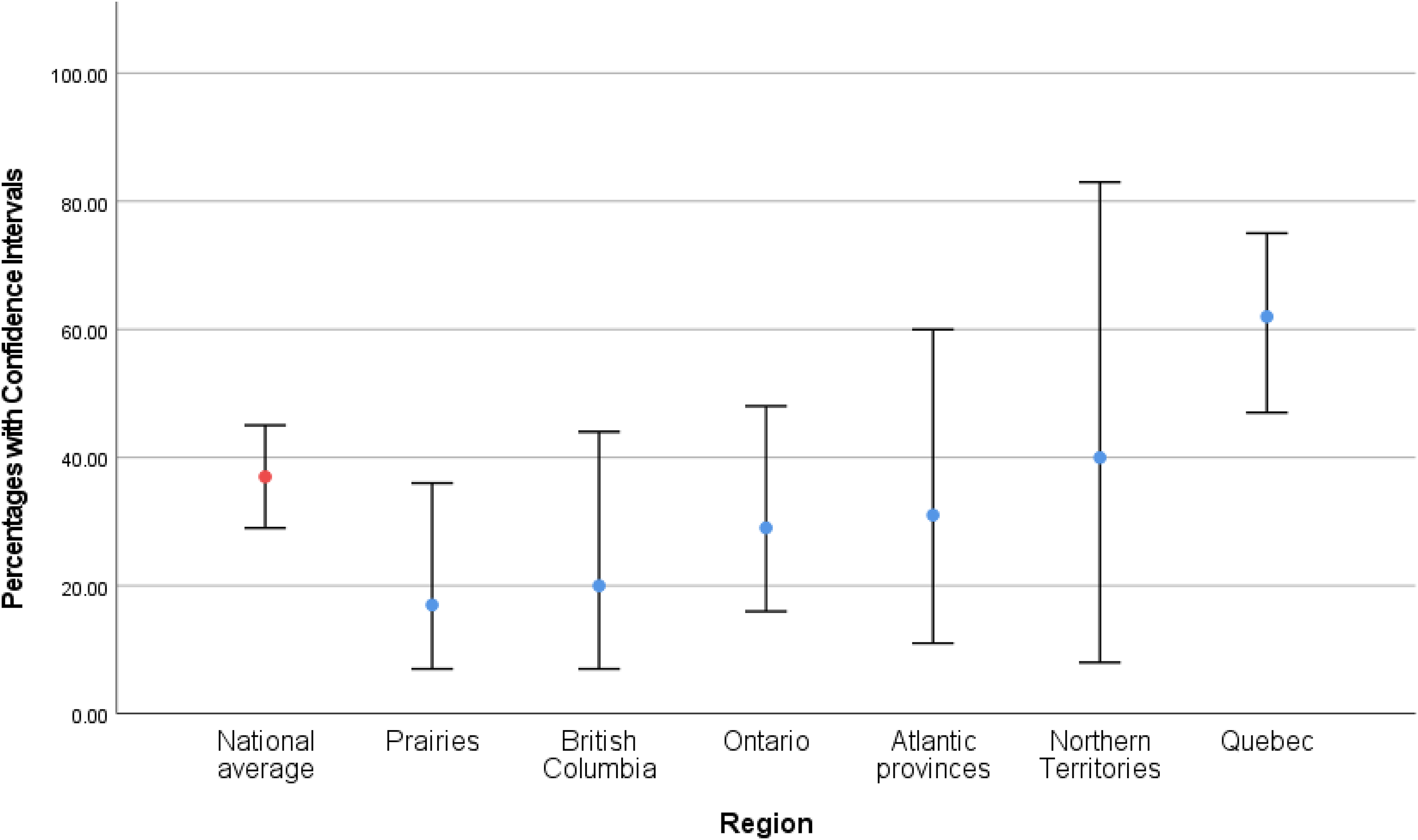
Percentage of organizations receiving an increased number of monetary donations from nongovernmental sources, by Canadian region.
Percentage of organizations where monetary donations accounted for a higher proportion of their overall income compared to 2019, by Canadian region.
Staffing Challenges Reported by Organizations
Staffing challenges were common during the pandemic. Most organizations reported that their staff faced an increased workload (n = 129, 88%, 95% CI [82%, 93%]) and two-thirds reported their staff were afraid to come to work due to COVID-19 (n = 96, 66%, [58%, 73%]). Organizations also reported challenges resulting from staff taking leaves of absence to care for children who were out of daycare or school (n = 94, 64%, [56%, 72%]), for mental health reasons (n = 72, 49%, [41%, 57%]), because a household member was immunocompromised (n = 67, 46%, [38%, 54%]), because they contracted COVID-19 (n = 56, 38%, [31%, 47%]), or because a member of their household contracted COVID-19 (n = 72, 49%, [41%, 57%]).
There is some indication that these staffing challenges varied across the country, as shown in Figures 6–8. Compared to national averages, organizations in Ontario were 31 percentage points more likely to report challenges due to staff taking leave for mental health reasons (PD: 0.31, 95% CI [0.15, 0.47]). Organizations in the Prairies were 28 percentage points more likely to have staff take leave because they contracted COVID-19 (PD: 0.28, [0.10–0.47]). Organizations in Quebec reported less fear of COVID-19 among their staff compared to the national average (PD: −0.23, [−0.39, −0.07]).
Percentage of organizations that faced challenges with staff mental health, by Canadian region.
Percentage of organizations that faced challenges due to staff fear of COVID-19, by Canadian region.
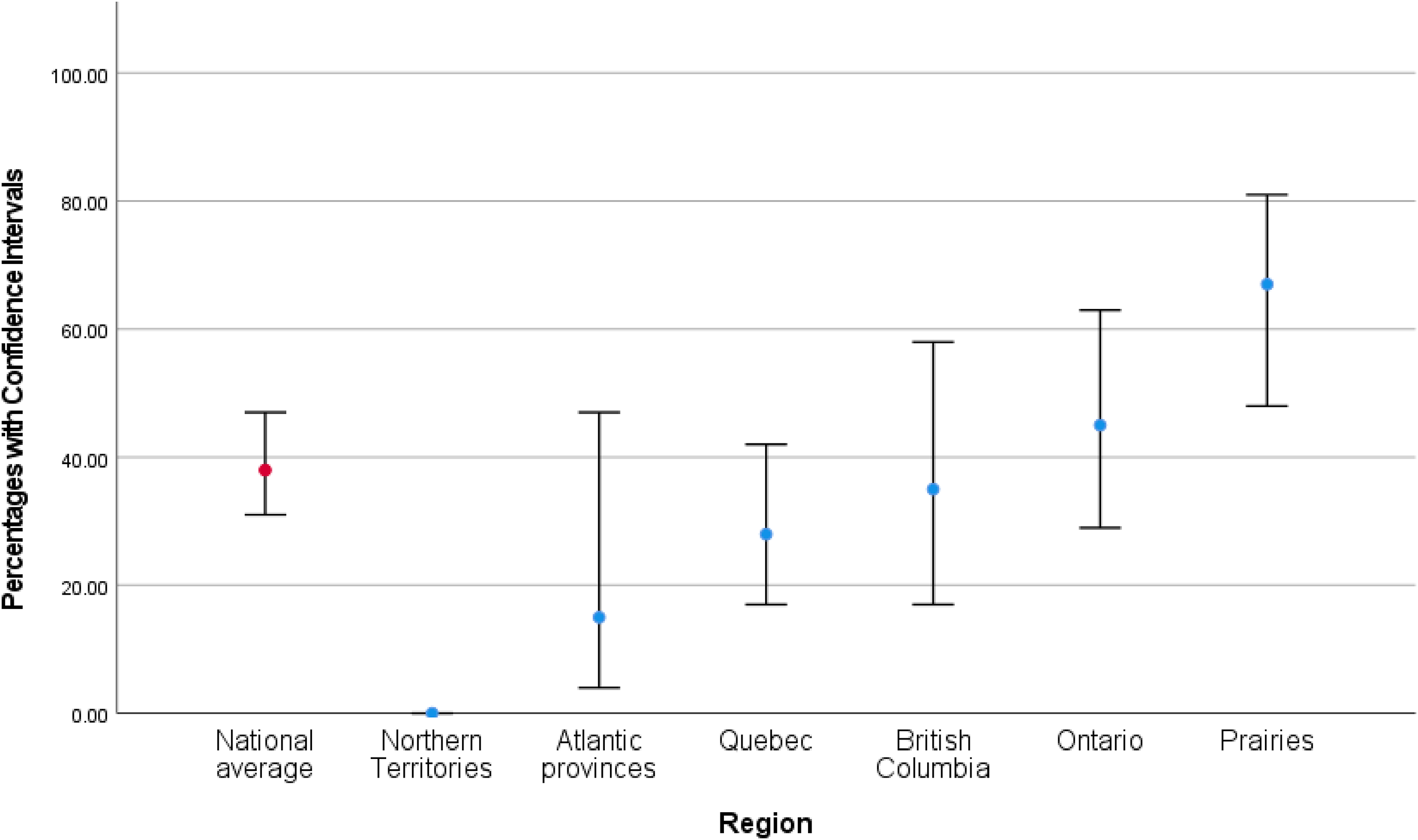
Percentage of organizations that faced challenges due to staff contracting COVID-19, by Canadian region.
Discussion
Our findings demonstrate that the pandemic challenged the way many IPV/SV organizations in Canada operated. Most organizations in our sample struggled with inadequate resources at the start of the pandemic, including material, human, and/or financial resources. Though most of these issues improved with time, 18 months into the pandemic nearly half of all organizations were still struggling with inadequate space to ensure physical distancing and inadequate human resources, reflecting longstanding systemic issues that are more difficult to surmount.
Over the past several decades, the Canadian federal government has continuously decreased funding to women's organizations, including IPV/SV organizations (Boucher & McWhinney, 2017). The situation improved when the current Liberal government took office in 2016; organizations that had been denied funding by the previous government were now reeligible for federal funds and funding to Status of Women Canada was increased (Smith, 2016, 2017). However, experts and organizations have remained critical, citing the government's lack of meaningful consultation about organizations’ needs, the prioritization of IPV organizations at the expense of SV services, and a funding model that emphasizes project funding over core funding as ongoing financial challenges (Boucher & McWhinney, 2017). In 2019, three-fourths of shelters in Canada reported that they were struggling with insufficient funding (Women's Shelters Canada, 2019b). Unstable levels of public funding have led organizations to develop mixed revenue streams that often combine public funds with income from charitable donations and social enterprises (Beres et al., 2009; Eakin & Graham, 2009). Even so, funding challenges remain and often result in low wages for staff and an increased reliance on unpaid volunteers (Merchant & Whiting, 2015). At the same time, staff at IPV/SV organizations often struggle with compassion fatigue, secondary trauma, and burnout due to the emotionally intense nature of their work (Dworkin et al., 2016; Kulkarni et al., 2013; Wood et al., 2019). This combination of low salaries, burnout, and job dissatisfaction can lead to higher staff turnover (Merchant & Whiting, 2015; Wood et al., 2019).
The COVID-19 pandemic began amidst this ongoing insecurity. In response, the federal government allocated approximately $300 million in emergency assistance to gender-based violence organizations (Women and Gender Equality Canada, 2022c). Nearly all organizations we surveyed received emergency funding from a government source and, by November 2021, only 10% reported insufficient funding to handle COVID-related expenses. However, our survey did not collect information on the amount of funding received or whether it was sufficient to offset other COVID-induced financial challenges like canceled fundraisers or to mitigate years of chronic underfunding. In interviews conducted with 17 IPV/SV workers across Canada during COVID-19, the majority (n = 13) emphasized that IPV/SV services were in crisis before the pandemic. While emergency government funding helped cover COVID-related expenses, several participants expressed that it did little to alleviate years of chronic underfunding (Michaelsen et al., 2022). Other studies from Canada have also highlighted how the pandemic exacerbated longstanding financial challenges amongst IPV/SV organizations, due to the cancelation of fundraisers and COVID-related expenses such as PPE and technological equipment (Mantler et al., 2021; Quinlan & Singh, 2020). Critics have also argued that the sudden attention around and funding given for IPV/SV during the pandemic gives the impression that it is an unforeseen public health emergency and masks its “everydayness” in “normal conditions” (Quinlan & Singh, 2020, p. 576).
Our findings also suggest that the pandemic aggravated pre-COVID staffing challenges. Two-thirds of organizations nationwide also reduced the number of volunteers or stopped allowing volunteers to come in entirely. Perhaps unsurprisingly, given shortages of both paid and unpaid staff, the vast majority (88%) of organizations reported that their staff faced an increased workload, and half of all organizations indicated they had staff take leaves of absence for mental health reasons. Burd et al.’s study (2022) corroborate these findings, as their participants emphasized the emotional ramifications of working during the pandemic, including distress, helplessness, reduced job fulfillment, and tensions between staff members, all of which increases the risk of burnout and staff exodus. This convergence of financial and staffing challenges is concerning, as it may have not only affected organizations’ ability to meet demand during a time when both the incidence and severity of IPV/SV are widely thought to have increased (Bucerius et al., 2021; Haag et al., 2022), but also their long-term sustainability. In our qualitative study, service providers expressed concern for their future, knowing that emergency funding was temporary, but the economic impacts of COVID-19 may be long lasting (Michaelsen et al., 2022). Our findings, in concertation with other studies conducted with IPV/SV organizations both before and during COVID-19, suggest that COVID-19 did not simply create new challenges for these organizations but also exacerbated longstanding issues.
Regional Differences
The province of Quebec emerged as unique in several aspects. Compared to national averages, organizations in Quebec were less likely to reduce the number of in-shelter clients, stop services temporarily, or reduce the number of volunteers, despite being the epicenter of the pandemic in Canada during the first wave (March–June 2020) and case counts remaining higher than most other provinces and territories during subsequent waves (Murall et al., 2021; Schiab, 2020). One possible explanation is related to another finding from our survey: a lower proportion of organizations from Quebec reported their staff were fearful of contracting COVID-19 compared to the national estimate (Figure 5). Quebec adopted some of the most stringent COVID-19 restrictions in Canada during the pandemic, including the introduction of a curfew (Cameron-Blake et al., 2021). It is possible that staff in Quebec felt relatively safe carrying out their duties as usual. This theory is consistent with findings from opinion polls. One survey, conducted in early February 2022, revealed that Quebecers were significantly less likely to feel uncomfortable about easing restrictions and to feel scared about COVID-19 (8% vs. national average of 15%), and significantly more likely to believe the worst of the pandemic was behind them (57% vs. national average of 44.5%), compared to other regions (Leger, 2022). Organizations in Quebec also reported a higher number of monetary donations from nongovernmental sources (Figure 4). This increased public support may have strengthened feelings of commitment and solidarity, encouraging IPV/SV organizations to ensure their services remained readily available with minimal disruption.
Another regional difference that emerged was that organizations in the Prairies were more than 1.5 times as likely to report staffing challenges due to staff contracting COVID-19 than the national average (Figure 6). Alberta and Saskatchewan had some of the least restrictive policies toward COVID-19 during 2021 (Cameron-Blake et al., 2021) and the Prairies also have lower vaccination rates compared to the rest of Canada. As of July 2021, 77.9% of the population in the Prairies were fully vaccinated (2+ doses) compared to a national average of 83.44% (Government of Canada, 2022), which could mean a higher rate of infection in the region compared to other parts of the country.
Finally, a startling 81% of organizations in Ontario reported staffing challenges due to staff taking a leave of absence for mental health reasons, compared to a national average of 49%. The reasons for this difference are unclear.
Strengths and Limitations
One of the main strengths of this study is that IPV/SV service providers assisted with the development of the survey, ensuring questions were relevant to their organizations and provided information of use to them. In addition, we created a comprehensive sampling frame and the response rate to our survey was high (47%) compared to other online surveys, which increases confidence that our sample is reasonably representative of service organizations across Canada. Our sample includes organizations from every province and territory and is evenly distributed among rural and urban areas. By providing the survey in two languages; English and French, we ensured that French Canadians, Canada's largest minority group, could easily participate.
Our study also had several limitations. Responses to questions regarding experiences during the first month of the pandemic may be affected by recall bias. As part of our instructions, only one member of management staff per organization was to complete the survey and their perceptions may have differed from other members of their team. Our questions may not have covered or captured all the experiences of organizations; for instance, we only asked about fluctuations in monetary donations and did not ask about variations in material donations such as clothes, food, hygiene products, etc. However, more than three-quarters of organizations stated they had stopped accepting material donations at some point during the pandemic. It is therefore unlikely that material donations helped make up for any losses in monetary donations. We were unable to estimate the impact of variations in the range and restrictiveness of public health intervention across or within provinces/territories using a cross-sectional survey design.
Conclusion
The COVID-19 pandemic disrupted the work of IPV/SV organizations in Canada in several ways. Those organizations adapted to shifting public health guidelines by scaling back or pausing activities altogether, temporarily stopping volunteers from coming in, reducing the number of in-shelter clients, and canceling fundraisers. Challenges resulting from the pandemic included increased costs, heavier workloads, and staffing shortages. These pandemic-induced challenges occurred within a broader context of chronic underfunding, compounding the many struggles such organizations faced prior to the pandemic. Predictable and adequate funding from governments to IPV/SV services in nonemergency times could help improve wages and working conditions for staff and thus ameliorate staff retention, which would both aid and minimize disruption to service delivery during crisis situations.
Footnotes
Acknowledgments
The authors would like to thank the rest of the research team, including the members who are management staff of IPV and SV organizations, who helped guide us in the design of the study and development of the interview guide.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Centre de Recherche en Santé Publique (Grant No. RQS00285).