
Abstract
Factors associated with IPV among immigrant women are not well understood. Using linked immigration and justice data, we compared the incidence of justice-identified IPV (JIIPV) among 58,564 international immigrant women born outside of Canada, 30,098 women born in other Canadian provinces (i.e., interprovincial migrants), and 88,662 long-term Manitoban resident women. International immigrant women had the lowest incidence of JIIPV compared to matched long-term Manitobans (adjusted hazard ratio (aHR) 0.49, 95% CI: 0.43–0.56) and interprovincial migrants (aHR 0.56, 95% CI: 0.43–0.73). Among immigrants, JIIPV varied substantially according to birthplace, increased with length of residence, and was less frequent among secondary immigrants.
Introduction
Intimate partner violence (IPV) includes physical, sexual, or psychological violence by a current or former intimate partner. It has been estimated that about one in three women encounter IPV in their lifetime (WHO, 2017). IPV is associated with negative acute and chronic health outcomes and death by homicide (Campbell, 2002; Velopulos et al., 2019). US crime data show that about one in five homicide victims are killed by an intimate partner (Cooper & Smith, 2011). In Canada, victims of IPV account for about 30% of all victims of violent crime reported to the police, and the vast majority are women (Burczycka, 2018). IPV is a significant public health concern across population groups, including immigrants. Immigrant women are vulnerable as immigration and settling in a new country can be stressful processes that impact mental health and increase domestic violence (Jayasuriya-Illesinghe, 2018; Raj et al., 2005). Also, cultural, legal, and institutional barriers, lack of supportive social networks, the fear of losing children, and financial concerns often keep immigrant women from seeking help and leaving abusive relationships (Barrett & Pierre, 2011; Guruge & Humphreys, 2009; Sabri et al., 2018). Moreover, the complexity and sensitive nature of IPV pose challenges to its measurement in research studies. The incidence of IPV among immigrant women in quantitative studies varies according to the use of different definitions, data collection approaches, and subgroups included in the studies (Brownridge & Halli, 2002; Daoud, O’Campo et al., 2012; Daoud, Urquia et al., 2012; Du Mont & Forte, 2012; Gonçalves & Matos, 2016).
The justice system plays a key role in deterring domestic violence and supporting victims by holding perpetrators accountable through legal processes. IPV captured by the criminal justice system represents a more extreme subset of IPV cases characterized by severe and repeated violence (Johnson, 2008). However, there has been limited research examining the risk of IPV using justice data (Cerulli et al., 2014; Koppa & Messing, 2019; Kothari & Rhodes, 2006; Rhodes et al., 2010) and, to our knowledge, particularly among immigrant women.
International immigration to Manitoba has steadily increased over time. Between 2007 and 2016, more than 141,800 immigrants have settled in Manitoba. In 2016, international immigrants accounted for 20.7% of Manitoba's labor force, up from 14.5% in 2006 (Manitoba Immigration Data Portal, 2016). All new permanent residents to Canada, including economic and refugee applicants and their dependents are eligible for the free-of-charge publicly funded universal health care coverage, which includes physician and hospital services that are provincially administered. Some temporary residents (work permit visas) are also eligible for the provincial healthcare coverage. A small proportion of refugee claimants (also known as asylum seekers) are not covered by the Manitoba Health Insurance Plan but by a federally funded program (i.e., the Interim Federal Health Program) while awaiting the resolution of their cases. Refugee claimants who are granted permanent residency become eligible for provincial healthcare insurance. Since health care and justice services are provincially administered, Canadians relocating to Manitoba from other provinces must also register as new residents to be able to receive free-of-charge health care services in the province. Eligibility for healthcare coverage ends at death or move out of province. The Manitoba Health Insurance Plan Registry collects and maintains information on all Manitoba residents ever registered, making it the most complete roster of the Manitoba population, which is used to conduct data linkages with other sectoral databases, such as education, housing, social programs, and justice.
By using linked justice and immigration data, we conducted a population-based, retrospective matched cohort study to examine the incidence of justice-identifiedIPV (JIIPV) among immigrant women compared to two groups of Canadian women: interprovincial migrants, defined as women born in other Canadian provinces, and long-term Manitoba residents with continuous residence in the province of Manitoba, Canada. We also assessed immigration characteristics associated with JIIPV among immigrant women, such as region of birth, secondary immigration, refugee status, knowledge of Canadian official languages, and duration of residence.
Methods
Study Design, Setting, and Participants
This population-based retrospective matched cohort study was conducted in Manitoba, Canada. We included immigrant women, interprovincial migrants, and long-term Manitoban women aged 18 to 64 years in Manitoba from January 1, 2002, to December 31, 2016. Interprovincial migrants were women born in other Canadian provinces. Long-term Manitobans included those born in Manitoba or with a Manitoba health coverage start before 1974 (when the Registry began, and not indicating a move from outside of Manitoba). Immigrant women were matched to two groups of nonimmigrants on age, marital status, and place of residence at the time of their provincial health coverage start (index date) (Figure 1). All women aged 18–60 years were followed as of their index date (between January 1, 2002, and December 31, 2012, to allow for a minimum of 4 years of follow-up) until the first occurrence of JIIPV, including violent death. Participants were censored if lost to follow-up (i.e., moving out of Manitoba), death due to causes other than JIIPV, or end of the study period.
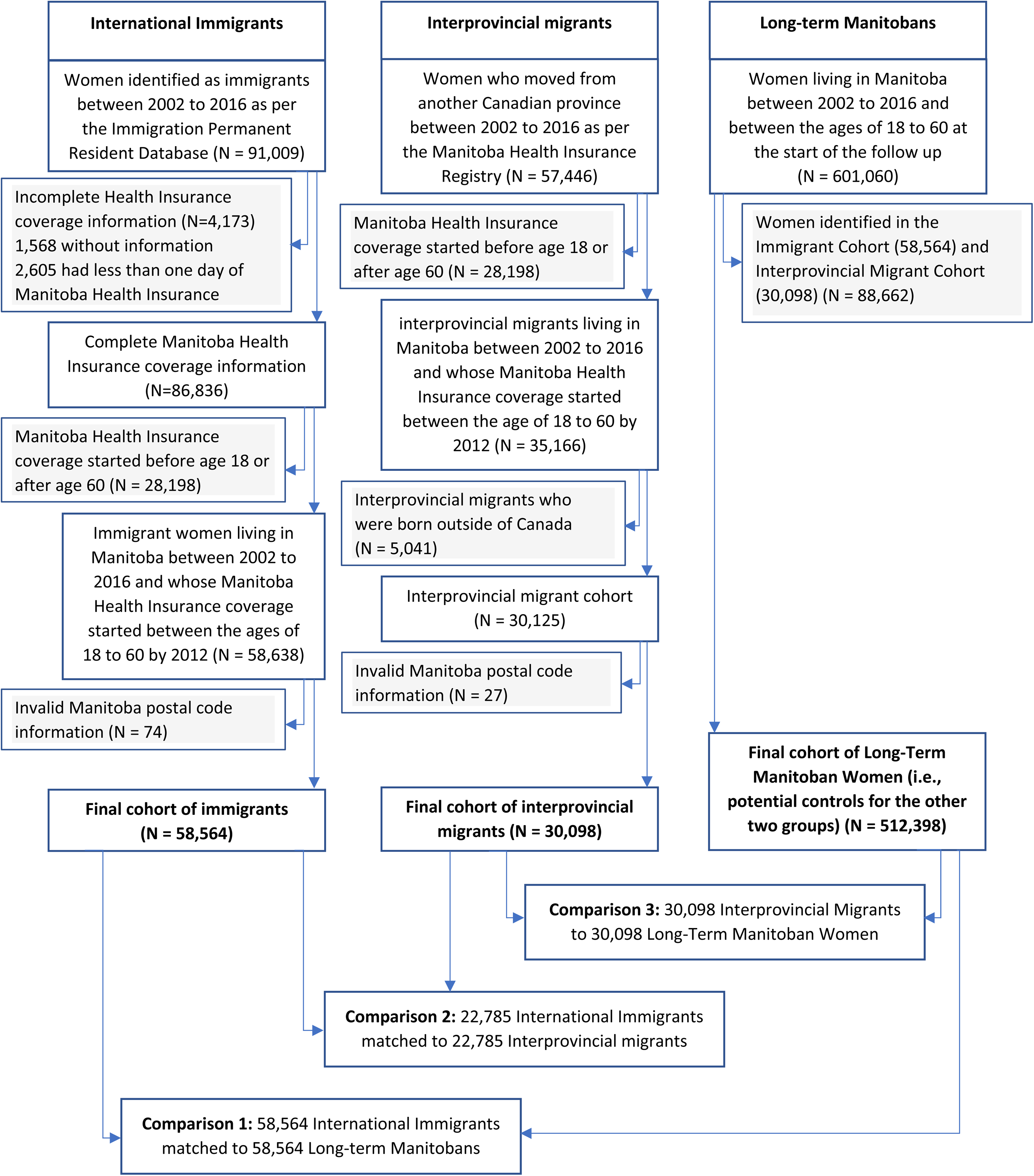
Flowchart of comparison groups.
Data Sources
Several de-identified administrative databases were linked at the individual level using a unique scrambled personal health identification number in the Manitoba Population Research Data Repository based on the Manitoba Health Insurance Registry (MHIR), which contains demographic data, dates of health care coverage, and residence location of all residents in the province. The Justice Prosecution Information and Scheduling Management (PRISM) and disposition records (Criminal Courts Automated Information Network, CCAIN) contain prosecutions and disposition records for crimes including domestic violence committed in Manitoba. The Immigration, Refugees and Citizenship Canada Permanent Resident (IRCC-PR) database contains individual-level information recorded for permanent residents who landed in Canada from January 1, 1985, to December 31, 2017. The IRCC has been linked to the MHIR with a 96% linkage rate (Urquia et al., 2021). The Tenant Management System (TMS) contains data on applicants for social housing. Employment Income Assistance (EIA) and Social Allowances Management Information Network (SAMIN) data contains information on households receiving financial support under the provincial employment and income assistance program. Vital statistics mortality data captures information on deaths in the province. Data from the 2006 Canadian Census contains information on community-level income.
Measurements
Justice-identified Intimate partner violence (JIIPV) was the dependent variable. An episode of JIIPV was present when an eligible woman appeared as a victim of a domestic violence incident in a prosecution or disposition record in the justice PRISM and CCAIN databases (Nesca et al., 2021). The incidence of JIIPV was defined as the first episode of IPV that occurred in the study period. The nature of the IPV incident may involve any type of violence (e.g., psychological, emotional, verbal, sexual, or physical). However, incidents only appear in the criminal justice databases when charges are laid by the Winnipeg Police Services or the Royal Canadian Mounted Police and the victim and the accused are identified in their initial reports. Disposition records are cross-referenced to prosecution records and contain the charges and corresponding sentences that apply to the accused. To remove cases of domestic violence that were not IPV, incidents in which the victim was a parent, a child, or a sibling of the accused were excluded, retaining records where the accused was a male who may be a spouse, common-law, or dating partner. Potential perpetrators of IPV may have been accused of multiple charges at the same IPV incident or at a subsequent incident. To remove duplicates, we retained only one charge made “against a person” directly related to the IPV incident and excluded administrative violations such as breaking curfews or offences against the law, such as speeding, that applied to the same individual.
Comparison Groups
International immigrants included foreign-born women who were granted permanent residence in Canada from January 1, 1985, to December 31, 2012, assessed by a valid record in the IRCC Permanent Resident Database, resided in Manitoba from January 1, 2002, to December 31, 2016, assessed by a valid registration for healthcare coverage during the period, and were 18 to 60 years between January 1, 2002, and December 31, 2012, to allow for a minimum 4-year follow-up until age 64 in 2016.
Interprovincial migrants included women with previous health care coverage in other Canadian provinces who were newly registered for Manitoba's healthcare coverage; were Manitoba residents from January 1, 2002, to December 31, 2016; were 18 to 60 years between January 1, 2002, and December 31, 2012, to allow for a minimum 4-year follow-up until age 64 in 2016; and were not in the IRCC Permanent Resident Database.
Long-term Manitobans included women born in Manitoba after 1974 or who were covered by the provincial healthcare coverage before 1974, when the current registry was created. An unknown, albeit small, proportion of women included in this group may have been born outside of Manitoba and migrated to the province before the registry existed. Likewise, a small proportion of international immigrants obtaining permanent residence before 1985 may be misclassified in this group, due to the lack of immigration data prior to that date.
Covariates
Covariates were measured at the time of the index date. Demographic variables included age, presence of children living in the household, and marital status as of the index date. Location of residence (urban or rural) was determined from the 6-digit postal code obtained from the Health Insurance Registry, as well as the neighborhood income quintile, which was measured by the Census mean small-area income where the residence was located. Other socioeconomic variables included receipt of income assistance, rent assistance, and living in social housing. Variables representing specific characteristics of immigrant women were the region of birth, based on the United Nations classification of countries (The United Nations, 1999); years of residence in Canada; secondary migration, defined as a migration from the country of last permanent residence that is different from the country of birth (Urquia et al., 2010); refugee status; education level; and knowledge of Canadian official languages (English/French).
Statistical Analysis
Descriptive statistics including means and standard deviations (SD), frequencies, and percentages were used to describe participant characteristics. Incidence of JIIPV was expressed as the number of events per 1000 women during the follow-up period.
Two sets of controls were used. Immigrant and migrant women were one-to-one matched to long-term Manitoban women based on age, marital status, and region of residence at the index date when they started their first health coverage in Manitoba (comparisons 1 and 2). Immigrant women were also matched one-to-one with interprovincial migrant women based on age, sex, region of residence, marital status, and date of moving to Manitoba (comparison 3). Unadjusted and adjusted conditional Cox proportional hazard models were used to estimate hazard ratios (HRs) with 95% confidence intervals (CIs) of JIIPV risk in three comparisons: immigrant women vs matched long-term Manitoban controls (comparison 1), immigrant women vs matched interprovincial migrant (comparison 2), and interprovincial women vs matched long-term Manitoban (comparison 3). To assess immigrant characteristics associated with the risk of JIIPV within the immigrant cohort, unconditional Cox proportional hazard models were used since comparisons were between immigrant subgroups. Covariates included in the models were selected a priori based on the literature and data availability. Women from West Europe, North America, and Oceania, more culturally related to Manitoban women due to the historically dominant European presence in the ethnic composition of Canada (Li, 2000), were used as the internal reference group for comparisons by region of birth. Records with missing data were very few and excluded during the cohort creation (see Figure 1, Flowchart). All analyses were conducted using SAS V9.4 (SAS Institute Inc., Cary, NC). Cell sizes less than 6 were not reportable under Manitoba's privacy regulations.
Ethics Approval
This study was approved by the University of Manitoba research ethics board (HS23239/2019:378) and the provincial Health Information Privacy Committee (2019/2020-33).
Results
Characteristics of Participants
Table 1 presents the sociodemographic factors of the participants. During the study period of 14 years, 58,564 immigrant women and 30,098 interprovincial migrant women aged 18–64 came to Manitoba, who were matched to a total of 88,662 long-term Manitoban controls (comparisons 1 and 2 in Figure 1). Among women in the immigrant cohort, 22,785 were matched to interprovincial migrants (comparison 3). As expected, similar frequencies are observed for the matching variables age, place of residence, and marital status. Immigrant women were overrepresented in the lower income quintile, less likely to have received income assistance, and more likely to have received rent assistance compared to their control counterparts.
Characteristics of the Matched Cohorts of International Immigrant, Interprovincial Migrant, and Long-Term Manitoban Women, 2002–2016a.
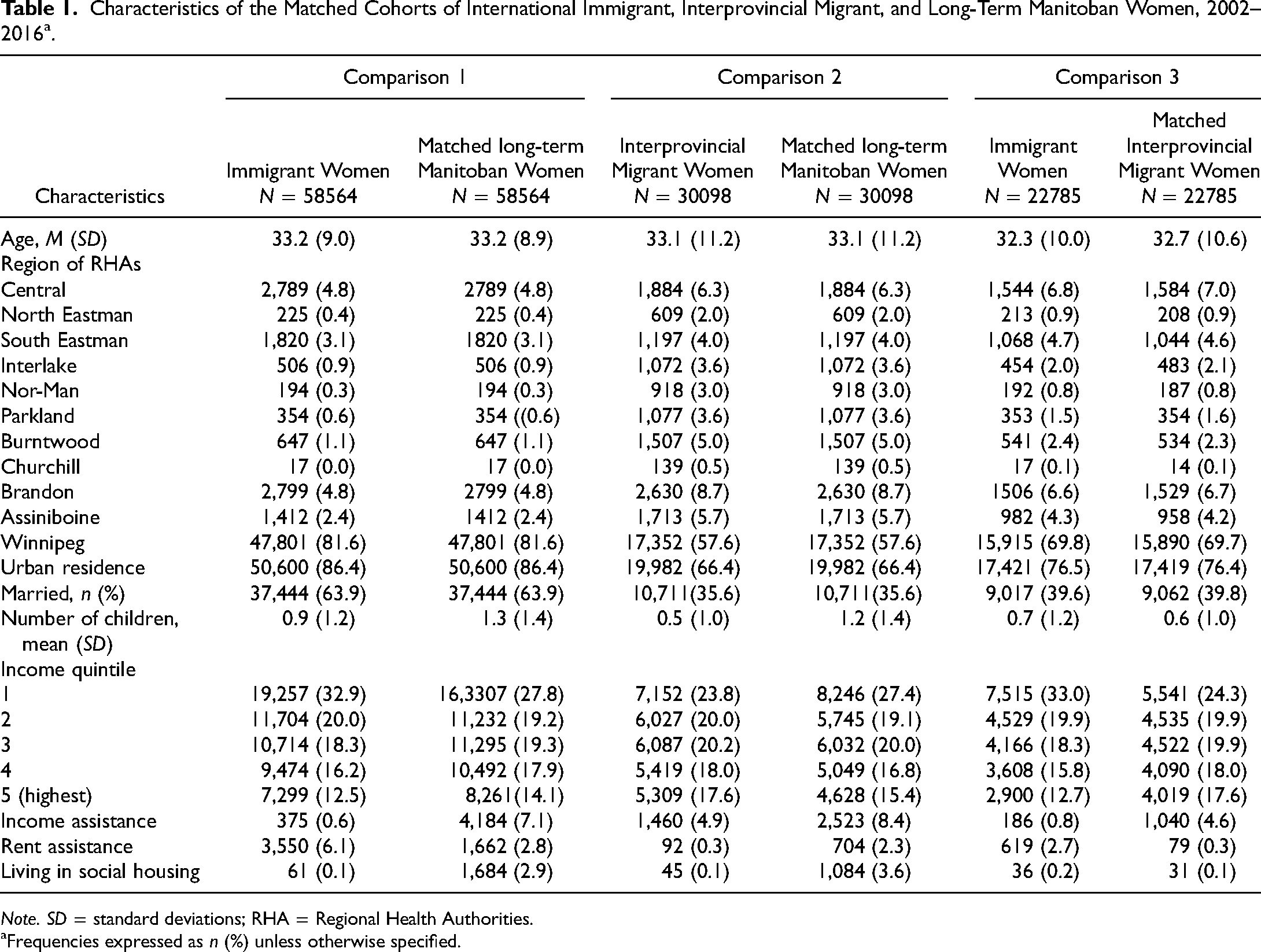
Note. SD = standard deviations; RHA = Regional Health Authorities.
Frequencies expressed as n (%) unless otherwise specified.
Comparison of JIIPV Between Immigrant and Nonimmigrant Women
Table 2 compares the incidence and HR of JIIPV among immigrant, interprovincial migrant, and long-term Manitoban women. Overall, in the unadjusted analysis, immigrant women had a lower incidence of JIIPV compared to their matched long-term Manitoban (comparison 1: 7.91 vs 26.43 per 1,000 women) and interprovincial migrant counterparts (comparison 3: 8.87 vs 13.56 per 1,000 women). The association was attenuated after adjustment for covariates, but it remained statistically significant. The adjusted HR was 0.49 (95% CI: 0.43–0.56) for comparison 1 and 0.56 (95% CI: 0.43–0.73) for comparison 3, respectively. Interprovincial migrant women also showed a lower incidence of JIIPV compared to their matched long-term Manitoban counterparts (15.71 vs 42.72 per 1,000 women), but the association was no longer statistically significant (p = 0.08) after adjustment.
Incidence and Hazard Ratios of JIIPV Among International Immigrant, Interprovincial Migrant, and Long-Term Manitoban Women, 2002–2016.
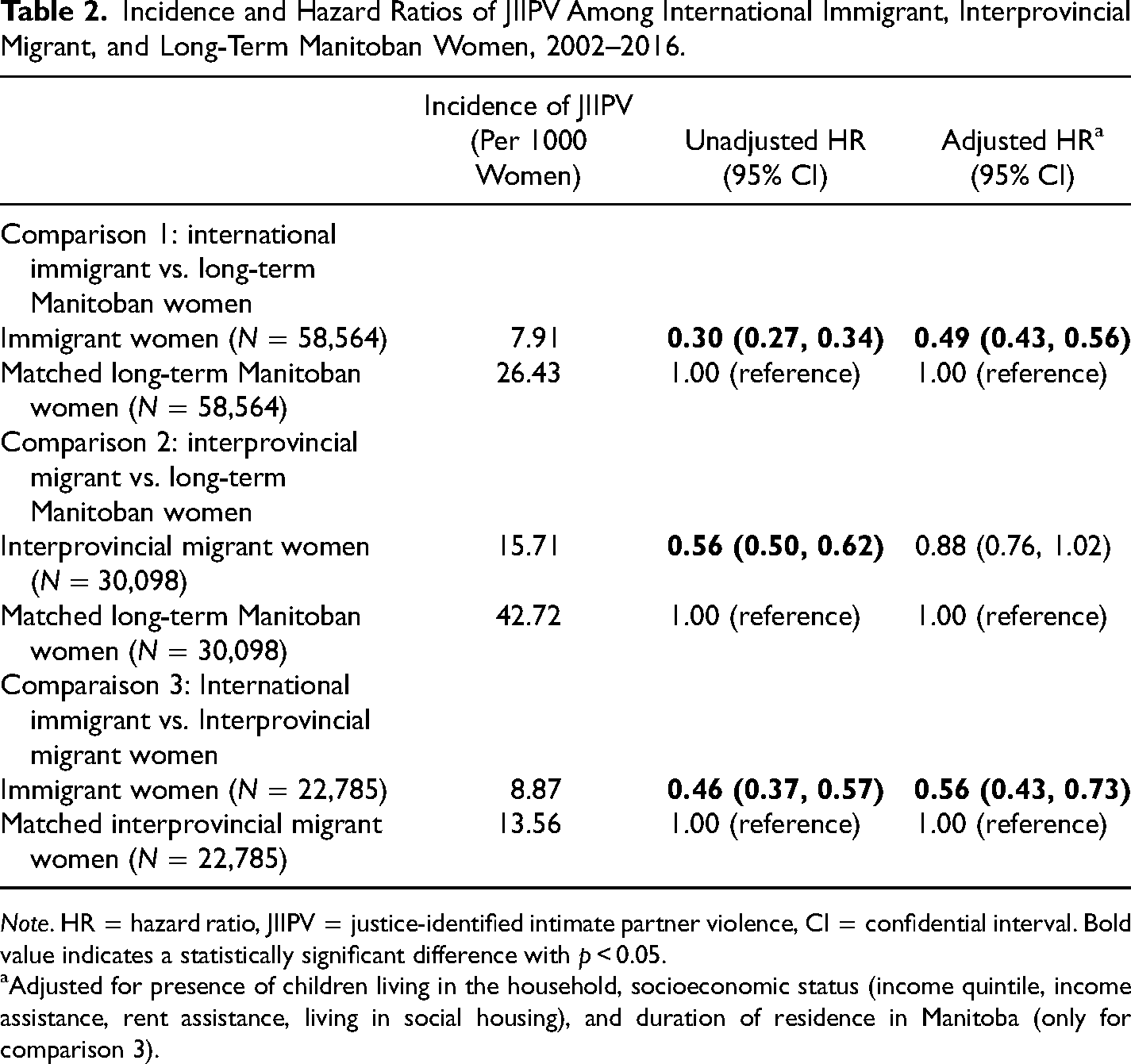
Note. HR = hazard ratio, JIIPV = justice-identified intimate partner violence, CI = confidential interval. Bold value indicates a statistically significant difference with p < 0.05.
Adjusted for presence of children living in the household, socioeconomic status (income quintile, income assistance, rent assistance, living in social housing), and duration of residence in Manitoba (only for comparison 3).
JIIPV Among Immigrant Women
Table 3 presents the incidence and HR of JIIPV associated with immigration characteristics among immigrant women. There was heterogeneity in the likelihood of JIIPV according to the region of origin. In the unadjusted analysis, women from Northern Africa, sub-Saharan Africa, Latin America and the Caribbean, and Southern Asia had a greater likelihood of JIIPV compared to their counterparts from West Europe, North America, and Oceania, while those from East and Southeast Asia and Central and Western Asia had decreased likelihood. The association remained statistically significant in immigrants from Northern Africa (aHR 2.07, 95% CI: 1.11–3.84), Latin America and the Caribbean (aHR 1.66, 95% CI: 1.03–2.68), and East and Southeast Asia (aHR 0.63, 95% CI: 0.41–0.97) after adjustment. We further explored these associations by closely examining regions or countries with more than 1000 immigrant women (Supplemental Table S1). In particular, those originally from Nigeria (aHR 2.18, 95% CI: 1.15–4.14) and the Philippines (aHR 0.61, 95% CI: 0.38–0.97) had the highest and lowest rates of justice-involved domestic violence by their partners, respectively, compared to those of West Europe, North America, and Oceania (Supplementary table S1). Furthermore, secondary migration was negatively associated with the likelihood of JIIPV, while 5 or more years of residence in Canada were positively associated with JIIPV. Lack of knowledge of Canadian official languages and refugee status were no longer associated with JIIPV victimization among immigrant women after adjustment.
Incidence and Hazard Ratios of JIIPV Among International Immigrant Women in Manitoba, 2002–2016 (N = 58,564).
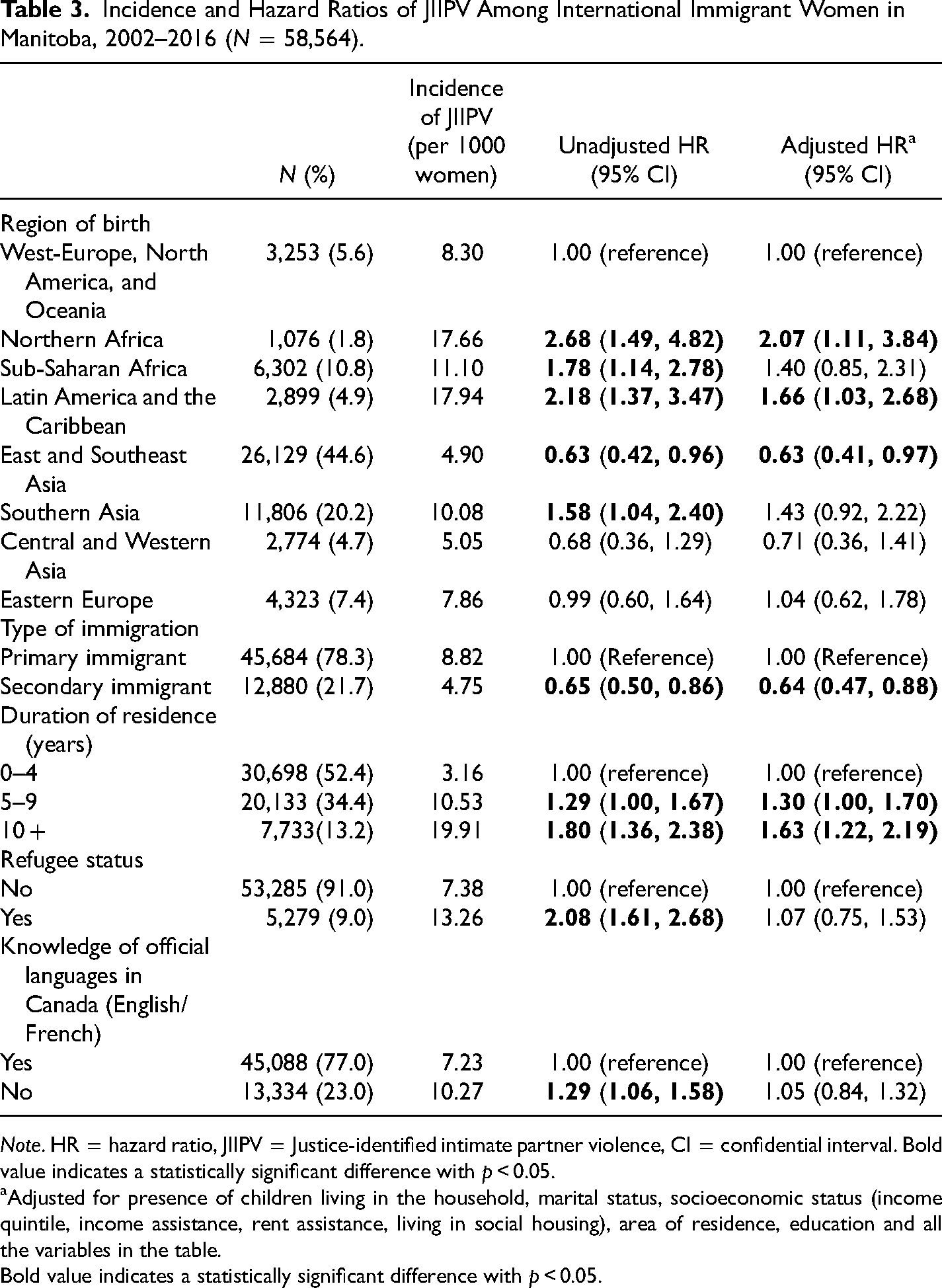
Note. HR = hazard ratio, JIIPV = Justice-identified intimate partner violence, CI = confidential interval. Bold value indicates a statistically significant difference with p < 0.05.
Adjusted for presence of children living in the household, marital status, socioeconomic status (income quintile, income assistance, rent assistance, living in social housing), area of residence, education and all the variables in the table.
Bold value indicates a statistically significant difference with p < 0.05.
Discussion
In this population-based cohort study, we found that immigrant women had a lower likelihood of JIIPV compared to that of matched interprovincial migrant and long-term Manitoban women. Immigrant women from Africa (particularly those from North Africa and Nigeria) and Central America and the Caribbean were more likely to experience JIIPV compared to their counterparts from West Europe, North America, and Oceania, while those from East and Southeast Asia (particularly those from the Philippines) were less likely to experience JIIPV. Furthermore, secondary migration was associated with a decreased likelihood of JIIPV, while longer length of residence in Canada was associated with greater likelihood.
Although no prior studies have examined whether the likelihood of JIIPV between immigrant women and women in the general population differs in the justice data, our findings are consistent with earlier Canadian studies that have reported a lower prevalence of IPV among immigrant women in a national survey (Daoud, O’Campo, et al., 2012; Daoud, Urquia, et al., 2012; Du Mont & Forte, 2012). Similarly, research of the 2014 General Social Survey (GSS) on Canadians’ Safety show that immigrants experienced a significantly lower rate of violent victimization than nonimmigrants (Ibrahim, 2018). In contrast, some population-based research focusing on broader definitions of IPV have reported conflicting results. For example, one study using data from two iterations of Statistics Canada's GSS (1999 and 2004) reported an inconsistent pattern of violence against immigrant women, particularly against those from developing countries whose rate of reporting IPV victimization relative to immigrant women from developed nations and Canadian-born women changed from being the highest in the 1999 GSS to the lowest in the 2004 GSS (Brownridge, 2009). Nonetheless, the lower incidence of JIIPV among immigrant women found in our study may also reflect the underestimation of IPV among immigrant women captured in the justice data and inequality in access to the criminal justice system. Compared to the native-born population, marginalized immigrant women have many unique concerns discouraging them from seeking formal help. These may include cultural attributes, financial dependency on their partners, lower levels of trust, experiences of discrimination in the host country (Du Mont & Forte, 2012; Eisikovits et al., 2004; Finfgeld-Connett & Johnson, 2013), and the fear of compromising their residence status, especially if the perpetrating partner was the sponsor (Raj & Silverman, 2002). Importantly, general fear of the police, perceptions of racial bias due to systemic structural racism and racial disparity in the justice system may also play a role in influencing immigrant women from reporting violent episodes to the police (Couture-Carron et al., 2022; Wortley & Owusu-Bempah, 2009).
Our results indicate that the likelihood of experiencing JIIPV varied according to immigrant women's characteristics, such as region of birth. This is not surprising since IPV victimization in a heterogeneous pool of immigrants may not only reflect socioeconomic disadvantage but also be related to characteristics of the sociocultural environment of their places of origin, such as traditional gender roles, patriarchal beliefs, normalization of abuse, and the reluctance to disclosure and leave the abused partner. For example, high lifetime rates of IPV have been observed among Latina women immigrants in the United States, which may reflect dominant male roles among Latinos and traditional family structures (Hass et al., 2000; Hazen & Soriano, 2007). In immigrants from Africa with a very high prevalence of IPV (Shamu et al., 2011), such as Nigerian women, spousal abuse is widely accepted as a private matter of the home (Boy & Kulczycki, 2008; Kalunta-Crumpton, 2013, 2017). In contrast, women from Asia are reported to be reluctant to use health care for physical abuse (Ahmad et al., 2009; Raj & Silverman, 2002) and less likely to disclose incidents of sexual and physical assault committed by an intimate partner due to beliefs in traditional values of preservation of family harmony (Huisman, 1996). IPV is often considered to be normative behavior in a patriarchal family, where women's acculturation and integration into a more liberal host society are viewed as a threat to their cultural norms (Agnew, 1998; Ahmad et al., 2009). Furthermore, we found that the likelihood of JIIPV increased with longer residence in Canada, which was also reported elsewhere (Brownridge & Halli, 2002; Du Mont et al., 2012; Hyman et al., 2006). Although the mechanisms behind this association are not clear, it has been suggested that the assimilation process distances immigrants from the protective factors of their cultures of origin and supportive social networks (Keefe, 1984; Vega, 1990). The higher incidence of JIIPV among refugees was explained out by sociodemographic and immigrant characteristics. Finally, we found that secondary immigrants who resided in an intermediate country before immigrating to Canada experienced significantly lower incidence of JIIPV than those who immigrated directly from their countries of birth, which is a novel finding. Secondary immigrants have been portrayed as a highly selected group of economic immigrants with higher educational credentials and upward global socioeconomic mobility and linked with favorable health outcomes (Urquia et al., 2010). Further research may elucidate the mechanisms explaining this association.
Limitations
Our study has some limitations. First, the administrative data used in this study were not collected for research purposes. Cases of IPV captured by the criminal justice system are thought to represent a subset of more severe and chronic cases of violence that came to the attention of the police and may severely underestimate the frequency of IPV in the population. Residual confounding cannot be ruled out due to our inability to control for unmeasured covariates, such as social support (Kim, 2019) and stress experienced by immigrants in the process of adaptation to the host country (Berry, 1997). Also, we were unable to address the impacts of systemic structural racism and racial disparity in the justice system (Wortley & Owusu-Bempah, 2009) among the immigrant minorities included in our study. Second, we focused on JIIPV victimization of immigrant women committed by intimate male partners, and therefore our findings cannot be directly generalizable to male victims or victims in nonheterosexual relationships. Third, our measure of JIIPV should not be regarded as an estimate of the incidence of IPV in the population because it captured only serious IPV episodes involving the police and the justice system. As well, many abused immigrant women, and particularly newly arrived immigrant women, may be less comfortable reporting to the police and getting involved with the justice system due to their socioeconomic vulnerability (Ahmad et al., 2009; Barrett et al., 2011; Tam et al., 2016), and therefore, the lower likelihood of JIIPV observed in this study may be also influenced by inequality in seeking formal help among immigrant women. According to the 2014 GSS in Canada, more than half of immigrant victims of violence did not contact the police regarding the incident (Ibrahim, 2018). Our measure of the duration of residence simply captures time since migration and should not be interpreted as synonymous with assimilation or integration. Lastly, JIIPV exposure was defined at the first incident of JIIPV in the study period and so subsequent JIIPV episodes were not considered. Nevertheless, because this study was based on population data, it provides an accurate portrait of JIIPV among immigrant women in Manitoba, Canada.
Conclusions
This population-based study indicates that, overall, immigrant women were less likely to experience JIIPV than nonimmigrants. However, among immigrant women, those from Northern Africa, Nigeria, Central America, and the Caribbean and those with more than five years of residence experienced higher rates of JIIPV. Immigrants constitute a heterogeneous group with diverse influences of origin. Future research needs to better investigate the contribution of protective factors associated with immigrants’ places of origin and further examine the mechanism behind the observed heterogeneity of risk, including systemic structural racism in the justice system and disproportionate policing of IPV among certain ethnic minorities and racialized groups.
Supplemental Material
sj-doc-1-vaw-10.1177_10778012231178001 - Supplemental material for Intimate Partner Violence Among International and Interprovincial Migrants: A Population-Based Analysis of Canadian Linked Immigration and Justice Data
Supplemental material, sj-doc-1-vaw-10.1177_10778012231178001 for Intimate Partner Violence Among International and Interprovincial Migrants: A Population-Based Analysis of Canadian Linked Immigration and Justice Data by Lixia Zhang, Wendy Au, Roheema Ewesesan, Alexa R. Yakubovich, Douglas A. Brownridge, and Marcelo L. Urquia in Violence Against Women
Footnotes
Author Acknowledgements and Disclosures
This research was supported by a Canadian Institutes of Health Research grant of MLU [grant number FDN-154280]. MLU holds a Canada Research Chair in Applied Population Health [grant number 950-231324]. ARY was supported by a CIHR Health System Impact Postdoctoral Fellow (HSI-166388). The funders had no involvement in the preparation or publication of the manuscript.
The authors acknowledge the Manitoba Centre for Health Policy for the use of data contained in the Manitoba Population Research Data Repository under project #2020-009. We would like to thank Randy Walld for helping with the matching of the groups. We acknowledge Immigration, Refugees and Citizenship Canada, Manitoba Health Seniors and Active Living, Manitoba Families, Manitoba Justice, the Winnipeg Regional Health Authority, and Manitoba's Vital Statistics Agency for the use of their data. The results and conclusions are those of the authors and no official endorsement by the Manitoba Centre for Health Policy, Manitoba Health, or other data providers is intended or should be inferred.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Canadian Institutes of Health Research, Canada Research Chairs, (grant number FDN-154280, HSI-166388, 950-231324).
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.