
Abstract
This cross-sectional study describes knowledge, perceived competence, and behaviors relative to intimate partner violence (IPV)-related brain injury (BI) among staff in residential domestic violence shelter programs across a New England state. A 23-item questionnaire was administered to registrants of an online IPV-related BI training series. Within this sample, knowledge about IPV-related BI was high, but relative to providing screening, accommodations, and specialized referrals to survivors with BI, perceived competence was low, and behaviors were infrequent. IPV shelter agencies should facilitate IPV-related BI training programs for staff and prioritize developing and implementing BI screening, accommodation, and referral policies and procedures.
Keywords
Intimate partner violence (IPV) is a public health problem that affects over 10 million people in the United States annually (Breiding et al., 2015). Although individuals of all gender identities 1 can experience IPV, individuals who identify as women are disproportionately affected (Smith et al., 2018). Nearly one in three women experience one or more forms of IPV in their lifetime and one in four women experience severe IPV (Breiding et al., 2014). IPV can include physical, sexual, or psychological abuse, including controlling or stalking behaviors (World Health Organization & the Pan American Health Organization, 2012). Experiencing IPV is linked to myriad adverse physical, biopsychological, social, behavioral, and economic outcomes (Breiding et al., 2015; Coker et al., 2002; Randle & Graham, 2011).
One of the most consequential outcomes of IPV is brain injury (BI) from physical abuse. IPV-related brain injuries are categorized as either traumatic brain injury (TBI), caused by a bump, blow, or jolt to the head that disrupts the normal function of the brain (Centers for Disease Control and Prevention, 2019), or strangulation-induced brain injury (aka anoxic/hypoxic brain injuries) caused by a complete (anoxic) or partial (hypoxic) restriction of oxygen to the brain or a vascular-related injury from the external pressure on the neck, resulting in cellular tissue death and/or build-up of blood in the brain (Lacerte et al., 2020; National Institute of Neurological Disorders and Stroke, 2020; Wilbur et al., 2001). Mechanisms of physical violence that have the potential to cause a BI may include pushing, shoving, or throwing the victim up against something, choking/ strangulation, or suffocation with objects such as pillows, violent shaking, hair-pulling, punching, hitting, and blows to the head, neck, or face with a fist or a heavy object (Kwako et al., 2011; Monahan & O’Leary, 1999; Valera & Berenbaum, 2003; Wilbur et al., 2001).
It is common for women to report instances and/or signs of BIs after experiencing physical violence by past or present partners (Jackson et al., 2002; Kwako et al., 2011; Monahan & O’Leary, 1999). One nationally representative study found that 14.6% of women—or approximately 6.2 million—aged 18 years or older reported being “knocked out after getting hit, slammed against something or choked” as a result of a rape, stalking, or physical violence by an intimate partner (Breiding et al., 2014). Research also suggests that IPV survivors often experience multiple head injuries over multiple incidents of violence (Jackson et al., 2002; Monahan & O’Leary, 1999; Murray et al., 2016; Valera, 2018; Valera & Berenbaum, 2003) and that there is a dose–response relationship with respect to the number of blows to the head or strangulation attempts and symptom severity, such that women who experience multiple-incident head or neck injuries experience more severe post-concussive symptoms than women who experience a single-stage isolated BI (Corrigan et al., 2003; Jackson et al., 2002; Kwako et al., 2011).
Symptoms of a BI include cognitive, physical, emotional, and behavioral impairments, and a loss of consciousness is not necessary for a BI to occur (Centers for Disease Control and Prevention, 2019). Symptoms may include difficulty thinking clearly, concentrating, remembering new information, problem solving, planning or processing, language deficits, headaches, fuzzy or blurred vision, nausea or vomiting, dizziness, sensitivity to noise or light, balance problems, fatigue, irritability, sadness, nervousness or anxiety, and sleep disturbances (Centers for Disease Control and Prevention, 2019; Jackson et al., 2002; Valera & Berenbaum, 2003). These symptoms may have an immediate onset, or they may be delayed and persist for months after the initial incident, causing sustained difficulties in daily functioning, interpersonal relationships, and work life (Monahan & O’Leary, 1999).
Community-based domestic violence emergency shelters provide short-term refuge and housing for IPV survivors and their children fleeing imminent harm or who are experiencing homelessness (Chanley et al., 2001; Lyon, 2008). They are typically staffed by advocates and volunteers who provide services including, but not limited to, support groups/emotional support, crisis counseling, individual counseling, parenting classes, child care, housing support, transportation, legal support, job training, immigration advocacy, and benefit counseling (Lyon, 2008). Shelter programs also work with other community agencies, such as social service and health care providers, law enforcement, education and outreach programs, and housing authorities, to provide on-going support for survivors and their children once they leave the shelter setting (Chanley et al., 2001).
Local community shelters are often the first point of contact between survivors and social, legal, and medical services, and survivors who seek services at shelters often have few resources other than the program itself (Macy et al., 2016; Mengo et al., 2020; Nemeth et al., 2019). Accordingly, shelter staff are regularly tasked with assessing survivors’ needs and designing tailored plans to help them access resources and build independent lives. For some survivors, screening for BI in a shelter may be their only opportunity to be evaluated for BI and their first or only chance to address their symptoms, design safety plans to avoid additional BIs, and receive referrals to specialized rehabilitation services (Goldin et al., 2016; Haag, Sokoloff, et al., 2019; Nemeth et al., 2019). Awareness of BI is crucial for both IPV survivors and individuals who interact with them because post-concussive symptoms can be misinterpreted if considered outside the context of BI. For example, irritability, fatigue, or poor frustration tolerance resulting from BI may be misinterpreted as non-compliance or aggression, and cognitive problems related to decision-making, planning, memory, and problem-solving may cause a survivor to appear disorganized or unreliable (Goldin et al., 2016; Hunnicutt et al., 2017). Given the complex expectations such as meeting a curfew, maintaining employment, and following the rules that many shelters require to receive assistance, misinterpreted symptoms by individuals who work with survivors can result in survivors being deemed problematic for community living and being deprived of needed services. Thus, routine screening for BI in shelters that serve IPV survivors is a common recommendation (Corrigan et al., 2003; Haag, Jones, et al., 2019; Jackson et al., 2002; Monahan & O’Leary, 1999; Murray et al., 2016). Yet, reports indicate that most domestic violence shelter workers feel ill-equipped to screen clients for BI and work for organizations that do not have policies or procedures in place for screening or accommodating clients with BI (Haag, Sokoloff, et al., 2019; Nemeth et al., 2019; Nicol et al., 2021).
The true prevalence of IPV-related BI is unknown, but available evidence suggests that between 35% and 100% of survivors report injuries to the head, face, or neck as a result of physical violence and up to 75% of survivors have a diagnosed or inferred history of TBI (Campbell et al., 2022; Haag, Jones, et al., 2019). Some estimates may underrepresent the prevalence of all IPV-related BIs because they do not include BIs incurred as a result of strangulation or do not consider injuries that were not reported; evidence suggests that only approximately 21–39% of IPV survivors seek medical care for BIs (Monahan, 2018; Smith et al., 2001; Wilbur et al., 2001). Evidence also suggests that survivors may not be aware of the relationship between IPV and BI or may not recognize their symptoms as the characteristics of BI, and therefore, may not disclose a history of injury unless explicitly asked (Haag, Sokoloff, et al., 2019; Murray et al., 2016; Nemeth et al., 2019). Thus, the onus to identify BI among survivors entering shelters is on shelter staff. To effectively work with survivors with BI, shelter staff must have sufficient knowledge about IPV-related BI and screening techniques, believe that they are capable of completing screening and accommodating survivors’ unique needs, effectively make accommodations for the effects of BI, and successfully make referrals to other agencies and providers for specialized and focused BI rehabilitation.
To our knowledge, only three other studies have examined community IPV-provider knowledge, perceived competence, and behaviors related to screening for BI and working with survivors with BI (Haag, Sokoloff, et al., 2019; Nemeth et al., 2019; Nicol et al., 2021). Nicol et al. (2021), Haag, Sokoloff, et al. (2019), and Nemeth et al. (2019) surveyed staff at IPV support agencies, including women's shelters, on their current TBI screening behaviors, knowledge of IPV-related BI, and factors that influence screening. Findings suggest that many IPV providers feel unprepared to identify signs and symptoms of BI and the impact it has on survivors’ ability to access, engage in, and benefit from advocacy services because they have limited knowledge about BI and limited known experience working with survivors with BI (Haag, Sokoloff, et al., 2019; Nemeth et al., 2019). Other providers are adept at identifying symptoms of TBI (e.g., emotional changes, sensitivity to noise and light, etc.) but struggle to differentiate symptoms associated with TBI from symptoms not associated with TBI (e.g., hallucinations, shortness of breath, etc.) (Nicol et al., 2021). Moreover, investigators find that the majority of providers report no previous education or training relative to IPV-related BI (Haag, Sokoloff, et al., 2019) and do not report engaging in routine screening behavior (Nicol et al., 2021). As a result, providers report apprehension to screen due to their lack of experience, perceived inability to do so, and concerns about survivor safety and potential unintended adverse consequences (Nemeth et al., 2019; Nicol et al., 2021). Findings from a scoping review of 42 articles focused on TBI and IPV consolidated recommendations made in response to survey results. Several of the articles reviewed by Haag, Jones, et al. (2019) suggest that because many providers and advocates lack knowledge and skills related to screening, increased training on the identification of BI among survivors, and its effects, is warranted (Haag, Jones, et al., 2019).
The present cross-sectional study aims to contribute to the small, but growing, research base seeking to describe knowledge, perceived competence, and behaviors relative to IPV-related BI among IPV shelter staff. This research was conducted in residential emergency domestic violence shelter programs across a New England state, and data were collected prior to a two-part training series designed to fill gaps in providers’ knowledge and screening practices.
Methods
Study Overview
Data described herein were collected as a pretest assessment for an evaluation of a training program about BI for advocates at domestic violence shelters. Two training modules were developed by BI specialists from the Statewide Head Injury Program at the Massachusetts Rehabilitation Commission and domestic violence specialists at the state Department of Public Health (DPH). The two-part training series was delivered using an online webinar format (Zoom) to 85 staff members from 26 emergency residential domestic violence centers across the state. The questionnaire was administered in conjunction with registration for the webinar. Completion of the questionnaire was voluntary.
Questionnaire Development
A 23-item questionnaire was derived from surveys provided by physicians and research scientists from the University of British Columbia (Paul van Donkelaar, PhD) and the University of Ohio (Julianna Nemeth, PhD) (See Haag, Sokoloff, et al., 2019; Nemeth et al., 2019; Nicol et al., 2021 for discussion of the original survey instruments). Using a Delphi-like process (Adler & Ziglo, 1996), the instrument was further adapted by staff from the Injury Prevention Center at Boston Medical Center (IPC) and injury prevention specialists at the DPH. To ensure content validity, an iterative process was employed that included input from BI specialists at the partnering statewide brain injury rehabilitation commission and injury prevention specialists at the DPH to design and select questionnaire items that were most relevant to this evaluation. Eight stakeholders from the Statewide Head Injury Program at the Massachusetts Rehabilitation Commission and the DPH were asked to rate 39 potential survey questions on a scale of 1–5 (where 1 = not at all important and 5 = extremely important) in terms of how important they believed each question was for inclusion in this questionnaire. An average score was calculated for each question based on the stakeholder feedback. Investigators from the IPC reviewed all questions that were rated 4 out of 5 or higher and included the highest rated questions in each section on the final survey. The final instrument included questions designed to assess: (a) knowledge about BI, (b) attitudes and perceived competence related to advocating for clients with BI, and (c) behaviors regarding screening and working with clients with BI.
The final version of the questionnaire comprised 23 questions, including 3 demographic questions. The questions represented 4 categories: (a) respondent demographics, including role at the domestic violence emergency shelter, (b) knowledge about BI, (c) beliefs and perceived competence relative to screening and accommodating IPV survivors with BI, and (d) BI screening and accommodation behaviors among program staff (see Appendix 1).
Survey Administration
Surveys were conducted using Redcap survey software licensed to researchers at the IPC. The questionnaire was sent to registered participants via email on September 15, 2020, two weeks prior to the delivery of the first training module. It remained open until 1 hour before the first training module began on September 29, 2020.
Data Analysis
Data presented herein are descriptive and were compiled using Microsoft EXCEL. Cronbach's alpha was calculated for true/false, and the Likert scale questions, and was used to assess scale reliability.
Human Subjects
This study was reviewed by the first author's Institutional Review Board and deemed exempt.
Results
Response Rate and Characteristics of Respondents
The questionnaire was sent to 85 registrants, and of these, 75% (64/84) completed it. Participants were asked to identify their role or job title within the domestic violence advocacy organization that they worked for. The majority of participants (59.4%) identified their role as “other.” Participants were not given an option to write-in a response to further explain their role, but all participants worked in roles relevant to the training and survey. Most of the remaining respondents identified themselves as either a shelter advocate (12.5%), a shelter director (9.4%), or a shelter manager (7.8%). Approximately 3.1% of participants identified themselves as a housing advocate or a part-time advocate; and 1.6% of participants identified themselves as a child advocate, an overnight advocate, and relief staff respectively (Table 1).
Demographic Characteristics of Participants (N = 64).
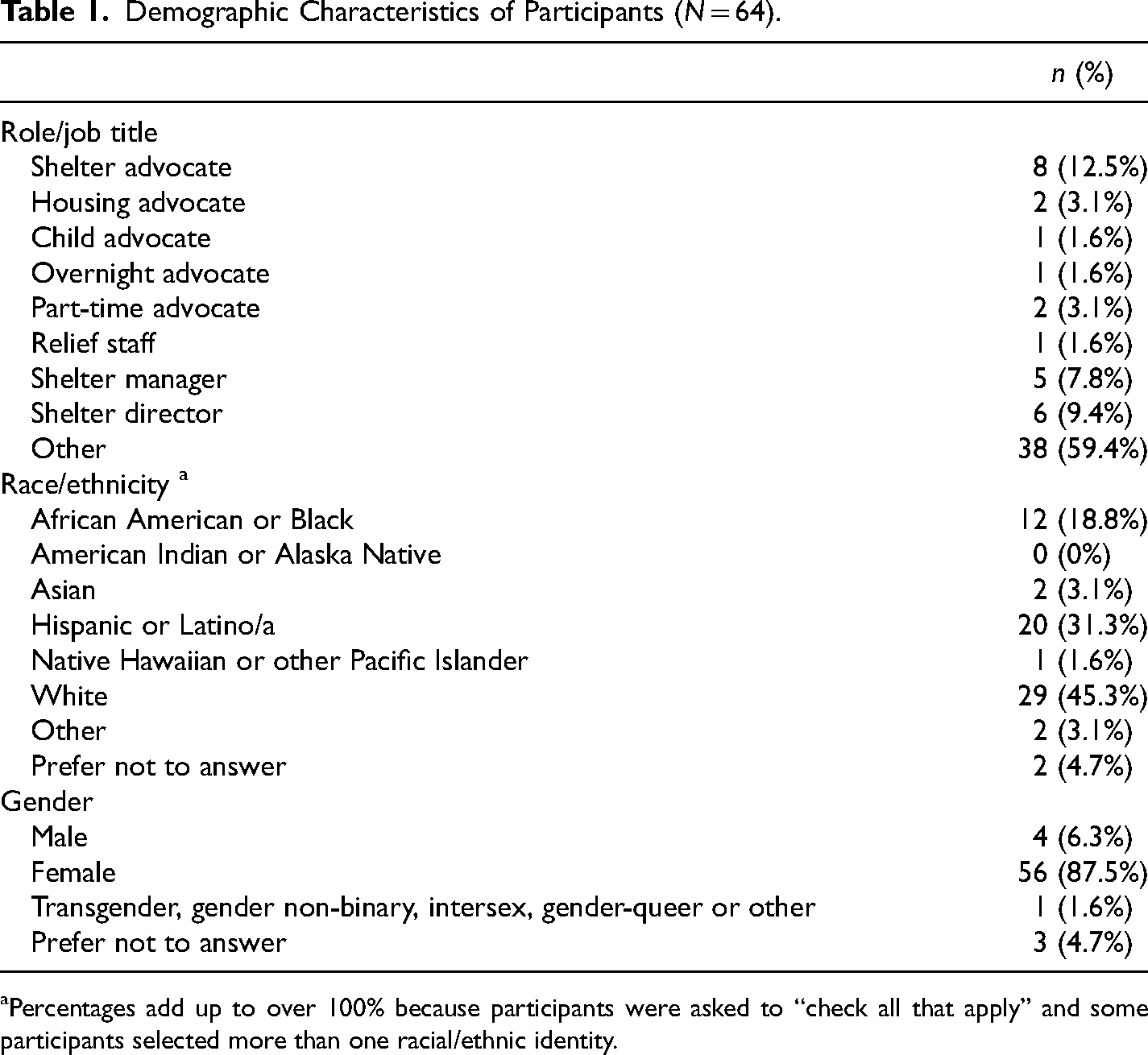
aPercentages add up to over 100% because participants were asked to “check all that apply” and some participants selected more than one racial/ethnic identity.
Participants were asked to identify their race/ethnicity and were permitted to select more than one option. The majority (45.3%) of participants identified their race/ethnicity as White, 31.3% identified as Hispanic or Latino/a, 18.8% identified as African American or Black, 3.1% identified as Asian or other, 1.6% identified as Native Hawaiian or Pacific Islander, and 4.7% of participants declined to answer the question. The majority of participants (87.5%) identified as female; 6.3% identified as male; 1.6% identified as transgender, gender non-binary, intersex, gender queer or other, and 4.7% of participants declined to answer the question (Table 1).
Knowledge About Brain Injury
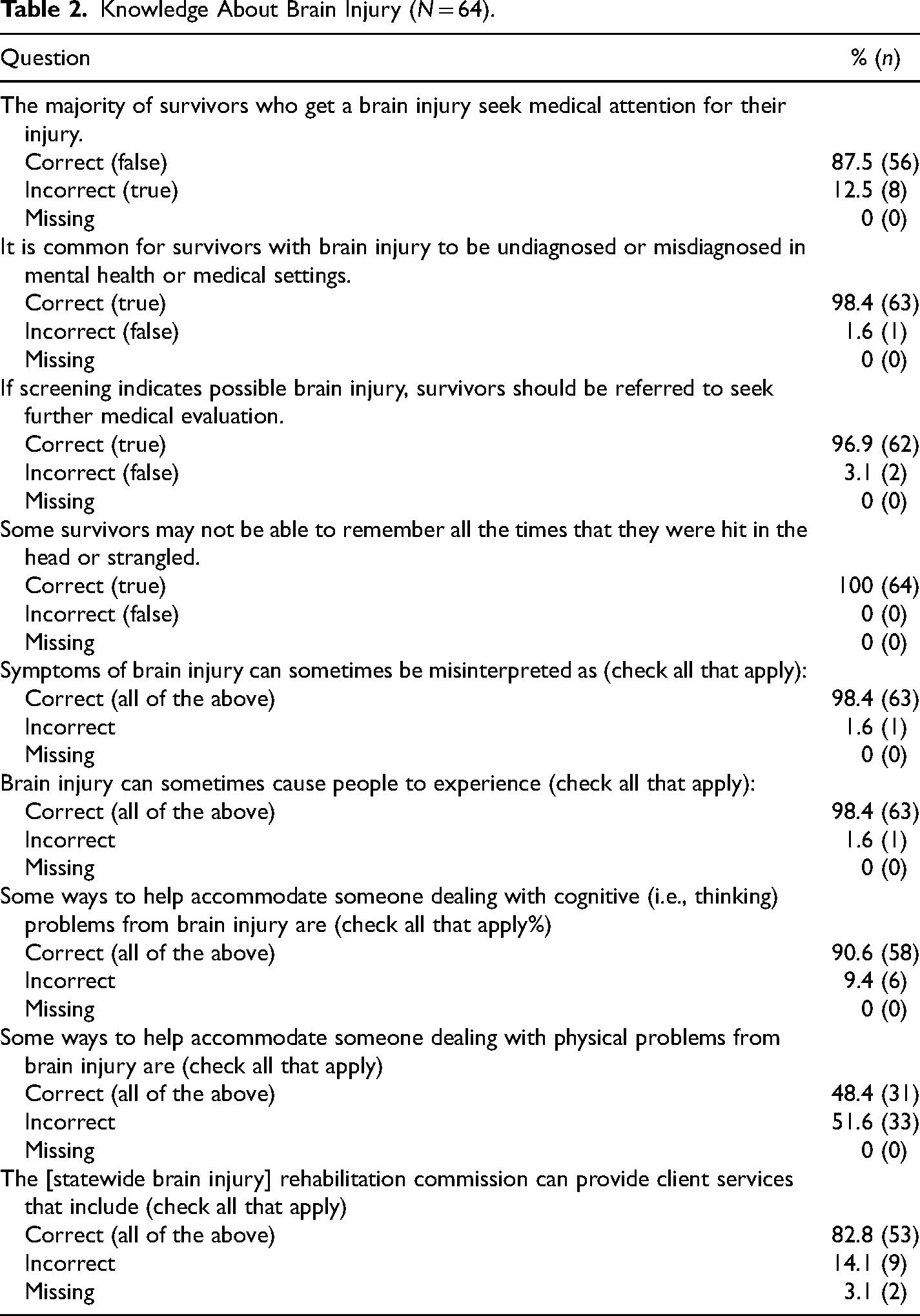
Participants were asked nine questions that assessed their knowledge about IPV-related BI. Of these, four were true/false questions and five were multiple choice questions. Overall, 43.8% of participants answered 100% of the knowledge-based questions correctly, 50% answered between 76% and 99% correctly, 4.7% answered between 51–75% correctly and 1.6% answered less than 25% correctly.
Most participants (87.5%) correctly identified that a majority of survivors who experience a BI do not seek medical care for their injuries. Nearly all participants correctly recognized that if screening indicates, survivors should be referred for medical care (96.9%), and also recognized that it is common for survivors with brain injury to be undiagnosed or misdiagnosed in mental health or medical settings (98.4%). All participants (100%) correctly identified that some survivors may not be able to remember all the times that they were hit in the head or strangled. Nearly all participants (98.4%) were able to identify common symptoms of brain injury and the ways in which symptoms of BI can sometimes be misinterpreted. While 90.6% of participants correctly identified some recommended accommodations for the cognitive effects of BI, only 48.4% correctly identified some recommended accommodations for the physical effects of BI (Table 2).
Knowledge About Brain Injury (N = 64).
Perceived Competence Regarding Working With Brain Injury Survivors
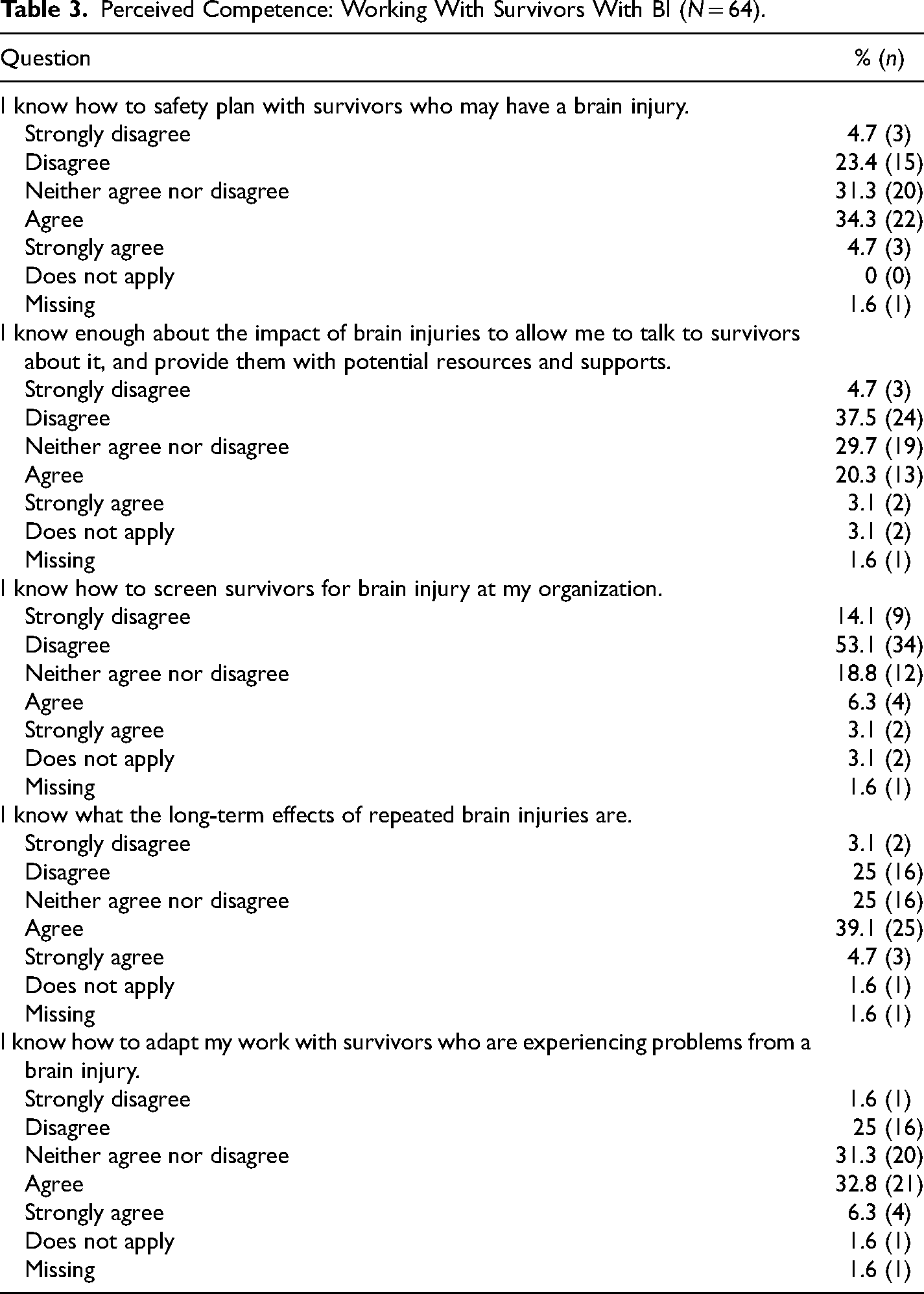
Participants were asked five questions that assessed their confidence or perceived competence regarding screening and working with IPV survivors with BI. All five questions used a 5-point Likert scale (where 1 = strongly disagree, 2 = disagree, 3 = neither agree nor disagree, 4 = agree, and 5 = strongly agree) that asked participants to rate how much they agreed or disagreed with the questionnaire statement. Cronbach's alpha for this set of items was 0.85.
Less than half (39%) of participants strongly agreed or agreed that they know how to safety plan with survivors with possible BI, and about a quarter (23.4%) strongly agreed or agreed that they know enough about the impact of BI to talk with survivors about it and provide survivors with potential resources and supports. Only about 10% of participants reported that they know how to screen survivors for BI, but 39% reported confidence in adapting their work with survivors who are experiencing problems from a BI. Finally, 43.8% of participants agreed or strongly agreed that they know what the long-term effects of repeated BIs are (Table 3).
Perceived Competence: Working With Survivors With BI (N = 64).
Screening and Accommodating Behaviors
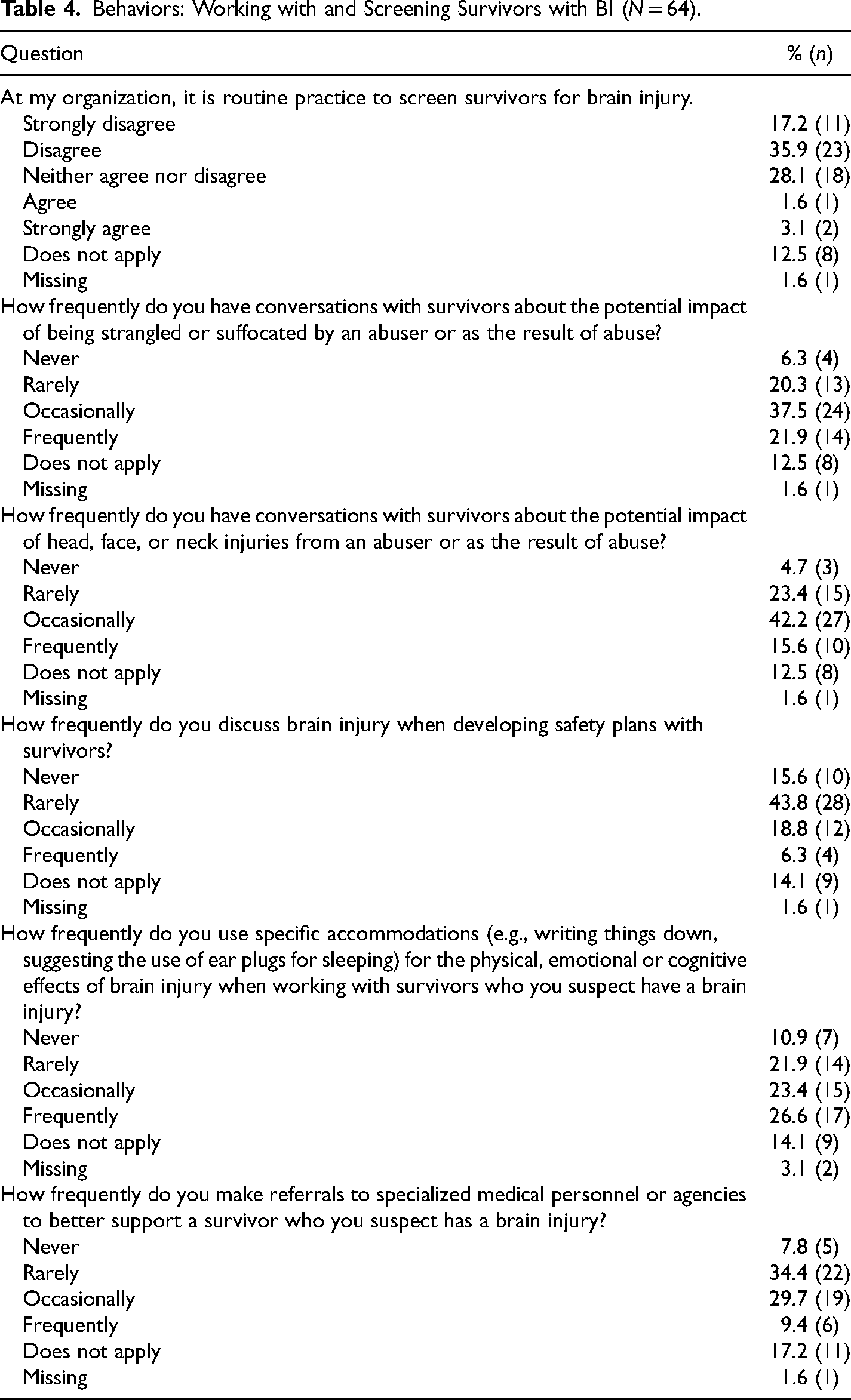
Participants were asked six questions that assessed their behaviors regarding screening and working with IPV survivors with BI. All six questions used a 4-point Likert scale (where 1 = never, 2 = rarely, 3 = occasionally, and 4 = frequently) that asked participants to rate how frequently they performed the stated behavior. Cronbach's alpha for this set of items was 0.78.
Only about 5% of participants indicated that it is routine practice to screen survivors for BI at their organization. Twenty-two percent of participants indicated that they frequently have conversations with survivors about the potential impacts of being strangled or suffocated by an abuser or as the result of abuse, and 37.5% indicated that they occasionally have these conversations. About 16% of participants indicated that they frequently have conversations with survivors about the potential impact of head, face, or neck injuries from an abuser or as the result of abuse, and 42.2% reported occasionally having these conversations. Furthermore, only 6.3% of participants reported frequently discussing BI when developing safety plans with survivors. Regarding making accommodations for survivors with suspected BI, 26.6% reported frequently suggesting specific accommodations for the physical, emotional, or cognitive effects of BI, and 23.4% reported occasionally making accommodations. Finally, 9.4% of participants reported frequently referring survivors with suspected BI to specialized medical personnel or agencies, and 29.7% reported occasionally making these referrals (Table 4).
Behaviors: Working with and Screening Survivors with BI (N = 64).
Discussion
Results of this survey suggest that among a sample of domestic violence shelter staff, knowledge about IPV-related BI was high, but overall perceived competence related to working with and screening IPV survivors for BI was low, and that screening, referral, and accommodation behaviors were infrequent. The majority of participants (94%) answered more than 75% of the knowledge-based questions correctly. This suggests that most domestic violence shelter staff in this sample are aware of the relationship between IPV and BI and have some foundational knowledge about symptoms associated with IPV-related BI and ways to accommodate survivors with BI. However, fewer than 40% of participants indicated knowing how to safety plan with survivors with BI, or how to adapt their work for survivors who are experiencing problems from a BI, and fewer than 25% of participants felt that they know enough about BI to provide survivors with potential resources and supports. Importantly, less than 10% of participants reported knowing how to screen survivors for BI and only about 5% of participants reported that it is routine practice to screen survivors for BI at their organization. While approximately 60% of participants reported frequently or occasionally having conversations with survivors about the potential impact of the head, neck, or face injuries, or strangulation as the result of abuse, only 25% reported frequently or occasionally discussing these injuries when safety planning with survivors, and less than 40% reported frequently or occasionally making referrals to specialized agencies to better support survivors with BI.
Screening and practice recommendations have been made for non-brain injury specialists who work with IPV survivors. These recommendations include learning to identify the symptoms of BI, being aware of IPV-related injuries that could result in a BI (e.g., black eyes and being thrown against a wall), learning how to differentiate the symptoms of BI from other symptom patterns related to substance use or mental illness, modifying assessments and requirements to meet survivors’ needs, administering screening in a conversational way to improve survivor comfort, building relationships with community treatment and rehabilitation services, safety planning to avoid additional BI, taking brain injury impairments into consideration when designing safety plans, and encouraging health-promoting and healing behaviors to the greatest extent possible (e.g., rest and gradual re-entry into normal activities) (Haag, Jones, et al., 2019, Haag, Sokoloff, et al., 2019; Monahan, 2018; Murray et al., 2016; Nicol et al., 2021). Shelters often make accommodations for other types of physical and cognitive disabilities (Lyon, 2008), and shelter staff have reported a willingness and capacity to provide BI-sensitive IPV services if provided with the appropriate education and support to do so (Haag, Sokoloff, et al., 2019). Therefore, it is not unreasonable to suggest that shelters have the capacity to make accommodations for survivors with BI and incorporate screenings into routine intake procedures. Identifying BI may also decrease frustration and burn-out among shelter staff if accommodations for the physical, cognitive, and emotional effects of BI help survivors perform tasks more efficiently and adjust to communal living more easily.
Prior research has investigated barriers to screening behavior among shelter staff working with IPV survivors with mental and/or physical health disabilities. In a state-wide study of community-based domestic violence programs in North Carolina, Chang et al. (2003) found that between 94% and 99% of agencies reported being either “somewhat” or “very” able to effectively provide services to survivors with disabilities. However, when asked about barriers to providing such services, providers cited a lack of funding for staffing, training, and equipment, and structural limitations of program facilities (Chang et al., 2003). Participants recommended networking and cross-collaborations with other community agencies that may be more equipped to provide survivors with the services they need (Chang et al., 2003). Similarly, shelter staff in studies by Nemeth et al. (2019) and Haag, Sokoloff, et al. (2019) reported willingness to provide accommodations and meet survivors with BI and other disabilities “where they’re at” but cite a lack of organizational guidance as a barrier to implementing recommended accommodations (Haag, Sokoloff, et al., 2019; Nemeth et al., 2019). In these studies, providers note that they are either unaware of services that directly address brain injury in their community or that services are limited or inaccessible to survivors in their community (Haag, Sokoloff, et al., 2019; Nemeth et al., 2019; Nicol et al., 2021). Inter-agency networking and cross-referrals have been shown to increase knowledge, self-efficacy, staff satisfaction, and service provision with respect to working with IPV survivors with co-occurring substance use disorders (Stone et al., 2022) and mental health disorders (Mason & O’Rinn, 2014). Thus, it is possible that increasing cross-agency training, networking, and referral procedures between IPV agencies and BI rehabilitation agencies may facilitate increased service provision to survivors with BI (Toccalino et al., 2022). Shelter staff may be more inclined to screen survivors for BI if they are confident that they can provide referrals to survivors with a positive screening result (Nemeth et al., 2019). An effort to facilitate inter-agency collaboration and relationship-building should be emphasized in addition to within-agency training programs. However, training programs are essential to improve shelter providers’ perception of their ability to correctly perform screenings and respond appropriately to survivors who screen positive to BI. Our findings relative to perceived competence are compatible with those reported by Nemeth et al. (2019), Mengo et al. (2020), Nicol et al. (2021) and Haag, Sokoloff, et al. (2019) who suggest that shelter providers understand that many survivors may have BI but do not feel that they have the skills or resources required to provide assistance to survivors or talk with survivors about the implications of their injury (Haag, Sokoloff, et al., 2019; Mengo et al., 2020; Nemeth et al., 2019; Nicol et al., 2021).
It is important that the complex nature and scope of BI is understood within the context of IPV and that screening practices and protocols are designed and implemented to reflect the emotional, behavioral, and social outcomes unique to survivors. For example, survivors with BI who remain in abusive situations face physical, emotional, and psychological conditions that can exacerbate the effects of BI. Furthermore, symptoms of BI can increase the risk of ongoing abuse and repeated BI (Hunnicutt et al., 2017). If appropriate trauma-informed supports and referral protocols are not readily available, screening may have the potential to increase stigmatization against a survivor or lead to increased harm by an abusive partner (Campbell et al., 2018; Nicol et al., 2021). Shelter staff report awareness of these potential harms and cite the potential for re-traumatization as a reason that they are apprehensive to screen (Haag, Sokoloff, et al., 2019). For example, Nemeth et al. (2019) and Haag, Sokoloff, et al. (2019) both found that shelter staff had mixed feelings about actually addressing BI while providing advocacy services because they were worried that being ill-equipped to follow-up with survivors after a positive BI screen could unnecessarily scare a survivor, or negatively impact a survivor if the information were to be used against them (e.g., in court) (Haag, Sokoloff, et al., 2019; Nemeth et al., 2019). Accordingly, it is crucial that provider training programs not only focus on increasing general knowledge about IPV-related BI, but also provide trauma-informed tips, skills, and tools for working with IPV survivors with BI in order to increase provider confidence (Toccalino et al., 2022). According to Bandura's theory of self-efficacy (Bandura, 1977), if providers perceive themselves as capable of successfully screening and working with clients with BI, they may be more likely to engage in screening and referral behaviors. Crucially, training programs should emphasize that screeners are careful not to imply that survivors with a BI are “damaged,” “incompetent” or unable to function. Such messages can increase stigma and a sense of learned helplessness (Murray et al., 2016), which directly contradicts the empowerment model upon which many shelter-service philosophies are built.
It is important to utilize standardized and validated instrumentation for screening in order to accurately identify BI and to obtain precise estimates of the prevalence of BI within emergency shelters. A significant challenge to screening in this population is that no standardized, validated TBI screening tool sensitive to the unique needs of the IPV context currently exists (Campbell et al., 2022). In an effort to make a recommendation for standardization, Goldin et al. (2016) conducted a literature review to identify TBI screening instruments that are compatible with the World Health Organization's (WHO) criteria for interviewing IPV survivors. These criteria include safety, privacy, confidentiality, and adequately trained interviewers (Goldin et al., 2016). Researchers identified nine tools that most closely met the WHO criteria and identified the Ohio State University TBI Identification Method (OSU-TBI-ID) as one of the two tools that has the high potential for detecting TBI within IPV survivor populations whilst adhering to the WHO recommendations (Goldin et al., 2016). The OSU-TBI-ID has been found to be reliable and shows high predictive validity (Corrigan & Bogner, 2007) and was recommended to participants in this study by experts from the statewide brain injury rehabilitation commission that we partnered with. The OSU-TBI-ID is designed to identify both traumatic and anoxic-hypoxic BIs and has been validated for use among different populations (Bogner & Corrigan, 2009; Corrigan & Bogner, 2007; Corrigan et al., 2012). There are no educational training or licensure requirements needed to administer the screening. Accordingly, it is appropriate for use by staff in shelter settings, provided it is adapted to fit the safety criteria recommended for use with IPV survivors (Goldin et al., 2016). Screening using the OSU-TBI-ID takes approximately 10 to 20 minutes, depending on the interviewee's processing speed, and can be administered anytime during a survivors’ shelter stay. Ideally, screening would be administered at intake so that accommodations and referrals can be made expediently; however it can be administered once a survivor is settled in shelter and feels comfortable, or anytime the staff notice symptoms or behaviors that may be explained by a BI.
Limitations and Future Directions
There are several study limitations of note. First, the respondents for this research represent a convenience sample rather that a random sample of all statewide domestic violence shelter staff. Shelter staff who signed up to participate in a training program about BI may be different from those who chose not to register for the training program; thus some selection bias may have influenced results. Second, our study population was limited to one state in New England and therefore may not represent domestic violence shelter staff in other states. Third, because the majority of participants did not indicate their role within their agency, it is not clear that everyone who participated in the survey works directly with survivors. Administrative staff or other non-direct service staff who completed the survey, but who do not interact with survivors on a daily basis, may have answered that they rarely or never perform certain screening or accommodation behaviors (as opposed to indicating that the statement did not apply to them) because such behaviors are outside the scope of their role. Nevertheless, given that all participants working at a domestic violence shelter have an impact on shelter practices and culture, their responses are valid and relevant regardless of their specific role. For example, administrator's knowledge and skills are critical with respect to revising agency-wide screening policies and procedures, and gathering and providing information for direct service workers regarding referral agencies and available resources. Fourth, portions of the data collection questionnaire did not undergo psychometric testing. And, fifth, as with most surveys, respondents may distort their answers to conform with perceptions of social desirability.
Further research is needed to investigate the ways in which IPV-related BI intersects with race, housing, income, mental health, access to healthcare, and gender identity. For example, in a national survey on IPV and sexual violence, 45.1% of non-Hispanic Black women, compared to 37.3% of non-Hispanic White women, 34.4% of Hispanic women, and 18.3% of Asian and Pacific Island women, reported IPV in their lifetime (Smith et al., 2018). While data suggest the likelihood of racial and ethnic disparities in the incidence of IPV-related BI, more research is needed to support this hypothesis. At least one study has identified systemic racism as a barrier to identification of, and support for, IPV-related BI for racialized women exposed to IPV-BI (Toccalino et al., 2022). Thus, training programs should consider the implications of inequities related to race, and the intersection of IPV-related BI with other social determinants of health. Because IPV survivors who seek emergency shelter often have numerous and complex needs, it is possible that there are disparities with respect to risk factors and health outcomes among survivors with BI in shelters compared to survivors with BI who do not require emergency housing and assistance. Future research should aim to identify survivors who have a heightened risk of experiencing IPV-related BI, and whether survivors with BI who do not seek emergency shelter are accessing medical care and resources for BI more or less often than the survivors that utilize emergency shelter services.
Conclusions
In this cross-sectional study, we examined knowledge, perceived competence, and behaviors relative to IPV-related BI among domestic violence emergency shelter providers in a New England state. The data suggest that the shelter providers in this sample have some knowledge about IPV-related BI, but lack confidence related to providing screening, accommodations, and specialized referrals to survivors with BI. These findings extend knowledge in the field by suggesting that perceived competence may be an important predictor of screening behaviors such that low perceived competence predicts infrequent screening, accommodation and referral behaviors. Given the high prevalence of BI among IPV survivor populations, and the damaging short and long-term impacts that BI can have on survivors’ daily functioning and ability to lead independent lives, shelter agencies that serve IPV survivors should facilitate IPV-related BI trainings for their staff and prioritize developing and implementing BI screening, accommodation, and referral policies and standard operating procedures.
Supplemental Material
sj-docx-1-vaw-10.1177_10778012231163577 - Supplemental material for Knowledge, Perceived Competence, and Behaviors Relative to Traumatic Brain Injury Among a Sample of Domestic Violence Emergency Shelter Advocates in a New England State
Supplemental material, sj-docx-1-vaw-10.1177_10778012231163577 for Knowledge, Perceived Competence, and Behaviors Relative to Traumatic Brain Injury Among a Sample of Domestic Violence Emergency Shelter Advocates in a New England State by Julia K. Campbell, Jonathan Howland, Brie Insalaco and Gabriela Lawrence-Soto in Violence Against Women
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Centers for Disease Control and Prevention (CDC) (grant number NU17CE924835)
Supplemental Material
Supplemental material for this article is available online.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.