
Abstract
Rape survivors face stigma when disclosing their experiences. We hypothesized that a rape survivor who formally reports their rape would experience more stigma than one who does not, and that this effect will be stronger when the perceiver is a man or low in support for sexual consent. Across two studies using self-report, observational, and psychophysiological measures, we found that a reporting survivor was seen more negatively than an identical survivor who did not report their rape. Men and those low in support for sexual consent also responded more negatively to the survivor. Implications of these findings are discussed.
Keywords
Sexual violence survivors face stigma that can harm their health (Kennedy & Prock, 2018; Ullman & Peter-Hagene, 2014). This stigma stems from cultural rape myths that delegitimize survivors’ experiences (e.g., myths that “it's not real rape if she didn’t fight back” and “women secretly enjoy being raped”; Edwards et al., 2011; Payne et al., 1999). Stigma may be worse for those whose experiences do not fit stereotypic rape scripts about stranger rape (McKimmie et al., 2014). The stigma survivors face also depends on to whom they disclose and how they describe their experience. Men have more negative reactions to rape disclosures (Edwards et al., 2022; Iles et al., 2021), and varying definitions of sexual consent can also impact perceptions of what counts as a “real” rape (Glace et al., 2021; Muehlenhard et al., 2016). Survivors may also face more stigma when they call their experiences non-consensual and/or make a formal report against the perpetrator versus when they do not. We investigate factors that influence survivor stigma, including two factors related to the disclosure recipient—gender and consent attitudes—and one factor related to the disclosure itself—how the survivor characterized and responded to their experiences. To investigate both overt and subtle stigma, we employ self-report, behavioral, and cardiovascular (CV) markers of stigma.
Survivor Stigma
Survivors who face negative or stigmatizing responses have poorer mental and physical health outcomes (Dworkin et al., 2019; Orchowski et al., 2013; Ullman & Peter-Hagene, 2014). These stigmatizing responses also decrease future help-seeking and increase a survivor's risk of revictimization (Kennedy & Prock, 2018). Conversely, positive responses to survivors’ disclosures can support survivors’ health and recovery (Ullman & Peter-Hagene, 2014). Both formal sources of support (e.g., law enforcement, healthcare workers, etc.) and informal sources of support (e.g., friends, family, etc.) can stigmatize survivors by expressing rape myths—harmful beliefs which minimize the incidence and severity of sexual violence and promote victim-blame (Kennedy & Prock, 2018; Orchowski et al., 2013; Ullman & Peter-Hagene, 2014). Survivors often internalize this stigma and blame themselves for their victimization (Kennedy & Prock, 2018). This stigma is related to system justification (Chapleau & Oswald, 2014; Iles et al., 2021) and ambivalent sexism (Koepke et al., 2014; Persson et al., 2018).
System Justification and Survivor Stigma
System justification theory (Jost et al., 2004) states that people are motivated to defend their current social system, including perceiving existing power hierarchies as just. Per this worldview, men's sexual violence against women must be deserved, as this type of oppressive violence would not happen to undeserving people in a just social system (Chapleau & Oswald, 2014). Ergo, sexual violence survivors are stigmatized as though they deserved or caused their own victimization—ideas that are also rape myths (Edwards et al., 2011).
Ambivalent Sexism and Survivor Stigma
Ambivalent sexism theory (Glick & Fiske, 1996) describes two distinct facets of sexism, including benevolent and hostile sexism. Benevolent sexism includes beliefs that women are special, pure, and must be cherished and protected; conversely, hostile sexist beliefs espouse overt hatred of women and justify violence against women (Glick & Fiske, 1996). Women who conform to patriarchal roles (e.g., chaste wives, devoted mothers, etc.) are rewarded with benevolent, albeit patronizing, treatment, while women who do not conform to these roles (e.g., sex workers, career women, etc.) are met with hostility (Glick & Fiske, 1996). Based on these beliefs, women survivors whose behaviors at the time of their victimization do not conform to patriarchal roles (e.g., behaving in a sexual manner) are met with victim-blame (Koepke et al., 2014).
System Justification Versus Ambivalent Sexism
While system justification and ambivalent sexism suggest similarly stigmatizing responses to survivors in some aspects (e.g., “survivors deserved their victimization”; Chapleau & Oswald, 2014; Koepke et al., 2014), there is a key difference between these models. System justification theory states that those who are most harmed by the system are just as likely—if not more likely—to justify it (Jost et al., 2004), making women and gender minority people as or more likely than cisgender men to derogate survivors in a system justification framework. However, men are known to be higher than women in hostile sexism (Glick & Fiske, 1996), making men more likely to derogate survivors in an ambivalent sexism framework.
Framing “Real” Rape and Stigma
Narratives regarding what constitutes a “real” rape can be further used to stigmatize survivors. The stereotypic rape is a stranger rape involving physical force or a weapon and no use of drugs or alcohol by the survivor (Kahn et al., 1994). Stranger rapes via physical force do occur, but acquaintance/date rapes using drugs and/or alcohol as methods of coercion are more common (Abbey et al., 2001; Brooks-Hay et al., 2018). Survivors are seen less positively when their victimization experiences do not match stereotypic rape scripts (Stuart et al., 2019). These scripts often reflect and are reinforced by cultural rape myths about which rapes are “real” (e.g., “real rapes must involve visible physical injuries”; Payne et al., 1999).
Social norms encourage men to see sex as a conquest in which the use of coercion is an acceptable tactic to obtain sexual access to a woman's body (Jozkowski et al., 2017). Women may also adhere to these views and feel that being pressured to have sex they do not want is a normal part of being in a relationship (Bay-Cheng & Eliseo-Arras, 2008). Some individuals justify instances of coerced sex based on the way the survivor resisted the assault. Most consent communication is indirect and nonverbal, but cultural narratives suggest that consent refusal that follows these norms is not enough to be called a “real” rape (O’Byrne et al., 2008). Individuals are less likely to perceive a perpetrator as guilty when the survivor did not use direct physical resistance than when the survivor did use such resistance (McKimmie et al., 2014).
These norms about what counts as “real” rape mean that survivors whose experiences do not fit these narratives are stigmatized more than survivors with more stereotypic experiences (McKimmie et al., 2014). Additional rape myths that uphold this script (i.e., women who drink alcohol caused their rape, women are not raped by their boyfriends, real rape must involve physical resistance; Payne et al., 1999) are especially stigmatizing for survivors whose experiences included alcohol, an existing relationship with the perpetrator, and nonverbal resistance (Humphreys, 2007; McKimmie et al., 2014). No survivor is responsible for their own victimization or the stigma they face. This research suggests that the way survivors frame their victimization when disclosing their experiences may impact the stigma they face. Survivors with less stereotypic experiences might be judged particularly harshly for labeling an experience as sexual violence and/or seeking accountability from the perpetrator by making a formal report of a rape that might not be seen as “real.” We investigate this by experimentally manipulating how a fictional survivor of less stereotypic sexual violence labels and responds to her experiences.
Gender
Men, more so than women, are high in rape-supportive attitudes, likely to identify with perpetrators rather than survivors, and have more negative reactions to disclosures of sexual victimization (Edwards et al., 2022; Emmers-Sommer, 2014; Iles et al., 2021). This contradicts a system justification perspective on sexual violence, which suggests that women, who are harmed more by the status quo, would be as or more likely to hold system-justifying beliefs and denigrate survivors than men (Jost et al., 2004). It is more consistent with an ambivalent sexist model of survivor stigma, as men are more likely than women to hold sexist beliefs (Glick & Fiske, 1996), which could lead men to exhibit more stigmatizing responses to sexual violence survivors. In this work, we also investigate disclosure recipient gender as a predictor of stigma toward sexual violence survivors.
The existing research in this area is based on mostly cisgender samples, leaving the attitudes and perspectives of trans people (i.e., transgender women/girls and transgender men/boys) and nonbinary people (e.g., agender, genderfluid, genderqueer, or Two Spirit individuals and others outside the gender binary, etc.) largely unexamined. To the authors’ knowledge, the rape myth acceptance, rape scripts, and disclosure responses of gender minority people have yet to be empirically examined. However, some research studies have indicated that nonbinary people and gender and sexual minority people overall may hold more favorable attitudes about sexual consent compared to their cisgender heterosexual peers (Glace & Kaufman, 2020; McKenna et al., 2021). Additionally, gender minority people face higher risks of sexual victimization than cisgender people (Stotzer, 2009).
Because gender minority people hold more favorable attitudes about sexual consent than their cisgender peers (Glace & Kaufman, 2020; McKenna et al., 2021) and face higher risks of victimization than cisgender people (Stotzer, 2009), nonbinary people are categorized with women for the purposes of this research. Our gender variable had two categories: men; and women and nonbinary people. Transgender men were grouped with cisgender men and transgender women were grouped with cisgender women.
Consent Attitudes
As discussed, survivor stigma is likely to vary based on what is seen as “real” rape. As the dividing line between sex and rape (Muehlenhard et al., 2016), an individual's attitudes about sexual consent play a role in labeling a “real” rape, and therefore in survivor stigma. The definition of sexual consent is not straightforward and individuals hold varying ideas regarding what constitutes acceptable consent to sex (Glace et al., 2021; Muehlenhard et al., 2016). Individuals lower in support for sexual consent (i.e., indicating attitudes and behaviors that place lower value on ongoing consent negotiations with one's sexual partner(s); Glace et al., 2021) may be less likely to see disclosures as “real” rape, and thus may have more stigmatizing reactions to sexual violence survivors. Consent attitudes are also investigated as a predictor of survivor stigmatization.
Subtle Stigma
Individuals are unlikely to explicitly report victim-blaming sexual violence survivors due to social desirability effects (Thelan & Meadows, 2022). Yet, most survivors still report at least some negative social reactions to their disclosures (Ullman & Peter-Hagene, 2014). This suggests implicit or unreported bias on the part of many disclosure recipients. Despite being less obvious, there are some cases where subtle bias is more harmful than overt bias (Walker et al., 2021). This may be because, while overt discrimination is easy to identify, subtle discrimination is more ambiguous, meaning that interpreting and responding to this discrimination requires more cognitive resources and is more stressful for the stigmatized individual (Walker et al., 2021). Further research suggests that subtle discrimination is at least as harmful as overt discrimination (Jones et al., 2016). Stigmatized individuals may even prefer interacting with explicitly (vs. implicitly) biased doctors (Penner et al., 2010).
Stigma Measurement
Survivor stigma might be becoming more subtle. Scores on the Illinois Rape Myth Acceptance Scale have declined over time, but rape myth acceptance is still observable using more subtle measurement techniques (Thelan & Meadows, 2022). This indicates that the cause is not that rape myth acceptance is becoming less common, just more impacted by social desirability and difficult to measure. Original rape myth acceptance scales were developed decades ago (Burt, 1980) and use language that is inaccessible to youth and emerging adults today. Alternative measures of stigma directed towards sexual violence survivors are needed.
Biopsychosocial Model of Challenge and Threat
Per the Biopsychosocial Model of Challenge and Threat, patterns of CV reactivity can index psychological states under certain circumstances (Blascovich, 2008). Challenge states occur when an individual feels they have the resources to meet the demands of a situation and are characterized by an efficient and adaptive CV profile (i.e., increases in cardiac output and decreases in total peripheral resistance). In contrast, threat states occur when individuals feel that they have insufficient resources to meet the demands of a situation, and are characterized by a less efficient CV profile that can have health consequences over time (i.e., little changes in cardiac output and increases in total peripheral resistance; Blascovich, 2008).
Classic work has identified CV challenge/threat as a way of indexing stigma processes (see Blascovich et al., 2000). For example, Blascovich et al. (2001) found higher levels of CV threat among participants interacting with a confederate with (vs. without) a facial birthmark and that past interracial contact reduced threat responses among White participants interacting with a Black confederate. Therefore, CV threat might be used to index the level of stigma-related discomfort, anxiety, and avoidance a perceiver experiences when interacting with a target individual.
Interpersonal Cues
Individuals’ nonverbal communication (e.g., body language) can indicate stigma they might feel towards an interaction partner (Kleck, 1968). Confederate-observed interpersonal warmth has been used to measure subtle bias in field studies of homophobic discrimination (Hebl et al., 2002). Self-reported warmth towards ethnic minority individuals is associated with the stigma a person feels towards that same group (Cheung et al., 2022). So, in this research, we use changes in the warmth with which a disclosure recipient treats a survivor from before to after a disclosure of sexual victimization as an indicator of the stigma that they feel towards the survivor related to their victimization.
Present Research
We examined participants’ responses to a fictional sexual violence survivor using self-report, psychophysiological, and observational measures. We also examined whether these responses would vary by the participant's gender, the participant's attitudes about sexual consent, and the ostensible survivor's reaction to their victimization (i.e., stating they did not consent to sex, filing a formal report against the perpetrator, or doing neither).
Hypotheses
We operationalized stigma in Study 1 using self-reported liking, blame, and warmth toward survivor and perpetrator. In Study 2, we operationalized stigma more subtly using CV threat reactivity and interpersonal warmth. We hypothesized that:
Study 1 Method
Participants
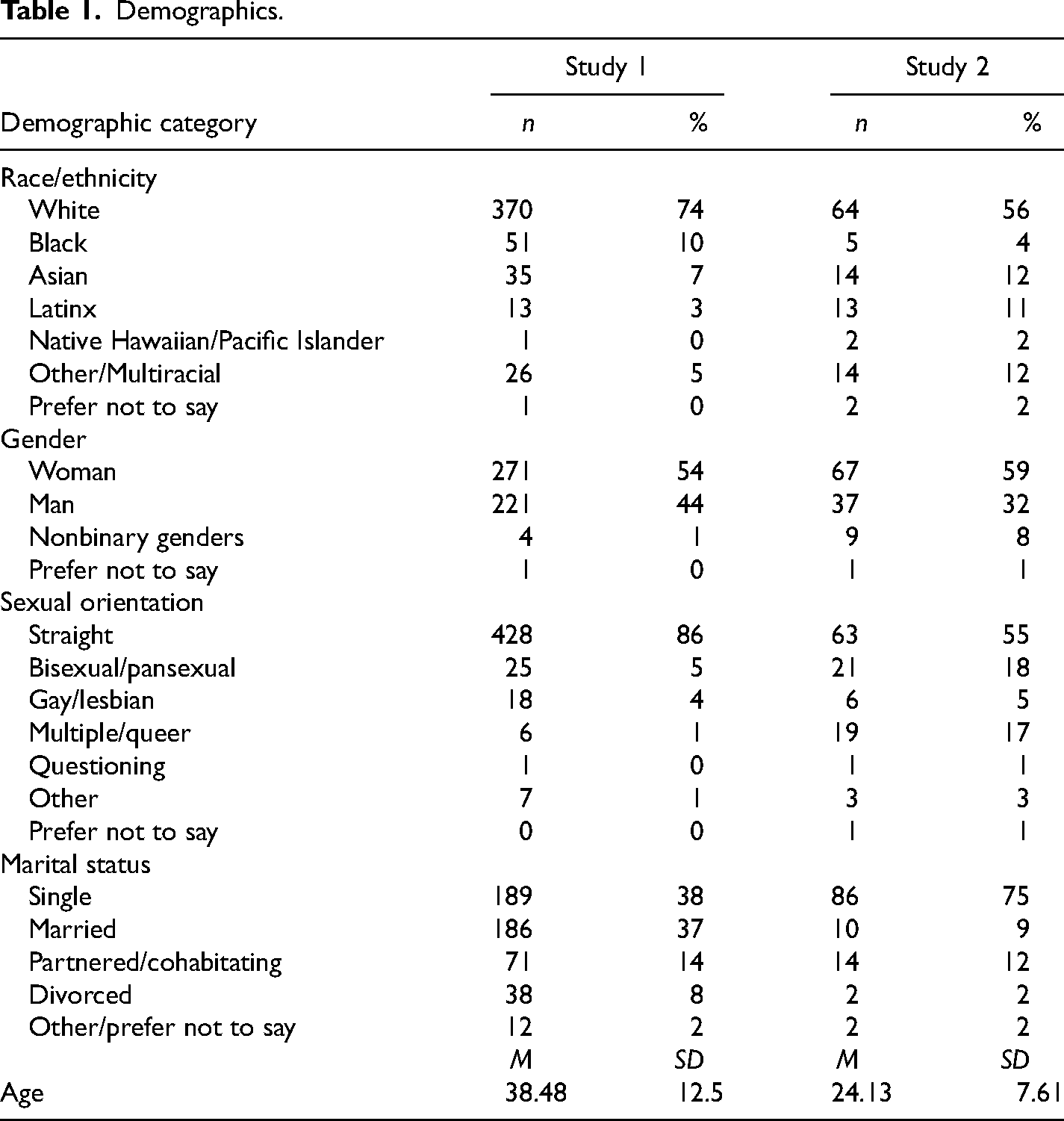
We surveyed a sample of adults on MTurk. The sample included 498 participants after excluding those who failed an attention check and listwise deletion was used to address missingness. Most participants were White and women. Demographics are shown in Table 1.
Demographics.
Procedures, Materials, and Measures
Participants were recruited on MTurk and directed into our survey. They were randomly assigned to read one of the study vignettes, which they were told was about a female college student, and then completed the measures of survivor liking, blame, and warmth, in addition to an attention check, the Process-Based Consent Scale (PBCS), and demographic items.
Study vignettes
Participants read one of the six study vignettes. All described the same alcohol mediated acquaintance rape written in the first person, as shown in Table 2. Vignettes were identical except for the end, in which the author dismisses the rape in one of three ways (control conditions), says she did not give consent to sex (no-consent condition), or files a formal report, worded one of two ways (reporting conditions). The control conditions and reporting conditions did not differ significantly within each condition on any outcome variable and so were combined for analyses, leaving three experimental conditions (i.e., control, no-consent, and reporting).
Study Vignettes.
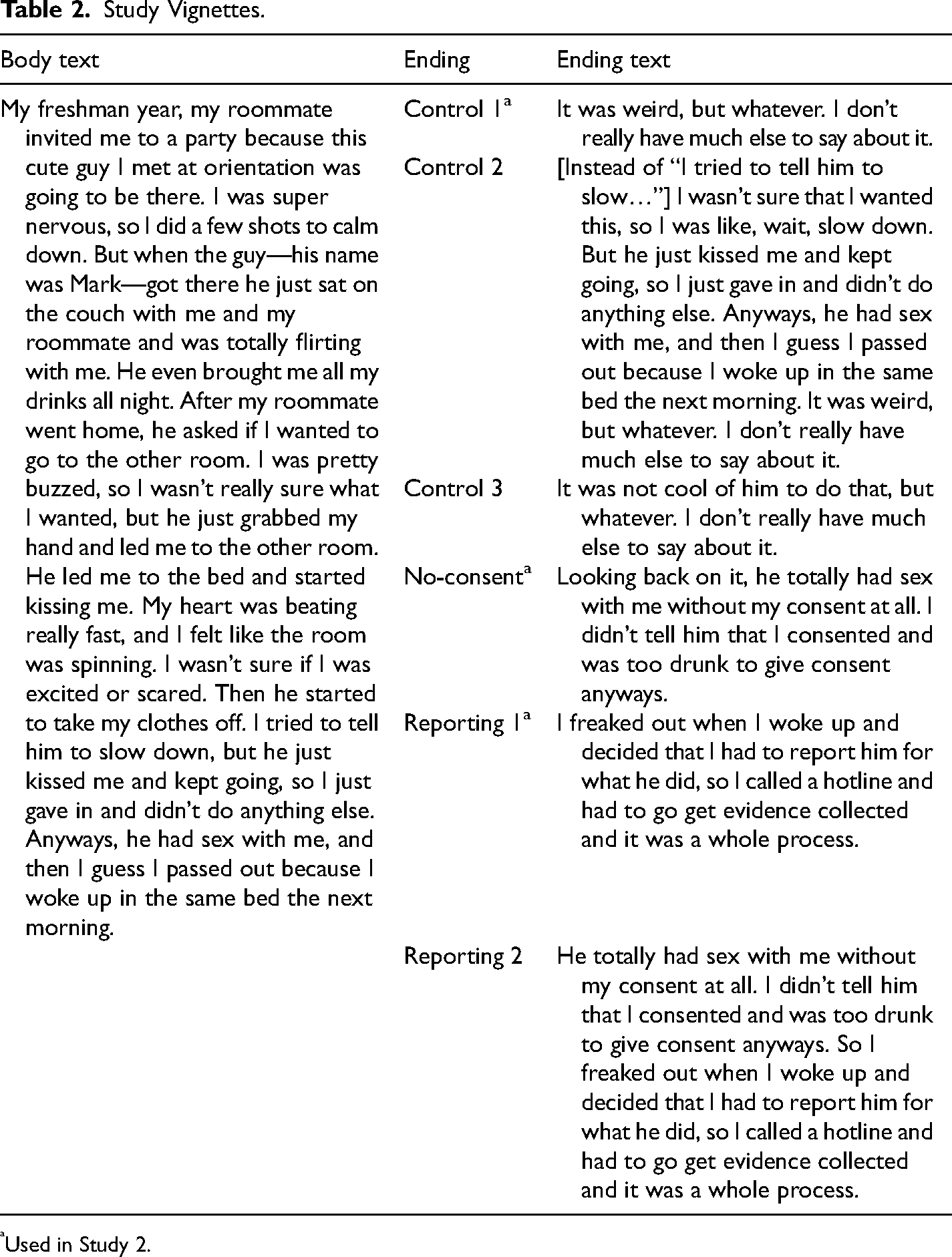
Used in Study 2.
Demographics
Items included age, race, gender, marital status, and sexual orientation. Gender was measured using a multiple-choice (select all that apply) item with options: man, woman, nonbinary, genderqueer, genderfluid, prefer not to say, and a write-in option. Participants were asked if they were transgender in a separate item. Only the initial item was used to calculate the gender variable, as transgender participants were included with cisgender participants of their same gender. Participants who selected man were placed in the “man” category regardless of transgender status and all others were placed in the “women and nonbinary people” category.
Process-based consent scale
Study 1 used a version of the PBCS; (Glace et al., 2021). This scale measures attitudes about sexual consent. It is a Likert-type scale, with options from 1 (strongly disagree) to 7 (strongly agree). Two subscales were included in the survey, including ongoing consent (e.g., “If my partner seems less than excited about sex, I will stop and ask if they want to be sexual with me”) and subtle coercion (e.g., “Sometimes, people need a little verbal convincing to have sex”). Subtle coercion items were reverse-coded and all items were averaged into one variable that had good reliability (α = 0.88). The original development of this scale confirmed a bifactor structure (Glace et al., 2021), supporting its use as a single variable or as subscales. A single variable was used for the sake of model parsimony.
Survivor liking
Several items were used to measure participants’ opinions of the survivor in the vignette that they read, including an item about their likelihood of being friends with the survivor, how much they would like the survivor in real life, the quality of the survivor's decision-making, the survivor's trustworthiness, and the extent to which the participant identified with the survivor. These items were highly related and formed a composite scale with good reliability (α = 0.87). As such, they were analyzed as a single variable.
Blame
Participants indicated how much blame they would assign to the perpetrator the survivor on separate scales of 0 to 100. Victim- and perpetrator-blame were separate variables. The sliding scales were not confined to adding up to 100%. Even if participants assumed that was the case, they were also asked to assign blame to a third character in the story (a bystander), so that victim-blame and perpetrator-blame were not two poles of the same continuum.
Warmth
As with blame, participants were asked to indicate how much warmth they felt towards the perpetrator and the survivor on separate scales of 0 to 100. These were separate variables for the same reasons as the blame variables and were not asked in terms of percentages.
Analysis Plan
We intended to examine consent attitudes and gender as moderators of the relationship between condition and perceptions of the survivor. We placed the PBCS after the manipulation to avoid priming participants’ expectations about the vignette. However, consent attitudes differed by condition. This was unanticipated, as the PBCS measures general consent attitudes unrelated to the vignette. As the conditions were randomly assigned, it is unlikely that these differences existed in theoretically consistent directions prior to the experimental manipulation. Thus, we tested the PBCS as an outcome. In Study 2, we moved PCBS measurement to before the experimental manipulation to test the originally hypothesized moderation.
We conducted an omnibus two-way MANOVA testing group differences in the outcome variables (i.e., survivor liking, PBCS, perpetrator-blame, victim-blame, perpetrator-warmth, and victim-warmth) based on condition, gender, and the interaction between the two. Following a significant omnibus test, we conducted follow-up ANOVAs for each outcome variable and tested pairwise comparisons using a Tukey test.
Study 1 Results
In the omnibus MANOVA, differences by condition were significant (Pillai's Trace = 0.05, f(12,896) = 2.05, p = .02), but differences by gender (Pillai's Trace = 0.02, f(6,447) = 1.84, p = .09) and the interaction term (Pillai's Trace = 0.02, f(12,896) = 0.86, p = .59) were not. The results of pairwise comparisons by condition are shown in Table 3. In the reporting condition (vs. no-consent condition), participants reported less liking of the survivor and more warmth towards the perpetrator. In the reporting condition (vs. no-consent and control conditions), participants reported lower support for sexual consent and less warmth towards the survivor. There were no significant differences between the control and no-consent conditions.
Study 1 Results.
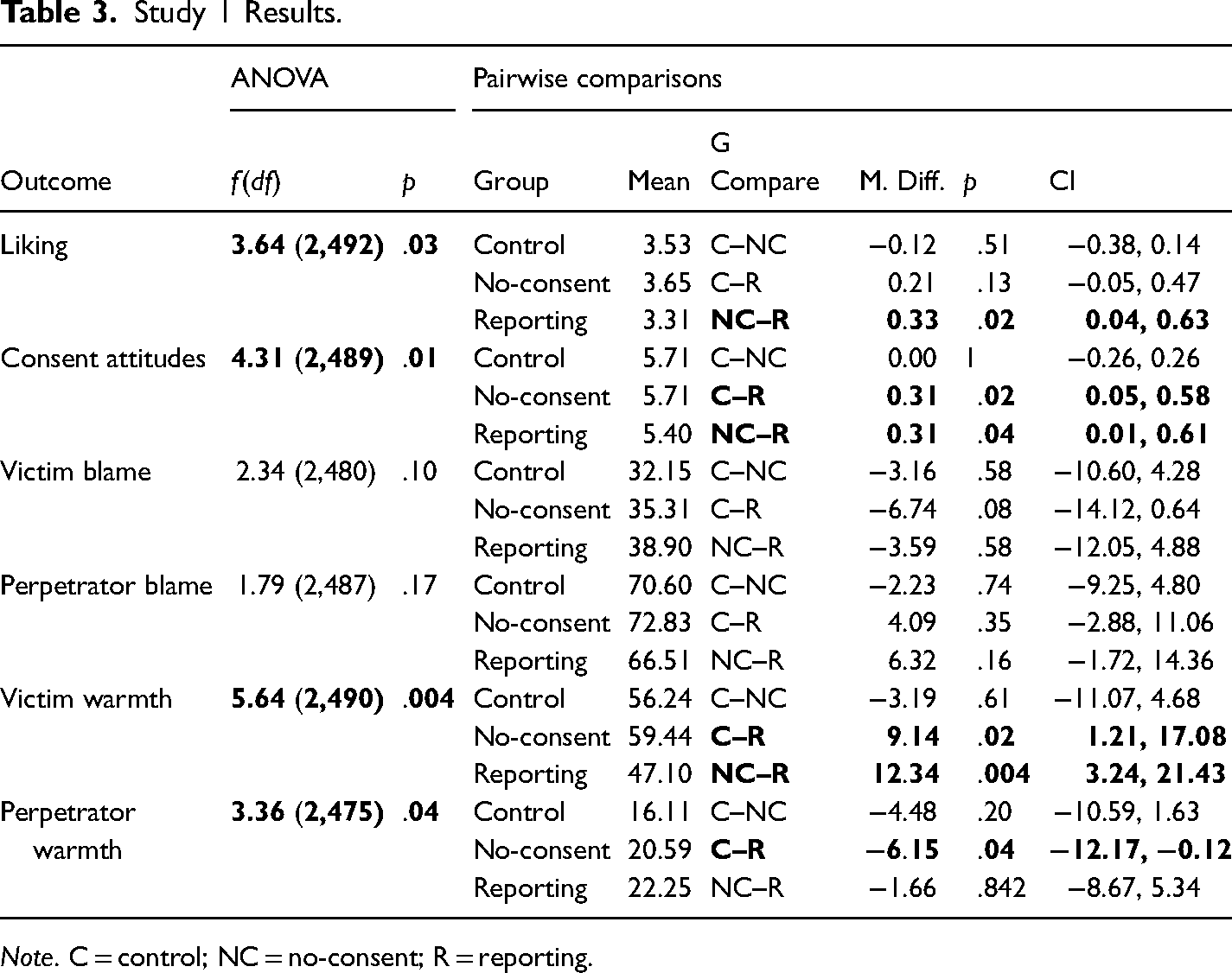
Note. C = control; NC = no-consent; R = reporting.
Study 1 Discussion
Participants had more negative responses to survivors who reported their victimization than survivors who said they did not consent or survivors who had no response to the situation, providing partial support for hypothesis 1. Because the study vignette depicted a statistically common rape as opposed to a stereotypic rape, participants may have been hesitant to label the offense a “real” rape (Kahn et al., 1994; McKimmie et al., 2014), and as such, reacted more harshly to the survivor. The effect was observed with self-report measures, suggesting that the stigmatization of survivors who seek justice is expressed overtly. Participants in the reporting condition also reported more warmth for the perpetrator; the idea that a perpetrator might be punished may lead perceivers to evaluate them against a different standard and thus less harshly.
Survivors who used consent language but did not report were not perceived differently than survivors in the control condition. In several instances (i.e., liking and warmth), survivors who used consent language were seen significantly more positively than survivors in the reporting condition when survivors in the control condition were not. Negative responses to the reporting survivor might be borne of system justification motives and consent language may not pose the same threat to the system. Alternatively, not filing a report, and therefore not claiming to have experienced “real” rape, may not prompt the same hostile sexist responses as choosing to seek accountability from the perpetrator. It is also possible that individuals’ reactions to sexual violence survivors who use consent language occur on an implicit level. In Study 2, we use non-self-report measures to examine responses to survivors who use consent language.
We planned to test consent attitudes as a moderator, but we instead found that the measure differed by condition. Specifically, in the reporting condition (vs. no-consent and control conditions), participants reported lower general support for sexual consent, unrelated to the vignette. Participants may have attempted to justify their negative reactions to the survivor by modifying their own beliefs to be more permissive of sexually coercive behavior.
Strengths and Limitations
Study 1 used random assignment in a sample of nearly 500 participants. Its experimental design is a strength, but it was a cross-sectional online survey in a homogeneous (i.e., mostly White and heterosexual) population. As such, experimental control was limited, and these findings may not generalize. We analyzed the data based on the interpretation that differences in consent attitudes between experimental conditions were not pre-existing due to random assignment. But, if these differences were genuinely pre-existing, some of the effects we attributed to the experimental conditions may have been more related to participants’ consent attitudes. Our results are also based on self-report measures and participants were not led to believe that they were interacting with a real person and were primed about the nature of the study. In Study 2, we address these limitations using a lab experiment with psychophysiological and observational measures and a cover story to avoid priming.
Study 2 Method
Participants
We collected data from a sample of 114 participants, the majority of whom were students at an urban university in the Pacific Northwest region of the United States. We recruited participants over 18 years of age from a participant pool that was collected using fliers around the university campus and the city. Participants were excluded at recruitment if they reported a heart condition or pregnancy, which could interfere with CV measures. One participant did disclose a diagnosis of Wolf Parkinson's White Syndrome after participation; they did not have an atypical heart rate during the experiment and were included in analyses. The sample was not limited to university students, but most of our participants were students at this university. Most participants were White and women. Demographics are shown in Table 1.
Confederates
Several confederates posed as participants and served two major roles in the study. First, confederates served as ostensible sexual violence survivors with whom the participants would interact. Second, confederates observed how much interpersonal warmth the participants displayed when interacting with them. All confederates were female-presenting emerging adult undergraduate research assistants and were instructed to wear plain jeans, a neutral shirt, and a (provided) neutral hoodie with the university logo. Confederates were unaware of the experimental condition. Prior to posing as participants, all confederates were trained on the study protocol, including the observational measures they would complete, and participated in practice runs of the protocol.
Experimenters
Experimenters were also all female-presenting emerging adults. They were trained to identify signs of distress if the content of the study triggered a participant and were given resources to provide in that case. They wore long pants, close-toed shoes, and a white lab coat. Long hair was tied back. Experimenters were also unaware of the experimental condition.
COVID-19 sample size limitations
Our intended sample size was 300 participants to achieve substantial cell sizes for each of our three experimental conditions. We collected data from October 2019 to March 2020 when the COVID-19 pandemic necessitated that we pause data collection. We intended to resume data collection, but due to our design, we decided to end data collection approximately 1 year after the initial pause. The psychophysiological measures in our design require close contact between the experimenter, confederate, and participant. The use of face masks would compromise the validity of our confederate-rated interpersonal warmth measure, as the confederate would be unable to see much of the participant's face. This situation would likely induce feelings of threat in many participants related to the risk of contracting COVID-19 independently of the experiment. We could not continue data collection without compromising the safety of our research team and participants and the integrity of our research design, so we ended the study early. Based on a sensitivity power analysis conducted in G*Power (Faul et al., 2007), a regression model with 11 predictors (i.e., the most complicated model we tested) and a sample size of 114 has 0.8 power to detect an effect size of f2 = 0.16, representing a medium effect size. The smaller sample size is a limitation of this study.
Procedures
Study procedures are presented in a timeline in Figure 1.
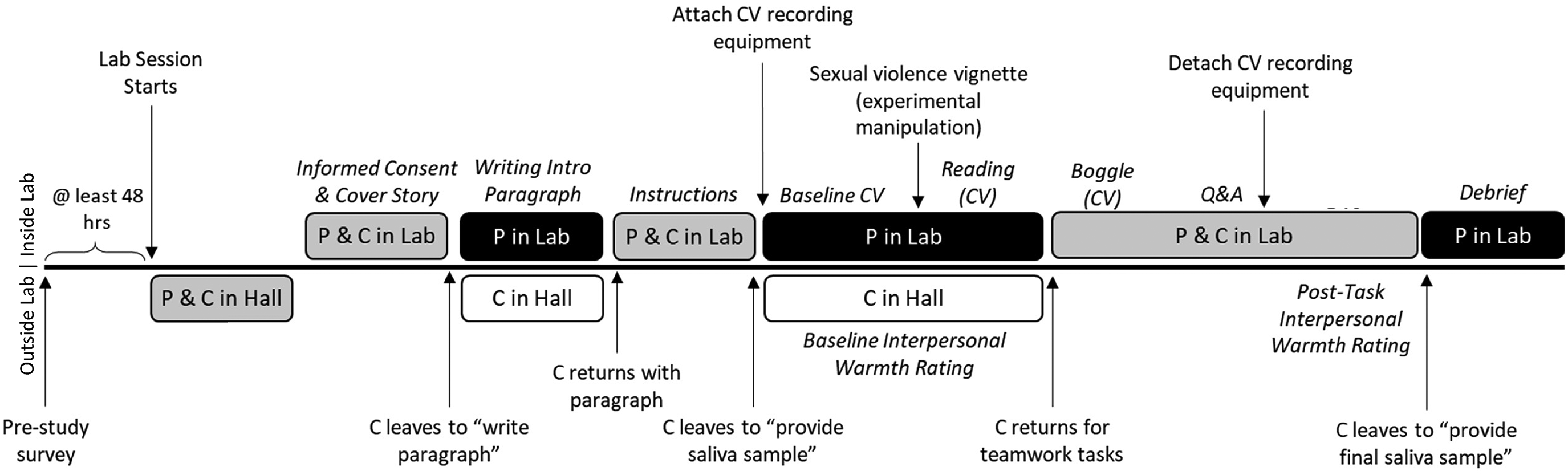
Study 2 experimental procedures.
Online survey
The participants were told that the study was about teamwork and were warned that it would contain sensitive content. To avoid priming, we provided participants with a list of sensitive topics including the true object of the study (i.e., sexual violence). The participants were asked to fill out an online survey including demographics, a measure of sexual consent attitudes, and several filler measures intended to disguise the true topic of the study. These included measures of alcohol use, experiences of racism, and antisocial personality traits.
Lab session
After completing the survey, the participants signed up for a time to participate in the in-lab portion of the study. The participants were only allowed to schedule their lab appointment 48 hours or more after they took the survey to avoid priming.
Participant arrival
When participants arrived at the lab, the confederate was posing as another participant waiting in the hall. The experimenter invited the participant and confederate into the lab, stated that the study was about teamwork, and gave the informed consent process.
Paragraph writing
Both participant and confederate were asked to write a paragraph about an impactful event that happened to them under the guise of needing to know information about their teamwork partner for the study. The experimenter gave the participant an envelope with a blank sheet of paper inside and the confederate an identical envelope with a prewritten paragraph inside. This prewritten paragraph was written in the confederate's handwriting and was one of the three conditions (control, no-consent, and reporting) randomly assigned before the start of the study. The confederate was then led outside to ostensibly write their paragraph in another room while the participant wrote their paragraph in the lab.
CV equipment attachment and baseline
The experimenter told the participant and confederate that they would give either saliva or CV measures. Using a rigged drawing, the participant was always chosen to have CV measures taken. The confederate left the lab to give a saliva sample, waited in the hall, and completed a baseline interpersonal warmth rating of the participant. The experimenter attached the CV equipment to the participant's body and recorded 3 min of baseline CV data (baseline CV) as the participant watched a screensaver.
Experimental manipulation
After baseline CV data were recorded, the experimenter left the laboratory room to “drop off” the participant's paragraph to the confederate. The confederate did not read the participant's paragraph. Upon return to the lab, the experimenter asked the participant to read the study vignette that the participant believed to be written by the confederate. One minute of CV data (reading CV) was recorded as the participant read the vignette. The experimental manipulation was at the end of the paragraph. After the participant was done, they returned the paper to the envelope, so the experimenter did not see it.
Teamwork task
After the reading portion, the confederate was brought back into the lab to complete two tasks with the participant. First, the confederate and participant played a modified version of boggle where they identified words together. This task served as the motivated task situation needed to support the biopsychosocial model of challenge and threat. Similar tasks have been used to assess stigma-related CV challenge/threat in the past work (e.g., Blascovich et al., 2001). The board was kept the same for each participant. All confederates were given a key to the words on the board and asked to alternate their answers with the participant. During this task, 3 min of CV data were recorded from the participant (boggle CV).
Question and answer
After the boggle task, the participant and confederate engaged in a question-and-answer task in which the confederate asked the participant a standardized series of questions about teamwork (e.g., “Why do you think teamwork is important for accomplishing tasks?”). This allowed the confederate more time to assess the interpersonal warmth of the participant. Unlike in the boggle task in which both participant and confederate were looking at the board, this task allowed the participant to make eye contact and exhibit other nonverbal behaviors. CV recordings from this task were not included in our analyses, consistent with past research (Blascovich et al., 2001).
Post-test interpersonal warmth
The confederate then completed the post-test interpersonal warmth rating on a tablet while the experimenter detached the CV recording equipment from the participant. The confederate was then escorted from the lab.
Debrief
The participant was debriefed by the experimenter while recording the participant's level of suspicion during the process. Before leaving, the participant completed a manipulation check of several questions about their memory of the vignette. Due to the sample size, we did not use these as exclusion criteria to avoid a significant decrease in statistical power.
Materials and Measures
Demographics
Demographic items were the same as those for Study 1.
Process-based consent scale
Study 2 used the same version of the Process-Based Consent Scale (Glace et al., 2021) as Study 1. The scale had an acceptable reliability (α = 0.78).
Sexual violence vignettes and experimental manipulation
All participants read one of the three vignettes used in Study 1, including the no-consent condition, a reporting condition, and a control condition. Vignettes were written in the confederate's handwriting and randomly selected before the experiment. The experimenter and confederate did not know the condition.
Interpersonal warmth
Confederates rated the interpersonal warmth they perceived from the participant before and after the participant read the study vignette on a Likert-type scale from 1 (cold/unfriendly) to 7 (warm/friendly). Items included warmth, smiling, eye contact, and friendliness of body language (T1 M = 4.29, α = 0.94; T2 M = 5.31, α = 0.93). No interrater reliability was used as each participant only interacted with one confederate.
Cardiovascular Measures
CV measures were collected continuously during the 3-min baseline period, the 1-min reading period, and the 3-min boggle task using MP160 data acquisition hardware and AcqKnowledge software from Biopac (Goleta, CA, USA).
Electrocardiography was collected using a Biopac amplifier (Model ECG100C). We used a modified Lead II electrode configuration; one spot electrode was placed directly under the right clavicle bone and the other was placed under the left rib cage. Noninvasive impedance cardiography was collected using a Biopac amplifier (Model NICO100C). Eight spot electrodes were placed on the participant's neck and torso; the inner electrodes were placed in pairs, with two electrodes on either side of the base of the neck and two on either side of the torso at the level of the xiphisternal junction (the base of the sternum). Outer electrodes were placed in pairs at least 1 inch away from the inner electrodes; two were placed on either side of the upper neck, and two on either side of the torso toward the bottom of the rib cage. Continuous blood pressure was collected from the participant's nondominant arm using a Biopac monitor and amplifier (Model NIBO100D). A brachial cuff was placed on the participant's upper arm, and a volume clamp was placed on the participant's index and middle fingers. The volume clamp, calibrated by the brachial cuff, assessed the blood pressure continuously using photoplethysmography.
All signals were collected and calibrated in AcqKnowledge software, and then scored by the first author in the Moving Ensemble Average Point-Marker (MEAP) software (Cieslak et al., 2018). More information on CV data scoring and cleaning can be found in the Appendix.
Per the Biopsychosocial Model of Challenge and Threat, we were interested in several key CV measures: First, heart rate (number of heartbeats per minute, measured using electrocardiography) and ventricular contractility (the force with which the heart muscle contracts, measured from electrocardiography and impedance cardiography) are used to establish task engagement. If both the heart rate and ventricular contractility increase from the baseline, the participant is engaged, and threat/challenge states can be measured and differentiated. Once the task engagement is established, two measures are used to differentiate challenge and threat states. The cardiac output (the total volume of blood pumped by the heart each minute, calculated from impedance cardiography) increases from baseline during states of challenge and remains stable or decreases slightly during states of threat. The total peripheral resistance (amount of constriction of the peripheral blood vessels, measured from blood pressure and impedance cardiography) remains stable or decreases from the baseline during states of challenge and increases from the baseline during states of threat. Formulae used for these calculations can be found in the Appendix.
We calculated an index of challenge/threat for each task (reading, boggle) by combining the cardiac output and the total peripheral resistance (Blascovich et al., 2004). Standardized cardiac output was subtracted from standardized total peripheral resistance and then the reactivity scores were calculated for both tasks relative to the baseline. In the resulting Threat–Challenge Index (TCI), higher values mean more threat/less challenge and lower values mean more challenge/less threat.
Analysis Plan
We conducted a series of multiple regression analyses for each outcome variable including the TCI difference scores between the baseline period and reading period (reading TCI), TCI difference scores between the baseline period and boggle period (boggle TCI), and interpersonal warmth difference scores between the pre-test and post-test. Predictor variables were mean-centered.
Step 1 models for each outcome variable included two dummy coded variables for the no-consent (vs. control) condition and the reporting (vs. control) condition. TCI models also included the heart rate and ventricular contractility reactivity as covariates. Step 2 models added the moderators (i.e., gender, consent attitudes). Step 3 models added the interaction terms (i.e., condition × gender, condition × consent attitudes, and gender × consent attitudes). Simple slopes were examined for significant interactions. The results are shown in Table 4.
Study 2 Results.
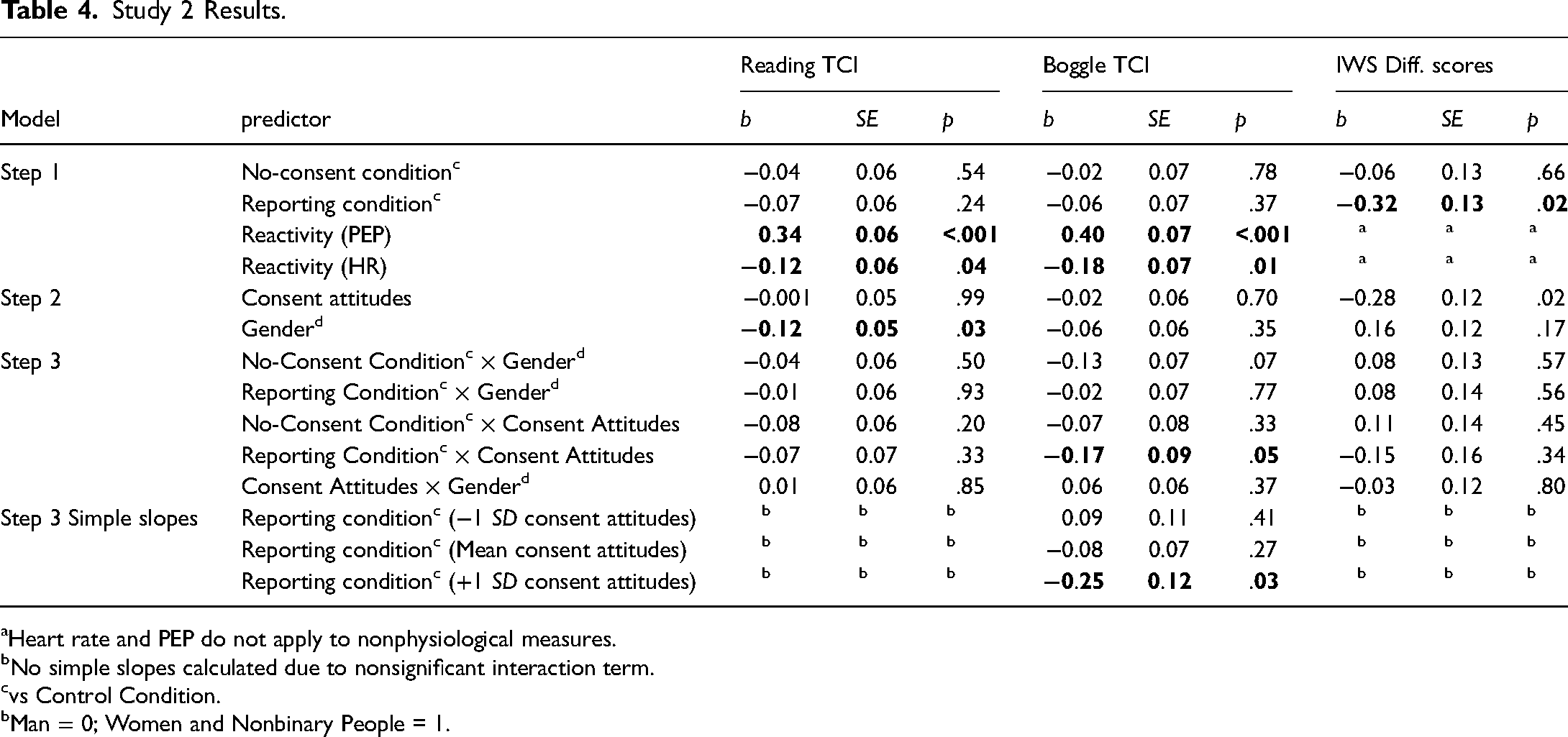
Heart rate and PEP do not apply to nonphysiological measures.
No simple slopes calculated due to nonsignificant interaction term.
vs Control Condition.
Man = 0; Women and Nonbinary People = 1.
Results
Task Engagement
Based on the heart rate (reading p < .001; boggle p < .001) and ventricular contractility (reading p < .001; boggle p < .001), participants were engaged in both tasks.
Reading TCI
Neither condition variable, interaction term, nor consent attitudes were a significant predictor of reading the TCI. Men were more threatened while reading than women and nonbinary people.
Boggle TCI
The dummy-coded condition variables, gender, and consent attitudes were not significant predictors of boggle TCI. The interaction between the dummy-coded variable representing the reporting (vs. control) condition and consent attitudes was a significant predictor of boggle TCI. For individuals low (−1 SD) and moderate (mean) in support for sexual consent, reporting (vs. control) condition was not a significant predictor of boggle TCI. However, for those high (+1 SD) in support for sexual consent, being in the reporting (vs. control) condition predicted significantly lower boggle TCI (see Figure 2).
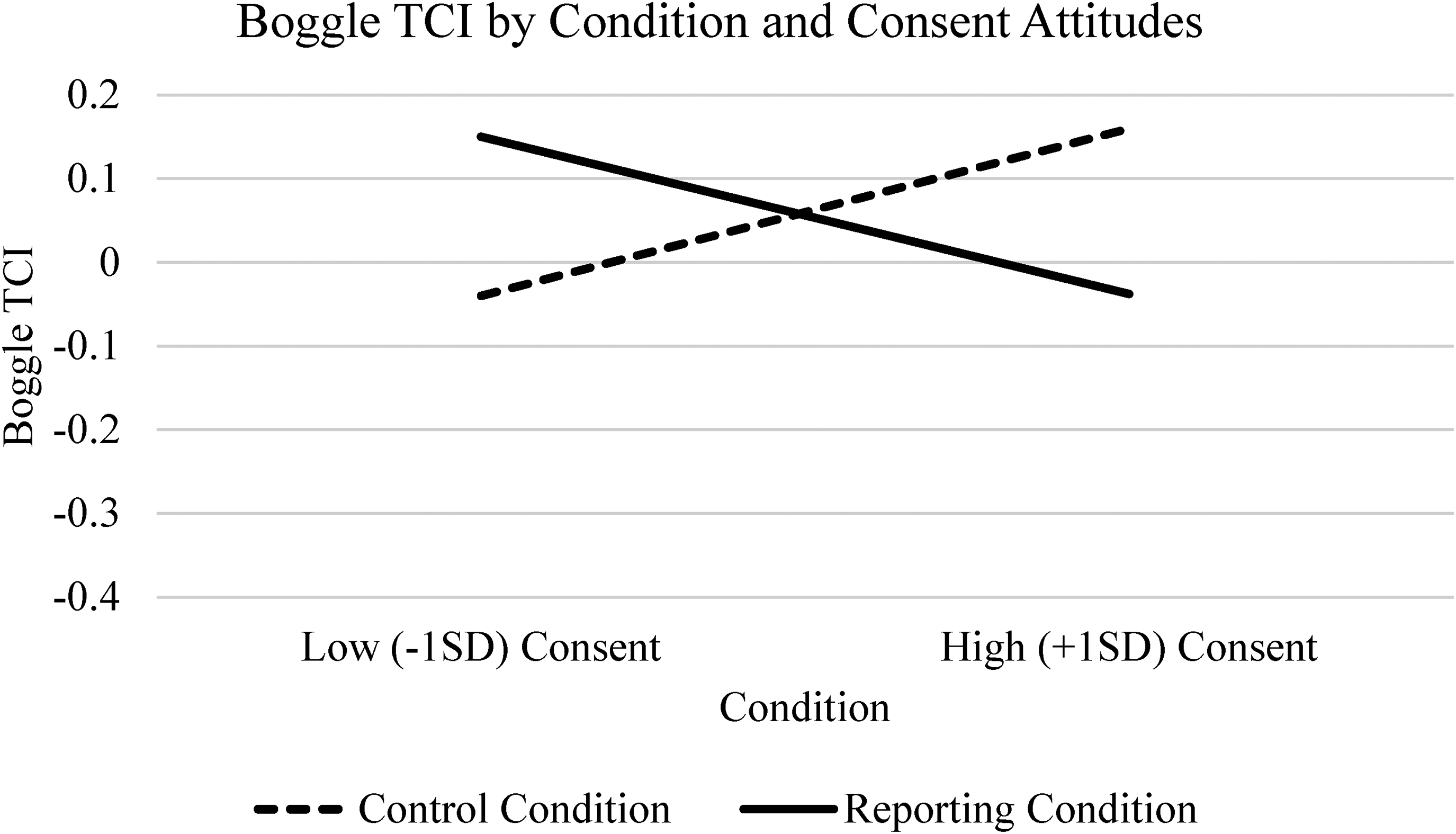
Study 2 boggle TCI by condition and consent attitudes.
Interpersonal Warmth
While interpersonal warmth increased from pre-test to post-test, this increase was significantly less among participants in the reporting condition than those in the control condition (see Figure 3). Higher support for sexual consent was associated with lower interpersonal warmth difference scores; those high in support for sexual consent increased less in interpersonal warmth from pre-test to post-test. No interaction terms were significant.
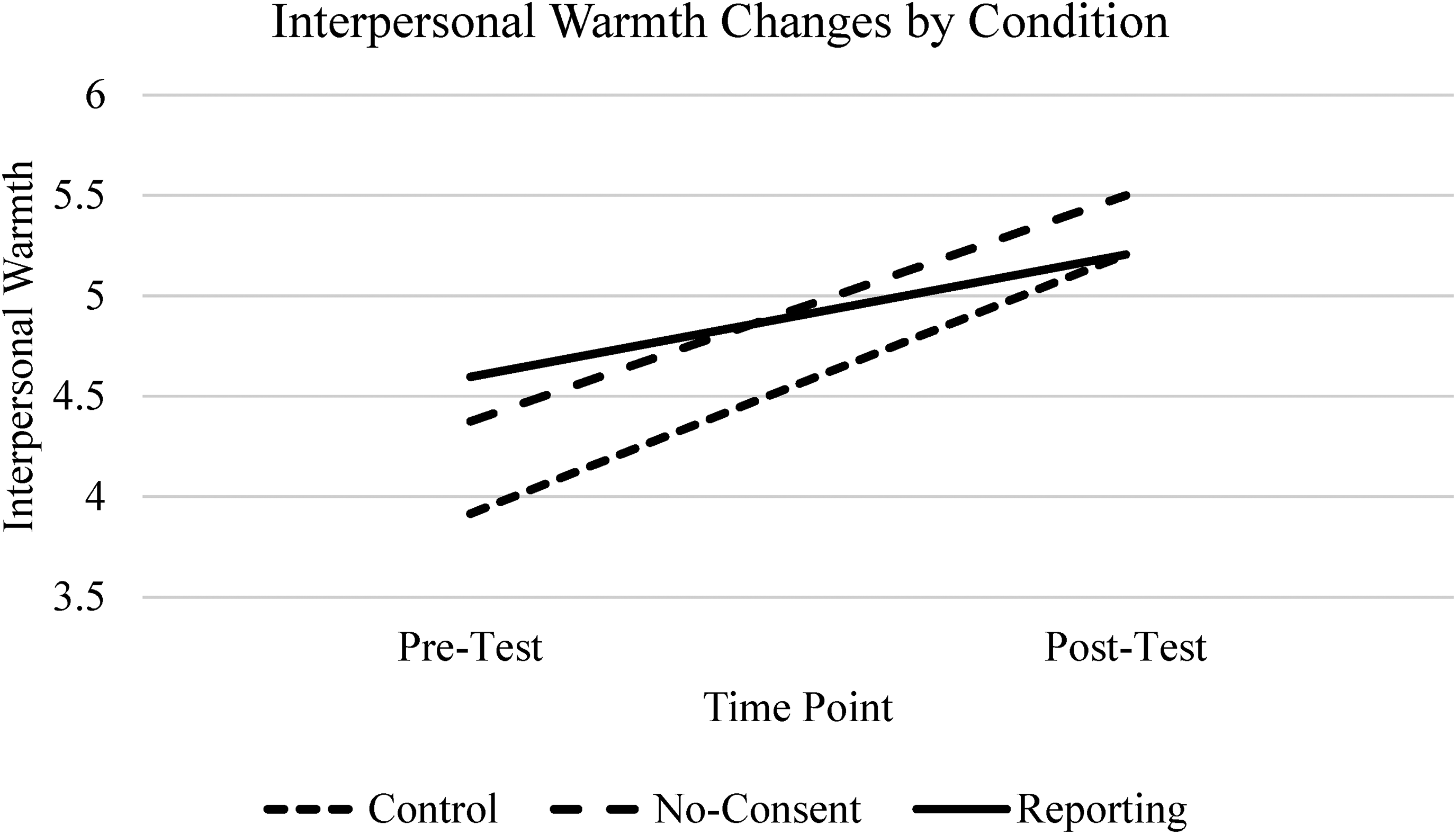
Study 2 interpersonal warmth changes by condition.
Study 2 Discussion
Experimental condition alone was not significantly associated with TCI. This is expected in the reading period, as participants did not encounter the experimental manipulation until the end of the measurement period. However, interpersonal warmth difference scores were significantly lower in the reporting condition than in the control condition, supporting hypothesis 1b. Unsurprisingly, interpersonal warmth increased from pre-test to post-test in general, as participants were encouraged to collaborate on a task in a way that increases liking (Deberry, 1989). That this change was lower in the reporting condition suggests that survivors who made a formal report did not experience this same increase in warmth.
While the reporting condition did not predict boggle TCI, there was a significant interaction between the reporting (vs. control) condition and consent attitudes in predicting boggle TCI. Among those high in support for sexual consent, being in the reporting (vs. control) condition was associated with a lower boggle TCI. The opposite set of simple slopes suggests that higher consent attitudes predict lower threat in the reporting condition but not the control condition. However, this result was determined by lower boggle TCI in those high in support for consent as opposed to a higher boggle TCI in those low in support for consent. Individuals high in support for consent may feel less threat when interacting with a survivor who does not believe that sexual violence should be dismissed compared to a survivor whose stance is more ambiguous.
Supporting the latter interpretation, participants high in support for sexual consent also had lower interpersonal warmth difference scores, such that they did not increase the warmth with which they treated the survivor to the extent that participants lower in support for sexual consent did. These participants may have appeared less warm because they were more likely to recognize the trauma the survivor had experienced and thus behaved less warmly (e.g., smiled less). Even disclosure recipients who hold supportive beliefs might seem cold to survivors due to their own sadness. However, it is possible that a genuine survivor could perceive a more somber response to be more supportive; future research is needed to determine what survivors perceive to be supportive in these contexts.
While gender did not relate to condition as hypothesized, men did show higher TCI during the reading session than women and nonbinary people. It is somewhat surprising that men, who are less likely to experience sexual victimization than women and nonbinary people (Iles et al., 2021), are more threatened when reading about sexual violence than those who are at a higher risk. This is contrary to a system justification interpretation of our results, which would suggest that those who are more harmed by the status quo should react just as or more defensively (Iles et al., 2021). Men are less likely than women to be recipients of sexual victimization disclosures (Orchowski & Gidycz, 2012). Women and nonbinary people might be more desensitized to disclosures than men and thus feel less threat related to the topic. Additionally, this finding does support an ambivalent sexism model of survivor stigma, as men are on average higher than women in rape myth acceptance and hostile sexism (Glick & Fiske, 1996; Kunst et al., 2019).
Strengths and Limitations
Study 2 took place in a lab setting with high experimental control, an experimenter and a confederate who were both unaware of the experimental condition and used measures unlikely to be impacted by social desirability. However, Study 2 also had limitations. Similar to Study 1, the sample was homogeneous (i.e., primarily White undergraduate students). Most of our sample was cisgender, such that our discussions of gender may not apply to gender minority people. We did use several confederates with different appearances and identities. Participant opinions may have been impacted by characteristics of the confederate with whom they worked (e.g., confederate race), but these differences in perception are unlikely to have impacted differences based on conditions due to our use of random assignment. Additionally, the sample size for Study 2 was small and fell well short of our planned sample size as the experiment was ended early due to the COVID-19 pandemic. The resulting lack of statistical power might have made it difficult for us to accurately detect significant effects, so the results of this research should be interpreted with caution and require replication. This study also lacks external validity that limits the interpersonal warmth measure. In real disclosure situations, survivors might perceive behaviors like smiling as unsupportive.
Overall Discussion
We hypothesized that individuals would have more stigmatizing reactions to survivors who used consent language or made a formal report of their experiences than survivors who did neither. In Studies 1 and 2, we found partial support for hypothesis 1. Survivors who file a report, but not survivors who only use consent language, were met with negative reactions. In Study 1, participants may have justified this negative reaction by altering their perceptions of consent in general to support more sexual coercion, though this finding requires further research. Survivors who used consent language and survivors who dismissed their victimization were treated similarly; consent language may not prompt the same backlash as filing a formal report. Negative reactions to survivors who file a formal report are consistent with both ambivalent sexist and system justification models of survivor stigma. Attempting to hold the perpetrator accountable over a non-stereotypic rape might prompt feelings of hostile sexism, leading to stigmatizing treatment of the survivor. Filing a formal report of an incident of sexual violence might be seen as a threat to the social system, prompting system-justifying motives.
Negative reactions to reporting survivors might be attenuated among those high in support for sexual consent, who may feel less stigma towards a survivor who files a report than one who does not. Among those who recognize both the importance of consent and that rape does occur, rape going unpunished might prompt a system justification motive more than a rape being committed in the first place. However, in Study 2, individuals high (vs. low) in support for consent showed less of an increase in interpersonal warmth towards survivors overall, controlling for condition. The individuals who theoretically should have the most supportive responses did not seem to become as warm to the confederates as those who theoretically might have less supportive responses. Survivors, regardless of reporting, may still face cold reactions even from supportive disclosure recipients.
Implications
Survivors of sexual violence who make a formal report face stigma. Survivors in this situation may be at higher risks of facing the negative social, emotional, and health consequences associated with unsupportive social reactions to disclosures of sexual victimization (Dworkin et al., 2019). These survivors may require additional support when disclosing their experiences and recovering from sexual victimization. There is also limited evidence that when survivors who chose not to file a report disclose their experiences to an individual high in support for sexual consent, the disclosure recipient might feel more threat, and could communicate stigma. Would-be supportive disclosure recipients may benefit from education on supportive responding. Universities might implement training for students to practice supportive disclosure responses; more research and program development is needed in this area.
Limitations
The biggest limitations of this research include generalizability and external validity. As mentioned, the samples are predominately White and heterosexual. For Study 2, the sample is mostly undergraduate students as well. Additionally, the vignette described a rape perpetrated by a man against a woman. The results of our research may not apply to disclosure recipients with experiences and identities that differ from our sample nor survivors whose experiences do not align with the study vignette. Additionally, our findings may not translate to stigma outside the lab. While the biopsychosocial model of challenge and threat demonstrates advantages over self-report measures, further research is needed to determine how cardiovascular threat might relate to real-life disclosure responses.
The way that gender was calculated in our research is also a limitation. We treated gender as a binary variable, comparing men vs. women and nonbinary people. This combination was necessary for sample size reasons but does limit the way that gender can be understood in interpreting our results. We acknowledge that this creates a complex situation for transgender men, who are both men and gender minority individuals. Our sample included only one transgender man, meaning this coding decision is unlikely to substantially impact our results. Still, this is a limitation on our study and an important topic for future investigation.
Future Directions
Future research should examine cases where people who intend to respond supportively to sexual violence survivors struggle to do so. Qualitative research with disclosure recipients would be useful to gain more insight into the processes underlying our findings. Future research should also investigate ambivalent sexism, system-justifying motives, and their role in responses to sexual violence survivors. Understanding how sexist attitudes and system-justifying beliefs might predict stigmatizing responses to survivors is important in preventing survivor stigma. Field research with higher external validity will be important in this regard. While genuine disclosures are very difficult to predict, often precluding baseline measurement, the way individuals react to fabricated disclosures from strangers in a lab is likely to differ significantly from how they would react to an authentic disclosure from a close other in their day-to-day life.
Conclusion
We conducted two experiments, finding that sexual violence survivors face stigma when making a formal report of their experiences, such that perceivers treat them with less warmth and may even alter their own attitudes about consent. However, this same effect is not observed when survivors claim that their experience was nonconsensual but do not make a formal report. All sexual violence survivors are at risk of experiencing stigma; those who seek accountability from the perpetrator may be at higher risk, especially when the victimization is not stereotypical.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded in part by a grant from the Society for the Psychological Study of Social Issues (SPSSI)'s Grants-In-Aid Program, awarded to Dr. Tessa L. Dover (grant number Grants-in-Aid).