
Abstract
Survivors of intimate partner violence (IPV) often experience violent blows to the head, face, and neck and/or strangulation that result in brain injury (BI). Researchers reviewed the de-identified forensic nursing examination records of 205 women. More than 88% of women were subjected to multiple mechanisms of injury with in excess of 60% experiencing strangulation. About 31% disclosed various symptoms consistent with BI. Women experiencing strangulation were 2.24 times more likely to report BI-related symptoms compared to those who reported no strangulation. In conclusion, women experiencing IPV are prone to BI suggesting early screening and appropriate management are warranted.
Keywords
Background
Intimate partner violence (IPV) refers to physical or sexual violence, stalking, and psychological aggression by a current or former intimate partner (Breiding et al., 2015). It is a global public health epidemic and the most common form of violence against women, affecting one in three women in their lifetime (Devries et al., 2013; WHO, 2021). Although individuals of all genders experience IPV, most public health statistics report a far greater incidence of IPV resulting in injury to women (Cotter, 2021). In Canada, the prevalence of women experiencing IPV is estimated to be more than four in 10 women (Cotter, 2021). In addition, more than 25% of women who experience IPV have episodes at least once a month, and approximately 10% experience it almost daily (Cotter, 2021).
It is increasingly recognized that brain injury (BI), resulting from violent blows to the head, face, and neck and/or episodes of strangulation, affects women experiencing IPV at high rates (Haag et al., 2019). Studies have shown 30% to 94% of women experiencing IPV report at least one BI (Ayton et al., 2021; Kwako et al., 2011; Valera & Berenbaum, 2003). Additionally, in a sample of 99 survivors, Valera and Berenbaum (2003) reported 27% of women surveyed sustained anoxic/hypoxic events related to strangulation. It has been recognized strangulation has significant negative effects on survivors’ mental health as it is often used as a coercive control tactic (Myhill & Hohl, 2019). Similar to post-concussive signs and symptoms, women experiencing IPV-caused BI from head impacts and/or strangulation demonstrate various chronic impairments. Long-term chronic cognitive impairments include deficits in memory, attention, reasoning, planning, and executive functioning (Maldonado-Rodriguez et al., 2021; Valera et al., 2019). The psychopathological problems include depression, anxiety, fatigue, and post-traumatic stress disorders (Valera & Berenbaum, 2003; Valera et al., 2019). The sensorimotor problems include paralysis or paresis of facial or extremity muscles, numbness, loss of sensation, muscle spasms, facial droop, and unilateral weakness (Patch et al., 2018). All these impairments ultimately impact the quality of life of women experiencing IPV-caused BI.
Survivors of IPV-caused BI are largely underserved due to an underestimation of the prevalence, little to no awareness of the issue by the public, women's shelters (Nicol et al., 2021), or healthcare providers, and the stigma underlying IPV in general (Yoshioka et al., 2003). In addition, staff working in IPV-related organizations may be aware of the high risk for BI among their clients, but due to different implementation barriers, may not routinely screen for BI. As a consequence, a large proportion of women remains unsupported and may be exposed to the cumulative effects of repetitive BIs (Kwako et al., 2011; Patch et al., 2018; Valera & Berenbaum, 2003) and chronic symptoms (Nicol et al., 2021; Smirl et al., 2019) as a result. Therefore, detection of BI at the acute stage (i.e., within a week or two; Gravel et al., 2013) through screening is crucial in order to recognize and treat BI in this underserved population. Early detection of IPV-caused BI, and thereby its timely treatment and rehabilitation, would mitigate the immediate impacts and minimize the long-term consequences of BI, and would improve the quality of life of victims. Thus, clearly and objectively characterizing the impact of BI on survivors of IPV at the acute stage will have far-reaching implications for social support policy and funding for this population and their caregivers.
Most of the studies on IPV-caused BI have been conducted at the chronic stage of the injury (>1 month; Ayton et al., 2021; Haag et al., 2019; Kwako et al., 2011; Valera & Berenbaum, 2003). A study by Ralston et al. (2019) may be the only study to date to report IPV-caused BI at the acute stage through the review of forensic nursing examination charts. In this study, 18 of 19 participants (94.7%) reported signs and symptoms consistent with BI and had visible injuries to the head and/or neck. All participants also reported a mechanism of injury with the potential to cause a BI. In addition, this study explored the rate of IPV-caused BI in a previously unstudied setting, a forensic nursing clinic. Given these findings and the fact forensic nursing clinics predominantly provide immediate support to individuals who have experienced IPV and/or sexual assault, we posit this may be a promising setting for the implementation of IPV-caused BI screening protocols at the acute stage of injury.
However, the study by Ralston et al. (2019) reviewed a relatively small number of charts (N = 19) and was restricted to cases involving strangulation experiences only. Yet, the available literature shows a large percentage of women experiencing IPV sustain head impacts (74%)—with or without strangulation—rather than strangulation alone (27%; Valera & Berenbaum, 2003). Because of these facts, the generalizability of the findings from the study by Ralston and colleagues may have been limited. In the current study, we addressed these limitations by conducting a retrospective forensic nursing examination chart review in a large sample of women who had experienced IPV. Notably, this project is the result of a collaboration between researchers and forensic nursing examiners (FNE). Throughout their clinical practice, the latter noticed women experiencing IPV frequently reported symptoms consistent with BI, and identified a need for more intentional screening for IPV-caused BI. As such, the overarching objective of this study is to provide suggestions and insights that will be helpful to both researchers and clinical practitioners.
Therefore, the purpose of this study was to (1) describe the rates of IPV-caused head impacts and strangulation in this cohort; (2) identify symptoms consistent with acute BI; and (3) explore the relationship between these symptoms of BI and various demographic and clinical characteristics. More specifically, we explored the relationship between symptoms of BI and age, strangulation, weapon applied, sexual assault, mechanism of injury, physical injury, as well as the history of previous similar incidents. Lastly, we provide recommendations to guide the implementation of IPV-caused BI screening in a forensic nursing examination setting.
Methods
Setting and Participants
In this retrospective study, we reviewed the de-identified forensic nursing examination records from the Forensic Nursing Service (FNS) at one of the largest hospitals in the Fraser Health Authority in British Columbia, Canada. The FNS provides acute, medical-forensic examination for survivors of recent interpersonal violence such as sexual assault, partner violence, exploitation, and abuse. Specially trained Registered Nurses acting in the role of FNEs are contacted when a patient presents to the emergency department disclosing recent interpersonal violence, which occurred within the last 7 days. Patients must be medically cleared by the emergency department staff to ensure urgent medical issues are dealt with prior to forensic examination. The FNE meets with the patient in a private location to gather a brief history of the recent incident using a Forensic Nursing Record. This record routinely collects specific information with respect to the incident, which may inform forensic examination. At this time, this record does not specifically explore head injury but does ask about specific acts of violence, including strangulation. With patient consent, the FNE can perform a head-to-toe forensic medical examination. This examination may include documentation of visible injuries, use of an alternate light source to identify injuries or body fluids not visible to the naked eye, and collection of forensic specimens such as swabs, fibers, debris, and body fluids (i.e., vomitus, urine, blood). Urgent medical concerns that arise during this exam are referred back to the emergency department team. Other medical issues that may require follow-up are addressed by the FNS outpatient clinic, Embrace Clinic.
Out of 864 Forensic Nursing Records available, there were only seven (0.8%) male victims. Most public health statistics consistently report a far greater incidence of IPV in women compared to men (Cotter, 2021). Therefore, male victims were excluded from this analysis. In total, 857 women visited the FNS between January 7th, 2018 and December 31st, 2020. The records of 247 women over the age of 16 years who reported domestic or partner violence with or without sexual assaults were available to review. We excluded those women who experienced violence from family members other than intimate partners (e.g., father, stepdad, cousin, brother, sister-in-law, mother-in-law, brother-in-law; n = 20, 2.3%), from friends (n = 13, 1.5%), or from an undisclosed perpetrator (n = 9, 1.1%). We conducted further analysis in the sample of 205 women (Figure 1). Approval to conduct the study was received from the Fraser Health Research Ethics Board (FHREB 2021–014) and the University of British Columbia Clinical Research Ethics Board (H21–00362).
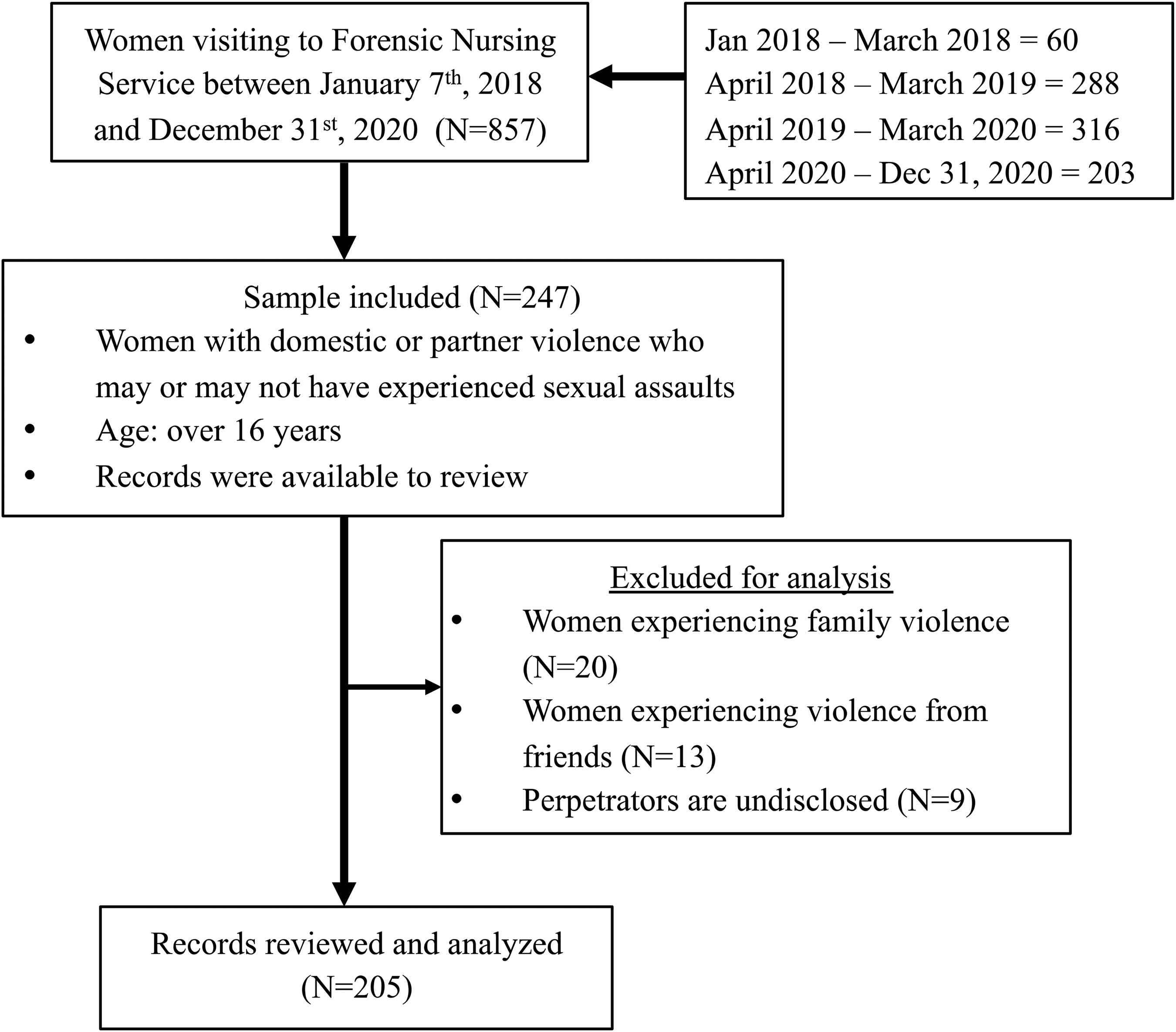
Process Flow Diagram.
Forensic Nursing Examination Records
The forensic nursing examination records contained de-identified demographics, examination data, time, location of the assault, and incident history. A narrative section included the patient's voluntary disclosure regarding the incident and its consequences, signs and symptoms, and information on the patient's pre- and post-incident habits and activities. There were no specific questions included in this section. Participants voluntarily disclosed information if they had any, under the sub-heading “patient voluntarily disclosed the following.” Information relevant to sexual assault and strangulation was collected in separate sections within the form. Additionally, a section to record all injuries through physical examination was also included.
Review of Records and Data Extraction
Five assessors (all are authors of this article) reviewed participants’ records to systematically extract the relevant information. To achieve consistency among assessors, two education sessions were conducted by the first and main author of this study before the beginning of the data extraction. Then, each assessor reviewed the records of five participants independently. The first author scored each assessor's review performance on a binary scale (1 = data correctly extracted, 0 = data incorrectly extracted) on 10 different variables of interest; age, violence type, post-incident duration, symptoms of voluntary disclosure, history of a previous similar incident, weapons applied, mechanisms of injury, sexual assault, strangulation characteristics, and physical injury measurement. This yielded a score between 0 and 10 for each assessor. The average score of assessors 1 through 5 were 10/10, 9.8/10, 9.8/10, 9.6/10, and 9.2/10, respectively. Intra-class correlation coefficient (ICC) was examined using SPSS to check the inter-assessor reliability. Cronbach's alpha was 0.99 and the ICC using a two-way random effects model for an absolute agreement was 0.98 (95% CI: 0.95–0.99, p < .001). Thus, inter-assessor reliability was excellent. A minor discrepancy among the assessors was found regarding the physical injury measurement, mechanism of injury, and symptoms of voluntary disclosure. Another education session was conducted in order to resolve the discrepancy and to gain absolute agreement among the assessors.
Demographic information included age, date of assault and date of examination (to calculate post-injury duration), violence type, history of previous similar incidents, and weapon applied by the perpetrators (Table 1). Symptoms or complaints that were consistent with BI were extracted from the patient's voluntary disclosure narrative as recorded by the forensic nurse examiner. As per the objective of this article, we focused on any symptoms potentially due to BI (Ralston et al., 2019; Valera & Kucyi, 2017). Therefore, symptoms related to alteration in consciousness (AIC), neurocognitive deficits, sensory-motor impairments of face, neck, and upper extremity, and emotional disruptions were extracted. It should be noted the forensic nurse examiners did not use any standardized measure for BI and did not prompt the patient to describe any signs and symptoms of BI. Therefore, such symptoms or complaints are termed “disclosed symptoms” in this article.
Descriptive Characteristics of the Women Who Experienced IPV (N = 205).
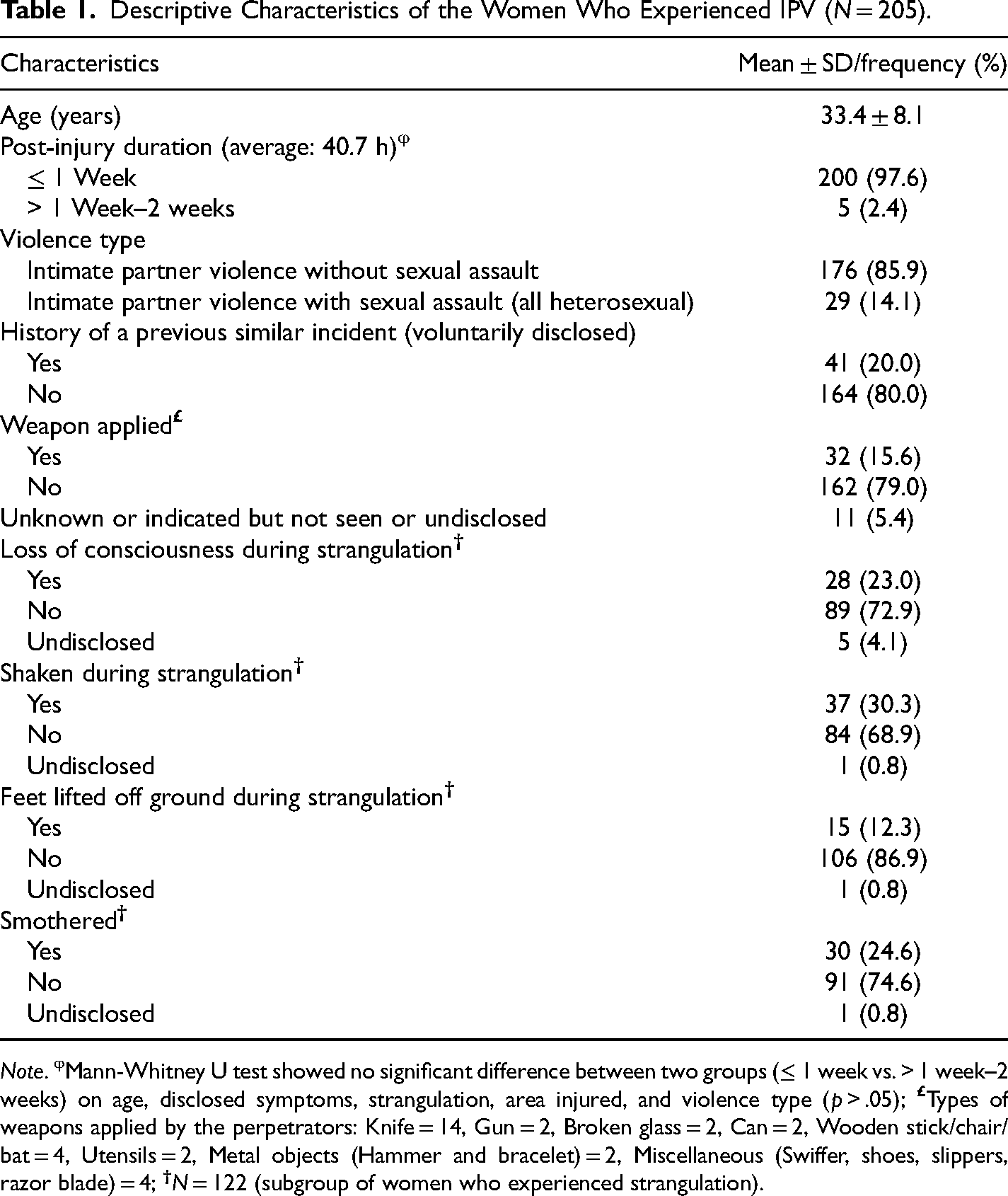
Note. φMann-Whitney U test showed no significant difference between two groups (≤ 1 week vs. > 1 week–2 weeks) on age, disclosed symptoms, strangulation, area injured, and violence type (p > .05);
The data on mechanisms of injury, with the potential to cause BIs are from participants’ self-report. Women were asked whether they had experienced sexual assault, strangulation, or other mechanisms of injury (such as being bitten, pushed, punched, slapped, kicked, etc.). FNEs inquire about strangulation by asking if anything was placed on or around the neck. FNEs are aware of the layperson and incorrect terminology “choking” to refer to strangulation and will use this term when needed to clarify in layperson’s terms. FNEs are very aware many people use the incorrect terminology but will professionally document using the correct word “strangulation” while placing a patient's words in quotations such as “he choked me.” They were further prompted to provide more detail if they answered “yes” to strangulation (Table 1). The forensic nurse examiners physically examined women and any injuries were recorded in the form of anatomical diagrams and in a table, which included the location of the injury, findings, description, and measurements. Injuries were classified on the basis of nine body regions; face, head, neck, upper extremities, lower extremities, torso, chest and breast, genitals and anus, or rectum. Area (in square centimeters) was calculated from the given length and breadth of each injury. Any injury <1 cm was considered 1 cm in the analysis. These measurements were added up to produce a total trauma size for each region and the average area injured. These values along with the number of areas injured were considered for analysis.
Statistical Analysis
The demographic and clinical characteristics of women are described with mean, standard deviation, and range or number and percentage. Prevalence was calculated as a percentage of the total number of women. Multistep, multivariable logistic, or multiple linear regressions were carried out to evaluate the relationships between different explanatory variables with categorical or continuous outcome variables respectively. Mann-Whitney U tests were used to compare women having various post-injury durations (≤ 24 h vs. > 24 h, and ≤ 1 week, vs. > 1 week to 2 weeks). The p-value was set to <.05. The analysis was carried out using the SPSS (Version 25.0, IBM Corp, Armonk, NY) and R (Version 3.6.3).
Results
Researchers reviewed the forensic nursing examination records of a sample of 205 women (mean age: 33.4 ± 8.1, from 18 to 50 years) who experienced IPV (Figure 1). All the women in this sample visited the FNS at the Hospital at the acute stage of the injury (within 2 weeks), of which 97.5% (n = 200) reported within 7 days of the incident. FNE saw five participants who had post-injury time beyond 7 days (Table 1).
Eighty-six percent of the women (n = 176) experienced IPV without sexual assault, with the remainder (n = 29, 14%) experiencing combined IPV and sexual assault, all of which occurred by a heterosexual assailant. As shown in Table 1, most of the IPV episodes (79%) did not involve a weapon. Approximately one-fifth of women voluntarily disclosed having had experienced similar incidents in the past. Assaults were most commonly by a spouse (n = 77, 38%), followed by a boyfriend (n = 59, 29%), ex-boyfriend (n = 26, 13%), or common law partner (n = 21, 10%). Ex-spouse, partner, ex-common law partner, fiance, and ex-fiance were the assailants in far fewer cases (varying between 2 and 5). Multiple intimate partners were involved in a small number of cases (n = 4), although it was unclear in the records whether this involved single or multiple incidents.
We found 60% of the cohort (n = 122) experienced strangulation. Because they were explicitly asked, the number of women who confirmed loss of consciousness (LOC) from strangulation was higher (n = 28, 23%) compared with the number who confirmed LOC in the voluntary disclosure section (n = 14, 11.5%). Out of 122, one-third (n = 37, 30%) of women were shaken during strangulation, 12% (n = 15) had their feet lifted off the ground during the strangulation, and 25% (n = 30) were smothered (Table 1). More than 91% of participants (n = 112) who experienced strangulation had physical injuries (such as swelling, bruises, abrasions, scratches, petechiae, redness, and tenderness) in the neck and/or head and/or face regions.
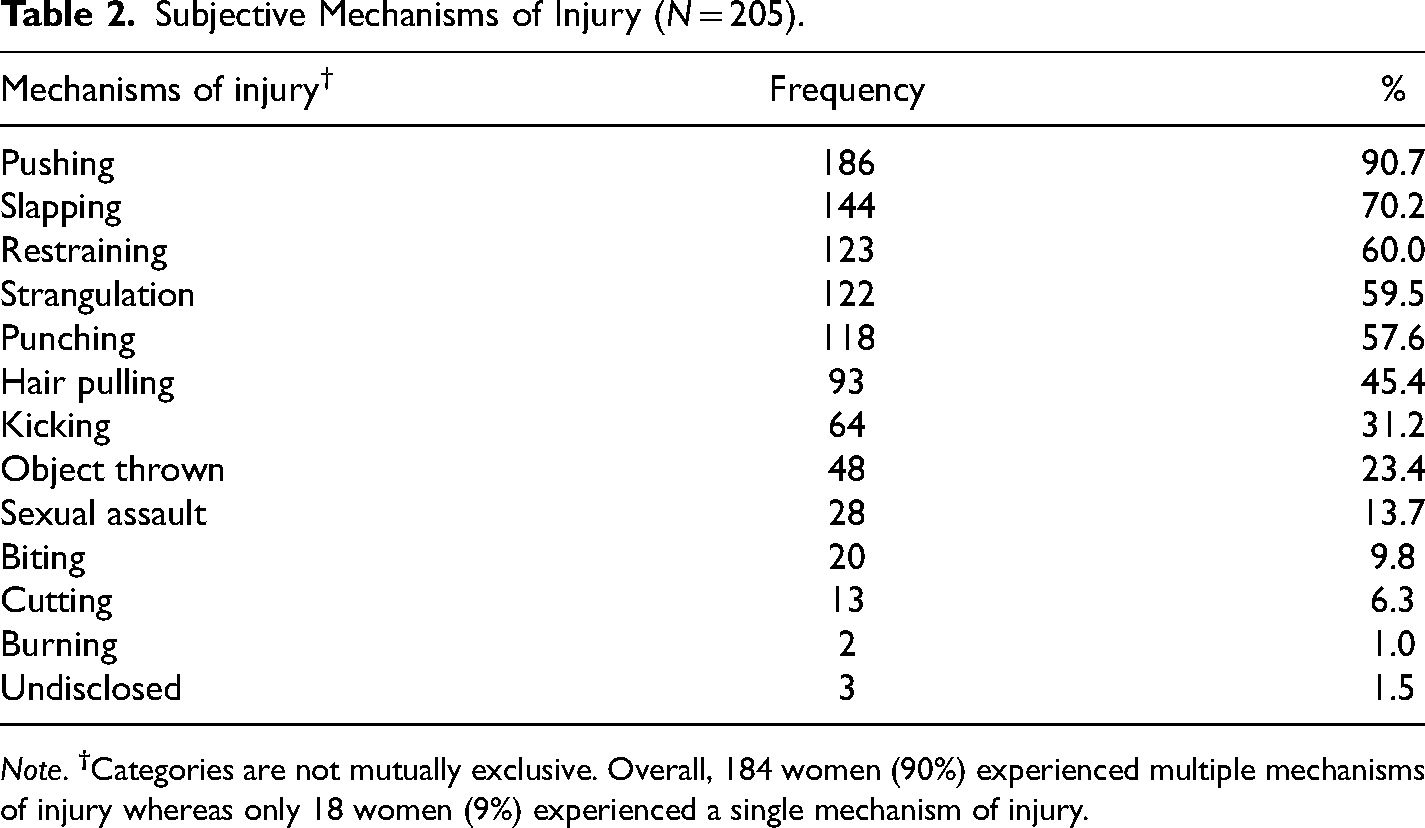
Eighty-nine percent of women (n = 182) were subjected to multiple mechanisms of injury based on participants’ self-reports. The most common mechanisms of injury included: pushing (91%), slapping (70%), restraining, (60%), strangulation (60%), and punching (58%). In women who experienced multiple mechanisms of injury, one or more of these five most common mechanisms emerged. Out of 18 women who had a single mechanism of injury, each experienced either pushing, slapping, strangulation, or punching. Other mechanisms of injury were hair pulling, kicking, object throwing, and sexual assault (Table 2). Three women did not report any mechanism of injury.
Subjective Mechanisms of Injury (N = 205).
Note.
The symptoms disclosed by women are summarized in Table 3. The disclosed symptoms are consistent with symptoms of BI extracted from the narrative section of the case charts. In total, 65 women (32%) disclosed various symptoms consistent with BI, which are listed under three-different sub-headings: AIC-related symptoms, sensory-motor symptoms, and emotional symptoms. Overall, LOC was the most commonly reported symptom (n = 17, 26%, of which 14 women experienced strangulation with or without head impacts, three women had head-only impacts) followed by other AIC-related symptoms: memory loss (n = 10, 15%), lightheadedness or dizziness (n = 6, 9%), seeing stars (n = 4, 6%), and blacked out (n = 4, 6%). Sensory-motor symptoms include mostly pain in and around the neck (n = 10, 15%) and breathing (n = 9, 14%) or swallowing (n = 4, 6%) difficulty. In addition, 11 women (17%) reported emotional disruptions. Approximately 25% of women (n = 16) disclosed experiencing multiple symptoms, most commonly a combination of two or three of the following: LOC, memory loss, seeing stars, blacked out, dizziness, headache, difficulty breathing and swallowing, pain, or emotional disruptions. Perhaps not surprisingly, the small number of women (n = 5) who did not experience any injury mechanism did not disclose any BI-related symptoms. Additionally, we ran an analysis to compare voluntarily disclosed symptoms between groups that were assessed at different post-injury timeframes (≤ 24 h, n = 116 vs. > 24 h, n = 86 and ≤ 1 week, n = 200 vs. > 1 week to 2 weeks, n = 5). The results showed no significant differences between groups (p > .05). This is likely due to the fact all participants were assessed in the acute stage (within 2 weeks) of the injury.
Disclosed Symptoms by the Women (N = 205).
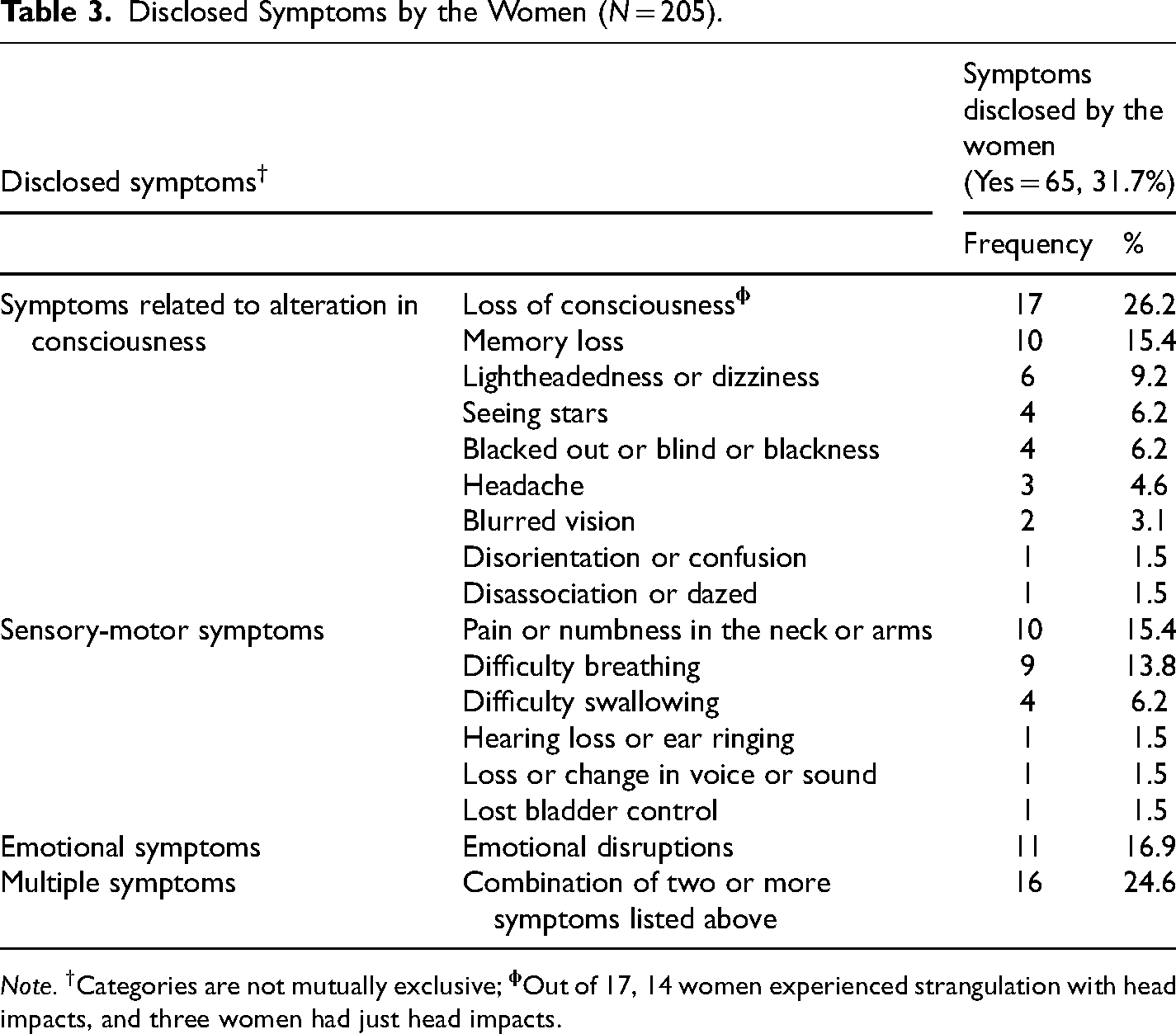
Note. †Categories are not mutually exclusive;
Overall, 198 women (97%) reported injuries to single (n = 9, 5%) or multiple (n = 189, 92%) body regions (Table 4). Most women reported injuries to five out of nine regions (n = 47, 23%), followed by four regions (n = 45, 22%), three regions (n = 43, 21%), and six regions (n = 24, 12%). A relatively smaller number of women reported injuries to 1, 2, 7, 8, and 9 regions. Seven women (3%) reported no injuries. Additionally, physical examination data showed the largest average absolute area of injury was in the lower extremities. However, the average percentage of injured areas referenced to the segmental body surface area of adult North American women based on the US Environmental Protection Agency (US EPA, 2011) was highest in the head and neck region (over 6%).
Physical Injury by Examination (N = 205).
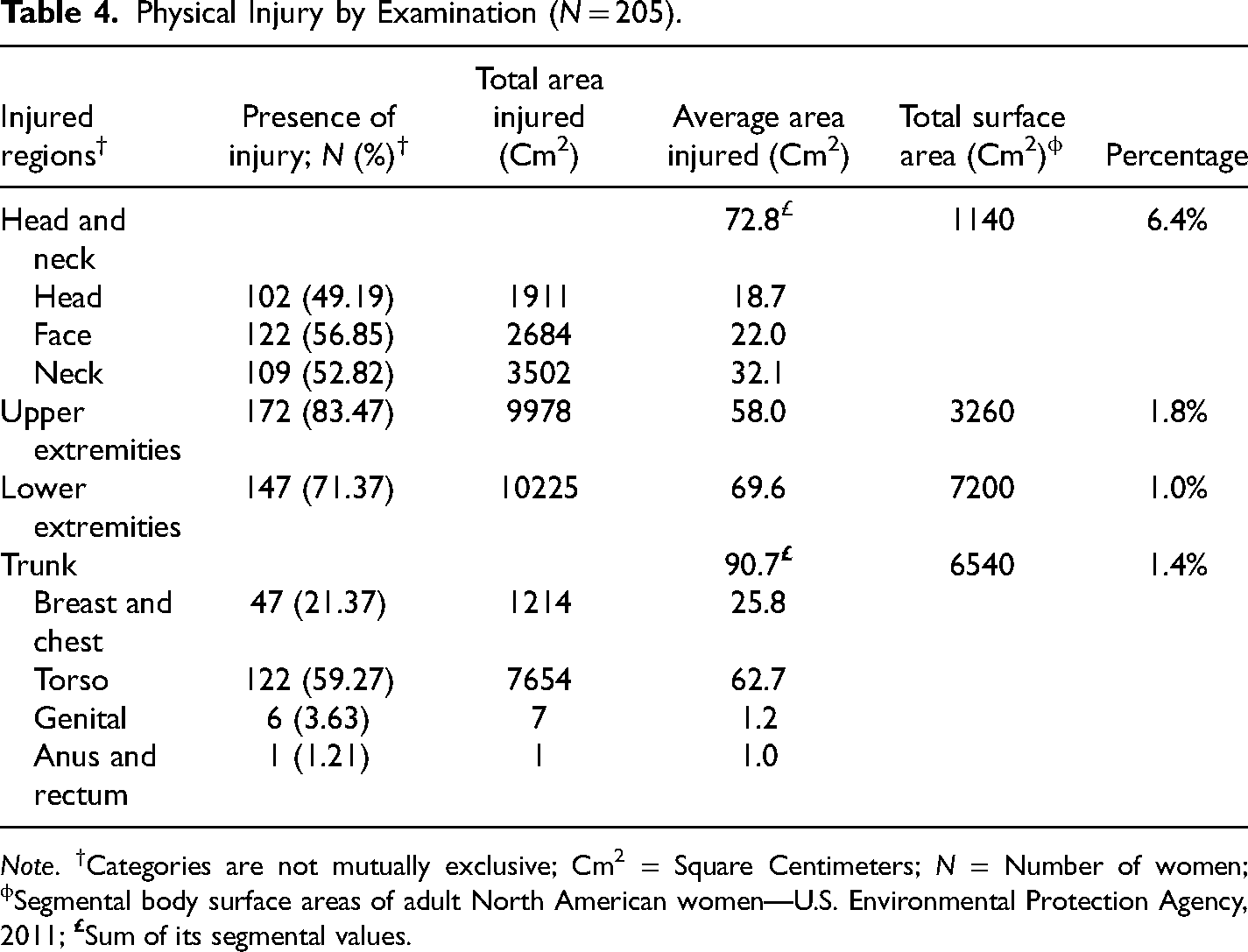
Note. †Categories are not mutually exclusive; Cm2 = Square Centimeters; N = Number of women; ϕSegmental body surface areas of adult North American women—U.S. Environmental Protection Agency, 2011;
Multistep multivariable logistic regression analysis demonstrated various relationships between different explanatory variables with disclosed symptoms and strangulation, adjusting for other covariates (Table 5). Women who reported strangulation were 2.24 times more likely to report BI-related symptoms (OR: 2.24, 95% CI: 1.12–4.50, p = .023) compared to those who reported no strangulation. Sexual assault, single versus multiple mechanisms of injury, age, weapon applied, history of a previous similar incident, head and neck area injured, and total surface area injured were not significantly related to disclosed symptoms (p > .05). In an analysis of a sub-group of women who reported strangulation, women who experienced LOC during strangulation were 3.87 times more likely to report BI-related symptoms compared to those who did not experience LOC (OR: 3.87, 95% CI: 1.50–9.93, p = .005). In another analysis of a subgroup of women who were assaulted using weapons, no significant relationship of strangulation, sexual assault, history of a previous similar incident and total area injured was found with disclosed symptoms. Furthermore, women who experienced strangulation were 3.07 times more likely to experience other mechanisms of injury in addition to strangulation (OR: 3.07, 95% CI: 1.08–8.71, p = .035) and 1.01 times more likely of having head and neck injury (OR: 1.01, 95% CI: 1.00–1.02, p = .042; Table 5). Additionally, multiple linear regression revealed women who were assaulted using a weapon had an average total injured area that was 119.96 cm2 larger (R2 = 0.081, 95% CI: 39.73–200.18, p = .004) compared to those who experienced an assault in which a weapon was not applied while adjusting for the covariates of sexual assaults, single versus multiple mechanisms of injury, strangulation, and history of previous similar incidents.
Multistep Multivariable Logistic Regression Examining Relationships of Different Explanatory Variables With Disclosed Symptoms and Strangulation.
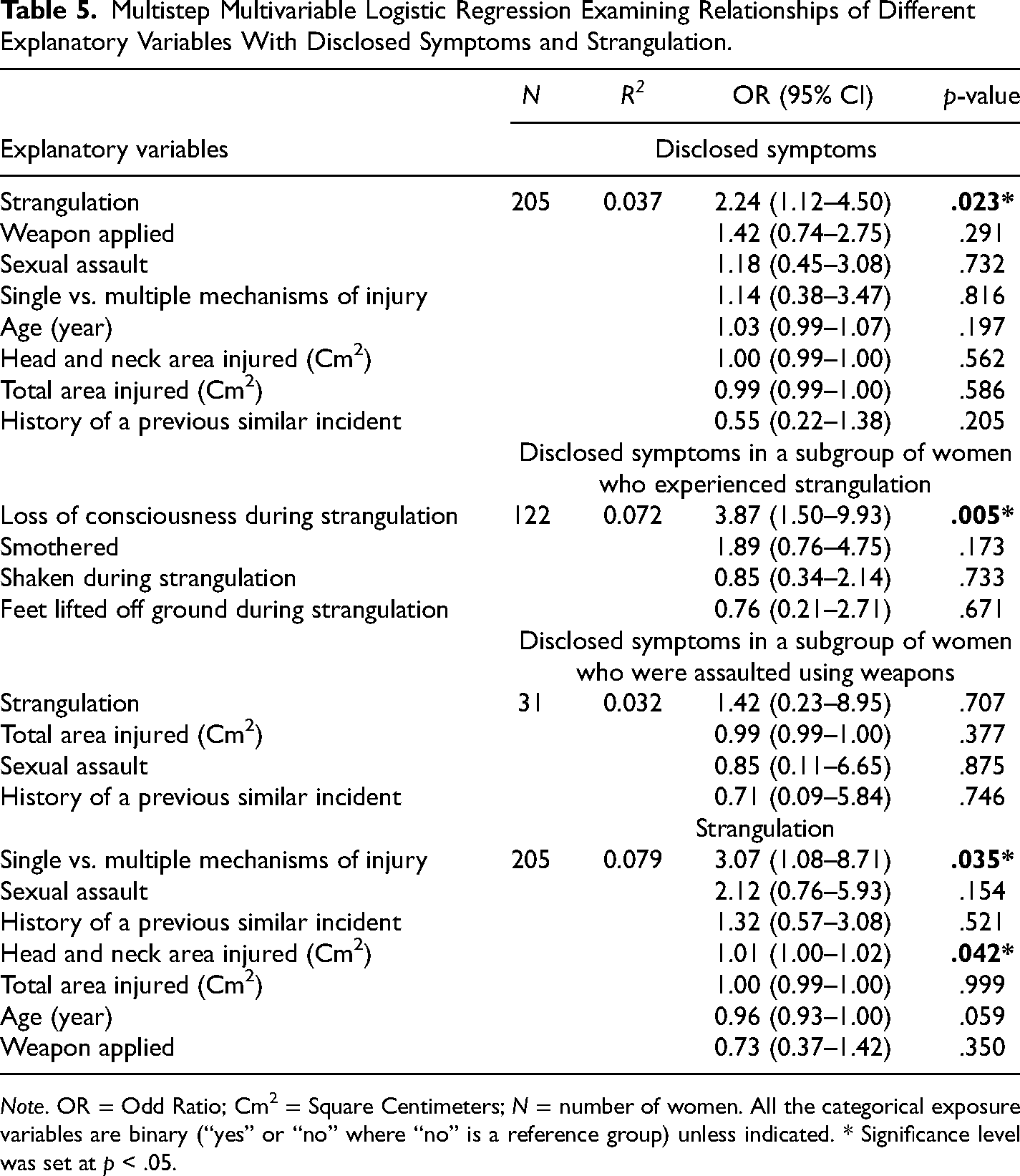
Note. OR = Odd Ratio; Cm2 = Square Centimeters; N = number of women. All the categorical exposure variables are binary (“yes” or “no” where “no” is a reference group) unless indicated. * Significance level was set at p < .05.
Discussion
In this retrospective chart review, approximately 58% to 91% of women presenting to the FNS reported a mechanism of injury (most common mechanisms: pushing, slapping, restraining, strangulation, and punching) resulting in symptoms consistent with BI. The prevalence of BI-related symptoms recorded in this chart review (32%) is likely an underestimation given BI-specific measures—other than LOC following strangulation—were not directly collected as part of the intake. More than 98% of women reported a mechanism of injury consistent with BI—either a direct blow to the head and/or strangulation. Four of the five most common mechanisms of injury (pushing, slapping, strangulation, and punching) may potentially cause BI. In addition, the AIC-related symptoms, sensory-motor impairments, and emotional disruptions disclosed by women in the acute state of injury are consistent with symptoms of BI. Lastly, women experiencing strangulation with or without head impacts reported higher rates of AIC compared to the women who reported only head impacts.
Our findings are broadly consistent with those reported by Ralston et al. (2019), which used a similar methodological approach. In the current study, the results from the physical examination showed that 97% of women had a visible injury and over 82% of women had an injury to the head and neck region with this region representing the largest relative proportion of the injured area. Such high rates of injury to the head and neck suggest probable BI in at least a subset of this sample. The symptoms disclosed were also consistent with those reported in two other retrospective chart reviews (Wong et al., 2014; Zieman et al., 2017), as well as the BI literature more broadly (Silverberg et al., 2020).
One important distinction to make is our results suggest the occurrence of possible BI, rather than its identification or diagnosis. Other than the specific question about LOC from strangulation, no BI-specific assessments were performed. Despite this limitation, the results of this study are consistent with existing literature (Ralston et al., 2019; Valera & Berenbaum, 2003; Valera et al., 2019), which has demonstrated a relationship between IPV and BI (Ralston et al., 2019). For instance, Zieman et al. (2017) conducted a retrospective chart review of 115 women who had been referred to a BI-specialized center from domestic violence and homeless shelters using the HELPS screening tool and found 88% sustained at least one BI. Valera and Berenbaum (2003) evaluated 99 women who had experienced IPV using the Brain Injury Severity Assessment (BISA) tool, and neuropsychological, psychopathological, cognitive functioning, and abuse history measures and found 74% of women sustained one BI and 51% of women sustained multiple BIs. This study provides additional evidence of possible IPV-caused BI in the acute phase following injury and supports the notion that women who have recently experienced IPV are at risk of sustaining BI. Approximately 32% of women in this study disclosed various BI-related symptoms. While this rate of symptom presentation appears low compared to the aforementioned studies, it is likely an underestimation given no BI-specific assessment tool was used. Additionally, women were not specifically probed about symptoms and experiences relating to BI. Thus, some women may have chosen not to disclose symptoms for a variety of reasons or the nurse did not document disclosures of symptoms. For example, twice as many women disclosed LOC resulting from strangulation when explicitly asked during the examination, compared to when they were asked to voluntarily disclose experiences of strangulation-related LOC. Therefore, it is possible the prevalence rate would be much higher if women completed a BI assessment tool, such as the BISA. The BISA was specifically developed for screening IPV-caused BI and explicitly asks about symptoms commonly reported by women, such as LOC, memory loss, dizziness or lightheadedness, blacking out, seeing stars, etc. Including an assessment tool specific to IPV-caused BI would likely increase the identification of potential BI and facilitate a pathway to referral and prompt medical follow-up.
More than half of the women (60%) experienced strangulation with or without head impacts. Almost 40% of women who experienced strangulation disclosed symptoms, which is almost double those who disclosed symptoms without having experienced strangulation (22%). Additionally, a positive significant association was found between experiences of strangulation and disclosed symptoms indicating possible anoxic-hypoxic injuries (Armstrong & Strack, 2016). Furthermore, symptoms such as dizziness, difficulty breathing, difficulty swallowing, headache, and pain around the neck reported by the women are in line with strangulation-related hypoxic-anoxic injuries (Ralston et al., 2019; Valera & Berenbaum, 2003).
Women who experienced strangulation were more likely to have been assaulted through multiple mechanisms and were more likely to report symptoms that are consistent with BI. This aligns with studies showing strangulation is a risk factor for severe physical IPV and future homicide (Glass et al., 2008). Beyond physical trauma, women experiencing strangulation also tend to have serious psychological problems (Myhill & Hohl, 2019). Close to 17% of women who disclosed emotional disruptions in this review indicated psychological challenges in line with this evidence.
The limitations of this study primarily included subjective information drawn from the narrative women provided and questionnaires on clinical characteristics. In the sample of 857 women who visited the FNS due to domestic or partner violence, the records of only 247 women aged over 16 years were available to review. Therefore, we could not provide the exact statistics on what percentage of IPV incidents resulted in a forensic nursing examination. We could not use any software or specific protocol or audit process or coding system to collate the data, which is another limitation of the study. Due to the lack of IPV-caused BI-specific measures and the retrospective nature of the study, these women could not definitively be identified as having BIs. However, the reported symptoms, mechanisms of injury, and characteristics of the violence indicated possible BI and suggest the use of appropriate BI assessments during forensic nursing examinations is warranted. Based on these observations, several recommendations are made below that could improve the ability of BIs to be detected in the context of forensic nursing examinations and those providing medical care for women of IPV.
Recommendations
Include a Screening Assessment of BI and Document BI-Related Symptoms
Including an assessment of BI wherever possible will increase the odds of detecting probable BI and help with referrals to physicians/nurse practitioners who will then be able to provide needed medical care, treatment, and/or support for women experiencing IPV. In this study, it was noted women were more likely to disclose symptoms related to BI if they were prompted directly compared to when they were asked to do so voluntarily. Several reasons may account for this. First, it is possible the time to build rapport between the forensic nurse and patient means women are more likely to disclose their symptoms closer to the end of the appointment (which is when they were prompted). Second, it is possible common psychosomatic symptoms related to BI, such as memory problems, may not be considered a high priority compared to physical injuries or more severe symptoms. This is understandable given the wide range of injuries reported in this retrospective review. In addition, this wide-ranging set of experiences and symptoms related to BI highlights the heterogeneous nature of BI and contributes to the challenges of detecting BIs. Third, it is also possible women assume these symptoms are not due to a physical injury, but rather to the stress related to experiencing IPV. While BI symptoms often overlap with mental health disorders, such as anxiety, depression, and post-traumatic stress disorder (Campbell et al., 2018; Valera et al., 2019; Valera & Kucyi, 2017; Zieman et al., 2017), it is essential to screen for potential BI to provide the medical referrals necessary for appropriate care, resources, and supports.
Ideally, a short, reliable, and validated BI screening tool designed specifically for the context of IPV should be used. However, validation of IPV-caused BI screening tools, such as the BISA (Valera & Berenbaum, 2003) is still underway. Other potential tools include the “HELPS” (Picard et al., 1991) or the modified version of the “HELPS,” which is termed “HELP” (Rajaram et al., 2021) and CHATS (ODVN, 2019), each of which provides a rapid assessment of potential BI by screening for previous injuries to the head, and cognitive, physiological, or affective symptoms related to BI. Although the HELPS tool was not designed specifically for IPV, it has been previously used to screen for IPV-caused BI (Hartwig, 2013; Zieman et al., 2017). By contrast, although it has not yet been validated, the CHATS tool was designed for the context of IPV-caused BI and has the advantage of asking specifically about incidents of strangulation, and the resulting risk for hypoxic-ischemic BI (ODVN, 2019). Short of incorporating a separate screening tool, it may be sufficient to update current forensic charts to include a question about BI-related symptoms. Such a list could resemble the one included in the Sports Concussion Assessment Tool 5 (Echemendia et al., 2017)—a standardized tool for the evaluation of sports-related concussions. It includes various on-field assessments including a memory test and off-field assessments including symptoms evaluation, and cognitive, and neurological screening. These practices may increase referral and follow-up medical care success by providing important information about the patient's acute response to the violent incident.
Improve Referral System for Survivors of IPV with Probable BI for Further Support and/or Management
We must emphasize the importance of improving the referral pathway for survivors of IPV to access further support and resources. As mentioned in the first recommendation, an assessment of BI is essential to provide BI-specific care, resources, and support. As such, a referral network that connects women to the appropriate expert(s) is essential. Following a positive screening for potential BI, women should be referred to an appropriate healthcare provider such as a nurse practitioner or physician for assessment and diagnosis. This referral system should ideally include a trauma- and violence-informed clinician with expertise in BI for potential diagnosis and referral to other health services, such as physical or occupational therapy, as needed.
Ultimately, improving screening for BI and documenting symptoms immediately following an IPV incident may help facilitate the pathway to referral, diagnosis, and support. Women who have experienced IPV are not typically aware they may have suffered one or more BIs as a result. Such knowledge can help validate and legitimize the challenges they have faced but not fully understood (Ivany et al., 2018). Such benefits should be contextualized within the sociocultural and legal-ethical environment. Ongoing work from our group (Boyle et al., 2022) suggests BI screening has the potential to be weaponized in family law parenting disputes as a means to undermine and minimize the perception of a mother's ability to parent. As such, the potential benefits of BI screening must be carefully measured against possible harms. This may also highlight the importance of follow-up and ongoing medical care for those who have experienced BI to better demonstrate prognosis.
Conclusion
A large majority of women presenting to an acute forensic nursing service reported strangulation, punching, slapping, and pushing either alone or in combination resulting in symptoms consistent with BI. The rate of BI-related symptoms recorded in this chart review is likely an underestimation given that BI-specific measures—other than LOC following strangulation—were not directly collected as part of the intake. Women experiencing strangulation with or without head impacts reported higher rates of AIC compared to the women who reported head-only impacts. Women experiencing IPV are prone to BI, therefore, BI screening is warranted during the examination; which could ultimately support the early management of BI and help to minimize the cumulative effects of repeated BIs and chronic symptoms. Such efforts could support a survivor's ability to thrive, parent, work, have a higher quality of life, and have healthy relationships and ultimately break free from the cycle of abuse.
Footnotes
Acknowledgements
The authors thank the clients and staff at the Embrace Clinic and Forensic Nursing Service, Surrey Memorial Hospital in the Fraser Health Authority in British Columbia, Canada.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received funding from the Department of Women and Gender Equality Gender-Based Violence Program to support this research (grant number 62R01998).