
Abstract
Women have experienced increased rates of intimate partner violence (IPV) since the onset of the COVID-19 global pandemic, and at the same time requirements for physical distancing and/or remote delivery of services have created challenges in accessing services. We synthesized research evidence from 4 systematic reviews and 20 individual studies to address how IPV interventions can be adapted within the context of the pandemic. As many interventions have been delivered via various technologies, access to technology is of particular importance during the pandemic. Our results can inform the provision of services during the remainder of the COVID-19 pandemic including how to support women who have little access to in-person services.
Introduction
The message “Go home and stay home” has been a consistent narrative from many elected leaders and public health officials during times when COVID-19 case numbers are high in their jurisdictions. During the COVID-19 pandemic, many women who are experiencing intimate partner violence (IPV) have had greater periods of isolation at home with abusers, and/or are at risk of IPV due to increased stress on individuals and families. Evidence from the World Health Organization shows that violence against women often increases during every type of emergency, and especially during global crises such as the COVID-19 pandemic (World Health Organization, 2020). A recent systematic review of 18 studies from the United States and 8 additional countries reported an increase in reports of domestic violence since stay-at-home or lockdown orders related to COVID-19 were implemented (Piquero et al., 2021). Intimate partner violence can have a detrimental impact on women including physical, mental, and sexual health problems (Bonomi et al., 2006; Ulloa & Hammett, 2016), and studies have begun to emerge documenting these impacts specifically related to COVID-19 (Sediri et al., 2020).
We define IPV as any type of abusive behavior (e.g., emotional, verbal, physical, sexual) that occurs between current or former intimate partners, such as spouses or those in romantic relationships. IPV is the most common form of violence that women experience; women account for 80% of those who experience IPV and 84% of IPV occurs in a private dwelling (Conroy et al., 2019). IPV among women is a problem that persists regardless of socioeconomic class, religious affiliation, race, ethnicity, or age (Rennison & Rand, 2003), although certain groups can be disproportionately affected (Steele et al., 2020).
IPV services are commonly offered in-person (e.g., individual and group counseling and support) and/or involve physically moving to short- and long-term protective housing (e.g., emergency shelters, second-stage housing) (Weeks et al., 2021). Due to the COVID-19 pandemic, many of these supports were diminished due to public health restrictions and regulations. This resulted in many organizations being unable to provide in-person services at their full capacity, if at all, due to challenges related to physical distancing within these settings (Bogart, 2020; Enright, 2020). There is increased research evidence about IPV services offered using information and communication technologies, such as videoconferencing and telehealth (Goldstein et al., 2017; Rempel et al., 2019), but women experiencing IPV may not have access to technology or have the ability to safely use technology, especially if their abuser is at home for prolonged periods (Zaidi et al., 2015). Our team synthesized research evidence about how IPV services can be effectively and safely delivered within the context of the COVID-19 global pandemic.
Through a preliminary literature search, we identified two relevant and interconnected bodies of research knowledge related to COVID-19: (1) the use of information and communication technologies in the provision of IPV services (El Morr & Layal, 2019; Ford-Gilboe et al., 2017; Hassija & Gray, 2011; Murray et al., 2015; Westbrook, 2007; Zaidi et al., 2015) and (2) research on the provision of IPV services that do not require in-person contact with diverse populations living in rural and/or remote contexts in both high and low-resource countries (Hughes, 2010; Neill & Hammatt, 2015; Shepherd, 2001; Strand & Storey, 2019; Wild et al., 2019; Zorn et al., 2017).
We conducted a search of PROSPERO, MEDLINE, the Cochrane Database of Systematic Reviews, and in addition the JBI Database of Systematic Reviews and Implementation Reports, and no current or in progress systematic reviews were identified that specifically focused on providing IPV services during the COVID-19 pandemic. The PROSPERO database includes a specific filter for registrations related to COVID-19. One rapid review that was ongoing at the time of our search, and recently completed, focused on the associations between social and geographical isolation and IPV, although not specifically focused on services provided during the COVID-19 pandemic (Mojahed et al., 2021). A recently completed rapid scoping review focused on interventions to promote gender equality in public health emergencies, such as economic empowerment, health promotion, and resettlement programs (Steinert et al., 2021).
To support the adaption of supports and services during the COVID-19 pandemic, we synthesized available research evidence to address the following primary research question: How can IPV services/interventions for women across the lifespan be adapted within the context of COVID-19 where physical distancing and/or remote delivery of services are required? In addition to the existence of services that can be adapted within the COVID-19 context, it is also important to identify if these services have a positive impact on women's lives and if women are willing and able to use these services. Thus, we also addressed two secondary questions in this review: What evidence exists for the impact of the identified services on the health and safety needs of women? What evidence exists for the feasibility and acceptability of the services identified?
The results of this review will inform the adaption and expansion of services during the remainder of the COVID-19 pandemic and any other situations that require physical distancing and/or remoted delivery of services. In addition, the results may inform further innovations in providing IPV services for people who do not wish to access in-person service delivery even when physical distancing measures are not in place, or who cannot access in-person services for various reasons (e.g., people living in rural and remote places where in-person services are limited).
Theoretical Perspectives
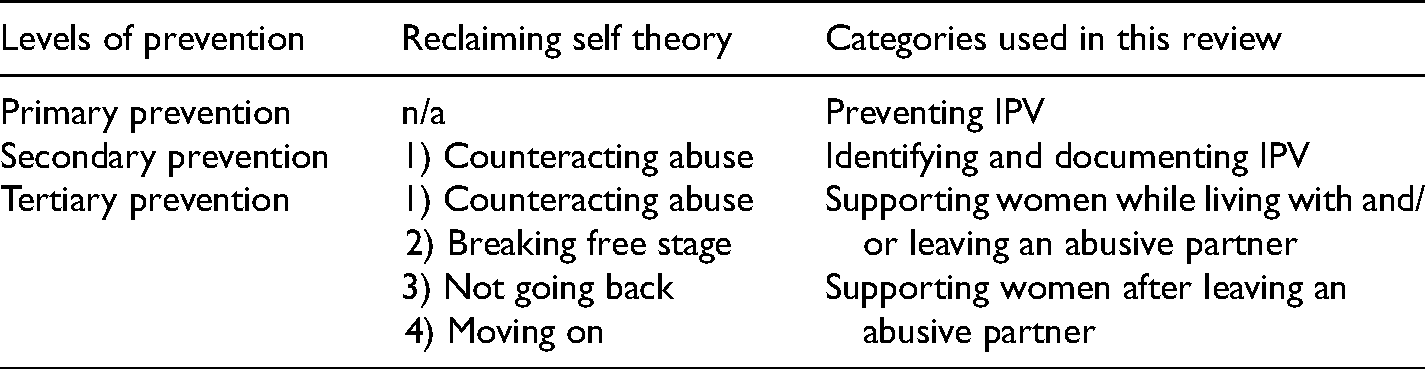
The categories used to organize the interventions included in this review were developed from two theoretical perspectives: (1) levels of prevention (i.e., primary, secondary, and tertiary; Issel, 2014; Weiss & Koepsell, 2014) and (2) reclaiming self-theory (Merritt-Gray & Wuest, 1995; Wuest & Merritt-Gray, 1999, 2001). Both theoretical perspectives have been recently utilized to organize IPV interventions in systematic reviews (Anderson et al., 2021a; Rempel et al., 2019).
Primary, secondary, and tertiary levels of prevention have been utilized broadly to conceptualize various forms of interventions, often related to health promotion (Issel, 2014). These levels are used to identify how to prevent a problem from occurring and addressing underlying causal factors (i.e., primary prevention), screening and early detection to implement early interventions to reduce impact and/or recurrent exposure (i.e., secondary prevention), and mitigating the impacts of current or previous experiences of IPV (i.e., tertiary prevention).
Reclaiming self-theory (Merritt-Gray & Wuest, 1995; Wuest & Merritt-Gray, 1999, 2001) has four stages: (1) “counteracting abuse” where women tend to relinquish valued parts of their self-identity, minimize their abuse, and fortify their defences to leave the relationship; (2) “breaking free” where women physically leave the relationship; (3) “not going back” to the abusive relationship; and (4) “moving on” stage after leaving an abusive relationship.
We utilized the levels of prevention and reclaiming self-theory (e.g., the specific stages women go through in leaving an abusive partner) to develop the four categories used in this review to organize interventions: preventing IPV; identifying and documenting IPV; supporting women while living with and/or the process of leaving an abusive partner; and supporting women after leaving an abusive partner.
Methods
We adapted Joanna Briggs Institute (JBI) systematic review methodology for conducting umbrella reviews (i.e., reviews of reviews) and mixed-methods reviews (Aromataris et al., 2020; Aromataris & Munn, 2020; Peters et al., 2020). JBI is a not-for-profit research institute located at the University of Adelaide and the mission is to facilitate the synthesis, transfer, and implementation of the best available evidence to ensure the feasibility, appropriateness, meaningfulness, and effectiveness of policy and practice related to health (www.jbi.global).
Inclusion Criteria
In this review, we included empirical research of IPV interventions that could be advantageous within the context of the COVID-19 pandemic, such as interventions utilizing physical distancing or remote delivery of services, many of which involve utilizing information and communication technologies. Sources included quantitative and qualitative study designs including published peer-reviewed studies, systematic reviews, and theses and dissertations. We also included media reports of IPV interventions developed or adapted since the onset of the COVID-19 pandemic, but these results were reported separately from the current article (Weeks et al., 2020). Due to the language capacity of our research team, only sources published in English or French were included. We included studies that included IPV interventions provided to women, and those who identify as women; we did not include studies focused specifically on girls.
Search Strategy
An initial limited search of MEDLINE, CINAHL, and Embase was undertaken followed by an analysis of the text words contained in the title and abstract, and of the index terms used to describe the article. A second search using all identified keywords and index terms was undertaken across all included databases CINAHL, MEDLINE, Gender Studies Database, Embase, PsychInfo, and NexisUni (media reports). The final search strategy of the databases was conducted in May 2020, except for NexisUni conducted in June 2020. Sources published since the inception of databases were included.
Study Selection
Following the implementation of the search strategy, all identified citations were collated and uploaded into Covidence systematic review software (Veritas Health Innovation, Melbourne, Australia) and duplicate were removed. Titles and abstracts were then screened by two independent reviewers against the inclusion criteria for the review. The full text of sources was retrieved for potentially relevant studies. Two independent reviewers assessed the full text of selected citations against the inclusion criteria. Reasons for the exclusion of full-text studies that did not meet the inclusion criteria were recorded. Any disagreements that arose between the reviewers at each stage of the study selection process were resolved through discussion, or with a third reviewer. The results of the search are presented in a Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) flow diagram (Page et al., 2021).
Data Extraction
The data extracted included specific details about the study characteristics including the study methods and key findings. We extracted any data included in the studies related to the impact of the interventions on mental well-being, physical health, and safety needs of women. We also extracted results related to the feasibility and acceptability of interventions. The data extraction tool was developed by the research team and pilot tested by having multiple reviewers completing data extraction and discussing the results at a virtual team meeting. Following established practices (Pandor et al., 2019; Tricco et al., 2017), one reviewer extracted all descriptive data from each included source (e.g., describing the interventions, study methods, sample characteristics), and the first author reviewed and verified these data. Two independent reviewers extracted data for all quantitative and qualitative outcome data (e.g., health impacts of interventions, feasibility, acceptability). Any disagreements between the reviewers were resolved through discussion, or with a third reviewer.
Results
The results have been divided into two sections. In the first section of the results, we include a description of the results of the search and the included studies. In the second section of the results, we include results about the outcomes of the interventions from the included studies.
Search Results and Description of the Included Studies
In this section, we include the search results, characteristics of the included studies, characteristics of the interventions in the included studies, and our theoretical categorization of the interventions.
Search Results
A total of 10,788 titles were identified. Of these, 4,266 were duplicates. At the title and abstract screening phase, 6,522 sources were screened, with 6,245 sources were found irrelevant. A total of 277 sources were assessed for eligibility through full-text screening, and 199 were excluded (see Figure 1). Common reasons for exclusion included the intervention was not relevant to COVID-19 (n = 60) and/or the source did not include a report of an intervention (n = 48). We also excluded 36 sources at the full-text review stage if an individual study was included in one of the 4 systematic reviews included in our review. The search results reported in Figure 1 include media reports. The media reports included descriptions of initiatives to support women experiencing IPV since the onset of the COVID-19 pandemic. The results of 51 media reports were synthesized and published separately from the other sources in this review as they were not empirical sources (Weeks et al., 2020). In this article we include a synthesis of 4 systematic reviews and 20 individual studies.
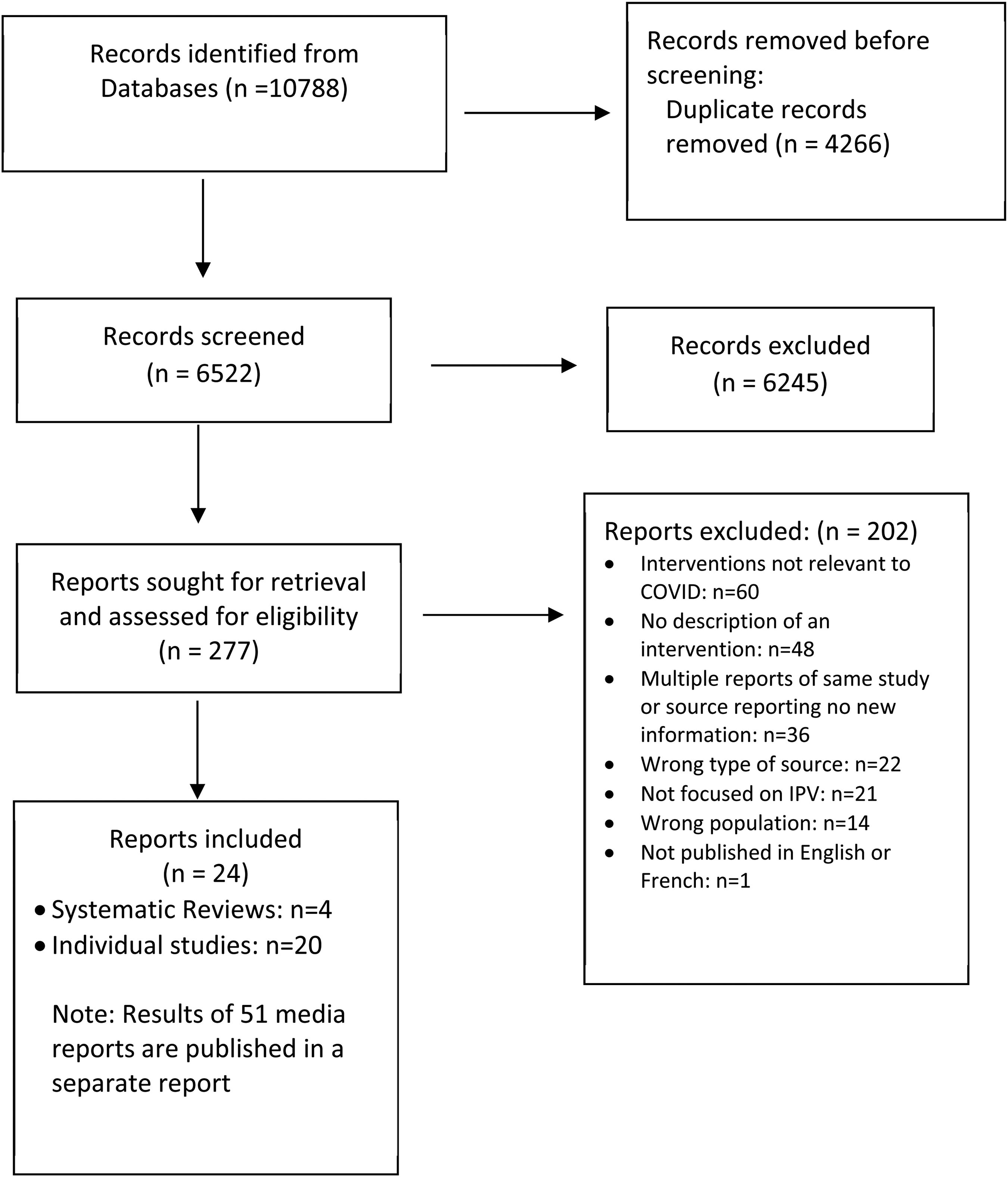
PRISMA diagram (Page et al., 2021).
Study Characteristics
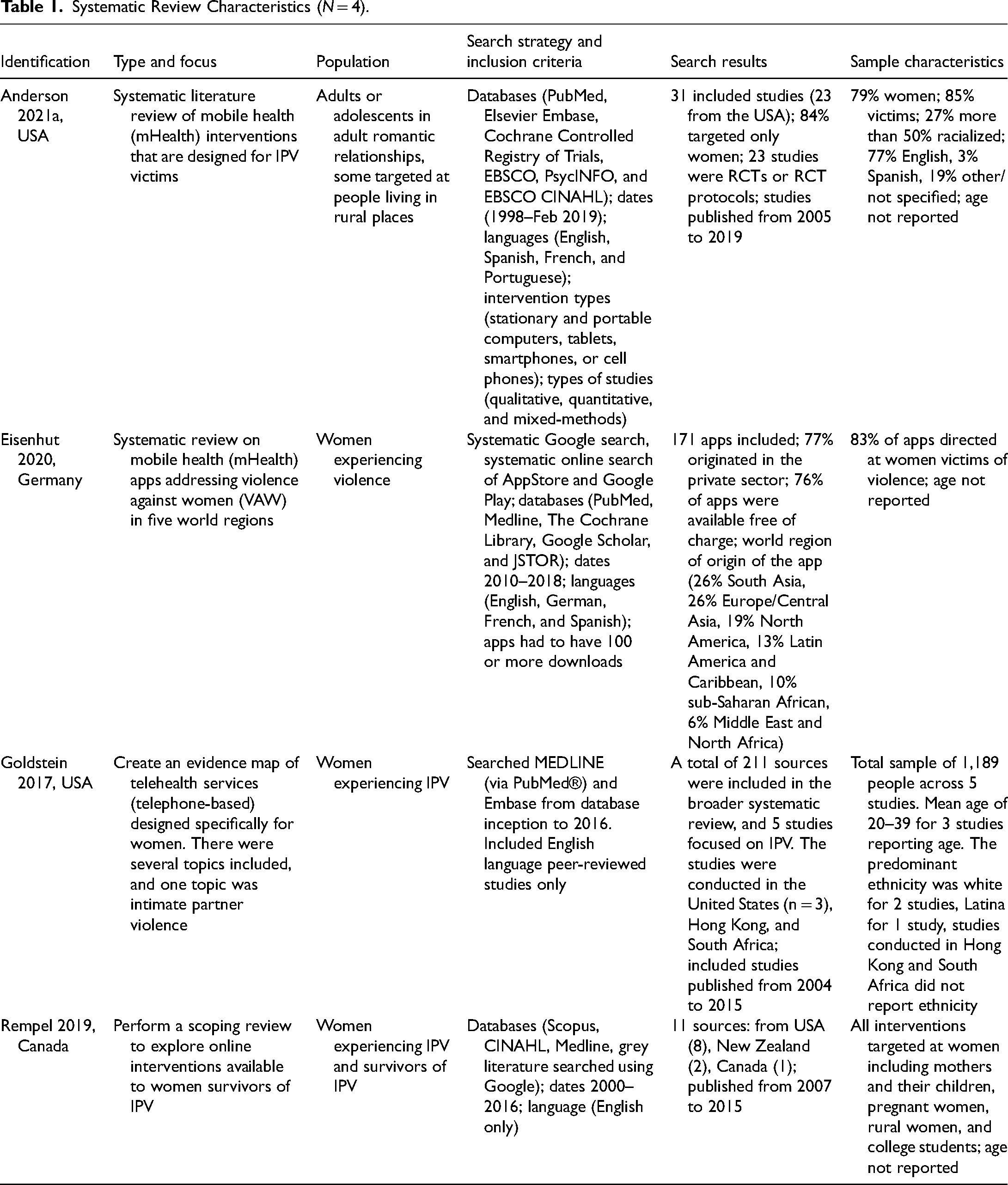
The characteristics of the 4 systematic reviews are included in Table 1 (Anderson et al., 2021a; Eisenhut et al., 2020; Goldstein et al., 2017; Rempel et al., 2019). These studies were published between 2017 and 2020 by authors in the United States, Canada, and Germany. The sources included in the systematic reviews were published from 2000 to 2019.
Systematic Review Characteristics (N = 4).
The characteristics of the 20 individual studies are included in Table 2. Most (n = 16) of these studies were published from 2015 to 2020 with the remainder published from 1998 to 2011 (n = 4). The individual studies were published by authors located in the United States (n = 14), with others published by authors in Canada (n = 2), Australia (n = 2), Hong Kong, and Tanzania. Most were published in peer-reviewed journals (n = 15), and the remainder were doctoral dissertations (n = 3), or studies published as book chapters (n = 2). The research designs of the individual studies varied greatly including randomized controlled trials and quasi-experimental designs (n = 5), other quantitative designs (n = 2), mixed methods (n = 7), and qualitative approaches including case studies (n = 6).
Characteristics and Results of Individual Studies by Category (N = 20).

Intervention Characteristics
Each of the 4 systematic reviews addressed technology-mediated interventions including a total of 218 sources focused on mobile health, telehealth, online tools, and digital applications (apps) targeting women experiencing violence. Three of the systematic reviews included published research (Anderson et al., 2021a; Goldstein et al., 2017; Rempel et al., 2019), and Eisenhut and colleagues (2020) conducted a systematic review of apps addressing violence against women in the five World Bank regions through searching various sources including Google, the AppStore, and Google Play (Eisenhut et al., 2020).
The characteristics of the interventions reported in the 20 individual studies varied greatly. In each of these studies, the researchers examined a unique intervention. Most involved some form of service delivery via technologies such as online apps, texts, social media, online discussion forums, and websites (e.g., Alvarez et al., 2018; Anderson et al., 2021b; Bacchus et al., 2016; Cameron, 2011; Chu et al., 2021; Doherty, 2017; Draucker et al., 2019; Fiorillo et al., 2017; Ford-Gilboe et al., 2017; Glass et al., 2017; Hatch et al., 2020; Khaki, 2016; Ross & Aitken, 2022). Other studies looked at individual psychotherapy and supports that were delivered via videoconferencing or by telephone (Burge et al., 2017; Chidanand, 2014; Gondolf, 1998; Steinmetz & Gray, 2017; Tschirch et al., 2006). One intervention in Tanzania utilized information and an educational program delivered by radio (Abeid et al., 2015). One intervention involved an innovative emergency shelter model relevant to the COVID-19 pandemic context as it involved supporting women and children in separate smaller residences versus larger more communal shelters (McDonald & Green, 2001).
Theoretical Categorization of Interventions
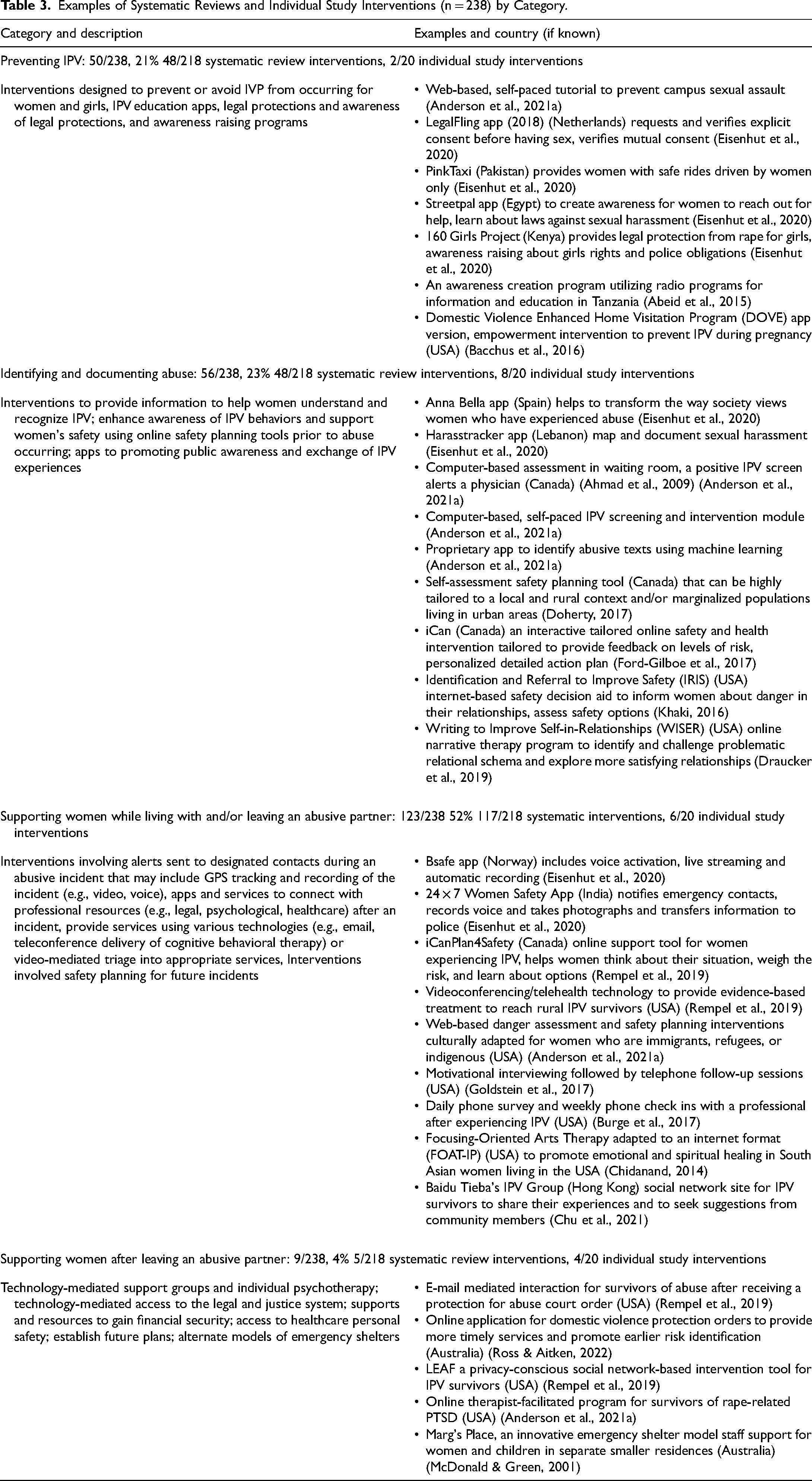
In Table 3, we included a summary of the interventions included in the systematic reviews and individual studies along with key examples of interventions representing each of the four categories we developed to organize the interventions. Approximately one-fifth of the interventions focused on preventing IPV from occurring. Many of these interventions were apps focusing on avoidance and education that were developed and implemented around the world (e.g., Eisenhut et al., 2020). Approximately one-quarter of the interventions focused on identifying and documenting IPV facilitated by various forms of technologies to understand and recognize IPV incidents, and to track and share information about IPV incidents. Just over one-half of the interventions focused on supporting women while living with and/or leaving an abusive partner. These interventions spanned the needs of women in reporting incidents, accessing professional resources, and safety planning. Very few (4%) interventions focused on supporting women after leaving an abusive partner.
Examples of Systematic Reviews and Individual Study Interventions (n = 238) by Category.
Intervention Outcomes
In this section, we include results on the health and safety outcomes followed by results about the feasibility and acceptability of the interventions from the included studies.
Health and Safety Outcomes
The authors of three of the systematic reviews reported results related to health and safety outcomes for women. In the Anderson and colleagues review (2021a), several studies found no significant differences between groups while others showed significantly less decisional conflict and uncertainty, improved mental health, reduced IPV exposure, and significantly less male-perpetrated aggression after one year. The lack of standardization of measurement tools across studies was a challenge in understanding experiences of IPV.
In the scoping review conducted by Rempel and colleagues (2019), some individual outcomes of the studies were reported including decreased anxiety, depression, and anger and increased personal and social support. Goldstein and colleagues (2017) did not report the outcomes of the interventions, but they reported that all outcomes focused on patient-level variables such as mental health and safety-promoting behaviors. One individual study in the Goldstein review (Tiwari et al., 2010) included an intervention involving a 30-min empowerment session and telephone calls once a week for 12 weeks and 24-h access to a hotline that resulted in significantly reduced depression and psychological aggression, improvement in perceived social support and the use of safety-promoting behaviors.
All of the 20 individual studies indicated some positive outcomes of the interventions for the health and safety needs of women although the findings in quantitative studies did not always reach statistical significance. Several researchers attributed positive outcomes to providing highly tailored interventions, such as providing feedback based on the women's individual responses to questions (e.g., Doherty, 2017; Ford-Gilboe et al., 2017).
In Table 4, we include a summary of the health and safety outcomes measured in the five individual experimental studies in our review organized by type of outcome. Few outcome measures were used consistently across studies, other than the utilization of the Centre for Epidemiologic Studies Depression Scale across three studies (Ford-Gilboe et al., 2020; Glass et al., 2017; Hatch et al., 2020). There were only a few statistically significant differences reported between the intervention and control groups. A 6-week internet-based safety decision aid intervention offering tailored feedback and safety plans resulted in the intervention group being statistically more likely to have reduced decisional conflict, improved usage of IPV strategies, and greater likelihood to end the abusive relationship (Glass et al., 2017). Abeid and colleagues (2015) found that their awareness program utilizing radio programs in Tanzania resulted in a statistically significant improvement in correct knowledge about violence and abuse.
Health and Safety Outcomes: Experimental Studies.
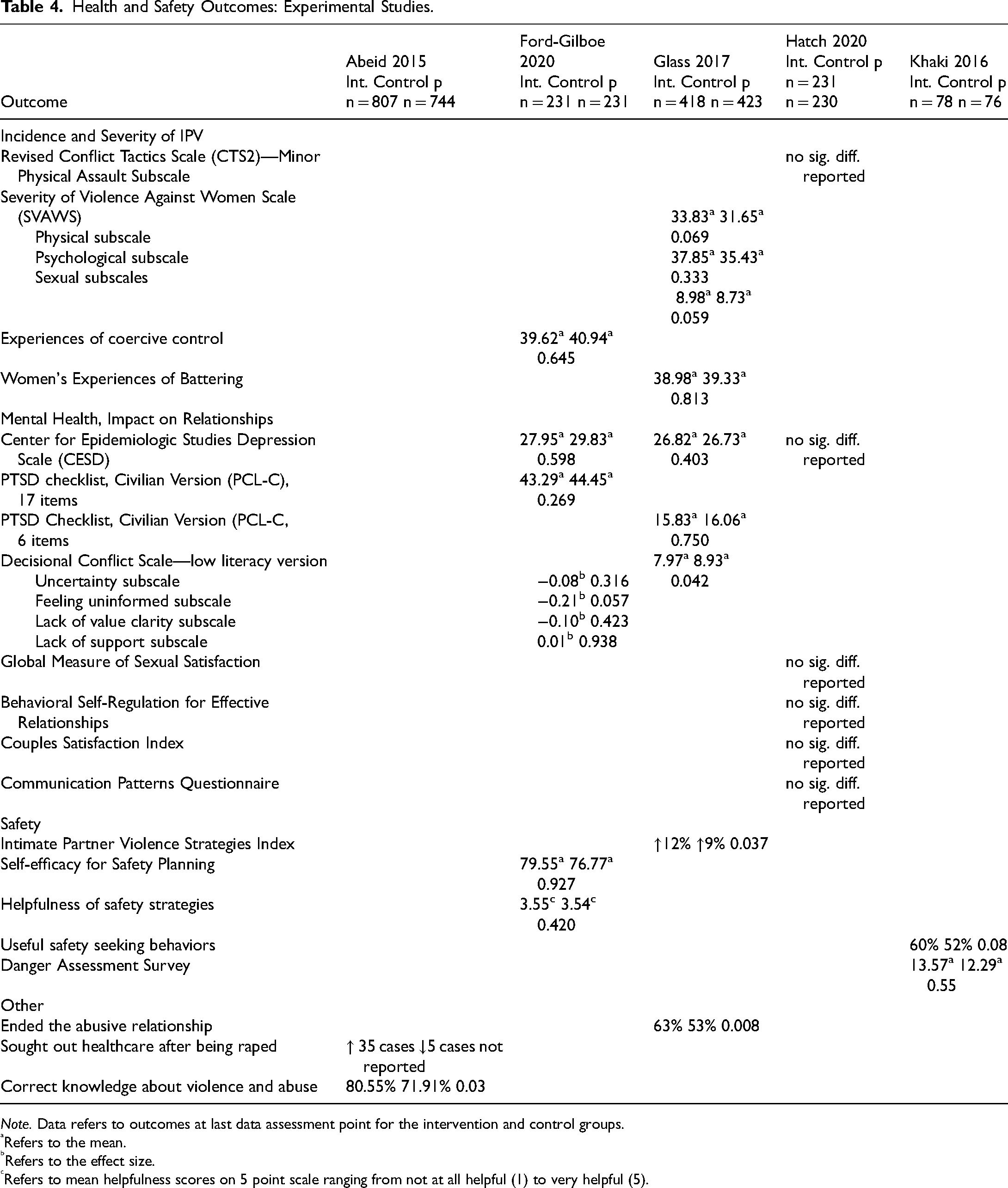
Note. Data refers to outcomes at last data assessment point for the intervention and control groups.
Refers to the mean.
Refers to the effect size.
Refers to mean helpfulness scores on 5 point scale ranging from not at all helpful (1) to very helpful (5).
In some studies, the researchers reflected on why expected and/or significant results were not found, such as needing a greater focus on intervention fidelity to ensure that the interventions were delivered consistently across participants (e.g., Hatch et al., 2020). Additional issues identified that may have affected expected intervention outcomes included participant literacy level (Alvarez et al., 2018; Anderson et al., 2021b), small sample size (Chidanand, 2014; Khaki, 2016), study samples lacking diversity, such as ethnic or racial diversity (Anderson et al., 2021b; Khaki, 2016), and access to technology (Bacchus et al., 2016).
Intervention Feasibility and Acceptability
Minimal evidence related to feasibility and acceptability was included in the four systematic reviews. In the Anderson and colleagues (2021a) review, attrition from studies that reported noncompliance (n = 19 studies) ranged from 4% to 36% (median = 15%) with computer-mediated interventions showing the highest rate of dropout. A small number of non-experimental studies did report strong interest in mHealth for IPV prevention (Anderson et al., 2021a). In several studies included in Rempel and colleagues (2019), participants reported positive results related to feasibility and acceptability. Eisenhut and colleagues (2020) reported that 77% of the apps originated in the private sector and 76% of the apps were available free of charge.
In the 20 individual studies, various aspects of feasibility and acceptability of the interventions were reported including intervention completion rates, value and satisfaction, and increased access to interventions. There were quite high levels of intervention completion rates across the experimental studies. Studies utilizing other designs also showed low attrition rates, such as 84% of participants completing all four web-based multimedia sessions (Fiorillo et al., 2017) and 74% of participants completing all aspects of a videoconference program involving assessment and three to four psychiatrist consultations (Tschirch et al., 2006). Conversely, few participants in a telephone counseling intervention participated in more than one offered session (Gondolf, 1998).
The value and satisfaction with the interventions were assessed in several ways. General results of usefulness and applicability were found across several studies (Anderson et al., 2021b; Chidanand, 2014; Chu et al., 2021). Several studies reported improved awareness of services and knowledge about IPV (Abeid et al., 2015; Alvarez et al., 2018; Bacchus et al., 2016; Cameron, 2011). The System Usability Scale was utilized to determine that a web-based multimedia intervention fell within the “good” range (Fiorillo et al., 2017). Participant satisfaction was assessed in a few studies, such as Fiorillo and colleagues (2017) who found a high level of satisfaction measured with the Client Satisfaction Questionnaire (CSQ). Hatch and colleagues (2020) assessed satisfaction with, and perceived utility of, a text-based relationship intervention. The participants read more than 70% of the messages they received. While they felt the messages encouraged them to be more mindful, provided good insight, and were helpful, they were less likely to agree that the content helped them make positive changes in their relationships or that they would recommend the intervention to their friends.
Some interventions provided increased access to interventions for women with specific characteristics, such as women living in rural or remote places (Abeid et al., 2015; Bacchus et al., 2016; Doherty, 2017; McDonald & Green, 2001; Ross & Aitken, 2022; Steinmetz & Gray, 2017). In some cases, the interventions specifically provided enhanced privacy and anonymity (e.g., Alvarez et al., 2018; Bacchus et al., 2016). Several sources were inclusive of women of various ethnic and racial backgrounds and nationalities, but only a few studies specifically compared results from different groups, such as African Americans and non-Hispanic White Americans (Khaki, 2016) or focused on a specific group, such as South Asian women living in the United States (Chidanand, 2014). One challenge identified was a high level of literacy needed to participate in the intervention (Anderson et al., 2021b).
Discussion
In this review, we synthesized evidence from four systematic reviews and 20 individual studies that primarily utilized various forms of technology that could be implemented in the COVID-19 pandemic context. Many of these interventions can also provide greater access to services for women who have little access to in-person services, women living in rural and remote places, and for women who do not wish to utilize in-person interventions. Due to the implementation of our search strategy in May 2020, it is not surprising that we did not identify reports of research studies evaluating the impact of interventions since the onset of COVID-19. However, the interventions are relevant to the COVID-19 pandemic context due to the characteristics of the interventions.
In a separate component of our research, we conducted a search of media reports of IPV interventions developed or adapted since the onset of the COVID-19 pandemic to June 2020 (Weeks et al., 2020). Most interventions we identified were reports of technology-mediated services, including various apps. Importantly we identified interventions that supported women experiencing many forms of IPV beyond physical abuse, such as initiatives to support information technology security skills. We recognize that additional interventions have been developed or adapted since June 2020, especially those related to new forms of technologies, and evaluations of these interventions are needed.
The categories we developed were useful in organizing IPV interventions. Many interventions fit into the category of supporting women while living with and/or leaving an abusive partner. While the theory of reclaiming self (Merritt-Gray & Wuest, 1995; Wuest & Merritt-Gray, 1999, 2001) divides this category into counteracting abuse and breaking free, this period can be a long process for many women, and evidence reveals that many women return to an abusive partner several times before breaking free (Anderson, 2003). Also, many interventions were relevant to both counteracting abuse and breaking free. While many interventions focused on supports for women who already experienced IPV, it is relevant that some interventions focused on preventing IPV and the early recognition and awareness of IPV. Very few interventions relevant to the COVID-19 pandemic context focused on supporting women after leaving an abusive partner. This may be because these interventions, such as emergency shelters and individual and group counseling, have been historically provided primarily in-person. It is clear that there is a need for more development of interventions appropriate to the COVID-19 context to support women after leaving an abusive partner, including supports for women who wish to remain living in their homes and communities.
Greater utilization of consistent outcome measures of quantitative studies would contribute greatly to our knowledge. There is also a need for replication research as few studies focused on examining the outcome of the same intervention. These actions could lead to improved evidence to support decision-making and the ability to conduct systematic reviews utilizing meta-synthesis.
The results of this review highlight that many initiatives relevant to the COVID-19 context are dependent upon various forms of technology. There are many implications of this finding for policy and practice including the need for access to technology. Women who do not have the financial resources to pay for smartphones or computers or reside in places where there is no reliable internet connection (e.g., rural and remote places) may be particularly vulnerable during the COVID-19 pandemic, and access to technology is crucial, especially for women living in low resource countries and women living in poverty in other countries (Yeager et al., 2015). Initiatives are needed to ensure the stability of communication networks, especially in rural or remote areas and in low-income countries. Interventions may also be needed to support women to learn to use technology who have low technology literacy.
While IPV researchers tend to focus much more on the needs of younger women versus older women there is a small body of knowledge that emphasizes the vulnerability and needs of older women (Stöckl & Penhale, 2015; Weeks et al., 2021). The sources included in our review clearly focused on women in midlife and younger. While we did not limit our search strategy to exclude older women, we found that these women were either overtly excluded from participating in studies or recruitment strategies did not result in their inclusion (e.g., Ford-Gilboe et al., 2020; Glass et al., 2017). It is clear that researchers need to expand their recruitment strategies to include older women, especially in studies examining the feasibility and usability of various technology-mediated interventions. Evidence indicates that many older adults who do not have cognitive decline can adapt to utilizing various technologies (Kim et al., 2017).
The included studies focused largely on research conducted in high resource countries with relatively well-educated and white samples; this may be due, in part, to our inclusion of studies only published in English or French. Some evidence of intersectionality in our synthesis was evident, such as a study focused on Spanish-dominant low-income Latinas (Alvarez et al., 2018), although a greater emphasis on intersectionality in study recruitment is needed. As most interventions were provided in one language only, efforts are needed to expand the availability of interventions in multiple languages. The synthesis of available evidence in languages other than English or French and with more diverse samples is warranted. It is important to ensure that interventions are tailored to meet the unique needs of diverse populations of women, such as those who live within social contexts where there are large economic inequities between men and women, where women have little mobility and autonomy, and where access to interventions is very limited (World Health Organization, 2005). IPV support services are very limited in low- and middle-income countries. In a recent review, Wood and colleagues (2021) identified that in these contexts, engaging informal networks of family members and friends was commonly utilized as a safety strategy in addition to strategies such as engaging in behavior change and building personal financial resources.
Conclusions
In this review, we contributed important and timely knowledge about IPV interventions for women that are relevant to the context of the COVID-19 pandemic. Importantly, these interventions can also benefit women who live in rural and remote places and women who do not wish to utilize in-person services, such as those who have concerns related to confidentiality. We found that the largest number of interventions focused on the identification of IPV and supporting women while living with and/or leaving an abusive partner. Additional interventions are needed that focus on the prevention of IPV from occurring, and interventions supporting women after leaving an abusive partner. Evidence across studies indicates many positive impacts of the initiatives on the physical health, mental health, and safety needs of women. However, greater consistency in data collection methods is needed. Additional work is also needed to determine the feasibility and acceptability of these interventions, especially interventions developed or adapted since the onset of the COVID-19 pandemic.
Footnotes
Acknowledgments
We recognize the contributions of Colleen MacQuarrie, Dave Neeb, and Kristal LeBlanc in the preparation of this manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the SSHRC Explore Grant, Dalhousie University.
Systematic Review Registration Number
The study protocol PROSPERO registration number is CRD42020194242.