
Abstract
Globally, significant numbers of women report obstetric violence (OV) during childbirth. The United Nations has identified OV as gendered violence. OV can be perpetrated by any healthcare professional (HCP) and is impacted by systemic issues such as HCP education, staffing ratios, and lack of access to continuity of care. The current study explored the experiences of OV reported in a national survey in 2021 by Australian women who had a baby in the previous 5 years. A content analysis of 626 open text comments found three main categories: “I felt dehumanised,” “I felt violated,” and “I felt powerless.” Women reported bullying, coercion, non-empathic care, and physical and sexual assault. Disrespect and abuse and non-consented vaginal examinations were the subcategories with the most comments.
Pregnancy, birth, and becoming a mother are significant events in a woman's life that are not forgotten. Being subject to disrespectful or abusive care can lead to a birth being considered traumatic by women, with significant resulting sequelae (Simonovic, 2019). Violence against women is a widely recognized international issue of systemic gender-based violence (United Nations, 1994). When this occurs in the context of birth it is referred to as obstetric violence (OV). OV is not routinely measured in country-specific birth data but is reported to range from 17% in the United States, 24% in Mexico, and 58% across African countries (Perrotte et al., 2020). Much of the research on OV to date has come from low- and middle-income countries (LMIC) leading to the impression that this issue does not affect women in high-income countries (HIC) such as Australia.
In a report to the United Nations (UN) General Assembly on the mistreatment and violence against women in reproductive health services, the Special Rapporteur asserted that the definition of violence against women from Article 1 of the Declaration on the Elimination of Violence against Women, was applicable to OV (Simonovic, 2019). This definition states violence against women is “any act of gender-based violence that results in, or is likely to result in, physical, sexual or psychological harm or suffering to women, including threats of such acts, coercion or arbitrary deprivation of liberty, whether occurring in public or in private life” (United Nations, 1994). Gender-based violence is violence against women because they are a woman, or violence that impacts women disproportionately (United Nations, 1994). OV was first recognized in the Venezuelan “Organic Law on the Right of Women to a Life Free of Violence” (2007) which describes OV as the experience in childbirth which becomes dehumanizing, physically and/or mentally abusive, and intrusive (Mena-Tudela et al., 2020; Michaels et al., 2019).
Obstetric Violence results in a loss of autonomy and leaves a women feeling confused and disempowered because they are conditioned by society to trust in the caregiver's authority and knowledge. This power imbalance and abuse of trust in the birth space (Mena-Tudela et al., 2020; Michaels et al., 2019) can result in birth trauma, higher rates of postnatal depression and post-traumatic stress disorder (PTSD) (Martinez-Vazquez et al., 2021; Souza et al., 2017).
Legislation identifying OV as both gender-based violence and clinical malpractice has been introduced into seven countries in Latin America (Simonovic, 2019). However, in HIC countries, the terminology of OV is resisted by some healthcare professionals (HCPs) (Lévesque & Ferron-Parayre, 2021; Savage & Castro, 2017) as not being relevant, as women have greater access to protections, rights, and opportunities which may not be the case in LMIC. The term OV has also been described as antagonistic toward HCP as it implies an intentional act to cause harm (Bohren et al., 2020) and there are polarized debates on the use of the term OV (Garcia, 2020; Lappeman & Swartz, 2021; Lévesque & Ferron-Parayre, 2021) which is often misunderstood by women and society (Sadler et al., 2016). It has also been suggested that using the term OV can be disempowering for women and potentially limits the potential for HCP to change (Lappeman & Swartz, 2021). However, this view was challenged by Lévesque and Ferron-Parayre (2021) who argued that identifying behaviors as OV can empower women through acknowledgment and education, thus releasing feelings of shame and blame, and through storytelling, women may become empowered.
It is not just women who experience harm resulting from OV. Witnessing OV can have a negative impact on HCP and support people. Rubashkin and Minckas (2018) explored the moral distress of US medical students observing OV during overseas placements. An Australian survey of midwives found those that witnessed a traumatic birth described feelings of helplessness, fear, and powerlessness, and 17% of the 601 midwives were identified as potentially reaching the diagnostic criteria for PTSD (Leinweber et al., 2017). A study from Turkey found 20% of 417 midwifery students in their study experienced PTSD symptoms which increased to above 24% if they witnessed a traumatic birth (Bayri Bingol et al., 2021).
Australia is one such HIC country where there is often resistance to acknowledging OV exists (Human Rights in Childbirth, 2019) and in the recently published Australian National Plan to End Violence against Women and Children 2022–2032 there was no mention of OV (Department of Social Services, 2022).
Like many countries, Australia has rising cesarean and intervention rates. In 2019, most women gave birth in hospital (97%) and the national cesarean rate was 36%, the VBAC (vaginal birth after cesarean) rate 12.2%, and 46.8% of primiparous women had an induced labor (Australian Institute of Health and Welfare [AIHW], 2021a). The episiotomy rate has increased from 12.7% in 2009 to 24.3% in 2019 (AIHW, 2021a; Li et al., 2011).
In Australia, there are a variety of maternity models of care that women can access, dependent on location and availability (Keedle et al., 2020). The largest model of care is fragmented (40.8%) in nature and results in women seeing different HCP during pregnancy, labor and birth, and the postnatal period (AIHW, 2021b). Women may be able to access continuity of care with a midwife through a public hospital in midwifery group practices (MGP) (15.1%) or through privately practicing midwives (PPM) (2.2%) who often offer homebirth services (AIHW, 2021b; Dawson et al., 2016; Wilkes et al., 2015). The private obstetrician model (10.5%) and shared care with a general practitioner (14.6%) offer different types of continuity under medical-led care through a private or public hospital (AIHW, 2021b; Keedle et al., 2020).
The aim of this paper is to explore the prevalence and experiences of OV reported by women who had a baby in Australia in the previous five years from 2021.
Theoretical Framework
The Reproductive Justice Framework is a framework that combines reproductive rights with social justice and has three primary principles—the right to have a child, the right to not have a child, and the right to parent in safe and healthy environments (Ross & Solinger, 2017). Reproductive justice uses a human rights framework to “draw attention to—and resist—laws and public and corporate policies based on racial, gender, and class prejudices. These laws and policies deny people the right to control their bodies, interfere with their reproductive decision making, and, ultimately, prevent many people from being able to live with dignity in safe and healthy communities” (Ross & Solinger, 2017, p. 10).
This study used a reproductive justice framework due to the recognition of reproductive oppression resulting from the intersection of many oppressions and the link to the struggle for social justice and human rights (Ross & Solinger, 2017). The study on OV is pertinent to the reproductive justice framework due to its focus on gender-based violence (Simonovic, 2019), and the fact that it is impacted by multiple intersecting oppressions such as body size, class, ethnicity, and indigenous status (Chattopadhyay et al., 2018; Delay & Sundstrom, 2019; Dietsch et al., 2010; Goli et al., 2019; LaMarre et al., 2020; Perrotte et al., 2020).
Methods
Participants, Ethics, and Methods
The data analyzed and reported in this paper come from a national survey undertaken as part of the Australian Birth Experience Study (BESt). This paper focuses on the prevalence of OV in a sample of 8,804 women. There were 8,546 completed responses to the question on OV and 63% (n = 626) of women who responded to the OV question responses provided open text comments about their experiences of OV. Descriptive statistics and content analysis as described by Schreier (2020) were used to analyze the data.
Survey Development
The Birth Experience Study (BESt) was a national survey launched in 2021 aiming to explore the experiences of women who had a baby in the previous five years in Australia. The online survey comprised 133 questions and included validated measurements such as the Mother's Autonomy in Decision Making (MADM; Vedam, Stoll, Martin, et al., 2017), Mothers on Respect index (MORi; Vedam, Stoll, Rubashkin, et al., 2017), and The Mistreatment Index (MIST; Vedam et al., 2019), demographic information and a combination of open and closed questions developed by the research team. The survey was available in English and translated into seven other languages which were Arabic, Simplified Chinese, Hindi, Filipino, Persian, Thai, and Vietnamese. The survey software Qualtrics was used for the design and distribution of the survey (Qualtrics©, 2019).
BESt was a co-creation between academics, consumers, and filmmakers (Birth Time). A consumer reference group made up of representatives from 10 Australian maternity advocacy organizations informed the study design and pilot tested the research questions. A cultural steering group of women from all of the different language groups advised on and informed the translations. During survey development, the survey was reviewed by the consumer reference group and cultural steering group, and recommended additions and changes were undertaken. The survey was piloted with women from the target group and any further suggestions were added to the survey. The final version of the survey was submitted with the ethics application. Ethical approval was obtained through the Western Sydney University Human Ethics Board, approval number: H14260.
Participant Sampling
This study utilized non-probability self-selection for the recruitment of participants using predominantly social media. The survey was distributed using social media and on postcards distributed at a variety of cinemas around Australia showing the documentary “Birth Time.” A social media page was formed, and posts were created in each designated language with information about the survey including a link and QR code to the survey landing page. A series of social media adverts in each designated language were undertaken throughout the survey collection duration. The survey became the largest birth experience survey conducted in Australia with over 12,000 partial and 8,804 completed responses and was live from March 2021 to December 2021. Women were asked to respond to the survey if they had had a baby in Australia in the past 5 years. There were 8,546 valid responses to the question “Do you think you experienced obstetric violence (dehumanized treatment or abuse by health professionals toward the body or reproductive process of women)?” If the response was “yes” or “maybe” the following open text question was displayed “Please give more information on your experience of obstetric violence,” of which there were 626 comments. Descriptive statistics were undertaken on the 8,546 responses and a content analysis on the 626 qualitative open text responses.
Content Analysis
Qualitative content analysis emerged from systematic and objective quantitative methods to analyze media content focusing on frequencies of words and themes and developed into a flexible methodology that systematically categorizes textual data using researcher interpretation (Hsieh & Shannon, 2005; Schreier, 2020). Schreier (2020) describes five steps to content analysis which include deciding on the research question and data, creating a preliminary coding frame, testing and updating the coding frame, coding the entire dataset, and presenting the findings. An inductive/conventional content analysis was used to allow for research findings to develop from raw data (Hsieh & Shannon, 2005; Thomas, 2006).
A preliminary coding frame of data-driven subcategories was created using the first 100 comments of the dataset which were read and re-read until the authors were familiar with the data. Once 100 comments had been analyzed the initial coding frame of subcategories was discussed within the research team and a coding frame of main categories and subcategories was created.
The coding frame was then used with the entire dataset of 626 comments where new subcategories were formed and organized as required. To ensure reliability, double coding was undertaken on 50 comments by a second member of the research team and continuous discussions occurred between the research team throughout the analysis process. Data saturation was reached after coding approximately 250 comments. During the coding process, longer quotes were separated into units of coding based on thematic criteria which made the total amount of units of coding 749 made by 626 women. The final coding frame was refined through discussions with the three members of the research team. The findings of the content analysis will be presented in a narrative format where each of the main categories and subcategories on the coding frame will be discussed and illustrated with units of coding in the form of quotes from the dataset. Similar to the content analysis used by Edmonds et al. (2021), the frequency distribution of the responses across the data is reported as the number count (units of coding) and percentage.
Reflexivity
In qualitative research, it is important to consider the positions of the researchers to increase validity and transparency (Pezalla et al., 2012). The first and last authors are midwives and midwifery researchers with experience in qualitative and mixed methods research, both have written extensively on the topic of women's experiences of maternity care and have a combined clinical career spanning 50 years. These two researchers have witnessed OV and supported women who have previously experienced OV. One of the researchers experienced an unconsented vaginal examination (VE) during their own birthing experience, which motivated their interest in conducting further research into the area of OV. The second author is a research assistant with experience in qualitative and quantitative research analysis. Regular research team meetings were undertaken and during the analysis process, these meetings also provided support to the team members due to the challenging nature of the content.
Findings
Participants
From the valid 8,546 responses, there were 991 (11.6% of the BESt survey cohort) respondents who identified “yes” or “maybe” to the question on OV. In total 626 respondents left comments and further information about their experience of OV. Most women were between the ages of 25–39 years, had a combined income of more than $100,000, and were university educated and married or in a long-term relationship. Although most women were born in Australia (87%) there was a range of ethnic backgrounds, with 79% identifying as Australian and 8% of women stating they spoke a language other than English at home. Just over 3% of women identified as Aboriginal. There was a representative spread of participants responding from all the States and Territories in Australia. Demographic information can be found in Table 1. There was no missing demographic data.
Demographic Information on Women Responding to a Question on Obstetric Violence (n = 8,546).
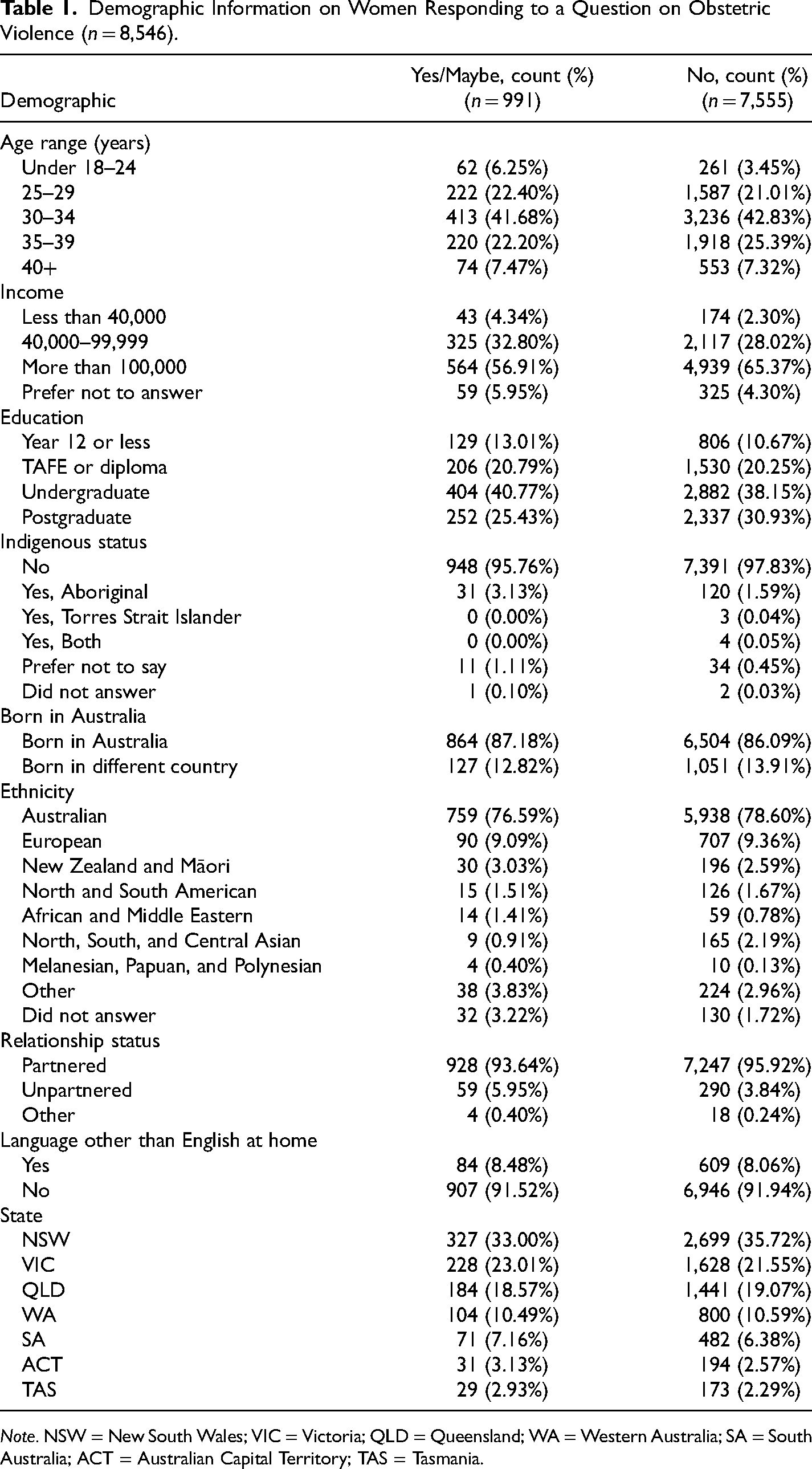
Note. NSW = New South Wales; VIC = Victoria; QLD = Queensland; WA = Western Australia; SA = South Australia; ACT = Australian Capital Territory; TAS = Tasmania.
Just under half of the women (48%) responding “yes” or “maybe” to the question on OV had standard maternity care in public hospitals that is fragmented in nature (40.8% of models in Australia) (AIHW, 2021b). There were 21% of women who had continuity of care with a midwife through a public hospital (15.1% of models in Australia) and 15% had continuity of care with a doctor, mostly situated in private hospitals (10.5% of models in Australia) (AIHW, 2021b).
Table 1 shows the demographics of women who answered “yes” or “maybe” to OV compared to those who answered “no.” Women who were younger, had a lower income, no tertiary education, identified as Aboriginal, or did not having a partner reported OV more. Although the total number of women responding to the survey was 8,804, there were 258 missing responses to the question on OV. Therefore, the number of valid respondents for the OV question was 8,546.
Main Categories and Subcategories
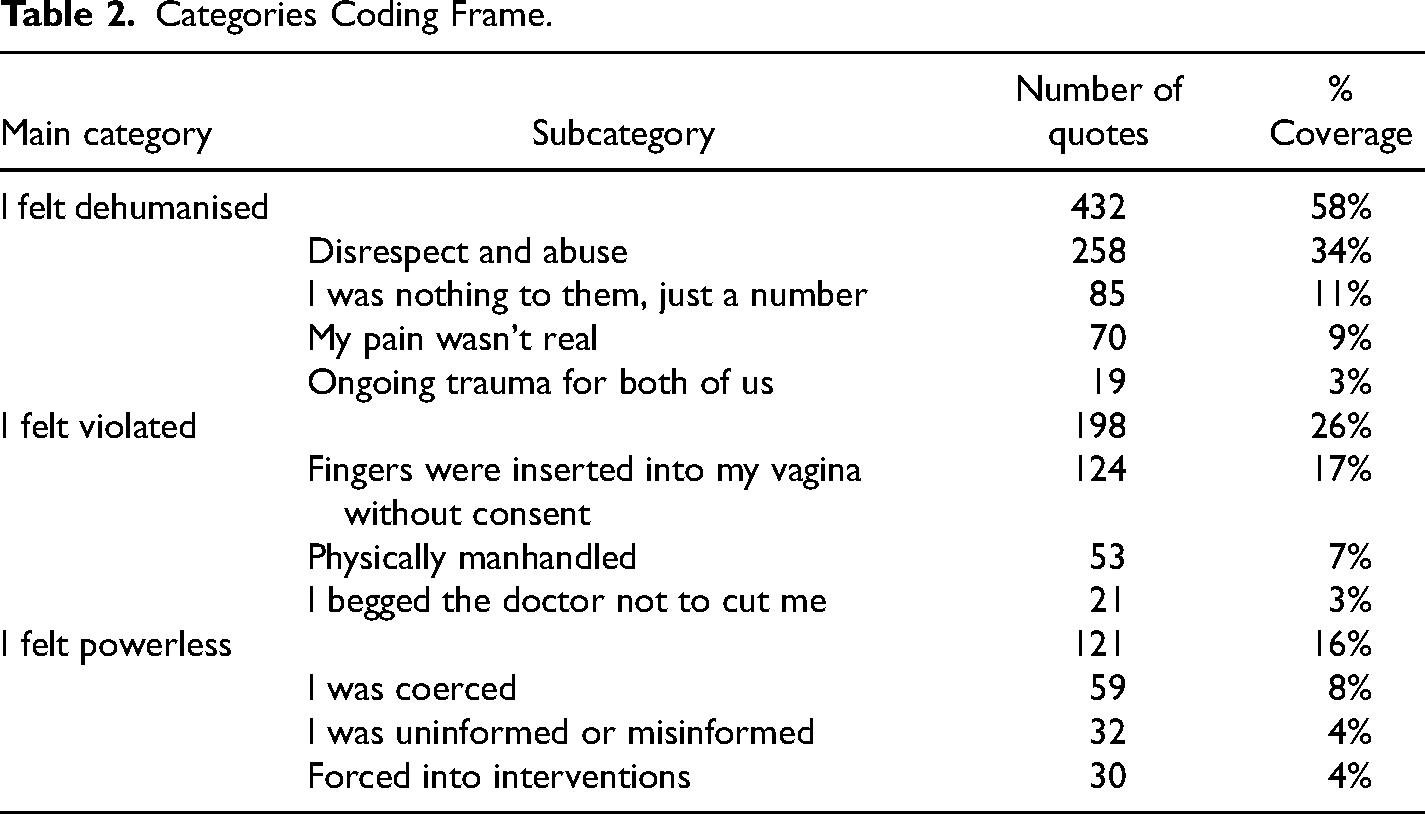
Three main categories were found that captured women's experiences with OV. These were: “I felt dehumanised,” “I felt violated,” and “I felt powerless.” Table 2 lists the categories and subcategories as well as the frequency distribution of the quotes in numbers and percentage in each category and subcategory. For example, the subcategory “Disrespect and abuse” had 258 quotes which were 34% of all quotes coded. The category “I felt dehumanised” encompassed 58% of the total coded quotes, “I felt violated” 26%, and “I felt powerless” 16% of the category quote coverage.
Categories Coding Frame.
The quotes presented in the findings are labeled with an identification number and model of care. The person who the women described as obstetrically violent may not be the main care professional but someone who they interacted with, either during a referral (i.e., midwife referring to a doctor) or some other HCPs they interacted with during their care. The models of care represented in the findings include public hospital care (PH), high-risk clinic (Highrisk), midwifery group practice (MGP), privately practicing midwife (PPM), GP Obstetrician (GPObst), GP shared care (GPshared) and private obstetrician (PrivObst).
I Felt Dehumanised
The largest category with 432 quotes making up 58% of all the quotes was “I felt dehumanised.” This category included experiences where women felt they weren't being treated as a human who deserved respectful maternity care. Subcategories include disrespect and abuse, I was nothing to them, just a body, my pain wasn't real and the ongoing trauma for both of us. This woman below summarizes this dehumanization: I felt dehumanised because A) nobody told me the procedure was optional or gave me choice to opt out. B) I was very clearly highly distressed and they didn't pause or stop the procedure to check my consent. C) there were three people I didn't know standing and looking at my exposed naked body. D) the midwife had joked about the procedure. (ID567, PH)
Disrespect and abuse
In this subcategory, women described experiences where they were treated by HCP in uncaring and inconsiderate ways, experienced psychological and emotional abuse, including the use of threats and bullying, or experienced care that was discriminatory or made them feel worthless. Some women felt disrespect due to feeling exposed. “The first OB while I was in labour didn't ask and just knelt down beside me while I was in no pants [underwear] completely exposed to do an ultrasound. I wasn't prepared to feel so uncomfortable, but he had built no rapport with me” (ID521, PH).
There were instances where women felt discriminated due to physical issues such as mental health issues, body size, age, or due to their personal beliefs. “Told I am obese and that I need to lose weight to have more children, that I wouldn't be a fit mother if I chose to not have scans ‘cause I couldn't afford them and that I had a mental illness cause my family turned on me” (ID570, PH).
In the following quote the woman experienced repeated comments about her age and body size, she also felt pressured to undergo sterilization and was body shamed for her choice of clothing during an appointment. “Too old, too fat, repeatedly asked me to have my tubes cut, threw a towel on me in the week before I gave birth because he could see my undies [underwear]. I wasn't wearing bike shorts under my dress because it was a hot summer” (ID573, Highrisk).
Some women had experiences of feeling ignored, having concerns dismissed, and having their choices and wishes taken from them. These experiences were during the antenatal period, labor and birthing as well as postnatally. In the example below, the woman transferred from a community midwifery program to a hospital during labor. The obstetrician stormed into my room without even introducing himself or considering anything about me and the situation I was in and demanded I had a caesarean. If he had have spoken to my midwives privately first, he would have learnt that a c-section was my worst fear and I did not want one, so speaking about me while I was having contractions and right there in the room listening was very inconsiderate and dehumanising and downright disgusting. (ID46, MGP)
A lack of compassion was felt by the woman in the following quote. “To sum it up. Multiple ppl [people] made me feel like I didn't do a good job and that I shouldn't have been in pain when I was. There was no compassion” (ID569, MGP).
Some women described psychological abuse and stated midwives and doctors yelled at them during their labor and birth. “A dr yelling at me while I have my legs spread … feels like rape” (ID10, GPObst).
One woman described the behavior of her private obstetrician who she felt didn't support her wishes for a vaginal birth. My obstetrician threw a tantrum to try to make me change my mind about labour. She yelled and jumped up and down! She threatened to take me to theatre during labour and walked in with everything she needed for an episiotomy but did not tell me that was her plan. She made me birth in lithotomy position, which I hated. I wanted hands and knees. (ID393, PrivObst)
Within the subcategory of disrespect and abuse women also referred to attitudes, behaviors, and systems that contributed to experiences of OV. The attitudes of HCP during interactions or procedures were not directed toward the woman but were hurtful or disrespectful and negatively impacted the woman. In the following quote, a woman recollects the inappropriate comments a doctor made and the concerns this caused her. While I’m looking at her, as the midwife starts stitching me up, the obstetrician is talking to the Paediatrician and says “great, she's ruined my shoes” and points to her shoes. My baby was on my chest, I’m being stitched for being cut, which was traumatic because I could hear it, and I screamed, “I can hear that,” and now I’m worried I’m going to have a stroke and might die and the female obstetrician is complaining about her footwear. (ID417, PH)
One woman describes how the cumulative effect of being disrespected was experienced as OV. I believe obstetric violence to be a spectrum. What I experienced was fairly low on the spectrum but shows the systematic way that we continually disrespect the birthing body. I was not believed about my previous birth and my place of birth was impacted by this information. I was forced to choose between coming into the hospital and birthing alone. (ID154, MGP)
I was nothing to them, just a body
The second largest (11% of quotes) subcategory in this main category “I felt dehumanised” was “I was nothing to them, just a number.” In this category, women experienced impersonal care, being ignored, feeling like “A body on the table that she has to treat rather than a woman who has just given birth” (ID18, MGP), and being disregarded.
Some women highlighted the impact of increasing numbers of strangers in the birthing room, like spectators with no regard for the woman giving birth. In the example below, the woman described the scene when she was birthing twins. “There were at least ten people in the room and two additional doctors/students staring at the delivery, without ever asking my permission. One didn't even introduce herself. It was utterly degrading and humiliating” (ID53, PH).
Some women felt their bodies were being used as teaching aids with little regard given to their wishes and privacy. Comments such as, “Brought male trainees in the room for an invasive and painful examination” (ID102, PH) and “Asking for extra internal exams to be done on me so the medical team could all feel the interesting position of the baby” (ID54, PH). In the data, there was repeated disregard shown to women by asking for multiple VEs for educational purposes.
The overall experience seen in this subcategory was how women felt part of an impersonal and automated system that had little respect for individual wishes and personal dignity. “I felt like I was on a conveyor belt of labour. Just people walking through the steps to deliver a baby without considering that I was involved” (ID205, GPshared).
My pain wasn't seen as real
There were 70 women (9% of quotes) in the study who referred to as being denied pain relief when requested or required. In the next example, the woman felt she was denied access to an epidural. “I believe I was abused as I didn't understand what was happening and I was denied pain medication” (ID153, PH).
In the example below, the woman felt that due to expressing her wishes for an epidural instead of a general anesthetic for a cesarean during labor she was punished through not being given local anesthetic for the insertion of the epidural, which took multiple attempts. I felt like I was thrown like a ragdoll in the theatre room after being given an epidural. Because I fought so hard to have epidural instead of general anaesthetic the Dr said there was no time for local anaesthetic first, so I had the epidural without local. It took the anaesthetist seven times to get the needle in place, each one was agonising pain. (ID520, PrivObst)
Women also described experiences of being denied pain relief post-birth. In the following example, the woman described how she was denied pain relief following an emergency cesarean where the doctor compared post-abdominal surgical pain to period pain. “I was belittled and denied access to pain medication from a male obstetrician who told me women who take pain medication for period pain are weak” (ID257, GPshared).
Ongoing trauma for the both of us
There were 22 comments where women identified the ongoing impact of experiencing OV. “It was a horrendous experience that has really impacted me and my mothering. It's a year next week and I still feel so emotional about how myself and my husband were treated” (ID417, PH).
Some comments identified the impact of witnessing OV on the partner, both at the time and following the event. “My husband couldn't watch as they were being so rough” (ID41, PH). In the example below, the woman describes how the fact her partner witnessed her care resulted in greater understanding of her ongoing issues. “My partner said it was horrible seeing it all happen and he wasn't shocked at all it resulted in long term issues” (ID228, PrivObst).
The ongoing implications following OV of difficulties with conception were highlighted by the women in the comment below. “Rather than a clear experience, it's a sense of disruption—I just wonder at the implications of the trauma and if there is some reason for our inability to conceive a second time” (ID465, PH).
I Felt Violated
The second largest main category “I felt violated” (17% of quotes) encompassed subcategories that focused on what women described as physical violence perpetrated by HCP. These included physical acts as described in the subcategory “physically manhandled,” the act of performing an episiotomy, and VEs that were non-consented or where consent was retracted during the procedure due to pain.
Fingers were inserted into my vagina without consent
The second largest subcategory in the dataset, with 124 comments, related to VEs given with or without consent that resulted in the woman feeling she experienced OV. Included in some of the comments were words that could be associated with sexual assault, such as penetrate, shoved, probing, rough, aggressive, violent, ripping open of legs, violated, torture, and raped. The examples below demonstrate the use of this language. “One time she [obstetrician] didn't even tell me she was going to penetrate me & I almost flew off the table with shock & pain” (ID18, MGP). It was a violation of my healthcare right. Consent was never sought. I work in healthcare and I know that not only did they have a legal obligation to seek/gain consent and explain everything that happened to me, but they had the time without it impacting care delivered. My birth experience was like being raped repeatedly over a 25 h period. (ID164, PH)
Repeatedly women expressed how they were given multiple vaginal and/or anal examinations (with suturing), often by different HCP, without consent and the impact this had on them. I was vaginally examined multiple times against my expressed consent. I kept screaming at them to take their hands out of my vagina and they would not. I had a midwife screaming in my face that I would kill my baby if I pushed with my body. (ID292, MGP)
Also in this subcategory were many situations when women received extra procedures during the VE that they didn't consent to or were unaware would happen, such as a manual stretch of the cervix with a finger sweeping the membranes (“stretch and sweep”) and artificial rupture of membranes. “A male midwife sexually assaulted me; he aggressively performed a stretch and sweep without consent—left it out of my notes and other midwives covered it up” (ID12, PH). I was told that they had to do a cervical check to see how thin it was because I was coming up to full term. I consented. They also asked if they could also do a stretch and sweep and I said no. When performing the check they also did the stretch and sweep while in there. At the time I felt extremely uncomfortable but didn't realise that's what he was doing until afterwards. I felt extremely violated. (ID287, GPshared)
One woman reflected on her experience in relation to the current climate of women speaking out about sexual assaults. We live in the “me too” generation. If someone wanted to have sex with me, and I said no, and then kept saying no, and then they told me someone I loved would die if I didn't agree to have sex with them, so I said yes and then cried and cried while they did it, that would be rape. I don't see how my experience was any different. (ID601, MGP)
Physically manhandled
In this subcategory, women gave 53 examples (7% of quotes) of physical interactions with their HCP that were rough, painful, restrictive, or felt inappropriate. In the example below, the woman describes two events that occurred after birth that she described as OV. Two midwives bounced on my tummy painfully for the afterbirth [placenta] whilst discussing other patients. I had to say ouch to get their attention and make them stop. One of the midwives grabbed my breast and expressed colostrum without warning and tried to jam my crying baby's head on to the breast. (ID466, PH)
Some women described being roughly maneuvered into different positions during labor and birth and “forcibly restrained” (ID591, MGP). One woman reported an experience after her emergency cesarean. “A male nurse kept performing an excruciating fundal massage while I was screaming at him to stop and he ignored me, telling the nurse he was handing over to, ‘she keeps screaming to stop but just ignore her” (ID556, Highrisk).
For one woman she described an experience that combined disrespect and abuse (being yelled at) and being physically manhandled. “I was hit by a dr [doctor] when I told her to stop touching me. She then yelled at me that I could die and hit my hand and touched me again” (ID270, MGP).
Overall, the women in this subcategory described feelings of helplessness and being ignored while they experienced rough, painful, or restrictive treatments by HCP. “Being held down on the bed so people could do things to me” (ID69, PH).
I begged the doctor not to cut me
In this subcategory, 21 women (3%) highlighted the experience of having an episiotomy as OV. In the example below, the woman describes having an episiotomy without her consent. I had a female junior registrar standing at my foot, repeatedly clicking the episcissors and saying “epis, epis, epis” while I was trying to birth my baby. I also had an episiotomy performed without consent (I was actually screaming “do not cut me” and trying to back up the bed away from the episcissors as the Dr did it). (ID401, Highrisk)
Some women found they were given limited information about episiotomy and no opportunity to give consent. I was told by the doctor who just appeared in the room that he would need to do a vacuum delivery and an episiotomy, and I felt him cut me as he was speaking before a numbing needle, it wasn't during a contraction and I hadn't had a chance to consent yet. (ID285, MGP)
I Felt Powerless
The final main category (16% of quotes) was “I felt powerless” which was made up of three subcategories. This category captured examples where women experienced coercive language, were given misinformation or were forced into interventions.
I was coerced
The subcategory with the highest number of related quotes in the category, “I felt powerless” (8% of quotes) was coercion. In this category, women experienced feelings of pressure to conform to HCP wishes rather than their own. “I said NO to the offered intervention over 6 min of repeated asking. I finally said yes when she COERCED me by getting me on my back with anaesthetic drawn up on a needle. I NEVER gave informed consent” [capitals used in open text response and retained] (ID239, MGP).
Coercion took many forms, such as emotional manipulation and blackmail. “Emotional blackmail used by Obstetrician to try to coerce me into consenting for unwanted (and unnecessary caesarean)” (ID109, PH).
Other women experienced coercive language and behaviors from healthcare professionals, often being presented with comments that their baby might die if they (women) didn't agree to the recommended treatment. At 42 weeks I presented for review of an ultrasound and the doctor spoke to me like I was absolutely stupid. Made fun of my wishes and told me, “it would suck to be one of the 4:1000 women whose baby dies” in relation to me declining an induction/caesarean section for gestation. (ID56, PPM)
I was uninformed or misinformed
There were 32 comments (4% of quotes) that indicated women felt they were not given the correct information or not given enough information to warrant the treatment they were given. In the quote below the woman felt pressured to have an elective cesarean throughout her pregnancy, which she didn't want. On reflection, she felt she was given incorrect information to be persuaded to have the cesarean. “My care provider lied to me and manipulated me about markers which were cause for a caesarean—I have subsequently seen two other Obs to look at these markers and they have both disagreed with the recommendation to carry out a caesarean” (ID380, PrivObst).
The misinformation could also be experienced as conflicting information, as seen below by this woman who had an emergency cesarean after five previous vaginal births. My future fertility was not treated as important. I felt cut open and slapped back together with the hope that I had the good sense never to fall pregnant again. When I asked if I could have a VBAC next time, one of the surgeons said it should be fine. My GP was sent a report stating I must not attempt a VBAC. (ID387, GPshared)
Forced into interventions
There were 30 quotes (4% of quotes) with descriptions of feeling forced to behave in a certain way, or forced to have an intervention. The interventions mentioned in this theme covered the spectrum of labor and birth, such as inductions, urinary catheters, epidurals, continuous fetal monitoring, stirrups, forceps, cesareans, and uterine massage. “I was put into stirrups without discussion or explanation and was restrained in them for the entire birth” (ID584, MGP).
Women felt powerless to refuse interventions, as demonstrated in the comment below. “Advised I would need to have an induction, continued to push medical intervention regardless of my wants or needs. OB would not allow me to decline the intervention” (ID437, MGP).
Women in this survey have described OV as resulting from actions by health care professionals that led to them feeling dehumanized, violated, and powerless. Experiences ranged from feeling belittled and coerced to physical assault. Women described procedures and interventions that were done to them without consent or when consent had been withdrawn and 20% of the total quote coverage were in relation to VEs or episiotomies involving women's genitals.
Discussion
This paper has identified more than 1:10 Australian women who feel they have experienced some form of OV. In total, there were 8,546 valid responses to the question on OV and 991 respondents who identified “yes” or “maybe.” Of those 991 respondents 626 left comments (63% of respondents) in the open text question which were analyzed, and three main categories were found; “I felt dehumanised,” “I felt violated,” and “I felt powerless.” Descriptive statistics demonstrated the demographic trends toward higher rates of OV, which included younger age range, lower income, no tertiary education, not having a partner, and identifying as Aboriginal. In this section, these main areas will be discussed in relation to current OV literature.
In the BESt survey, some women responded “maybe” when asked if they experienced OV and then explained in the open-ended comment the violence was perpetrated by midwives and not obstetricians. This highlights some of the confusion that the term OV just refers to obstetricians. However, the word “obstetric” (Cambridge Dictionary, 2022) is recognized as meaning, “that which is related to childbirth and the process associated with it” and so midwives and other HCP can and do participate in OV. Therefore, OV doesn't only mean violence perpetrated by the obstetric medical profession alone, but violence perpetrated by any HCP working in maternity settings, including midwives, nurses, and allied HCP.
The BESt study focused on women's experiences of maternity care. In their conclusion, Lappeman and Swartz (2021) stated that researchers should consider the voices of women in their own context. This has been achieved with the BESt survey responses. The responses coded were from the direct question: “Do you think you experienced obstetric violence (dehumanized treatment or abuse by health professionals towards the body or reproductive process of women)?” Only if a woman answered “yes” or “maybe” were they given the option to write a comment. These findings demonstrate the scope of OV as experienced by women. By claiming aspects of their treatment weren't violent enough to be classified as violence demonstrates minimizing and trivializing attitudes from researchers. This study identifies what constitutes OV from the women's perspective. To prevent future experiences of OV, it first needs to be recognized by academia, HCP, and society (Keedle et al., 2022).
Structural Violence
In this study, women were exposed to the use of coercion by HCP. It has been suggested that HCP use coercion to influence women's decision making to comply with the HCP recommendations (Grace & Anderson, 2018; Keedle et al., 2022). Health care professionals may base these recommendations on a need to follow institutional policies and guidelines. This focus on institutional policies and practices can lead to women experiencing impersonal care as was found in the category, “I was nothing to them, just a number.” Terms such as “a body on a table” and “conveyer belt” identify the impact of being a woman in the middle of an institutionalized and structured maternity machine. The impact of institutionalization can lead to systemic and structural OV.
There is a discussion in OV research about the role and impact of the systemic and structural level of OV (Briceno Morales et al., 2018). Briceno Morales et al. (2018) explored the origin and motives of HCP who perpetuate OV in Colombia and highlighted the need to understand the context that facilitates OV, which was identified as structural violence. Their qualitative study, comprising 18 interviews with women, found that OV was the result of behavior that had become routine through the inequitable vertical hierarchal hegemonic biomedical model, with women placed at the bottom of this hierarchy. The researchers also suggested that the context of increased societal violence in Colombia and the high level of violence experienced by women throughout their lives contributed to the normalization of OV (Briceno Morales et al., 2018). The recognition that globally maternity care is dominated by overmedicalization, and a patriarchal, technocratic view of birth has been discussed extensively by feminist academics and researchers (Fahy et al., 2008; Kitzinger, 2006; Shabot, 2021; Yuill, 2012).
It is important to get an understanding of the factors causing HCP to perpetuate OV in order to work toward a solution to prevent OV from occurring. Suggestions such as addressing staffing issues, restrictive policies, impact of bias, and a lack of awareness and education have been offered in the literature as contributing to structural violence (Chadwick, 2017; Keedle et al., 2022; Sadler et al., 2016). Since the rise of the online #MeToo movement, women have used social media platforms to speak out about their experiences of OV, reporting that OV is both widespread and entrenched in patriarchal health systems (Simonovic, 2019). However, it is important not to minimize the HCP individual role in OV. If the systemic or structural reasons behind OV are identified as the only cause of OV then potentially all HCP would commit OV, yet this isn't the case. The individual HCP who commits OV needs to have professional accountability through reporting and sanctioning by professional bodies and women should be aware of the processes for complaint (Simonovic, 2019). There is little data on how many women make formal complaints after experiencing OV. Reasons women may not complain can include feelings of shame, and the invisibility and the normalization of OV (Shabot, 2021). Further research is needed to identify maternity models of care, and the practice of individuals that contribute positively or negatively to OV.
This study highlighted a range of experiences of OV, but the most severe forms of violence were in the category “I felt violated.” The forms of violence described in this category included physical and sexual violence. Two common and often routine practices viewed as sexual/physical assault by the participants were VEs and episiotomy.
Vaginal Examinations
Vaginal examinations are seen as a routine internal examination of the vagina, cervix, and fetal head within a maternal pelvis. During labor, VEs can be performed every four hours or more, yet the role and impact of having a VE is rarely discussed. In this study, it was evident that a VE can be viewed as a sexual assault and it was the second largest OV subcategory in this dataset. Women described experiences where consent was never given or was retracted during the examination and many of the descriptions included terms synonymous with sexual assault, which has been found in previous research (Perrotte et al., 2020; Sadler et al., 2016; Shepherd & Cheyne, 2013). It is imperative that researchers, academics, and HCP address the role and necessity of routine VEs and the role of informed consent. The practice of VEs has become routine and widespread, even without sufficient evidence of benefit (Moncrieff et al., 2022; Nash, 2020), and HCP may have become desensitized and indifferent about the practice. A Cochrane systematic review found no evidence that routine VE improved maternal or neonatal outcomes (Moncrieff et al., 2022). Having a VE can be a systemic practice required before gaining access to labor ward, waterbirth, and pain relief (Nelson, 2021). As was found in this study, research demonstrates that women experience multiple VEs, often by multiple HCP throughout labor and often exceeding the suggested four-hourly protocol (Shepherd & Cheyne, 2013).
A negative VE experience can be exacerbated by the power imbalance between HCP and women. With the woman lying supine, her legs are opened and gloved hands insert two fingers into the vagina to check cervical dilation and the presenting part of the baby. The VE can be quick or long, easy, or complex, gentle, or rough and this is all dependent on the HCP. If you add a lack of consent and explanation, it is easy to see how this practice could be experienced as a violent, intimate assault. A study from the Netherlands found 35% of women found having a VE during labor a negative experience, and the odds of having a negative experience were increased with the amount of VEs and the number of HCP who performed them (De Klerk et al., 2018). A qualitative study from Turkey found women experienced pain, embarrassment, fear, and anxiety during VE (Teskereci et al., 2020). Further research is needed on the use of external physiological and behavioral signs to display progress in labor, such as observing the purple line, movements, and positions of the woman, and vocalizations, in place of routine VE (Nash, 2020; Teskereci et al., 2020).
Episiotomy
In this study, some women described the experience of having an episiotomy as a form of OV. Considering the episiotomy rate has doubled in Australia over the past 10 years this issue is likely to become more significant (AIHW, 2021a; Li et al., 2011). Clesse et al. (2018) undertook a systematic review on global statistical trends of episiotomy rates and found that except for East Asia, the episiotomy rates were declining. The data from Australia included in their review showed the decline from 65% in 1986 to 12.7% in 2009 (Clesse et al., 2018; Li et al., 2011); however, 10 years later in 2019, the rate has increased to 24.3% (AIHW, 2021a). A longitudinal cohort study from the UK found women who experienced an episiotomy reported a more negative birth experience with a decreased sense of control during the birth and less ability to influence their birth situation compared to women who had a first- or second-degree tear (Molyneux et al., 2021). Following a review of research, the International Federation of Gynecology and Obstetrics (FIGO) released a statement that endorsed the restrictive use of episiotomy compared to routine use, yet a qualitative study of obstetricians and midwives found they tend to rely on clinical experience and personal judgment over evidence-based practice (Zaami et al., 2019). The Special Rapporteur on OV found women often experienced episiotomy without anesthesia and without informed consent (Simonovic, 2019). A well-intentioned recent focus on trying to reduce severe perineal trauma rates in several western countries, including Australia, may inadvertently be leading to rising episiotomy rates, despite high-level evidence not supporting this (Australian Commission on Safety and Quality in Health Care, 2021; Jiang et al., 2017).
In this study, women described experiences of not giving consent, or having a procedure continue when consent had been withdrawn. As detailed in the UN report of the Special Rapporteur on violence against women in reproductive health services: “Women are frequently denied their right to make informed decisions about the healthcare they receive during childbirth and other reproductive health services; this lack of informed consent constitutes a human rights violation that could be attributed to States and national health systems” (Simonovic, 2019, p. 7).
Recommendations
OV is recognized in some countries as a criminalized act and women are protected under legislation (Mena-Tudela et al., 2020; Michaels et al., 2019). The Special Rapporteur on violence against women in reproductive health services encourages governments to review and strengthen laws that address violence against women and to include OV (Souza et al., 2017), which in Australia is a view supported by human rights organizations (Human Rights in Childbirth, 2019).
Recommendations coming from this study include a recognition of OV and a combined approach to address OV in Australia by obstetric and midwifery professional colleges in collaboration with maternity consumer organizations. It is also recommended that OV be recognized as a form of gendered violence in Australia with the implementation of legislation protecting women from OV. At the HCP level, it is recommended that training on trauma-informed care is implemented to deliver respectful and appropriate care for women with a history of OV, previous trauma, and/or a previous traumatic birth.
Limitations and Strengths
A limitation of this study is the use of a self-selected sample of women recruited from social media. The survey was available in English and seven other languages which is a strength but a limitation for women who were unable to read and understand any of the eight languages offered.
A limitation to the interpretation of the quantitative data in this paper is that the descriptive statistics only demonstrated trends and further analysis is needed. A more detailed statistical analysis of the positive and negative factors relating to OV will be published in a subsequent paper.
The demographics of the respondents highlighted that most women were between the ages of 25–39 years, had a combined income of more than $100,000, and were university educated and married or in a long-term relationship. This indicates that there was a lack of representation for younger women, women from a lower income bracket, and those not in a relationship or without tertiary education. Although there was a wide variety of ethnicities represented, the majority of women identified as Australian. A strength of the study was that there was a representative spread of respondents from all States and Territories in Australia. There were slightly more respondents in this study that had access to continuity of care with a midwife or doctor compared to national statistics (AIHW, 2021b).
Conclusion
This study demonstrates that OV is experienced by more than 1:10 women in Australia responding to a large national survey. Women experienced OV as feeling dehumanized, violated, and powerless. Disrespect and abuse and non-consented VEs received the most comments and need urgent attention. OV is gendered violence and can be perpetrated by any HCP. It is impacted by systemic issues such as HCP education, staffing ratios, and lack of access to continuity of care. A multi-level approach is needed involving consumer organizations, HCP professional organizations and individuals, academics, and health authorities in order for OV to be recognized, reported, reduced, and legislated against in Australia.
Footnotes
Acknowledgments
The BESt research team would like to acknowledge the consumer organizations involved in the co-design and funding of this study: Birth Time Documentary, Maternal Health Matters, Maternity Consumer Network, Homebirth Australia, Maternity Choices Australia, Canberra Mothercraft Society, Human Rights in Childbirth, Lamaze Australia, PBB Media, and Rhodanthe Lipsett Indigenous Midwifery Charitable Fund.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study received funding from the “Qiara® Vincent Thiang Memorial Award” and Western Sydney University.