
Abstract
Sexual violence increases the risk of adverse health outcomes among female sex workers (FSWs). Using data from the 2015 national bio-behavioral survey, we explored the experience of sexual violence and its associated factors among Iranian FSWs. Lifetime and recent sexual violence were reported by 40.1% and 16.9%, respectively. History of substance use, ever engaging in anal sex, engaging in group sex within the last year, a high number of clients, recent unstable housing, and incarceration increased the likelihood of experiencing recent sexual violence. These findings underscore the need for community-empowerment and policy-level interventions to address violence among FSWs in Iran.
Introduction
Sexual violence against female sex workers (FSWs) is recognized as a widespread public health problem (World Health Organization, 2005) and a violation of human rights (Decker et al., 2015). A systematic review of existing research reported a global prevalence of 14% to 54% of lifetime sexual workplace violence among FSWs (Deering et al., 2014). Sexual violence among FSWs can increase the risk of several adverse health outcomes, including HIV and other sexually transmitted infections (STIs) acquisition through unprotected sex, vaginal trauma, and lacerations (Gupta, 2002; Maman et al., 2000). Refusing to use or removing condoms during sex by a paid or unpaid partner as well as diminished self-efficacy for condom negotiation among FSWs have been proposed as immediate and sustained effects of sexual violence among this population (Shannon et al., 2015). In addition, fear of violence may force FSWs into unprotected sexual episodes or certain types of high-risk sexual encounters (Reeves et al., 2017).
Sexual violence is perpetrated against FSWs by their clients, non-paying partners, police, and other individuals (Deering et al., 2014). An increasing body of literature indicates that sexual violence is affected by factors beyond individual-level characteristics. Alongside individual factors such as alcohol and drug use (Odinokova et al., 2014; Zhang et al., 2013) or psychosocial distress (Jewkes et al., 2006), partner-level sexual and substance use practices (Heylen et al., 2019; Shaw et al., 2012), as well as a broad range of structural factors such as legal policies and sex work criminalization (Deering et al., 2013; Erausquin et al., 2011), and types of solicitation venues (Katsulis et al., 2015; Odinokova et al., 2014), have affected sexual violence among FSWs. The illegal and highly stigmatized status of sex work in most settings prevents FSWs from seeking legal resources (World Health Organization, 2005) and renders them more vulnerable to violence and exploitation (Decker et al., 2015). In settings where sex work or certain aspects of it are criminalized, no proper surveillance of violence is available and FSWs receive little to no protection from police and judicial systems (Shannon, 2010; Shannon & Csete, 2010). These can lead to a climate of tolerance where discrimination and use of violence against FSWs are deemed acceptable (World Health Organization, 2005).
FSWs in Iran are considered the second most affected population by HIV after people who inject drugs (PWID) (Mirzazadeh et al., 2020). Around 228,700 FSWs are estimated to live and work in urban settings in Iran (Sharifi et al., 2017) with a pooled HIV prevalence of 2.23% (95% confidence interval [CI] = [0.82, 3.64]) (Karamouzian, Nasirian, et al., 2019), and lifetime non-injection and injection drug use prevalence of 76.1% and 10.7%, respectively (Tavakoli et al., 2021). Sexual transmission of HIV, particularly among women and FSWs is on the rise in Iran (Shahesmaeili et al., 2018). In 2014, 36.8% of the registered HIV cases were attributed to unsafe sexual practices (National AIDS Committee Secretariat, 2015). Iran benefits from a relatively functioning HIV/STIs surveillance system (Karamouzian, Madani, et al., 2017) and follows a harm reduction approach toward FSWs (Fahimfar et al., 2013). Harm reduction programs such as free condom distribution and HIV testing and counseling services are provided for FSWs for free and mostly through centers for vulnerable women in major cities across the country (Fahimfar et al., 2013; National AIDS Committee Secretariat, 2015). Nevertheless, as a Muslim majority country, sex work continues to be an illegal and criminalized activity in Iran (Karamouzian et al., 2016). The existing cultural, religious, and political complications of sex work in Iran (Karamouzian, Nasirian, et al., 2019) have made the discussion around sexual violence challenging. The majority of data related to sexual violence come from the general female adult population of Iran and are mainly focused on intimate-partner violence (Hajnasiri et al., 2016). The magnitude and determinants of sexual violence among FSWs have received comparably much less attention in Iran (Sadati et al., 2019).
Indeed, identifying the factors associated with experiencing sexual violence among FSWs may assist in reducing the harms attributed to involvement in sex work and preventing violence and its associated health consequences among these historically marginalized women. Therefore, this study aimed to estimate the prevalence of lifetime and recent (i.e., within the past 12 months) sexual violence and to examine multiple factors associated with recent experiences of sexual violence among FSWs in Iran.
Methods
This study used a quantitative, cross-sectional design to investigate the prevalence and associated factors of sexual violence among FSWs in Iran. Iran is a middle-income country in the Middle East and North Africa (MENA) region. The research was conducted in 2015 as a part of the second national bio-behavioral surveillance survey (BBSS) to measure the prevalence of HIV, as well as risk behaviors, such as sexual and drug use practices, among FSWs. The present study applied data from this national survey in Iran. The details of study design and procedures have been previously published (Mirzazadeh et al., 2020; Shokoohi et al., 2017). Briefly, using a cross-sectional survey design, a total of 1,337 FSWs were recruited from centers for vulnerable women (n = 1,185) and through outreach efforts from street-based locations (n = 152). Centers for vulnerable women provide harm reduction services (e.g., free-of-charge HIV testing and counseling, drug and sexual health-related services) to vulnerable and at-risk women including FSWs (Fahimfar et al., 2013). Recruitment was completed in 13 major cities (20 sites) across the country between January and August 2015. The study sites were selected in line with the first round of BBSS among this population, as well as the recommendations received from the Ministry of Health’s HIV/AIDS control office. Women were eligible for the study if they were 18 years or older, reported having sexual penetrative intercourse in exchange for livelihood (i.e., money, goods, services, or drugs) with more than one client within 12 months prior to the interviews, held Iranian citizenship, and lived or worked in the city where the study was carried out. In each city, the sampling, data collection, and data quality and assurance were overseen and supervised by a project manager affiliated with the local medical university. FSWs were invited to participate in the study after receiving a brief introduction to the study aims and the potential risks and benefits of participating in the study. Those who provided verbal informed consent were interviewed one-on-one in a private room by a trained female interviewer. The study questionnaire was a BBSS (Joint United Nations Programme on HIV and AIDS, 2007) containing questions about demographics, history of sexual behaviors, HIV status, history of drug use and injection, and other relevant information. Participants received a monetary incentive for the one-hour interview (∼2 US dollars). The study protocol and procedures were approved by the Research Ethics Committee of Kerman University of Medical Sciences (Ethics reference number: K/93/209).
Dependent Variable: Experience of Sexual Violence
The present study evaluates the prevalence and correlates of experiencing sexual violence among FSWs using a self-reported measure. FSWs were asked, “Have you ever experienced any act of forced/threatened sexual contact from a paying or non-paying sexual partner?” with yes and no response options. Those who reported a lifetime experience of sexual violence were asked about their recent experience (i.e., within the previous 12 months). Recent experience of sexual violence was treated as a binary variable with “yes” or “no” response options.
Covariates
Our selection of covariates was informed by a socio-ecological model, a commonly used theoretical model in examining risk factors aiming to allow us to understand the impact of multiple risk factors at different levels that put FSWs at risk of sexual violence (Baral et al., 2013). Our analysis relied on the core indicators that are collected in the BBSS to measure the effectiveness of the national HIV response among key affected populations, including FSWs. We classified the covariates into three main categories: individual and behavioral, interpersonal, and environmental/structural.
Individual factors included age (less than 25 vs. 25–34 vs. 35 or more years old); early sex work initiation defined as sex work debut before 18 years old (before 18 years old vs. 18 or more); length of involvement in sex work (2 years or less vs. 3–5 vs. 6–10 vs. more than 10 years); ever being married (yes vs. no); current marital status (single vs. married vs. widow or divorced vs. temporary marriage); the highest level of education (illiterate vs. primary school or less vs. middle and high school vs. diploma and above); having any income source other than sex work (yes vs. no); and the history of substance use, including ever using of injection drugs, non-injection drugs, or alcohol (yes vs. no). Interpersonal factors included engaging in group sex (never vs. yes, but not in the last year vs. yes, within last year), ever engaged in anal sex (yes vs. no), and the number of paying clients in the past month (less than 5 vs. 5 and more). Environmental/structural factors included recent unstable housing defined as currently living in welfare facilities, streets, or shelters (yes vs. no); primary solicitation venue (street-based vs. others [e.g., independent, home-based or indoor]); and incarceration history (never vs. ever, but not in the last year vs. within the last year).
Statistical Analysis
Descriptive statistics including absolute and relative frequencies along with 95% CIs were used to describe the outcome variables overall and in subgroups of covariates. Univariate analyses were examined using the Rao-Scott modified Chi-Square test considering the clustering effect of the survey design (Rao & Scott, 1981) to report the prevalence of both lifetime and recent sexual violence across subgroups of the included covariates. Covariates with a p-value <.15 for the recent experience of violence were considered to be included in the adjusted models. For examining the multivariable association of the study covariates with sexual violence, we considered recent sexual violence as the main study outcome due to a better establishment of the associations between the covariate and the recent sexual violence (i.e., addressing the issue of temporality). We applied multivariable logistic regression using a generalized linear model (GLM) with Poisson as family and log link function (Zou, 2004) to report adjusted prevalence ratios (aPR) and their 95% CIs for the association of the included covariates with recent sexual violence. For each cluster of the included covariates, one separate adjusted model was performed: (a) multivariable model for individual factors within which only individual factors were considered to be included in the multivariable regression model, (b) multivariable model for only interpersonal factors, and (c) multivariable model for only environmental/structural factors. Covariates with adjusted p-value <.15 in each cluster were included in the final multivariable regression model. Finally, we conducted a survey analysis using the survey package to adjust for the clustering effect of the study cities within which participants were nested. All statistical analyses were done by Stata 15.0 using the survey command (StataCorp, College Station, Texas, USA).
Results
Sexual Violence, Overall and by Subgroups
From a total of 1,335 FSWs who provided valid responses to the lifetime experience of sexual violence question, 40.1% (95% CI = [33.9, 46.6]) had ever experienced sexual violence. Of 1,333 valid responses to the query on recent experience of sexual violence, 16.9% (95% CI = [13.1, 21.6]) reported such experience (Table 1). Among the individual factors, recent experience of sexual violence was significantly higher among participants who were less than 25 years of age, initiated sex work before 18, and reported a history of substance use. Among the interpersonal factors, recent experience of sexual violence was significantly higher among FSWs who had engaged in group sex within the last year, had ever engaged in anal sex, and those who had 5 or more paying partners in the last month. Among the environmental/structural factors, recent experience of sexual violence was significantly higher among participants who reported recent unstable housing, those who reported streets as their primary solicitation venue, and FSWs who reported incarceration within the last year.
Lifetime and Recent (Last-Year) Experiences of Sexual Violence Among Female Sex Workers in Iran, 2015.
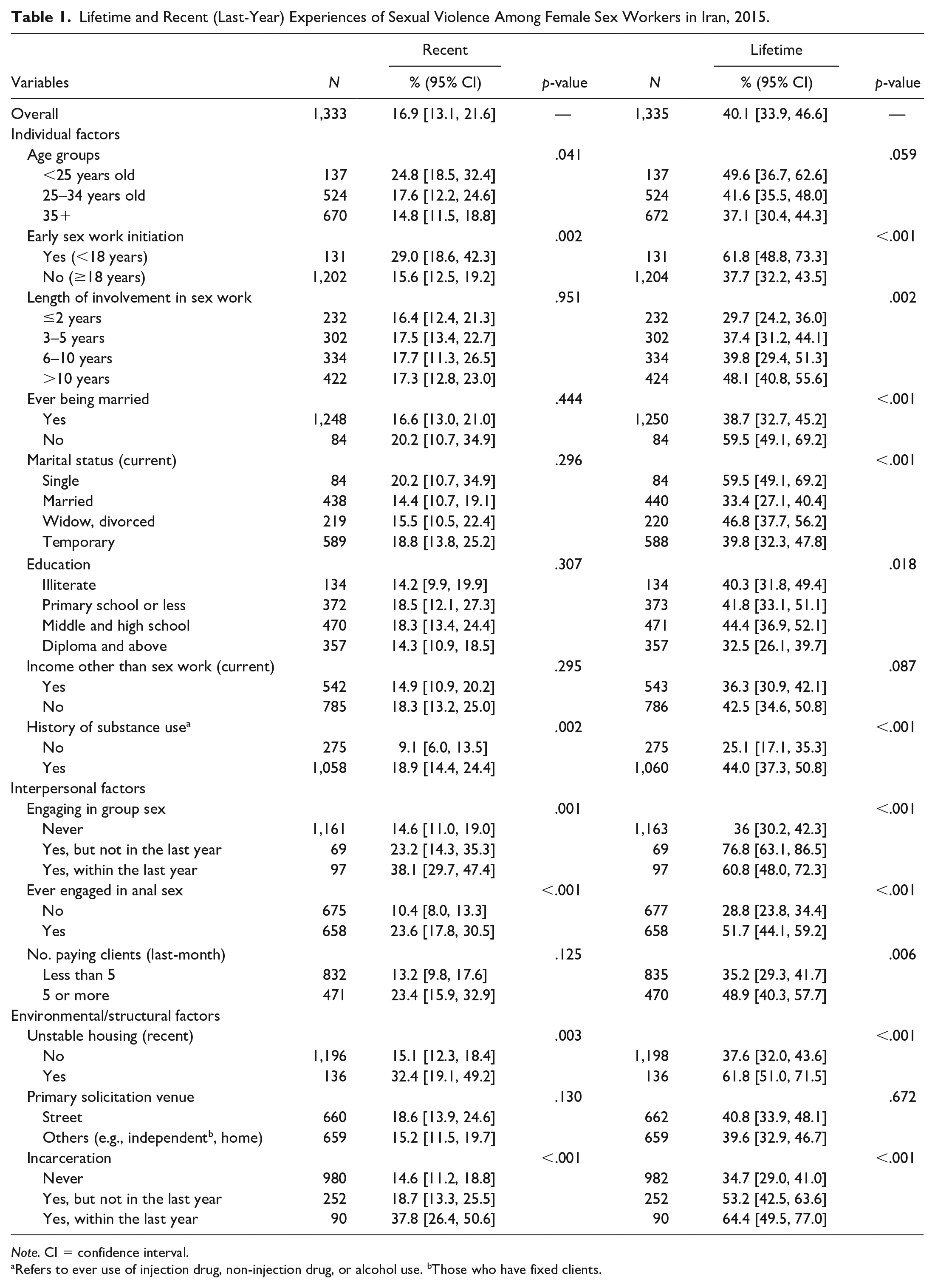
Note. CI = confidence interval.
Refers to ever use of injection drug, non-injection drug, or alcohol use. bThose who have fixed clients.
Factors Associated With Recent Sexual Violence
Being younger than 25 years, early initiation of sex work, and history of substance use from the individual-level adjusted model; engaging in group sex within the last year, ever engaging in anal sex, and a frequent number of paying partners from the interpersonal-level adjusted model; and recent unstable housing and incarceration within the last year from the structural-level adjusted model were significantly associated with an increased likelihood of recent experience of sexual violence (Table 2). In the final multivariable regression model where covariates with p-value < .15 from individual-, interpersonal-, and structural-level adjusted models were all included, the higher likelihood of recent experience of sexual violence was reported by FSWs who reported a history of substance use (aPR = 1.63; 95% CI = [1.01, 2.62], p-value = .044), engaging in group sex within the last year (aPR = 1.75; 95% CI = [1.25, 2.44], p-value = .002), ever engaging in anal sex (aPR = 1.89; 95% CI = [1.42, 2.50], p-value <.001), frequent number of paying partners within the last month (aPR = 1.43; 95% CI = [1.06, 1.92], p-value = .022), recent unstable housing (aPR = 1.75; 95% CI = [1.25, 2.46], p-value = .002), and incarceration within the last year (aPR = 1.73; 95% CI = [1.23, 2.45], p-value = .003) (Table 2).
Multivariable Models on Recent (Last-Year) Experience of Sexual Violence.
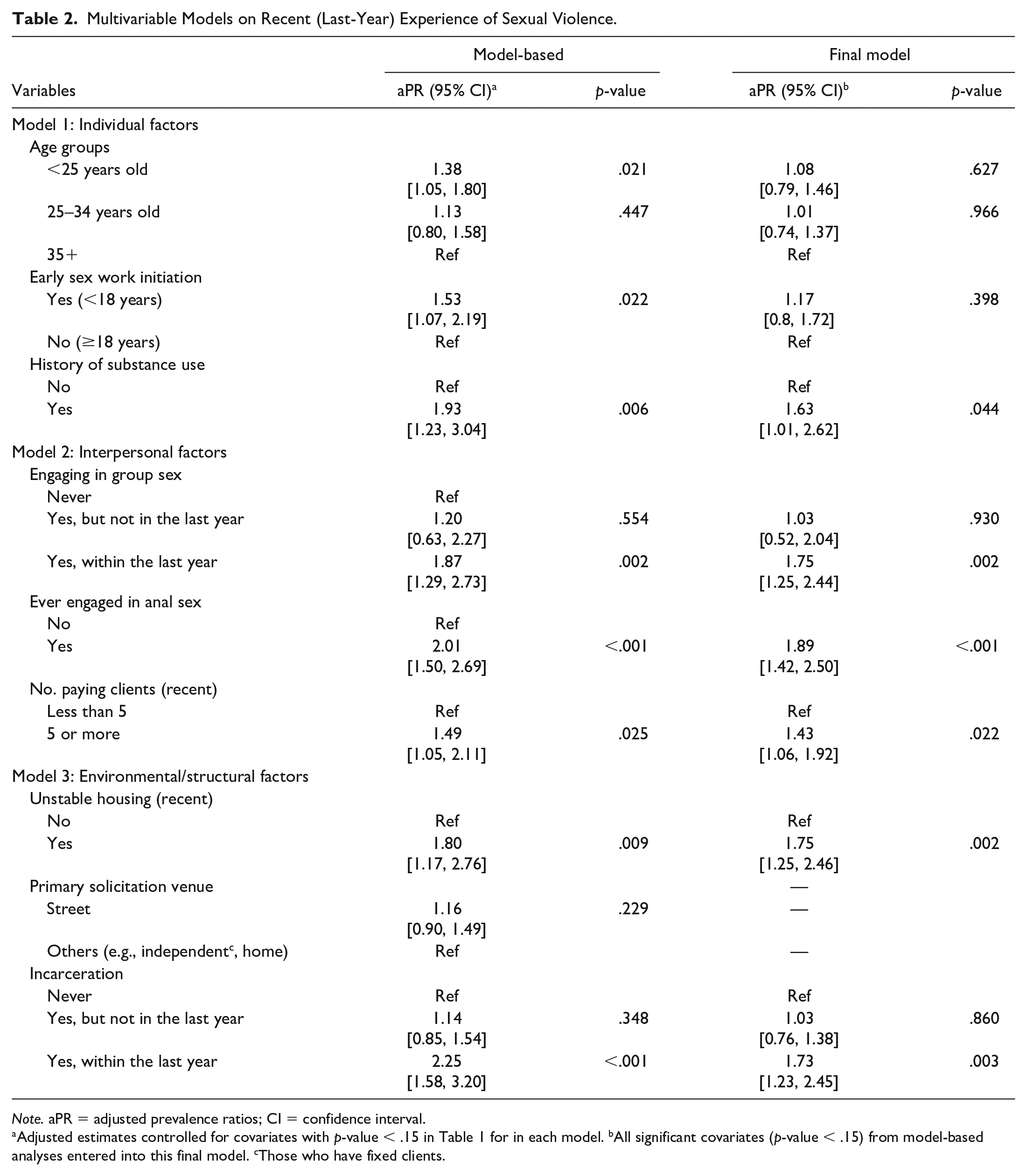
Note. aPR = adjusted prevalence ratios; CI = confidence interval.
Adjusted estimates controlled for covariates with p-value < .15 in Table 1 for in each model. bAll significant covariates (p-value < .15) from model-based analyses entered into this final model. cThose who have fixed clients.
Discussion
Our data revealed that about two-fifths of FSWs in Iran have experienced sexual violence at least once during their lifetime. In addition, one in every six FSWs reported recent experience of sexual violence, an estimate that lies within the global ranges of past-year sexual violence perpetrated by paying (15%–31%) and non-paying (8%–19%) partners (Deering et al., 2014). Our analyses further showed that a history of substance use, ever engaging in anal sex, engaging in group sex within the last year, frequent number of paying partners, recent unstable housing, and recent incarceration increased the likelihood of a recent experience of sexual violence among FSWs in Iran.
We found that a history of substance use was associated with an increased level of recent experiences of sexual violence. Substance use has been linked with elevated rates of sexual violence among FSWs in multiple settings, such as the United States (Carrington & Betts, 2001; El-Bassel & Witte, 2001), Russia (Odinokova et al., 2014), and China (Zhang et al., 2013). Tensions or conflicts over drugs and hostile behavior under the influence of drugs have been suggested to expose FSWs to violent situations, individuals, or activities (World Health Organization, 2005). FSWs have also been shown to resort to alcohol and drug use to cope with the violence they experience in their work (Alexander, 1998). With vulnerabilities associated with drug use among FSWs (Karamouzian, Mirzazadeh, et al., 2017; Shokoohi et al., 2021) and a higher risk of violence among those with substance use practices, there is indeed a need for integrating novel approaches such as community empowerment and education into care and harm reduction delivery alongside removing barriers to facilitate access to substance use treatment services among this subgroup of FSWs.
We also documented higher levels of recent experiences of sexual violence among those who reported group sex, anal sex, and a frequent number of paying partners, highlighting the major role of interpersonal factors in recent experiences of sexual violence. High-risk sexual behaviors have been shown to put FSWs at an increased risk of violence in international studies. For example, engaging in anal sex with five or more sexual partners was associated with sexual violence experienced by FSWs in India (Shaw et al., 2012), and the higher number of sexual partners was correlated with higher levels of sexual violence among FSWs in Kenya (Chersich et al., 2007). When possible, avoiding new clients has been suggested as a strategy to moderate potentially violent situations (Thukral, 2005); however, that might not be a feasible option for many FSWs. Violence reduction interventions addressing the issue of sexual violence among FSWs should do their best to reach and target their clients and partners and enhance their perception of risks associated with high-risk sexual encounters (Huang et al., 2012).
Our findings also highlight the association between sexual violence and structural level factors including unstable housing and incarceration. These two key determinants are linked with other risk behaviors such as drug and poly-drug use in our previous international reports (Shokoohi et al., 2018, 2019, 2021). Unstable housing has been identified as a significant correlate of both physical and sexual violence among FSWs across international settings (Reed et al., 2011; Shannon et al., 2009). Similarly, literature endorses a strong correlation between arrest or incarceration history and increased levels of sexual violence experienced by FSWs (Deering et al., 2013). Incarceration is a direct indicator of criminalization of FSWs (Deering et al., 2014) and has been linked with substantial vulnerabilities that could place FSWs at higher risk for sexual violence (Deering et al., 2013; Karamouzian, Shokoohi et al., 2019). Fear of police and incarceration has been shown to displace FSWs to more isolated settings where they might be at higher risk of violence (Shannon et al., 2008). These findings highlight the need for multi-level interventions that target such structural determinants to address and eliminate sexual violence among FSWs.
The findings of this analysis have important implications for policymakers in Iran. Community empowerment interventions aimed at FSWs may provide education on their rights and mechanisms for reporting violations of those rights. Such interventions alongside psychological and behavioral counseling services can be integrated into the existing harm reduction services. Gender-sensitive, peer-run prevention and treatment services have been emphasized in policy and development programs to address the unique needs of this population in Iran (Karamouzian et al., 2014; Karamouzian, Mirzazadeh, et al., 2017; Shokoohi et al., 2019). The structural-level vulnerabilities need to be addressed to provide a holistic approach toward sexual violence prevention. Regular screening and referrals through outreach efforts are warranted to identify FSWs who are at a higher risk of experiencing sexual violence and link them to ongoing care. Addressing the role of legal practices (i.e., arrest and/or incarceration) on sexual violence is also of particular importance in violence prevention interventions. While the involvement of the police in any violence prevention or reduction programs appears to be necessary, we believe that this might be hard to consider as the nature of sex work is criminalized and illegal in Iran. This indeed requires revisiting the current policies and developing decriminalizing policies toward sex work and FSWs. The adverse public health effects of criminalized laws and policies on sex work among FSWs need to be addressed. This calls for advocacy on decriminalization of sex work as a crucial step that could ultimately help address the individual- and structural-level vulnerabilities associated with involvement in sex work in Iran (Beyrer et al., 2015; Shannon et al., 2015; World Health Organization, 2012).
We acknowledge the limitations of our study. First, this study may not be representative of the overall experiences of sexual violence among FSWs in Iran. The most vulnerable FSWs that have no access to services, as well as those who find their clients online or highly paid FSWs, might be less represented in the present study. Therefore, we are not confident that our findings have overestimated or underestimated the true prevalence of sexual violence among FSWs. However, we managed to include 152 FSWs from street-based venues to provide some insight on non facility-based FSWs. Second, due to the cross-sectional design of our study, the cause-effect relationships between exploratory variables and sexual violence are difficult to establish. For this reason, we considered experiencing sexual violence in the previous 12 months as the main study outcome when examining the association of other variables to take the issue of temporality into account. Third, as the findings of this study relied on self-reported measures, they are subject to social desirability and recall biases; as a result, such measurements may impact the validity of our study. To partially mitigate the issue of social desirability bias, we involved experienced female interviewers from local staff to increase the trust between the interviewees and interviewers. Fourth, the recent experience of sexual violence among FSWs in this study was assessed in relation to both non-paying partners and paying clients; however, the effects of client-perpetrated sexual violence may differ from intimate partner violence, since it occurs in the context of commercial sex. Future studies in Iran should make a distinction based on the type of partners/clients or from any other sources (e.g., police) when estimating sexual violence and other types of violence among FSWs. Finally, although the dataset applied for the analyses of this study represents the most updated national survey of FSWs in Iran, data were collected in 2015 and may not represent the current levels and predictors of sexual violence among FSWs in Iran. There is a need to update and develop interventions with the present data for accurate estimating and monitoring of sexual violence among FSWs in the near future in Iran.
Conclusion
This study provides evidence of a high burden of sexual violence against FSWs in Iran and has implications for their health and safety. It also reveals the links between structural and policy-level factors, alongside interpersonal and individual factors, and elevated rates of sexual violence against sex workers. Our findings highlight the need for further research in intervention design and evaluation to better document and respond to sexual violence experienced by FSWs in Iran. Community empowerment interventions alongside counseling services may be integrated into the existing care and harm reduction services to address sexual violence among FSWs. Clients and partners of FSWs need to be involved in violence prevention and reduction programs. The structural-level vulnerabilities such as housing instabilities need to be addressed by regular screening and referrals to support services through outreach efforts among more marginalized FSWs. The adverse public health effects of criminalized laws and policies on sex work and drug use among FSWs need to be addressed. Finally, evidence-based interventions plus culturally sensitive programs should be considered and developed to reduce the burden of sexual violence among FSWs in Iran.
Footnotes
Acknowledgements
A special thanks to the study participants who took part in the survey. We are thankful for the important contribution of medical university supervisors and field staff from all collaborative universities who helped in the design, data collection, and implementation of the survey. M.K. is supported by the Vanier Canada Graduate Scholarship and the Pierre Elliott Trudeau Foundation Doctoral Scholarship. M.S. is supported by a Canadian Institutes of Health Research (CIHR) Postdoctoral Fellowship.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Global Fund to Fight AIDS, Tuberculosis and Malaria through UNDP Iran, and by Iran’s Ministry of Health. For this article, we also received support from the University of California, San Francisco’s International Traineeships in AIDS Prevention Studies (ITAPS), U.S. NIMH, R25MH064712.