
Abstract
Low-income, ethnic, and/or displaced mothers are frequently victimized; we explored the burden of intimate partner violence (IPV) among such women. Teams administered IPV and maternal distress questionnaires to quantify victimization after the birth of a child. Of 250 mothers reporting abuse, 133 (53%) reported their husband hitting; 111 (44%) kicking, dragging, or beating; 61 (24%) choking or burning; and 33 (13%) injuring them with a knife or gun (12 case-patients per 100 person-years). Women who experienced more forms of victimization reported more distress (p = .01). Mothers in this low-income community experienced severe victimization and distress.
Introduction
Intimate partner violence (IPV) includes physical, sexual, psychological, or emotional, or threat of violence, perpetrated by a current or former partner, which can take place along a continuum from a single episode to ongoing battering (Saltzman, Fanslow, McMahon, & Shelley, 2002). Survivors often report a poor quality of life, frequent health problems, and greater health care utilization than those unaffected by IPV (Fischbach & Herbert, 1997; Wisner, Gilmer, Saltzman, & Zink, 1999). In the United States, the direct and indirect costs of IPV are approximately US$5.8 billion a year. This includes costs for medical and mental health services and lost productivity among survivors with maternal mental distress, depression, anxiety, chronic pain, substance abuse, suicidality, and disabilities as a result of such violence (Hathaway et al., 2000; McCauley et al., 1995; McFarlane, Parker, & Soeken, 1996; Silverman, Raj, Mucci, & Hathaway, 2001). In families with children, IPV also has a profound effect on child witnesses who grow up steeped in a subculture of violence and are at greater risk of becoming perpetrators themselves (Groves, 2002; McCloskey, Figueredo, & Koss, 1995). Recurrent patterns of severe violence can culminate in permanent disability or death (Heise & Garcia-Moreno, 2002; Rennison, 2003).
Studies suggest that certain communities experience higher rates of IPV than others (Krahé, Bieneck, & Möller, 2005; Menjívar, 2002; Watts & Zimmerman, 2002). A large multi-country World Health Organization (WHO) study (Garcia-Moreno, Jansen, Ellsberg, Heise, & Watts, 2006) found that the lifetime prevalence of physical or sexual violence by an intimate partner ranged widely between high-, middle-, and low-income countries, for example, from 15% in Japan to 71% in Ethiopia. In South Asian countries, IPV is a prevalent public health problem. Data from Thailand, a country that is also in the South East Asian Region of the WHO, suggest that 16% to 17% of adult women reported sexual victimization by an intimate partner during 2000. The World Report on Violence and Health suggests that 30% to 45% of Indian women aged 15 to 65 years, and 42% of Bangladeshi women aged 15 to 49 years were physically assaulted by intimate partners during their relationship at the time of the study (Heise & Garcia-Moreno, 2002). Similarly, Silverman, Gupta, Decker, Kapur, & Raj (2007) found that approximately one half to three quarters of married women interviewed in Bangladesh experienced IPV at any given time from a current spouse. Survey data suggest that immigrant, displaced, or otherwise disenfranchised communities within Bangladesh experience higher rates of IPV victimization and perpetration than other communities. Naved and Persson (2005) reported that 62% of men in low-income communities in Dhaka punched, kicked, or choked their wives during their lifetime, a proportion that was greater than in higher income communities (45%). In the same study, 48% of women living in low-income communities believed that IPV could be justified compared with 32% among women living in higher income communities in Dhaka. Naved and Persson also demonstrated that low education among husbands, low socioeconomic status, Muslim religion, dowry demands, and conventional views about the roles of males and females were risk factors for perpetrating violence against female partners.
Such studies suggest that although the general population in Bangladesh experiences a high burden of IPV, ethnic, low-income communities within Bangladesh may experience even higher rates of IPV with secondary health consequences (Bates, Schuler, Islam, & Islam, 2004; Heise & Garcia-Moreno, 2002). To explore such a hypothesis, we surveyed mothers in a low-income community of Bangladeshis and mothers in a displaced ethnic minority of Biharis. The Bihari populations, who originate from Pakistan, remained in Bangladesh after the 1971 liberation war between Bangladesh and Pakistan but are still culturally isolated and speak their native Urdu as opposed to the Bengali language of Bangladeshis. Estimates of IPV prevalence and incidence among such potentially vulnerable communities are necessary to describe the burden of victimization and to guide investment of limited public health resources to prevent and mitigate IPV. In this study, we quantified the prevalence and incidence of IPV and its potential association with maternal mental distress among mothers of low-income Bangladeshi and displaced ethnic-minority Bihari communities before and after the birth of a child.
Method
Study Population
Our study was conducted in Ward 3 of Pallabi thana (thana is the lowest administrative unit in Bangladesh), Dhaka. This ward of low-income Bangladeshis and displaced ethnic Biharis has 20,576 persons/km2 (i.e., 0.4 miles2), 39% of which are aged less than 17 years; a mean literacy of 59% among females (76% of whom are homemakers); and a median monthly household expenditure (a proxy for income) of US$290 among >90% of the households. Women in our study were previously enrolled during pregnancy in a community-based influenza birth cohort study that explored potential associations between severe respiratory illness and cognitive development by identifying influenza illness, assessing household factors, and quantifying the development of children from birth to 2 years of age (Homaira et al., 2012).
Outcome Measures for the IPV Study
For the IPV study, we quantified the prevalence of IPV and rate among the subset of mothers who began experiencing IPV for the first time in their relationship. Field teams visited cohort households to administer standardized questionnaires about members’ medical history, acquired wealth, and parent education. Field teams trained on ethical protection, standardized interviewing, and protection of participants’ anonymity then privately requested separate consents from mothers to complete a standardized 13-item questionnaire that asked them about IPV during the preceding year (Ebell, 2004; Straus, Hamby, Boney-McCoy, & Sugarman, 1996). The questionnaire has been previously used in large population-based surveys in Bangladesh (Beusenberg & Orley, 1994; Naved & Akhtar, 2008) to document a history of emotional abuse (e.g., insults, humiliation, intimidation, or threats), physical violence (e.g., slaps, shoves, punches, kicks, dragging, choking, or injury with a weapon), and sexual violence (e.g., forced or coerced sexual intercourse) perpetrated by a husband. We added one point for each type of violence participants ever experienced in the current relationship to generate a composite IPV score, which we analyzed as a continuous variable (possible scores ranged from 0-13). We presented overall IPV findings stratified by physical, sexual, and emotional violence.
We anticipated that disclosing IPV to someone outside the family nucleus could provoke further IPV. To protect participants’ confidentiality, we administered the questionnaires in the privacy of the study field office. The interviews were conducted only if respondents were alone or with children aged less than 2 years (i.e., pre-verbal children). In addition, we did not record participants’ names, opting instead to use unique codes kept separately from other study data in locked cabinets. The protocol for this investigation was reviewed and approved by the U.S. Centers for Disease Control and Prevention and the International Centre for Diarrhoeal Diseases Research, Bangladesh (icddr, b) human subjects committees.
Mental Distress Within the Community-Based Study
As a secondary objective, we sought to also explore the impact of IPV on mothers’ maternal mental distress and well-being. Teams assessed mothers’ mental distress using a version of the Centre for Epidemiological Studies–Depression (CES-D) questionnaire (Radloff, 1977) with 20 questions. Sixteen questions were about the number of days that participants had a depressed mood, irritability, poor appetite/unwillingness to eat, despondency, feelings of failure, poor self-esteem, inattentiveness, lassitude, insomnia, isolation, crying spells, apathy, ahedonia, and lack of energy, which served as indicators of mental distress. Four questions were about the number of days that participants enjoyed themselves or felt happy, worthy, or optimistic, which served as indicators of emotional health. We added the days during which participants reported symptoms compatible with mental distress and subtracted the days during which participants reported symptoms compatible with emotional well-being to generate a composite mental distress score for the week prior to the interview. We analyzed this composite mental distress score as a continuous variable (possible scores ranged from −112 to +28).
Estimating IPV Prevalence and Rates
We counted the number of mothers reporting ever being subject to specific types of violence in the current relationship with their husband to quantify the prevalence of IPV in their marriage (the primary outcome). We assumed that mothers would correctly recall whether IPV in the marriage began for the first time after the birth of the child or prior to that time. We also estimated the rate of IPV by dividing the number of mothers who began experiencing IPV for the first time in their relationship after the birth of the cohort child over the total study person-time of mothers who had never experienced IPV before the birth of the cohort child (a secondary outcome). This person-time represented each participant’s time at risk of new-onset victimization. We used the birth of the cohort child as a reliable marker of time that predated the interview (i.e., to define a quantifiable risk period) but did not assume the birth event to be associated with victimization. We only counted mothers’ person-time after enrollment because we did not believe we could accurately assess mothers’ relationship status before enrollment.
Exploring Risk Factors for IPV and Maternal Distress
We explored participants’ demographics and described mothers’ and fathers’ age, number of dependents, ownership of a mobile phone or TV (as proxies of wealth), and education. Although the household sample size was chosen to optimize the potential to study respiratory viruses among cohort children (i.e., the primary goal of the influenza study), we used linear regression models to explore the association between victimization (i.e., elevated composite IPV score) and risk factors (i.e., young maternal age, relative lack of wealth [TV and cell phones], lack of education, female birth cohort child, and household crowding [number of household members per dwelling]). We also assessed the potential association between maternal mental distress (i.e., elevated composite mental distress score), victimization, young maternal age, relative lack of wealth, lack of education, female birth cohort child, and household crowding.
Results
Demographics
During 12 months, we followed 250 cohort mothers for 272 person-years, including 15 mothers (for a total of 16 person-years) who had not experienced IPV in their relationship before the birth of the cohort child. The median age of mothers was 25 years (interquartile range [IQR] = 22-30 years). Only 3 (1%) had a diagnosed pre-existing condition: Two had asthma and one tuberculosis. With one exception, all mothers were in their first marriage. Mothers lived in dwellings with an average floor space of 9 m2 (i.e., 10.8 feet2) and four household members (IQR = 3-5; that is, 2 m2 of floor space per person) typically with their child, husband, and one other family member. Ninety-one (36%) of the 250 mothers did not have formal education, 87 (35%) had primary education, 68 (27%) had secondary education, and 4 (2%) had vocational training. Most of the 250 households had cell phones (165 [66%]) and televisions (156 [63%]).
Prevalence of IPV During Marriage
The majority (237 [95%] of 250) of mothers in the cohort experienced events of physical, sexual, psychological, or emotional violence, or threat of violence, during their marriage. Mothers reported an average of seven types of violence out of the 13 explored by the questionnaire (IQR = 4-10). Of the 250 mothers reporting physical IPV, 205 (82%) were victimized: 133(53%) reported ever being hit with a fist or some other object; 111 (44%) were kicked, dragged, or beaten; 61 (24%) were choked or burnt; and 33 (13%) were injured with a knife or gun (Table 1). Of the 250 mothers reporting sexual IPV, 187 (75%) were sexually victimized: 154 (61%) were forced into sexual intercourse by their husband, and 162 (65%) were threatened or coerced into sex by their husbands. Of the 250 mothers reporting emotional IPV, 222 (89%) were emotionally victimized: 222 (89%), were insulted or made to feel bad about themselves, 201 (80%) were scared or intimated, 138 (55%) were belittled or humiliated in front of other people, 80 (32%) were threatened with injury, and 105 (42%) were threatened with harm to someone close to her. Out of 133 mothers who reported that their husband hit them with a fist or some other object, 118 (89% of 133) experienced this violence before the birth of the cohort child and 98 (74%, p < .01) after, including two who had not experienced IPV before in their relationship.
Descriptive Analysis of IPV in a Community of Low-Income Bangladeshis and Displaced Ethnic Bihari Mothers—Dhaka, 2008-2009 (n = 250).
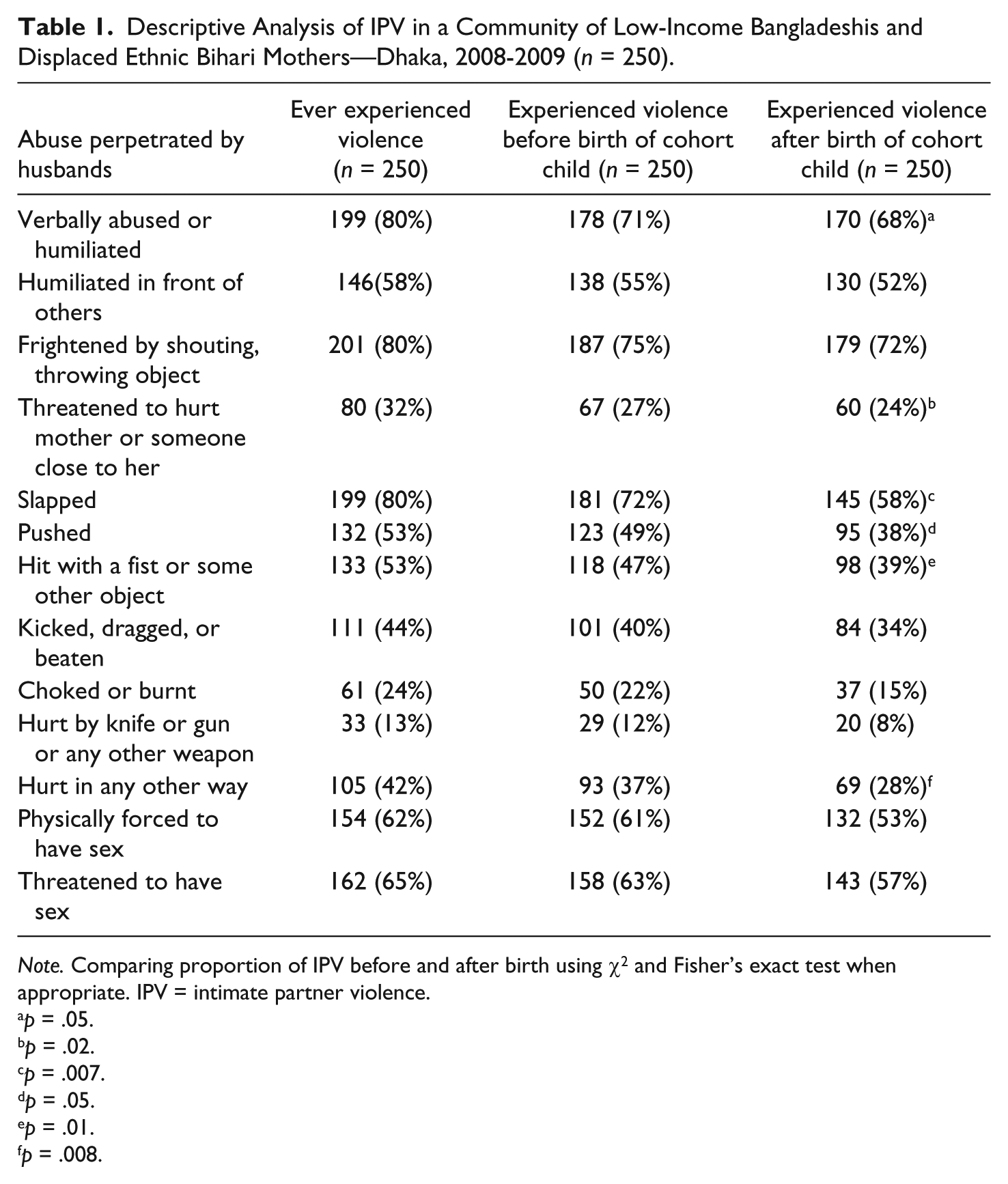
Note. Comparing proportion of IPV before and after birth using χ2 and Fisher’s exact test when appropriate. IPV = intimate partner violence.
p = .05.
p = .02.
p = .007.
p = .05.
p = .01.
p = .008.
Rates and Risk Factors for IPV
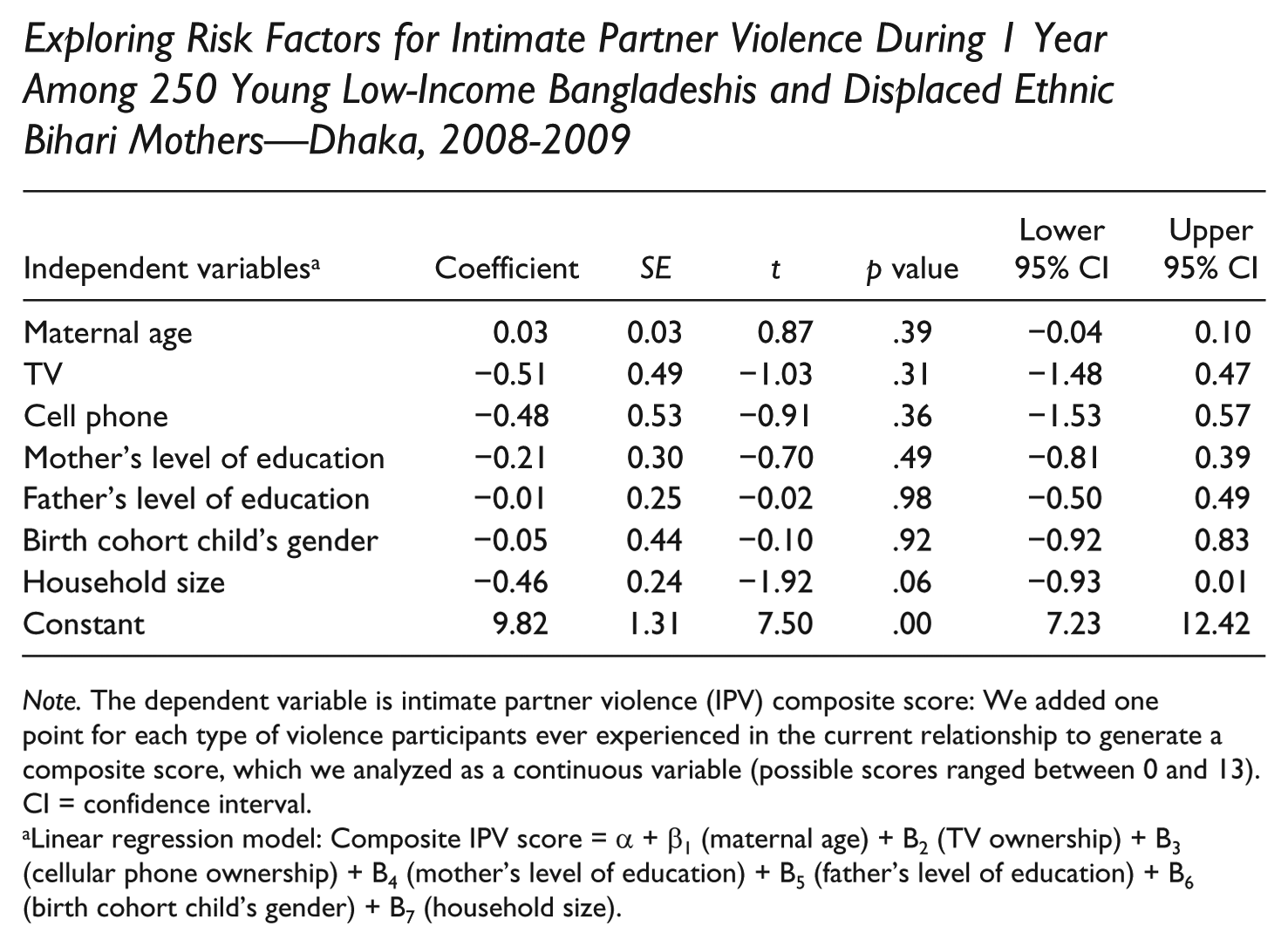
The 15 mothers who had never experienced IPV during their relationship before the birth of the cohort child contributed 16 years of at-risk person-time to the study. Two (13%) of these 15 mothers reported that IPV began, for the first time during their relationship, after the birth of their child (12 mothers victimized through physical IPV per 100 person-years). Both of these mothers reported that their husbands slapped them or threw objects that could hurt them after the birth of the cohort child. IPV composite score was associated with maternal age, accumulated wealth, parental education, or household size among our 250 participants (see Appendix A).
Maternal Mental Distress
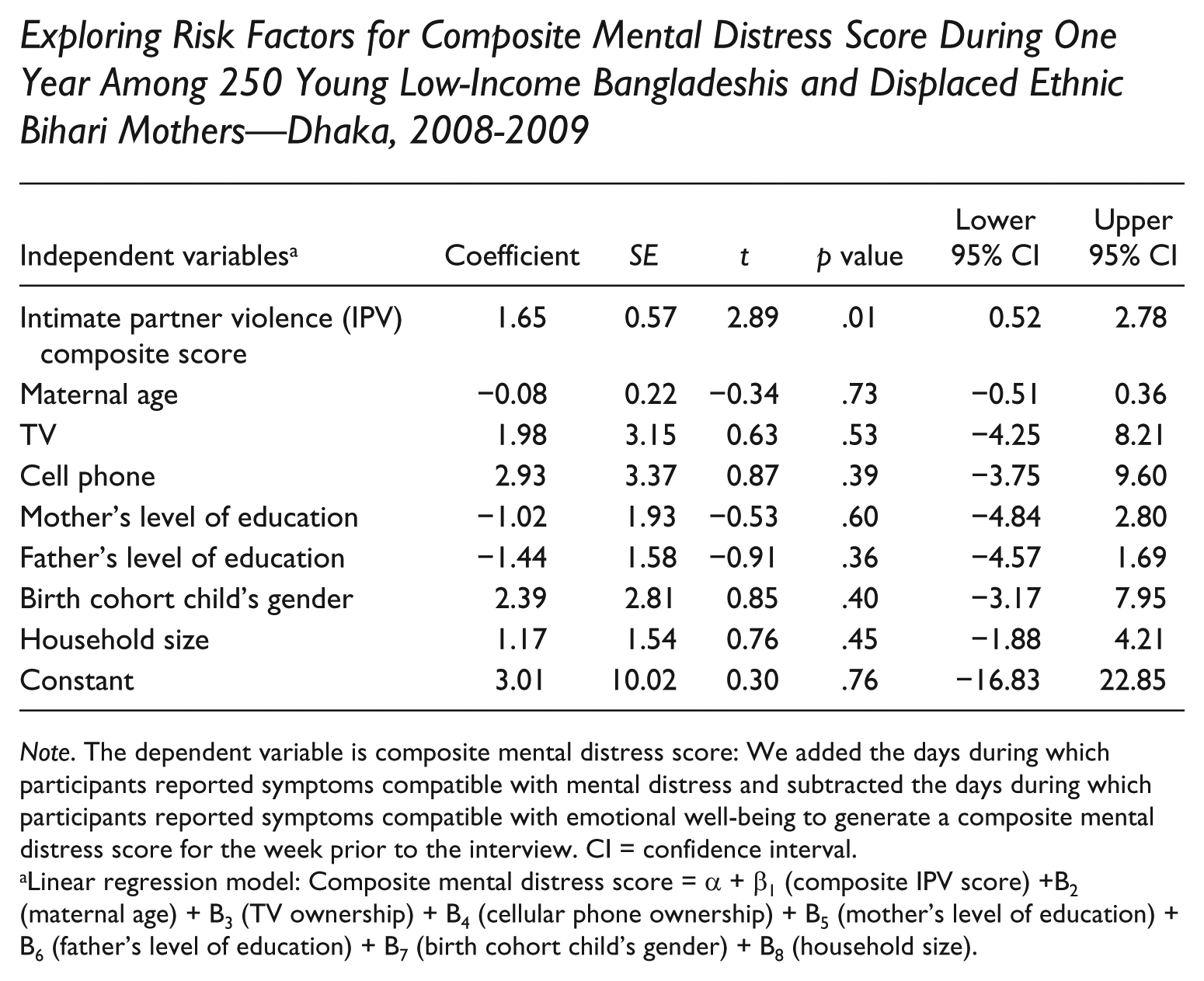
On average, mothers felt inconsolable, ahedonic, and depressed, and indicated they had a poor appetite during 2 days [IQR = 1-3 days] the week before their interview (median composite mental distress score = 17 out of a potential maximum of 140 [IQR = 7-26]). Mothers also felt that their life was a failure during 2 days (IQR = 1-4 days), felt like crying 1 day (1-2 days), and that something bad was going to happen to them 1 day (IQR = 1-3 days) the week before the interview. In contrast, mothers reported enjoying themselves 1 day (IQR = 0-2 days), feeling happy 1 day (IQR = 0-3 days), and feeling hopeful about the future 3 days (IQR = 1-5 days) the week before the interview. The composite mental distress score was associated with the IPV composite score (linear regression coefficient 1.6, p = .01) after adjusting for maternal age, possession of a TV or cell phone, schooling, gender of cohort child, and household size (Figure 1; see Appendix B). The 223 mothers who reported IPV after the birth of the cohort child were more likely to report poor appetite, despondency, inattentiveness, depression, feeling overwhelmed, withdrawn, crying, or poor self-esteem during one additional day than the 27 mothers who did not report post-partum IPV (p < .04; Table 2).
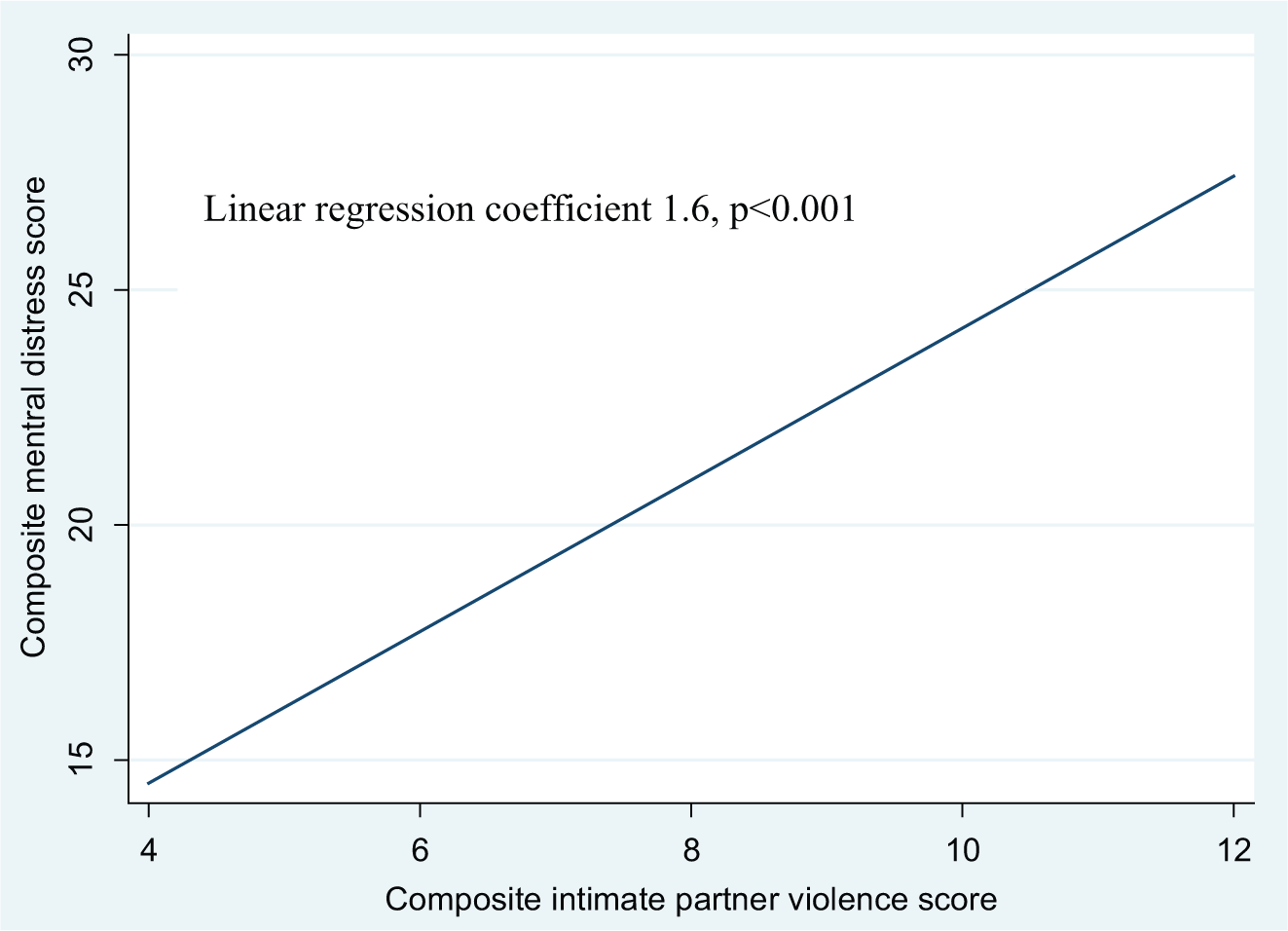
Association between composite mental distress and intimate partner violence scores in a community of low-income Bangladeshis and displaced ethnic Bihari mothers—Dhaka, 2008-2009.
Descriptive Analysis of IPV in a Community of Low-Income Bangladeshis and Displaced Ethnic Bihari Mothers—Dhaka, 2008-2009.
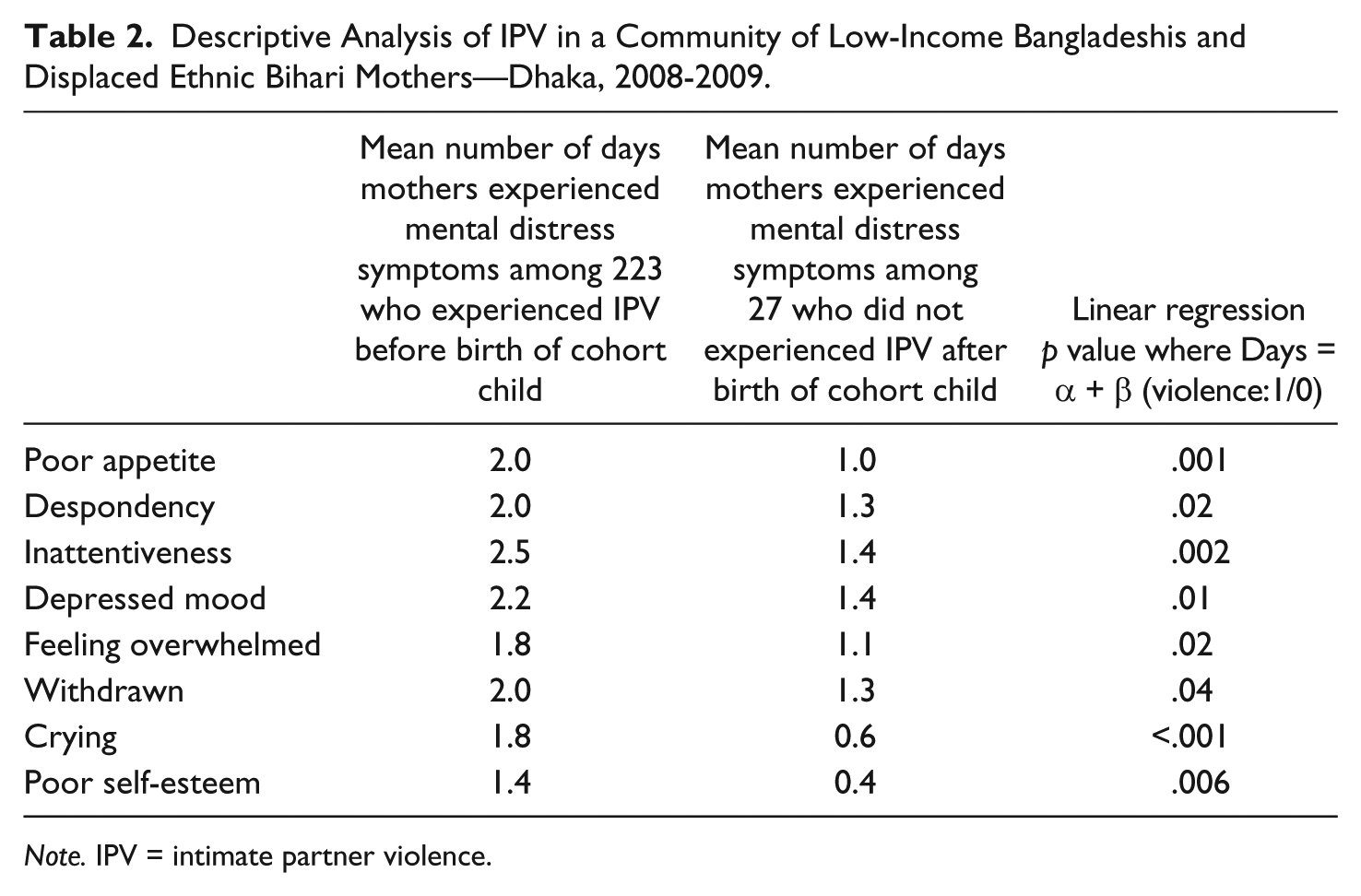
Note. IPV = intimate partner violence.
Discussion
Our survey of birth-cohort mothers suggests that IPV is a common occurrence in this community of low-income Bangladeshis and displaced ethnic Biharis. The majority of mothers interviewed had experienced most forms of IPV during their relationship, both before and after the birth of their cohort child. Only a few mothers reported that IPV began for the first time after the birth of their child. The occurrence of IPV was higher in this study population than that reported in previous surveys from Bangladesh (Heise & Garcia-Moreno, 2002; icddr, b, 2006).
This disproportionately high IPV burden may have been exacerbated by the community’s low income and low education. Studies by Naved and Persson (2005) and Naved and Akhtar (2008) have also previously documented a high level of acceptance and justification of IPV by 48% of women surveyed in low-income Dhaka communities when compared with those surveyed in district municipalities (32%). Limited legal rights and integration into the surrounding neighborhoods may have also increased displaced ethnic Biharis’ risk of IPV as has been identified in other minority communities (Azziz-Baumgartner, McKeown, Melvin, Dang, & Reed, 2010).
Mothers who experienced IPV were more likely to report symptoms compatible with mental distress. Although this is the first time that such an association is demonstrated in Bangladesh, previous multi-country WHO studies have suggested that IPV is frequently associated with mental distress and depressive symptoms (Campbell et al., 2002; Crofford, 2007; Ellsberg, Jansen, Heise, Watts, & Garcia-Moreno, 2008; Heise & Garcia-Moreno, 2002). Long-term follow-up of the cohort mothers or older female household members may reveal a pattern of chronic medical problems (e.g., generalized anxiety disorder) and economic burden related to IPV typically identified in other studies (Campbell et al., 2002; Crofford, 2007).
Limitations
This study has several limitations. The IPV questionnaire was not designed to quantify the number of IPV events, thus making it difficult to stratify among women who frequently experienced IPV versus those who seldom experienced IPV. The unexpectedly high proportion of mothers victimized made it difficult to explore anticipated risk factors for IPV and maternal distress (i.e., young maternal age, relative lack of wealth, lack of education, female birth cohort child, and household crowding) among the 95% of exposed and the 5% of unexposed mothers during our limited 1-year follow-up. In addition, we believed that mothers would correctly recall whether IPV had occurred before or after the birth of the child, an assumption that may have been accurate only when IPV was particularly severe and not affected by memory loss associated with the puerperium. We could not censor the person-time of the two mothers who experienced new-onset IPV in their relationships after the birth of their cohort child because we did not assess when their victimization began. Such a limitation would underestimate the rate of IPV by overestimating the person-time. We may have also underestimated rates because of under-reporting of IPV due to the stigma associated with disclosure and because we estimated the incidence of IPV among participants who were older than the typical age when victimization begins. Last, our survey was not intended to diagnose clinical depression or post-partum depression, but merely serve as a marker of maternal distress.
Conclusion
Our data suggest that IPV is a common occurrence in this low-income community of Bangladeshis and displaced ethnic-minority Biharis, where these events may occur more frequently than in other communities of Bangladesh. As has been previously described, young mothers were frequently victimized by male partners through physical, sexual, and emotional abuse. Mothers who reported IPV were more likely to report symptoms compatible with mental distress. The disproportionately high burden of IPV in these communities suggests that a better understanding of risk factors for victimization and perpetration of IPV may help the public health community develop and target interventions for these vulnerable communities (Hadi, 2005; Pronyk et al., 2006).
Footnotes
Appendix A
Exploring Risk Factors for Intimate Partner Violence During 1 Year Among 250 Young Low-Income Bangladeshis and Displaced Ethnic Bihari Mothers—Dhaka, 2008-2009
| Independent variables a | Coefficient | SE | t | p value | Lower 95% CI | Upper 95% CI |
|---|---|---|---|---|---|---|
| Maternal age | 0.03 | 0.03 | 0.87 | .39 | −0.04 | 0.10 |
| TV | −0.51 | 0.49 | −1.03 | .31 | −1.48 | 0.47 |
| Cell phone | −0.48 | 0.53 | −0.91 | .36 | −1.53 | 0.57 |
| Mother’s level of education | −0.21 | 0.30 | −0.70 | .49 | −0.81 | 0.39 |
| Father’s level of education | −0.01 | 0.25 | −0.02 | .98 | −0.50 | 0.49 |
| Birth cohort child’s gender | −0.05 | 0.44 | −0.10 | .92 | −0.92 | 0.83 |
| Household size | −0.46 | 0.24 | −1.92 | .06 | −0.93 | 0.01 |
| Constant | 9.82 | 1.31 | 7.50 | .00 | 7.23 | 12.42 |
Note. The dependent variable is intimate partner violence (IPV) composite score: We added one point for each type of violence participants ever experienced in the current relationship to generate a composite score, which we analyzed as a continuous variable (possible scores ranged between 0 and 13). CI = confidence interval.
Linear regression model: Composite IPV score = α + β1 (maternal age) + B2 (TV ownership) + B3 (cellular phone ownership) + B4 (mother’s level of education) + B5 (father’s level of education) + B6 (birth cohort child’s gender) + B7 (household size).
Appendix B
Exploring Risk Factors for Composite Mental Distress Score During One Year Among 250 Young Low-Income Bangladeshis and Displaced Ethnic Bihari Mothers—Dhaka, 2008-2009
| Independent variables a | Coefficient | SE | t | p value | Lower 95% CI | Upper 95% CI |
|---|---|---|---|---|---|---|
| Intimate partner violence (IPV) composite score | 1.65 | 0.57 | 2.89 | .01 | 0.52 | 2.78 |
| Maternal age | −0.08 | 0.22 | −0.34 | .73 | −0.51 | 0.36 |
| TV | 1.98 | 3.15 | 0.63 | .53 | −4.25 | 8.21 |
| Cell phone | 2.93 | 3.37 | 0.87 | .39 | −3.75 | 9.60 |
| Mother’s level of education | −1.02 | 1.93 | −0.53 | .60 | −4.84 | 2.80 |
| Father’s level of education | −1.44 | 1.58 | −0.91 | .36 | −4.57 | 1.69 |
| Birth cohort child’s gender | 2.39 | 2.81 | 0.85 | .40 | −3.17 | 7.95 |
| Household size | 1.17 | 1.54 | 0.76 | .45 | −1.88 | 4.21 |
| Constant | 3.01 | 10.02 | 0.30 | .76 | −16.83 | 22.85 |
Note. The dependent variable is composite mental distress score: We added the days during which participants reported symptoms compatible with mental distress and subtracted the days during which participants reported symptoms compatible with emotional well-being to generate a composite mental distress score for the week prior to the interview. CI = confidence interval.
Linear regression model: Composite mental distress score = α + β1 (composite IPV score) +B2 (maternal age) + B3 (TV ownership) + B4 (cellular phone ownership) + B5 (mother’s level of education) + B6 (father’s level of education) + B7 (birth cohort child’s gender) + B8 (household size).
Acknowledgements
We acknowledge Tapon Kumar Bose, Dorothy Southern, Emily Gurley, and the Mirpur surveillance and cognitive teams for helping us gather and prepare the study findings for publications. We would like to especially thank participating mothers for their candor in discussing this difficult issue with the study teams. International Centre for Diarrhoeal Diseases Research, Bangladesh (icddr, b) also acknowledges with gratitude the commitment of Centers for Disease Control and Prevention (CDC) and National Institutes of Health (NIH) to its research efforts.
Authors’ Note
The opinions expressed by the authors contributing to this article do not necessarily reflect the official position of the Centers for Disease Control and Prevention (CDC) or the institutions with which the authors are affiliated.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the U.S. Centers for Disease Control and Prevention (CDC), Grant U01/CI000628-02, and the National Institutes of Health, USA (NIH), Grant 5R01 AI043596.