
Abstract
This article draws on the power of creative methods to call for a more collaborative, ecological approach to awareness, education, and research analysis of Borderline Personality Disorder (BPD). Drawing on affect theory and empirical research using a co-creation methodology, we advocate for the power of peer-directed support provision for those experiencing BPD. Through recognition and advocacy for this emerging area, the article advances the ways in which more holistic, ecological protocols can help shift research into BPD from a deficit-framed diagnostic approach to a more strengths-based agentic approach that recognizes the wider context and multiple factors beyond the individual.
Keywords
Introduction: BPD’s Defective Discourse
A borderline personality disorder (BPD) diagnosis is often accompanied by strong negative associations within health settings and often poor outcomes. For many diagnosed with BPD, it is hard “to say anything positive” in relation to treatment and stigma they experience health settings (Carrotte et al., 2019, p. 531). Lived experience advocates and consumers 1 have noted a BPD diagnosis can feel as though one possesses a spoiled or defective identity (Lovell & Hardy, 2014; Ng et al., 2019; Whynacht, 2018). This may be due to the highly stigmatized nature of this disorder. The entrenched stigma surrounding a diagnosis of BPD is well-documented, with a large body of literature capturing the negative attitudes of health professionals toward consumers. Health professionals have been found to interpret patients’ actions as manipulative, chaotic, impulsive, and malicious (D. W. Black et al., 2011; G. Black et al., 2014; Day et al., 2018; Deans & Meocevic, 2006; Markham, 2003). The ubiquitous use of the term “manipulative” by health professionals to describe those with a diagnosis of BPD offers an historical window into the pervasive bias shown in the clinical BPD literature (Lewis & Appleby, 1988; Potter, 2006).
The influential 1988 study Personality Disorder: The Patients Psychiatrists Dislike found psychiatrists regarded the suicidal behavior of patients diagnosed with a personality disorder as “disingenuous, noncompliant, annoying and undeserving of resources” (Lewis & Appleby, 1988, p. 47). Similar findings were made during a 2016 experimental study, where 265 clinicians were asked to give a diagnostic assessment after watching footage of a woman describing her experience of uncomplicated panic disorder (Lam et al., 2016). Three groups of clinicians were provided with different information on the patient’s background. The group given information that this patient had a previous diagnosis of BPD, adopted a more negative attitude toward the patient, assuming a poorer prognosis for the participant (p. 263).
Clinicians treating those with BPD have likened the disorder to a form of “emotional haemophilia,” in which individuals are “lacking emotional skin” (Kreisman & Straus, 2010, p. 19). Consequently, people living with a diagnosis of BPD have been typified as violent, chaotic, and dangerous (usually) women, who pose the threat of countertransference to professional staff (Holmes, 2003, p. 528). One therapist noted treating BPD was analogous to “encountering those Dementors in Harry Potter. Borderlines suck the life right out of you’” (Lester, 2009, p. 285). Tanya Luhrman’s (2000) ethnographic research conducted in American psychiatric facilities highlighted the way in which psychiatric staff stereotyped people living with a diagnosis of BPD as defective and deviant women who can be detected through the “meat-grinder” sensation: . . . if you were talking to a patient and felt as if your internal organs were turning into hamburger meat (you felt scared; you felt manipulated by someone unpredictable; still, you liked her), that patient most likely had a borderline personality disorder. (p. 113)
This defective discourse constructs the poor life outcomes, long-term suffering, and self-destructive behaviors of those diagnosed with BPD as the result of an individual’s moral failing. A mother who acted as a carer for her daughter diagnosed with BPD in the Australian public health system explains: The term, “borderline personality disorder,” it sort of implies that there’s something lacking in the individual. There’s something defective in the individual. When, in fact, in my experience, a lot of it is a response to unacceptable levels of trauma. (Carrotte et al., 2019, p. 530)
When behaviors of individuals diagnosed with BPD are perceived through the lens of this defective discourse, they can have tangible effects on the treatment that patients and their families receive. Those with BPD diagnoses have reported that they frequently experience discrimination, dismissive attitudes from hospital staff, as well as poor treatment and care when presenting at emergency departments (Fallon, 2003; Vandyk et al., 2019). A study conducted in Melbourne, Australia, demonstrated 89% of a sample of 47 registered psychiatric nurses working in community and inpatient psychiatric units perceived those diagnosed with BPD as manipulative (Deans & Meocevic, 2006). Self-injury and preoccupation with suicidality associated with BPD are often interpreted by mental health professionals as forms of emotional blackmail and attention-seeking behaviors, which are undergirded by the intention to manipulate others (Deans & Meocevic, 2006; Warne & McAndrew, 2007). In addition, an Australian BPD survey demonstrated three quarters of respondents waited more than 4 hours for treatment of self-injury in Australian emergency departments (Lawn & McMahon, 2015, p. 517). This compared to half of general patients who present at Australian emergency departments receiving treatment within 19 minutes of their arrival (Australian Institute of Health and Welfare, 2013; Lawn & McMahon, 2015, p. 517). Unsurprisingly, people living with a diagnosis of BPD, their families and advocates have expressed the urgent need for more honest, compassionate, and sensitive treatment from health professionals and hospital staff (Carrotte et al., 2019; Lawn & McMahon, 2015; Vandyk et al., 2019).
These frequent negative interactions with health professionals can create a looping effect, in which people who experience poor and dismissive treatment can engage in increased self-destructive behavior “to gain power over life, death and the environment and trying to make people listen” (Lovell & Hardy, 2014, p. 236). Self-destructive behaviors can, in this context, be understood as a “weapon of the weak” (or vulnerable), where marginalized individuals engage in methods of resistance to make their “political presence felt” in spaces where they feel threatened, invalidated, and misunderstood (Scott, 1987, p. xvii). The behavior of those with a diagnosis of BPD can thus be reimagined to “indicate enormous resilience, adaptation, creativity, and a struggle to survive environments that have been invalidating, abusive, or erasing” (Lester, 2013, p. 72).
Co-Design, Creativity, and “Consumer” Research: Mad About Mad Studies
Treatment in health settings and emergency departments is not the only area those with a diagnosis of BPD experience exclusion and stigma. Both in education settings, and in research scholarship, the experiential knowledge of people with lived experience, their families, and advocates, has largely been excluded. Clinical studies position medical practitioners as singular credible knowers, who interpret, and draw meaning from patients’ behaviors through a largely hierarchical biomedical lens (Blencowe et al., 2018; Lock & Nguyen, 2010). Patients’ inclusion in these texts has often been relegated to short case studies and vignettes recording their behaviors. Yet this is now beginning to substantively change, with the emergence of consumer-led research, co-design research methodologies, and mental health activist scholarship, including “mad studies.”
The emerging discipline of mad studies offers a rich critique of the absence of lived experience perspectives in mental health research (Beresford, 2002; Ingram, 2016; Menzies et al., 2013). Mad studies argues that the devaluing and exclusion of lived experience perspectives can result in the obfuscation of unequal power relationships, abuses of power and the sidelining of personal and socio-cultural accounts of creative, every day, and spiritual aspects of identity (Faulkner, 2017; Faulkner et al., 2021; Russo & Beresford, 2015). Scholars in this field have advocated for various participatory methodological approaches which situate “expertise by experience” at the forefront of knowledge production (Gillard et al., 2010, p. 1127; Sweeney and Beresford 2009, 2019). These approaches include: coproduction (Gillard et al., 2010; Roper et al., 2018), survivor-led research (Sweeney et al., 2009), consumer leadership (Happell & Roper, 2006), Community-Owned and Managed Research [COMR] (K. A. Jones, 2012; N. Jones et al., 2014), and participatory action research (Ochocka et al., 2002). Broadly speaking, these approaches seek to value consumers’ experiential knowledge through the implementation of a nonhierarchical research design where consumers actively and meaningfully contribute to the production and dissemination of knowledge that enacts social change (King & Gillard, 2019; Slay & Stephens, 2013), not simply act as informants or advisory members (as in our study).
Co-design (or co-production) involves embedding consumers as equally valued lead researchers, team members, or co-researcher panel members throughout the planning, design, delivery, and evaluation stages of the research project (Pinfold et al., 2015; Roper et al., 2018). Survivor researchers argue emancipatory research approaches offer a more empowering and ethically robust way for consumers/survivors to share experiential knowledge, compared to methods of user-involvement research and participation (Campbell, 2005; N. Jones et al., 2014; Rose, 2017). Studies which use user-involvement have been critiqued as depoliticizing and disempowering, due to their preoccupation with micro-politics and failure to address the macro-political structures underpinning survivors and consumers lives (Beresford, 2002; King & Gillard, 2019).
The rise of the consumer perspective has come to be valued by governments, advocacy bodies, and academic research institutions (Daya et al., 2020). The involvement of academic consumer researchers (ACRs) has been shown to result in more nuanced ways of conceptualizing mental illness, education, and service delivery (Harris and Thompson 2020; Faulkner, 2017, p. 509), the improvement of participant recruitment and retention, and the increased real-world impact of research outputs (Happell et al., 2018). Nonconsumer researchers argue that ACRs conduct research in a “forceful and committed way” with their contributions getting to “the significance of things” (Happell et al., 2018, p. 1235). Despite the benefits of consumer-led research, consumers’ efforts to theorize, analyze and produce research outputs are often frustrated by lack of funding and publication opportunities, as well as exclusion from peer-reviewing processes (Rose et al., 2018; Sweeney & Beresford, 2019). Co-design with consumers has often been critiqued as “ad hoc, sporadic, and often tokenistic” when undertaken in practice (Happell et al., 2018, 1231; Read & Maslin-Prothero, 2011). In addition, survivor-led research has been criticized as lacking diversity due to the exclusion of the perspectives of those from racially diverse backgrounds (King & Gillard, 2019).
How Can These Co-Designed Processes and Products Help Educate Differently?
Creative and co-designed methods offer a way to conceptualize and communicate consumers’ experiences beyond traditional moral panic, deficit-framed or “patient porn” approaches. Recovery narratives can valorise notions of self-control and self-regulation, often asking consumers to condense and refashion ambiguous, temporally fragmented, traumatic and highly emotionally intense experiences into individualized, neat, and digestible episodic tales for audiences to consume (Recovery in the Bin, 2019). As Figure 1 shows below, arts-based methods can create environments which encourage and foster forms of creative expression instead of the production of bounded, linear forms of self-narrativity (Strawson, 2004). Daniel Harris (Author 1) has lived experience of both BPD and academic scholarship, and has written about the benefits of collaborative writing and creative methods elsewhere (Thompson & Harris).
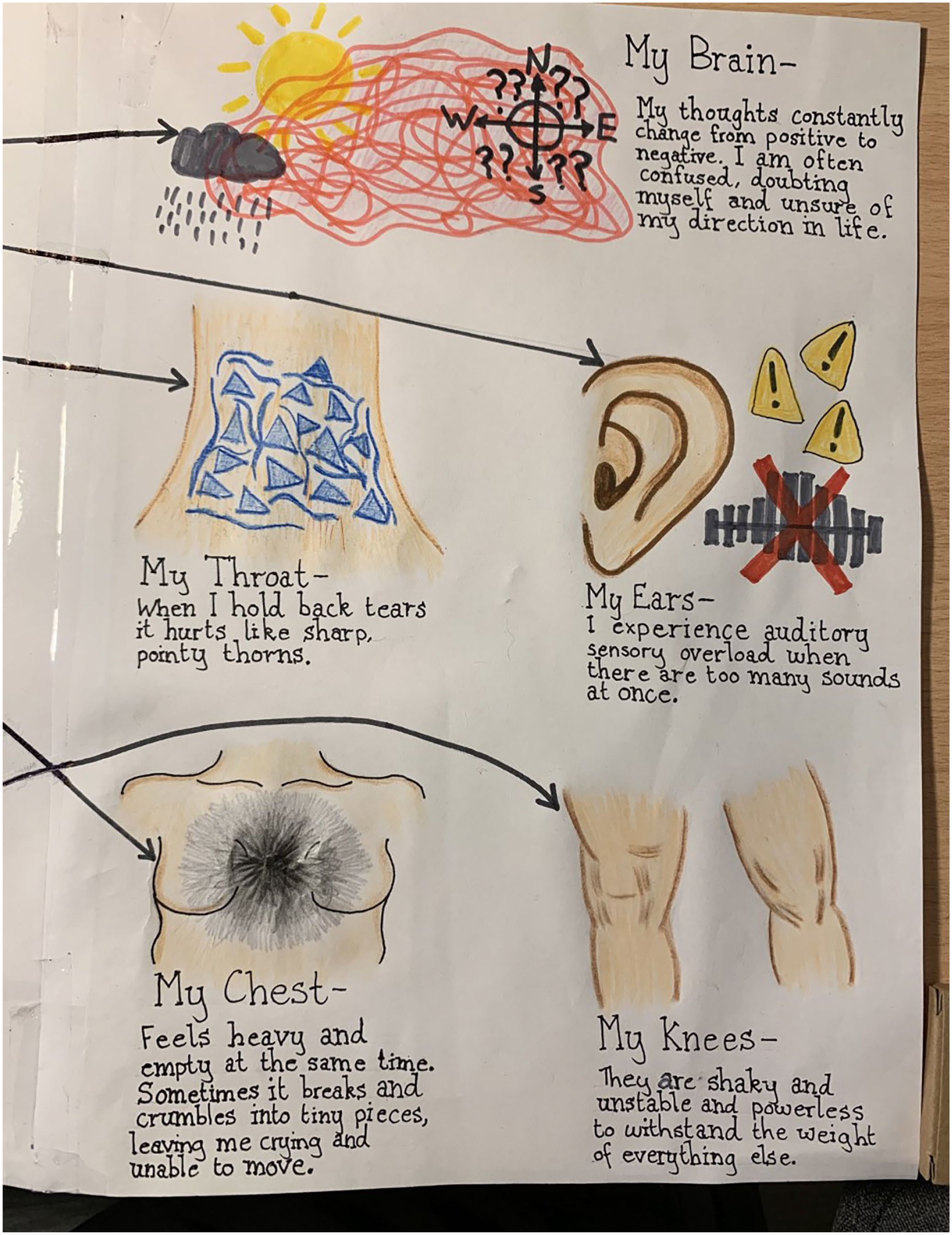
Body Drawing.
Sociologist Ardath Whynacht found this when she conducted a series of arts-based workshops with 16 participants living with a diagnosis of BPD (Whynacht, 2018). The study employed visual art, poetry, and drawings to express and validate participant’s experiences. Whynacht’s creative, participatory methods allowed the research to move beyond the “Black/White moralisms” associated with BPD and its public image (19). A 2015 study also utilized arts-based methods, employing collages and objects as mechanisms for participants to express their life story of living with BPD (Larivière et al., 2016). We acknowledge the need for further work in this area, with an increased focus on diversities within participant groups (importantly, of gender, race, and age diversity).
Harris advocates using a “creative ecologies” framework (Harris, 2021) to mental health research, an approach which decentres the individual and focuses instead on the whole environment (ecology) in which the consumer lives. The framework highlights five P’s of interest: partnerships (people), place, processes, products, and policies. There is a dearth of BPD research that equally focuses on so many factors in the lived experience of those with BPD, rather than solely on the individual. By decentring the consumer, a creative ecological approach to treatment acknowledges the many factors at play (both past and present) and identifies multiple areas of focus for attention.
Materials and Methods: This Study
The arts-based workshops which are the focus of this article were part of a larger interdisciplinary study exploring the lived experiences of individuals diagnosed (or self-diagnosed) with BPD. The focus of the broader research was to explore how a diagnosis of BPD is co-produced alongside sociocultural dimensions, familial, and community relations, health care treatments and supports, and interactions between practitioners and those with lived experience, particularly in relation to stigma and marginalization. Consistent with a creative ecological approach, this research positions a diagnosis of BPD as socio-material co-produced phenomena, one that is rooted in social disadvantage, marginalization, gender inequalities, and complex trauma. The study was approved by [anonymised] University Human Research Ethics Committee.
The arts-based workshops provided a creative platform and art-based tools to support people living with a diagnosis of BPD to explore various aspects of their experience. The workshops were delivered in the second phase of the larger study by the authors. They followed the completion of a nation-wide qualitative survey that provided an anonymous platform for participants to share aspects of their experience of living with BPD. Following the survey, a yearlong period of arts-based workshops deepened the team’s understanding of affective and embodied aspects of lived experience, after which the third phase of this research, consisting of narrative interviews with lived experience participants and health practitioners, commenced.
The arts-based component of the research included a series of eight arts-based workshops focusing on storytelling (two workshops), filmmaking (two workshops), visual making (two workshops), and creative movement (more than one workshop) tailored specifically to explore lived experience of a diagnosis of BPD via arts-based methods. Owing to COVID lockdowns, the workshops were held in a variety of formats, with the first workshop in July 2021 in person, three workshops held entirely online via Zoom and four hybrid workshops with some participants attending in person and some attending online. Following feedback from participants in the first workshop, the timeframe for the sessions was expanded from 3 to 4 hours. The sessions were offered (mostly) monthly across 2021 and 2022 as follows:
Workshop 1: Storytelling Workshop 3 July 2021, (3 hours, in person)
Workshop 2: Storytelling Workshop 1, 14 August (4 hours, online)
Workshop 3: Visual Storytelling and Filmmaking, 4 September 2021 (4 hours, online)
Workshop 4: Zoom Filmmaking, 9 October 2021 (4 hours, online)
Workshop 5: Visual Making, 27 November 2021 (4 hours, hybrid)
Workshop 6: Visual Making, 5 March, 2022, (4 hours, hybrid)
Workshop 7: Reflection and Analysis, 19 March, 2022 (4 hours, hybrid)
Workshop 8: Creative Movement, 9 April, 2022 (4 hours, online)
Participation
We had a total of 15 participants across the workshops. Most participants took part in more than one workshop, and five participants took part in more than four of the workshops. The number of participants per workshop varied from 5 to 12. The workshops held online during COVID-19-related lockdowns had larger participation compared to in-person and hybrid workshops facilitated following the lockdowns.
Participant Demographics
Out of 15 participants across all arts-based workshops, 12 identified as female, two as male and one participant identified as nonbinary. Their age range was between 22 and 48 years old, with most participants in the age group 22 to 35. All participants lived in metropolitan environment, and all but two participants had achieved university-level education. One had completed compulsory education and one had below university-level education. Only 2 participants were not employed in some capacity during the workshop period, while others studied and worked, in a part time or full-time capacity. Only four participants were in long-term partner relationships (married or de facto) at the time of this research, and the remaining 11 were declaring as single. Five participants identified as heterosexual, three as bisexual, two as queer and two as pansexual. Three participants chose not to disclose their sexuality. Thirteen of the participants had been given a diagnosis of BPD by a health professional and were receiving some kind of treatment (medication, therapy, case management etc.), one was self-diagnosed with BPD, and one was uncertain whether BPD was one of psychiatric diagnoses they were previously given but assumed it was.
Facilitation
The storytelling, filmmaking, visual making, and analysis sessions were facilitated by Dan Harris and Stacy Holman Jones. Tamara Borovica led the creative movement session.
The following is a brief outline of the workshops format, and consistency was important. When considering a creative ecological approach, “processes” often includes the need for collaboration and consistency in order to foster the best context for creative expression.
Workshops Format
Welcome, acknowledgment of country, and introductions.
Background on the research project/permissions and requests to share artworks and (in the case of the online sessions) to record the Zoom session.
Development of and additions to our guidelines for working together: People are free to communicate about their experience. People are free to not participate in activities/take a break and come back later. What is said in the session stays in the session. No talking while someone else is speaking.
Links to support services, should participants experience discomfort or distress.
Artmaking activities.
Check out and next workshop announcement.
Each workshop included a series of three to four artmaking activities in the medium, designed to (1) encourage participants to both get comfortable with/experiment with the artform and (2) to explore various facets of lived experience associated with a diagnosis of BPD. For example, in a storytelling workshop, participants worked with metaphor to write about their experiences of living with BPD in exercises like “The Town,” (see Figure 2) which asked them to imagine their BPD as a place they inhabit. In creating their stories or poems (and in one case a song), they were asked to consider the town’s name, ecology, architecture, and people, and to consider questions such as What thrives in a town like this? Who or what is its mayor? What is considered a crime? What is considered a gift? What is the soundtrack? What is the sky filled with? What runs in the rivers and streams? What is empty or vacant? What is too plentiful?
The Town of No Regrets.
In a filmmaking workshop held on Zoom, participants were invited to create their own “BPD How-to Shows” using the format of a cooking show. Participants considered, for example, how they used cooking as a source of meditation or a way to express themselves or to make a how-to video to demonstrate the complexities of navigating lived experience of BPD (in one case humourously trying to follow hundreds of instructions supplied in DIY macrame kit).
In a visual making workshop, participants “Make a (healthy) meal of BPD” by creating a salad that they felt communicated something about their experience of BPD. They did this by choosing from among a number of salad ingredients and assembling a salad, considering the elements that make up their BPD experience. These ingredients included superpowers, skills, best qualities you want a lot of/are good for you (and others) as well as qualities you prefer to have in limited quantities (for flavor, for a bit of spice, etc.). They shared and photographed their salads and then ate their creations in a community lunch.
In a creative movement workshop held on Zoom, participants were invited to listen to, explore and make movement from sensations and feelings as encountered in the body. They were guided to make short individual dance performances inspired by bodily exploration of how BPD “feels” in their body in general, how it feels on a particularly good day and how it feels on particularly bad day. The participants were offered an embodied, creative medium in which to explore and express their emotional experience without needing to make it “intelligible” to others. In this way, creative movement or dance as a medium was utilized for its capacity to work with emotionality and imagination and to emphasize nonverbal experiences associated with BPD in a creative, playful way.
In session 7, we invited participants in the previous six workshops to reflect upon and analyze their experience in the workshops and the storytelling, film, and visual artworks created. In this workshop, participants worked in pairs to choose and reflect on a collection of three visual artworks (photos, paintings and drawings), three pieces of writing, and two videos made by other participants. They were asked to identify:
Emergent themes common throughout the artworks.
Anything that seems to be missing or absent from the artworks.
How the particular art form helps express aspects of BPD (including discussing how art forms might lend themselves to exploring certain kinds of emotion/experience).
What kinds of arts methods seemed to work best/be chosen the most, and why.
The group discussed their responses to these prompts for each of the rounds, collectively summarizing their insights and identifying themes that emerged across the discussion of artworks/forms of making, including, in some cases, discussion of the policies that impact those living with BPD. Insights generated by the participants regarding individual art forms are discussed in the following section.
Results and Discussion
The participants discussed how each distinct modality affords different ways of communicating their meaning, from those which speak to audiences clearly and directly, to those modalities better suited to leaving things open to interpretation and expressions of emotional fragmentation.
Visual Methods and Artworks
Convey a sense of bodily experience/sensation and emotions, without words getting in the way.
Create a bridge between image and text.
Provide a “way in” to sensemaking and understanding.
Show varied experiences, and not only extremes.
Highlight relationships and loneliness as existing simultaneously.
Written Methods and Artworks
Create a sense of mystery/unfolding of experience.
Show the “other side” of experience.
Show how things work/processes in motion.
Facilitate affirmation.
Give a sense of flow and patters of movement.
Allow for compression of experience into sharp focus.
Allow direct communication to an audience/reader.
Are a vehicle for metaphor and dichotomy.
Filmmaking Methods and Artworks
Use metaphor/objects/the natural world to create context.
Enable the creative use of humor.
Show people as instructors/teachers and as such can be used to educate.
Show “living with” BDP and don’t focus on extremes.
Show people as heroes, not villains.
Show layers of BPD experience—for example, conveying the “dark side” of BPD as “there but not there” and “show the impossible while conveying a sense of calm.”
Some of the themes and insights that the group identified as operating across artmaking multiple methods and works included:
Showing what’s not said/what you can’t see leaves a viewer wanting more (i.e., are spaces that resist a “complete” picture or beginning/middle/end format).
Doing something “by hand” shows patterns of mind and movement of bodies in the moment (see Figure 3).
Artworks create a desire to hear the artist’s voice/see the artist’s body and/or experience that physicality through the medium.
Arts media help in showing the differences within BPD experience (i.e., conveying a sense of departure from “normative” or “stereotypical” understandings while underscoring how we can still be “more alike than unalike”).
Arts-based methods and artworks emphasize the importance of removing/sidestepping judgment.
Artworks can show the “other side” of a duality/create complexity and nuance.
Artworks evoke the importance of creating/showing temporality (ie “how things come and go”).
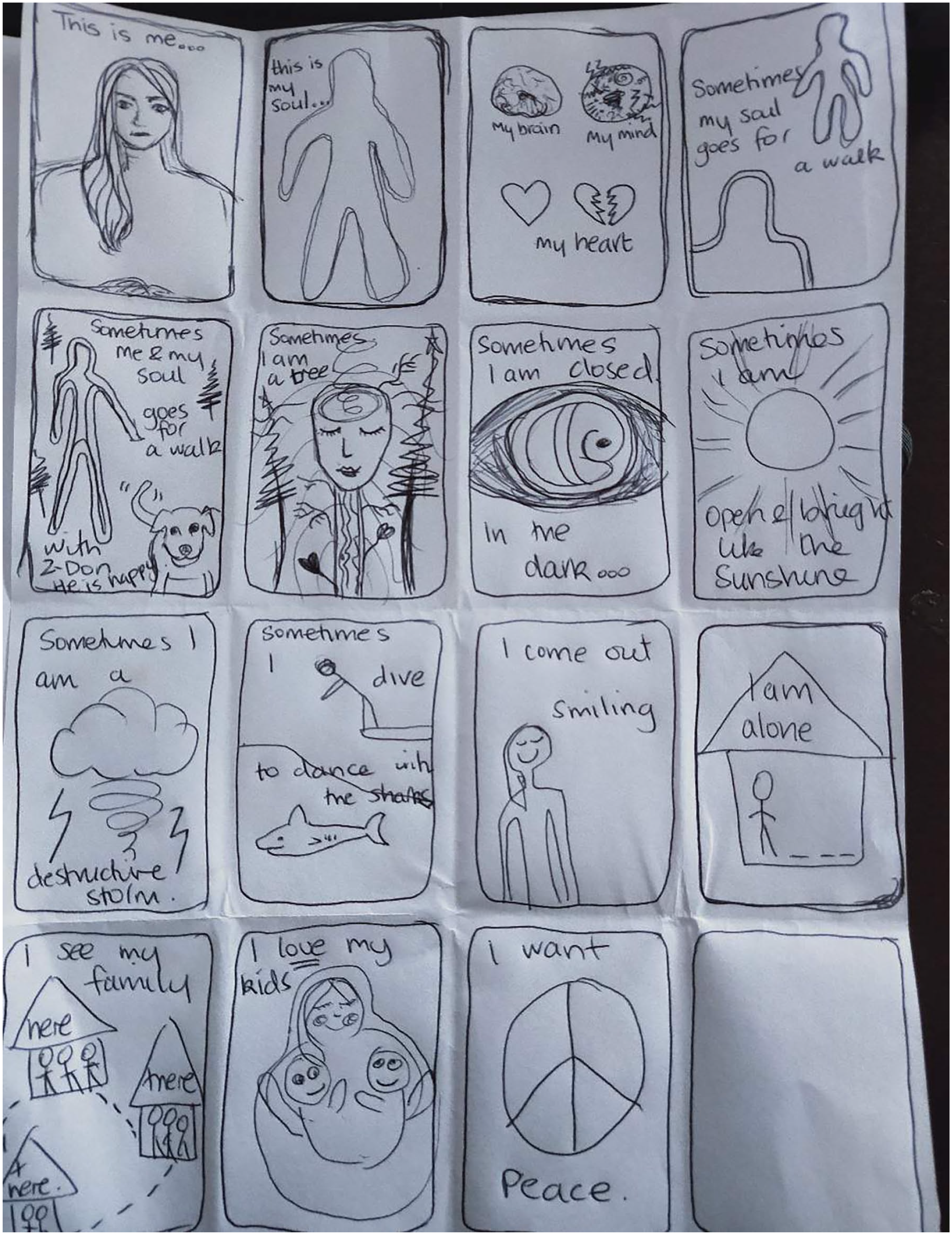
Graphic Novel of Me.
Based on the analytic conversations generated in the session around individual art-making methods and outputs, participants shared the following general understandings and insights regarding arts-based methods making activities:
Combining methods (images, language and embodiment) helps build a sense of experience and/or tell a “stronger” story.
Arts-based methods encourage participants to “have a go” and not be judgemental about the results, especially for methods new to participants (Figure 4).
There’s an initial sense of fear/apprehension in trying new arts-based methods that transitions into a “sense of relief” in using the methods that is satisfying; this is an experience/skill that can be transferred to other aspects of life.
Arts-based works models the learning of a new skill/is therapeutic.
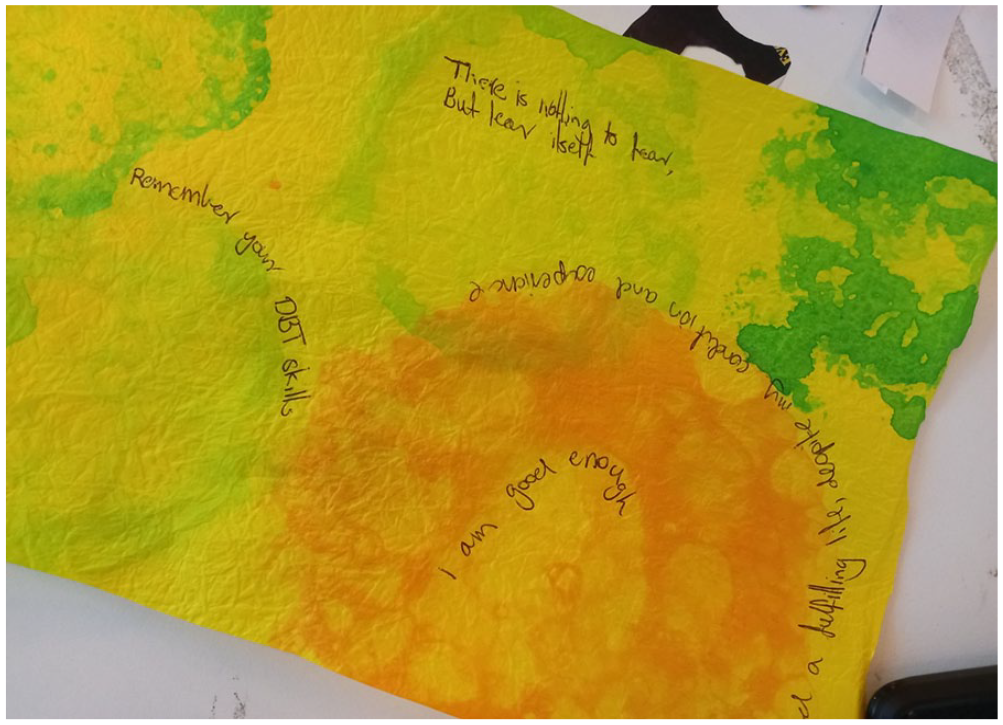
Watercolor and Writing.
In general, participants observed that they were able to use arts practices to communicate their experiences in new and/or fulsome ways. As one participant observed, “We’ve managed to create things that express what BPD is really like,” and to see things from a systemic (macro) view, rather than the pervasive individualist (micro) analysis that was more common in previous experiences.
Conclusion
In addition to and building on the insights generated by the participants themselves, our project team analysis noted that:
Arts-based methods are helpful in conveying both an intensity of emotions/relations and providing a more “neutral” or otherwise nonexpected portrayal.
The use of fragmentation in text-based arts methods and white space and or images only in visual, film, and creative movement methods signaled an openness to interpretation or questioning and worked to direct the attention of an observer.
The use of metaphor works as both a tool for conveying experience and as a way to move in between/across various arts-based methods.
Arts-based methods encouraged participants to explore difference and how distinctions are made, as well as what aspects of experience are excluded from expected or normative messages about BPD experience and how those exclusions matter.
Arts-based methods serve to create or invoke an (external) audience in relational to a personal or “internal” expressions of BPD experience.
Reviewing Harris’s (2021) “creative ecologies” framework as applied in this arts-based mental health research, we recognize the complexities of the multiple environments within which people with a BPD diagnosis live and become. This application offers a holistic and affective way to explore the five P’s that make up the creative ecologies framework (people, place, processes, products, and policies). In relation to people, we explore how the lived experiences of BPD feel, sound, move, look, and taste like for an individual and their immediate circles (i.e., “Graphic Novel of Me” activity). In relation to place, we explore socio-cultural and ecological contexts where BPD happens and what these places afford to a consumer in terms of self-knowledge, empathy, and living well (i.e., “Figure 2: 6 Word Memoir” activity). Processes were made more tangible when looking at relationships and events through which lived experience is enacted and lived (i.e., “Movement of BPD on a Good/Bad day” activity). Products and policies relate more closely to health and social care policies and practices were explored more directly in other phases of this study, although here they were inevitably identified as aspects of participants’ experiences of living with a diagnosis of BPD (i.e., “BPD How-to Show” activity). This way of exploring lived experiences of mental ill health decentres the individual and instead focuses on relations, events, and practices that contribute to shaping people’s lives.
There is considerable opportunity and growing interest in creative methods approaches to researching-with consumers and consumer-led projects, both inside and outside of academia. We acknowledge too the productive intersections between the rise in peer-support approaches to BPD care, and the efficacy of creative arts methods in this area. By extending these peer support and creative methods modalities into a more holistic creative ecological approach, research into BPD can begin to join personal lived experiences with the health provider partners, policies, and best practice processes for mental health improvement.
Footnotes
Acknowledgements
The authors would like to thank the participants who generously shared their experiences and to project partners for their generous support: National Mental Health Commission, Victorian Department of Health, Spectrum Personality Disorder and Complex Trauma Service, Orygen, Mind Australia, Mental Health Victoria, Lived Experience Australia and NEAMI National.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by an Australia Research Council Linkage Project grant (grant no. LP190100247).
Notes
Author Biographies
![]() . Harris is editor of the book series Creativity, Education and the Arts (Palgrave), and has authored, co-authored or edited 22 books and over 150 books and articles as well as plays, films and spoken word performances.
. Harris is editor of the book series Creativity, Education and the Arts (Palgrave), and has authored, co-authored or edited 22 books and over 150 books and articles as well as plays, films and spoken word performances.