
Abstract
While existing psychological maltreatment frameworks recognize verbally aggressive behaviors as a key mechanism of harm, childhood verbal abuse has not been independently operationalized as a distinct construct, complicating recognition and response across safeguarding systems. Prevalence estimates vary widely from 18% to 92%, reflecting inconsistent operationalization across studies. This study combined systematic review of 275 sources with expert consultation to establish a consensus-based definition. A six-round Delphi process involved 21 experts with lived experience or professional expertise in child health, education, or social care. Participants evaluated candidate definitions, behaviors, impacts, stakeholders, and actions until ≥70% consensus was reached. The panel endorsed 27 definitional components, 46 abusive behaviors, and 45 recognized impacts. Consensus identified 29 stakeholder groups and 19 recommended actions, prioritizing public awareness, parent education and teacher training. Experts endorsed subtle, digital, and indirect forms of abuse underrepresented in existing research. This study provides a structured, multidisciplinary consensus definition and framework for childhood verbal abuse developed through a process integrating lived experience perspectives. It offers a necessary complement to existing psychological maltreatment frameworks and a foundation for improving identification, prevention, and policy development across health, education, and social care systems.
Introduction
Verbal abuse has been loosely defined as “language intended to cause distress to the target” (Brennan, 2001). Examples include shaming, ridiculing, criticizing, belittling, threatening, and humiliating another person through spoken or written communication (Bernstein et al., 1997; Brennan, 2001; Teicher et al., 2006; Vissing et al., 1991). Such behaviors may be overt, as in explicit insults or threats, or more covert, emerging through chronic negative commentary that may be less visible to outsiders (Vissing et al., 1991). While verbal abuse can occur across the lifespan, it is particularly concerning in relationships characterized by emotional dependence or power imbalance (Wang & Kenny, 2014). Given the central role of language in communication and socialization during development, verbally abusive interactions may have significant implications for children’s emotional wellbeing and psychological development.
Exposure to verbally abusive caregiving environments has been associated with a range of adverse psychological outcomes. Immediate impacts include increased depression, anxiety, and attentional difficulties (e.g., Dube et al., 2023; Sharratt et al., 2023). Longer-term consequences include mood and personality disorders, psychological distress, eating disturbances, and heightened vulnerability to revictimization (e.g., Dube et al., 2023; Salwen et al., 2015). These outcomes may arise through mechanisms such as persistent shame, diminished self-worth, and the internalization of negative relational expectations (e.g., DeRobertis, 2012; Palazzolo et al., 2010). Chronic exposure has also been linked to difficulties in emotional regulation, interpersonal functioning, and cognitive processing, as well as behavioral outcomes such as anger, antisocial tendencies, and substance misuse (e.g., Brendgen et al., 2007; Kawabata et al., 2011; Teicher et al., 2016. These effects may extend into adulthood, influencing educational attainment, employment stability, and broader health outcomes (e.g., Felitti et al., 1998), and may also contribute to intergenerational transmission of harmful communication patterns (Greene et al., 2020). Together, these findings position childhood verbal abuse as a significant form of developmental adversity.
Within the child protection literature, verbally abusive behaviors are typically conceptualized within the broader framework of psychological maltreatment. Psychological maltreatment refers to repeated patterns or extreme incidents of caregiver behavior that convey to a child that they are worthless, unloved, unwanted, or endangered (Hart et al., 1996, 2019). Building on the American Professional Society on the Abuse of Children (APSAC), Slep et al. (2022) proposed an operationalized definition to support more consistent identification across child welfare, clinical, and legal systems. Importantly, specifying caregiver behaviors—rather than relying on the overarching label of psychological maltreatment—may improve communication with professionals, caregivers, and policymakers. Verbal abuse, as a communicative subtype of psychological maltreatment, is embedded within these frameworks but has not been independently operationalized as a distinct construct. This has practical consequences: even among professionals familiar with APSAC definitions, identification and reporting remain inconsistent, with only a minority of psychological maltreatment behaviors reliably recognized (Baker et al., 2021). A construct-specific definition of childhood verbal abuse is therefore a necessary complement to existing frameworks.
While verbal abuse is closely related to emotional abuse and psychological maltreatment, these constructs are not interchangeable. Psychological maltreatment encompasses a broad range of caregiver behaviors—including rejection, terrorizing, isolation, exploitation, and emotional neglect—that undermine a child’s emotional security (Hart et al., 1996; Slep et al., 2022). Emotional abuse, often used interchangeably in policy contexts, similarly includes non-communicative behaviors—such as exposing a child to domestic violence or using the child to meet the parent’s psychological needs—that extend beyond direct verbal interaction (Glaser, 2002). Verbal abuse may therefore be understood as a communicative subtype within these broader constructs.
A related construct—harsh or authoritarian parenting—occupies a contested boundary with verbal abuse. Harsh parenting involves coercive or punitive communication styles that vary across cultural and familial norms (Infante & Rancer, 1996; Wang & Kenny, 2014). Verbal abuse, by contrast, is distinguished by its gratuitous or extreme nature: communication that functions to degrade, intimidate, isolate, or undermine the child’s sense of self rather than guide behavior. Its identification therefore requires consideration of content, intent, function, frequency, and impact within the relational context.
Despite increasing recognition of its harms, childhood verbal abuse is rarely examined as a distinct construct. Instead, it is often subsumed within broader categories such as childhood maltreatment or emotional abuse (Glaser, 2002; Hibbard et al., 2012; Teicher & Samson, 2013; Warmingham et al., 2019). Widely used assessment tools, including the Childhood Trauma Questionnaire (Bernstein et al., 2003) and the Adverse Childhood Experiences checklist (Anda et al., 2010), incorporate verbally aggressive behaviors within broader emotional abuse items rather than measuring them independently. As a result, the conceptual boundaries of childhood verbal abuse remain inconsistently defined.
This lack of clarity has contributed to substantial variability in prevalence estimates, which range from approximately 18% to over 90% depending on measurement approach and definition (Bellis et al., 2014; Teicher & Parigger, 2015; Vissing et al., 1991). Such variation reflects not only population differences but also methodological heterogeneity, definitional inconsistency, and cultural variation in thresholds for recognizing harmful communication. In contexts where harsh verbal discipline is normalized or disclosure is discouraged, verbal abuse may be underreported or interpreted differently (Hamarman et al., 2002; Wang & Kenny, 2014). These inconsistencies hinder reliable estimation and limit shared understanding across professional systems. This ambiguity also has direct implications for identification, reporting, and intervention. Unlike physical or sexual abuse, verbally abusive communication occupies a more ambiguous boundary with normative parenting. Caregivers may perceive their behavior as discipline, while children experience it as degrading or threatening. These ambiguities are compounded by power asymmetries, which may inhibit recognition or disclosure. Without a shared conceptual framework, professionals may lack a common language for identifying verbal abuse, and children may struggle to interpret their experiences as harmful.
Developing a clearer conceptual framework may therefore improve both precision and practice. Treating verbal abuse as a communicative subtype within psychological maltreatment—rather than a diffuse component—may enhance measurement, increase visibility, and support targeted prevention strategies. Addressing this issue requires integrating multiple forms of expertise. Professionals across clinical, educational, and safeguarding contexts bring applied insight, while individuals with lived experience provide critical perspectives on how abuse is perceived and experienced. Without such integration, definitions risk limited relevance or legitimacy (Tseris, 2013). Incorporating these perspectives alongside academic evidence may strengthen both conceptual clarity and practical applicability (Harris & Fallot, 2001; National Institute for Health and Care Excellence, 2018).
To address these challenges, the present study employed a Delphi methodology to develop expert-informed consensus on childhood verbal abuse. The Delphi technique is widely used to establish agreement on complex or poorly defined phenomena through iterative rounds of structured feedback (Diamond et al., 2014; Hasson et al., 2000; Keeney et al., 2006). It also accommodates a broad conception of expertise, including both professional and lived experience (Taggart et al., 2025). The study aimed to: (1) develop a consensus definition of childhood verbal abuse; (2) identify associated behaviors and impacts; (3) determine relevant stakeholders; and (4) prioritize actions for organizational response.
Methods
Study Design
This study employed a two-phase modified Delphi method. In Phase 1 (item generation), participants independently generated items based on their knowledge and experience (Delphi Round 1), while academic and gray literature were reviewed in parallel to construct a comprehensive item pool. In Phase 2 (item refinement), this pool was iteratively rated, refined, and prioritized across Delphi Rounds 2–6 until consensus (≥70% agreement) was achieved. Alongside quantitative ratings, open-ended feedback was collected in Rounds 2–6 to support iterative refinement of items and subsequent analysis of areas of conceptual disagreement. Figure 1 provides an overview of the study process. Overview of the Delphi Study Process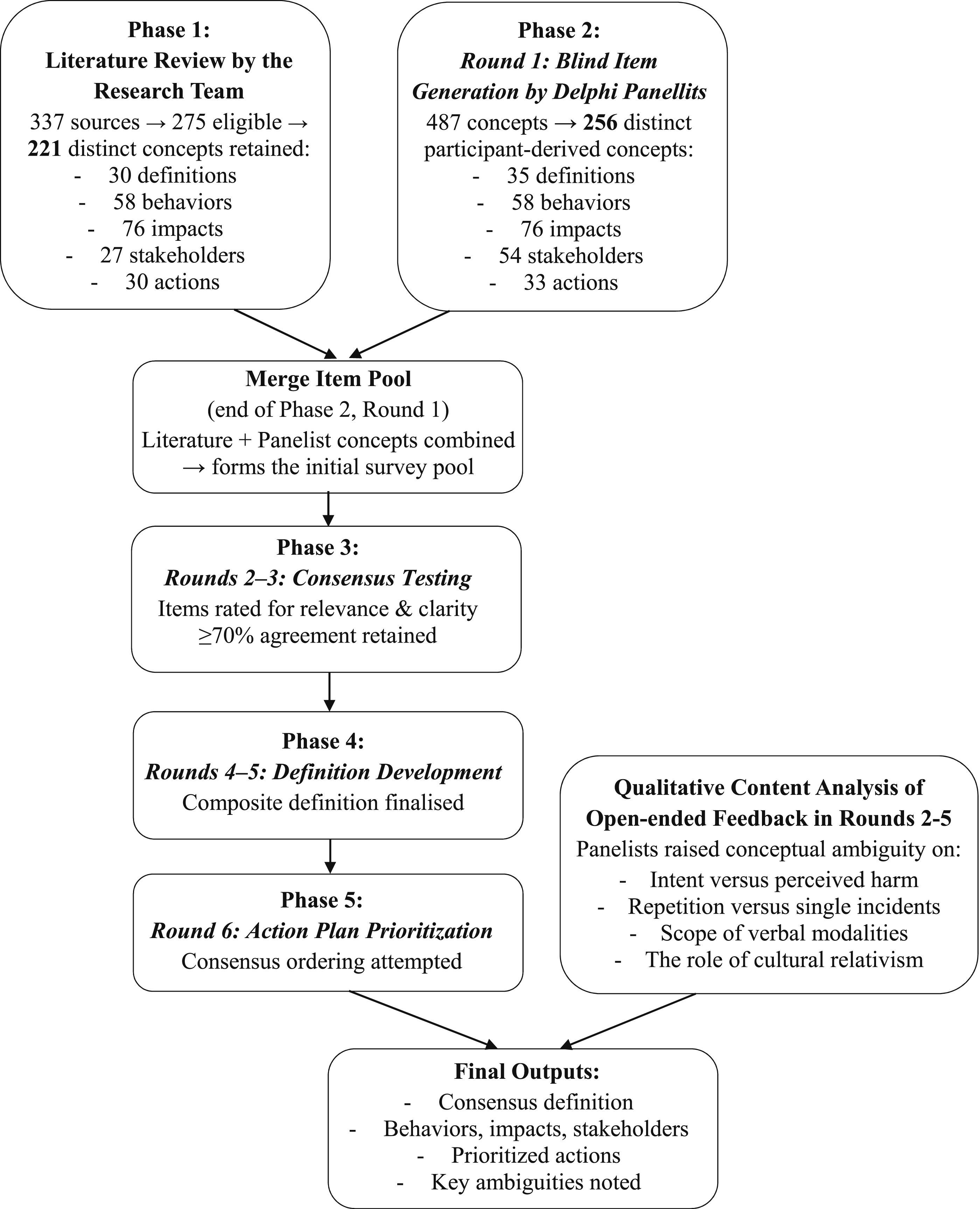
The Delphi method was selected due to its suitability for boundary-setting and the development of shared conceptual language, rather than causal inference (Diamond et al., 2014; Hasson et al., 2000). Its anonymity reduces the influence of participant seniority, while its iterative structure allows reconsideration of judgments in light of group feedback, supporting convergence while preserving disagreement (Keeney et al., 2006). Alternative approaches (e.g., nominal group technique, expert panels) do not offer this combination of anonymity, iteration, and accommodation of diverse expertise.
Participants
Participant Composition and Delphi Round Completion Across Expert Groups (N = 21)
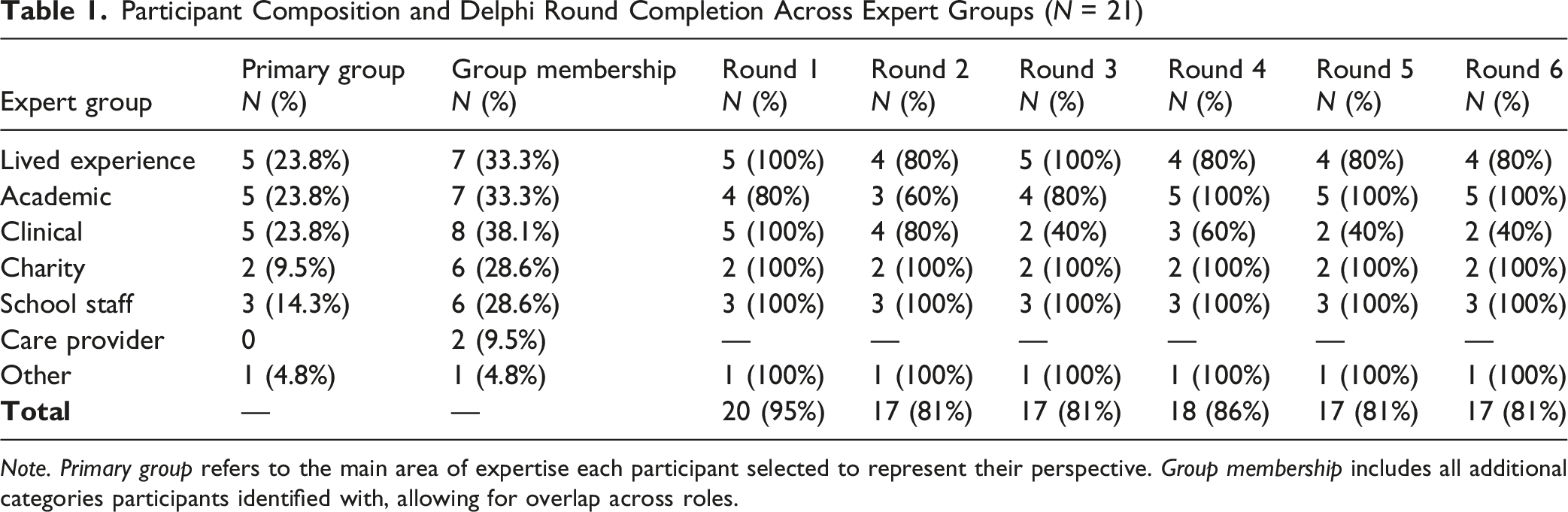
Note. Primary group refers to the main area of expertise each participant selected to represent their perspective. Group membership includes all additional categories participants identified with, allowing for overlap across roles.
The inclusion of participants across academic, professional, and lived experience backgrounds reflects a purposive approach to expertise consistent with established Delphi methodology (Hasson et al., 2000; Keeney et al., 2006). Within this framework, expertise is defined not solely by academic credentials but by relevant knowledge, experience, and capacity to provide meaningful insight into the phenomenon under study. Professionals including clinicians, educators, and social care practitioners bring applied expertise derived from direct work with children and families affected by verbal abuse. Individuals with personal experience of childhood verbal abuse constitute experts in their own right, offering knowledge of how such behaviors are perceived, experienced, and responded to that cannot be derived from professional or academic sources alone (Taggart et al., 2025; Tseris, 2013). Critically, the panel was convened to define, prioritize, and evaluate normative and practical questions, for which this breadth of expertise is not only appropriate but necessary. It was not tasked with adjudicating causal empirical claims, which remain the province of the empirical literature reviewed in Phase 1.
A total of 23 experts consented to participate. Two did not complete any Delphi rounds and were excluded, yielding a final sample of 21 participants. This group represented disciplinarily and experientially diverse forms of expertise across academia, clinical practice, education, charity work, and lived experience. Of these, 17 participants completed all six rounds, yielding a retention rate of 80.9%. Participants reported an average of 8.6 years in their current roles and included professionals from higher education, National Health Service (NHS) hospitals, schools, charities, and parent–child services. This mixed composition was intentionally designed to ensure that the outputs reflected both practitioner expertise and survivor perspectives, enhancing the practical relevance and legitimacy of the findings.
Ethical approval was granted by the University College London (UCL) Research Ethics Committee (ID: EP/2021/017). Informed consent was obtained from all participants. Pseudonymity was maintained throughout: participants’ responses were coded and only accessible to the research team, ensuring confidentiality while enabling iterative feedback. Participants could withdraw at any point.
Procedure
Participants received each survey round via individualized email links hosted on SurveyMonkey software. All responses were submitted pseudonymously. Two reminder emails were issued per round: the first one week after release and the second on the working day prior to the deadline. Each Delphi round consisted of items grouped into thematic sections aligned with the study’s five research questions, presented to participants in their original wording: (1) How should childhood verbal abuse be defined? (2) What behaviors would you say constitute childhood verbal abuse? (3) What outcomes would you say result from childhood verbal abuse? (4) Which stakeholders should be engaged in an evidence-based response? (5) What actions, and in what priority, should be taken in response?
Phase 1: Item Generation
The research team first conducted a review of empirical, theoretical, and gray literature to identify potential definitions, abusive behaviors, outcomes, stakeholders, and recommended interventions relevant to childhood verbal abuse. Searches were conducted using combinations of terms including verbal abuse, psychological maltreatment, emotional abuse, and child maltreatment, across academic databases and gray literature sources.
The initial review of 337 resources yielded 275 eligible sources, comprising 209 academic articles (76.0%) and 66 gray literature sources (24.0%). Exclusions of 62 resources were made for studies focusing exclusively on adult abuse, general aggression, or inaccessible full texts. The academic literature was predominantly quantitative (90.5%), with smaller proportions of qualitative (6.3%) and mixed-methods designs (3.2%). Publication dates ranged from 1977 to 2023, with two-thirds (66.3%) published in the past decade. Sources spanned 51 countries, most frequently the United States (51.3%), United Kingdom (8.1%), Canada (4.8%), and India (3.7%). Gray literature contributions were drawn from 59 organizations and represented a diverse set of formats, including news sites (18.6%), blogs (15.3%), charities (13.6%), and educational or clinical websites. Intended audiences ranged from the general public (32.9%) and parents (30.1%) to children (6.8%).
Commonly Identified Concepts Related to Childhood Verbal Abuse in the Literature (N = 275) and Among Expert Participants (N = 21), Grouped by Category
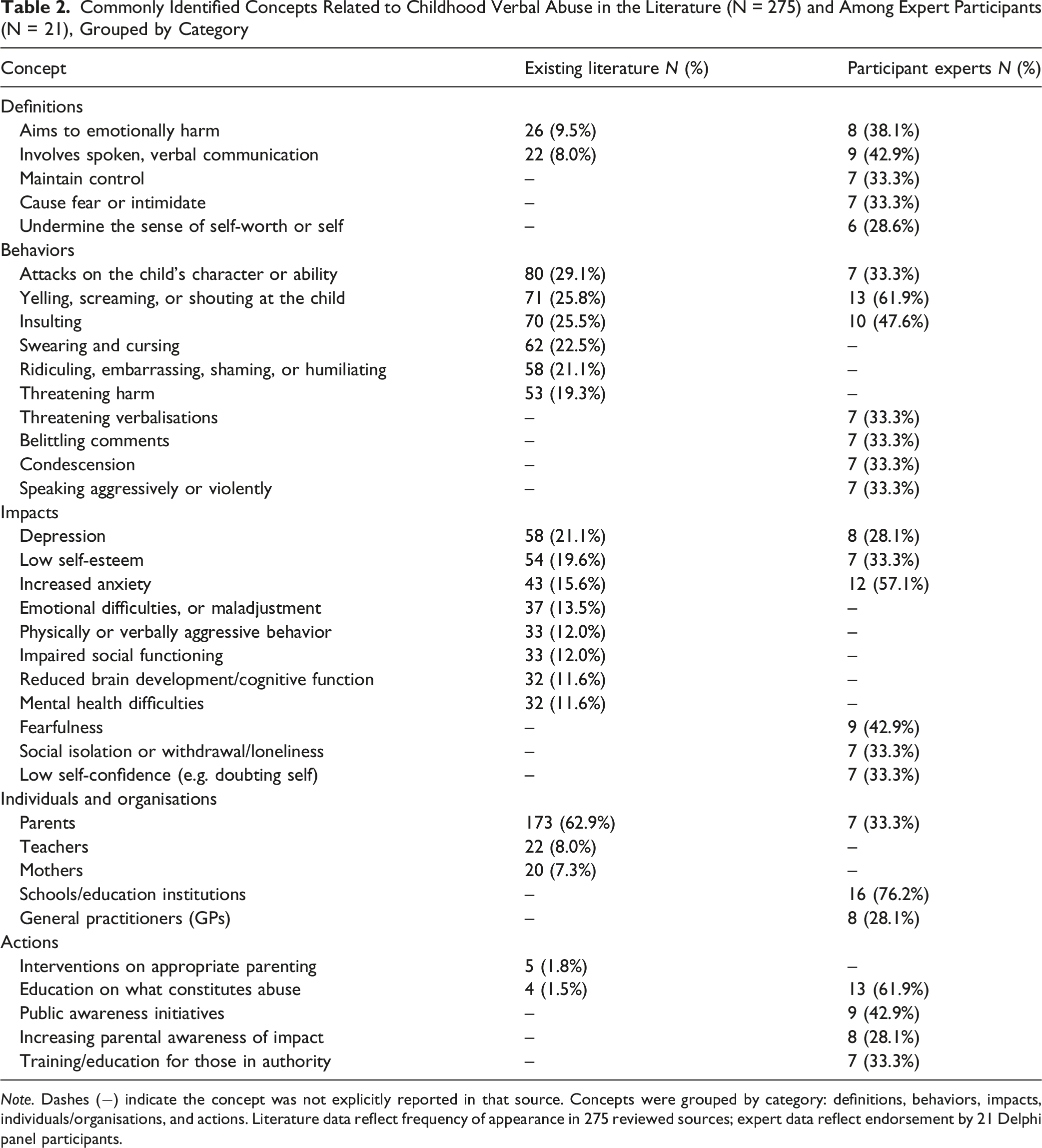
Note. Dashes (−) indicate the concept was not explicitly reported in that source. Concepts were grouped by category: definitions, behaviors, impacts, individuals/organisations, and actions. Literature data reflect frequency of appearance in 275 reviewed sources; expert data reflect endorsement by 21 Delphi panel participants.
In parallel, Delphi participants submitted free-text responses to the five guiding questions, yielding 487 raw concepts. These were screened, consolidated, and reduced to 256 distinct items: 35 definitions, 58 behaviors, 76 impacts, 54 stakeholders, and 33 actions. The most frequently suggested definitions referred to spoken communication (42.9%), intent to harm emotionally (38.1%), use of language to control (33.3%), instilling fear (33.3%), and undermining self-worth (28.6%). Common behaviors included yelling (61.9%), swearing (47.6%), character attacks (33.3%), belittling (33.3%), and threatening language (33.3%). Commonly identified impacts were anxiety (57.1%), fear (42.9%), depression (38.1%), low self-esteem (33.3%), and social isolation (33.3%). Stakeholders most frequently identified were schools and education professionals (76.2%), general practitioners (38.1%), and parents (33.3%). Proposed actions included education about verbal abuse (61.9%), public awareness campaigns (42.9%), and training for adults in positions of power (33.3%). These participant-derived concepts were then combined with those from the literature to create the initial item pool for consensus testing in Rounds 2–6. A comparison between literature- and participant-derived concepts is presented in Table 2.
Phase 2: Item Refinement
Phase 2 involved iterative refinement of the combined item pool across Delphi Rounds 2–6. Between rounds, quantitative agreement ratings and qualitative free-text comments were reviewed by the research team. Percentage agreement was calculated for each item across respondents. Free-text comments were reviewed within each domain to identify suggestions for item revision, merging, removal, or addition where supported by broader panel feedback. Revised item lists were then prepared for each subsequent round based on the integration of quantitative and qualitative feedback. A consensus threshold of ≥70% agreement was adopted, consistent with recommendations in the Delphi methodology literature for health and social research studies of this kind (Diamond et al., 2014; Keeney et al., 2006). Items reaching this threshold were retained without further modification. Items that did not reach the threshold were either revised based on participant feedback and reintroduced in the subsequent round, or discarded if they were judged to be unclear, redundant, or lacking sufficient conceptual validity across multiple rounds. Items were not automatically discarded after a single round of non-consensus; rather, the decision to discard or revise was guided by the qualitative feedback received alongside the quantitative ratings. By providing both quantitative ratings and narrative comments, panelists contributed to an iterative decision-making process that ensured a balance between group convergence and the inclusion of minority perspectives. This process encouraged reflection, allowed panelists to reconsider their ratings in light of the broader group’s views, and supported gradual convergence of opinion.
Rounds 2 and 3 focused on systematically refining the broad item pool. In Round 2, participants evaluated definitions, behaviors, impacts, stakeholders, and actions generated in Phase 1 and the literature, indicating whether they agreed with their inclusion. Round 2b further explored which stakeholders and actions should fall within the remit of a childhood verbal abuse charity. Round 3 then revisited items that had not yet achieved consensus, presenting panelists with agreement percentages from the previous round and incorporating additional items suggested in free-text responses.
Rounds 4–6 revisited all categories, with unresolved definitions, behaviors, impacts, stakeholders, and actions carried forward for further evaluation. Some domains reached consensus more quickly than others. For example, definitions largely stabilized by Round 4 and were progressively integrated into a composite draft definition, which was refined through subsequent participant feedback until it surpassed the ≥70% agreement threshold. In contrast, actions required more extended deliberation: beginning in Round 4 and continuing through Round 6, participants evaluated, refined, and ultimately prioritized alternative lists of potential actions derived from earlier consensus items. The six rounds were conducted at two-week intervals between 21 November 2022 and 23 February 2023. A full record of the questions posed and items presented to participants across rounds is provided in Supplemental material A.
Data Analysis
Quantitative responses were summarized using descriptive statistics, including the proportion of participants endorsing each item across rounds. These proportions were used to determine whether items met the predefined ≥70% consensus threshold. Qualitative comments provided by participants in each round were reviewed within each domain (definitions, behaviors, impacts, stakeholders, and actions) by the research team to identify suggestions for item revision, merging, or removal, and to incorporate participant-proposed additions where supported by broader panel feedback. Separately, open-ended responses across rounds were subjected to content analysis to identify recurring areas of conceptual ambiguity and contention, the findings of which are reported alongside the consensus results. The integration of quantitative ratings and qualitative feedback allowed the Delphi process to combine structured consensus measurement with participant-driven conceptual refinement.
Results
Consensus on Core Components
The panel endorsed 27 definitions, 46 behaviors, 45 impacts, 29 stakeholders, and 19 actions, which together formed the building blocks of the definition and prioritized action plans.
Definitions
27 were endorsed, centering on verbal abuse as a destructive form of communication that causes emotional harm, undermines self-worth, and exerts control or intimidation (for more details, please see Supplemental material Table B1. Consensus definitions of childhood verbal abuse).
Behaviors
46 behaviors reached consensus, including yelling, insults, threats, and character attacks, alongside more subtle forms such as withholding communication or using intonation to belittle (for more details, please see Supplemental material Table B2. Consensus behaviors identified as childhood verbal abuse).
Impacts
45 outcomes achieved consensus, most prominently anxiety, depression, isolation, and diminished self-esteem. Physical health outcomes and longer-term societal outcomes (e.g., criminality) did not achieve consensus (for more details, please see Supplemental material Table B3. Consensus impacts of childhood verbal abuse).
Stakeholders
29 stakeholders were retained, with mental health professionals, teachers, parents, and safeguarding organizations identified as essential actors (for more details, please see Supplemental material Table B4. Stakeholders identified as important for responding to childhood verbal abuse).
Actions
19 actions reached consensus, nine of which were prioritized as essential. Strongly endorsed actions included respectful communication training, parental mental health support, and public education campaigns (for more details, please see Supplemental material Table B5. Priority actions for responding to childhood verbal abuse).
Consensus on Definition
Drawing on the agreed components, the research team drafted a composite definition of childhood verbal abuse which was iteratively refined by the panel. In Round 5, this definition surpassed the ≥70% consensus threshold, receiving endorsement from 83.8% of participants. The final consensus definition stated: “Childhood verbal abuse is a form of emotional and/or psychological abuse, involving non-physical aggression in the form of destructive communication. It can be deliberate (intends to cause harm), or perceived as deliberate (causes harm anyway), and carried out in an active or reactive way. Childhood verbal abuse is often directed at a child, but can also be indirect (e.g., directed at others about the child) and aims to do any of the following: cause fear or intimidate, humiliate or demean, ridicule, undermine sense of self-worth or self, emotionally harm, maintain control, isolate, and manipulate or coerce. This can occur via spoken, verbal communication, intonation, written communication (e.g., social media), or even gestured/non-verbal communication, and usually occurs as a pattern of behavior or to a gratuitous or extreme amount. However, it can also occur in an unplanned, impulsive or unpredictable way. The behaviors which make up childhood verbal abuse include: verbal attempts to isolate or control, threatening verbalizations, character attacks, denial of wrongdoing (on behalf of abuser), verbal putdowns and making the child feel inferior, withholding, and controlling the conversation.”
This definition integrates both functional aspects (emotional harm, intimidation, control) and modalities (spoken, written, digital, and gestural), offering a comprehensive and consensus-driven characterization of childhood verbal abuse.
Prioritization of Actions
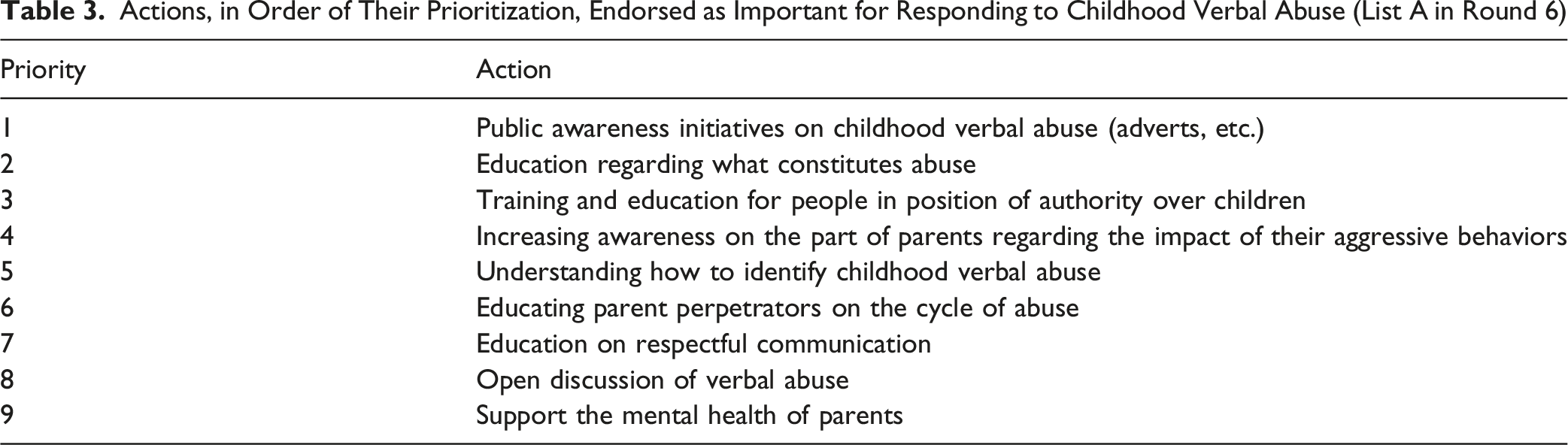
Actions, in Order of Their Prioritization, Endorsed as Important for Responding to Childhood Verbal Abuse (List A in Round 6)
Comparison with Literature
Alongside these consensus outcomes, it was important to consider how the findings aligned with, or diverged from, the existing academic and gray literature. Many items strongly represented in the literature were also endorsed by the expert panel, including behaviors such as yelling, insults, and character attacks, and impacts such as anxiety, depression, and low self-esteem. These areas of agreement indicate a solid foundation of shared understanding between published research and expert consensus. However, several concepts that were absent or rarely addressed in the literature achieved strong consensus among Delphi participants. These included subtle or quiet forms of verbal abuse (e.g., withholding communication or using intonation to belittle), the use of written and digital modalities (e.g., messaging, social media), and nonverbal gestures that convey humiliation or control. Their endorsement by experts but omission from much of the literature suggests that academic discourse may underrepresent less visible or less traditionally recognized forms of verbal abuse, despite their perceived salience among practitioners and survivors.
Conversely, some outcomes commonly cited in the literature, such as physical health consequences or long-term associations with criminality, did not achieve consensus within the Delphi panel. This indicates that while such outcomes may appear in correlational studies, the panel felt there was not yet sufficient evidence to establish them as core or defining impacts of childhood verbal abuse. Similarly, certain behaviors emphasized in the literature, including scolding or jealousy directed toward the child, were discarded during the consensus process for lacking conceptual clarity or broad agreement. Taken together, these patterns illustrate the distinctive contribution of the Delphi process: confirming the relevance of widely documented behaviors and impacts while also identifying important omissions in the literature and filtering out less robust or less agreed-upon concepts. This strengthens the validity of the final consensus framework and highlights priority areas for further empirical research, particularly around subtle, digital, and nonverbal forms of childhood verbal abuse that remain underexplored in academic and policy discourse.
Content Analysis of Open-Ended Responses
Alongside quantitative ratings, panelists provided open-ended feedback in Rounds 2–5. A content analysis of these responses highlighted four areas of ongoing conceptual ambiguity and disagreement: (1) intent versus perceived harm; (2) repetition versus single incidents; (3) scope of verbal modalities (e.g., nonverbal, written, and digital); and (4) the role of cultural relativism. Key illustrative quotes are presented for each category.
First, participants debated the role of intent, with some emphasizing deliberate harm and others prioritizing the child’s subjective experience of abuse. Several panelists argued that verbal abuse is defined by intentionality, where the adult seeks to harm or exert control: “Verbal abuse is designed to be undermining, used to demean and gain power where an imbalance of power, often age (adult to child).” “Targeted negative interactions… are likely to be far more harmful.”
In contrast, others maintained that the child’s subjective experience should take precedence over intent: “Intentionality is irrelevant.” “Calling people hurtful names—can be on purpose, or not.” “The word potential is important: abuse impacts individuals in different ways.”
Second, repetition was viewed as an aggravating factor, though many argued that single incidents could still constitute abuse if sufficiently damaging. While there was broad agreement that repetitive abuse is particularly harmful, views diverged on whether isolated incidents should qualify as abuse: “This might be a one-off incident, or insidious behavior over time.” “As a one-off, these don’t always constitute abuse... but if the behavior continues over time, then it becomes abusive.” “[…] particularly when repeated or persistent, although single remarks can be very wounding.”
Third, participants debated whether nonverbal behaviors (e.g., silence, facial expressions, tone) and written or digital communication (e.g., texts, social media posts) should fall under the umbrella of verbal abuse.
Support for a broad interpretation included: “Verbal abuse is about more than simply what is said and includes how words are spoken as well.” “Shouting, yelling, saying things with a certain look… tone, facial expression, stance.” “Ignoring a child when they speak to you—even though not verbal, you are choosing to not respond verbally for a reason.” “Verbal abuse can be either spoken or written.”
Others favored a narrower scope: “Disagree that silent treatment is verbal abuse as the definition of verbal is about words.” “Gestures or nonverbal communication cannot be included under the heading of verbal abuse.”
Finally, views diverged on how cultural norms should influence definitions and interventions. Some panelists emphasized the importance of cultural context: “I would say that to fully understand the impact of the verbal abuse, the cultural context may be important. But verbal abuse transcends culture.” “The definition should not restrict verbal abuse to a cultural context.”
Others rejected cultural relativism as inappropriate within safeguarding definitions: “…this should not impact on or be present in the definition of a type of abuse.” “I agree with the point about cultural relativism, but it is not a definition.”
Together, these findings indicate that while strong consensus was achieved on the core content of definitions, behaviors, outcomes, stakeholders, and actions, divergence remains around intent, repetition, modality, and cultural context.
Discussion
This Delphi study develops an expert-informed consensus through a structured, multidisciplinary process integrating lived-experience perspectives on the definition, behaviors, impacts, stakeholders, and actions relevant to childhood verbal abuse. By integrating empirical and gray literature with diverse panel perspectives, the study responds to a critical gap in child maltreatment research: the lack of definitional clarity and operational precision surrounding verbal abuse as a distinct construct. The consensus-derived framework provides an important foundation for research, policy, and practice.
Establishing a Robust and Shared Definition
While verbal abuse is widely acknowledged as a component of childhood maltreatment, its specific parameters have remained poorly defined across academic, clinical, and policy contexts. Existing psychological maltreatment frameworks, including the APSAC-endorsed definition (Hart et al., 2019) and the operationalized definition proposed by Slep et al. (2022), provide an important foundation by identifying verbally aggressive behaviors—such as spurning and terrorizing—as key subtypes. However, these frameworks situate verbal abuse within the broader psychological maltreatment construct rather than as an independently operationalized domain. Our literature review identified 30 distinct and often contradictory definitions, indicating that verbal-abuse-specific operationalization remains underdeveloped. In response, the expert panel endorsed 27 definitions and reached consensus on a composite characterization encompassing verbal, gestural, and written communication. This extends existing frameworks by operationalizing verbal abuse as a distinct construct while complementing prior definitional work, with applicability across research, educational, clinical, and legal contexts.
Unlike definitions that emphasize overt behaviors such as shouting or explicit insults (Glaser, 2002; Hibbard et al., 2012; Teicher & Samson, 2013), the panel incorporated subtler forms of harm, including belittling, threatening non-verbal gestures, repeated written messages, and communicative withholding. Consistent with National Institute for Health and Care Excellence (NICE, 2018) principles, the definition integrates empirical evidence, practitioner expertise, and lived experience (Mays et al., 2005; Nutley et al., 2013), and extends to indirect and non-verbal communication (e.g., character attacks made to third parties).
This conceptualization is reflected in the range of behaviors identified by the panel. A total of 46 behaviors reached consensus, spanning overt acts such as shouting, insulting, and threatening, as well as more covert forms including scapegoating, emotional manipulation, repeated humiliation, exclusionary threats, communicative withholding, and belittling intonation. The inclusion of both commonly recognized and less visible behaviors underscores that childhood verbal abuse cannot be defined solely by volume or intensity, but by its communicative function—how language and communication are used to degrade, silence, or exert control over a child. Notably, the panel emphasized that “verbal abuse does not need to be yelling/screaming, it can be quiet and subtle,” challenging assumptions that harmful communication must be overt (Infante & Rancer, 1996; Wang & Kenny, 2014).
A central feature of the definition is its emphasis on communicative intent. The panel agreed that abusive acts must be experienced as gratuitous rather than corrective, while allowing for both deliberate and emotionally reactive behaviors. This aligns with ongoing debates regarding intentionality and repetition in psychological maltreatment (Hart et al., 2019; Slep et al., 2022). At the same time, areas of contention remain. While perceived intention was considered essential, there was no consensus on whether a single harmful incident is sufficient or whether repetition is required. The final definition therefore accommodates both singular and patterned acts, provided they are experienced as harmful and gratuitous. Panelists also rejected the inclusion of “unintentionally harmful” behaviors, reinforcing the centrality of perceived intent in classification.
The panel further distinguished childhood verbal abuse from broader emotional abuse. While overlap exists, verbal abuse was defined by its communicative function, encompassing speech content, tone, non-verbal expression, and communicative withholding. Behaviors such as lack of privacy, jealousy, or inconsistent care—though harmful—did not meet criteria for inclusion. This distinction supports treating verbal abuse as a discrete construct rather than a diffuse emotional climate, which may improve both research precision and practitioner training. Finally, although most panelists supported a universal definition independent of cultural norms, some disagreement persisted, reflecting ongoing tensions between universalism and cultural relativism in child protection frameworks and highlighting considerations for cross-cultural application.
Psychological and Functional Impacts
Both the literature and panel responses indicate that childhood verbal abuse is associated with a wide range of psychological, behavioral, and functional difficulties. A total of 45 impacts reached consensus, including depression, anxiety, low self-esteem, social withdrawal, academic underachievement, and behavioral dysregulation (Aloia, 2022; Brendgen et al., 2007; Kawabata et al., 2011; Salwen et al., 2014, 2015; Sharratt et al., 2023). These findings align with evidence linking verbal abuse to both internalizing and externalizing psychopathology, and to outcomes distinct from other forms of maltreatment (Dutra et al., 2009; Rich et al., 2005; Salwen et al., 2015; Teicher & Parigger, 2015). Panel endorsement reflects perceived salience rather than causal inference; however, the empirical evidence base for these associations is independently well established (Dube et al., 2023).
No physical health outcomes reached consensus, despite their documentation in the literature (e.g., headaches, sleep disturbances, cardiovascular symptoms, chronic fatigue; Dube et al., 2023), and agreement was also limited regarding associations with clinical diagnoses such as schizophrenia, post-traumatic stress disorder (PTSD), or personality disorders. This lack of consensus likely reflects caution in attributing causality and the complexity of isolating verbal abuse from co-occurring adversities. These gaps highlight the need for future research to examine physical health correlates, clarify diagnostic pathways, and disentangle the specific effects of childhood verbal abuse from other forms of adversity (Aloia, 2022; Brendgen et al., 2007; Herrenkohl & Herrenkohl, 2009; Kawabata et al., 2011; Witt et al., 2016).
Stakeholder Engagement: Bridging the Implementation Gap
An important contribution of this study is the identification of stakeholders involved in responding to childhood verbal abuse. The academic literature provides limited guidance on this issue, with parents identified in 62.9% of sources and little attention given to other actors. In contrast, the expert panel identified a broader network of 29 stakeholder groups spanning health, education, and community sectors, including educators, therapists, general practitioners, social workers, mental health organizations, and parental support services (see Supplemental material B, Table B4). These actors were considered essential for both direct intervention and public education, underscoring the need for a multi-system response beyond the parent-focused emphasis in existing research.
The panel also strongly endorsed the involvement of individuals with lived experience of childhood verbal abuse in shaping definitions and responses. This aligns with broader trends in child protection and public health, where survivor involvement is increasingly recognized as essential for legitimacy, relevance, and impact (Mays et al., 2005; National Institute for Health and Care Excellence, 2018; Nutley et al., 2013; Taggart et al., 2025). However, such perspectives are rarely incorporated systematically in the literature, highlighting the added value of the Delphi process. At the same time, the panel identified practical barriers to stakeholder involvement, including limited time and resource capacity among frontline professionals. These constraints highlight the importance of ensuring that expanded stakeholder engagement remains feasible and sustainable in practice.
Prioritizing Actions: Education, Awareness, and System-Level Response
The academic literature rarely advances beyond conceptual discussion, with only 3.3% of reviewed papers proposing concrete actions. In contrast, the panel reached consensus on 19 recommended actions, nine of which were deemed suitable for immediate implementation. These prioritized actions focused on improving public awareness, educating parents and authority figures, and disseminating the consensus definition of childhood verbal abuse, reflecting the view that shared conceptual understanding is a necessary foundation for effective intervention and policy development.
Although no consensus was reached on the precise ordering of actions, a preferred set emerged, prioritizing public awareness initiatives, education about verbal abuse, and training for those in positions of authority over children. The panel also identified ten additional actions requiring longer-term infrastructure, including therapeutic services, media outreach, and policy advocacy. This distinction between immediate and longer-term actions provides a practical framework for implementation within resource-constrained contexts.
These findings have implications across three key systems. In child welfare and safeguarding, the consensus definition may support clearer referral thresholds and more consistent identification of verbal abuse as a distinct form of harm. In educational settings, the strong endorsement of teachers highlights the importance of incorporating verbal abuse into training, particularly for subtle and indirect forms that may be overlooked. In mental health services, the findings underscore the value of routine screening for verbal abuse and the use of trauma-informed approaches that recognize it as a distinct adverse experience.
Future Research Directions
The present findings highlight several important directions for future research. First, there is a need to develop and validate a psychometrically robust measure of childhood verbal abuse, grounded in the new consensus definition. Such a tool would allow for more precise prevalence estimates and clearer distinctions between verbal abuse and related constructs. Second, longitudinal research is needed to examine the developmental trajectories of children exposed to verbal abuse, particularly in differentiating its impacts from other adversities. Third, the panel highlighted the importance of investigating the relative impact of written, spoken, and non-verbal abuse, given contemporary concerns about digital communication and online harms. Fourth, more attention should be directed toward clarifying the frequency–intensity threshold: whether single incidents can have long-term consequences, and under what conditions repetition amplifies harm. Finally, research should examine the physical health correlates of verbal abuse, integrating psychological and biomedical approaches. Together, these directions provide a strategic agenda for the next phase of empirical inquiry.
Limitations and Applicability
The applicability of the study is strengthened by its rigorous design, disciplinarily and experientially diverse panel, and iterative process. Participants spanned academia, clinical practice, social care, and lived experience, with professional tenures ranging from five months to 24 years. Nonetheless, several limitations warrant consideration.
First, in accordance with data minimization principles, race, ethnicity, and sex data were not collected from participants, which means that the demographic composition of the panel cannot be fully described. Future Delphi studies in this area should consider whether collecting such data — with appropriate ethical safeguards — would allow for more nuanced interpretation of how demographic diversity shapes consensus outcomes, particularly given the known cultural variation in perceptions of verbal abuse. Second, participants were recruited through professional networks focused on childhood verbal abuse and were likely to hold a high degree of pre-existing investment in the topic. Their views may not fully represent the wider field, particularly among frontline practitioners with lower awareness or engagement with this specific construct. The findings should therefore be interpreted as reflecting the perspectives of an engaged and informed expert community rather than a representative sample of all professionals working with children.
Moreover, the sample size was modest and the panel was geographically constrained, limiting cross-cultural generalizability. The application of this consensus definition in diverse cultural contexts — particularly where normative boundaries between discipline and verbal abuse may differ — represents an important direction for future research. Cross-cultural replication studies, involving panels drawn from non-Western and lower-income contexts, would strengthen the universality of the framework. Similarly, future research should examine whether the consensus definition performs consistently across different professional and community settings, and how it might be adapted for culturally specific applications without undermining its core protective intent. Finally, Delphi methodology brings inherent challenges. Consensus thresholds may suppress minority viewpoints; however, the explicit identification of areas of disagreement—such as those relating to intentionality, repetition, and cultural relativism—represents a key strength of the approach, providing a structured means of highlighting unresolved issues and directing future research.
Conclusion
In sum, this study delivers a timely and practical contribution to the understanding and prevention of childhood verbal abuse. By integrating academic literature, practitioner insight, and lived experience through a structured Delphi process, the findings address longstanding ambiguities in the conceptualization, identification, and response to verbal harm. The expert-endorsed definition, expanded behavioral taxonomy, clarified intent criteria, and prioritized action list together bridge the gap between conceptual debate and practical response. These findings offer a coherent, evidence-informed foundation for advancing awareness, prevention, and intervention strategies. They highlight strategic priorities—such as public and professional education, stakeholder coordination, and the development of robust measurement tools—that can guide effective resource allocation. The inclusion of quiet, indirect, and written forms of abuse within the framework marks an important shift from fragmented awareness toward a more coordinated and evidence-informed response. More broadly, this study contributes to the growing recognition of verbal abuse as a distinct and serious form of harm within the broader psychological maltreatment framework. By providing a clearly defined, consensus-informed, and practically oriented framework, the findings support improved detection, accountability, and intervention across systems of care.
Supplemental Material
Supplemental Material - Childhood Verbal Abuse: Expert-Informed Delphi Consensus on Definition and Actions
Supplemental Material for Childhood Verbal Abuse: Expert-Informed Delphi Consensus on Definition and Actions by Elizabeth Li, Reilly Bugden, Kumayl Khamisa, Nikita Singh and Jennifer McGowan in Child Maltreatment
Footnotes
Acknowledgements
Our deepest thanks go to all the individuals with lived experience and the partner organisations who generously shared their insights, expertise, and examples throughout this process. We are especially grateful to: all of our lived experience participants; the University of Cambridge; Echo Research and KPMG/NLT; Essential Parent; FrameWorks UK; Frances Holland School; Great Ormond Street Hospital for Children; Laine Jäderberg Associates; Mental Health Innovations; NHS and private practice contributors; Norwich Lower School; Place2Be; Thomas’s London Day Schools; the University of Oxford; and the University of the West of England.
Ethical Considerations
Ethical approval was obtained from University College London (UCL) Research Ethics Committee (ID: EP/2021/017). Informed consent was secured from all participants, and participants could withdraw at any point. The study was conducted in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments.
Consent to Participate
Written informed consent to participate was obtained from all participants. Participants were provided with detailed information about the study purpose, procedures, and their rights, including the right to withdraw at any time without penalty.
Consent for Publication
Informed consent for publication was obtained from all participants as part of the study. Participants were informed that anonymous data may be published in academic outlets. All participant responses were coded anonymously and only accessible to the research team, ensuring confidentiality.
Authors’ Contributions
EL wrote the current manuscript. RB collected and analysed the data and prepared an initial draft with JM. KK and NS contributed to initial data collection. JM oversaw the entire project and led the study design and overall coordination.
Funding
This study was funded by the Words Matter charity (charity number 1201281).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and analysed during the current study (Delphi responses from each round) are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.