
Abstract
Policy changes that improve access to immediate postpartum long-acting reversible contraceptives (IPP LARC carveouts) were examined as a potential prevention measure against parent-perpetrated child maltreatment, neglect and physical abuse of children under five. Generalized differences-in-differences was applied to state-year outcome trends from the National Child Abuse and Neglect Data System child file. Findings suggest IPP LARC carveouts did not yield significant reductions in substantiated parent-perpetrated physical abuse (ATT = −22.9% or 49.97 fewer cases per 100,000 children under 5, p-value = 0.18) nor investigated parent-perpetrated physical abuse (ATT = −18.7% or 57.78 fewer cases per 100,000 children under 5, p-value = 0.26). However, among states whose proportions of births covered by Medicaid fall above the median, the policies were associated with significant reductions substantiated (ATT = −33.7% or 74 fewer cases per 100,000 children under 5, p-value = 0.05) and investigated (ATT = −38.7% or 120 fewer cases per 100,000 children under 5, p-value = 0.05) parent-perpetrated physical abuse cases per 100,000 children under 5. Collectively, findings suggest that enabling Medicaid to reimburse separately for IPP LARC may reduce parent-perpetrated physical abuse among young children.
Introduction
An estimated one in seven (15.2%) US children have experienced maltreatment (defined as neglect, or physical, emotional, or sexual abuse) in the past year (Finkelhor et al., 2015), and more than one in three (37.4%) of US children will have a Child Protective Services investigation for suspected maltreatment before age 18 (Kim et al., 2017). Child maltreatment and related trauma can adversely impact an exposed person’s physical, mental, and behavioral health across their lifespan, and impede social competencies that lay the foundation for successful coping and economic productivity (Corso et al., 2008; Taillieu et al., 2020). Identifying effective strategies to prevent the occurrence and mitigate the consequences of child maltreatment entails considerable societal benefit.
Previous research suggests unintended pregnancy and birth spacing heighten risk of child maltreatment (Guterman, 2015; Runyan, 2021; Rybińska et al., 2024). Unintended pregnancy is associated with both economic instability (Bailey et al., 2012; Bailey & Lindo, 2017; Nuevo-Chiquero, 2014; Parks & Peipert, 2016; Sonfield et al., 2013) and adverse maternal health outcomes, (Barton et al., 2017; Conron et al., 2009) including maternal depression. These may serve as important mechanisms between unintended pregnancy and child maltreatment. For example, parent financial stress can increase the occurrence of child maltreatment and at-risk parenting behaviors (Brooks-Gunn et al., 2013; Leinonen et al., 2002; Schwab-Reese et al., 2016). Children in families with low socioeconomic status are estimated to be five times as likely to experience child maltreatment than those in families with high socioeconomic status (Sedlak et al., 2010). Evidence from longitudinal and cross-sectional samples suggests that maternal depression is associated with increases in child maltreatment (Ayers et al., 2019; Choi et al., 2019; Conron et al., 2009; McLearn et al., 2006).
Recent strategies to improve contraceptive access and influence unintended childbearing have largely focused on the availability and affordability of long-acting reversible contraceptives (LARCs), intrauterine devices and implants which are highly effective (less than 1% failure rate) and reversible (M. Bailey & Lindo, 2017; Hatcher, 2018). Since LARC devices are worn internally and do not require user action after placement, these devices may be optimal for mitigating pregnancy in instances of reproductive/sexual abuse. Strategies encouraging LARC uptake may be particularly salient to maltreatment prevention because abusive partners (Gracia et al., 2020; Sijtsema et al., 2020) and abused partners (Chiesa et al., 2018) are at high risk for being abusive parents. The Affordable Care Act (ACA) attempted to improve financial access to LARCs by mandating the coverage of all FDA-approved contraceptive supplies and services without patient cost-sharing (HRSA, 2016). However, following implementation of the ACA, healthcare organizations still struggled to stock LARCs and offer same-day LARC services due to their high acquisition costs and the traditional two-visit system used by outpatient clinics for contraceptive counseling and insertion (Aiken et al., 2014; American College of Obstetricians and Gynecologists, 2015; Beeson et al., 2014). Medicaid’s episode-based payment for pregnancy related services made payment particularly challenging in inpatient settings as providers had no way to bill for the device and procedure outside of the bundled rate (Aiken et al., 2014). To address this, many state Medicaid agencies separated the cost of the LARC device and insertion procedure from bundled payments for insertions immediately following delivery in the inpatient setting (IPP LARC) (Bogan & Marthey, 2021; Romero et al., 2022). In states with an IPP LARC carveout, providers can bill for the LARC device and/or insertion procedure, separately from the bundled pregnancy-related medical services. The policy was enacted in 9 states by 2014, 28 states by 2016, and to 40 states by 2018 (Bogan & Marthey, 2021). State adoption status as of 2019 (42 states) is summarized graphically in Figure 1. IPP LARC Medicaid carveout adoption status & year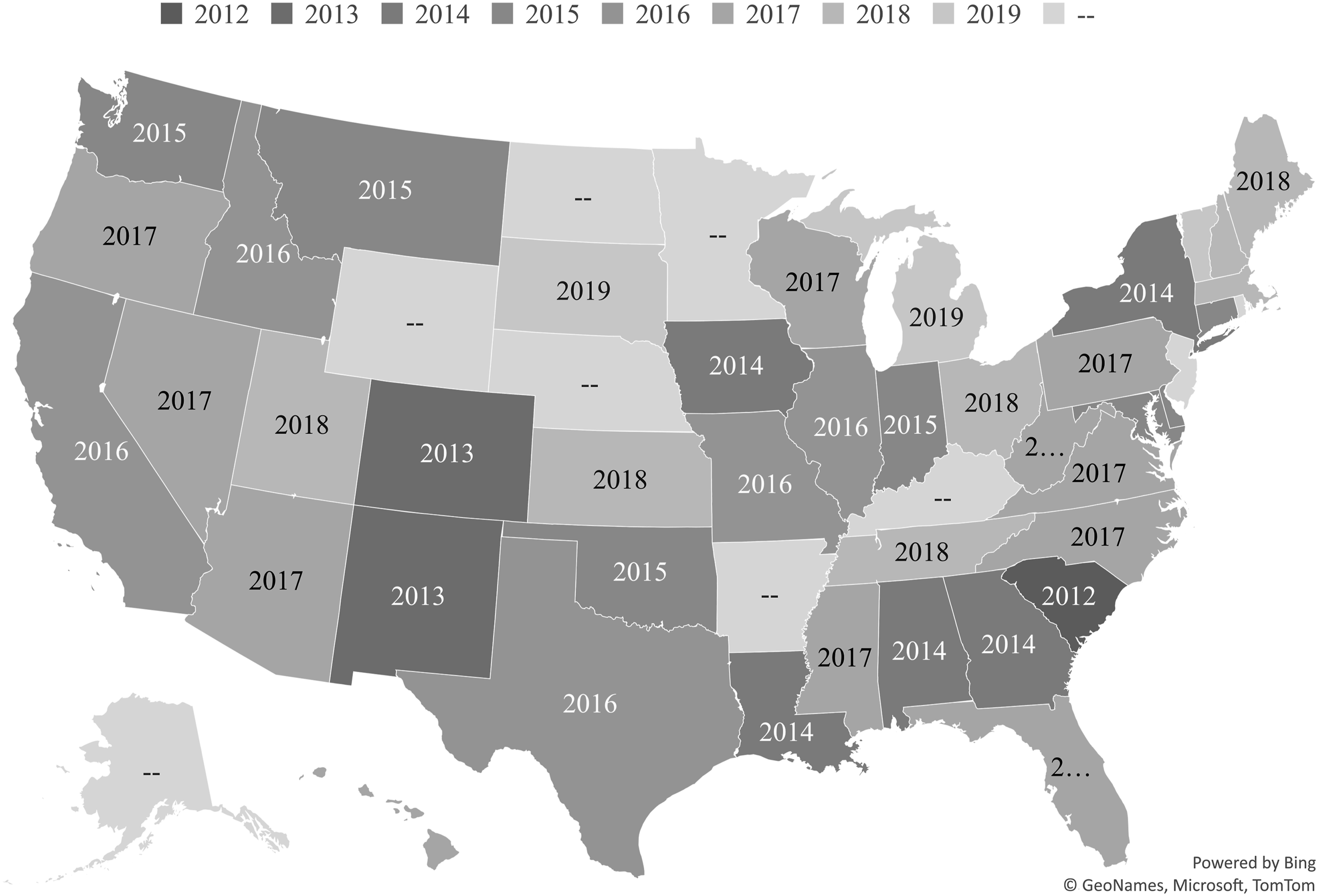
Policy evaluations from states that have unbundled LARCs from the Medicaid global labor and delivery fee find LARC unbundling is broadly effective at increasing IPP LARC initiation (Caudillo et al., 2022a; Goldin Evans et al., 2019; Steenland et al., 2021a, 2022). This policy change is also associated with increases in subsequent birth spacing (Liberty et al., 2020; Steenland et al., 2019).
Hypothesis
Few studies have assessed the impacts of IPP LARC carveouts beyond LARC uptake and birth outcomes. The well-established relationships between unintended pregnancy and risk factors for child maltreatment (i.e., parental mental health and financial stress), and recent evidence that IPP LARC carveouts improve the mental health of low-income mothers (Marthey et al., 2024) lead to the following hypothesis: the improved reproductive autonomy IPP LARC carveouts confer may be protective against child abuse through reductions in parental stress, and child neglect through reductions in financial stress. ‘Reproductive autonomy’ constitutes the power to decide and control one’s own contraceptive use, pregnancy and childbearing (Nguyen et al., 2019). This mechanism is supported by evidence from Aslim et al. (2024) who show that increased travel distance to abortion services is associated with large increases in investigated reports of child maltreatment, particularly among younger children (Aslim et al., 2024). Previously cited policy evaluations and the study at hand reflect the socioecological model (CDC, 2025; Letourneau et al., 2022) and the public health law framework (Burris et al., 2010) (Figure 2). Integration of the socio-ecological model & public health law framework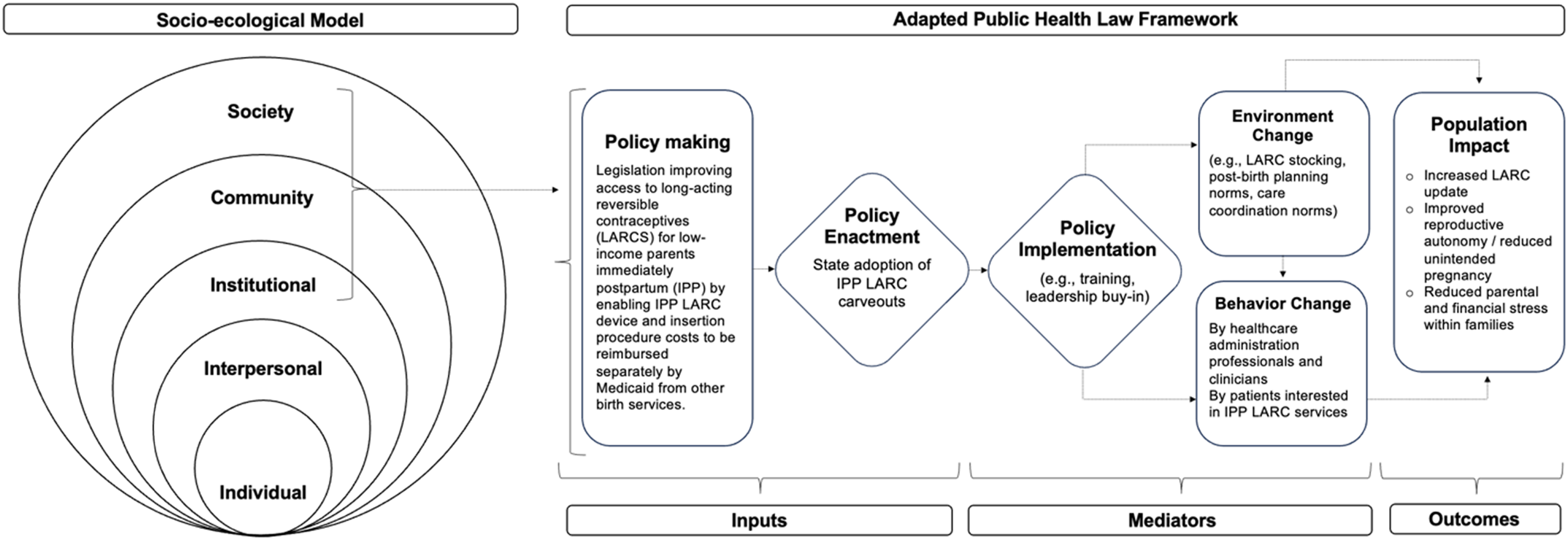
We apply a generalized differences-in-differences approach to compare parent-perpetrated child physical abuse, child neglect, and child maltreatment trends in children under five for states that did and did not carve out postpartum LARC.
Methods
Population
National Child Abuse and Neglect Data System (NCANDS) Child Files for states participating in the system every year between 2006–2019 were used to estimate annual state rates of parent-perpetrated maltreatment, physical abuse, and neglect of children under five. This subgroup of children has been appropriately prioritized by other works examining how changes in Medicaid programs shape maltreatment (Assini-Meytin et al., 2022; Brown et al., 2019; McGinty, 2022). Here, it is similarly reasonable to expect that any IPP LARC carveout impact would be particularly salient to this group given (1) about 30% of maltreatment cases have victims under two, and 45% under five; (2) parents of children under five may face heighted financial stressors per the need to work less and/or pay for expensive day care given these children are not yet in school; and (3) beneficiaries who receive a LARC immediately postpartum will have at least one child under five upon receipt of the device, and may or may not have older children.
NCANDS Child files contain de-identified administrative records and are a census of Child Protective Services (CPS) investigations from participating states. Each NCANDS observation includes indicators related to the incident (date and state of the notified CPS agency), child (age, sex, race/ethnicity, history of previous substantiated maltreatment), the type(s) of maltreatment reported (physical abuse, neglect or deprivation of necessities, medical neglect, and psychological or emotional maltreatment), as well as information about the relationship between the child and suspected perpetrator(s). Parent-perpetrated cases are defined as those where the suspected perpetrator is a parent, legal guardian, or a parent’s significant other.
Each individual record can include up to four maltreatment types. Each maltreatment type is assigned a disposition status to indicate if the reported maltreatment was unsubstantiated, suspected, substantiated, or had some other disposition status. It should be noted that substantiation is not a strong indicator of report validity (Peterson et al., 2018). Patterns of substantiation reflect important community- and jurisdiction-level norms (e.g., parenting standards, definitions of maltreatment definitions, budget resources, and processes for screening cases that warrant investigation) (Pac, 2021). A lack of substantiation may reflect an inability to meet a legal standard, rather than a lack of harm, or lack of reason to believe maltreatment occurred (Kohl et al., 2009). Accordingly, analyses were performed on cases where physical abuse or neglect was ‘substantiated’ or ‘suspected’ by an investigator, and on investigated cases regardless of disposition. The former are referred to as ‘substantiated cases’, and the latter as ‘investigated cases’.
Measures
The primary specification sample (referred to as the ‘most restrictive’ sample) had two exclusion criteria. To avoid confounding shocks from Medicaid expansion, states that did not adopt expansion and those who expanded after 2014 were excluded (Kasier Family Foundations, 2024). States that experienced other major changes in public programs that facilitate contraceptive access during the period of interest were similarly excluded (e.g., loss of Title X funding, carveouts for LARCs administered in Federally Qualified Health Centers (FQHC) or Rural Health Centers (RHC), and implementation of other comprehensive contraceptive programs). This sample includes 288,657 investigated reports of child physical abuse (215,599 substantiated) with 249,731 (187,108 substantiated) residing in treatment states and 38,926 (28,491 substantiated) residing in control states. State and report year indicators were used to aggregate individual observations into annual counts of each outcome by state, yielding 266 state-year observations (19 states, 13 treatment and 6 control, over 14 years) in the most restrictive sample. State-by-year counts were then converted to rates of maltreatment per 100,000 children aged zero to four years. Child population denominators were obtained from the National Cancer Institute Surveillance, Epidemiology, and End Results (SEER) Program.
Data on state adoption of Medicaid carve-out reforms were obtained from Medicaid State Plan amendments compiled elsewhere (Bogan & Marthey, 2021). Additional state-by-year demographic characteristics came from the US Census Bureau and Kaiser Family Foundation (KFF) State Health Facts. State-level covariates meant to capture group differences in access to health services included the Medicaid income eligibility level for pregnant beneficiaries and proportion of individuals under the federal poverty level. State-level covariates meant to capture differences in experiences with Child Protection Services included total child welfare expenditures, the proportion of Black individuals in a state, and the proportion of Hispanic individuals in a state.
Restricting state sample selection avoided confounding shocks from contemporaneous contraceptive access initiatives that have gone beyond Medicaid payment reform. Should the proposed mechanism be correct, one would expect estimates to be larger in states experiencing additional policy changes that improve reproductive autonomy for parents. To test this, the exclusion criteria was relaxed and all analyses were repeated including states that issued carveouts for LARC devices inserted in outpatient FQHC and RHC settings. This ‘partially relaxed’ iteration still excluded any state that did not expand Medicaid in 2014 and any state that had a comprehensive contraceptive program during the study period. The partially relaxed sample included 308 state-year observations (22 states, 16 treatment and 6 control, over 14 years).
To test this further, the exclusion criteria was relaxed to an even greater extent and all analyses were performed again with states that had comprehensive contraceptive programs, states that issued carveouts for LARC devices inserted in outpatient FQHC and RHC settings, and binary covariates indicating the presence of any comprehensive contraceptive program and of any FQHC/RHC carveout. This ‘fully relaxed’ iteration still excluded any state that did not expand Medicaid in 2014. The fully relaxed sample included 350 state-year observations (25 states, 19 treatment and 6 control, over 14 years). Larger estimates in the latter samples (as these states are experiencing IPP LARC carveouts as well as other policies shaping contraceptive access) relative to the main estimates would confer support for the hypothesized mechanism.
A key analytic challenge here was the inability to isolate children whose parents would qualify for Medicaid if they were pregnant. To partially address this, sensitivity analyses were performed where the IPP LARC treatment indicator was interacted with a binary indicator for whether a state had a below median (0) or an above median (1) proportion of Medicaid-covered births.
To ensure the estimates reflect the consequences of IPP LARC carveouts rather than another endogenous shock, all analyses were repeated on state rates of child maltreatment perpetrated by non-parents. While it is possible that IPP LARC carveouts would impact risk for maltreatment by non-parents in some circumstances, IPP LARC carveouts would have the most direct consequences for parents and children relative to other constituents. Therefore, expected changes in non-parent perpetrated maltreatment would be notably smaller in magnitude and significance relative to changes in parent-perpetrated maltreatment. For non-parent estimate comparisons, see Appendix Table 1.
Statistical Analysis
Intent-to-treat estimates of the effect of IPP LARC carveouts on child maltreatment were calculated using a series of generalized difference-in-differences (DD) approaches. The identifying assumption of difference-in-differences and all generalizations is that in the absence of the policy change, states with IPP LARC carveouts (“treated” states) would have experienced similar outcome trends to states without IPP LARC carveouts (“control” states), controlling for observable time-variant and unobservable time-invariant differences. The models compare substantiated and investigated rates of child physical abuse in states with and without an IPP LARC carveout policy, before and after the adoption year conditional on aforementioned covariates and state and year fixed effects that account for unobservable time-invariant differences and common secular trends across states, respectively.
To assess estimate validity, an event study model was specified. This provides an indirect, visual test of the parallel trends assumption of the DD design by depicting the evolution of treatment effect estimates over the study period. This model was constructed by including binary indicators for treatment states for each year prior to implementation within the prior regression equation. The reference category is the year before implementation. Event times that were four or more years prior to implementation in a given state, and those four or more years after implementation were grouped.
To address concerns about the consistency of DD estimates in studies of staggered treatment adoption, Gardner’s (2022) strategy was applied to overcome known bias from two-way fixed effects (TWFE) (Goodman-Bacon, 2021). The appendix provides details on both TWFE and Gardner’s approach. All analyses were conducted in 2024 using Stata version 18.0 (StataCorp).
Results
An annual weighted average of states’ rates (per 100,000 children) of parent-perpetrated maltreatment, physical abuse, and neglect cases screened in for investigation are displayed below for children of all ages (Figure 3, left column), and for children under age 5 (Figure 3, right column). Average annual state rate of parent-perpetrated maltreatment, physical abuse, and neglect, 2006–2019.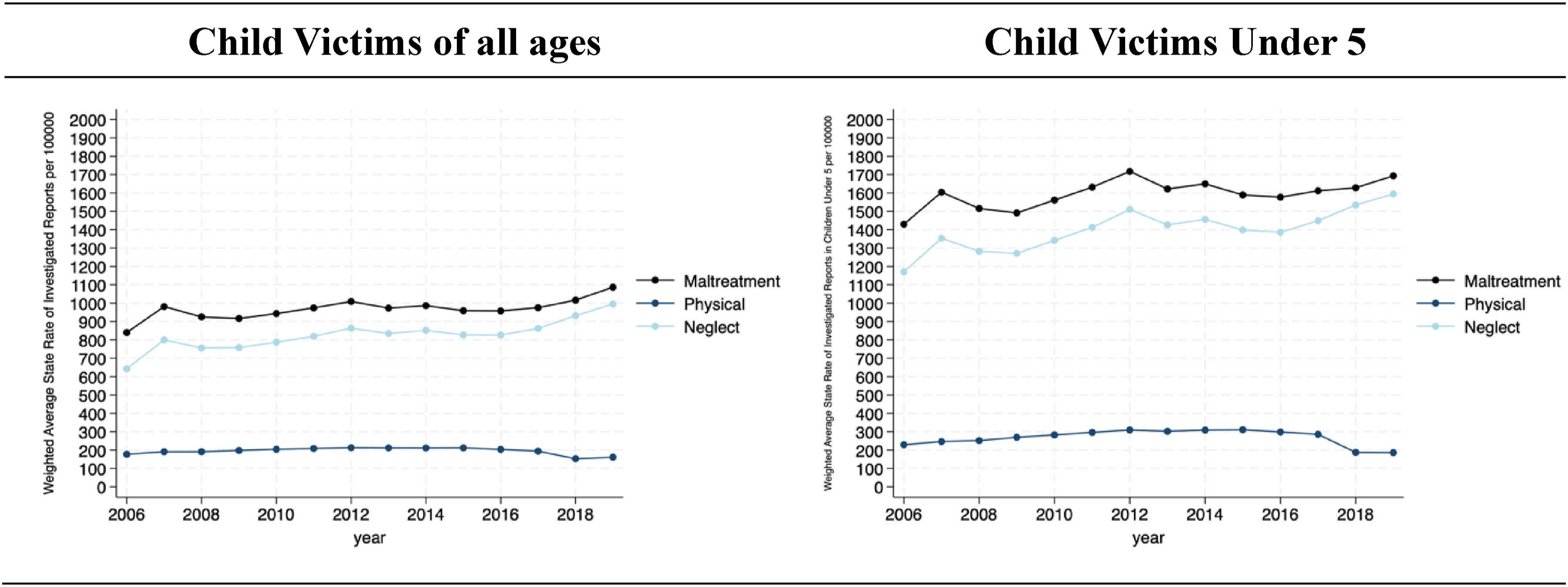
Across all included years rates of neglect are higher than rates of physical abuse among children of all ages and among children under 5. In both the under-five and all-age cohorts, rates of maltreatment and neglect increased gradually until peaking in 2012. After 2012, both cohorts experience a slight decline followed by a return to 2012 rates by 2019. Rates of physical abuse were more constant across the included period until a decline in 2017. Said decline was more pronounced in children under 5 than in the all-age cohort.
Demographics for Investigated Child Protective Service Reports of Parent-Perpetrated Physical Abuse With Child Victims Under Age 5 and for all Children Under 5, 2006–2019
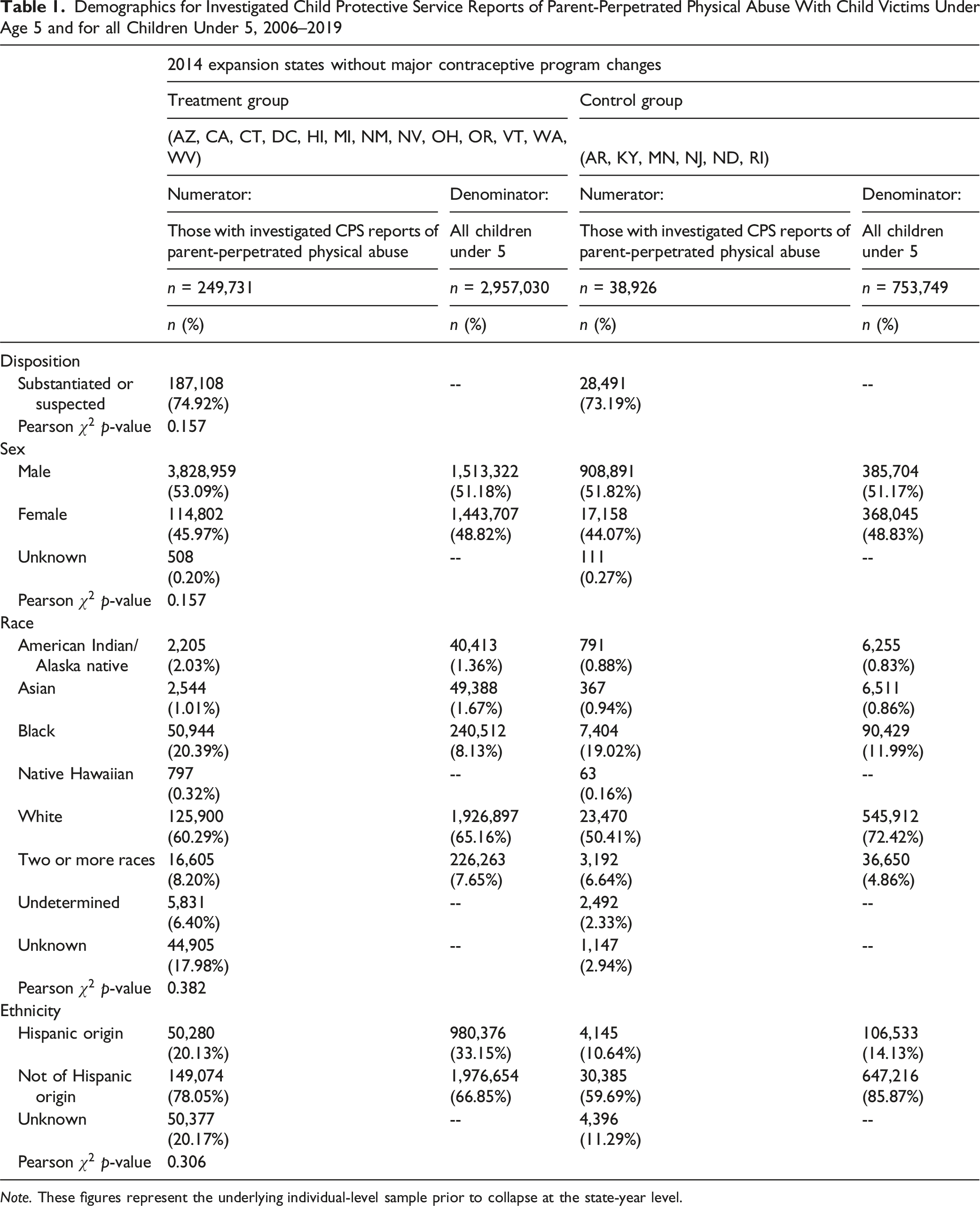
Note. These figures represent the underlying individual-level sample prior to collapse at the state-year level.
Average Post-Period Regression Estimates for the Impact of IPP LARC on Maltreatment, Physical Abuse, and Neglect, Parent-Perpetrated Cases Victimizing Children Under 5
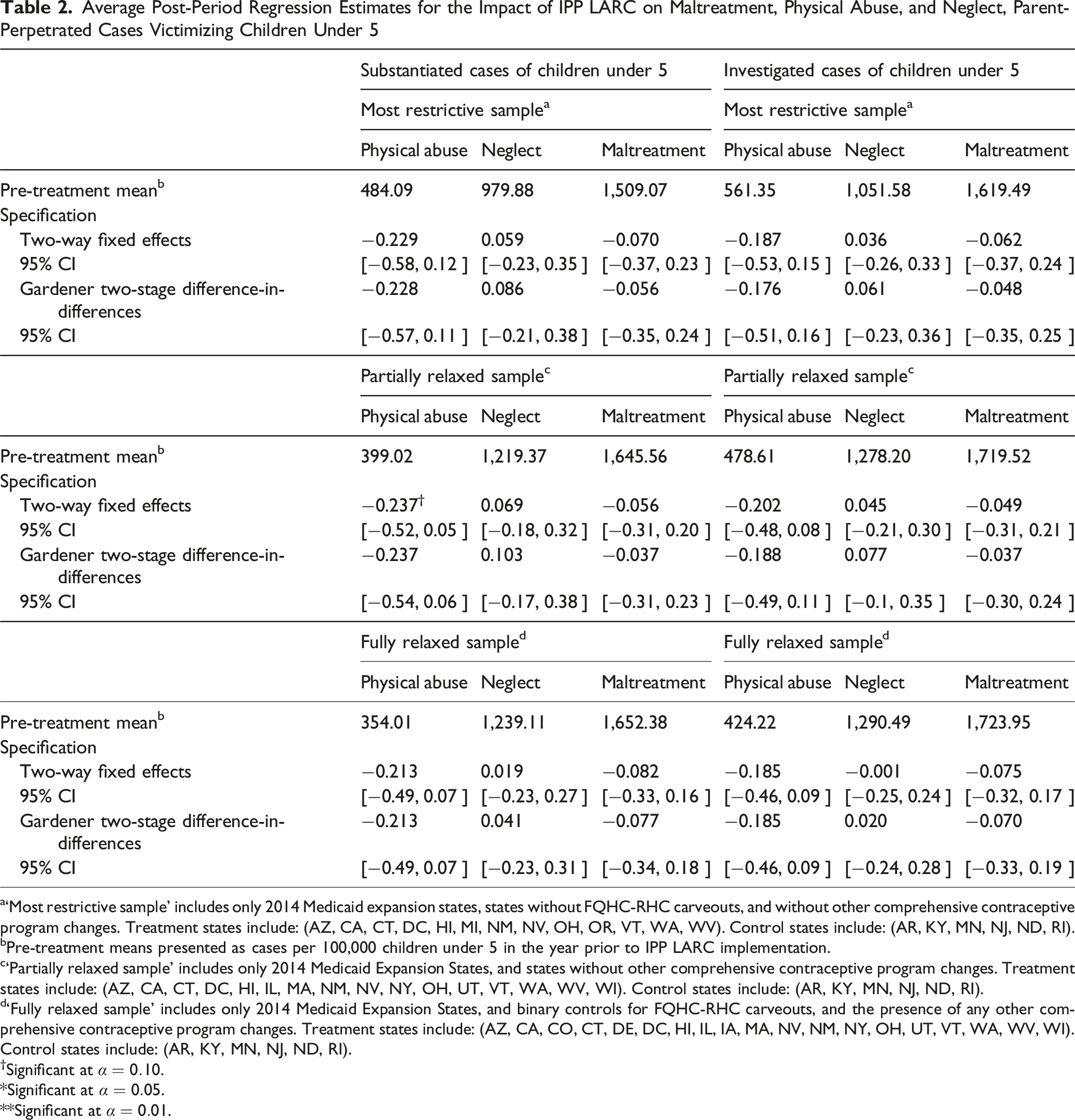
a‘Most restrictive sample’ includes only 2014 Medicaid expansion states, states without FQHC-RHC carveouts, and without other comprehensive contraceptive program changes. Treatment states include: (AZ, CA, CT, DC, HI, MI, NM, NV, OH, OR, VT, WA, WV). Control states include: (AR, KY, MN, NJ, ND, RI).
bPre-treatment means presented as cases per 100,000 children under 5 in the year prior to IPP LARC implementation.
c‘Partially relaxed sample’ includes only 2014 Medicaid Expansion States, and states without other comprehensive contraceptive program changes. Treatment states include: (AZ, CA, CT, DC, HI, IL, MA, NM, NV, NY, OH, UT, VT, WA, WV, WI). Control states include: (AR, KY, MN, NJ, ND, RI).
d‘Fully relaxed sample’ includes only 2014 Medicaid Expansion States, and binary controls for FQHC-RHC carveouts, and the presence of any other comprehensive contraceptive program changes. Treatment states include: (AZ, CA, CO, CT, DE, DC, HI, IL, IA, MA, NV, NM, NY, OH, UT, VT, WA, WV, WI). Control states include: (AR, KY, MN, NJ, ND, RI).
†Significant at
*Significant at
**Significant at
A negative relationship was observed between IPP LARC carveouts and state rates of parent-perpetrated physical abuse, however this relationship did not reach the 0.05 threshold for statistical significance. Figure 4 displays event studies and average treatment effect on the treated (ATT) estimates derived using TWFE. All specifications include aforementioned covariates (state-year Medicaid income eligibility threshold for pregnant beneficiaries, population proportion that are women of reproductive age, total child welfare expenditures, population proportion at or below the federal poverty level, Medicaid expansion status, and population proportion identifying as Black, and population proportion identifying as Hispanic). The left column displays models performed on the most restrictive sample, the center column displays models performed on the partially relaxed sample, and the right column displays models performed on the most relaxed sample. Row one displays models performed on substantiated physical abuse cases, and row two displays models performed on investigated physical abuse cases. Marginal significance ( Two-way fixed effects event studies & estimates, parent-perpetrated cases of child physical abuse victimizing children under 5.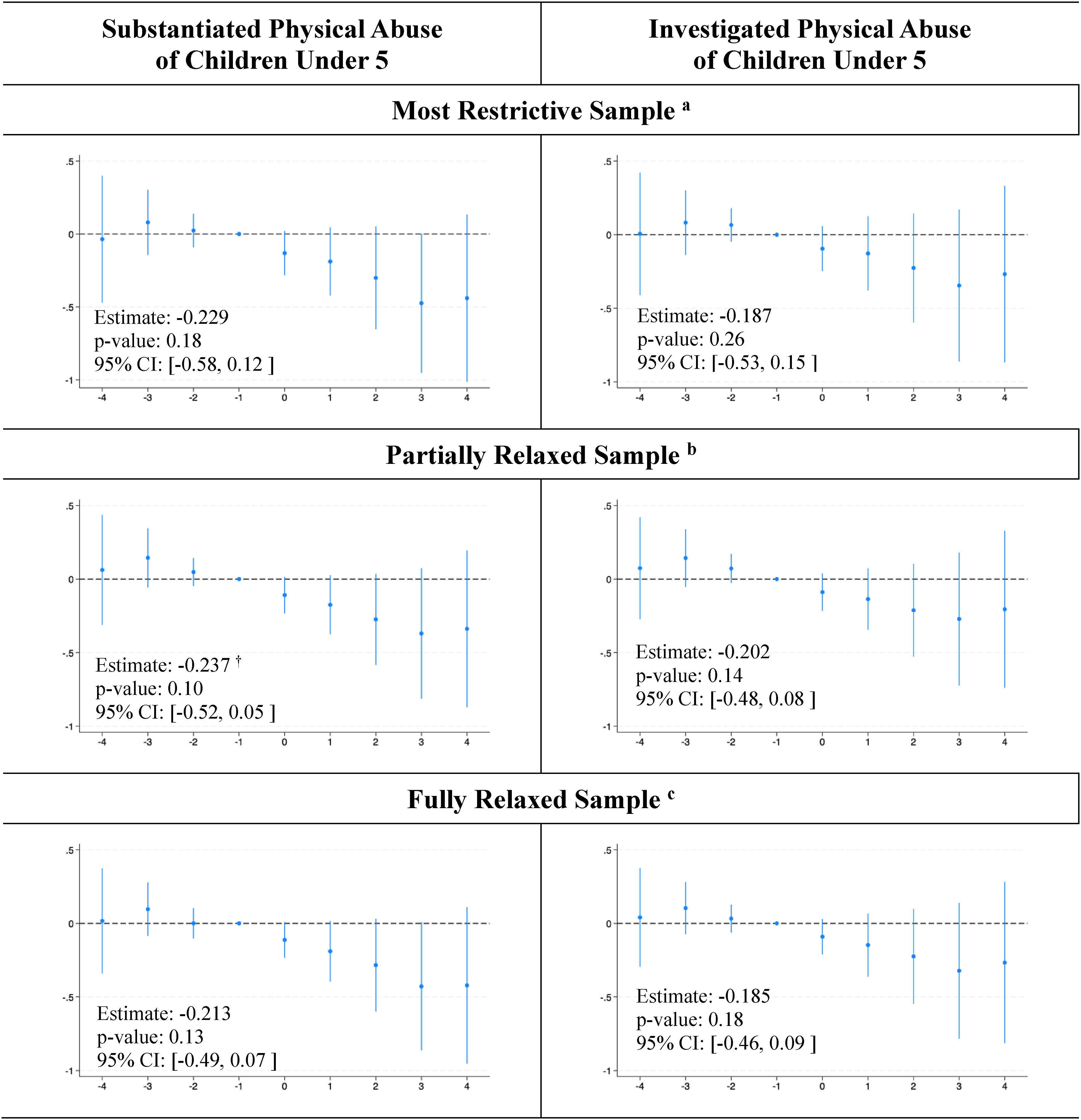
One limitation of the NCANDS data is the inability to observe exposure to Medicaid coverage or take-up of IPP-LARC. As a sensitivity test, we restricted the sample to states with above median deliveries covered by Medicaid (Figure 5). In the TWFE sensitivity analyses, statistical significance was observed across samples for both investigated and substantiated parent-perpetrated physical abuse. This confers support for the underlying mechanism in that as the proportion of potentially eligible patients increases, so too does the impact’s estimated magnitude and significance. Specifically, in the most restrictive sample, estimates were significant, negative and larger in magnitude than the primary specification (ATT = −33.7%, p-value: 0.05 for substantiated physical abuse; ATT = −38.7%, p-value: 0.05 for investigated physical abuse) (see Figure 5). Two-stage difference-in-differences event studies & estimates, parent-perpetrated cases of child physical abuse victimizing children under 5 within states with above-median proportions of Medicaid-covered births.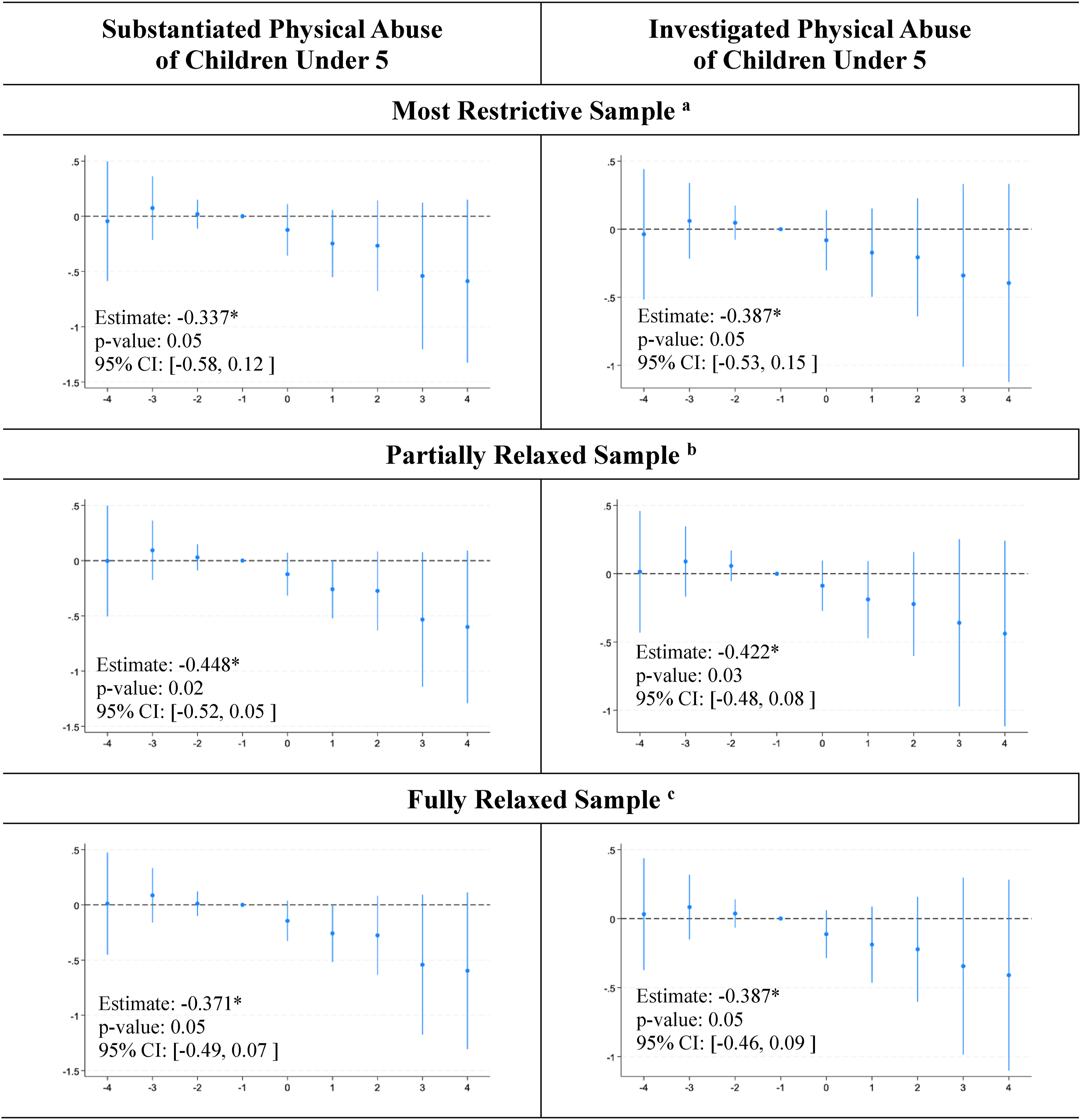
Gardener’s two-stage DD estimates are summarized in Figure 6. In this series, state rates of substantiated physical abuse were approaching marginal significance in the partially (ATT = −23.7%, p-value: 0.12) and fully relaxed (−21.3%, p-value: 0.13) samples. In the most restrictive sample, substantiated and investigated estimates were again negative, smaller in magnitude, and less significant. The ATT for investigated physical abuse in the most restrictive sample was −17.6% (p-value: 0.30) and 22.8% for substantiated physical abuse (p-value: 0.19). Two-stage difference-in-differences event studies & estimates, parent-perpetrated cases of child physical abuse victimizing children under 5.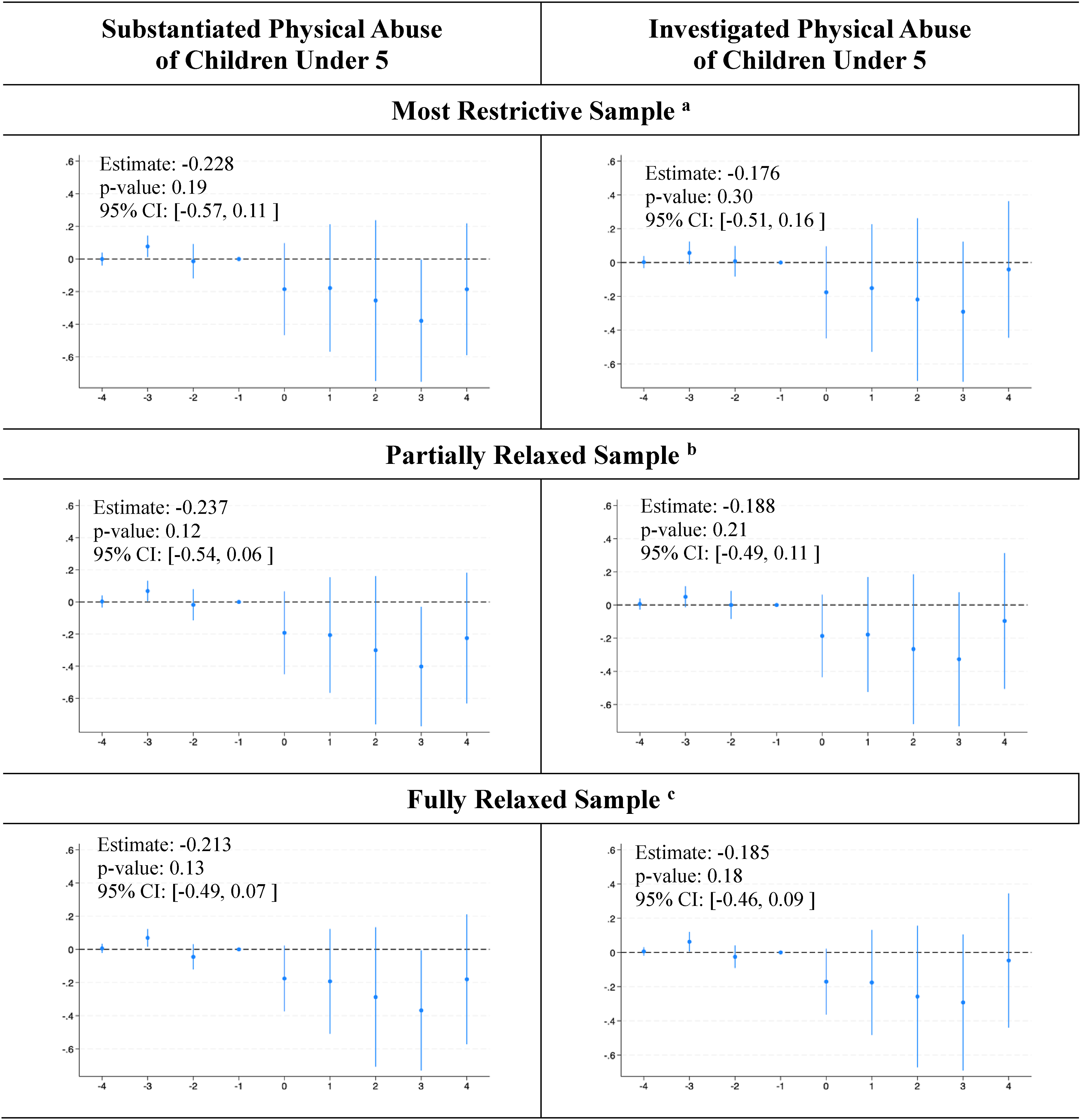
Corresponding estimates and event studies analyses are available in Appendix Figures 1-2 for parent-perpetrated neglect rates, and in Appendix Figures 3-4 for parent-perpetrated maltreatment rates.
After restricting the sample to states with above median deliveries covered by Medicaid (Figure 7), two-stage DD sensitivity analyses suggest that the policy was associated with significant reductions in investigated cases of physical abuse (ATT = −19.1%, p-value: 0.04). The point estimate for substantiated physical abuse was of similar magnitude, but did not reach statistical significance (ATT = −28.3%, p-value: 0.08). Two-stage difference-in-differences event studies & estimates, parent-perpetrated cases of physical abuse victimizing children under 5 within states with above-median proportions of Medicaid-covered births.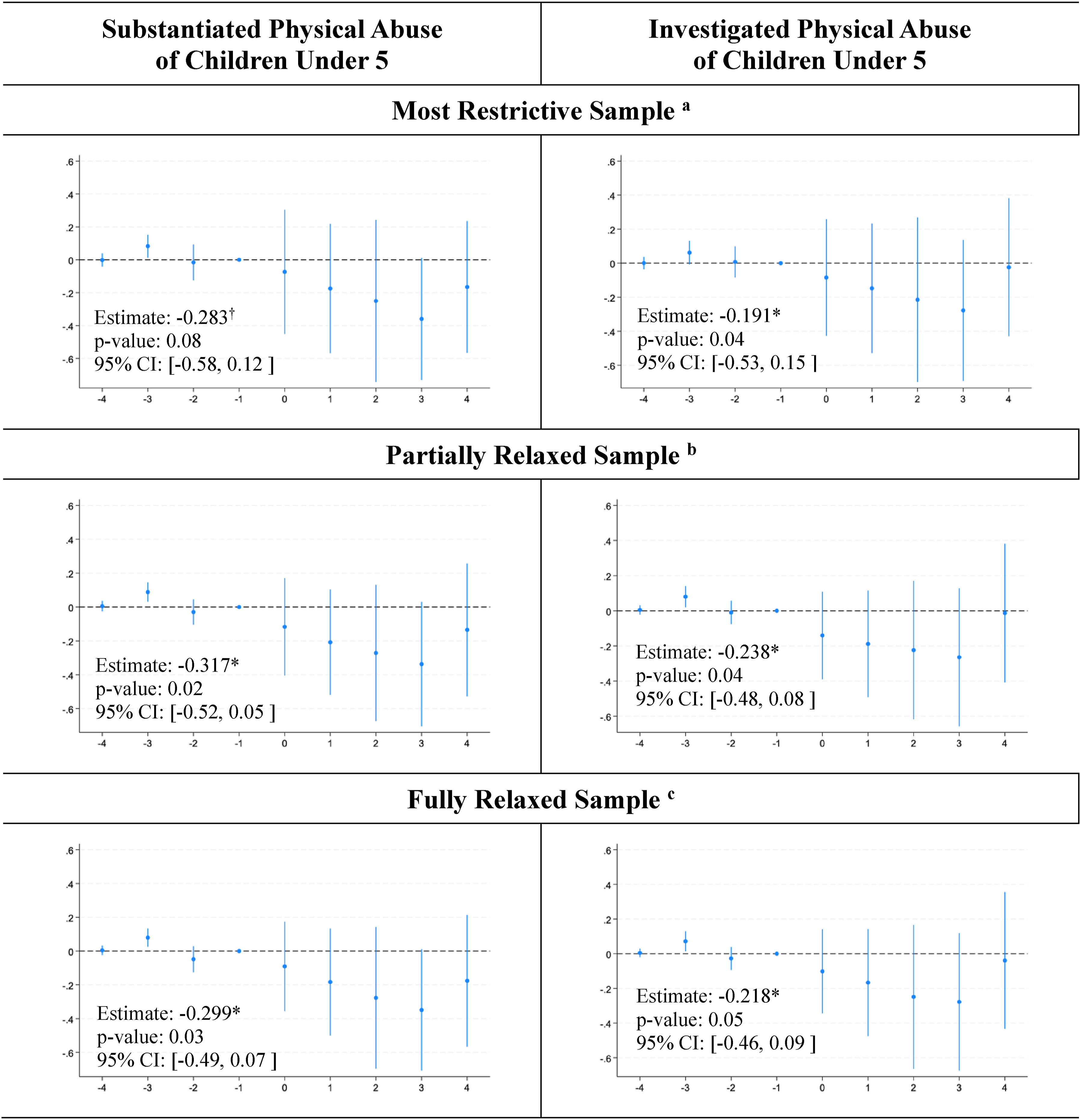
Rates of non-parent perpetrated cases maltreatment, physical abuse, and neglect toward children under 5 appear unrelated to IPP LARC carveouts (see Appendix Table 1), which supports the prior hypothesis that IPP LARC carveouts are only associated with parent-perpetrated maltreatment.
Discussion
Our findings suggest IPP LARC carveouts did not yield significant reductions in substantiated parent-perpetrated physical abuse (ATT = −22.9% or 49.97 fewer cases per 100,000 children under 5, p-value = 0.18) nor investigated parent-perpetrated physical abuse (ATT = −18.7% or 57.78 fewer cases per 100,000 children under 5, p-value = 0.26). However, results from sensitivity analyses among states with above median births covered by Medicaid suggested the policies were associated with fewer (ATT = −33.7% or 74 fewer cases per 100,000 children under 5) substantiated parent-perpetrated physical abuse cases and a 38.7% reduction (120 fewer cases per 100,000 children under 5) of investigated cases of parent-perpetrated physical abuse. These mixed findings suggest we may not have the power to detect population-level reductions. Collectively, our findings provide suggestive evidence that state decisions to allow Medicaid providers to bill separately for LARC placement may be associated with reductions in parent-perpetrated physical abuse toward children under five. However, our analysis did not have the power necessary to come to firm conclusions.
None of the findings offered here should be contorted to justify policies that threaten the ability of certain individuals (based on income or other identity) to have children when they desire. The harmful, and recent history of eugenic practices encountered particularly by communities of color create barriers for many patients (Gomez et al., 2014; Thorburn & Bogart, 2005). Evidence suggests inequitable recommendations/prescribing practices remain a concern (Dehlendorf et al., 2010). As the reproductive autonomy landscape continues to evolve, future research should aim to understand potential heterogeneity of policy impacts across demographic groups.
Limitations
A key limitation of this work is the inability to isolate children with parents that may be eligible for Medicaid, and most directly impacted by IPP LARC carveouts. This limitation likely dilutes estimates relative to the policy change’s true impact, as evidenced by the differences in estimates yielded by our primary specification and by our sensitivity analyses accounting for differences in the proportion of births covered by Medicaid. While NCANDS includes a general ‘public aid’ indicator for whether a child’s family is receiving support from any number of public programs, it is not populated consistently enough for a subsample to be explicitly identified. However, prior works indicate that efforts to improve contraceptive access for low-income populations who desire them increase IPP LARC uptake among publicly and privately insured populations alike (Caudillo et al., 2022b; Steenland et al., 2021b; Yoder & Boudreaux, 2023). Post-enactment provider behavior changes regardless of their patient’s primary payor.
Further, it is not possible to ascertain information regarding affected families’ size or birth spacing. The inability to adjust for/stratify by family size and birth spacing impedes understanding of potential heterogeneity of IPP LARC carveouts impact across family compositions. As the reproductive autonomy landscape continues to evolve, future research should aim to understand potential heterogeneity of policy impacts across demographic groups. These analyses may be particularly important as evidence suggests inequitable contraception recommendations and prescribing practices across sociodemographic groups remain a concern (Dehlendorf et al., 2010). These trends may render differences in parents’, and therefore children’s propensity to benefit from changes in LARC access policies.
Conclusions
Policies that enable separate reimbursement for IPP LARC may be protective against parent-perpetrated physical abuse toward children under five (Aslim et al., 2024). Continued investigation of policy-driven approaches to support child wellbeing should consider factors that influence access to healthcare.
Supplemental Material
Supplemental Material - Immediate Postpartum Long-Acting Reversible Contraception Access and Child Maltreatment Rates
Supplemental Material for Immediate Postpartum Long-Acting Reversible Contraception Access and Child Maltreatment Rates by Hannah Rochford, Daniel Marthey, Elena Andreyeva in Child Maltreatment.
Footnotes
Acknowledgements
The authors would like to thank attendees at various seminar and conference presentations of this project’s preliminary findings for their constructive feedback. Dr. Hannah Rochford conceptualized the study, co-designed the analyses, performed all analyses, generated all tables and figures, drafted the initial manuscript, and critically reviewed and revised the manuscript. Dr. Daniel Marthey acquired and managed secure storage for the restricted outcome data, co-designed the analyses, and critically reviewed and revised the manuscript narrative, tables, and figures. Dr. Elena Andreyeva co-designed the analyses, and critically reviewed and revised the manuscript narrative, tables, and figures.
Ethical Considerations
This study was deemed non-human subject research by the Institutional Review Board of Texas A&M University.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The outcome data applied here is derived from restricted National Child Abuse and Neglect Data System (NCANDS) Child files. These can be requested here: https://www.ndacan.acf.hhs.gov/datasets/request-restricted-data.cfm. All explanatory data can be accessed from Bogan C, Marthey D. Health Policy and Access to Long-Acting Reversible Contraceptives. University of Delaware, Center for Community Research and Service; 2021. ![]() . All outcome data was accessed from public sources specified in the methods session.
. All outcome data was accessed from public sources specified in the methods session.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.