
Abstract
The Continuum of Care Reform (CCR) aimed to reduce California’s reliance on congregate care by expanding behavioral health services for youth in family-like placements. This is the first study to leverage population-level data to explore this policy’s impact despite its implementation a decade ago. Using a sample of 17,344 adolescents in California’s foster care system, this study examined changes in congregate care outcomes following the CCR. Results indicated that youth in care after the CCR had a lower likelihood of congregate care placement and fewer congregate care placements overall. However, they experienced a greater risk of out-of-county congregate care placements, and the amount of time spent in congregate care remained unchanged. Findings suggest the CCR has yielded mixed results, highlighting opportunities to integrate behavioral health services across all placement types. Further collaboration between child welfare and behavioral health systems may be needed to fully realize the CCR’s vision.
Introduction
In the United States, nearly one in five youth ages 11 to 17 in out-of-home care are placed in group homes or residential treatment facilities (“congregate care 1 ”; U.S. Department of Health and Human Services, nd). Congregate care refers to group care settings that provide 24-hour supervision and, in some cases, treatment to youth in out-of-home care. Historically considered a “placement of last resort” (James, 2011), congregate care is increasingly reserved for adolescents whose behavioral health needs cannot be met in family-like placements (e.g., kinship care, therapeutic foster care; U.S. Children’s Bureau, 2015).
Despite this shift, the use of congregate care remains controversial (Dozier et al., 2025). Congregate care is costly, and evidence of its effectiveness is limited and mixed (Alpert & Meezan, 2012; James, 2011). Leading scholars in developmental science have all but condemned congregate care, calling it a harmful alternative to family-based care (Dozier et al., 2025; Van IJzendoorn & Bakermans-Kranenburg, 2022; van IJzendoorn et al., 2020). However, evidence supporting their claims is of questionable relevance, with many researchers citing studies of child institutions and group care settings that hardly resemble modern congregate care facilities in the U.S. (Dozier et al., 2025; van IJzendoorn et al., 2020). In the child welfare literature, several studies report correlations between congregate care and later placement instability, legal system involvement, and inadequate social support (Park et al., 2025; Prindle et al., 2025; Zinn & Havlicek, 2014). Still, few studies have shown that congregate care uniquely causes (or prevents) negative outcomes. Links between congregate care and poor outcomes often disappear after accounting for placement instability, behavioral health issues, maltreatment histories, and other factors shaping the population in congregate care (Okpych & Courtney, 2015).
A Developmental Dilemma
Efforts to create a developmentally-informed child welfare system have sparked discussions about balancing the at-times conflicting behavioral health and developmental needs of adolescents in care. Known as the “second window of opportunity,” adolescence kickstarts a period of immense neuroplasticity and brain development (Dahl et al., 2018; Dahl & Suleiman, 2017; Dozier et al., 2025). These neurological changes prime adolescents to explore and engage in social and relational learning contexts, which inform identity development, the understanding of self-other relationships, and motivations to contribute to society (Dahl et al., 2024). Over time, social learning experiences lay the foundation for self-sufficiency and well-being in early adulthood.
Youth in congregate care often have a strong need for positive social and relational learning experiences. These youths are more likely to have insecure and disorganized attachments, which can impede their engagement in social learning (Lionetti et al., 2015; Muzi & Pace, 2022). Although any out-of-home placement can restrict opportunities for social exploration and identity development (Berzin et al., 2014; Massinga & Pecora, 2004), congregate care facilities may be particularly ill-equipped to meet adolescents’ social learning needs. These facilities are more restrictive than family-like placements and are more likely to be farther from youths’ communities (Kelly et al., 2019; Zelechoski et al., 2013), therefore hindering social exploration and straining relationships with loved ones. Limited training, shift staffing models, and complex caseloads can prevent facility personnel from effectively serving as substitutes for caregivers and mentors who facilitate adolescents’ social learning (Dahl et al., 2018; Kelly et al., 2019; Morris et al., 2017; Santos et al., 2023; Schwartz et al., 2012).
Although family-like placements are generally considered more developmentally appropriate (Bakermans-Kranenburg & Van IJzendoorn, 2024), caregivers may not have the training to effectively address youths’ behavioral health needs. Unaddressed behavioral health needs are a leading cause of disruption in family-like placements, which can result in greater behavioral problems, poorer social outcomes, and a lower likelihood of reunification (Chamberlain et al., 2006; Konijn et al., 2019). In short, finding placements that are developmentally and clinically fit for adolescents with complex needs remains a challenge for child welfare agencies.
Past Efforts to Reduce Congregate Care Utilization
Concerned about the developmental consequences of prolonged stays in group care, some states have launched initiatives to minimize congregate care utilization. Studies of these efforts highlight the need for a robust network of therapeutic, family-based alternatives before closing congregate care facilities. Illinois closed many of its group homes before enhancing its network of therapeutic foster care homes, resulting in increased placement instability as youth moved between non-therapeutic foster homes before eventually entering residential treatment (Budde et al., 2004). Conversely, Tennessee expanded its use of therapeutic foster care, which offered a clinically suitable alternative to group homes (Alpert & Meezan, 2012).
The Continuum of Care Reform
California’s Assembly Bill 403 (2015) marked a similar shift in the state’s approach to addressing the behavioral health and developmental needs of youth in foster care. Known as the Continuum of Care Reform (CCR), this law combined existing and new reforms to prioritize family-like foster care placements. Like efforts in Illinois and Tennessee, the CCR’s focus on family-like care was rooted in the belief that youth fare better developmentally when surrounded by family (i.e., kinship care) or other adults with whom they can forge enduring, caregiving relationships (California Department of Social Services, nd). Among other changes, the CCR aimed to create a family-forward child welfare system by increasing resources for kinship caregivers, enhancing crisis services for youth in family-like placements, and introducing child and family team decision-making (California Department of Social Services, nd).
Importantly, the CCR codified concerns about the developmental consequences of congregate care into policy. The fundamental principles of the CCR state that “all children in foster care [should experience] normalcy in development while establishing permanent, lifelong family relationships. Therefore, children should not remain in a group living environment for long periods of time” (California Department of Social Services, nd). The CCR aimed to reduce California’s reliance on congregate care by (1) integrating behavioral health services into family-like placements, and (2) converting existing group homes into short-term residential therapeutic programs (STRTPs)—a new type of facility staffed with personnel offering trauma-informed services to youth aged 12 and older with complex behavioral needs. The newfound therapeutic orientation of STRTPs was intended to stabilize youth and prepare them to transition into family-like settings over a short period of time. Consistent with the CCR’s developmental principles, STRTP placements were limited to six months, except in certain circumstances. Ideally, integrated behavioral health supports in family-like placements would offer ongoing treatment after leaving an STRTP, thereby reducing the need for future STRTP placements.
Current Progress
Only one peer-reviewed study has examined the CCR’s effects. Using a sample of 359 child welfare-supervised youth from one Southern California county, Metcalf et al. (2022) reported improvements in placement stability following the CCR. Nonetheless, youth were less likely to be placed in family-like settings after the CCR, and the length of congregate care stays remained the same. The authors attributed mixed findings to the closure of congregate care facilities before family-based alternatives could be put in place. Publicly available data support this interpretation. Legislative reports show the number of congregate care facilities in California declined by more than 50% between 2019 and 2024 (California Department of Social Services, 2019; 2024a), largely because existing group homes did not meet the stricter STRTP licensing requirements. In a case of unfortunate timing, rising insurance and operational costs for foster family agencies (FFAs), private agencies that operate most intensive services foster homes (i.e., therapeutic foster care) in California, simultaneously limited the number of family-like placements with behavioral health supports (California Alliance, 2024; Lara, 2024).
The resulting decrease in treatment-oriented settings left many counties with few or no viable settings for youth with complex needs. As of November 2025, 21 California counties had no STRTPs, and an additional nine counties had only one (California Community Care Licensing Division, 2025). Consequently, youth in need of residential care may be more likely to experience an out-of-county placement. While such placements may be clinically appropriate, placing youth outside of their counties of origin can disrupt family, peer, and community relationships that form the crucible for social and relational learning during adolescence. Considering the length of congregate care placements has remained the same (Metcalf et al., 2022), extended stays in out-of-county STRTPs may be especially detrimental to youths’ development and well-being.
Current Study
The CCR aimed to balance the developmental and behavioral needs of youth in foster care. However, emerging data indicate that some aspects of its implementation may have had unintended developmental consequences. To date, there remains a paucity of population-level studies examining congregate care outcomes after the CCR. Building evidence on the CCR’s impact is important at both the state and national levels. The Family First Prevention Services Act (FFPSA; Bipartisan Budget Act, 2018) adopted a similar approach toward minimizing congregate care placements nationwide. While they share similar goals, the CCR was enacted two years before the FFPSA, providing a natural experiment to assess the FFPSA’s potential nationwide effects.
To this end, the present study is the first to utilize population-level data to analyze changes in four outcomes directly related to the CCR’s objectives of aligning congregate care practices with the developmental needs of adolescents in care. Specifically, this study answers four questions: (1) How have rates of congregate care placements changed after the CCR?; (2) How have rates of out-of-county congregate care placements changed after the CCR?; (3) Has the average time spent in congregate care changed after the CCR?; and (4) Has the average number of congregate care placements changed after the CCR?
Method
Sample and Design
Data were derived from statewide administrative child protective case records from California’s Child Welfare Services Case Management System (CWS/CMS). Administrative records were accessed through a longstanding research partnership between the California Department of Social Services (CDSS) and the California Child Welfare Indicators Project at the University of California, Berkeley. Their use for research was approved by California’s Committee for the Protection of Human Subjects (PROTOCOL ID: 12-10-0800) and the Office for Protection of Human Subjects at the University of California, Berkeley (PROTOCOL ID: 2010-01-592).
The sample includes 17,344 youth who (1) were placed in child welfare-supervised foster care between the ages of 12 and 17, (2) stayed in care for at least eight days, and (3) were not initially placed in congregate care. Youth were assigned to one of two mutually exclusive cohorts (pre- or post-CCR) based on whether they turned 18 before (2013-2014) or after (2023-2024) CCR implementation. The sampling strategy was guided by the developmental framework, the CCR’s design and implementation, and the analytic approach. The observation period (between youths’ 12th to 18th birthdays) aligns with the CCR’s goal to limit congregate care placements to youth ages 12 and older (California Department of Social Services, nd). This timeframe also coincides with increased neuroplasticity and social development during adolescence. I adapted Metcalf and colleagues’ (2022) approach by selecting cohorts of youth whose adolescence (the period between youths’ 12th and 18th birthdays) occurred entirely before or after the CCR’s implementation (see Appendix A, Figure A for a sampling frame timeline). The CCR included a sunrise provision that allowed county child welfare agencies to transition group homes into STRTPs ahead of its official implementation in January 2017 (California State Association of Counties, 2016). I incorporated a policy “washout” period by excluding adolescents in care during the sunrise period (2015-2016). Youth were followed until their 18th birthday, final exit from care, or three years after their first adolescent entry (whichever came first; see Analytic Plan for more information).
Finally, I excluded adolescents whose first placement was in congregate care (N = 3,006). First, these youth may differ systematically from those first placed in less restrictive environments. Second, these youth would be excluded from survival models because they have a survival time of zero (see Analytic Plan for more details). First placements in congregate care became less common following the CCR (19.3% vs. 8.6%, OR = 0.39, p < .001, 99% CI [0.35, 0.44]. More details about excluded youth can be found in Appendix A (Table A).
Measures
Dependent Variables
Four dependent variables were used to assess changes in congregate care outcomes: (1) congregate care placement, (2) out-of-county congregate care placement, (3) months spent in congregate care, and (4) number of congregate care placements. Congregate care placement measured whether youth were ever placed in a group home or STRTP during adolescence (1 = yes, 0 = no). Out-of-county congregate care placement measured whether youth were ever placed in a group home/STRTP outside their supervising county (1 = yes, 0 = no). Months spent in congregate care measured the cumulative months that youth spent in a group home/STRTP during adolescence. This was calculated by totaling the number of days spent in congregate care during adolescence and dividing by 30. Number of congregate care placements measured the number of group home/STRTP placements during adolescence.
Independent Variable
Post-CCR indicated whether youth were in care before or after the implementation of the CCR. Pre-CCR youth (youth who turned 18 in 2013 or 2014) were coded as 0, while post-CCR youth (youth who turned 12 in 2017 or 2018) were coded as 1.
Covariates
Multivariate models accounted for demographic and case characteristics associated with congregate care (Palmer et al., 2020; Prindle et al., 2025; Zinn & Havlicek, 2014). Demographic characteristics included birth sex, race and ethnicity, mental health concerns, and substance use concerns. Birth sex was measured as male and female, with female used as the reference group (male = 1, female = 0). Race and ethnicity were recoded into five dichotomous variables based on two administrative data fields (primary race and Hispanic status) entered by caseworkers: Latine 2 , Black, White, Multiracial, and Other (Native American, Asian/Pacific Islander, and Missing). Latine was the largest group and used as the referent. Mental health concerns indicated that a caseworker documented the youth was diagnosed with or exhibited any of the following conditions or behaviors: suicidal ideation or behavior, violence toward self or others (including externalizing behaviors and disorders), psychiatric hospitalization, psychotropic medication use, disordered eating (Anorexia or Bulimia Nervosa), depression, emotional disturbance, bipolar disorder, or schizophrenia (yes = 1, no = 0). Substance use concerns indicated that a caseworker documented substance use issues (yes = 1, no = 0).
Case characteristics included substantiated child maltreatment, age at first foster care entry, months in care, number of placements, placement in kinship care, probation supervision, and county urbanicity. Substantiated child maltreatment was measured using five dichotomous (yes = 1, no = 0) variables indicating the presence of a substantiated allegation of neglect, abuse (physical, sexual, and emotional), and exploitation (labor or commercial sexual exploitation). Age at first foster care entry was a categorical variable indicating youth’s age at their first child welfare-supervised foster care placement (0 = age 0–5; 1 = age 6–11; 2 = age 12–17). Months in care measured the cumulative months that youth spent in care during adolescence. To improve the interpretability of the zero-truncated negative binomial models, I collapsed this variable into time in care, a dichotomous variable indicating whether youth had been in care for two or more years (≥2 years = 1, <2 years = 0). Number of placements measured the cumulative number of placements during adolescence. Placement in kinship care indicated whether youth were ever placed with a relative or non-related extended family member during adolescence (yes = 1, no = 0). Probation supervision indicated whether youth had ever been in probation-supervised foster care, adjudicated 601/602, or incarcerated (yes = 1, no = 0). County urbanicity categorized youths’ supervising county by population size, resulting in four categories: rural, urban, large urban, and Los Angeles County (referent). Los Angeles County was separated from other large counties because it supervises one-third of California’s foster care population. The large size of Los Angeles County’s foster care population is not surprising given that it is home to a quarter of California’s total population (U.S. Census Bureau, 2024).
Analytic Plan
Analyses were conducted using Stata 17 (StataCorp, 2021). Following a descriptive analysis, I explored the unadjusted associations between CCR implementation and youth outcomes using bivariate logistic and zero-truncated negative binomial regression. Next, I fitted two multivariate Cox proportional hazard models with time-varying covariates to examine associations between CCR implementation and the rate of congregate care placement and out-of-county congregate care placement. Hazard models estimate the hazard function for the event time of individual youth (e.g., timing of youths’ first congregate care placement). The following variables were modeled as time-varying covariates: mental health concerns, substance use concerns, substantiated child maltreatment, months in care, number of placements, placement in kinship care, and probation supervision. Months in care and number of placements were modeled as running counts, while the other dichotomous covariates switched from zero to one based on the date they were recorded in the youth’s case file.
Cox models used the Breslow method for ties and set t = 0 as the first day the youth spent in foster care during adolescence. Survival time was measured in months. Survival time did not include gaps introduced by runaway episodes or periods when youth had exited care before reentering during the observation period. Observations were censored at the youth’s 18th birthday, final exit from foster care, or three years after their first adolescent entry—whichever occurred first. I added this final criterion to ensure model stability and validity. Nearly 90% of youth spent less than three years in care, which limited the ability to reliably model outcomes beyond 36 months. I examined Schoenfeld residuals and used Stata’s phtest procedure to check for violations of the proportional hazards assumption. Results indicated that race (Black) and county urbanicity violated this assumption in the first model, suggesting the presence of time-varying coefficients. Time-varying coefficients occur when a variable with a fixed value has a time-varying effect on survival time (StataCorp, 2025; Zhang et al., 2018). I modeled these variables following the procedure outlined in StataCorp (2025) and report hazard ratios at t = 0 and t = 36. I confirmed the robustness of this approach by stratifying Model 1 by race and county urbanicity (not shown). Results were nearly identical.
I used zero-truncated negative binomial regression to examine changes in the number of months and placements in congregate care. Zero-truncated negative binomial regression is used to model overdispersed count data when a value of zero is not possible (UCLA Statistical Consulting Group, nd). Due to collinearity concerns, total time in care was omitted from the model examining months in congregate care. Total adolescent placements were omitted from the model assessing the number of congregate care placements. I report marginal means (MM) to facilitate interpretation. Given the use of population-level data, I used 99% confidence intervals to determine significant differences between the parameter and the observed estimate at the 1% level (p-values are reported for context but are not emphasized). When interpreting multivariate results, readers should note that covariate coefficients (e.g., youth and foster care characteristics) reflect associations regardless of whether youth were in care before or after the CCR.
Efforts to transition or close group homes continued after the CCR was implemented in 2017 (California Department of Social Services, 2024a). As a result, nearly one-third (30.1%) of the sample placed in congregate care after CCR implementation were placed in group homes. STRTPs are more treatment-oriented than group homes, and there may be differences in the outcomes of youths placed in STRTPs versus group homes. I addressed this by stratifying analyses of out-of-county congregate care, months in congregate care, and the number of placements based on post-CCR facility type: STRTPs only (n = 787), group homes only (n = 136), or both (n = 203). 3 Sensitivity analysis results are reported in the Results and Appendix A.
Results
Sample Characteristics (N = 17,664)
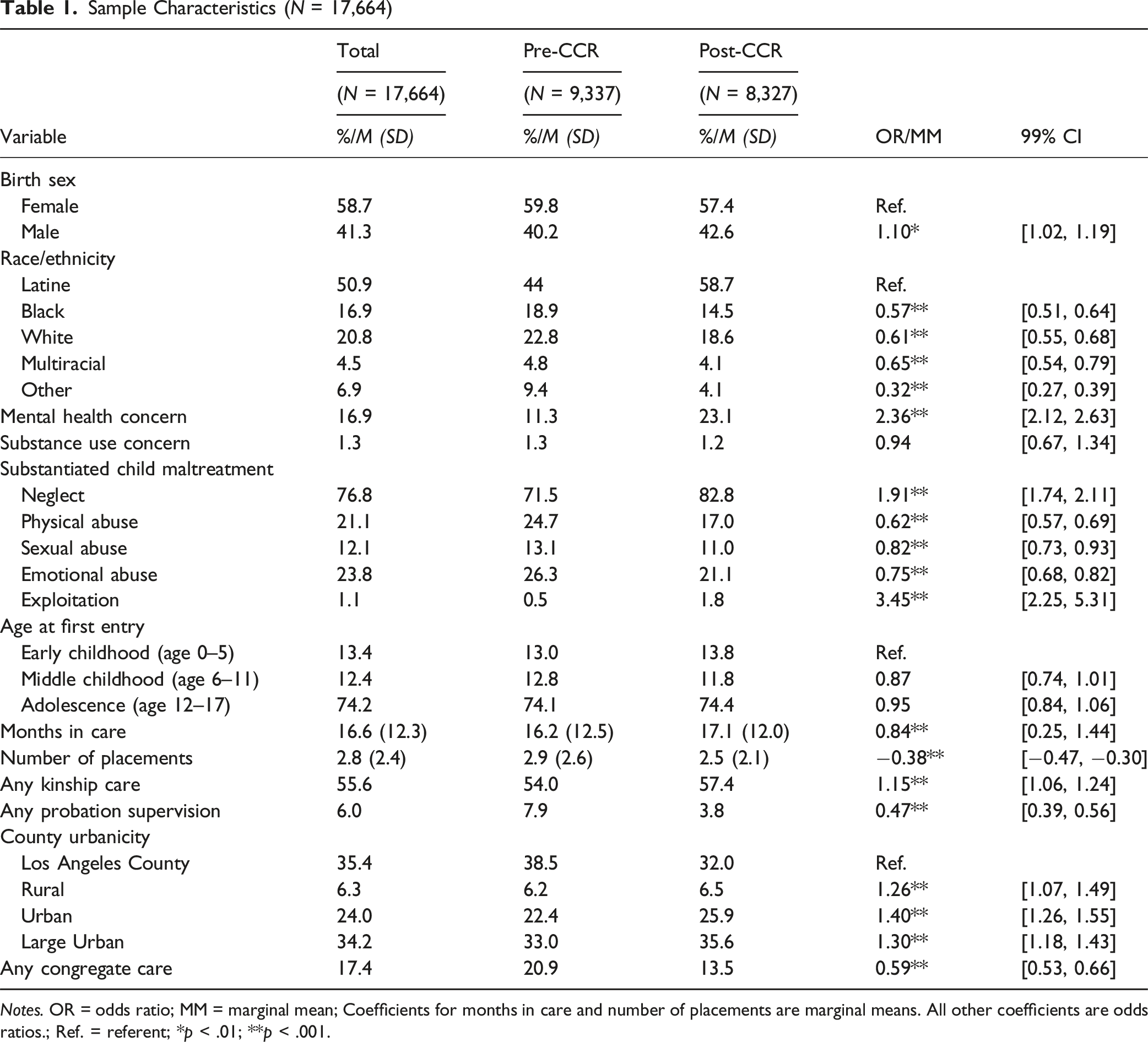
Notes. OR = odds ratio; MM = marginal mean; Coefficients for months in care and number of placements are marginal means. All other coefficients are odds ratios.; Ref. = referent; *p < .01; **p < .001.
Characteristics of Youth Placed in Congregate Care (N = 3,074)
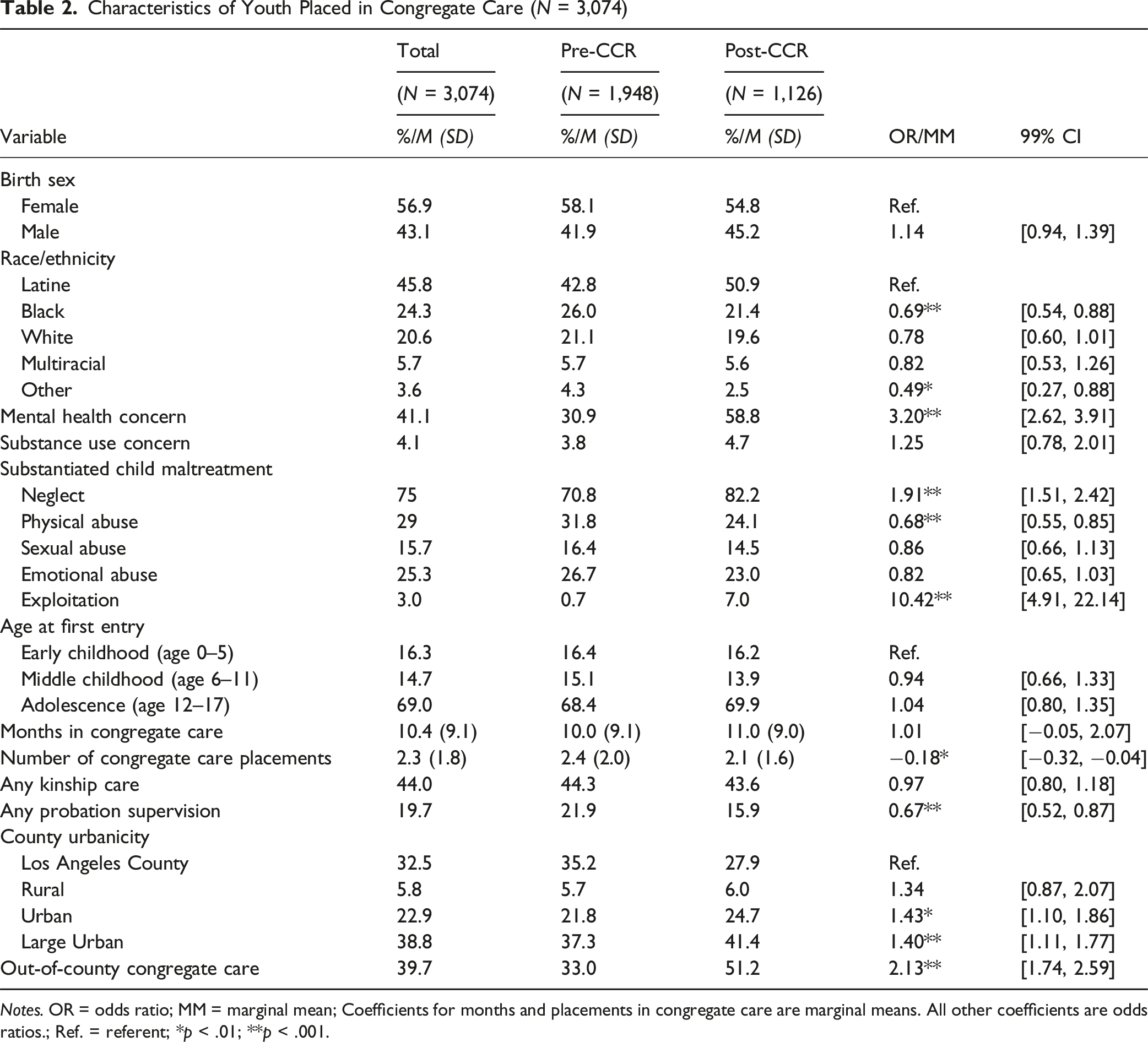
Notes. OR = odds ratio; MM = marginal mean; Coefficients for months and placements in congregate care are marginal means. All other coefficients are odds ratios.; Ref. = referent; *p < .01; **p < .001.
Estimated Hazard Ratios for Any and Out-of-County Congregate Care Placements
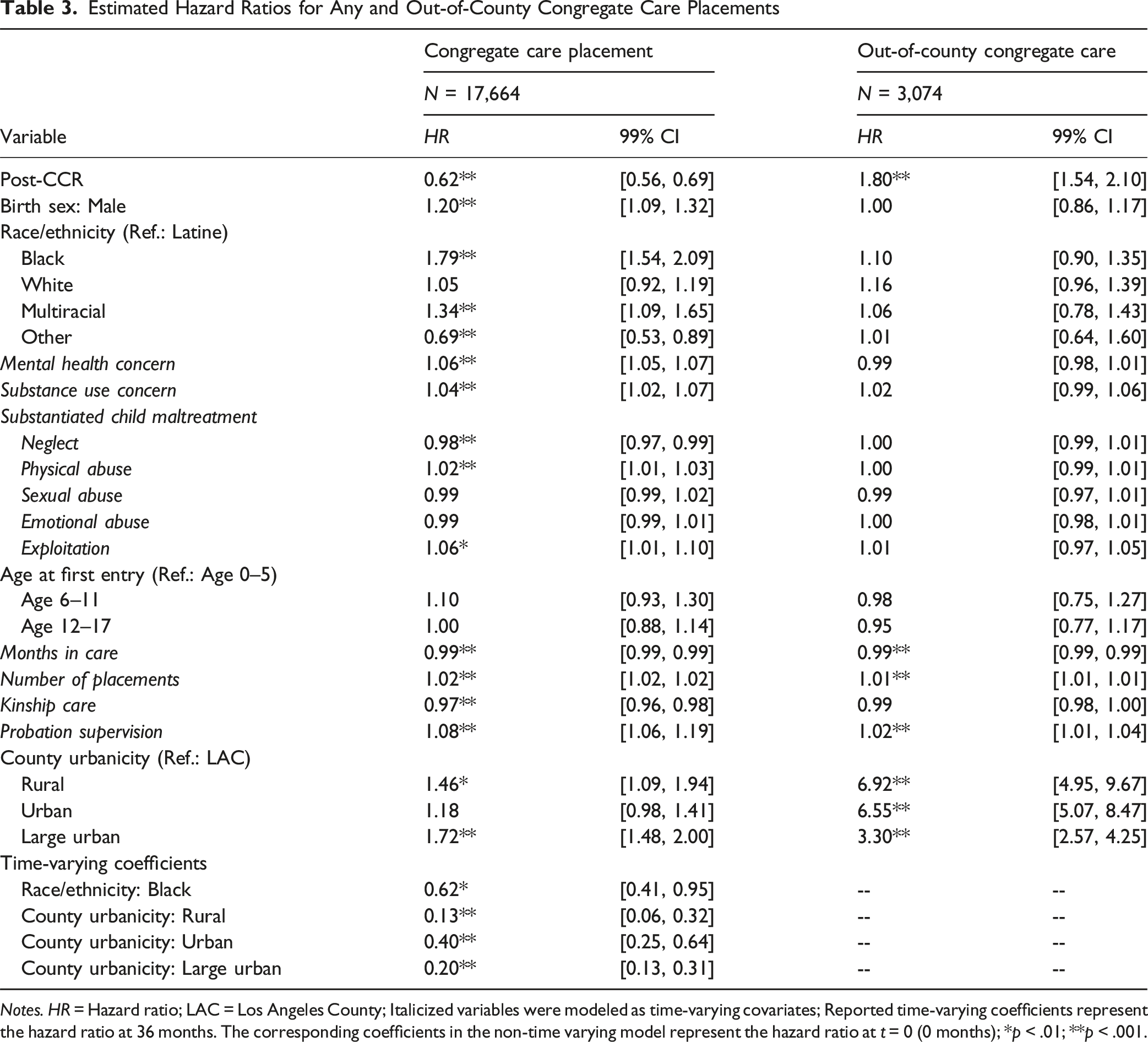
Notes. HR = Hazard ratio; LAC = Los Angeles County; Italicized variables were modeled as time-varying covariates; Reported time-varying coefficients represent the hazard ratio at 36 months. The corresponding coefficients in the non-time varying model represent the hazard ratio at t = 0 (0 months); *p < .01; **p < .001.
The rate of out-of-county congregate care placements rose by 80% following the CCR (HR = 1.80; 99% CI [1.54, 2.10], p < .001; Appendix A, Figure B2). Placement changes led to a 1% increase in the rate of an out-of-county placement (HR = 1.01, 99% CI [1.01, 1.01], p < .001). Conversely, the rate of out-of-county placements declined by 1% for each additional month spent in care (HR = 0.99, 99% CI [0.99, 0.99], p < .001). Youth supervised by rural (HR = 6.92, 99% CI [4.95, 9.67], p < .001), urban (HR = 6.55, 99% CI [5.07, 8.47], p < .001), and large urban counties (HR = 3.30, 99% CI [2.57, 4.25], p < .001) had higher rates of out-of-county placements compared to youth supervised by Los Angeles County.
Zero-Truncated Negative Binomial Models Predicting Time and Placements in Congregate Care (N = 3, 074)
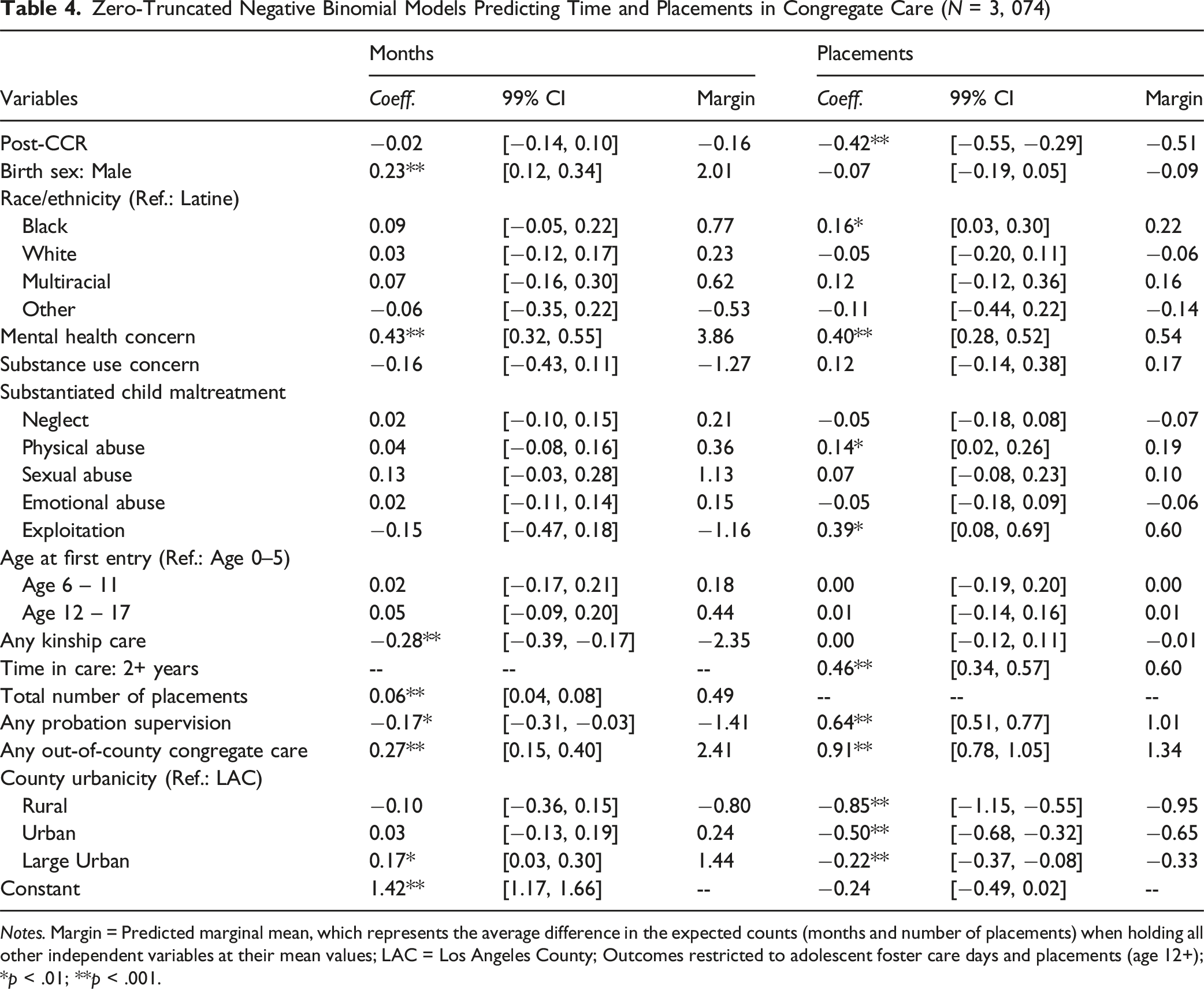
Notes. Margin = Predicted marginal mean, which represents the average difference in the expected counts (months and number of placements) when holding all other independent variables at their mean values; LAC = Los Angeles County; Outcomes restricted to adolescent foster care days and placements (age 12+); *p < .01; **p < .001.
On average, youth had 0.51 fewer congregate care placements following the CCR (coeff. = −0.42, 99% CI [−0.55, −0.29], p < .001). Black youth (MM = 0.22, coeff. = 0.16, 99% CI [0.03, 0.30], p = .002) and youth with a mental health concern (MM = 0.54, coeff. = 0.40, 99% CI [0.28, 0.52], p < .001) had more congregate care placements than Latine youth and youth without mental health concerns, respectively. Substantiated physical abuse and exploitation increased the average number of congregate care placements by 0.19 and 0.60, respectively (physical abuse: coeff. = 0.14, 99% CI [0.02, 0.26], p = .003; exploitation: coeff. = 0.39, 99% CI [0.08, 0.69], p = .001). Spending two or more years in care increased the average number of placements by 0.6 (coeff. = 0.46, 99% CI [0.34, 0.57], p < .001). Probation supervision increased the average number of placements by one (coeff. = 0.64, 99% CI [0.51, 0.77], p < .001). Youth placed in out-of-county congregate care facilities had 1.3 more placements, on average, than youth never placed out-of-county (coeff. = 0.91, 99% CI [0.78, 1.05], p < .001). Compared to youth from Los Angeles, youth from rural (MM = −0.95, coeff. = −0.85, 99% CI [−1.15, −0.55], p < .001), urban (MM = −0.65, coeff. = −0.50, 99% CI [−0.68, −0.32], p < .001), and large urban counties (MM = −0.33, coeff. = −0.22, 99% CI [−0.37, −0.08], p < .001) had fewer placements.
Sensitivity Analysis
Sensitivity analyses generally corroborated the primary findings. Among youth placed in congregate care after the CCR, 69.9% were placed in an STRTP, 12.1% in a group home, and 18% in both an STRTP and a group home (Appendix A, Table B). Compared to youth placed in group homes before the CCR, post-CCR youth in STRTPs were more likely to be placed out-of-county (HR = 1.78, 99% CI [1.50, 2.12], p < .001; Table C). Meanwhile, post-CCR youth placed in both facility types were more likely to be placed in an out-of-county group home or STRTP (HR = 2.19, 99% CI [1.70, 2.83], p < .001) than pre-CCR youth placed in group homes. The rate of out-of-county placements did not change for youth solely placed in group homes. Youth placed only in STRTPs or group homes did not show significant changes in the number of months spent in congregate care (STRTP: MM = −0.94, coeff. = −0.12, 99% CI [−0.25, 0.02], p = .03; group home: MM = −1.34, coeff. = −0.21, 99% CI [−0.53, 0.11], p = .10; Table D). Youth placed in both facility types spent nearly four more months in congregate care after the CCR (coeff. = 0.39, 99% CI [0.16, 0.62], p < .001). Youth placed in STRTPs or group homes alone had fewer congregate care placements after the CCR (STRTP: MM = −0.65, coeff. = −0.60, 99% CI [−0.76, −0.44], p < .001; group home: MM = −0.91, coeff. = −1.23, 99% CI [−1.68, −0.78], p < .001; Table E). Those placed in both facility types did not show a significant change in the number of congregate care placements (MM = 0.28, coeff. = 0.17, 99% CI [−0.02, 0.36], p = .02).
Discussion
This study is the first to use population-level data to examine changes in congregate care outcomes after the implementation of the CCR. Youth in care after the CCR had a 38% lower likelihood of being placed in congregate care, and fewer congregate care placements, on average. However, the cumulative time spent in congregate care remained stable, and youth were 80% more likely to be placed in congregate care outside of their supervising county after the CCR. Altogether, this study provides critical evidence to inform state and federal efforts to minimize the use of congregate care (Keefe et al., 2024).
Because the CCR encompassed multiple large-scale reforms to child welfare and behavioral health systems, findings should be interpreted in the context of this complex, multifaceted implementation effort. Consistent with the CCR’s goals, youth were less likely to be placed in congregate care after its implementation. Whether this is due to a decreased need for congregate care is less clear. More than half of California’s congregate care facilities closed in the wake of the CCR (California Department of Social Services, 2019, 2024a). Granted, some of these closures are to be expected given California’s declining foster care population (Webster et al., 2025). However, the limited number of these facilities after the CCR has likely made it more difficult to place youth in congregate care when clinically indicated.
Where youth were placed instead of STRTPs remains a topic for future research. Widespread FFA closures strained California’s supply of family-based alternatives to congregate care (California Alliance, 2024), as indicated by a six percentage-point decrease in the proportion of adolescents placed in FFAs since 2015 (Webster et al., 2025). Additionally, data from California’s Department of Health Care Services show that foster youth’s access to specialty mental health services—which constitute most Medicaid-funded behavioral health services for youth in care—has remained stagnant or declined since the CCR’s implementation (California Children’s Trust, 2021; Department of Health Care Services, 2022). As was the case in Illinois, agencies may have had limited placement options for adolescents with acute behavioral health needs (Budde et al., 2004).
Therefore, the increased risk of out-of-county congregate care placements after the CCR is likely explained by the simultaneous contraction of California’s congregate care facilities and treatment-oriented family-like placements. Youth from rural or less populous counties, which make up many of the 21 counties without STRTPs, faced a 230-592% higher risk of out-of-county placement (California Community Care Licensing Division, 2025). Out-of-county placements increased the time spent in congregate care by nearly 2.5 months and the number of congregate care placements. Since half of all post-CCR congregate care placements were outside youths’ supervising counties, these findings suggest that youth, especially those from rural or small counties, are at risk of spending longer periods in facilities farther from their communities.
Despite fewer such placements overall, the average length of congregate care stays held steady after the CCR. This pattern may reflect compositional changes in the population placed in STRTPs. Consistent with the CCR’s intent, lower-acuity youth may be stepping down to less restrictive settings more quickly, while higher-acuity youth make up a larger share of those remaining in STRTPs. These youth likely need more time to stabilize, producing offsetting effects that keep the average length of stay constant. Indeed, we found evidence of rising acuity in this population: rates of mental health concerns among youth in congregate care nearly doubled following the CCR (31% vs. 59%). Given that behavioral acuity often increases placement instability (Konijn et al., 2019), the modest decrease in congregate care placements after the CCR may reflect the promise of emerging STRTPs. However, this interpretation should be treated cautiously. CPS records underreport behavioral health concerns (Palmer et al., 2024), making it difficult to accurately estimate changes in acuity. Improved documentation may also account for the increased prevalence of mental health concerns over time. Future research using more reliable sources of mental health data is needed to corroborate this interpretation.
Sensitivity analyses corroborated the main findings, although there were some differences in the characteristics of youth placed in each facility type. Youth placed only in group homes after the CCR showed lower acuity than their peers placed in STRTPs or both facility types. Youth placed only in group homes spent less time in congregate care, had fewer congregate care placements, and were less likely to have an out-of-county placement than youth placed in STRTPs or in both facility types. Furthermore, youth placed only in group homes after the CCR had the lowest rates of mental health concerns (43% vs. 60-61%) and probation supervision (4% vs. 15–25%). Even so, this group spent nearly nine months in group homes, on average, which raises concerns about the developmental consequences of extended stays in group homes that are not equipped to provide therapeutic services. More research is needed to understand why these youth could not be placed in family-like settings (e.g., the absence of therapeutic foster homes), and whether this pattern persists as CCR implementation continues.
Limitations
This study is not without limitations. Administrative data are subject to data entry errors and variation among counties. Administrative CPS records underreport behavioral health diagnoses, especially among youth placed in congregate care (Palmer et al., 2024). The actual prevalence of behavioral health disorders is likely higher than that reported here. Future research should use more reliable data sources (e.g., Medicaid claims records). The observation period in the current study encompasses the COVID-19 pandemic, which may have influenced placement practices and data documentation (e.g, staffing shortages, telework). Placements in out-of-state residential treatment facilities were banned effective July 1, 2022, which may have shaped the observed outcomes (Chapter 86, Statutes of 2021). Additionally, California has a decentralized, county-administered child welfare system. Findings may not generalize to jurisdictions with different administrative contexts.
Findings should be considered preliminary. California continues to expand its continuum of behavioral health services, and future research is needed as child welfare practice further aligns with the CCR’s initial intent (California Department of Social Services, 2024b; Youth Law Center, 2022). Despite its pre-post design, the current study design does not facilitate causal inference. California began reducing its congregate care utilization before the CCR was enacted (Webster et al., 2025), suggesting that agencies may have prioritized family-like placements before the CCR. Moreover, the conversion of group homes to STRTPs took longer than anticipated. While the lengthy observation window reflects the implementation of the CCR, other policies and initiatives implemented during this period may also have shaped findings.
Implications for Practice, Policy, and Research
The current study highlights the vexing challenges and unexpected outcomes of policies striving to balance the behavioral health and developmental needs of adolescents in foster care (Budde et al., 2004; Pecora et al., 2009). As in Illinois, findings suggest California may have prematurely condensed and specialized its congregate care facilities before integrating behavioral health services into family-like placements. Without family-based alternatives to address their behavioral health needs, youth in congregate care were placed farther from their communities. This practice can be harmful to youth who, from a developmental standpoint, may face difficulties in social and relational growth (Berzin et al., 2014; Dozier et al., 2025; Lionetti et al., 2015; Massinga & Pecora, 2004). Youth from rural and smaller counties may be especially vulnerable. However, there can be benefits to out-of-county placements, such as helping youth receive specialized treatment, moving them closer to supportive adults, or removing them from geographically bound risks (e.g., gang involvement; human trafficking). More research is needed to examine potential heterogeneity in outcomes for youth in out-of-county congregate care.
Study findings may give some policymakers pause. This study adds to previous evidence emphasizing the importance of a strong network of therapeutic, family-like placements and behavioral health supports before reducing congregate care capacity (Alpert & Meezan, 2012; Budde et al., 2004; Keefe et al., 2024; Metcalf et al., 2022). Policymakers might hesitate to back similar reforms due to concerns over unintended consequences and the costs of scaling therapeutic foster care. However, the present study is not a comprehensive evaluation of the CCR. It does not examine where youth went instead of congregate care or how they fared in other placements. Given the developmental advantages of family-like care (Bakermans-Kranenburg & Van IJzendoorn, 2024), youth may have experienced unmeasured developmental benefits after the CCR. In short, more research is needed to understand the CCR’s impact.
Still, these results provide direction for policymakers looking to enhance the child welfare system’s capacity to support adolescents’ developmental and psychological well-being. Additional state and federal resources are needed to improve coordination between child welfare and behavioral health agencies, build provider networks, and implement therapeutic foster care models at scale, particularly in rural and smaller counties (Alpert & Meezan, 2012; Keefe et al., 2024). In California, new initiatives such as the Children’s Crisis Continuum Pilot Program, CalAIM, and the Tiered Rate Structure expand on the CCR to improve collaboration between child welfare and behavioral health systems, and increase youths’ access to extracurricular activities that promote positive development (California Department of Social Services, 2024b; California Assembly Bill 153, 2021; Youth Law Center, 2022).
Much remains to be learned about the effects of the CCR and congregate care more broadly. Studies of modern residential treatment facilities are needed to update our understanding of the consequences—and potential benefits—of congregate care (Dozier et al., 2025; van IJzendoorn et al., 2020). There is a particular need for research on residential treatment models that facilitate social learning and other developmentally enriching experiences. We also understand little about the systemic factors driving elevated rates of congregate care placements among Black, American Indian, and LGBTQ + youth (Covington et al., 2023; McCormick et al., 2017). Consistent with prior research, results showed that Black and Multiracial youth faced a higher risk of congregate care placement (Covington et al., 2023; Palmer et al., 2020). Recently, a U.S. Senate report ignited concerns for the safety and well-being of LGBTQ + youth placed in residential settings (U.S. Senate Finance Committee Minority Staff, 2025). Qualitative methods that uplift youth and practitioner voices may identify barriers to family-based care. Finally, future studies should examine the downstream effects associated with congregate care reforms. For instance, there is some evidence to suggest that decreasing congregate care capacity without providing suitable alternatives can increase the risk of youth homelessness (Keefe et al., 2024). Understanding where youth go in lieu of congregate care will be a critical component of evaluating the effectiveness of the CCR and similar reforms.
Conclusion
The current study leverages population-level data to show how the CCR has shaped congregate care outcomes in California since its enactment into law ten years ago. Results are mixed and highlight service gaps introduced by the still-ongoing implementation of the CCR. Even so, findings underscore the need for policy solutions that can build a child welfare system that is more conducive to supporting the social and relational learning of youth with complex behavioral health needs. Increasing behavioral health service offerings and aligning behavioral health and child welfare systems will likely be the first necessary steps in realizing the CCR’s intended potential. As the nation similarly reduces its reliance on congregate care, results suggest that investing in therapeutic foster care before consolidating and specializing congregate care may yield a more efficient transition to a developmentally informed child welfare system.
Supplemental Material
Supplemental Material - Congregate Care Outcomes After the Continuum of Care Reform
Supplemental Material for Congregate Care Outcomes After the Continuum of Care Reform by Anthony Gómez in Child Maltreatment
Footnotes
Acknowledgements
This research would not have been possible without the feedback and support of my dissertation committee: Dr. Jill Duerr Berrick, Dr. Andrea Lane Eastman, Dr. Ronald Dahl, and Dr. Kristina Lovato. I would also like to extend my gratitude to Dr. Mark Courtney, the California Child Welfare Indicators Project, and the extended network at the Transition-Age Youth Research & Evaluation Hub. Your thoughtful feedback and conversations played an essential role in the evolution of this study.
Ethical Considerations
Study procedures were approved by the Institutional Review Board at the University of California, Berkeley (Protocol ID: 2010-01-592) and the California Committee for the Protection of Human Subjects (Protocol ID: 12-10-0800).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Transition-Age Youth Research & Evaluation Hub (TAY-Hub) seeks to improve policies and practices affecting TAY by monitoring outcomes and through applied research that is grounded in engagement with members of the child welfare services community, including those with lived experience of foster care. The TAY-Hub is deeply grateful for the generosity of our funders: the Conrad N. Hilton Foundation, Walter S. Johnson Foundation, and California College Pathways Funders Alliance. This research was generously supported by the Grand Challenges for Social Work Doctoral Award and the California Policy Lab Graduate Fellowship.
Declaration of Conflicting Interests
The author has no conflicting interests to disclose.
Data Availability Statement
The data used in this study are not publicly available.
Disclaimer
This study was performed with the permission of the California Department of Social Services; however, the opinions and conclusions are solely those of the author and do not represent the policy or opinions of the collaborating agencies or any California department.
Supplemental Material
Supplemental material for this article is available online
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.