
Abstract
Recent research has shown that the child welfare system (CWS) often splits sibling groups, with at least one child removed to foster care and their siblings remaining at home. Yet, little is known about the nature and outcomes of this form of sibling separation. We use linked CWS and Medicaid data from Pennsylvania to address the following research questions: (1) What child, sibling and case characteristics predict split removal decisions? (2) Is having one or more siblings in foster care a risk factor for recurrent CWS involvement among children left at home? Multinomial regression and survival analyses are used to examine each, respectively. We find that child behavioral health issues are a common contributor to split removal decisions. Among children left at home, having siblings in foster care is associated with over three times the hazard of CWS reinvolvement within the first 100 days following the initial case-planning decision.
One in 20 U.S. children will experience foster care by age 18 (Wildeman & Emanuel, 2014). An unknown additional share of children, while not entering foster care themselves, will experience the removal of a sibling. When a family is reported to the child welfare system (CWS), the agency determines for each child whether foster care placement is necessary. Because foster care is an intervention of last resort, agencies may place some members of a sibling group in foster care and leave other siblings in parental custody. Despite broad recognition that sibling separation can be traumatic for children (Barnea et al., 2023), little is known about this form of sibling separation. A recent national study estimated that, among child maltreatment referrals leading to the removal of at least one child, 27.4% included one or more siblings who were not removed (Jones et al., 2025).
Such high rates of split removal decisions raise fundamental questions. Specifically, it is unclear how such a large share of homes deemed unsafe for at least one child remain safe for others. Neglect – the most common reason for foster care entry (U.S. Department of Health and Human Services, 2023) -- is often jointly experienced within sibling groups (Ahn et al., 2025). Are siblings left in the home under such conditions neglected relatively less than other siblings? Among instances of abuse, which can sometimes be targeted toward a specific child, are non-targeted siblings left in the home safe once the targeted sibling is removed? Knowledge of whether children left in the home experience repeated or new abuse and neglect is essential to ensure their wellbeing.
Critical to being able to ensure the wellbeing of children in split groups is to understand when groups get split. One potential explanation is the presence of variation in the needs of children in the group. Many children enter foster care for behavioral health concerns, or to access health services involves medically complex children (Gross et al., 2025). We may expect that when a sibling has behavioral health problems or complex medical needs, that they would likely be removed than their siblings who do not. Answering these questions provide CWS administrators increased knowledge on how and to assess the safety of children left in the home and how to facilitate sibling’s connectedness during their separation. However, these questions have not yet been explored in the literature.
This study uses linked CWS records and Medicaid claims from Pennsylvania. We address two research questions: (RQ1) Which child and case attributes predict the decision to split a sibling group upon foster care placement? (RQ2) Among children left at home following the index CWS referral, is having a sibling in foster care associated with subsequent CWS intervention, net of child and initial case characteristics?
Methods
Sample
The study population is Pennsylvania children with a substantiated child abuse investigation or a validated alternative response referral between January 1st, 2015 and September 30th, 2019, the observation window of the data. Alternative response in Pennsylvania includes all but the most severe allegations of neglect as well as child behavioral health concerns. Children were identified as siblings if they had the same biological mother as identified on the CWS referral. We then restricted the sample to children with at least one sibling on their referral (as a victim or non-victim) and then selected the first referral attached to each biological mother during the observation period. This initial subset yielded 138,243 children in 50,992 sibling groups.
The sample was further limited in order to measure medical complexity using the Pediatric Medical Complexity Algorithm (PMCA), which requires three years of Medicaid claims to make classifications. Children in the sample had to have been enrolled for the three years prior to the index referral. For children under three, they had to have been enrolled since birth. This restriction yielded a final sample size of 88,225 children in 41,824 sibling groups. As shown in Table A1 in the Appendix, this restriction did not substantially change the composition of the sample.
Measures
Split Status
A child-level (time-invariant) measure of split sibling status categorized children into one of four mutually exclusive categories related to the sibling group’s foster care entry within one year of the index referral. A child was labelled (1) intact-home if neither they or their siblings were placed in foster care, (2) all-placed if they and all of their siblings were placed, (3) split-home if their siblings were placed and they were either never placed or were placed on a later date, and (4) split-placed if they were placed and at least one of their siblings was either never placed or placed on a later date.
For the regression analysis under research question 2, split status was a time-varying measure. Children were censored from the analysis upon placement, such that all children in the model were either intact-home or split-home. Because the intact-home group included some children whose families received no formal monitoring or services following the CWS report (whereas families where at least one child was placed would be subject to ongoing court and CWS oversight), the intact-home group was divided based on whether a case was opened for services. The final measure of split status under research question 2 had three categories: intact-home without services, intact-home with services, and split-home.
CWS Allegation Type and Status
Four non-mutually exclusive variables measuring allegations on the index referral were created: physical abuse, sexual abuse, child behavioral problem, and neglect. At the child level, each variable was labelled with one of three mutually exclusive statuses: (1) allegation not present (neither the child nor their siblings had that allegation type); (2) child allegation (the child had that allegation type), or (3) sibling allegation only (the child did not have that allegation type but at least one of their siblings did).
Medical Complexity
The PMCA stratifies children into three categories: non-chronic, chronic non-complex, or complex chronic (Simon et al., 2014). The algorithm flags 19 different body systems and determines chronicity and complexity based on the number of body systems involved and the frequency of medical encounters. Among the flags are “mental health”. Given the prevalence of mental health disorders among children involved with CWS (Herd et al., 2023; Palmer et al., 2024) we further disaggregated the three categories based on the presence of a mental health condition or not, yielding six mutually exclusive groups: non-chronic without a mental health condition, non-chronic with a mental health condition, chronic non-complex without a mental health condition, chronic non-complex with a mental health condition, chronic complex without a mental health condition, and chronic complex with a mental health condition.
Subsequent CWS Intervention (RQ2)
Intervention following the index referral was measured using the occurrence of either a new CWS case or placement. We use a combined measure because, when a sibling is already placed or the family is open for services, a child may be placed in care (due to escalation or lack of resolution of index case factors) without initiating a new CWS case.
Controls
Child-level covariates were child age at index referral, race/ethnicity (non-Hispanic Black, Hispanic, non-Hispanic White, and other/unknown), and sex (male, female). At the sibling group level, indicators for the birth mother having a substance use disorder and a mental health disorder were coded based on Medicaid claims in the year prior to the index referral. Birth father risk factors were not available in the data. Covariates related to the index case are the number of children, year, and county.
Analytic Approach
We apply multinomial logistic regression to model the probability of each split status, with intact-home serving as the reference group.
We generated a person-day dataset, with the first day being the earliest of either the outcome date for the index referral or the date that the first child (self or sibling) was placed following the index referral. By measuring the first day with this criterion, as opposed to the referral date itself, we define the observation period as starting from the date when the case-planning team made its first decision. In-home services, if present, were assumed to be received as of the first day. Split status could only change from intact-home without services to split-home and intact-home with services to split-home. Children placed on the start date were thus excluded from the analysis. Children were censored after one year, upon turning 18, or at the end of the data observation window (October 1st, 2020).
Three models were fit. M1 included only the split-services variable (no controls). M2 added the allegation type, medical complexity, and other covariates. Based on visual inspection of smoothed hazard estimates, M3 added a time-dependent effect with the split-services coefficients moderated by whether at least 100 days had elapsed since the start of observation. 1
Results
Sample Description (N = 88,225 Children and 41,824 Sibling Groups). Column Percentages Are Given in Parentheses
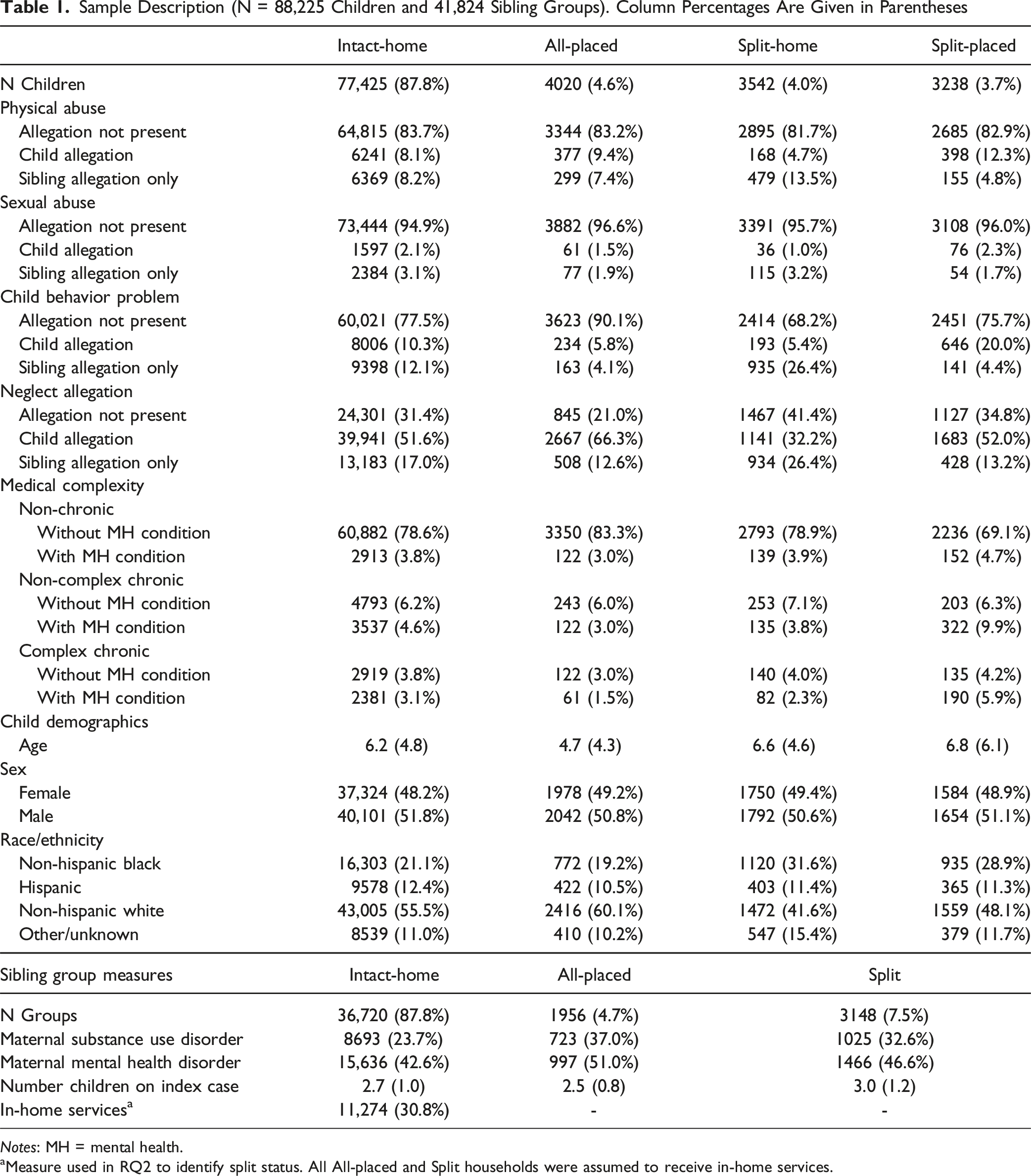
Notes: MH = mental health.
aMeasure used in RQ2 to identify split status. All All-placed and Split households were assumed to receive in-home services.
Compared to intact-home, all-placed, and split-home children, split-placed children had the highest rates of mental health conditions, regardless of the level of medical complexity (non-chronic, non-complex chronic, or complex-chronic). For example, 4.7% of split-placed children had non-chronic medical concerns with a mental health condition, compared to 3.0% of all-placed children and 3.9% of split-home children. Similarly, 9.9% of split-placed children had non-complex chronic medical concerns including a mental health condition, compared with 3.0% of all-placed children and 3.8% of split-home children.
Figure 1 illustrates the predicted probabilities from a multinomial logistic regression for allegation types and medical complexity, holding all other variables at their means. For each allegation type, the probabilities for the base category (allegation not present) are not shown. Among both child behavior problem and neglect allegation types, a child with a sibling allegation only label had higher probabilities of being split-home than being all-placed or split-placed. For example, among children with a sibling allegation only label for a child behavioral problem, the predicted probability of being a split-home child was 0.057, compared with 0.019 for all-placed and 0.011 split-placed. Among physical and sexual abuse allegation types, children with sibling allegation only labels had higher probabilities of being all-placed than split-home or split-placed. The probability of being split-placed was particularly high among children with child allegation labels for a child behavioral problem. Under this condition, the predicted probability of being split-placed was 0.059, vs 0.04 and 0.011 for all-placed and split-home, respectively. Multinomial probabilities of split status (omitted reference group: intact-home). Allegation not present statuses omitted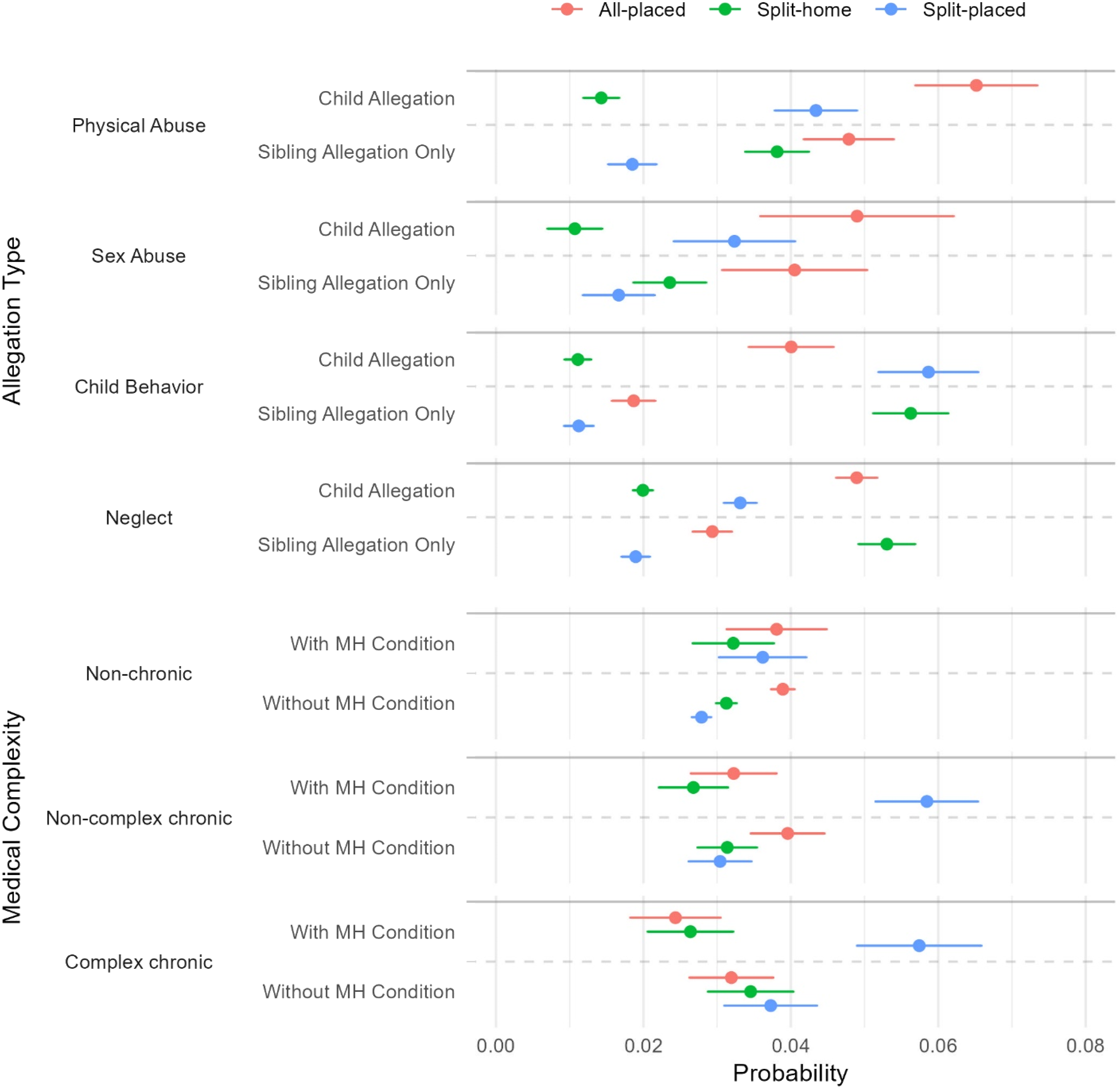
Medical complexity only significantly differentiated the probability of split status when a mental health condition was present among non-complex chronic and complex chronic categorizations. Among these two scenarios, the probabilities of being split-placed were nearly identical (0.059 for non-complex chronic and 0.058 for complex chronic). Both probabilities were approximately double the magnitude of being all-placed or split-home.
Hazard Ratios Predicting Subsequent CWS Intervention Among intact-home and split-home Children (N = 84,381 Children, 17,965 Experienced Subsequent CW Intervention)
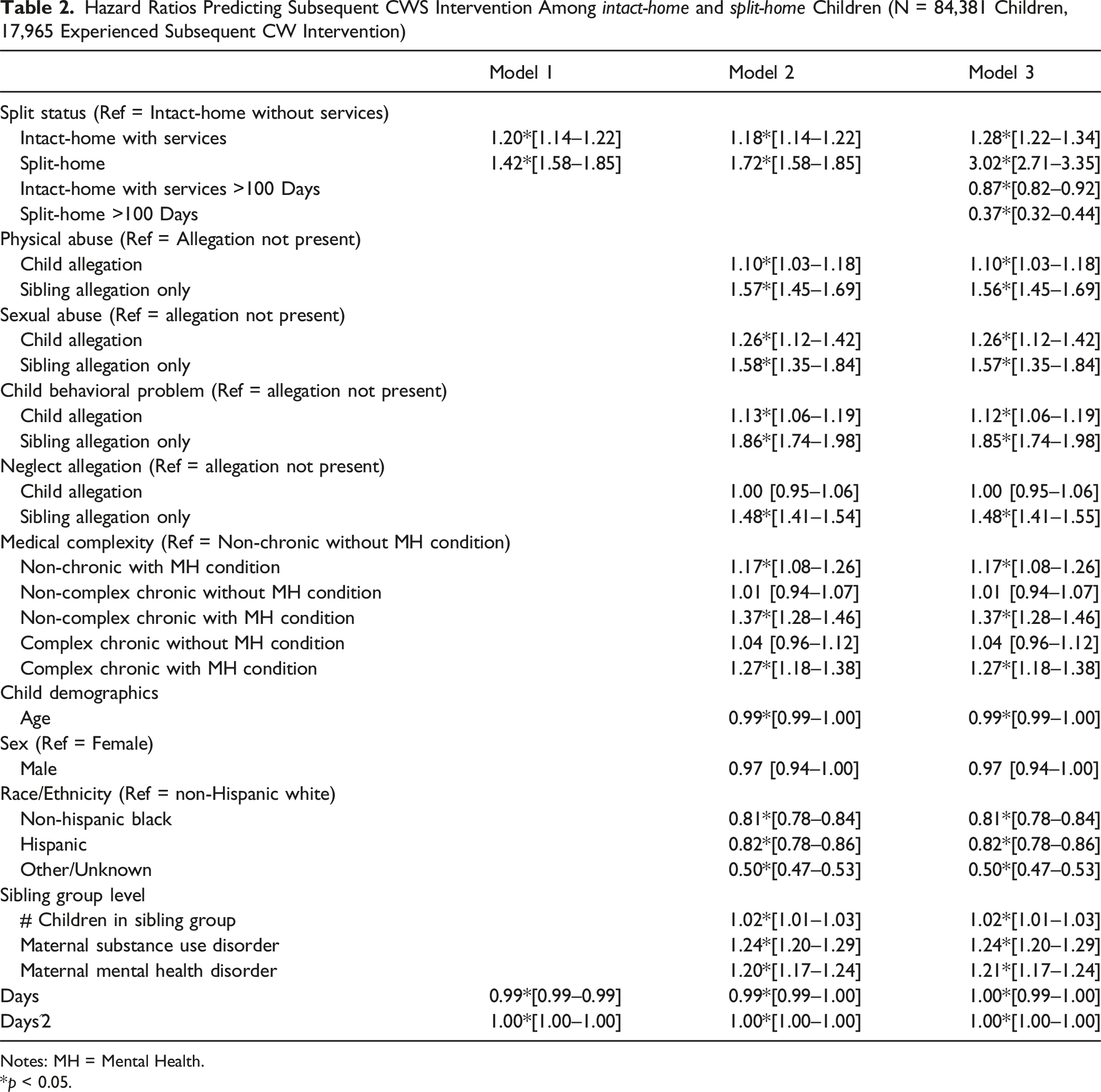
Notes: MH = Mental Health.
*p < 0.05.
Limitations
The study has some important limitations. First, we cannot determine whether all non-removed children remain at home: some may be informally placed with relatives (e.g., kinship diversion) and others may go to live with their other parent (e.g., a nonresident father), neither of which would be identified in our records. Second, we cannot ascertain whether CWS caseworkers sought removal of all children – in other words, it is unclear whether the decision to split the sibling group was made by the CWS agency or by the dependency court.
Discussion
This study used linked administrative CWS and Medicaid data in Pennsylvania to examine the prevalence and conditions of split sibling groups and the safety of children left at home when a sibling is removed. We find that, among sibling groups where at least one child is placed, most groups were split. Jones et al. (2025) estimated that 27% of sibling groups where at least one child was placed were split nationwide; however, their estimate was lower-bound because only ten states included data on siblings who did not have any allegations on the report. Pennsylvania is not an outlier among states where non-victim information is available. Formal policies may not adequately address visitation and continued connection of separated siblings when only some siblings are in state custody. Federal law requires reasonable efforts related to sibling visitation for children in foster care, but this does not explicitly apply to siblings left at home. Of course, visitation with children not in care can only occur with the consent of the legal parent or guardian (the state cannot make decisions for children not in its custody), but policies can impose requirements on agencies to pursue visitation in these circumstances. Minnesota’s Foster Care Sibling Bill of Rights (2025) provides one such model (2025).
Both CWS allegation types and medical complexity appear to influence split decisions. Relative to being an all-placed or split-home child, the probability of being a split-placed child is highest when the child has a behavior problem allegation. As we show in Tables A2 and A3 in the Appendix, children with both a behavioral problem allegation and a chronic mental health condition have nearly twice the probability of being split-placed compared to those with only one of these factors. For children removed in these circumstances, there is limited information as to why the behavioral health needs could not be addressed without state custody. It is possible that expanded funding under the Family First Prevention Services Act (FFPSA) for behavioral health services can be leveraged to prevent behavior-related foster care entries, but these funds are not yet widely used.
Lastly, we find that during the first 100 days following the initial CWS decision point, children who remain at home when a sibling is removed face more than three times the hazard of subsequent CWS intervention. This finding of a heightened and time-varying risk experienced by split-home children is consistent with Jones et al. (2025). CWS agencies should exercise tremendous caution when retaining children in a home where maltreatment was severe enough to warrant removal of a sibling and ensure that these children receive heightened levels of services and safety monitoring than is typically provided to non-removed children. One mechanism of doing so is by utilizing title IV-E prevention funds available as part of the Family First Prevention Services Act. Some states, including California, Connecticut and Kentucky, have already adopted this strategy (Children’s Bureau, 2024).
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded with help from the National Institute of Child Health and Human Development R01 HD095946 and P50HD089922.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclaimer
Data for this project was provided by the Pennsylvania Department of Human Services, Juvenile Court Judges Commission and Office of Medical Assistance Programs, but these entities do not certify the accuracy of results or endorse any positions taken by the authors.
Note
Appendix
Description of Sample Before Medicaid Enrollment Restriction Note. Maternal substance and mental health are omitted, along with the PMCA measures, as maternal enrollment in Medicaid was assumed to co-occur along with the child’s enrollment.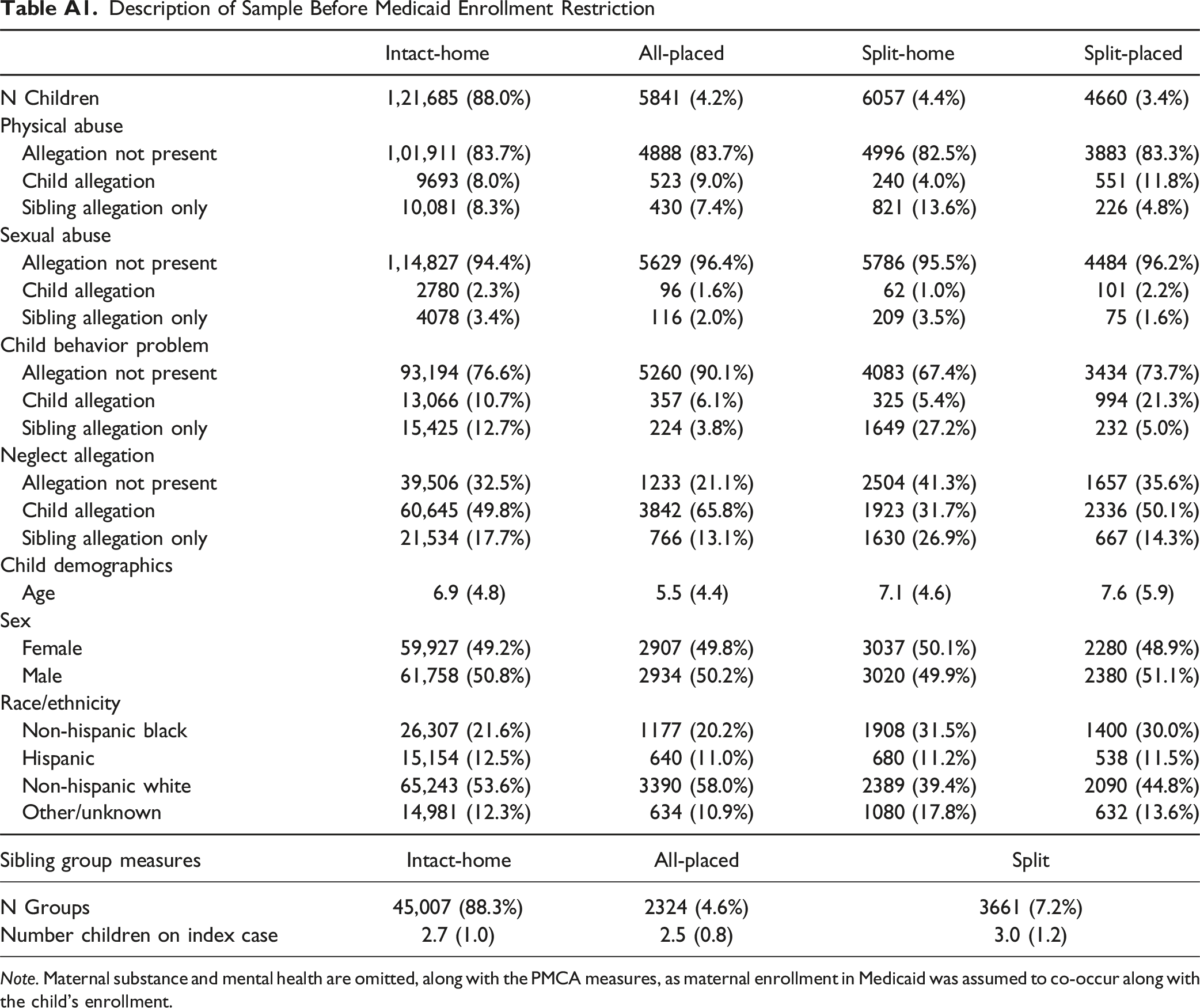
Intact-home
All-placed
Split-home
Split-placed
N Children
1,21,685 (88.0%)
5841 (4.2%)
6057 (4.4%)
4660 (3.4%)
Physical abuse
Allegation not present
1,01,911 (83.7%)
4888 (83.7%)
4996 (82.5%)
3883 (83.3%)
Child allegation
9693 (8.0%)
523 (9.0%)
240 (4.0%)
551 (11.8%)
Sibling allegation only
10,081 (8.3%)
430 (7.4%)
821 (13.6%)
226 (4.8%)
Sexual abuse
Allegation not present
1,14,827 (94.4%)
5629 (96.4%)
5786 (95.5%)
4484 (96.2%)
Child allegation
2780 (2.3%)
96 (1.6%)
62 (1.0%)
101 (2.2%)
Sibling allegation only
4078 (3.4%)
116 (2.0%)
209 (3.5%)
75 (1.6%)
Child behavior problem
Allegation not present
93,194 (76.6%)
5260 (90.1%)
4083 (67.4%)
3434 (73.7%)
Child allegation
13,066 (10.7%)
357 (6.1%)
325 (5.4%)
994 (21.3%)
Sibling allegation only
15,425 (12.7%)
224 (3.8%)
1649 (27.2%)
232 (5.0%)
Neglect allegation
Allegation not present
39,506 (32.5%)
1233 (21.1%)
2504 (41.3%)
1657 (35.6%)
Child allegation
60,645 (49.8%)
3842 (65.8%)
1923 (31.7%)
2336 (50.1%)
Sibling allegation only
21,534 (17.7%)
766 (13.1%)
1630 (26.9%)
667 (14.3%)
Child demographics
Age
6.9 (4.8)
5.5 (4.4)
7.1 (4.6)
7.6 (5.9)
Sex
Female
59,927 (49.2%)
2907 (49.8%)
3037 (50.1%)
2280 (48.9%)
Male
61,758 (50.8%)
2934 (50.2%)
3020 (49.9%)
2380 (51.1%)
Race/ethnicity
Non-hispanic black
26,307 (21.6%)
1177 (20.2%)
1908 (31.5%)
1400 (30.0%)
Hispanic
15,154 (12.5%)
640 (11.0%)
680 (11.2%)
538 (11.5%)
Non-hispanic white
65,243 (53.6%)
3390 (58.0%)
2389 (39.4%)
2090 (44.8%)
Other/unknown
14,981 (12.3%)
634 (10.9%)
1080 (17.8%)
632 (13.6%)
Sibling group measures
Intact-home
All-placed
Split
N Groups
45,007 (88.3%)
2324 (4.6%)
3661 (7.2%)
Number children on index case
2.7 (1.0)
2.5 (0.8)
3.0 (1.2)
Crosstabulation of Child Behavioral Problem Allegation Type and Medical Complexity Note. MH=mental health condition.
Non-chronic No MH
Non-chronic with MH
Non-complex chronic No MH
Non-complex chronic with MH
Complex chronic no MH
Complex chronic with MH
No allegation
55,437 (80.9)
2119 (3.1)
4243 (6.2)
2373 (3.5)
2623 (3.8)
1714 (2.5)
Child allegation
5383 (59.3)
793 (8.7)
545 (6.0)
1334 (14.7)
291 (3.2)
733 (8.1)
Sibling
8441 (79.4)
414 (3.9)
704 (6.6)
409 (3.8)
402 (3.8)
267 (2.5)
Percentages of Children Split-Placed, by Child Behavioral Problem Allegation Type and Medical Complexity
Non-chronic No MH
Non-chronic with MH
Non-complex chronic No MH
Non-complex chronic with MH
Complex chronic No MH
Complex chronic with MH
No allegation present
3.3
4.1
3.8
6.6
4.4
5.9
Child allegation
5.5
7.7
6.1
11.5
5.8
11.5
Sibling allegation only
1.3
1.2
1.1
3.2
0.5
1.9