
Abstract
The present study examined couples’ childhood maltreatment (CM) profiles and their associations with both partners’ sexual health over one year. Participants were 885 couples (Mage = 31.22) who completed measures of CM (baseline) and sexual satisfaction, distress and function (baseline, 6- and 12-months). Dyadic latent profile analyses yielded five profiles: Partner 1 Neglected, Low CM, Partner 2 Physically Abused, Partner 2 Sexually Abused, and Partner 1 Sexually Abused. Initial levels of sexual satisfaction, distress and function showed the greatest sexual health in Low CM and the worst in Partner 1 Neglected. Decreases in sexual satisfaction were steeper in Partner 1 Sexually Abused than Low CM; sexual distress decreased for Low CM and increased for Partner 1 Neglected and Partner 2 Sexually Abused; decreases in sexual function were steeper in Partner 1 Neglected and Partner 2 Sexually Abused than Low CM. Profiles involving greater CM are associated with worse sexual health.
Childhood maltreatment (CM) – an interpersonal trauma encompassing abuse and neglect (Briere, 2002; Gilbert et al., 2009) – is reported by 35% to 40% of individuals in North American epidemiological studies (Cyr et al., 2013; MacDonald et al., 2016). Although it is now well documented that CM is associated with a host of negative consequences, including depression, posttraumatic stress, substance abuse, and an overall increase in morbidity and mortality (Latham et al., 2021; Lewis et al., 2021; Miller et al., 2011), its associations with sexual health are still poorly understood. In fact, very little work has focused on CM’s impact on sexuality beyond at-risk behavior (e.g., unprotected sex) (Abajobir et al., 2018), despite the fact that current prevalence rates of sexual problems in the general population hover around 40% (McCabe et al., 2016) and that 58% of individuals in sex and couple therapy report at least four forms of CM (Bigras, Godbout, et al., 2017).
Cross-sectional work conducted among individuals suggests that experiences of CM are associated with lower sexual function and satisfaction (Bigras et al., 2015; Najman et al., 2005), whereas the only two prospective dyadic studies suggest that CM is associated with decreased sexual satisfaction over one year (Vaillancourt-Morel et al., 2019, 2021). However, most research focusing on interpersonal trauma and sexuality has examined the contribution of childhood sexual abuse (CSA) exclusively (Rellini & Meston, 2007) using a variable-centered approach (e.g., correlational studies) (Bigras et al., 2021), despite growing evidence that different forms of CM tend to co-occur (MacDonald et al., 2016) and that those with profiles characterized by multiple types of abuse and neglect (i.e., poly-victimization) have poorer psychosocial outcomes (Lewis et al., 2021). Further, the focus has been primarily on women’s sexuality (Pulverman et al., 2018; Rellini, 2008), neglecting men and individuals who are sexually and gender diverse (SGD). Importantly, most studies have ignored the relationship context in which sexuality is experienced, espousing an intra-individual rather than an interpersonal lens to capture the role of CM in adult sexual health (Bigras, Daspe, et al., 2017). This is a significant gap in knowledge, as both CM and sexuality are relational experiences, and trauma can be triggered in intimate, vulnerable interactions such as sexual activity with a romantic partner (Vaillancourt-Morel et al., 2016). Moreover, each partner brings their own childhood history to the relationship, which can interact with the other’s past experiences, potentially creating a sexual dynamic unique to their combined backgrounds. Thus, while intra-individual variable-centered correlational studies suggest that CM may be associated with adverse sexuality outcomes, little is known concerning (1) the extent to which couples’ profiles of CM prospectively relate to sexual health, and (2) which couples’ profiles may be the most detrimental over time. Using a person-centered dyadic approach, the present study’s aim was to investigate couples’ CM profiles and their associations with their sexual health trajectories over one year (i.e., sexual satisfaction, sexual distress, and sexual function).
Conceptual models of trauma and relationships highlight how CM may have longstanding impacts on sexuality (MacIntosh et al., 2020; Vaillancourt-Morel et al., 2016). Attachment theory proposes that when the child’s environment is not reliably available and supportive, as in neglecting or abusive families, they may form a model of self as shameful or flawed, and of others as unresponsive or abusive (Mikulincer & Shaver, 2016). These models could be re-evoked in intimate relationships, including in sexual interactions, which may lead to sexual difficulties (Briere, 2002; Finkelhor & Browne, 1985). Similarly, the Self-Trauma model suggests that the breach of trust involved in CM could impact the capacity to self-regulate in the emotionally evocative interactions inherent to sexual relationships and that unprocessed traumatic reactions could be triggered during partnered sexual activity, which in turn would hinder couples’ capacity to navigate sexual challenges and thrive in their sexual relationships (Rosen & Bergeron, 2019). Adopting a systemic perspective, the Couple Adaptation to Traumatic Stress model assumes that traumatic experiences will generate symptoms not only in the primary trauma survivor but also in their partner, in addition to potentially dysfunctional relational dynamics within the couple system (Goff & Smith, 2005).
Empirical work has yielded mixed findings. A first longitudinal study examined the associations between CM and trajectories of sexual frequency and satisfaction among 202 newlywed mixed-sex/gender couples over two years across three time points (DiLillo et al., 2009). Results showed that CM was not significantly related to mean levels or trajectories of sexual frequency or sexual satisfaction over time. However, the assessment of sexuality outcomes was limited to one-item unidimensional measures of satisfaction and frequency, and dyadic analyses accounting for the interdependence of partner data were missing. Another longitudinal study using more comprehensive validated measures focused on the associations between CM subtypes and sexual health among a community sample of 269 mixed gender/sex couples followed over one year across three time points (Vaillancourt-Morel et al., 2021). Greater levels of most of women’s CM experiences (i.e., childhood sexual, physical and psychological abuse, and psychological and physical neglect) were related to a sharper decrease in their sexual satisfaction (i.e., subjective evaluation of the positive and negative aspects of one’s sexual relationship) (Lawrance & Byers, 1995) over one year, and women’s history of CSA was associated with a steeper increase in their sexual distress (i.e., sexuality-related negative emotions) (Santos-Iglesias et al., 2018). Women’s greater emotional neglect was also related to their partners’ lower initial level of sexual satisfaction, and women’s greater emotional abuse and neglect were related to their partners’ lower initial level sexual function (i.e., sexual desire, arousal and orgasm) (Rosen et al., 2000). Unfortunately, this variable-centered study did not account for the common co-occurrence of CM experiences in individuals and couples, or profiles of CM. Nevertheless, findings underscore how one partner’s CM may contribute to the other partner’s poorer sexual health (Vaillancourt-Morel et al., 2024).
Adverse effects could be further compounded in cases where both have experienced CM, i.e., dual-trauma couples (Goff & Wampler, 2000). In a population-based sample of couples, one partner reporting childhood physical abuse increased the likelihood by 2.4 times that the other partner also reported the same trauma, suggesting that this phenomenon might be relatively common (Whisman, 2014). These dual-trauma couples could face additional challenges in co-regulating their sexuality and experience worse sexual health outcomes relative to no-trauma couples or to those where only one partner reports CM, although evidence of this phenomenon is scant, in part because dyadic profiles of CM have not been established (MacIntosh et al., 2020). While most research focused on the contribution of single forms of CM to sexuality (Bergeron et al., 2022), person-centered research on individuals reporting CM has yielded distinct profiles combining different forms of CM and predicting unique psychosocial outcomes, with most studies identifying three profiles: a no/low-trauma group, a predominantly CSA group, and a high-trauma, poly-victimized group, the latter being associated with worse psychological outcomes (Debowska et al., 2017). Identifying couples’ CM profiles and their associations with sexual health trajectories over time could provide much needed empirical support for current theoretical conceptualizations of trauma, intimate relationships and sexuality, and yield invaluable information to develop targeted, trauma-informed sex and couple therapy interventions.
Although previous research has found associations between some forms of CM and sexuality outcomes, most studies were characterized by intra-individual rather than dyadic approaches, focused exclusively on CSA – primarily in women, neglected to include sexually and gender/sex diverse couples, and adopted variable-centered cross-sectional designs. In the current study involving community couples from four combined longitudinal studies, we assessed both partners’ CM (physical, sexual and psychological abuse, as well as physical and psychological neglect) at baseline, and reports of their sexual health collected at three time points over one year. Using a person-centered, bifactor dyadic approach that allowed us to disentangle the overall CM burden from the unique contributions of specific CM types, we examined: (1) how different aspects of CM among couples combined into distinct dyadic trauma profiles; and (2) the associations between the obtained couple profiles and both partners’ initial levels and trajectories of three indicators of sexual health (i.e., sexual satisfaction, distress, and function) over one year. Based on past latent profile analyses of CM in individuals, we hypothesized that at least three distinct dyadic trauma profiles would be identified, with the largest one characterized by low levels of all types of CM in both partners, a second where sexual abuse predominated in one or both partners, and a third with high levels of multiple forms of CM in both partners (Debowska et al., 2017). We hypothesized that couples in which both partners reported lower levels of cumulative CM and of specific types of CM (e.g., CSA, beyond what is captured by cumulative CM) would show higher initial sexual health and little or no decline over time. In contrast, we expected that couples with moderate to high levels of cumulative CM and of specific types of CM, particularly CSA, would show lower initial levels of sexual satisfaction and function with greater declines over time along with higher initial sexual distress and a greater increase over time. In an exploratory manner, we compared the profiles along socio-demographic characteristics including pregnancy status, age, relationship duration, gender, and sexual orientation, as existing work suggests that these are associated with sexual health (Schmiedeberg & Schroder, 2016) and that women and sexual/gender diverse individuals report greater CM relative to cisgender men (Diamond & Alley, 2022).
Method
Participants and Procedure
This study included four distinct longitudinal samples of community couples of different sexual orientations and genders/sexes, involving three time points each: baseline (Time 1), 6-month (Time (2) and 12-month (Time (3) data collections. All couples were recruited via online advertisements (e.g., social media, classified advertisement web sites), email lists, and posters or flyers distributed in various locations in Canada and the US. Advertisements informed participants about an online study on how sex and relationship intimacy contribute to the well-being of couples. All interested participants were contacted by a research assistant for a brief telephone eligibility interview. Eligible couples independently accessed a unique hyperlink to complete a consent form and self-report questionnaires hosted on Qualtrics. Three attention-testing questions were included in the Time 1 survey, and participants failing two out of three of these were excluded from the study. Couples for Samples 1, 2 and 4 could be located anywhere in Canada and the US. Couples for Sample 3 had to live in City 1 or City 2 in Canada given there was an in-person component to the data collection (not included in the present study). Couples for Sample 1 were recruited in 2016, and for Sample 2, between March 2017 and June 2018. Couples for Sample 3 were recruited in City 1 and City 2, Canada, between May 2019 and January 2020. Couples for Sample 4 were recruited between January and November 2020. Each of the four initial studies was approved by the institutional review boards of participating universities. This study’s design, hypotheses and analytic plan were preregistered after data had been collected but before analyses were undertaken: https://osf.io/hnfqv/?view_only=b8bc174ff5104327ae96db2d9880a21c.
In all studies, both partners had to be at least 18 years of age. Across the four samples, both partners had to have been together for at least six months (Sample (1) or 12 months (Sample (2) or living together for 12 months (Samples 3 and (4) and to have been sexually active at least once a month over the past three months (Samples 2 and (4) or in their lifetime (Sample 3). Couples were excluded if one partner was pregnant, breastfeeding, or if the couple had a child of less than one year at Time 1, given changes in sexuality during pregnancy and postpartum (Samples 1, 2 and 3). Couples were not eligible if one partner self-reported a severe mental or physical illness or took prescribed medications that affected their sexuality (Samples 2 and (3) or was currently being treated for sexual problems or considering starting such treatment during the study (Sample 3). Figure S1 shows the flow of participating couples throughout the four studies. The final sample size was 885 couples.
Measures
Childhood Maltreatment
CM was measured at Time 1 (baseline) for each sample using the 25-item short form of the Childhood Trauma Questionnaire (CTQ; Bernstein et al., 2003). This measure retrospectively assesses the extent of five types of CM with five items for each type: physical, emotional, and sexual abuse as well as physical and emotional neglect over the entire “growing up” period, without reference to specific ages (Bernstein et al., 2003). Participants were instructed to think about these experiences in their own family and rated each item on a five-point scale ranging from never true (1) to very often true (5). Scores were summed to obtain a total score ranging from 5 to 25 for each five-item subscale, with higher scores indicating higher frequency of this type of CM. The CTQ has good internal consistency (Cronbach’s α = .81 to .95), measurement invariance across four samples including a community sample, good temporal stability over a 2- to 6-month interval (r = .79 to .95), and good convergent validity with a structured interview (Bernstein et al., 2003).
Sexual Satisfaction
At each time point, the Global Measure of Sexual Satisfaction (GMSEX; Lawrance et al., 2011) was used to evaluate participants’ subjective global satisfaction with their sexual relationship with their partner. It includes five items rated on seven-point bipolar scales: good-bad, pleasant-unpleasant, positive-negative, satisfying-unsatisfying, and valuable-worthless. Items were summed to provide a total score (5 to 35), where higher scores reflect greater sexual satisfaction. This scale demonstrates good internal consistency (Cronbach’s α = .96), 3-month test-retest reliability (r = .78 to .84), and convergent validity with other sexual satisfaction measures (Lawrance & Byers, 1995).
Sexual Function
At each time point, women’s sexual function in the previous four weeks was measured with the Female Sexual Function Index (FSFI; Rosen et al., 2000), a 19-item scale that assesses sexual desire, arousal, lubrication, orgasm, satisfaction, and pain. Scores obtained in these sexual domains were summed and multiplied by a respective factor that homogenizes the influence of each dimension to form a total score ranging from 2 to 36, with a higher score indicating better sexual function. The FSFI has excellent internal reliability (Cronbach’s α = .97) and good 4-week test-retest reliability (r = .88; Rosen et al., 2000). Men’s sexual function in the past four weeks was measured with the International Index of Erectile Function (IIEF; Rosen et al., 1997), a 15-item scale that assesses sexual desire, erectile function, orgasm, intercourse satisfaction, and overall sexual satisfaction. Items were summed to provide a total score ranging from 5 to 75, with a higher score indicating better sexual function. The IIEF has good internal consistency (Cronbach’s α = .91 to .96), 4-week test-retest reliability (r = .82), and convergent validity with clinical interviews (Rosen et al., 1997). Participants reporting a gender-diverse identity were given the choice to complete the male or female anatomy version of the scale or to skip it completely.
Sexual Distress
At each time point, sex-related personal distress was measured with the Female Sexual Distress-Revised (FSD-R) which has been validated with men and gender-diverse individuals (DeRogatis et al., 2008; Santos-Iglesias et al., 2018). Participants rated 13 items that assess how often a sexual problem has bothered them or caused distress during the past 30 days (e.g., feeling sexually inadequate, bothered by low desire) on a five-point frequency scale (0 = never, 4 = always). Items were summed to obtain a total score ranging from 0 to 52 with higher scores indicating more sexual distress. The FSD-R demonstrates good internal consistency (Cronbach’s α = .88), good 28-day test-retest reliability (ICC = .88), and adequate convergent validity with sexual bother and concerns (DeRogatis et al., 2008; Santos-Iglesias et al., 2018).
Data Analysis Plan
Mplus 8 (Muthén & Muthén, 2021) was used to test our main hypotheses using the weighted least squares mean- and variance-adjusted estimator (WLSMV) or robust maximum likelihood (MLR) estimation methods depending on the distribution of the variables.
Preliminary Analyses
For CM, we relied on the bifactor exploratory structural equation modeling (bifactor-ESEM) framework (Morin et al., 2016, 2020) to compare alternative representations of CM: first-order CFA and ESEM, and bifactor CFA and ESEM solutions. In these models, partners’ latent factors were treated separately to capture CM for each person. Models were evaluated based on: (1) commonly used fit indices (Marsh et al., 2005): comparative fit index (CFI), Tucker-Lewis index (TLI), root mean square error of approximation (RMSEA); (2) the examination of parameter estimates (i.e., factor loadings, cross-loadings and factor correlations); and (3) the theoretical conformity of the models. We also calculated model-based omega (ω) composite reliability indices (McDonald, 1970) from the standardized parameter estimates. Factor scores (standardized units with M = 0 and SD = 1) were saved from the most optimal measurement model and used as input for the latent profile analyses (LPAs). These analyses are described and reported in the online supplementary materials and supported the bifactor CFA and ESEM solutions and the adequacy and composite reliability of all variables: global CM (ω = .984), physical abuse (ω = .829), emotional abuse (ω = .724), physical neglect (ω = .516), emotional neglect (ω = .882), sexual abuse (ω = .970).
Regarding the indicators of sexual health (sexual satisfaction, function, distress), we first examined the psychometric adequacy of their measures using CFA and their temporal stability using tests of measurement invariance (Millsap, 2011). These analyses are reported in the online supplementary materials and supported the adequacy, composite reliability, and longitudinal measurement invariance of all variables: sexual satisfaction (ω = .946 to .954) and sexual distress (ω = .957 to .967). For these outcomes, factor scores (estimated in standardized units with a mean of 0 and a variance of (1) were saved and used in the dyadic latent curve model. For sexual satisfaction and distress, the factor scores were used to estimate latent growth models, resulting in intercept (i.e., initial levels) and slope (i.e., changes) values which were used as outcomes of profile membership. As the IIEF includes 15 items and the FSFI includes 19 items, it was not possible to conduct CFA on these scales in the APIM framework with indistinguishable dyads. Hence, manifest scale scores on the FSFI were rescaled using the following formula ((score −(2) × (75/34)) to match scores on the IIEF (Corsini-Munt et al., 2017) to estimate latent growth models for sexual function.
Latent Profile Analysis (LPA)
The main analyses involved estimating latent profile analytic models using Mplus’ MLR estimator including one to 10 solutions with freely estimated profile indicator means. The CM factor scores (separated for each person within the couple) were used simultaneously as profile indicators. To account for the interdependence of the two partners, following the APIM guidelines with indistinguishable dyads (Kenny et al., 2006), matching profile indicators were allowed to correlate (Roberson et al., 2020). To avoid convergence on local maxima and to maximize the replicability of the best loglikelihood value, models were estimated using 10,000 random start values, 1000 iterations, and 500 final optimizations (Hipp & Bauer, 2006).
The selection of the optimal number of profiles was guided by the theoretical meaningfulness and statistical adequacy (e.g., the absence of negative variance estimates) of the extracted profiles (Marsh et al., 2009; Muthén, 2003). In terms of statistical indicators, we relied on a variety of information criteria and likelihood ratio tests: the Akaike Information Criterion (AIC), the Bayesian Information Criterion (BIC), the Constant AIC (CAIC), the Sample-Size-Adjusted BIC (SSABIC), the adjusted Lo-Mendell-Rubin (aLMR) likelihood ratio test, and the Bootstrap Likelihood Ratio Test (BLRT). Lower values on AIC, BIC, CAIC, and SSABIC suggest a better fitting solution, whereas non-significant p-value associated with aLMR and BLRT suggest the superiority of a model including one less profile. We also report the classification accuracy (i.e., entropy; ranging from 0 to 1 where the latter indicates perfect classification accuracy) for each LPA model (Lubke & Muthén, 2007). As all information criteria are heavily impacted by sample size and often keep on improving with the addition of profiles to the solution (Marsh et al., 2009), indicators should be graphically presented as “elbow plots” where the point after which the slope flattens suggests that the optimal number of profiles have been reached and that the contribution of additional profiles becomes negligible (Morin & Litalien, 2019).
Once the optimal solution was selected in each sample 1 , the profile membership of each participant was exported and the profiles were compared along a series of socio-demographic variables (pregnancy status, age for both partners separately, relationship duration combined for each couple, gender, and sexual orientation). When categorical variables were used, comparisons were made via chi-square (χ2) tests; in the case of continuous variables, comparisons were made using one-way analyses of variance (ANOVAs).
Dyadic Latent Curve Model (DLCM)
We then estimated dyadic latent curve models (Bollen & Curran, 2006; Kashy et al., 2008) to represent each partner’s distinct growth trajectories. As we included same- and mixed-gender/sex couples, dyads were treated as indistinguishable. Given the availability of three measurement waves, we tested and compared intercept-only, linear and multibase parameterizations to get estimates of an intercept factor (reflecting the average initial level of sexual health across all participants) and a slope factor (reflecting the average amount of change per time point across all participants). Upon selecting the most optimal DLCMs, the intercept and slope factors, separate for each partner, were saved as factor scores and used as profile outcomes. These person-specific outcome levels were directly integrated into the final LPA model and contrasted simultaneously across the profiles in a single step using the multivariate delta method and Mplus’ Model Constraint function (Raykov & Marcoulides, 2004). We were thus able to model each parameter (e.g., covariance) of the partners’ scores simultaneously.
Results
Profile Selection and Interpretation
Goodness-of-fit indices associated with the one to 10 profile solutions are reported in Table S9 and are graphically depicted in Figure S3 of the online supplements. The fit indices revealed a similar decreasing trend across all indicators: while the CAIC supported the 9-profile solution, the AIC, BIC, SSABIC, and the BLRT failed to reach a minimum value, while the aLMR supported the 3-profile solution. The examination of the elbow plot showed that this decrease in fit indices becomes more negligible around the 6-profile solution. On this basis, solutions including 4 to 7 profiles were more thoroughly inspected. This inspection revealed that all solutions were statistically proper, had moderate-to-high levels of classification accuracy (entropy values ranged from .793 to .802). Importantly, increasing the number of profiles results in the addition of theoretically meaningful, well-defined and interpretable profiles up to the 5-profile solution. Conversely, adding a sixth (or seventh) profile to the solution led to the identication of profiles that did not have theoretically meaningful associations with the outcomes (in the 6-profile solution) or were small in size (in the 7-profile solution). The 5-profile solution was thus retained for interpretation and further stages of the analyses – see Figure 1 and Table S8 for associated parameter estimates. Final 5-Profile Solution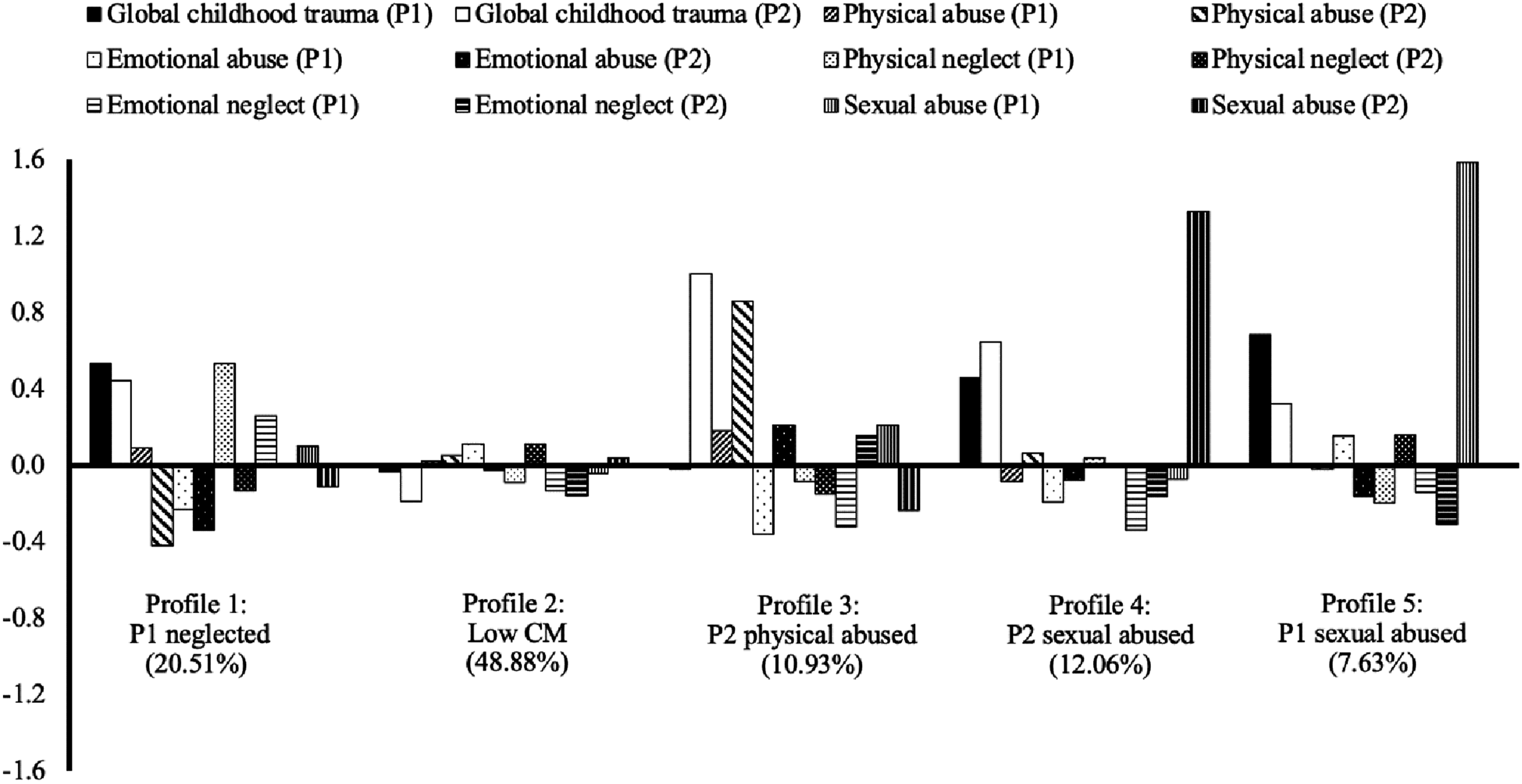
Visual Presentation of the Identified Profiles and Their Trauma-Based Characteristics
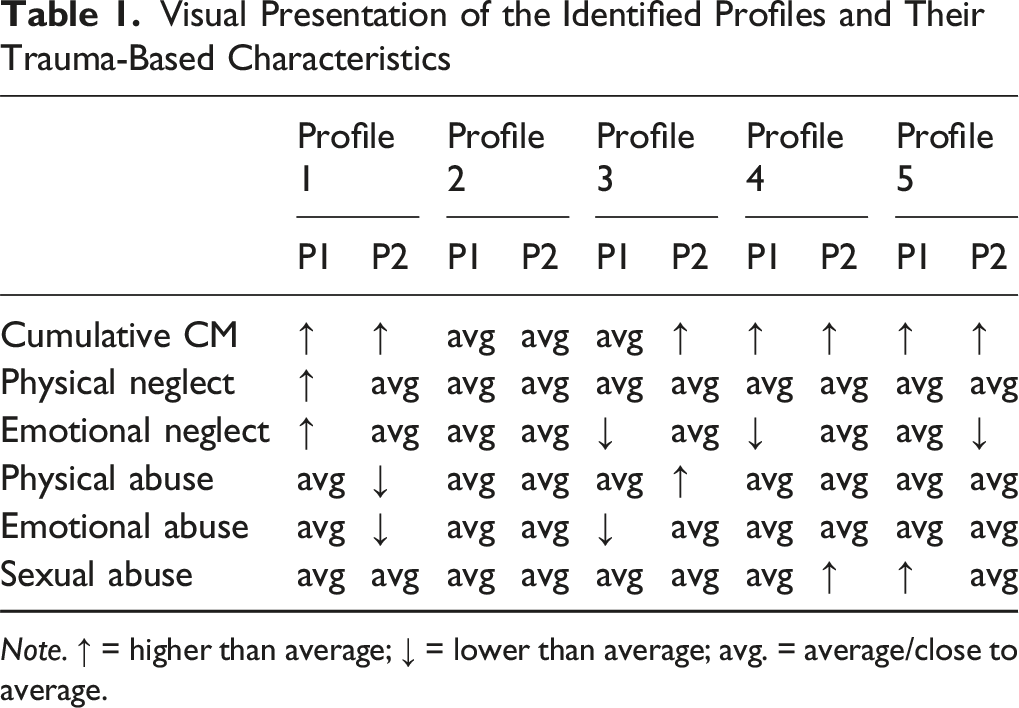
Note. ↑ = higher than average; ↓ = lower than average; avg. = average/close to average.
Demographic Comparison of the Final 5-Profile Solution
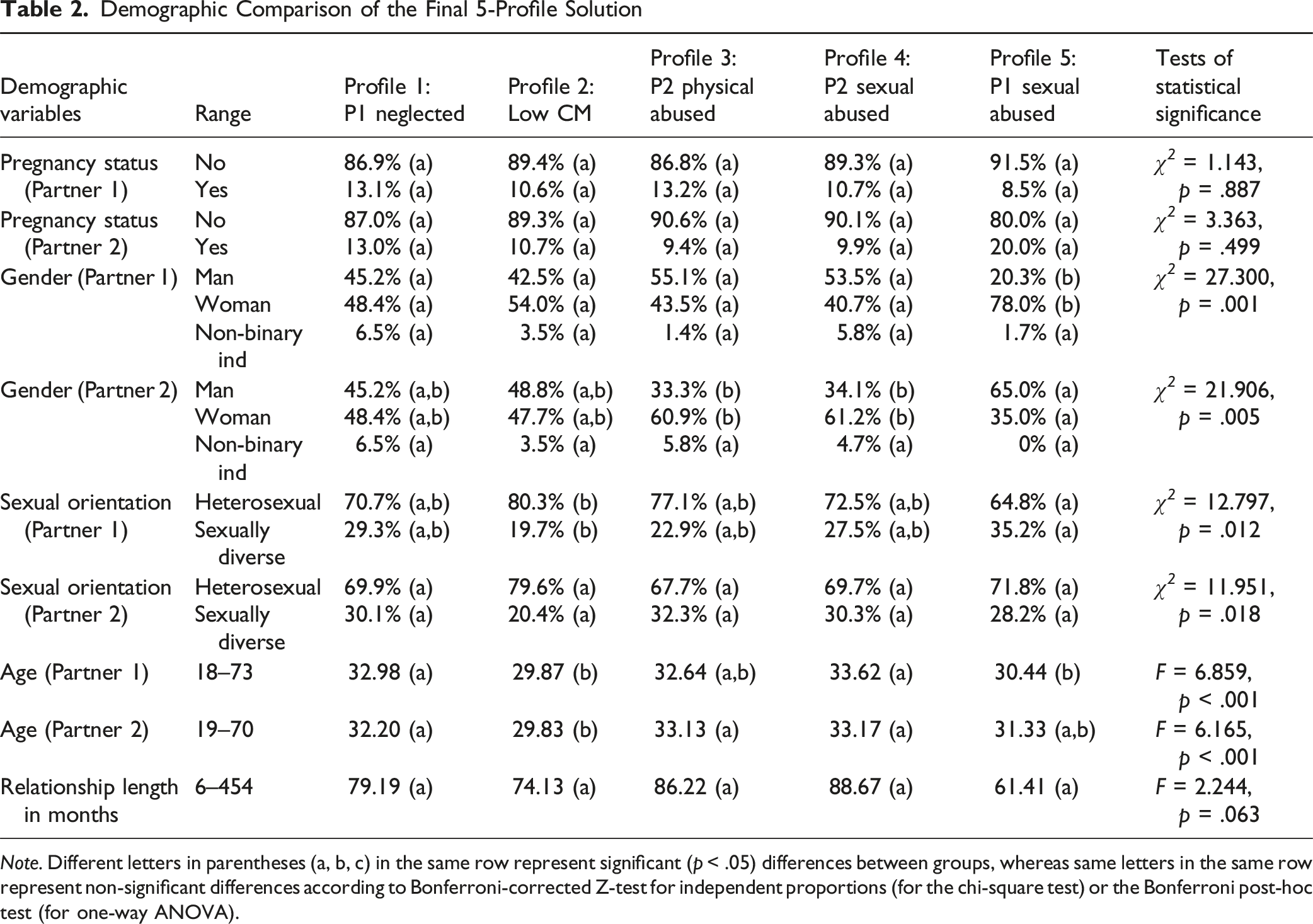
Note. Different letters in parentheses (a, b, c) in the same row represent significant (p < .05) differences between groups, whereas same letters in the same row represent non-significant differences according to Bonferroni-corrected Z-test for independent proportions (for the chi-square test) or the Bonferroni post-hoc test (for one-way ANOVA).
Outcomes of Profile Membership
Outcome Means and Pairwise Comparisons Between the Five Profiles
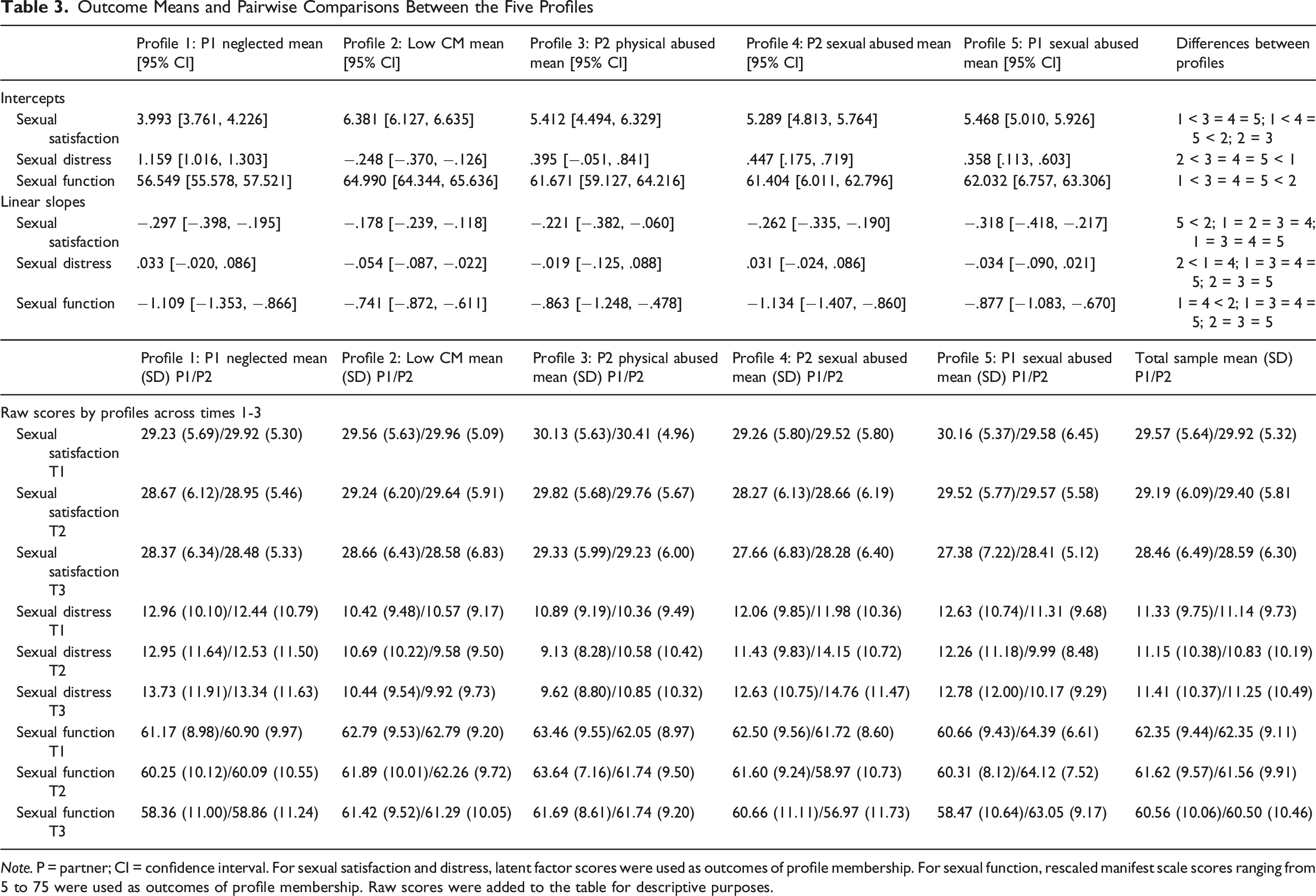
Note. P = partner; CI = confidence interval. For sexual satisfaction and distress, latent factor scores were used as outcomes of profile membership. For sexual function, rescaled manifest scale scores ranging from 5 to 75 were used as outcomes of profile membership. Raw scores were added to the table for descriptive purposes.
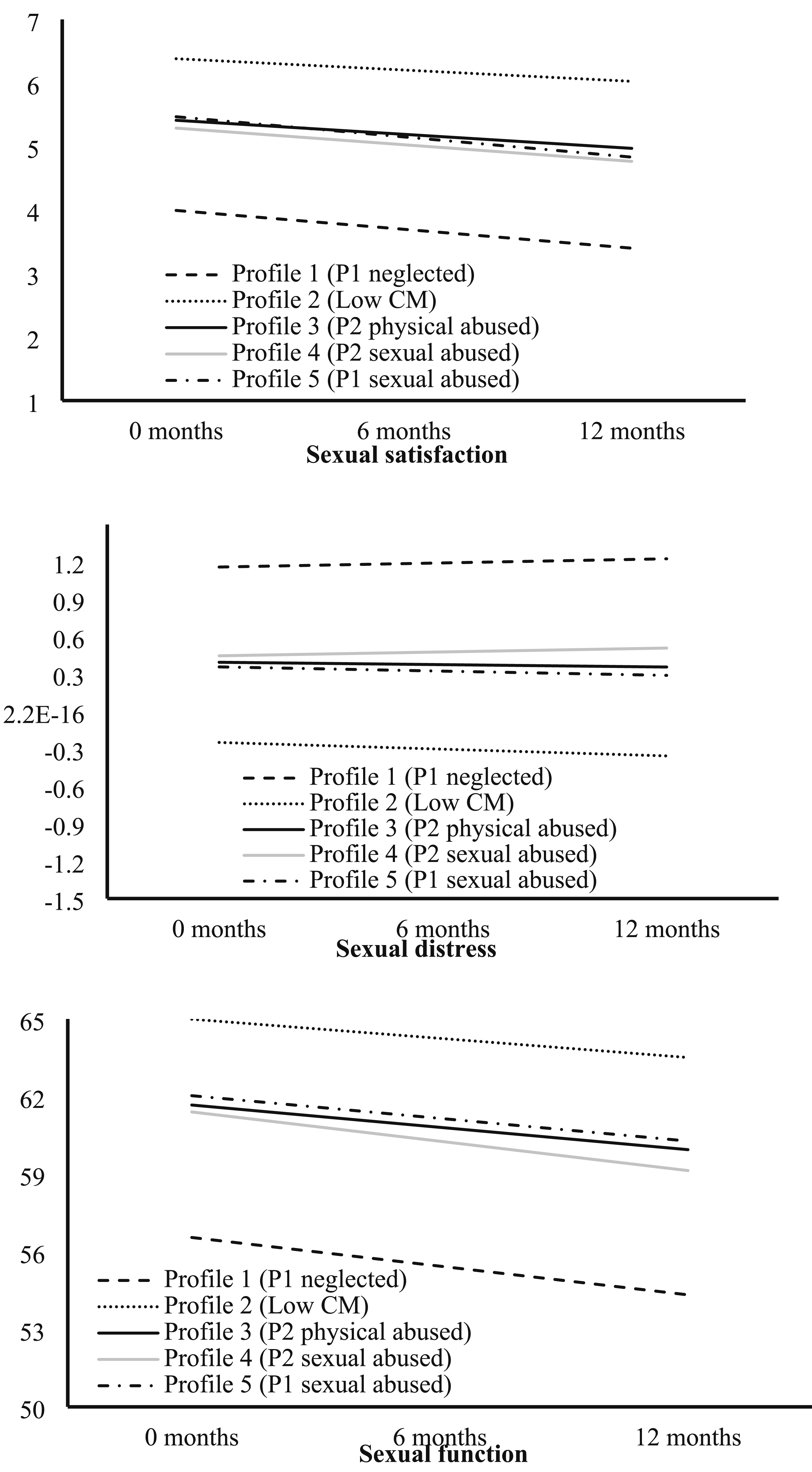
Profile-specific Trajectories for the Sexual Health Outcomes
Associations between profile membership and the outcome changes over time (i.e., slopes) were less numerous. Overall, sexual satisfaction and function showed decreasing trajectories for all profiles, whereas sexual distress showed stable, slightly increasing, or slightly decreasing trajectories. Three statistically significant differences emerged: first, decreases in sexual satisfaction were steeper in Profile 5, Partner 1 Sexually Abused than in Profile 2, Low CM; the other profiles were not distinguishable from one another. Second, changes in sexual distress differed between Profile 2, Low CM; 1, Partner 1 Neglected; and 4, Partner 2 Sexually Abused: while sexual distress decreased slightly for members of Profile 2, Low CM, it increased slightly for members of the other two profiles. The other comparisons were not statistically significant. Third, decreases in sexual function were less steep in Profile 2, Low CM, compared to Profiles 1, Partner 1 Neglected and 4, Partner 2 Sexually Abused.
Discussion
The present study’s aim was to examine couples’ CM profiles and their associations with both partners’ initial levels and trajectories of sexual health over one year. Dyadic latent profile analyses yielded five profiles: Profile 1, i.e., Partner 1 Neglected, Profile 2, i.e., Low CM, Profile 3, i.e., Partner 2 Physically Abused, Profile 4, i.e., Partner 2 Sexually Abused, and Profile 5, i.e., Partner 1 Sexually Abused. Initial levels of sexual satisfaction, sexual distress and sexual function formed a pattern showing the greatest sexual health in the Low CM profile and the worst sexual health in the Partner 1 Neglected profile. As for trajectories over 12 months, decreases in sexual satisfaction were steeper in the Partner 1 Sexually Abused profile than the Low CM profile; sexual distress decreased for the Low CM profile and increased for the Partner 1 Neglected and the Partner 2 Sexually Abused profiles; and decreases in sexual function were steeper in the Partner 1 Neglected and Partner 2 Sexually Abused profiles than the Low CM profile. Findings underscore how couples’ greater CM is associated with worse sexual health initially and over time, particularly when one partner reports higher levels of neglect or sexual abuse in the context of both reporting higher CM (i.e., profiles 1, 4 and 5). Results extend past work by shedding light on the important role of all CM experiences in couples’ sexual health and show how specific patterns between partners are critical to their sexuality outcomes over time. They also extend interpersonal models of trauma (Goff & Smith, 2005) and sexual dysfunction (Rosen & Bergeron, 2019).
Partially confirming our hypothesis that at least three distinct dyadic trauma profiles would be identified, with the largest one involving low levels of all types of CM in both partners, analyses yielded five profiles. Profile 1 (20.51%), Partner 1 Neglected, described couples in which both partners displayed higher than average cumulative CM, Partner 1 displayed higher than average physical and emotional neglect, and Partner 2 displayed lower than average physical and emotional abuse. Profile 2 (48.88%), Low CM, described couples reporting average-to-low CM experiences where both partners were younger. Profile 3 (10.93%), Partner 2 Physically Abused, described couples in which Partner 1 reported average-to-low CM experiences, whereas Partner 2 reported higher than average cumulative CM coupled with higher than average physical abuse, i.e., only one partner had high levels of trauma. Profile 4 (12.06%), Partner 2 Sexually Abused, described couples in which both partners reported higher than average cumulative CM and Partner 2 also reported higher than average sexual abuse. Profile 5 (7.63%), Partner 1 Sexually Abused, was similiar to Profile 4, except that Partner 1 had higher odds of being a woman with higher than average sexual abuse and of identifying as a sexual minority (e.g., bisexual, etc.), yet partnered with a man – suggesting that gender and sexual orientation may play a role in couples’ profiles.
Overall, profiles 1, 4 and 5 can be characterized as dual-trauma couples, profile 3 as one-partner-trauma couples, and profile 2 as low-level-trauma couples. Taken together, findings indicate that about half of community couples presented with higher than average levels of CM, and that of these, the majority were dual-trauma couples. This result is striking and implies that inviduals tend to choose partners with similar levels of CM (DiLillo et al., 2009; Whisman, 2014), with only Profile 3 combining low and high CM partners and characterizing a small proportion (10.93%) of the entire sample. Both partners’ prior CM histories may interact to challenge their shared sexuality (Bergeron et al., 2022).
Initial levels of sexual satisfaction, sexual distress and sexual function (i.e., at T1) were indicative of significantly better sexual health in the Low CM profile, followed by the Partner 1 Sexually Abused, Partner 2 Physically Abused and Partner 2 Sexually Abused profiles, and significanty worse sexual health in the Partner 1 Neglected profile. These results show a consistent pattern whereby couples in which both partners reported low levels of CM fared the best, and couples in which both reported higher than average levels of cumulative CM and Partner 1 reported higher than average physical and emotional neglect fared the worst, as hypothesized. Findings corroborate those of a variable-centered dyadic study showing associations between greater CM of all types and lower initial sexual health (Vaillancourt-Morel et al., 2021). Importantly, they extend prior work by highlighting the particularly salient contribution of neglect to sexuality outcomes, relative to the emphasis on sexual abuse found in the cross-sectional literature (Bergeron et al., 2022; Najman et al., 2005). This novel finding suggests that sexual health may be disrupted not only via previously theorized traumatic sexualization (Finkelhor & Browne, 1985), but also by the powerlessness, invisibility and disregard characterizing emotional and physical neglect (Briere, 2002; Colman & Widom, 2004). When both partners present high CM, greater neglect in one of them could feed models of self as flawed, and of others as unresponsive. Clinically, enhancing couples’ ability to validate each other could counter this sense of unresponsiveness and facilitate communication of their sexual needs (Brassard et al., 2015).
Not only did dual-trauma couples present with worse sexual health at baseline, but their trajectories across the three time points tended to be steeper in the direction of worsening sexual health relative to the Low CM couples. Partner 2 Physically Abused, or one-partner-trauma couples, also fared better than the dual-trauma couples. Specifically, the Partner 1 Sexually Abused profile – in which Partner 1 had higher odds of being a woman with high levels of sexual abuse and identifying as sexually diverse but partnered with a man – presented with steeper decreases in sexual satisfaction than the Low CM profile. This corroborates findings from two systematic reviews showing lower sexual health among women with CSA (Bigras et al., 2021; Pulverman et al., 2018). In a recent study, both intrusive thoughts and pleasing the other during sex moderated the association between greater CSA and worse sexual function (Gewirtz-Meydan & Godbout, 2023) which could result in decreasing sexual satisfaction over time. The present finding sheds light on a dyadic profile characterized by one partner with high levels of CSA in a system where both partners report high levels of CM. According to The Couple Adaptation to Traumatic Stress model (Goff & Smith, 2005), trauma may yield dysfunctional relational dynamics fueled by both partners, as the non-CSA/high CM partner may exhibit the same cognitive biases, insecure attachment and emotion dysregulation as the CSA survivor (Vaillancourt-Morel et al., 2024).
Sexual distress decreased over a period of one year for the Low CM profile and increased for the Partner 1 Neglected and the Partner 2 Sexually Abused profiles, and sexual function decreased more steeply in the Partner 1 Neglected and Partner 2 Sexually Abused profiles than in the Low CM profile. This pattern of findings is noteworthy and points toward the greater vulnerability of dual-trauma couples concerning how their sexuality unfolds over time. Results indicate that not only did they experience lowering sexual desire, arousal and orgasmic capacity (i.e., poorer sexual function) over one year, but that this was accompanied by increasing sexual distress – indicative of potential sexual dysfunction.
The present study boasts several strengths, namely the use of novel dyadic person-centered analyses, a large and diverse sample of couples including from the sexual and gender diversity, a longitudinal design, the measurement of multidimensional aspects of sexual health and CM using validated instruments, and conceptually, the focus on the contributions of both cumulative CM and its specific subtypes to sexual outcomes. Nevertheless, this study presents some limitations. The constraints of the dyadic latent profile analyses did not allow us to examine the sexual health trajectories of each member of the couple, nor to examine cross-partner effects, i.e., how one partner’s CM relates to the other’s sexual health. The Childhood Trauma Questionnaire is retrospective and may involve recall bias. Couples in the study reported relatively good sexual health, with low variability in scores on the sexual outcomes. As such, they may not be representative of couples in therapy.
Findings yield three novel insights for sex and couple’s therapy. First, both partners’ CM experiences may play a role in couples’ sexual health and should be queried. Second, dual-trauma couples fare worse than those with low CM or a single partner reporting CM, and as such could benefit from trauma-informed care with an emphasis on attachment and emotion regulation (MacIntosh et al., 2020). Third, neglect may be as detrimental for couples’ sexual health as sexual abuse and should be an integral part of the initial assessment.
In conclusion, results indicate that for initial associations, sexual satisfaction, distress, and function formed a pattern showing the greatest sexual health in couples with lower CM and the worst, in those with high CM/high neglect in one partner. As for trajectories, sexual health decreased more steeply over one year across all outcomes for couples presenting with higher CM and either high neglect or high sexual abuse in one partner, i.e., for dual-trauma couples, relative to couples with lower CM. Results extend the growing body of literature on the role of trauma in individuals’ sexual health by focusing on novel couple profiles. All forms of CM should be examined in the assessment and treatment of sexual difficulties.
Supplemental Material
Supplemental material - Couples’ Childhood Maltreatment Profiles and Trajectories of Sexual Health over One Year
Supplemental material for Couples’ Childhood Maltreatment Profiles and Trajectories of Sexual Health over One Year by Sophie Bergeron, Natalie O. Rosen, Beáta Bőthe, Marie-Ève Daspe, Katherine Péloquin, Natacha Godbout, Audrey Brassard, Noémie Bigras, Marie-Pier Vaillancourt-Morel in Child Maltreatment
Footnotes
Acknowledgements
We thank István Tóth-Király for his help in conducting the pre-registration and data analyses. We thank Mylène Desrosiers, Gillian Hyslop, Jean-François Jodouin, Kathleen Merwin, Myriam Bosisio, Justin Dubé and Alice Girouard for their help in conducting this research.
ORCID iDs
Ethical Considerations
All procedures were approved by Université de Montréal and Dalhousie University’s Institutional Review Boards.
Author Contributions
Sophie Bergeron: Conceptualization, funding acquisition, investigation, methodology, project administration, resources, supervision, writing – original draft. Natalie O. Rosen: Funding acquisition, investigation, methodology, project administration, resources, supervision, writing – review and editing. Beáta Bőthe: Data curation, formal analysis, investigation, methodology, project administration, supervision, visualization, writing – review and editing. Marie-Ève Daspe: Conceptualization, methodology, supervision, writing – review and editing. Katherine Péloquin: Conceptualization, funding acquisition, methodology, writing – review and editing. Natacha Godbout: Conceptualization, writing – review and editing. Audrey Brassard: Conceptualization, writing – review and editing. Noémie Bigras: Conceptualization, writing – review and editing. Marie-Pier Vaillancourt-Morel: Conceptualization, data curation, investigation, methodology, project administration, supervision, writing – review and editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported in part by a Social Science and Humanities Research Council of Canada grant (435-2016-0668) and a Canada Research Chair awarded to the first author.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Transparency and Openness
This study’s design, hypotheses and analytic plan were preregistered after data for each of the four combined studies had been collected but before analyses for the present study were undertaken; please see ![]() . Given the sensitive nature of the data, the first author can provide data upon justified request.
. Given the sensitive nature of the data, the first author can provide data upon justified request.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.