
Abstract
State responses to substance use during pregnancy have included policies designed to increase access to substance use treatment as well as punish such substance use. Prior research has found that punitive policies are associated with increased rates of child maltreatment reporting, but it is unclear if the presence of punitive-promoting policies also moderate the association between access-promoting polices and maltreatment reports. Using data from the National Child Abuse and Neglect Data System and state-level fixed effects models, this study investigates how interactions between access-promoting and punitive prenatal substance use policies are associated with rates of substance use-associated maltreatment reports among infants. In states with punitive policies, access-promoting policies were associated with smaller decreases in these reports than in states without punitive policies. In some cases, access-promoting policies were associated with greater increases in these reports when punitive policies were also present than when only one type of policy was adopted. Interactions between prenatal substance use policies may result in unintended and counterproductive consequences for maternal and child health and the child welfare system.
In 2020, 8.3% of pregnant people reported illicit drug use in the past month (SAMHSA, 2022). These individuals are not only less likely to receive adequate prenatal and postnatal care (Simmons & Austin, 2022), but are also less likely to receive substance abuse treatment (Terplan et al., 2012) due to barriers like cost, stigma, lack of childcare, time limitations, and lack of providers (Salameh et al., 2021). With the number of pregnant people using drugs on the rise without access to adequate care (Admon et al., 2019), neonatal abstinence syndrome rates have increased over five-fold between 2004 and 2016 (Leech et al., 2020) and rates of substance use-associated foster care entries have increased 71% between 2008 and 2017 (Meinhofer et al., 2020). To respond to these concerns, states have adopted several policies aimed at identifying and addressing substance use during pregnancy, such as mandating substance use testing and reporting. However, some of these policies may have contradictory effects, such as expanding funding to treatment programs while deterring individuals from seeking access to these programs out of a fear of being reported. Prior studies have investigated how each of these policies in isolation are associated with substance use-associated maltreatment report rates; this study builds upon this important foundation by analyzing how these policies may operate in conjunction with one another. Specifically, this study uses administrative child maltreatment report data from the National Child Abuse and Neglect Data System (NCANDS) and state prenatal substance use policy data from the Guttmacher Institute to examine how interactions between policies promoting access to substance use treatment for pregnant people and policies promoting surveillance and punishment of prenatal substance use may be associated with changes in states’ substance use-associated maltreatment report rates among infants.
Theoretical Background
Punitive Policies
In this study and in prior research, punitive prenatal substance use policies refer to policies that expand surveillance of pregnant individuals’ potential substance use and increase civil penalties for such use. At the federal level, the Child Abuse Prevention and Treatment Act mandates that healthcare professionals identify substance-exposed newborns, create a safe plan of care, and notify child welfare agencies. However, this legislation does not require defining substance exposure as abuse, testing newborns for prenatal substance exposure, or for notifications to take the form of child maltreatment reports (National Advocates for Pregnant Women, 2020). Nevertheless, states have adopted policies defining substance use during pregnancy as child abuse, requiring health care workers to test for suspected substance use during pregnancy, and requiring health care workers to report such use to child welfare agencies. Intervention by the child welfare system in the case of prenatal drug exposure, however, is not always necessary when a child’s safety and well-being is not otherwise at risk (Lloyd et al., 2019), such as when pregnant people are using prescription opioids for pain management or opioid use disorder under the care of a physician. Lack of clinical knowledge of opioid dependence among child welfare professionals can result in inappropriate requirements such as withdrawing from medication treatment (also known as medication-assisted treatment; SAMHSA, 2016). The ostensible goal of such policies is to decrease the adverse health effects of prenatal drug exposure; however, recent studies generally do not find a reduction in the number of infants with prenatal substance exposure in states with these policies (Atkins & Durrance, 2020; Faherty et al., 2022), with some showing an increase in such rates in these states (Faherty et al., 2019; Meinhofer et al., 2022).
Prior research also demonstrates that punitive policies are associated with an increase in both maltreatment reports (Maclean et al., 2022) and foster care entries (Atkins & Durrance, 2021; Sanmartin et al., 2019). This association may exist for three major reasons. First, most directly, these policies promote greater surveillance of prenatal drug exposure; greater testing of pregnant individuals and infants could result in a greater number of cases of exposure. Second, when states statutorily define prenatal substance use as child abuse, certain types of exposure that might not have been considered maltreatment in other states (e.g., medication treatment for opioid use disorder) may be screened in by child welfare workers as potential abuse. Third, these policies may increase substance use-associated maltreatment reports because pregnant individuals are less likely to seek treatment for substance use disorders out of a fear of being reported (Atkins & Durrance, 2020) and, when they do seek out treatment, are less likely to receive high-quality treatment (Angelotta et al., 2016; Tabatabaeepour et al., 2022).
Furthermore, punitive policies neither address implicit (or explicit) bias among healthcare providers in screening for prenatal substance use, nor inequitable access to effective substance abuse treatment. Mounting evidence suggests that healthcare providers are more likely to screen people of color for prenatal substance use (Cohen et al., 2023) regardless of patients’ substance use history or other risk factors (Jarlenski et al., 2023). Among patients identified as having prenatal substance use, Black patients are also more likely to be reported to child protective services (Roberts & Nuru-Jeter, 2012). Universal screening and reporting protocols, two commonly suggested remedies, do not reduce these disparities (Patel et al., 2021; Roberts et al., 2015). In addition, although required reporting and testing may help healthcare providers identify and refer parents to substance abuse treatment, treatment rates remain low overall (one study estimates only 13% of pregnant people with substance use disorders obtain treatment; Salameh et al., 2021), with especially low rates of medication treatment, the gold standard treatment, among Black parents (Salameh et al., 2019; Schiff et al., 2020). Overall, punitive policies are not effective in reducing neonatal abstinence syndrome, reducing child maltreatment cases associated with substance use, increasing uptake of substance abuse treatment treatment, or reducing racial disparities in these outcomes.
Access-Promoting Policies
Another strategy states have taken to address prenatal substance exposure is expanding access to substance abuse treatment for pregnant people. Such policies include targeted funding of substance abuse treatment programs for pregnant individuals, prohibiting discrimination against pregnant individuals in substance abuse treatment programs, and priority access to substance abuse treatment programs for pregnant individuals. The evidence for the efficacy of these programs in improving maternal and infant health outcomes is somewhat mixed (Faherty et al., 2022; Meinhofer et al., 2022; Tabatabaeepour et al., 2022). Previous research indicates that these policies were not associated with a decrease in maltreatment reports (Maclean et al., 2022). However, these policies have the potential to reduce substance use-associated maltreatment reports in particular by improving access to high-quality substance abuse treatment and destigmatizing substance use disorders among pregnant people (Roberts et al., 2019).
Interaction Between Punitive and Access-Promoting Policies
It is possible that the reason access-promoting policies do not appear to be associated with maltreatment reports is because prior studies have not investigated variability in how these policies operate based on other elements of state policy environments regarding substance use during pregnancy. These environments are complex and often include both punitive and access-promoting elements, which may have unintended and/or conflicting consequences for families affected by substance use disorders. One potential interaction is that punitive policies would limit the efficacy of access-promoting policies in reducing infant maltreatment reports due to parental substance use. At the implementation level, government leaders report difficulty in adopting access-promoting policies due to conflicting punitive laws, stigma against pregnant individuals who use drugs, and a lack of treatment facilities (White et al., 2022). At the individual level, pregnant individuals may be more likely to avoid seeking out treatment in states with punitive policies due to fear of being reported (Stone, 2015), even when resources are available.
Another possibility is that the combination of both punitive and access-promoting policies could lead to greater maltreatment report rates rather than adopting one type of policy alone because greater access to treatment may entail greater opportunities for the detection of substance use, particularly in states requiring prenatal drug testing and reporting (Goodman et al., 2019). For example, participation in treatment may trigger a report if a substance abuse counselor observes and reports maltreatment (Center for Substance Abuse Treatment, 2000). Treatment may also lead to a report because a toxicology screening report ordered by a healthcare provider detects not only illicit drug use, but also prescribed substances like drugs for medication-assisted substance abuse treatment (e.g., methadone). State legislation can be ambiguous in its definition of prenatal drug exposure and can include prenatal exposure to prescribed substances as a mandatory reason for reporting (Goodman et al., 2019; McCourt et al., 2022; Radel et al., 2018). In other words, greater access to substance abuse treatment can also make pregnant individuals and their children more vulnerable to surveillance, facilitating contact with the child welfare system.
The Current Study
The current study addresses how the interplay of punitive and access-promoting prenatal substance use policies shape states’ rates of substance use-associated maltreatment report rates among infants using state-level fixed effects models. The following hypotheses will be tested: Access-promoting policies will be associated with lower substance use-associated maltreatment report rates in states without punitive policies. However, in states with punitive policies, access-promoting policies will either not be associated with substance use-associated maltreatment report rates or will be associated with greater report rates.
Data and Methods
Data
Child maltreatment report data came from the 2008 to 2019 National Child Abuse and Neglect Data System (NCANDS) Child Files, which includes case-level data on each report of alleged child maltreatment that received a response from child protective services (Children’s Bureau, 2019). Rates of maltreatment reports per 1000 infants were calculated using intercensal and postcensal estimates of the population of infants ages 0–1 by state and year from the U.S. Census Bureau (National Center for Health Statistics, 2012; 2020). Data on prenatal substance use policies came from a dataset compiled by the Guttmacher Institute (Guttmacher Institute, 2022) and obtained through direct communication with their Public Policy team. This dataset tracked the status of the six policies discussed below across states each year and has been used in a number of publications investigating the associations of prenatal substance use policies and infant health and child welfare outcomes (Kozhimannil et al., 2019; Maclean et al., 2022; Meinhofer et al., 2022; Sanmartin et al., 2019; Tabatabaeepour et al., 2022). State sociodemographic covariates came from the 2008-2019 American Community Survey (ACS) 1-year estimates (U.S. Census Bureau, 2020). Additional data sources for covariates included the Centers for Disease Control and Prevention (2021; opioid prescription dispensation rate) and the Kaiser Family Foundation (2022; Medicaid expansion status).
Measures
Substance Use-Associated Maltreatment Report Rate
State substance use-associated maltreatment report rates per 1000 infants were calculated using the total number of substance use-associated maltreatment reports among children ages 0–1 for each state and year divided by the population of children ages 0–1 for each state and year multiplied by 1000. Reports included whether multiple types of caregiver or child risk factors were present; reports were considered to be “substance use-associated” if the report indicated “drug abuse” or “prenatal exposure to drugs” as a caregiver or child risk factor. Children could have multiple reports per year and per day. Multiple reports per day were considered to be one report; if any of these reports included “drug abuse” as a risk factor, then the report was coded as substance use-associated. Multiple reports per year for a single child with substance use as a risk factor were each counted in a state’s total substance use-associated report rate.
Policies
Six policies regarding substance use during pregnancy were the independent variables of interest in this study. Three of these policies were considered punitive: substance use during pregnancy defined as child abuse under civil child welfare statutes, requirements for health care professionals to report suspected substance use during pregnancy, and requirements for health care professionals to test for suspected prenatal drug exposure. The other three policies were considered to be access-promoting with regards to substance use treatment for pregnant people. These policies included the creation of drug treatment programs targeted to pregnant individuals, protection from discrimination against pregnant individuals in state-funded drug treatment programs, and priority access to these programs for pregnant individuals. A dichotomous variable for each policy indicated if the policy was present in each state in a given year.
Covariates
The models included five time-varying state-level socioeconomic confounders from the 2008 to 2019 American Community Surveys: the percentage of the population with an income below 150% of the federal poverty level, the percentage of the population ages 16 and older that is unemployed, the percentage of the population ages 25 and older with a college degree or higher, the percentage of the population with health insurance, and a state’s Gini coefficient indicating its level of income inequality. Additionally, because children of color, particularly American Indian/Alaska Native (AI/AN) and Black children, are more likely to experience a child maltreatment report (Kim & Drake, 2019), models controlled for changes in states’ racial composition by including three variables indicating the percentage of the population that was non-Hispanic white, Black, or AI/AN. Finally, the models included a time-varying dichotomous indicator of whether or not a state had expanded Medicaid eligibility for adults with incomes up to 138% of the federal poverty level, as well as states’ opioid prescription dispensation rate per 100 people.
Methods
The analysis was conducted using state-level fixed effects regression models, which control for all unobservable and observable time-invariant confounders at the state level. In other words, states serve as their own controls and coefficients can be interpreted as how change in one characteristic (policy adoption) produces change in another (substance use-associated maltreatment report rates) over time. Analyses were conducted in Stata/SE 17.0 (StataCorp, 2021) using the xtreg package (Allison, 2009). Following the advice of Kropko and Kubinec (2020), year-level fixed effects are not included so that the coefficient estimates clearly represents how policy change within each state is associated with change in report rates within that state, generalized to all states, rather than mixing over-time and between-state variation. Importantly, these models focus only on how policies are associated with variation in report rates over time within states and thus do not explain variation in maltreatment report rates between states. The first baseline model assessed the impact of the policies without any interaction terms. The following nine models included interaction terms for each pairwise combination of access-promoting and punitive policies (i.e., each of the three punitive policies interacted with each of the three access-promoting policies). All models included all time-varying indicators of whether each policy was present, as well as time-varying control variables. The adjusted predicted rates of substance use-associated maltreatment reports for each combination of punitive and access-promoting policies were calculated following each model using the margins command.
Results
Although the NCANDS began in 2000, not all states participated in the initial years. By 2008, at least 48 states and D.C. consistently participated in NCANDS, covering 97% of the child population (U.S. DHHS, 2010). North Dakota and Oregon did not submit data in 2008–2009 and 2008–2011, respectively. With these exclusions, the final sample size was 606 state-years (51 states across 12 years minus 6 missing state-years).
Figure 1 plots the number of states with each type of policy (punitive or access-promoting) and the rate of overall child maltreatment reports and substance use-associated reports among infants between 2008 and 2019. The number of states with any type of policy regarding prenatal substance use grew over time: from 24 in 2008 to 33 in 2019 for access-promoting policies, from 27 in 2008 to 32 in 2019 for punitive policies, and from 14 in 2008 to 23 in 2019 for both types of policies. See Supplementary Table 1 for the average number of years each policy was in effect between 2008 and 2019 among all states and among only those where each policy was ever adopted. In terms of maltreatment reports among infants, overall maltreatment report rates per 1000 infants increased by 19.2% from 64.0 to 76.2 reports per 1000 infants between 2008 and 2019. Substance use-associated maltreatment report rates, however, tripled from 4.4 to 13.5 reports per 1000 infants between 2008 and 2019, going from making up 7.0% in 2008 to 17.7% of all reports among this age group in 2019. Number of states with each type of policy and rates of child maltreatment reports per 1000 infants, 2008–2019.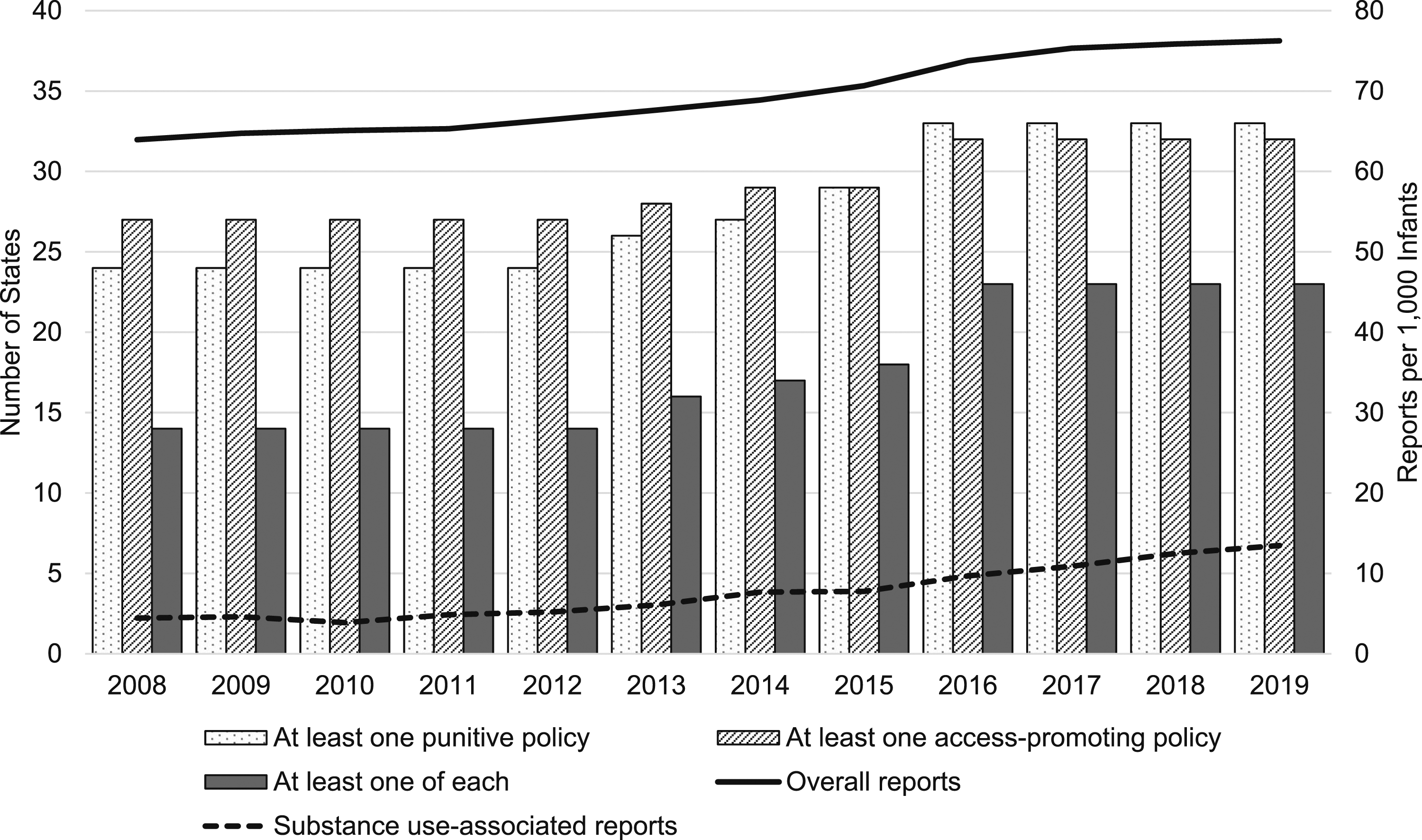
Descriptive Statistics of Sample (N = 606 State-Years).
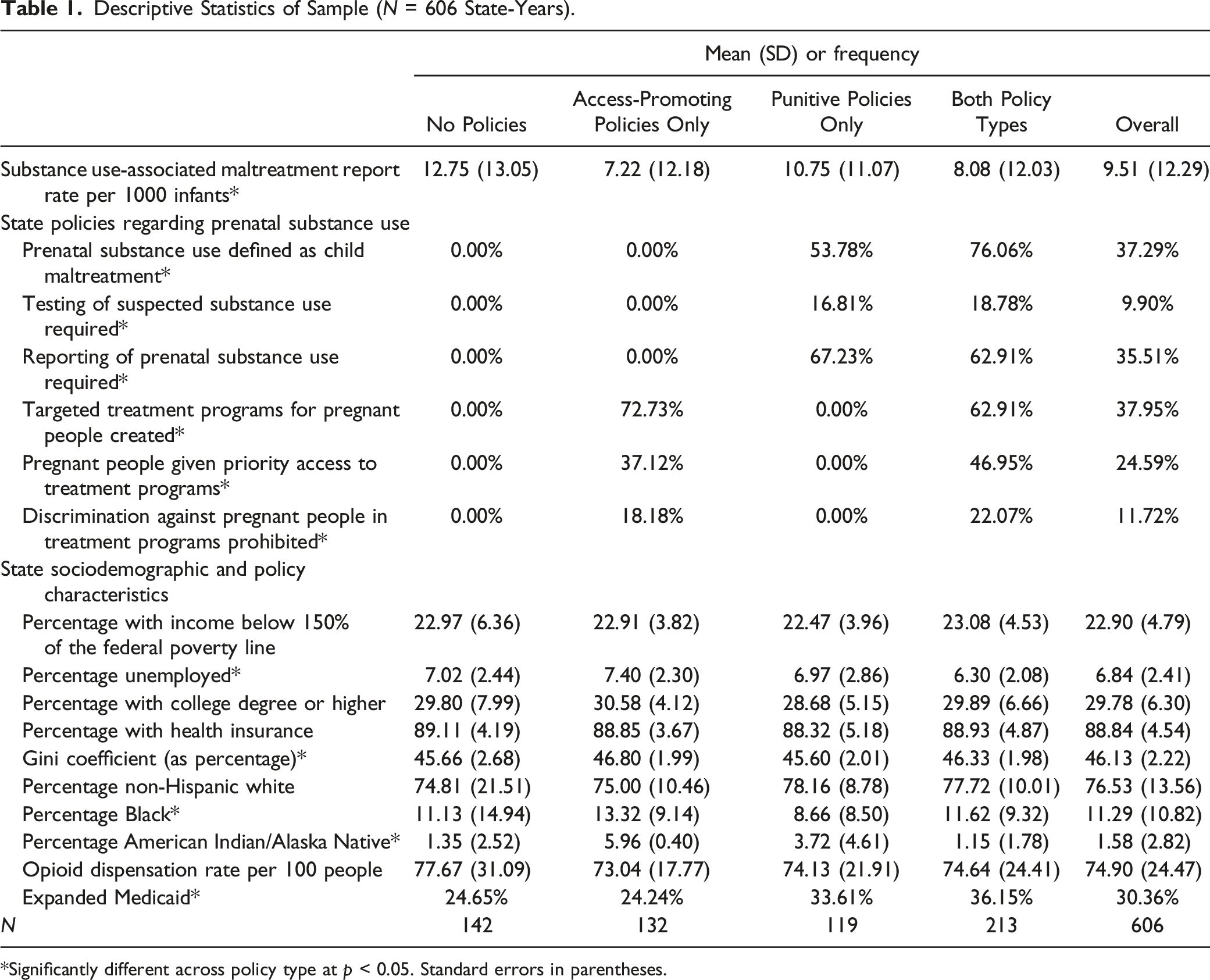
*Significantly different across policy type at p < 0.05. Standard errors in parentheses.
Main Models
State-Level Fixed Effects Models Predicting Rates of Substance Use-Associated Child Maltreatment Reports Among Infants, Prenatal Substance Use Defined as Child Maltreatment (N = 606 State-Years).
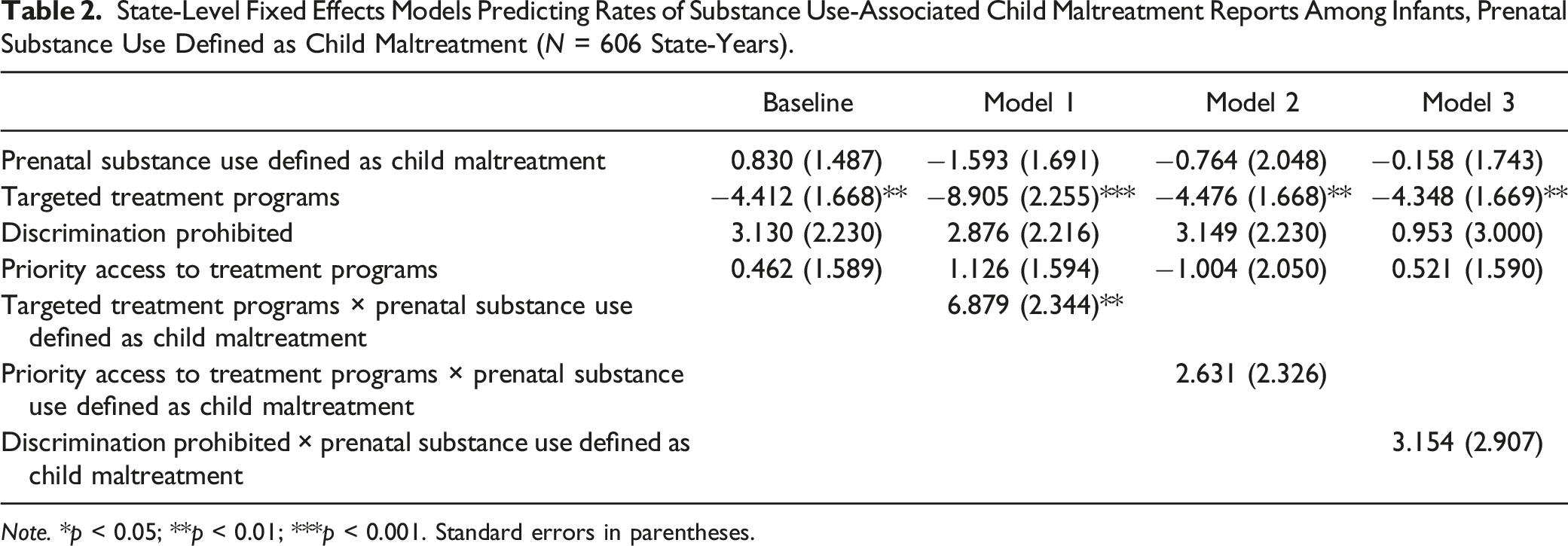
Note. *p < 0.05; **p < 0.01; ***p < 0.001. Standard errors in parentheses.
State-Level Fixed Effects Models Predicting Rates of Substance Use-Associated Child Maltreatment Reports Among Infants, Reporting of Prenatal Substance Use Required (N = 606 State-Years).
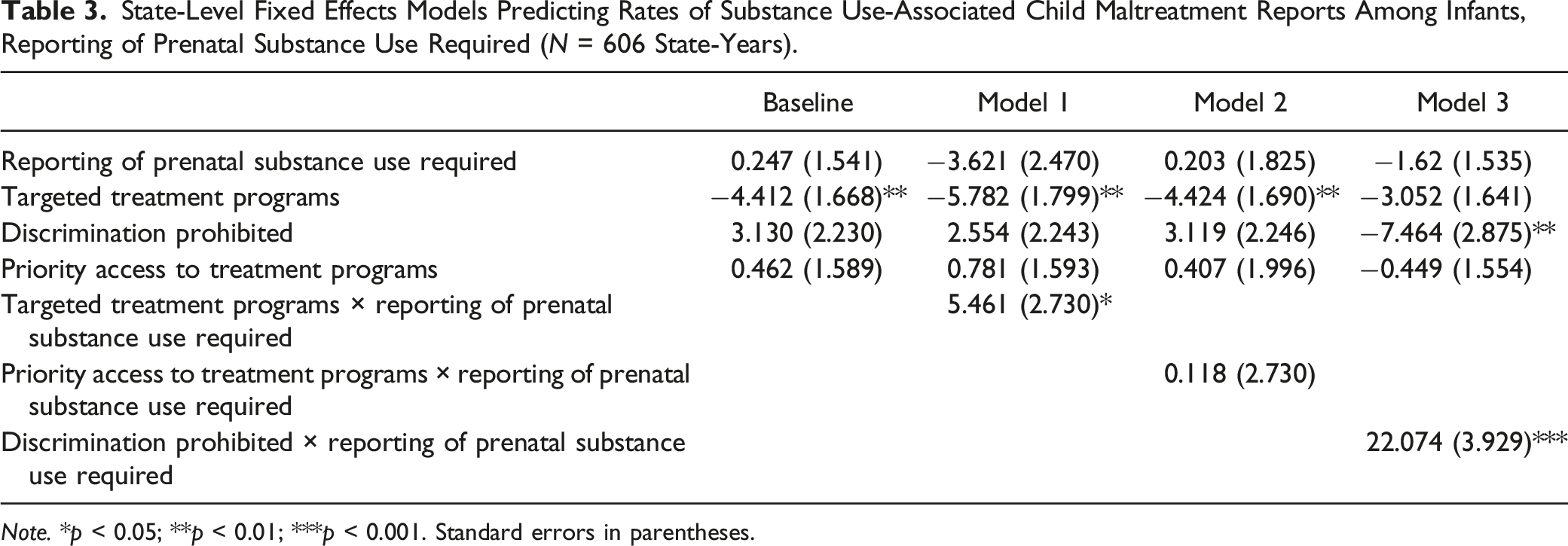
Note. *p < 0.05; **p < 0.01; ***p < 0.001. Standard errors in parentheses.
State-Level Fixed Effects Models Predicting Rates of Substance Use-Associated Child Maltreatment Reports Among Infants, Testing of Prenatal Substance Use Required (N = 606 State-Years).
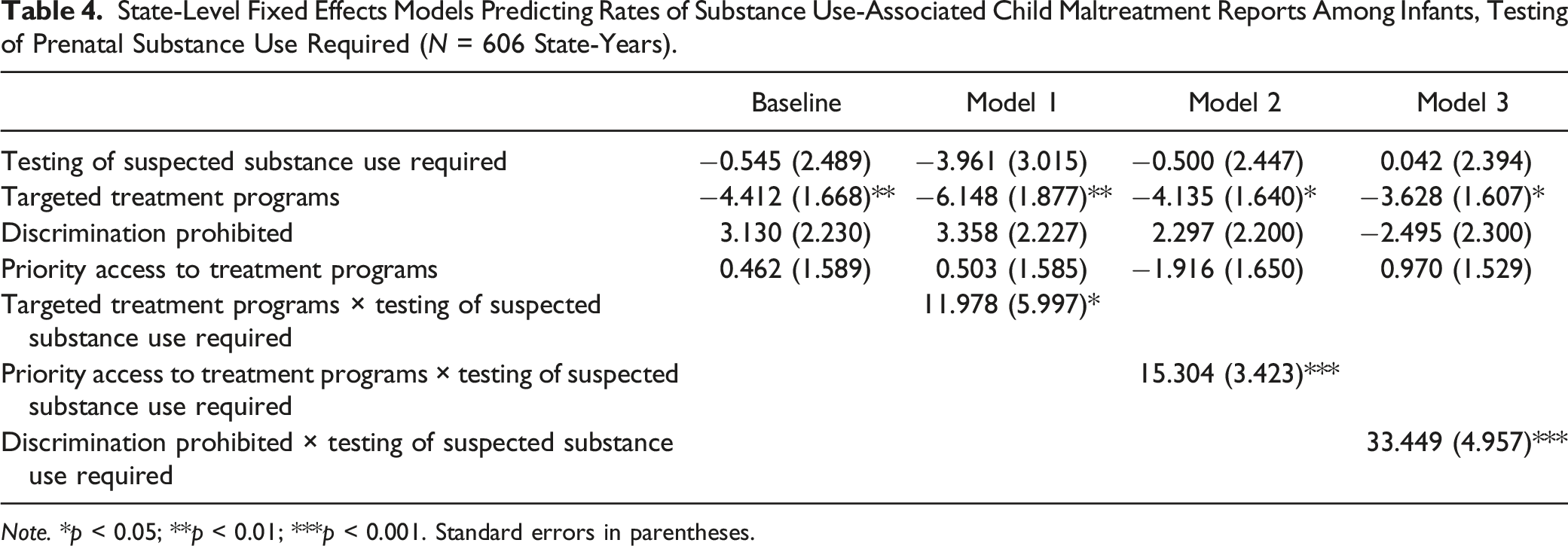
Note. *p < 0.05; **p < 0.01; ***p < 0.001. Standard errors in parentheses.
Models 1–3 of Table 2 show the interactions between prenatal substance use defined as child maltreatment and each of the access-promoting policies. There was a significant interaction between targeted treatment programs and prenatal substance use defined as child maltreatment such that prenatal substance use defined as child maltreatment attenuated the association of targeted treatment programs with lower substance use-associated maltreatment report rates. Specifically, in states where prenatal substance use was not defined as child maltreatment, targeted treatment programs were associated with a decrease of 8.91 substance use-associated reports per 1000 infants. However, in states which had both targeted treatment programs and prenatal substance use defined as child maltreatment, targeted treatment programs were associated with a decrease of 2.03 substance use-associated reports per 1000 infants. No other interactions with prenatal substance use defined as child maltreatment were statistically significant. Figure 2 summarizes these findings with predicted rates for each combination of policy interactions shown in Table 2. States in years with targeted treatment programs had a predicted substance use-associated maltreatment report rate of 3.34 reports per 1000 infants, compared to 8.63 reports per 1000 in states in years with both targeted treatment programs and prenatal substance use defined as child maltreatment. Predicted rates of substance use-associated child maltreatment reports per 1000 infants by state policy combination, prenatal substance use defined as child maltreatment.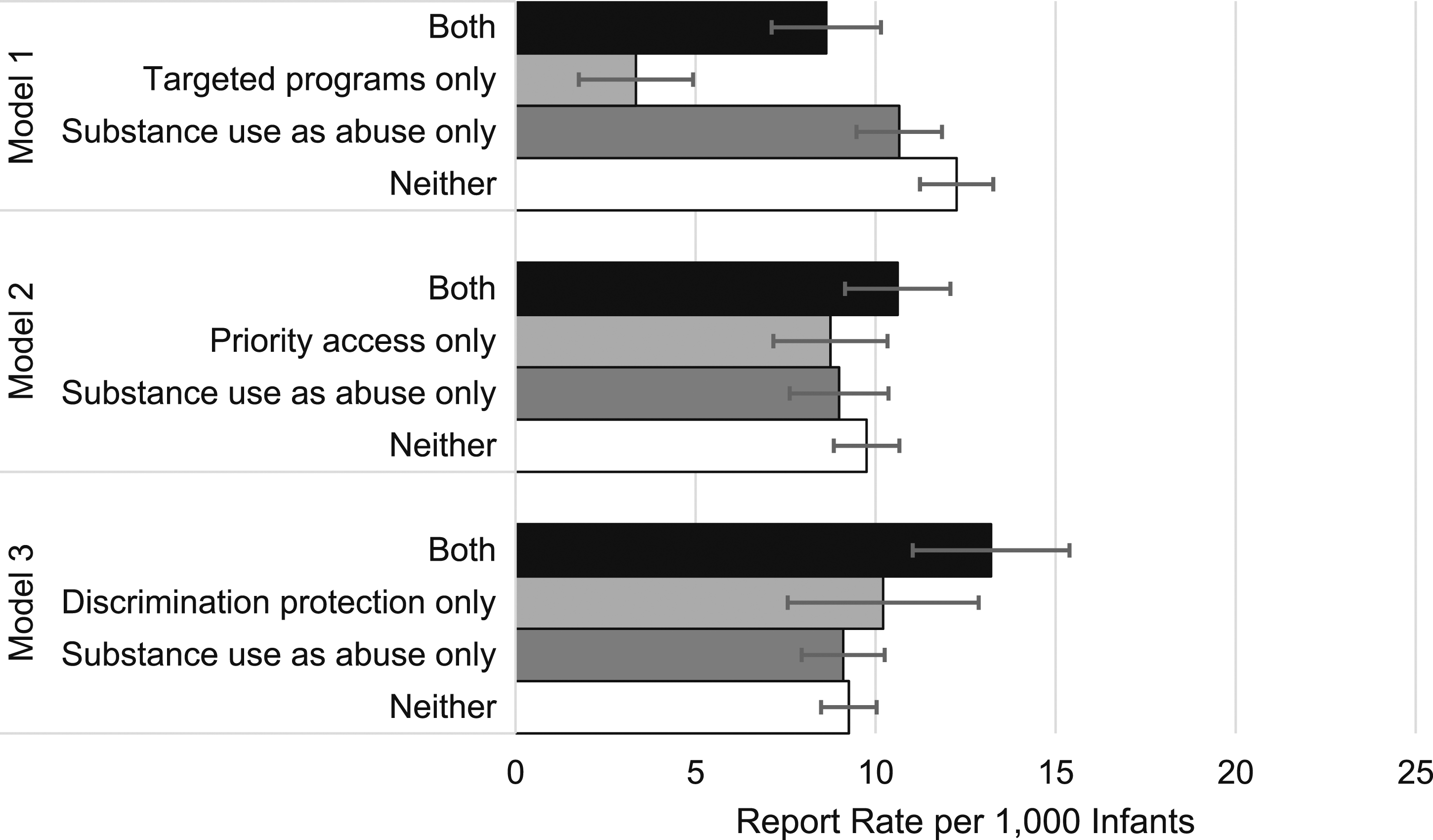
Turning to the next punitive policy, Models 1–3 of Table 3 show the interactions between required reporting of suspected prenatal substance use and the three access-promoting policies. Similar to prenatal substance use being defined as child maltreatment, required reporting use attenuated the association of targeted treatment programs with lower substance use-associated child maltreatment report rates. In states in years without required reporting, targeted treatment programs were associated with a 5.78 decrease in maltreatment report rates, but in states in years with required reporting this decrease dropped to 0.32. Required reporting reversed the association of prohibited discrimination against pregnant individuals in treatment programs with lower maltreatment reports. Prohibitions against discrimination in states during years in which reporting was not required were associated with a decrease of 7.46 reports per 1000 infants. However, in states in years with required reporting, prohibitions against discrimination were associated with an increase of 14.61 reports per 1000 infants. Like Figure 2, Figure 3 shows the predicted rates of child maltreatment reports for each policy interaction shown in Table 3. Predicted rates of substance use-associated child maltreatment reports per 1000 infants by state policy combination, reporting of prenatal substance use required.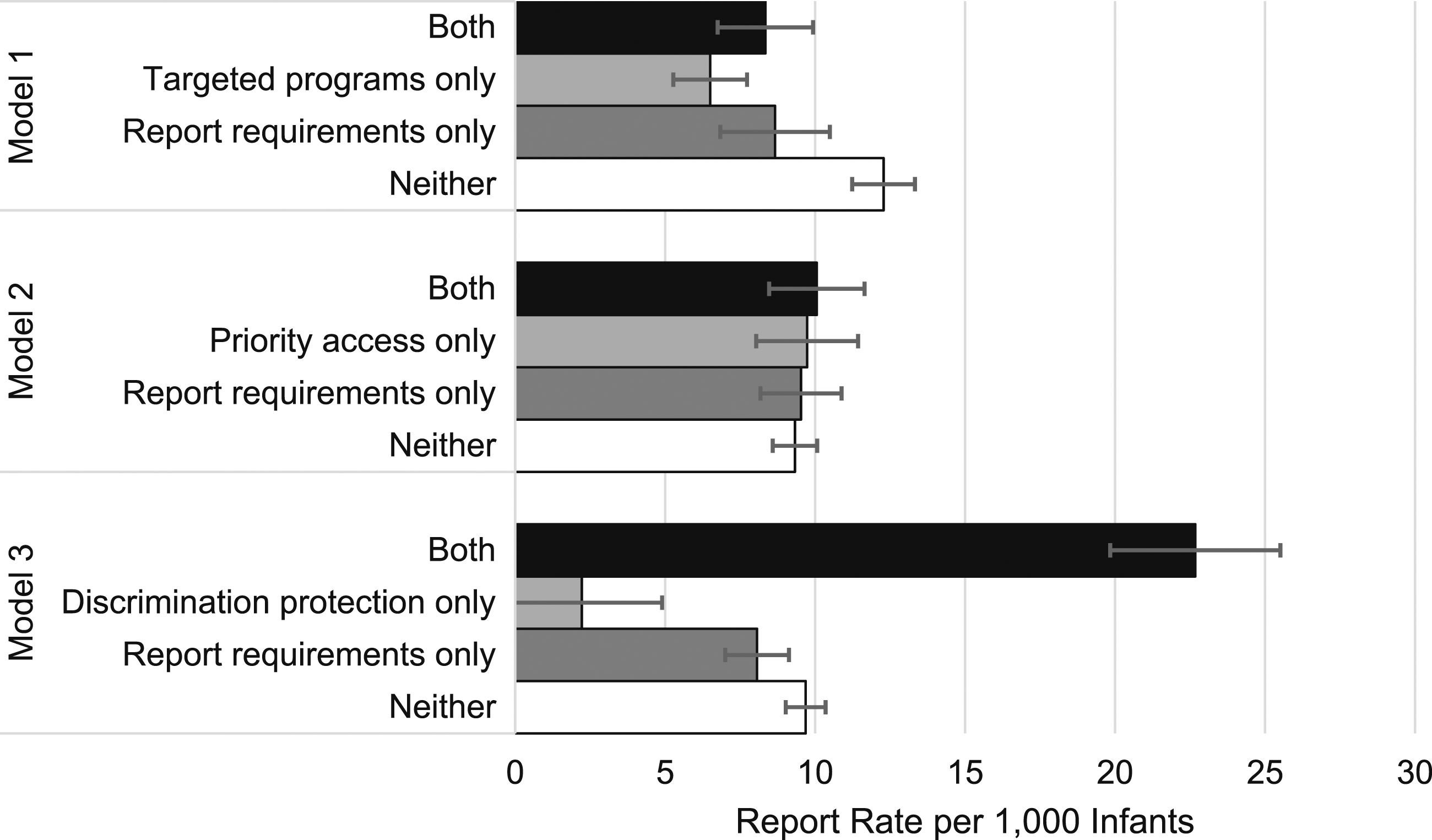
Lastly, Table 4 presents the interactions between required testing of suspected prenatal substance use and the three access-promoting policies. As with required reporting and prohibitions against discrimination, required testing reversed the association of targeted substance use treatment programs for pregnant individuals with lower substance use-associated maltreatment report rates. In states in years without required testing, targeted treatment programs were associated with a 6.15 decrease in the substance use-associated maltreatment report rate; in states in years with required testing, targeted treatment programs were associated with a 5.83 increase in these rates. There was no significant main effect of required testing or priority access to treatment programs. However, in states in years with both policies, priority access to treatment programs was associated with a 13.39 increase in rates compared to a decrease of 1.92 in states in years without required testing. A similar pattern was present for required testing and prohibitions against discrimination. Although there were no significant main effects of either policy, in states in years with both policies, prohibitions against discrimination were associated with a 30.95 increase in rates compared to a decrease of 2.50 in states without required testing. Figure 4 summarizes the predicted rates for each combination of policies explored in Table 4. Predicted rates of substance use-associated child maltreatment reports per 1000 infants by state policy combination, testing of prenatal substance use required.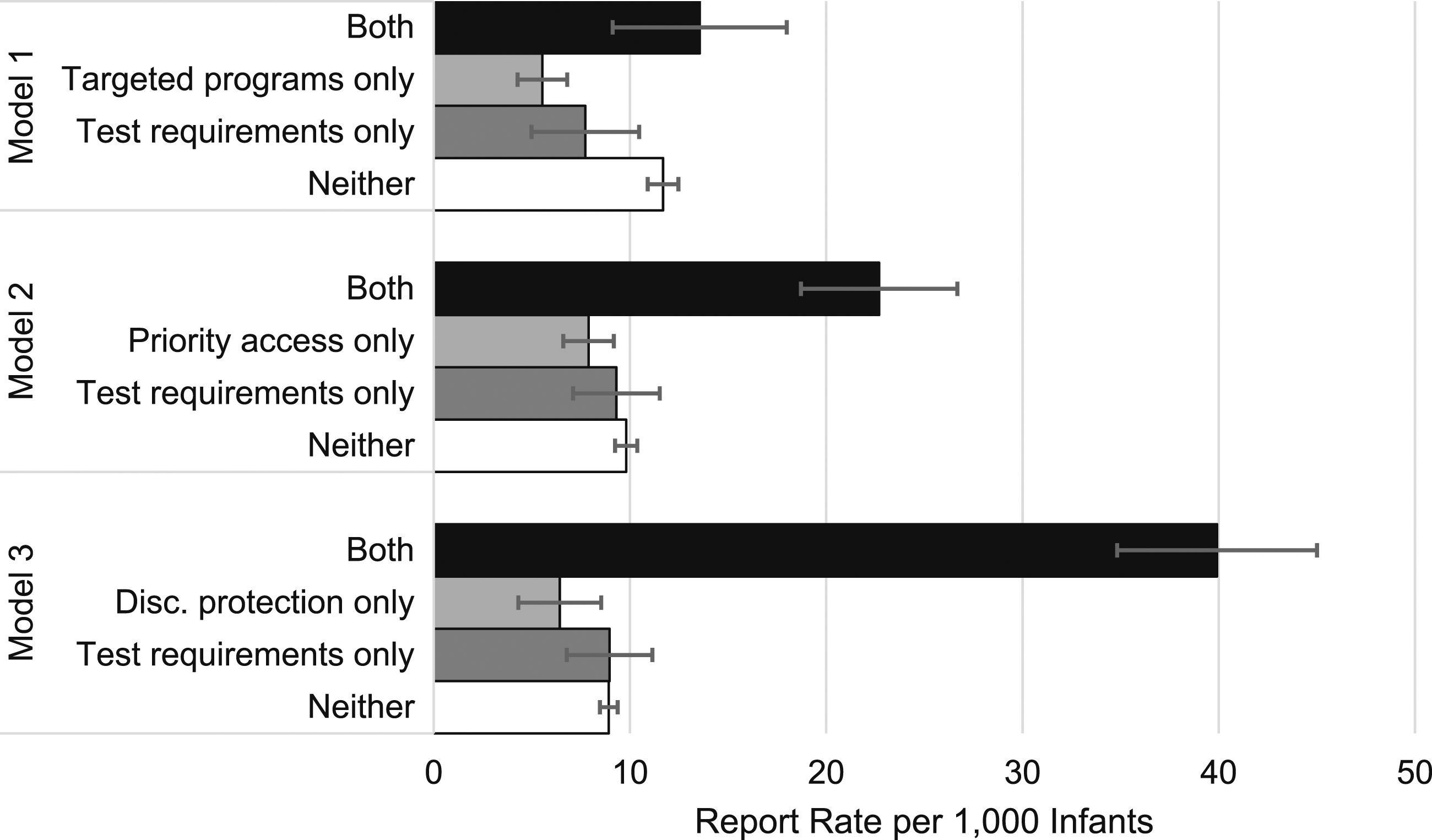
Sensitivity Analyses
In additional models, the interactions between punitive and access-promoting policies were similar but weaker in magnitude for substance use-associated maltreatment report rates among youth ages 2–17, which may be due to siblings of infants with exposure to substances becoming involved with the child welfare system following a report. Interactions between policies were also weaker for maltreatment reports not involving substance use among both infants and older youth, lending support to the idea that greater detection and reporting of prenatal substance use drives the main results. See Appendix 1 in the Supplementary Material for details about additional robustness checks, including controlling for states' female incarceration rate (Bureau of Justice Statistics, 2019) and lagging substance use-associated report rates by one year .
Discussion
This study used administrative child welfare data and state-level fixed effects models to examine how policies promoting treatment access for pregnant people were associated with substance use-associated maltreatment reports depending on whether punitive policies were also present. Two main patterns emerged. First, some access-promoting policies were associated with a decrease in substance use-associated maltreatment reports, but this inverse association was attenuated in the presence of punitive policies. Second, some access-promoting policies were associated with an increase, rather than a decrease, in substance use-associated maltreatment reports when a punitive policy was also present.
One likely reason that punitive policies attenuated the association of access-promoting policies with lower substance use-associated maltreatment reports is that these policies may prevent individuals from seeking care for substance use disorders. Pregnant individuals with substance use disorders report fearing intervention from child welfare agencies if they disclose substance use to their healthcare providers or engage in substance abuse treatment (Frazer et al., 2019; Jessup et al., 2003; Ostrach & Leiner, 2019; Paris et al., 2020). Although access-promoting policies may reduce some of the logistical barriers to treatment, fear and stigma, particularly in states with punitive policies, may prevent pregnant people from accessing timely substance abuse treatment that would prevent child welfare involvement (Atkins & Durrance, 2020; Choi et al., 2021). Beyond reducing parents’ access to substance abuse treatment, punitive policies are also associated with later prenatal care initiation, lower rates of adequate prenatal care, and lower rates of postpartum health care visits (Austin et al., 2022; Meinhofer et al., 2022). This avoidance of care means fewer opportunities for healthcare providers to detect and treat not only substance use disorders, but also other pre- and postnatal health conditions, like gestational diabetes or postpartum depression.
In some cases, the combination of both punitive and access-promoting policies was associated with a greater increase in substance use-associated maltreatment reports among infants than when only one type of policy was adopted. This finding parallels a study by Edwards (2016), who finds that larger social welfare bureaucracies attenuate the inverse association between generous welfare regimes and foster care entries and hypothesizes that this finding is due to increasing opportunities for surveillance. Indeed, substance abuse treatment entails greater exposure to surveillance for pregnant individuals, and responses to their substance use may be harsher in states with punitive policies in place. For example, substance use counselors are mandated reporters of child abuse and neglect, and it is unclear if they are required to report pregnant patients when states statutorily define substance use during pregnancy as child maltreatment (Center for Substance Abuse Treatment, 2000). In addition, some healthcare providers report the use of medication treatment to child protective services as maltreatment (Kaminsky, 2019); in other words, attempts to address substance use disorders, which state legislation may encourage, is also punished according to state legislation. This lack of policy clarity and the resulting punitive approaches are counterproductive for both family well-being and the child welfare system. Cases involving infants at low risk of abuse or neglect, such as parents whose use of opioids or other prescriptions is under the care of a doctor, unnecessarily add pressure to an already overburdened child welfare system characterized by large caseloads, insufficient funding, rapid staff turnover, and high staff burnout (Patrick et al., 2019). Furthermore, testing and reporting for a medical problem – substance use disorder – is ethically questionable when adequate treatment may not be available (Hadland et al., 2020) and/or seeking treatment will be punished.
The findings of this study may also have implications for racial and socioeconomic inequalities in the child welfare system. A previous study found that punitive policies reduce the access-promoting effects of Medicaid expansion on substance use treatment for low-income pregnant people (Choi et al., 2021). Similarly, low-income families disproportionately rely on the programs that the access-promoting policies examined in this study fund, and punitive policies may curtail their access. Although this study does not directly test this hypothesis, the increase in substance use-associated report rates in states with a combination of access-promoting and punitive policies may be disproportionately concentrated among low-income parents and parents of color. Parents with Medicaid and parents of color are more likely to be screened (Patel et al., 2021; Roberts & Nuru-Jeter, 2012) and reported for substance use during pregnancy (Rebbe et al., 2019; Wakeman et al., 2022), but are less likely to receive medication treatment, the gold standard treatment for opioid use disorder, especially in states with punitive policies (Angelotta et al., 2016). Pregnant individuals of color are also less likely to complete substance abuse treatment compared to white individuals, which may be in part due to fear of punitive approaches to substance use during pregnancy (Suntai, 2021). In sum, previous research indicates that low-income families and families of color disproportionately face the downsides of prenatal substance use policies (e.g., greater risk of contact with the child welfare system) without the benefits (e.g., referral and access to high-quality treatment). Future research should investigate how changes in prenatal substance use policy may ameliorate or exacerbate racial and socioeconomic disparities in child maltreatment reports associated with parental substance use.
In addition to changing policies, this study found that changes in states’ racial composition, Medicaid coverage, and rate of opioid prescribing were also associated with states’ substance use-associated maltreatment reporting among infants. The positive association between states’ proportion of AI/AN and white residents and substance use-associated report rates reflects that AI/AN and white children have had the highest growth in substance use-associated report rates in recent decades (Meinhofer et al., 2020). For AI/AN children in particular, this finding reflects the social and economic vulnerability and lack of access to important harm reduction resources in these communities (Luken et al., 2021). Expansion of Medicaid may be positively associated with substance use-associated report rates due to low-income parents with substance use disorders coming into greater contact with mandatory reporters in the healthcare system (Stritzel, 2022). The finding that opioid prescription rates had a small but inverse association with maltreatment report rates was somewhat counterintuitive and may reflect state-level heterogeneity in the association between opioid prescriptions and child welfare outcomes (Quast, 2018).
Limitations of this study include error in measurement of the outcome variable, such as the unavailability of child maltreatment reports that did not receive a response from child protective services (89.1% of substance use-associated reports received a response in 2020 [U.S. DHHS, 2022]). There may also be variability in how child welfare workers decide which reports to define as associated with substance use (Seay, 2015). The NCANDS variables used to identify prenatal substance use exposure in this study indicate if the child or caregiver has a problem with “compulsive use of drugs that is not of a temporary nature”, including a child’s prenatal exposure to drugs. Thus, this definition could capture reports involving exposure to substances that is not specifically in-utero, but given that the analysis is limited to infants ages 0–1, reports associated with substance use likely indicate maternal use in the pre- or perinatal period. Furthermore, state-level fixed effects are able to account for differences in how states define and report prenatal substance use exposure if these differences do not change over time. In addition, the type of drug involved in the child maltreatment report is not identified in the NCANDS data, so it is unclear if these policies differentially affect rates of reporting for different types of substances. This analysis was conducted at the state rather than individual level, thus hypotheses about the individual-level mechanisms driving these associations are preliminary. Classifying and defining policies across states as one of six types also requires some subjectivity and a binary indicator of whether a given policy type was in place leaves out some variation in state-specific regulations. Future research will need to describe how changing policy environments are associated with the decision-making processes of healthcare providers and parents with substance use disorders. Nevertheless, the strength of this analysis is revealing how macro-level interactions between state policies may have unintended consequences for infant health and child welfare outcomes.
The findings of this study support several policy recommendations, which have been echoed by legal scholars and obstetricians/gynecologists (Faherty et al., 2020). First, substance use should be decoupled from definitions of child abuse and not automatically trigger a maltreatment report in the absence of evidence of child abuse or neglect. Under some current state laws, using appropriately prescribed opioids during pregnancy may be considered child abuse even if there are no threats to an infant’s safety or well-being. Furthermore, defining substance abuse as child maltreatment is at odds with medically accepted conceptions of substance abuse as a chronic illness that requires treatment, not civil or criminal scrutiny (Nguemeni Tiako & Sweeney, 2022). Second, states should create a separate system outside of the child welfare system for collecting anonymized data on infants born with substance use exposure (Wakeman et al., 2022) so that states can fulfill reporting requirements of the Child Abuse Prevention and Treatment Act without unnecessarily involving low-risk families with the child welfare system. Lastly, decisions about testing and reporting prenatal substance use exposure should be made in the context of an individual’s full medical history and with the individual’s consent. Arguably, one potential benefit of reporting is that parents and children may receive care that they would not have otherwise. However, decisions about substance use treatment and medical care should ideally be made by healthcare professionals rather than social workers or judges, who are operating under different perspectives, policies, and organizational goals (SAMHSA, 2016). Judges and caseworkers should be better informed about the efficacy and safety of medication treatment in managing substance use disorders (Radel et al., 2018) and recognize that use of such treatment is not in and of itself incompatible with effective parenting. Overall, current prenatal substance use policies need to better support pregnant people’s access to and participation in substance abuse treatment in order to keep families together and healthy.
Supplemental Material
Supplemental Material - Substance Use-Associated Infant Maltreatment Report Rates in the Context of Complex Prenatal Substance Use Policy Environments
Supplemental Material for Substance Use-Associated Infant Maltreatment Report Rates in the Context of Complex Prenatal Substance Use Policy Environments by Haley Stritzel in Child Maltreatment
Footnotes
Author’s Note
The analyses presented in this publication were based on data from the National Child Abuse and Neglect Data System (NCANDS) Child File, FFY 2008-2019. These data were provided by the National Data Archive on Child Abuse and Neglect at Cornell University, and have been used with permission. The data were originally collected under the auspices of the Children’s Bureau. Funding was provided by the Children’s Bureau, Administration on Children, Youth and Families, Administration for Children and Families, U.S. Department of Health and Human Services. The collector of the original data, the funding agency, NDACAN, Cornell University, and the agents or employees of these institutions bear no responsibility for the analyses or interpretations presented here. The information and opinions expressed reflect solely the opinions of the authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author acknowledges the support of grants from the Eunice Kennedy Shriver National Institute of Child Health and Human Development [P2C HD050924; T32HD007168] to the Carolina Population Center and the National Science Foundation [1904311] to the author. Opinions reflect those of the author and not necessarily the opinions of the granting agency.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.