
Abstract
Earlier reviews to discover research on interventions for children after neglect have concluded little was available, despite the well-documented prevalence and harmful effects of neglect on children. We revisited this question through a systematic literature review to discover the state of research on interventions for children who have experienced neglect. We searched MEDLINE, PsycINFO, ERIC, Sociological Abstracts and EMBASE for studies published between 2003 and 2021. Studies were included if neglect could be distinguished, and child outcomes reported. Eight reports describing six studies about six interventions were identified. These studies differed in interventions, age-groups, definitions of neglect, and outcomes. Four studies reported positive child outcomes though with varying degree of quality. More research is needed to inform a coherent theory of change following neglect. There remains an urgent need for research on interventions to help children recover from neglect.
Child neglect is one of the most pervasive forms of maltreatment (e.g., Australian Institute of Health and Welfare, 2022; Fallon et al., 2021; U.S. Department of Health, 2022) and a major public health and human rights issue (Krug et al., 2002). There is substantial evidence of the deleterious effects of child neglect including physical, developmental, emotional, behavioral, and social consequences (Jackson et al., 2022; Maguire et al., 2015; Naughton et al., 2017). This paper is a systematic review on interventions for children who experience difficulties as a result of neglect. It aims to inform ideas for a theory of change to underpin available or emerging interventions applied to this population.
A confounding issue is the lack of agreed definition of neglect (Dubowitz et al., 2005). In this article, neglect refers to when a child’s essential needs are not met (Daniel et al., 2013; Dubowitz, 2009; Frederico et al., 2006). Neglect comes in many forms and its subtypes include physical, emotional, medical, supervisory, educational neglect, and abandonment. Institutional neglect, such as occurred in some Eastern European child institutions in the 1990s, is another subtype involving pervasive physical, emotional, and social deprivation (Nelson et al., 2014). Another complex factor when defining neglect is, despite its strong correlation with poverty, it is recognized as a separate phenomenon (Wald, 2015). Whether it is a causal, contributing, or confounding factor with neglect, poverty can leave its own mark and should be recognized in its own right in interventions with families and children (Tanner & Turney, 2006).
Notwithstanding its prevalence and harms, child neglect continues to elude the level of research undertaken on other types of maltreatment. In particular, there is a dearth of research about whether children recover from the impact of neglect and what interventions might support recovery (Allin et al., 2005; Berry et al., 2003; Daniel et al., 2011; DePanfilis, 2006; Department of Community Services, 2006; Proctor & Dubowitz, 2014; Sesar & Dodaj, 2021; Tanner & Turney, 2006; Taussig et al., 2013). The limited research available is largely focused on the important question of interventions to prevent neglect, yet research has not sufficiently explored interventions that redress the harms already experienced by the child. Taussig et al. (2013) noted: Given the adverse consequences of neglect, one might expect to find several evidence-based interventions aimed at ameliorating the impact of neglect on social and emotional functioning. Unfortunately, few programs were found to demonstrate efficacy for neglected youth. Even rarer are programs that demonstrated efficacy for certain subtypes of neglect, despite different subtypes predicting different symptomatology. (p. 57)
The high frequency and impact of neglect signifies an imperative to prevent and mitigate its consequences. A primary step in intervention following neglect is to safeguard the child from further neglect (Daniel et al., 2011; Horwath, 2013). Horwath (2013) describes several interventions with evidence of effectiveness in working with families to prevent neglect occurring or re-occurring. These include SafeCare® (Gershater-Molko et al., 2002), an enhanced version of Triple P-Positive Parenting Program (Sanders et al., 2004), an enhanced Incredible Years (IY) program (Webster-Stratton & Reid, 2010), and Multisystemic Therapy (MST; Brunk et al., 1987). Horwath (2013) and Daniel et al. (2011) also note children not able to be protected from further neglect within the family home, may be placed by child protective services (CPS) in out-of-home care on a time-limited or permanent basis.
A proposition underpinning this paper is that for all the importance of preventing further neglect by improving economic and social conditions, working with families, or providing alternative care, this is unlikely to sufficiently address existing impacts for children. Although interventions with families, such as those mentioned above, aim to prevent further neglect, most research on these interventions do not report child outcomes. On a positive note, there is substantial research on various interventions for many child-specific problems including biopsychosocial problems associated with neglect. Most of that research, however, does not explore if outcomes differ depending on whether the child experienced neglect. It is not known, therefore, whether existing evidence-based treatments or other approaches are effective with children who experience neglect. The question remains, should knowing the child experienced neglect inform which interventions to use and how they are applied? We contend the answer is yes based on the following premises: 1. Knowing the etiology of the child’s problems informs which mechanisms were at play leading to the problem (Bush et al., 2016). Children who never developed a sleep routine due to neglect, for example, may have a longstanding dysregulated arousal system that differs from children who had a regulated arousal system, and then were exposed to significant stressors or trauma through abuse (Semsar et al., 2021). 2. Mechanisms involved in how neglect leads to certain difficulties can inform mechanisms to target through intervention (Center on the Developing Child, 2016; Lipsey & Pollard, 1989; Perry & Pollard, 1998). Developing sleep routines for children who never had one, for example, requires different interventions than helping children overcome fears of hearing noises in the night. There are existing interventions available for both problems but recognizing the foundation of the problem can inform the optimal choice of intervention (Tinker, 2019). 3. The intrapsychic experience and meaning of neglect for the child can provide an undercurrent for other problems (Naughton et al., 2017). For example, children with difficulties trusting others who believes “no one loves me” has different challenges than children with trust problems who believes “daddy gets angry when he drinks.”
Lipsey and Pollard (1989, p. 31) concept of treatment theory “attempts to describe the process through which an intervention is expected to have effects on a specified target population”. They contend the aim is to define and describe the problem, intervention, mechanisms by which the intervention would impact the problem, and outcomes as precisely as possible. This concept influenced the theory of change approach to designing an intervention or its evaluation (e.g., Astbury & Leeuw, 2010; Funnell & Rogers, 2011).
In 2005, Allin and colleagues undertook a systematic literature review on the treatment of child neglect. Of 697 studies on treatment of neglect, five focused on children; namely, therapeutic child care (Culp et al., 1987), play therapy (Reams & Friedrich, 1994; Udwin, 1983), resilient peer training (Fantuzzo et al., 1996), and MST (Brunk et al., 1987). Allin and colleague’s review concluded there was some limited evidence for positive outcomes for children who had experienced neglect. Most of the studies reviewed did not distinguish outcomes for children who experienced neglect compared to other forms of maltreatment, therefore, it was not possible to ascertain whether the children with positive outcomes were those who experienced neglect.
The only study which separated findings between neglect and other maltreatment was by Brunk et al. (1987). They reported positive findings for children who experienced neglect between MST and the control intervention in terms of changes in parental responses. However, they did not find positive changes in the only child-specific measure used, which was about passive non-compliance. Allin et al. (2005) concluded “effectiveness of treatment for children exposed to neglect alone (i.e., without co-occurring abuse) cannot be determined from the existing literature” (p. 499).
For this systematic review, treatment, therapy, or interventions referred to any effort aimed to help a child achieve positive outcomes in the aftermath of neglect. While interventions may have included or focused on families or other caregivers, results were needed on child outcomes. This review aimed to identify any interventions used to help children recover from the negative sequelae of neglect in any of its forms. It was hoped this would shed light on possible mechanisms leading to recovery and inform a theory of change to support the development and use of interventions.
Method
The search protocol for ‘A systematic review of interventions to help children recover from the impacts of neglect’ was registered under PROSPERO (International Prospective Register of Systematic Reviews – Registration No. CRD42017068362A). It was twice updated on PROSPERO given changing timelines due to the COVID-19 pandemic. This review was part of a Ph.D. study through La Trobe University, with no external funding.
This systematic review was based on an open exploratory design regarding all neglect subtypes, interventions, research-type, or child-focused outcomes. Allin et al. (2005) were similarly inclusive. Though this review, similar to Allin et al., included studies where neglect co-occurred with other forms of maltreatment, this review excluded studies where it was not possible to separate neglect from other maltreatment.
Inclusion and Exclusion Criteria for Systematic Review.
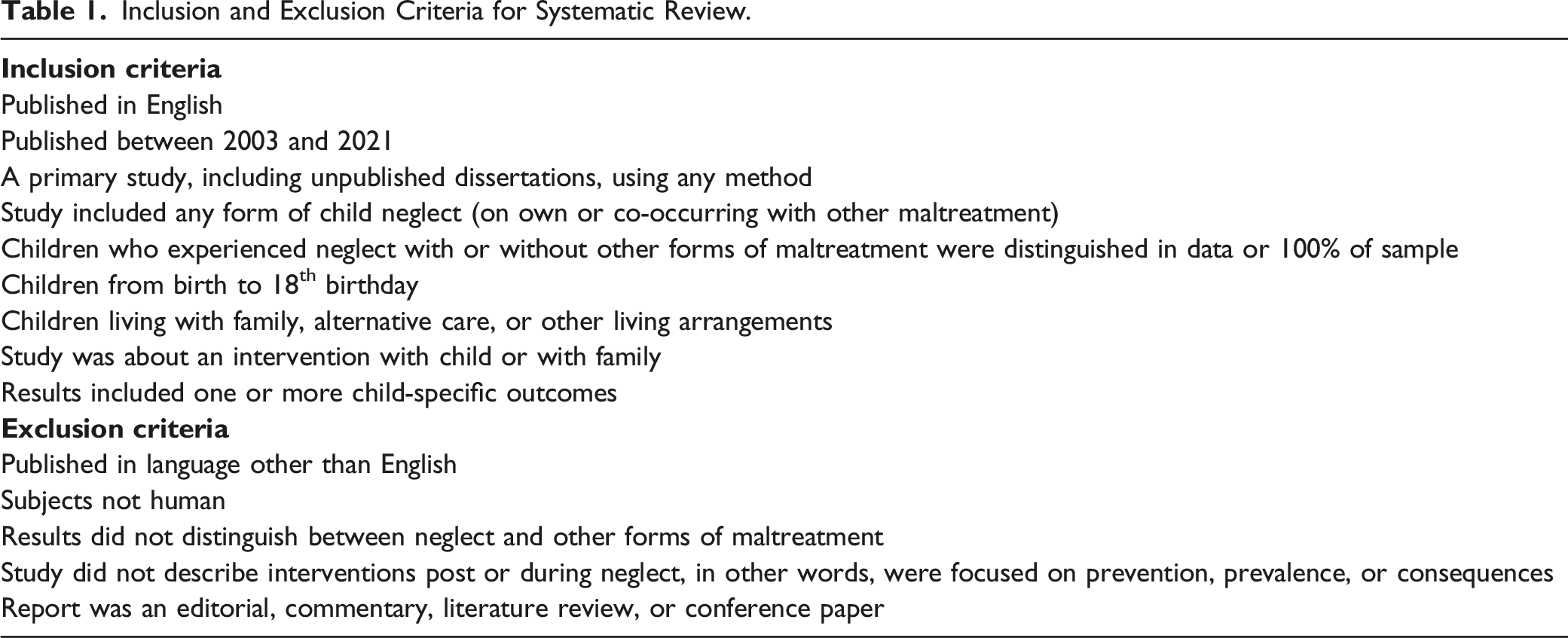
The type or quality of the study was not a reason for exclusion but informed discussion on its implications. There were no apparent conflicts of interest involved in this systematic review. Some articles published by one or more of the reviewers were included in the initial screen but did not meet criteria for inclusion. Multiple reviewers were involved at each stage.
In addition to searching the same databases as Allin et al. (2005), namely Medline, PsycINFO, and ERIC, this review searched Sociological Abstracts and EMBASE. The Cochrane Collaboration and Campbell Review were also reviewed but no studies were identified. Two other records were found separate to the database search. The final database search occurred in May 2022. One record was identified in January 2023.
As Allin et al. (2005) searched for studies from 1980 to May 2003, this review searched from 2003 to 2021. All titles and abstracts retrieved were independently screened by two reviewers, with duplicates removed. Articles that appeared to meet the criteria were read by four reviewers to determine if they met the criteria. A fifth reviewer moderated any disagreement, which occurred in one instance. An Excel spreadsheet was used to track all records, reports and decisions throughout the process. The review team consisted of four experienced social workers as well as a child and adolescent psychiatrist.
This systematic review protocol used PRISMA (Preferred Reporting Items for Systematic review and Meta-Analysis Statement) (Page et al., 2021). Figure 1 shows the flow from 3897 records initially screened, then distilled to 64 reports read in detail. This identified eight reports on six studies about six interventions which met the criteria. PRISMA flow diagram for record search for this systematic review. Note. Categorization of number of articles excluded at either initial screening or eligibility phase is indicative. There were often multiple reasons for excluding an article but only the primary one was listed.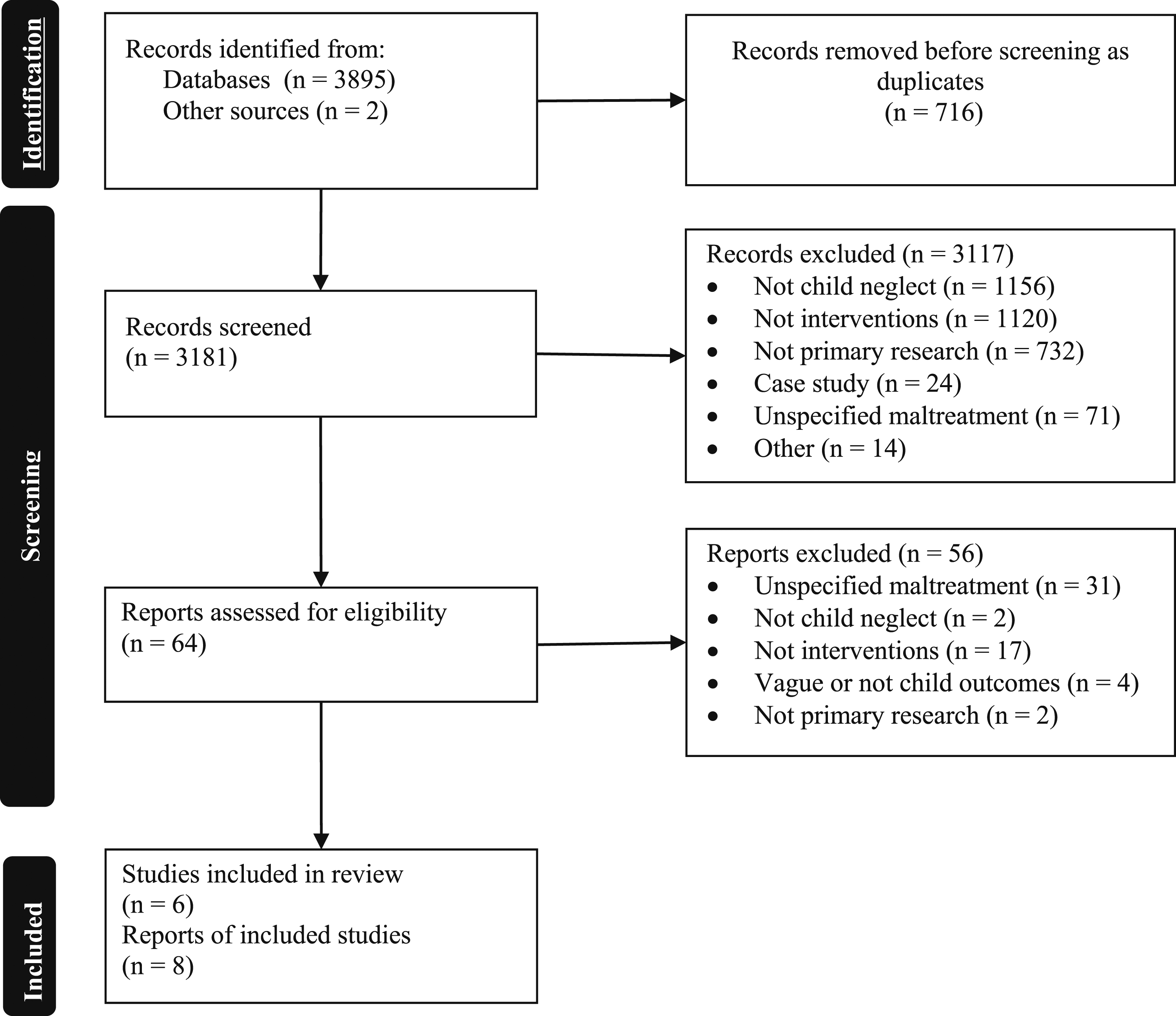
Findings
Many reports in the first screening phase were manifestly unrelated to child neglect and included topics such as clubfoot or tropical diseases. Of the reports on child neglect, a large number focused on prevalence or consequences. Most reports on interventions highlighted parental behavior change with no description of child outcomes. The 64 reports identified as possibly meeting the search criteria are described in a supplementary file. The most common reason for exclusion was a lack of distinction between children who were neglected compared to other maltreatment (71%) experiences.
Description of Studies Deemed to Meet Criteria for Inclusion (n = 8).
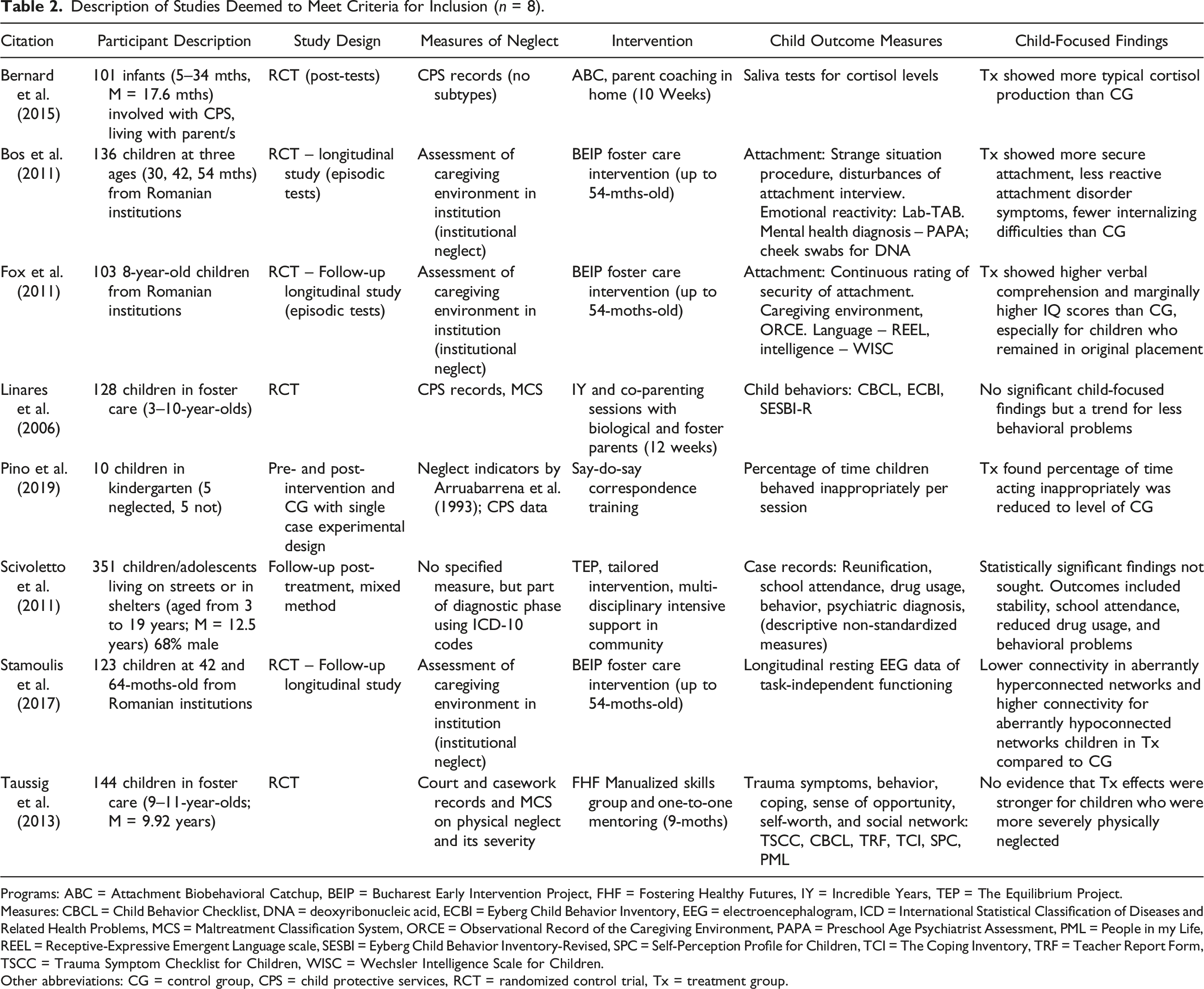
Programs: ABC = Attachment Biobehavioral Catchup, BEIP = Bucharest Early Intervention Project, FHF = Fostering Healthy Futures, IY = Incredible Years, TEP = The Equilibrium Project.
Measures: CBCL = Child Behavior Checklist, DNA = deoxyribonucleic acid, ECBI = Eyberg Child Behavior Inventory, EEG = electroencephalogram, ICD = International Statistical Classification of Diseases and Related Health Problems, MCS = Maltreatment Classification System, ORCE = Observational Record of the Caregiving Environment, PAPA = Preschool Age Psychiatrist Assessment, PML = People in my Life, REEL = Receptive-Expressive Emergent Language scale, SESBI = Eyberg Child Behavior Inventory-Revised, SPC = Self-Perception Profile for Children, TCI = The Coping Inventory, TRF = Teacher Report Form, TSCC = Trauma Symptom Checklist for Children, WISC = Wechsler Intelligence Scale for Children.
Other abbreviations: CG = control group, CPS = child protective services, RCT = randomized control trial, Tx = treatment group.
Bucharest Early Intervention Program (BEIP)
The three reports focused on the BEIP study described different outcomes data from the same randomized control trial (RCT) (Bos et al., 2011; Fox et al., 2011; Stamoulis et al., 2017). This study was strong methodologically utilizing randomization between a treatment and control group, a community comparison group, longitudinal follow-ups, and a variety of standardized measures. The inclusion of these reports on the BEIP study was predicated on the well-documented evidence of extreme social deprivation experienced by children raised in such institutions (Nelson et al., 2014), rather than specific measures denoting the children’s experience of neglect.
In the BEIP study, children from Romanian institutions were randomly assigned to a foster care program in Romania (treatment), or a ‘care as usual’ control group. There was also a never-institutionalized comparison group of children in Romania. Children were under 30-months-old at the beginning of the study. As foster care was scarce in Romania, a program informed by a USA-based model and supplemented by local Romanian knowledge was created. This model emphasized training carers, providing material and emotional support by social workers, and access to specialist input such as pediatricians to assist the children and carers. “This approach, focused on providing enhanced experiences for the child, made the [foster] parent-child relationship the central component of the intervention, in keeping with contemporary research and practice” (Nelson et al., 2014, p. 102). The intervention phase concluded when the child reached 54-months-old and their placement was transferred to local Romanian services, as foster care had become more established. Although the intervention phase ceased, the child’s placement did not, and neither did the study (Nelson et al., 2014). The control group were children whose planning was not influenced by the study and who were either placed in a different foster care program, reunited with family, or remained in the institution.
Findings from Report 1
Bos et al. (2011) reported on the findings regarding 136 children’s mental health assessed at baseline and then at 30-, 42-, and 54-months of age. In follow-up assessments, children in the BEIP treatment group were more likely than the control group to demonstrate secure attachments and showed fewer symptoms consistent with reactive attachment disorder. The treatment group also showed greater positive affect and fewer internalizing symptoms, although no significant difference was found for externalizing symptoms.
Findings from Report 2
Fox et al. (2011) continued the analysis on a reduced sample of 103 children due to attrition, with a focus on cognitive intelligence, including follow-up when the children were eight-years-old. There was a consistent pattern of children in the treatment group having higher sub-scale scores in the Wechsler Intelligence Scale for Children–IV (WISC–IV; Wechsler, 2003) compared to the control group, noting that verbal comprehension was the only scale with significant difference. Fox and colleagues found children placed in the BEIP foster care intervention before 26-months-old were more likely to show higher cognitive scores. Further analysis indicated one of the mediating variables was security of attachment at 42-months-old and that children placed in the treatment group before 26-months-old were more likely to have age-typical intelligence.
Findings from Report 3
Stamoulis et al. (2017) described the findings of brain electrical activity of children at ages 42- and 96-months examining task-independent brain networks. These are neural networks activated when a person is not undertaking a task, such as when their eyes are closed. These assessments were undertaken using a resting-state electroencephalogram (EEG). The study identified two aberrantly connected neural networks for children in the treatment and control groups compared to the never-institutionalized group, particularly at 96-months-old. They found children in the control group were more atypical than those in the treatment group, suggesting the BEIP foster care program had some positive impact. The impacted parieto-occipital gamma network and the frontotemporal network are involved in cognitive functioning, such as memory, visual-motor learning, visual processing, social communication, and language.
Attachment and Biobehavioral Catchup (ABC)
As part of a larger RCT on the ABC model with children who experienced abuse and neglect, Bernard et al. (2015) focused on neglected children. Infants and their parents were randomly assigned into either the ABC treatment group or the control group using Developmental Education for Families (DEF).
The ABC intervention consisted of 10 weekly home-based sessions by coaches with parents using techniques such as observation, in-the-moment feedback, and replaying footage of parent-child interactions to assist parents’ reflection. Sessions followed a sequence beginning with assessing parents’ beliefs and behaviors and alerting them to signals from their child to elicit nurturing responses. Parents were coached to be responsive, follow the child’s lead and to interact in a non-frightening and non-intrusive manner. There was also exploration of how the parents’ childhood may influence their parenting. The DEF model for the control group used a similar timeframe in home visits during which, parents were taught about child development (Bernard et al., 2015).
Bernard and colleague’s (2015) study was informed by research, such as by Gunnar et al. (2001), who found children who experienced neglect had atypical patterns of cortisol suggesting biological dysregulation. Bernard and colleagues studied 101 infants across the ABC and DEF groups ranging from five to 34-months-old and their parents at post-intervention. The children were living with parents and were referred by CPS due to concerns about neglect. Although this study did not test pre- and post-cortisol levels, the researchers had undertaken pre-tests on a subset from the ABC and DEF groups and found no significant differences before the intervention.
Bernard et al. (2015) found children in the ABC intervention were more likely to have a closer to typical cortisol pattern when they awoke showing a medium effect size; and, as it changed throughout the day, to a small to moderate effect size, compared to the DEF group. They concluded “an intervention designed to enhance synchronous and nurturing parenting, even under chronically challenging conditions, may support children’s cortisol regulation” (Bernard et al., 2015, p. 838).
The Equilibrium Project (TEP)
Scivoletto et al. (2011) used mixed methodology over 2 years. The participants were 351 children and adolescents who had experienced many adversities––all experienced neglect. TEP was developed through a community and academic partnership with children and adolescents who lived on the streets or in group shelters in São Paulo, Brazil.
TEP aimed to make intensive professional services accessible within the community and associated with recreational activities. It was located in a safe setting away from adverse environmental elements and provided supported access to other resources. Participants were referred by group shelter staff or via the Children’s Court as an alternative to custodial sentences. Participation was voluntary. The project’s main goals were to decrease children and adolescents’ symptomatology, promote education and social development, and “ultimately enable social and family reintegration” (Scivoletto et al., 2012, p. 4).
Eligible participants underwent a screening, followed by a multidisciplinary assessment, including a psychiatric assessment. An individualized intervention plan was tailored to meet the child or adolescent’s needs as well as those of their family. Clinical services included psychiatric treatment, individual or group psychotherapy, art therapy, family psychotherapy, occupational therapy, and speech therapy. Recreational activities included theatre and sports activities. The plan was implemented through assertive case management. The case manager aimed to develop a therapeutic alliance with each child and adolescent, and where possible, their family. Although choices of interventions were led by the child and adolescent and adapted to their situation, there was a foundational focus on communication skills (Scivoletto et al., 2011, 2012).
Scivoletto et al. (2011) did not provide statistically significant findings relating to the outcomes of interventions. There were no pre- and post-test results nor was there a comparison or control group. The preliminary results of the study noted 63.5% of participants had successfully completed the program or were continuing to participate. Of the 122 children and adolescents who reunited with their families, 68.3% were described as “stable, attending to school, without drug use or any behavior problems and had been living with their families for more than 6 months” (Scivoletto et al., 2011, p. 92).
Fostering Healthy Futures (FHF)
Before describing their study, Taussig et al. (2013) offered a useful description of the dilemmas in exploring the effectiveness of interventions with children who experienced neglect. With these in mind, they examined the effectiveness of FHF using the severity of neglect as an independent variable. Having previously demonstrated FHF to result in positive effects (Taussig & Culhane, 2010), they wanted to see if it had a greater effect for children exposed to more serious physical neglect.
FHF was a 9-month intervention of a skills group and mentoring for pre-adolescent children living in foster care. The skills groups aimed to bring children in foster care together to reduce stigma and learn social skills. It followed a manualized curriculum involving cognitive-behavioral skills group activities and process-oriented material. Topics included emotional recognition, perspective-taking, problem-solving, anger management, cultural identity, change and loss, healthy relationships, peer pressure, and abuse prevention. The group intervention was informed by evidence-based skills programs such as Promoting Alternative Thinking Strategies (Kusché & Greenberg, 1994) and Second Step (Committee for Children, 2001).
The mentoring component occurred over the same period as the skills group, involving individual time with a mentor and child. Mentors received weekly supervision as well as training. The mentor roles aimed to support children by: (1) creating empowering relationships as positive examples for future relationships; (2) ensuring they received services in multiple domains; (3) helping them generalize and adapt skills learned in the group to their own world through weekly activities; (4) engaging them in extracurricular, educational, social, cultural, and recreational activities; and (5) promoting their positive future orientation.
To determine the presence and severity of physical neglect, legal and casework documents from CPS were coded using the Maltreatment Classification System (MCS; Barnett et al., 1993). According to the MCS, 47.2% of the children had experienced physical neglect. The study collected data at the baseline interview (2 months prior to intervention). Data collected at Time 3 (6 months post-intervention) included interviews with children, caregivers, and teachers (Taussig et al., 2013). The hypothesis that FHF would be most effective for children who experienced more severe neglect was not supported with the outcomes measured, such as mental health, coping, social acceptance, and self-worth. In other words, the effectiveness of FHF with children who experienced neglect, especially severe neglect, was not proven.
Incredible Years (IY) and Collaborative Co-Parenting
Linares et al. (2006) undertook a prevention trial for children at high risk for externalizing problems. The intervention was a combination of the IY program (Webster-Stratton, 2001) and a collaborative co-parenting initiative involving biological and foster parents. Children did not directly participate in the intervention, but child outcomes were measured.
The group program was delivered in two-hour weekly sessions for 12 weeks. Topics covered were play, praise and rewards, effective limit setting, and responding to misbehavior. Strategies included videotaped vignettes, role plays, and homework. Each group consisted of four to seven biological and foster parent pairs. The same facilitator ran a session for the individual biological and foster parent pair, focusing on co-parenting. The session aimed for participants to learn about each other and the child, develop open communication, and better negotiate potential areas of conflict. It also included family systems strategies. There was training, supervision, and implementation support for the facilitators and monitoring of fidelity of the intervention.
Sixty-four biological and foster parent pairs participated and were randomly assigned to an intervention (n = 40 pairs) or care as usual control group (n = 24 pairs). To be eligible, children in foster care had substantiated child maltreatment and a plan of family reunification. Most of the children in the overall study (83%) had experienced neglect, although this was less (71%) in the intervention group. Because of this difference, analyses were run for the entire sample and then re-run for children subjected to neglect. The analysis showed no difference and the results were considered applicable for children who experienced neglect. The biological and foster parent pairs were assessed at baseline, 3 months later, and then 3 months after the 12-week intervention ceased. Children ranged between three and 10-years-old and had, on average, been in foster care for 8.4 months at baseline. The IY-adapted intervention group showed more positive results than the control group on positive discipline, clear expectations, co-parenting flexibility, co-parenting problem solving, and co-parenting. Children in the intervention group were reported as having fewer behavioral problems, but these were not significant.
Say-Do-Say Correspondence Training
Pino et al. (2019) applied a form of Say-Do-Say Correspondence Training in a Spanish kindergarten with five children who experienced neglect and compared them to a control group of five children who had not experienced neglect and did not receive the intervention. The two groups were matched by age, gender, social class, and their mothers’ age. Children who had experienced neglect averaged 12 months behind their expected level, at baseline, compared to children in the control group who were 5 months ahead of their expected level. The hypothesis was that children trained in Say-Do-Say would improve their behaviors.
The Say-Do-Say Correspondence Training is a form of behavioral modification known as correspondence or saying-doing training (Di Cola & Clayton, 2017). Typically, the say-do sequence involves participants saying they will do a certain action and receiving reinforcement upon undertaking that action. This is generalized to other actions so when they promise to perform a behavior, they are more likely to do that behavior (Bevill-Davis et al., 2004). They are later asked if they did the action they had promised to do.
Pino et al. (2019) conducted this study in three stages. At baseline, researchers observed the presence or absence of three behaviors of the 10 children over 10 sessions. These behaviors were standing up when they should be sitting, being absent in terms of attention to the activity, and disruptive behavior such as fighting, shouting or disturbing other children. The second stage involved each child in the intervention group participating in an individual session with a psychologist outside the classroom. The psychologist (researcher) used the Say-Do-Say Correspondence Training with each child for a simple behavior, and then generalized this to two other simple behaviors. Positive reinforcements were part of the intervention. The training occurred in 10–15 minute sessions over 2 days until each child complied with the initial behavior and demonstrated they had generalized this to two other activities. Stage 3 was implemented by the teacher within the classroom. The teacher used similar training to what had been provided by the psychologist, but in a group setting for all 10 children, gradually withdrawing the level of reinforcement. The time period for the intervention used by Pino et al. (2019) was unclear but appeared to be within 2 weeks.
Pino et al. (2019) measured neglect through a measure developed in Spain that included physical, medical, supervisory and educational neglect (Arruabarrena et al., 1993). Information to complete this measure was gathered from CPS who were involved with the children’s families. It appears all children were in their parents’ care.
Pino et al. (2019) reported there was “a drastic reduction” (p. 7) observed for the five children in the intervention group in percentage of time spent using inappropriate behavior. The time spent in disruptive behavior became similar to those in the control group. Children in the control group, maintained their baseline levels of behavior. The number of participants was too small to measure statistical significance. Pino et al. remarked this study provided preliminary support for an intervention that could be easily used by teachers with children who have experienced neglect.
Discussion
Aligned with Allin and colleagues’ (2005) earlier systematic review, this review posed the question: What interventions are used with children who have experienced neglect? The answer is very few, or at least very few studies of interventions that reported child outcomes. Of the four out of six interventions in this systematic review where positive outcomes for children were found, one was a foster care intervention for children from Romanian institutions (Bos et al., 2011; Fox et al., 2011; Stamoulis et al., 2017), one was an attachment-based intervention, (Bernard et al., 2015), one was a community-based intervention (Scivoletto et al., 2011), and one was a kindergarten-based behavioral modification intervention. Of note is the study by Taussig et al. (2013) which commendably published results when their hypotheses were not proven, which occurs too infrequently (see Lederman & Lederman, 2016).
The studies in this systematic review ranged in sample size from 10 children (Pino et al., 2019) to 351 (Scivoletto et al., 2011). Most of the reports discussed limitations with sample size in terms of statistical power. With the exception of Pino et al. (2019) all sample sizes were larger than studies described by Allin et al. (2005). The study by Scivoletto et al. (2011) had the largest sample but did not describe their methodology. The study’s intent to integrate research in a community-based practice model with a rarely studied population of homeless children, involving a combined clinical and community intervention occurring ‘in the streets’, is laudable. This type of research is important to contribute new information to the broader field; however, it was considered weaker methodologically than the other studies due to insufficient description of its method and scant information on outcomes (quantitative and qualitative).
Seven of the eight reports described various limitations of their study. In the ABC study, Bernard et al. (2015) noted the lack of a comparison group and that they did not routinely collect cortisol before the intervention. They also described variation in the length of time (one to 12 months) when cortisol was collected post-intervention. Taussig et al. (2013) and Linares et al. (2006) described the need to increase their sources of data. Taussig and colleagues noted this in terms of coding maltreatment, whereas they used a variety of self and other report measures for children’s mental health functioning. Linares et al. (2006) discussed the value of moving beyond parent self-report data for future studies. Each report on the BEIP study described limitations relating to certain measures and provided relevant cautions. For this systematic review, the BEIP study was found to be limited due to its minimal description of neglect and of the foster care intervention which could impede the application of the findings to other settings. The study by Pino et al. (2019) was acknowledged by the authors to have a very small sample size and was non-randomized, both limiting its generalizability.
Neglect is difficult to define and measure for the purposes of research (Allin et al., 2005). The least defined description of neglect was by Scivoletto et al. (2011). Although they used the International Statistical Classification of Diseases and Related Health Problems (ICD-10) (World Health Organization, 2016) coding system for assessing neglect, it was unclear how neglect was distinguished from the extreme poverty experienced by this population (Scivoletto et al., 2012). There was no attempt to describe the neglect or use any validation approach. Two studies used the MCS for coding CPS records (Linares et al., 2006; Taussig et al., 2013). Although the MCS includes four neglect subtypes, it does not distinguish emotional neglect from emotional abuse. Bernard et al. (2015) noted while their definition of neglect was informed by CPS records, they could not access detailed records. Their description of neglect is, therefore, vague and homogenous, although validated by CPS as an external authority. The measure of neglect used by Pino et al. (2019) was completed by incorporating information from CPS. They articulated the most neglect subtypes compared to the other studies, although they were grouped together as one construct (Arruabarrena et al., 1993). Scivoletto et al. (2011) described neglect as a single construct. Taussig et al. (2013), however, cautioned when neglect subtypes are collapsed there can be confounding findings. A lack of specificity on which essential needs of the child were not met (i.e., what neglect subtype was the focus of study) is a key limitation for applying the findings in practice.
The frequent co-occurrence of neglect with other types of maltreatment is a major complicating factor when researching neglect (Allin et al., 2005; Widom, 2013). The reports on BEIP (Bos et al., 2011; Fox et al., 2011; Stamoulis et al., 2017), ABC (Bernard et al., 2015), Say-Do-Say Correspondence Training (Pino et al., 2019) and TEP (Scivoletto et al., 2011) noted 100% of their treatment population experienced neglect. Pino et al. (2019) was the only study that contended the children did not experience other maltreatment. In recognition of the difficulties in research on neglect, due to its common co-occurrence with other maltreatment, Taussig et al. (2013) examined whether FHF had greater effect for children exposed to more serious physical neglect. Their definition of exposure to physical neglect was limited to neglect that occurred in the previous 2 years due to data quality concerns associated with a longer time period. Given the potentially harmful impacts of physical or other forms of neglect occurring for younger children (Becerra, 2016), this was a limitation of the design.
In considering the risk of bias, all six interventions were developed in part or entirely by members of the study teams. The four studies that utilized RCT methodology had documented processes of randomization and followed intent-to-treat analyses and used independent raters and inter-relator reliability for the measures. The researchers who undertook the observations in the study by Pino et al. (2019), were rotated through the intervention and control group. The study by Scivoletto et al. (2011) was the one most susceptible to claims of bias with no apparent attempt to reduce those reported.
Descriptions of Interventions in this Systematic Review.
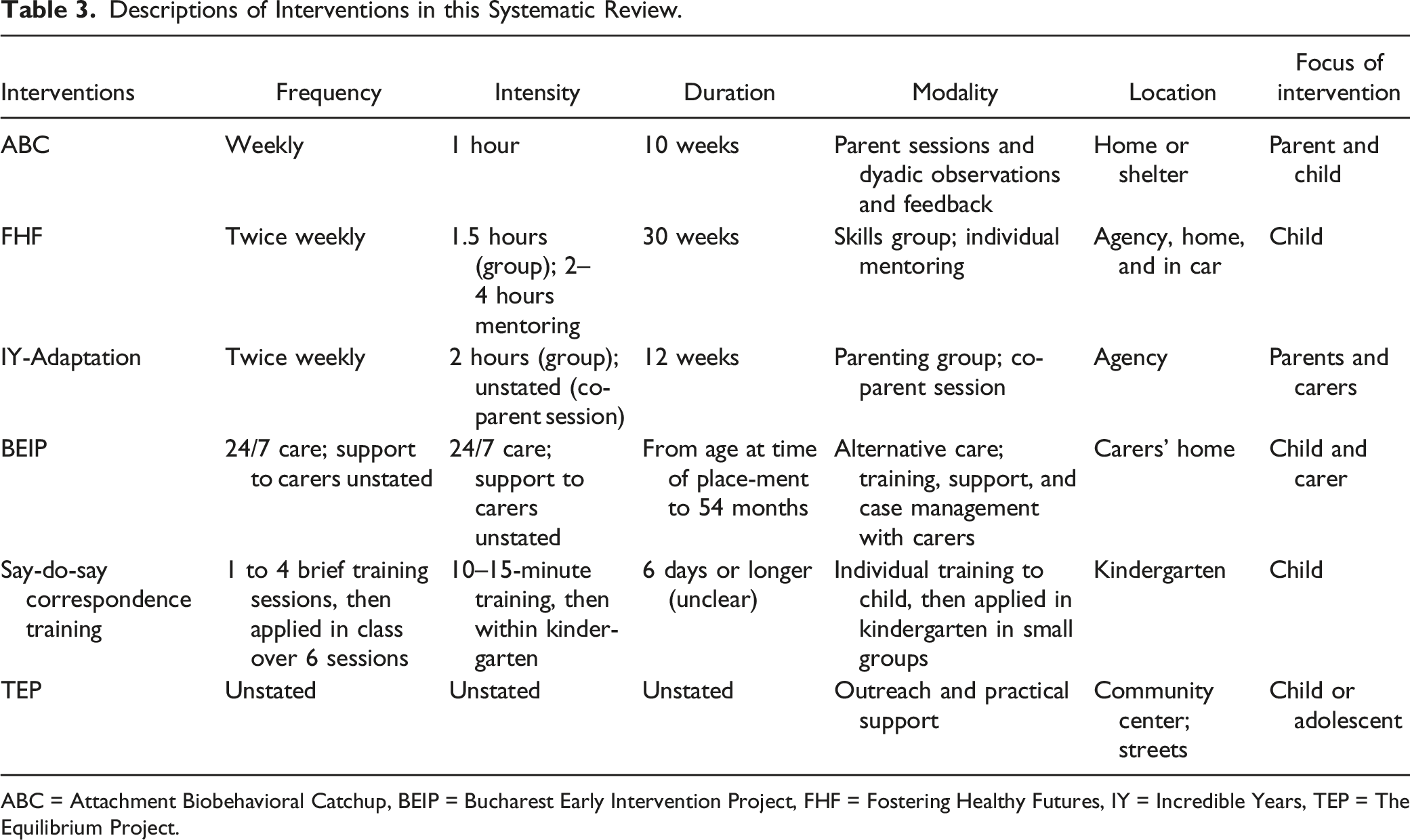
ABC = Attachment Biobehavioral Catchup, BEIP = Bucharest Early Intervention Project, FHF = Fostering Healthy Futures, IY = Incredible Years, TEP = The Equilibrium Project.
The Say-Do-Say Correspondence Training (Pino et al., 2019) was the shortest intervention in duration of approximately 2 weeks. Other intervention durations were 10 weeks, nine months, up to 48 months, to an unspecified amount of time. Some were direct interventions with the child (Pino et al., 2019; Scivoletto et al., 2011; Taussig et al., 2013), and others were interventions with the parents with the intent to impact child outcomes (Bernard et al., 2015; Linares et al., 2006). The other category was interventions providing alternative care for the child with a focus on supporting the carers, namely the BEIP intervention (Bos et al., 2011; Fox et al., 2011; Stamoulis et al., 2017). The IY-adapted intervention involved both parents and foster parents (Linares et al., 2006). The modality of interventions varied from providing supported alternative care to individual or group sessions. TEP, FHF, and BEIP incorporated case management and referrals to other services.
Outcomes measured for these interventions included neurobiological outcomes, such as cortisol levels (Bernard et al., 2015) and neural connectivity (Stamoulis et al., 2017); cognitive and language development (Fox et al., 2011); security of attachment (Bos et al., 2011); trauma symptoms (Taussig et al., 2013); and behavioral problems (Linares et al., 2006; Pino et al., 2019; Scivoletto et al., 2011; Taussig et al., 2013).
BEIP was the only intervention purposefully designed for children subjected to neglect, albeit a particular type of neglect. This was also the only intervention predicated on the notion of ceasing the children’s exposure to neglect by removing them from a harmful situation. FHF was implemented with children already placed in care, but this was not described as part of the intervention. Although not designed explicitly for neglect, both the IY-adaptation and ABC incorporated goals of enhancing the children’s situation at home in order to meet their needs and, at the same time, ensure they were not neglected.
Theory of Change
For each intervention, other than TEP, there was a body of literature articulating the underlying theory of change. The articles on BEIP, ABC, and FHF proposed potential mechanisms for recovery and a theory of change for children who experience neglect. Bos et al. (2011) and Fox et al. (2011) reported on the essence of the BEIP foster care model demonstrating the value of stable enriched environments and secure attachments as key features toward positive outcomes for children. This appears to be their core theory of change for ameliorating harms from institutional neglect (see Nelson et al., 2014).
The ABC intervention aimed to influence parenting behaviors that promote biological regulation for young children. These parental behaviors include being synchronous with the child’s signals, providing a nurturing response when the child is distressed, and not frightening them. Their theory of change suggests children may develop a sense of control over their environment and become more biologically and behaviorally regulated. Cortisol levels are a measure of biological regulation. Bernard et al. (2015) acknowledged their study did not test this mechanism as they did not examine the ways “parenting behaviors change, and how they may contribute to changes in child outcome” (p. 837).
Taussig et al. (2013) proposed that FHF may be beneficial for children who have experienced neglect to “ameliorate gaps in their upbringing, for example, by modeling healthy relationships, exposing children to enriching activities, and teaching children social skills” (Taussig et al., 2013, p. 57). This is consistent with Perry’s (2008) neurobiological definition of neglect as “the absence of an experience or pattern of experiences required to express an underlying genetic potential in a key developing neural system” (p. 94). This definition suggests a theory of change incorporate sufficient dose and pattern of experiences required to express the potential for children’s developing neural systems.
The theory of change for the Say-Do-Say Correspondence Training aimed to modify nonverbal behaviors by changes in verbal behaviors (Bevill-Davis et al., 2004). The literature review on correspondence training by Bevill-Davis et al. noted three key conditions consistent with principles underpinning behavioral modification: (1) prompting children to say they would do the behaviour and then giving them the opportunity to follow through; (2) reinforcing content where children are supported in their intent to do the behavior, whether or not they do so; and (3) reinforcement of correspondence, where reinforcement is contingent on engaging in the behavior. This last condition was considered the most necessary. The theory behind providing individual sessions for each child prior to the group session, was informed by the children’s additional needs due to their young age and developmental delays as a result of neglect (Pino et al., 2019). It is possible that the one-to-one interaction over 2 days between the child and psychologist may also be part of the mechanism for change.
This systematic review offers considerations for a theory of change to support children’s recovery from neglect, but these would need to be tested with different populations. An underlying theme for most interventions was the children’s experience of neglect had ceased, and their needs were being met, whether through guiding parents or other caregivers to meet the child’s needs, supporting the child in alternative care, or both. An aspect not explicitly covered in these studies, but related to this theme, is assessing what the child had missed in terms of developmental, relational, and other opportunities, and planning how to elevate the child’s exposure to these previously absent experiences (Perry, 2008). The closest to describing a tailored approach informed by assessment was by Scivoletto et al. (2011), which did not include detailed outcomes.
The exception to the premise of ceasing the neglect, was the Say-do-Say Correspondence Training. Pino et al. (2019) posited “in spite of the significantly delayed development these children displayed (associated with their situation of neglect), they can be treated and their behavior at school improved, with no need for any other change agent except their teacher” (p. 9). This intervention was considered by Pino et al. to be effective, apparently regardless of whether the children were still subjected to neglect. Amongst other differences, this illustrates the outcome was narrowed to reduce disruption in the classroom, rather than broader outcomes on the children’s wellbeing.
The paucity of studies demonstrating interventions to support children’s recovery from neglect meant elements of a comprehensive theory of change were limited. The sequencing of interventions was implied in some interventions but not explicitly discussed. The ABC model, IY-adaptation, and FHF incorporated sequencing of what should be covered in the intervention. Their modality of intervention, however, remained the same throughout. In contrast, the TEP model appeared to provide a more tailored response to the changing needs of children and young people. This concept of sequencing is a core construct of the trauma literature, such as the importance of ensuring safety before working to integrate the person’s trauma experiences (Herman, 1992), and is a hallmark of neurodevelopmental literature including recovery from neglect (Perry & Pollard, 1998).
Limitations
This systemic literature review did not attempt a rigorous examination of the risk of bias or quality of the method due to the focus on open enquiry. The study by Scivoletto et al. (2011) would have typically been excluded in a systematic review where the emphasis was on the type of research. Yet too many populations and types of interventions are omitted from further analysis and dissemination unless a more open enquiry approach is adopted. Only five databases were searched, and other information sources were limited. It is possible more studies on additional interventions could have been sourced through other means such as reviewing reference lists.
Conclusion
We need to approach this question on how to help children recover from the impact of neglect from several angles. Any intervention design with articulated theories of change for children who have experienced neglect, should be informed by the nature of the neglect. Whether they have experienced other forms of maltreatment, the question should include: How has neglect, in any form, impacted these children and what could support their recovery? One of the strengths of the BEIP studies is their continued exploration of multiple lines of inquiry on cognitive, relational, physical, and neurodevelopmental implications, rather than selecting one area of interest. Neglect, in all its heterogeneity, requires research to follow multiple leads from biopsychosocial, cultural, and ecological-systems perspectives.
There is the ubiquitous call for more research, however, the research needs to be expanded rather than just replicated. Those researching interventions need to consider methodological ways of distinguishing between different maltreatment experiences, including neglect and its subtypes. The scarcity of publications on interventions with children who experienced neglect is partly due to this lack of distinction. Many programs refer to their cohort of children as having experienced abuse and neglect as if this is one phenomenon. Hopefully, beneficial interventions exist which, with further research, can be more intentionally applied to help children recover from the aftermath of neglect. It is also hoped that research on neglect will lead to further efforts to develop new interventions for these children, building on strong and coherent theoretical and practice foundations.
Supplemental Material
Supplemental Material - Interventions to Support Children’s Recovery From Neglect—A Systematic Review
Supplemental Material for Interventions to Support Children’s Recovery From Neglect—A Systematic Review by A. L. Jackson, M. Frederico, H. Cleak, and B. D. Perry in Child Maltreatment
Footnotes
Acknowledgments
We are grateful for the contribution of Julie English as an independent reviewer.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.