
Abstract
Child maltreatment is associated with substance use beginning in adolescence and throughout early adulthood. Substance use disorders (SUD) are most likely to develop during emerging adulthood (18–25 years old). Thus, to develop effective substance use prevention strategies, it is useful to know the ages at which associations between maltreatment exposure (prior to age 18) and SUD are most strongly tied. This study examined the age-varying association between child maltreatment and past-year SUD in emerging adulthood by sex and by maltreatment type using time-varying effect models (TVEM). Data were from the National Epidemiological Survey on Alcohol and Related Conditions (NESARC-III). The analytic sample consisted of 5194 emerging adults. The association was strongest at younger ages, with individuals who experienced child maltreatment having three times greater odds of reporting SUD in the past-year. Differential associations were found by sex, racial-ethnic group, and maltreatment type across age. Prevention efforts may be more effective if their development is informed by these important differences and targeted at emerging adults rather than adolescents.
Introduction
Child maltreatment is estimated to affect 40% of youth before age 18 in the United States (Kim et al., 2017a) and has a lifetime economic burden estimated to exceed $428 billion (Peterson et al., 2018). Child maltreatment – defined herein to include physical or sexual abuse, emotional or physical neglect– is associated with myriad long-term consequences (Chapman et al., 2007; Gilbert et al., 2009; Toth & Manly, 2019), including substance use (Cicchetti & Handley, 2019). Among those with a history of child maltreatment, the odds of experiencing substance use disorder (SUD) are significantly higher among men and women (Afifi et al., 2012). Specifically, the likelihood of engaging in illicit drug use is two to four times higher compared to those with no history (Dube et al., 2003). One study found a significant association between any childhood abuse with prescription opioid use in the prior 4 weeks (Austin et al., 2018). Prior literature has focused on the relationship between child maltreatment and initiation of substance use in adolescence, or ages 12–18 (Halpern et al., 2018b; Hovdestad et al., 2011; Tonmyr et al., 2010). To some extent, substance use is normative adolescent development (Spear, 2000); however, it is during emerging adulthood, defined as the ages of 18–25, that substance use and use disorders peak (Arnett, 2000; Center for Behavioral Health Statistics and Quality, 2016).
As the focus has been on preventing substance use initiation in adolescence, the relationship between child maltreatment exposure and SUD in emerging adulthood is not well understood. Additionally, current understanding is largely drawn from retrospective or cross-sectional studies. It is unclear how the relationship between child maltreatment and SUD might vary across the emerging adulthood developmental period. The current study innovatively used nationally representative, non-child welfare data and time-varying effect modeling (TVEM), a statistical technique that can flexibly model associations across continuous age or time, to explore the relationship between child maltreatment and SUD in emerging adulthood.
Emerging Adulthood (18- to 25- Years Old)
The 2020 National Survey on Drug Use and Health indicates that 37% of emerging adults reported illicit drug use and 24% (or 8.2 million people) met criteria for a SUD in the past year (Substance Abuse and Mental Health Services Administration, 2021). At this age many emerging adults leave home for the first time and are learning to become independent and exploring their identity (Arnett, 2005). It is also during this age when drugs and addictive substances are more easily accessible (Sussman & Arnett, 2014a). Emerging adulthood is a particularly important point of intervention because this developmental stage sets the stage for later adult development (Arnett, 2000; 2005; Bergman et al., 2016).
Individuals who have experienced child maltreatment may be at even higher vulnerability for disordered use during emerging adulthood. For example, in one study using data from the Longitudinal Studies of Child Abuse and Neglect, those who experienced physical abuse prior to age 12 were significantly more likely to report alcohol use disorder (AUD) in early adulthood (Dubowitz et al., 2021). Given the high co-occurrence of maltreatment (Kim et al., 2017b), a different study examined patterns of maltreatment and found heightened SUD in emerging adulthood among those with any exposure prior to age 18 (Guastaferro & Bray, 2020). It remains unknown however how risk for SUD varies throughout the emerging adulthood developmental period.
The Need to Understand Time-varying Effects
The development of SUD over time is complex and seldom linear. Modeling the development of SUD across time (or a developmental age period) can inform opportunities for prevention and targeted intervention strategies. Time-varying effect modeling (TVEM), an extension of linear regression, allows the research question to move from “is there a relationship between child maltreatment and SUD” to “what is the relationship between child maltreatment and SUD across emerging adulthood” (Lanza & Linden-Carmichael, 2021). Bayly et al. (2021) used TVEM to model the relationship between maltreatment and heavy episodic drinking between adolescence and young adulthood using data from the National Longitudinal Study of Adolescent to Adult Health. Findings suggested that risk for frequent heavy episodic drinking varied by age; for example, the age at highest risk among those who experienced neglect was around age 21 whereas the age at highest risk among those who experienced physical abuse was 27 (Bayly et al., 2021). The present analysis adds to the burgeoning literature base of time-varying substance use by focusing specifically on SUD in a child maltreatment exposed population.
Given the high prevalence of SUD in emerging adulthood specifically, it is important to understand this relationship throughout the emerging adulthood developmental period. The current study used TVEM to answer three research questions (RQs):
How does the cross-sectional association between child maltreatment and past-year SUD covary across emerging adulthood?
How does this association differ by sex and racial-ethnic group?
How does this association differ based on child maltreatment type? Using data from the 2012 to 2013 National Epidemiologic Survey on Alcohol and Related Conditions-III (NESARC-III; Grant et al., 2014), the current study leverages longitudinal panel data in which child maltreatment was not the phenomenon of interest. Findings may provide an important step in developing prevention strategies to mitigate one of the most prevalent and deleterious consequences of child maltreatment (Dube et al., 2003).
Method
Participants and Procedure
NESARC-III is a nationally representative sample of 36,309 noninstitutionalized U.S. adults. Multistage probability sampling was used to select respondents and higher selection probabilities were assigned to Hispanic, Black, and Asian adults than non-Hispanic white adults. Data were adjusted for oversampling and nonresponse, then weighted to represent the US population at the time of data collection. The target population for NESARC-III included U.S. adults (ages 18+) who resided in households or noninstitutionalized group quarters. Adults were randomly selected within this population. Face-to-face interviews were conducted between April 2012 and June 2013. The panel survey included elements related to alcohol and drug use disorders, risk factors (including exposure to child maltreatment), and associated physical or mental disabilities (Grant et al., 2014). Participants were compensated $90 for their time. The survey protocol was approved by the institutional review board of the National Institutes of Health and Westat.
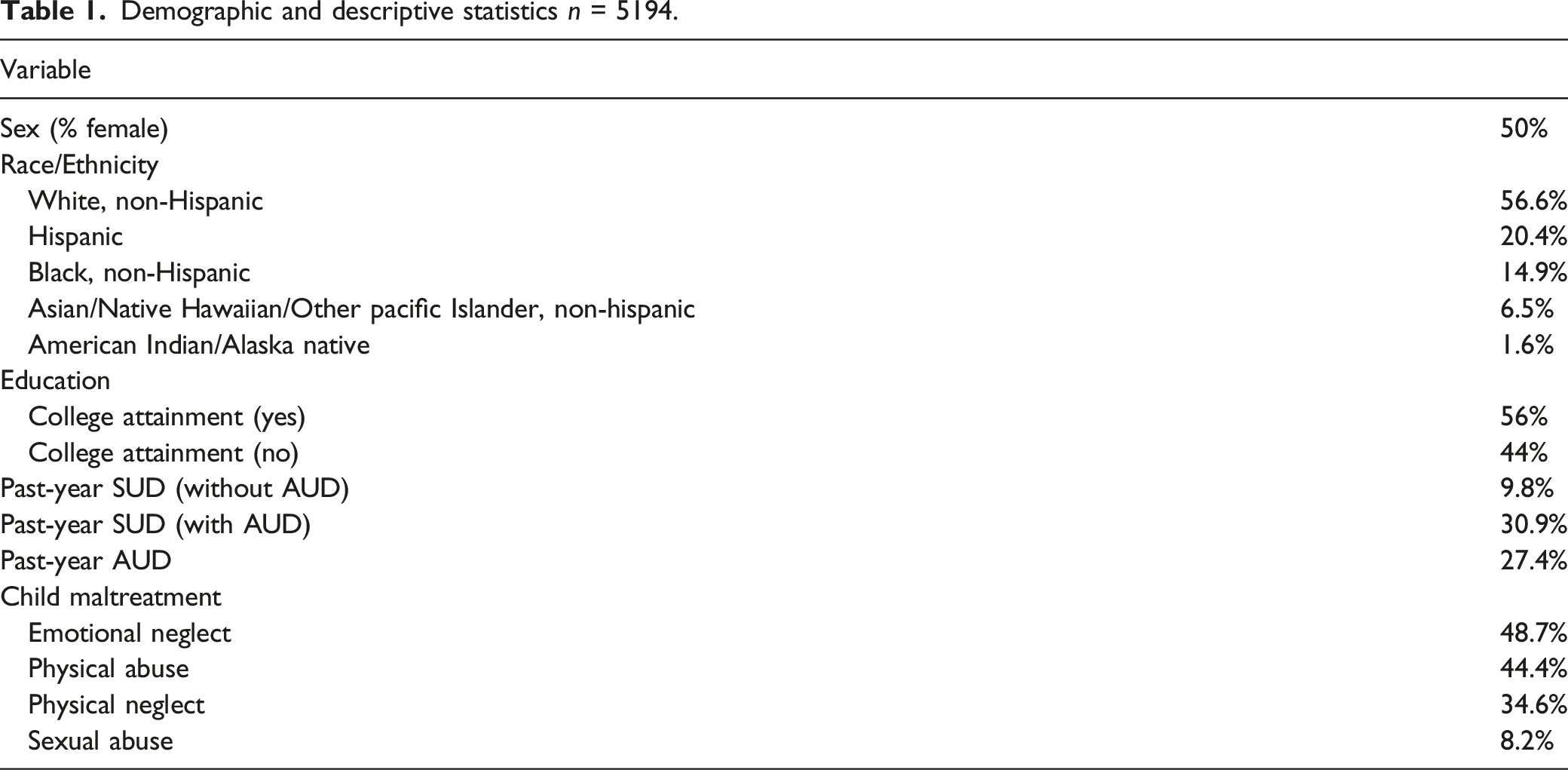
Demographic and descriptive statistics n = 5194.
Measures
Child Maltreatment
Questions involving child maltreatment were adapted from empirically-validated scales including the Conflict Tactics Scale-2 (Straus et al., 1996) and the Childhood Trauma Questionnaire (Bernstein et al., 1994). Participants reported whether they experienced a variety of types of maltreatment prior to the age of 18 on a 5-point scale ranging from Never (1) to Very Often (5). Based on participant responses, four subscales representing physical neglect, physical abuse, sexual abuse, and emotional neglect were created. Participant responses were coded dichotomously based on whether they experienced any maltreatment overall as well as for each of the four domains (0 = no; 1 = yes, any maltreatment).
Substance Use Disorder
The Alcohol Use Disorder and Associated Disabilities Interview Schedule (AUDADIS-5; Grant et al., 2015), a diagnostic interview for nonclinician interviewers with good psychometric properties (Grant et al., 2016), was used to measure whether individuals met criteria for a Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5) use disorders including alcohol, sedatives, cannabis, opioids, cocaine, stimulants, hallucinogens, inhalants/solvents, club drugs, heroin, and other drugs. Participants were coded based on whether they had experienced SUD in the past year (0 = no, 1 = yes). Because scholars have suggested alcohol use to be part of developmentally normative tasks (Schulenberg et al., 2014; Schulenberg & Maggs, 2002; Sussman & Arnett, 2014b), we also chose to examine AUD independently from the other SUDs.
Data Analytic Plan
Survey weights were used in all analyses. Separate weighted TVEMs (Dziak et al., 2017; Lanza & Linden-Carmichael, 2021; Tan et al., 2012) were used to examine the association between experience of any child maltreatment and SUD across age (RQ 1), the association between any child maltreatment and SUD across age by sex and racial-ethnic group (RQ 2), and associations between each subtype of child maltreatment and SUD across age (RQ 3). Each TVEM can be interpreted as the relative odds of experiencing a past-year SUD for emerging adults who reported child maltreatment relative to emerging adults who did not report child maltreatment, across age. As TVEM estimates coefficients as a function of continuous age or time, results are plotted as figures. Points at which the associated 95% confidence intervals including 1.0 are considered non-significant. Given the low prevalence rates of some types of child maltreatment, each type by sex and racial-ethnic group was not further examined. All models were estimated using SAS version 9.4 (SAS Institute Inc, 2013). We included parent drug use problems (“In your judgment, has your blood or natural father [or mother] had problems with drugs at ANY time in his [or her] life?”) and age of onset of any substance use (the age at which participants first smoked a first full cigarette, had at least 1 drink of any kind of alcohol (not counting small tastes or sips), college attainment (whether ever attend college or more education), family received government assistance before age 18, used cannabis, or cocaine/crack (consistent with other work using NESARC-III data; Blanco et al., 2018; Lopez-Quintero et al., 2011) as time-invariant covariates in all models.
Results
TVEM was used to test the relative odds of experiencing a past-year SUD for those who reported child maltreatment relative to those who did not, across ages 18–25 years. When AUD was included in SUD, there was no significant difference across age (Supplemental Figure (A)). There was also no significant difference in AUD alone (excluding other SUDs) across age (Supplemental Figure (B)). However, there were significant differences between the ages of 18–25 when SUD was examined without AUD. Subsequent analyses focus on SUD without AUD.
As depicted in Figure 1, individuals who reported any child maltreatment were found to be at significantly higher odds of experiencing a SUD in the past year between the ages 18.5 and 21 (ORs range from 2.09 to 1.58), relative to individuals who did not experience child maltreatment. Odds ratios were highest at approximately age 19, such that those who reported prior child maltreatment were at three times greater odds of a past-year SUD. This effect generally declined across cross-sectional age. Age-varying association between child maltreatment and past year substance use disorder across age. Note. Age-varying odds ratio indicating the increase in odds of past-year substance use disorder among individuals reporting any prior experience of child maltreatment compared to those who did not experience any child maltreatment. Dashed lines represent 95% confidence intervals.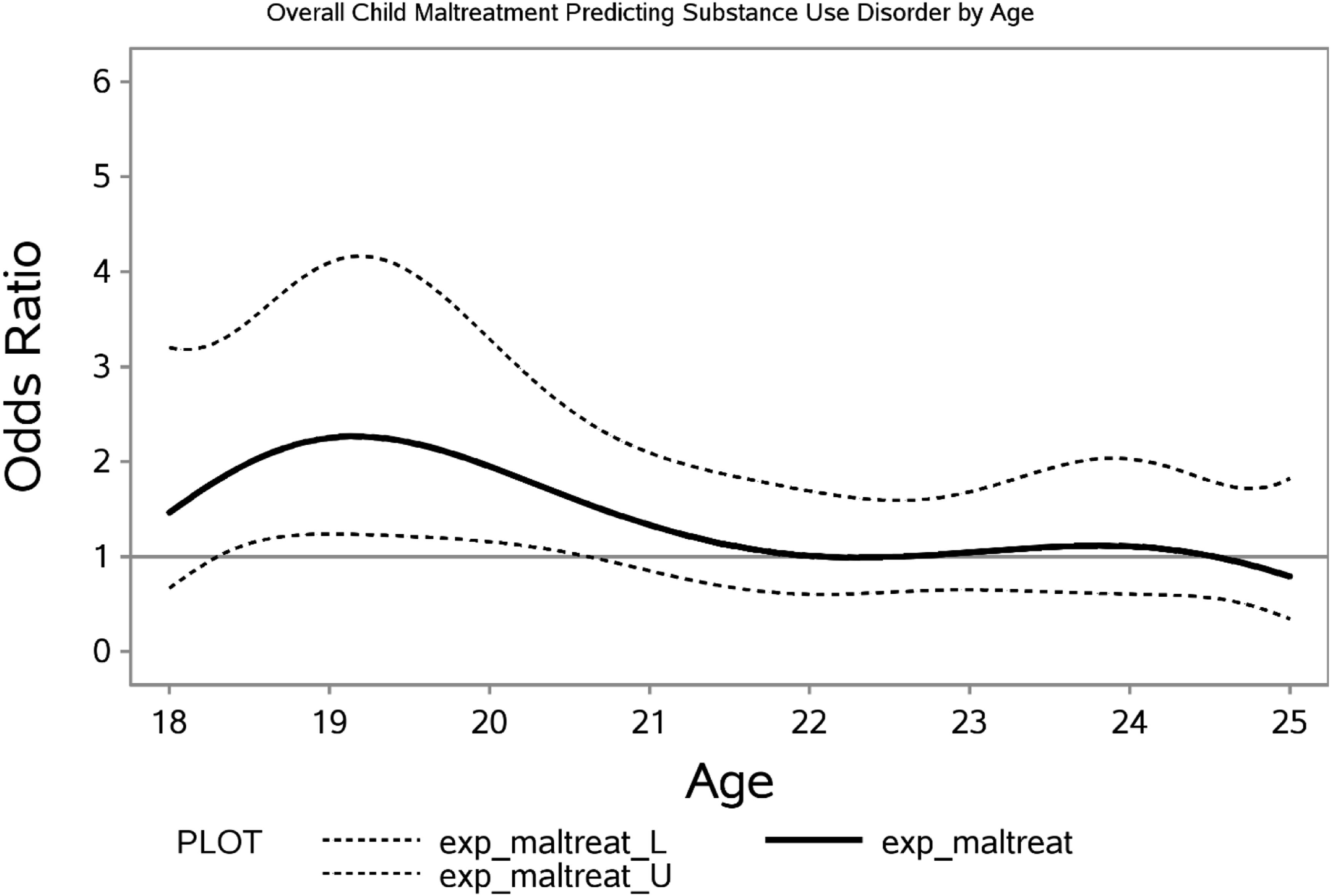
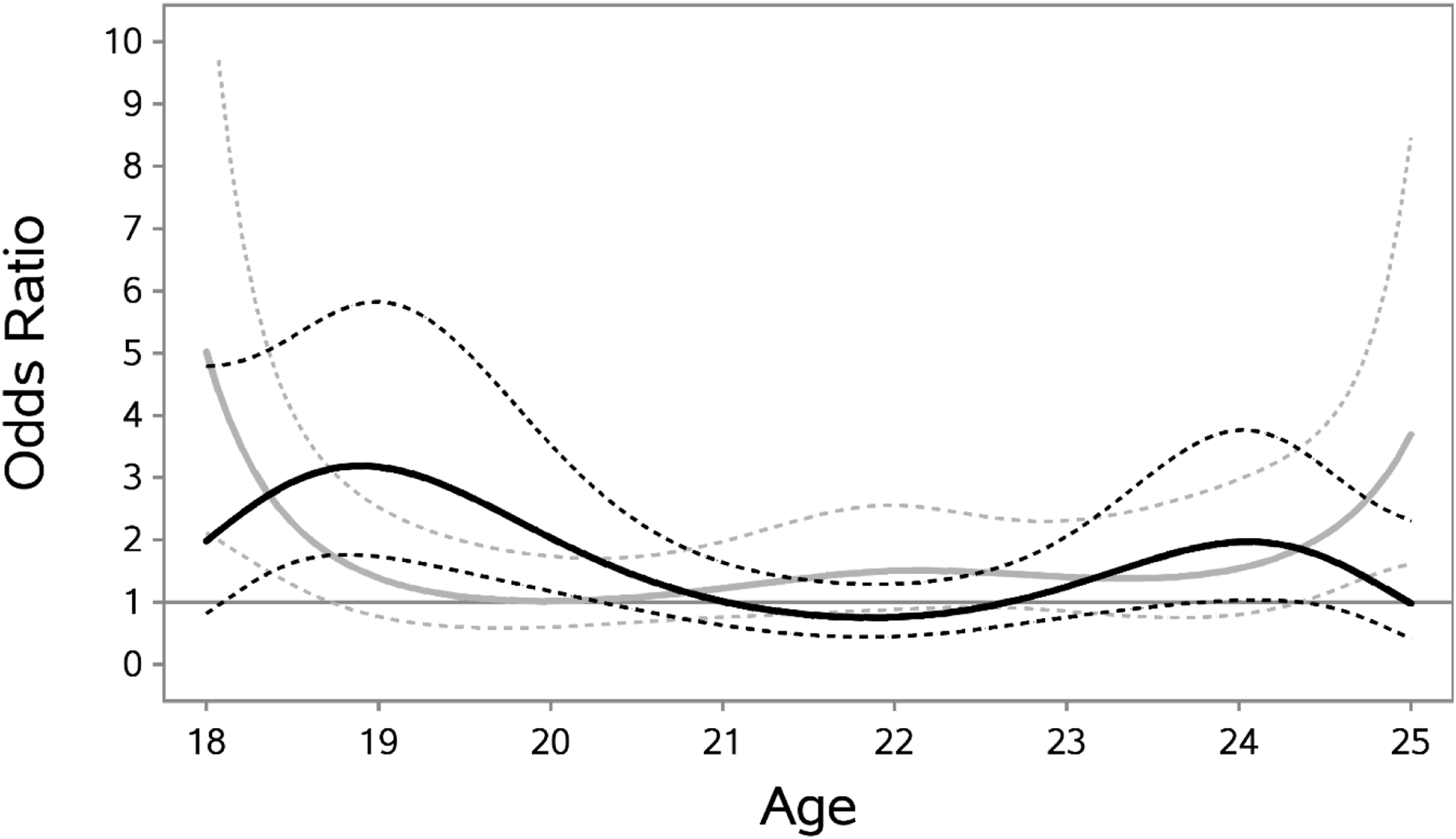
To examine potential sex differences, sex was added as a time-invariant effect in the TVEM. As shown in Figure 2, men (black line) who experienced child maltreatment were at significantly elevated risk for experiencing a past-year SUD relative to men who did not experience maltreatment from approximately ages 18 to 20 (ORs range from 2.04 to 1.62). Females (gray line) who reported child maltreatment were at greater odds of a past-year SUD from approximately ages 18.5 to 21 (ORs range from 1.87 to 1.67). Confidence intervals overlapped for males and females across all ages, but females relative to themselves reported greater odds of a past-year SUD around age 19.5 (nearly 4 times greater odds), and odds steadily declined across age. We also examined racial-ethnic differences in study associations by including Hispanic (vs. White) and Black (vs. White) into time-invariant effects in the TVEM. As shown in Figure 3, Hispanic (black line) adults who experienced child maltreatment were at significantly elevated risk for experiencing a past-year SUD relative to White adults from approximately ages 18 to 20 (ORs range from 2.29 to 1.78). Black (gray line) adults who experienced child maltreatment were at significantly elevated risk for experiencing a past-year SUD relative to White adults from approximately ages 18 to 18.5 and 24.5 to 25. Age-varying association between child maltreatment and past year substance use disorder across age, by sex. Note. Age-varying odds ratios indicating the increase in odds of past-year substance use disorder among males (black line) and females (gray line), separately, reporting any prior experience of child maltreatment compared to those who did not experience any child maltreatment. Dashed lines represent 95% confidence intervals. Age-varying association between child maltreatment and past year substance use disorder across age, by race/ethnicity. Note. Age-varying odds ratios indicating the increase in odds of past-year substance use disorder among Hispanic versus White (black line) and Black versus White (gray line), separately, reporting any prior experience of child maltreatment compared to those who did not experience any child maltreatment. Dashed lines represent 95% confidence intervals.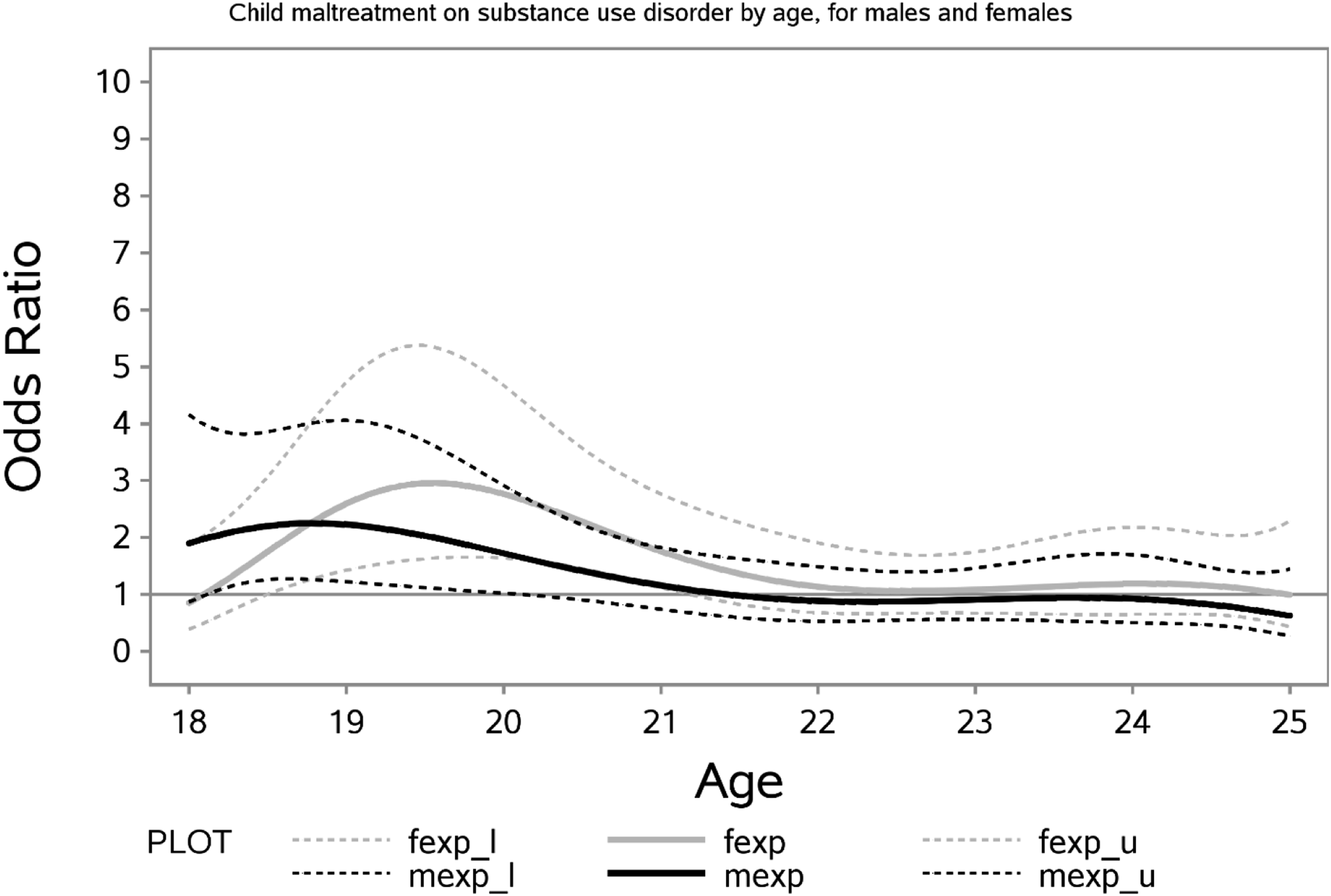
The relationship between child maltreatment and SUD was further examined by observing the individual associations between each type of maltreatment and SUD across age. Figure 4 depicts each type of maltreatment and the odds of reporting SUD in the past year across the ages of 18–25. Individuals who reported sexual abuse (black line) were found to be at significantly elevated risk for a past-year SUD from ages 22 to 24 relative to individuals who did not experience sexual abuse. The association between sexual abuse and SUD steadily increased around age 22 with odds ratios of approximately 2, peaking at 3.0 at age 23, and then declining after age 24. Physical neglect (blue line) was associated with higher odds of SUD from approximately ages 20 to 22.5, with odds ranging from about 1.5 to 2 during these ages. The association between emotional neglect (red line) and SUD was strongest earlier in age, with odds ratios over 2.0 at age 19, declining steadily with age. Individuals experiencing emotional neglect relative to those who did not experience emotional neglect were at elevated risk for a past-year SUD from approximately ages 18.5–21 years. Finally, physical abuse (gray line) and SUD was significant from approximately ages 18 to 23, with odds of about 2.0 at age 18 and peaks of odds ratios exceeding 3.0 around ages 20 and 21, and subsequent declines across age. Age-varying association between child maltreatment and past year substance use disorder across age, by maltreatment type. Note. Age-varying odds ratios indicating the increase in odds of past-year substance use disorder for individuals reporting any prior experience of physical abuse (gray line), sexual abuse (black line), emotional neglect (red line), or physical neglect (blue line), relative to individuals who did not. Confidence intervals are omitted for clarity; significant differences are described in text.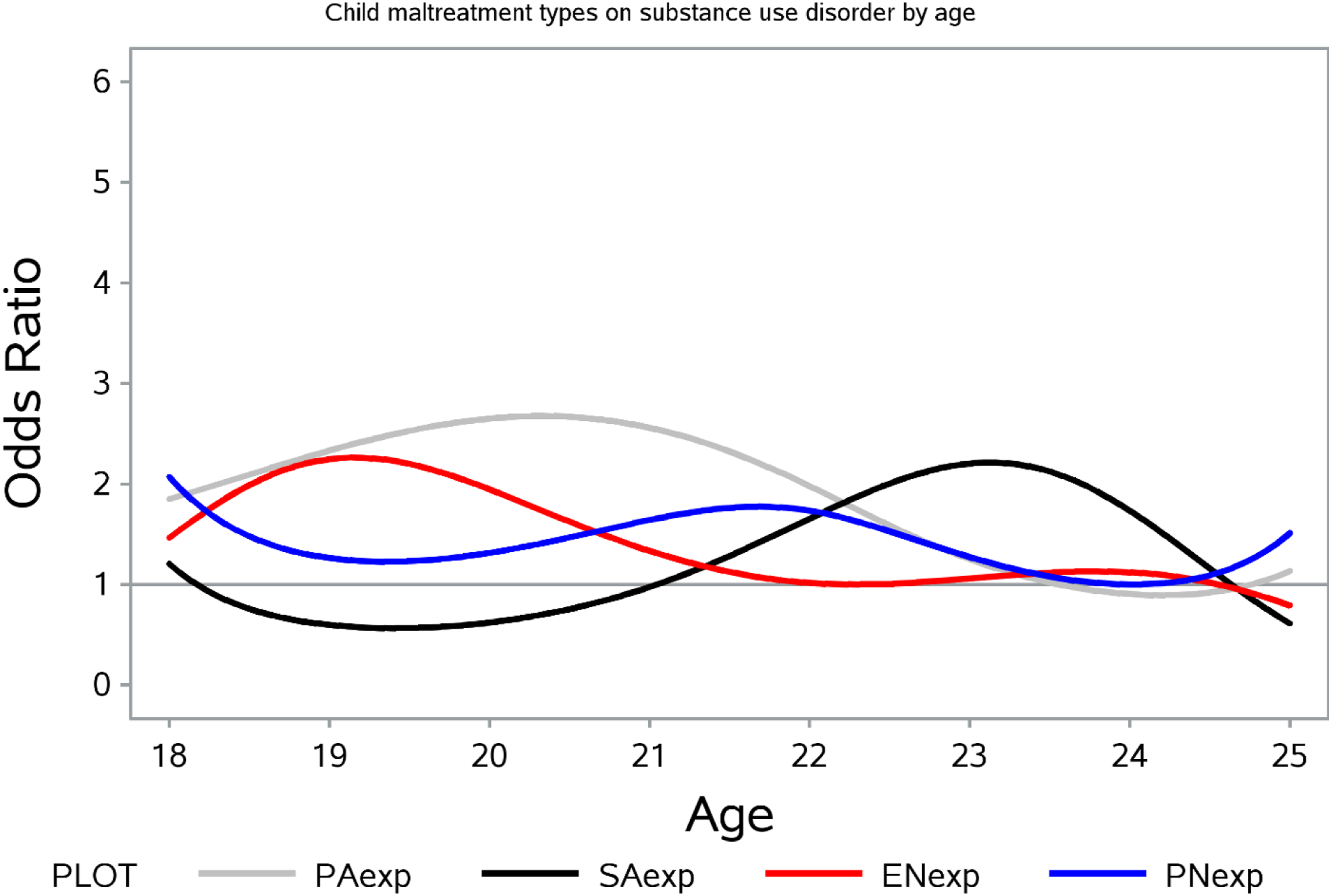
Discussion
The lack of understanding about how relationship between child maltreatment and SUD might vary across developmental periods, specifically emerging adulthood (age 18–25) when SUD is most prevalent (Stone et al., 2012), has stymied the public health impact of prevention efforts. Using TVEM, results presented here suggest that the experience of child maltreatment prior to age 18 is significantly associated with increased risk for SUD within the past year, particularly from ages 18 to 21. The link between child maltreatment and SUD peaked in severity at age 19, which is consistent with developmental theory related to emerging adulthood (Arnett, 2005). Enhanced substance use prevention strategies or increased screening around age 19 among those with, and without, a history of child maltreatment, may be worth considering. Recognizing early intervention points has the greatest potential to affect public health impact. We found significant differences in ages of highest risk between emerging adults identifying as Hispanic as well as Black compared to their White counterparts. This is aligned with prior research indicating a significant increase in SUD among Black emerging adults (Goings et al., 2022); however, these findings should be interpreted with caution. Scholars have called attention to what is known as the “crossover effect” wherein minority groups switch from low to high risk for SUD as they age (Banks & Zapolski, 2018; Geronimus et al., 1993). For example, also using TVEM with the NESARC-III dataset, Vasilenko et al. (2017) found a crossover effect for Black and White participants between the ages of 18 and 90 – prevalence of SUD was higher at younger ages for White participants and higher for Black participants at older ages. Prior research has demonstrated the crossover effect in a child maltreatment exposed population (Yoon et al., 2020); however the present study adds to the literature by using TVEM to identify a potential crossover effect in emerging adulthood among individuals with exposure to child maltreatment prior to age 18. Moreover, though this sample was not a child welfare population, it is worth acknowledging that recent research has called attention to the overrepresentation of racial and ethnic minorities in the child welfare system (Luken et al., 2021; Maguire-Jack et al., 2021). More research is needed to inform potential tailoring of interventions to prevent substance use disorder among emerging adults in racial and ethnic minorities.
Prior research has largely focused on the association between child maltreatment and substance use in adolescence (ages 12–18). Indeed, all types of maltreatment have been associated with adolescence substance use (Benedini & Fagan, 2020a; Hamburger et al., 2008; Harrison et al., 1997; Hussey et al., 2006; Lansford et al., 2010; Moran et al., 2004; Sartor et al., 2013; Thornberry et al., 2001; White & Widom, 2008). Importantly, this association varies by sex (Benedini & Fagan, 2020b; Halpern et al., 2018a; Horan & Widom, 2015; Lansford et al., 2010; McHugh et al., 2018) and maltreatment type (Harrison et al., 1997; Huang et al., 2011; Moran et al., 2004). Our results suggest this variability holds in emerging adulthood as well. In this sample, females were at greatest risk from 18.5 to 22.5 whereas men were more likely to report a SUD from age 18 to 21.5 and 22.5 to 24. This second period of risk for men may be a unique target for tailored, male-focused prevention efforts.
We also found that ages associated with heightened risk varied by child maltreatment type. The highest risk for sexual abuse was later in emerging adulthood (ages 21–24.5) compared to physical abuse, emotional neglect, and physical neglect (ages 18–23.5). The delay in risk observed among those with exposure to sexual abuse is not well understood. It is possible that the therapeutic efforts commonly provided to sexual abuse victims has a treatment effect that reduces the risk of SUD or suppresses risk for a period of time. The results presented herein are epidemiological in nature and should motivate future research to better understand these associations such that prevention efforts can be tailored to periods of heightened risk rather than solely the prevention of substance use initiation.
These results extend the line of prior research using NESARC-II data which demonstrated an association between child maltreatment and SUD in men and women with and without exposure to maltreatment prior to age 18 (Afifi et al., 2012). This is one of the first applications of TVEM to understand the sequalae of child maltreatment. Findings indicate the need for differential intervention strategies at different ages for victims of different types of child maltreatment, aligned with prior research (Bayly et al., 2021; Guastaferro & Bray, 2020). Early intervention increases the potential for public health impact; however, findings should be interpreted with caution as one application of TVEM to one dataset is unlikely to answer all unknowns and as such there are several limitations to note. This study used data from NESARC-III. While this dataset has strengths in its national representative sample, the focus of the study was not child maltreatment resulting in little nuance in the types of maltreatment asked (e.g., no measure of supervisory neglect; (Mennen et al., 2010; Sokol et al., 2021). Further, there are no questions regarding the age at the time of maltreatment, frequency, intensity, duration of the maltreatment, as well as the relationship of the victim to perpetrator. These data are also cross-sectional which precludes any determinations about longitudinal effects or trajectories. Exposure to multiple types of maltreatment was not accounted for in models. There is a high co-occurrence of multiple types of maltreatment and greater risk of substance use is associated with exposure to multiple types (Arata et al., 2005). It is likely these variables play an important role in the development of SUD (Jonson-Reid et al., 2012) and should be explored in future research efforts leveraging administrative data when possible. Moreover, the frequency of exposure to all subtypes was not equal and, thus, precluded the examination of SUD by subtype and sex across emerging adulthood. Child maltreatment is a prevalent public health problem but is not often the sole focus of prospective cohort studies. Given the impact of child maltreatment on health outcomes, future epidemiological surveys, across public health topics, should consider a more comprehensive and nuanced panel of questions related to child maltreatment exposure.
Substance use is highly prevalent during emerging adulthood, but our findings underscore the increased risk for SUD among individuals with a history of child maltreatment. This is an at-risk group in need of targeted prevention efforts; however, prevention efforts remain largely focused at early childhood and adolescence (Hill, 2019). Though primary prevention efforts are underway to stop the experience of maltreatment in the first place, to fully impact this public health priority prevention must also focus on reducing the negative consequences, such as substance use, among those who have already experienced child maltreatment. Interrupting the progression of risky behavior, a priority for prevention science (Schwartz & Petrova, 2019), is referred to as prevescalation (Villanti et al., 2019). To this end, if differences in outcomes by sex and maltreatment type are better understood across developmental periods with high risk, then prevention efforts can be better informed and likely more effective.
Supplemental Material
Supplemental Material - Association Between Child Maltreatment and Substance Use Disorder Across Emerging Adulthood
Supplemental Material for Association Between Child Maltreatment and Substance Use Disorder Across Emerging Adulthood by Kate Guastaferro, Ashley N. Linden-Carmichael, and Shou-Chun Chiang in Child Maltreatment
Footnotes
Acknowledgments
The authors would like to thank Drs. Toria Herd and Stacey Shipe for their reviews of early drafts of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by the National Institute on Drug Abuse of the National Institutes of Health under award numbers P50 DA039838 and T32 DA017629 as well as the National Institute on Alcohol Abuse and Alcoholism by award K01 AA026854. The NIH did not have any role in study design, collection, analysis, and interpretation of the data; writing the report; and the decision to submit the report for publication. The content is solely the responsibility of the authors and does not necessarily represent the official views or opinions of the National Institutes of Health or the U.S. government. This manuscript was prepared using a limited access dataset obtained from the National Institute on Alcohol Abuse and Alcoholism.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.