
Abstract
Infants face the highest risk of abuse and neglect nationally. There is a compelling need to understand the individual risk factors and needs of families of maltreated infants so that prevention efforts can be tailored for optimal effectiveness. Using linked birth certificate and CPS records data, we employed latent class analysis to identify distinct profiles of perinatal health factors associated with infant maltreatment. Classes were then regressed onto two key child welfare outcomes—removal from the home and re-report. Results indicated 10 latent classes primarily associated with supervisory neglect and presumed prenatal substance exposure. Rapid repeat pregnancy, smoking during pregnancy and inadequate prenatal care emerged as key risk factors. Presumed substance exposure was associated with high risk of removal from the home and low risk of re-report. The opposite was found for supervisory neglect. Substantial variation existed across classes and types of maltreatment, suggesting a need for tailored prevention strategies.
Introduction
Young children are particularly vulnerable to maltreatment. In 2019, children under 1 year of age (infants) were maltreated at a rate of 25.7 per 1,000, more than twice the rate for any other age group (Federal Interagency Forum on Child and Family Statistics, 2021a). Nationally, neglect is the most common subtype of maltreatment among infants (81.3%), followed by physical abuse (18.6%), other or unknown subtype of maltreatment (6.4%), medical neglect (3.2%), psychological maltreatment (2.8%) and sexual abuse (0.4%) (Federal Interagency Forum on Child and Family Statistics, 2021b). Neglect is more likely to recur (i.e., result in a re-report to child welfare) and is a significant cause of maltreatment-related death in infancy (Bartlett & Easterbrooks, 2015; Chiang, Yang, Wittenberg, & Jonson-Reid, 2022).
Because there is significant variation in the way that child welfare systems record and respond to prenatal substance exposure (PSE), it is not known exactly how many cases of physical abuse or neglect can be attributed to PSE. Nevertheless, prenatal exposure to substances such as drugs and alcohol is a major concern in the US and is placing an outsized burden on child welfare systems. Recent state-level analyses for Washington and California showed that 40–60% of births with documented prenatal substance exposure were reported to CPS, and many of these infants were removed from the home (Prindle, Hammond, & Putnam-Hornstein, 2018; Rebbe, Mienko, Brown, & Rowhani-Rahbar, 2019). In Texas, 66% of cases in which children are removed from the home are due to parental substance use, and when children are placed in foster care before age 3, they are unlikely to be reunited with their families (Kohler & Murphy, 2018). Infant maltreatment, including PSE is a major focus of prevention research both because of its prevalence and potential for adverse outcomes, including recurrence and/or removal from the home. The purpose of this study is to assess the co-occurrence of risk factors in families and whether these patterns of co-occurrence are differentially associated with maltreatment type and protective services outcomes. The aim of assessing these risks is to help understand the myriad of prevention strategies that will be needed to ultimately reduce infant maltreatment.
A Prevention Approach to Maltreatment
While the child welfare system was initially designed to investigate and respond to maltreatment, state and federal governments now recognize the need for greater attention to prevention (Child Welfare Information Gateway, 2017). Beginning in FY 2020, the Family First Prevention Services Act allows states to use federal funds to provide preventive services to families with a child at-risk for foster care placement (Children’s Defense Fund, 2018). Further, the 2018 reauthorization of Child Abuse Prevention and Treatment Act (CAPTA) emphasizes the roll of early identification and support to pregnant persons by expanding the scope of Plan of Safe Care as a prevention and mitigation strategy for abuse associated with PSE before the family becomes involved with child protective services.
A large body of research literature has documented risk factors for maltreatment that can be measured at or before a child’s birth. Demographic risk factors include low income or poverty, single motherhood, higher parity (or larger numbers of children in the household), low maternal education, and race (Austin, Parrish, & Shanahan, 2018; Kotch, Browne, Dufort, Winsor, & Catellier, 1999; Kotch et al., 1995; Mulder, Kuiper, van der Put, Stams, & Assink, 2018; Slack et al., 2011; Wu et al., 2004; Zhou, Hallisey, & Freymann, 2006). Other maternal characteristics such as depression and stress, low levels of social support, and intimate partner violence (Kotch et al., 1995, 1999; Mulder et al., 2018; Shanahan, Runyan, Martin, & Kotch, 2017), as well as behaviors such as substance use, smoking during pregnancy, inadequate prenatal care, and short intervals between pregnancies/births have also been linked with increased risk of infant abuse and neglect (Austin et al., 2018; Wu et al., 2004; Zhou et al., 2006). Additionally, maltreatment has been found to occur more commonly among infants with certain risk factors at birth, such as low birth weight (Wu et al., 2004), prematurity, admission to the neonatal intensive care unit (NICU), poor APGAR scores, perinatal complications (Zelenko, Lock, Kraemer, & Steiner, 2000) and congenital abnormalities (Van Horne et al., 2015). This information can be leveraged to develop interventions and systems for primary prevention of key forms of maltreatment.
These risk factors commonly present in healthcare interactions and/or are screened for by healthcare providers. Further, most pregnant women will receive some form of health care during pregnancy and/or delivery, and/or seek pediatric care for their newborn. Thus, the healthcare system is a critical access point for a comprehensive prevention strategy. However, none of the above-mentioned risk factors alone is predictive of maltreatment, and few occur in isolation of each other. A prevention approach to child welfare requires an in-depth understanding of the multiple and interrelated risk factors associated with child maltreatment.
Person-Centered Analysis
Maltreatment is not a unitary construct and risk factors within families that are associated with maltreatment are not homogeneous. Thus, person-centered data analysis methods can be particularly useful in the context of prevention research. Variable-centered methods, like regression and factor analysis, are used to determine the relative influence of one variable on another. Person-centered methods—including cluster analysis, latent profile analysis and latent class analysis (LCA)—analyze the clustering of characteristics from multiple variables within individuals (Hagenaars & McCutcheon, 2002). Groups, or classes, are formed based on specific patterns of item responses. Given the complex relationships between risk factors and the many possible configurations of risk factors that individual families may face in real-world experience, LCA is a useful tool for identifying opportunities for prevention at the family level.
The value of person-centered methods for maltreatment research has been highlighted in the literature. Roesch, Villodas, and Villodas (2010) and other recent studies have used LCA to examine different aspects of child maltreatment and adversity (Brown, Rienks, McCrae, & Watamura, 2017; Kang, Bae, & Fuller, 2015). Holbrook and Hudziak (2020) used LCA to develop classes of maltreatment based on initial status (substantiated or not) and recurrence within 5 years. Caregiver-reported domestic violence, caregiver substance abuse, and poverty significantly differentiated the latent classes. Kim et al. (2020) used LCA to examine family and social characteristics associated with maltreatment re-report for children birth to age 15. Prindle, Foust, and Putnam-Hornstein (2021) conducted an LCA to identify classes of maltreatment for children from birth to age 18, which were differentially associated with CPS outcomes substantiation and out-of-home placement. Waid, Santaularia, Piescher, and Laliberte (2021) identified latent classes of risk among families who experienced a child maltreatment re-report or maltreatment recurrence within 12-months of initial case closure. These studies have shown that within-individual clustering of risk factors, rather than single variables, are associated with a variety of CPS outcomes.
Only a very small number of studies have attempted to classify and predict maltreatment outcomes based on risk factors identified at or before birth. Prendergast and MacPhee (2021) identified latent classes of maternal and family risk factors reported in surveys carried out at the time of the child’s birth, including family functioning, maternal mental health history, nutrition, smoking, substance use during pregnancy, housing insecurity. number of children in the home, marital status, poverty, and maternal education were predictive of abuse trajectories. This study found that classes with high neighborhood cohesion and lower parenting stress were associated with low maltreatment risk; it highlights the importance of considering these two factors jointly. Eastman, Mitchell, and Putnam-Hornstein (2016) used LCA to create classes of risk factors identified from birth certificate records. The study identified profiles of maternal demographic characteristics associated with higher versus lower risk of a second CPS report within 5 years for children who remained in the home following the initial investigation. Two groups had equally low risk of re-report at 44% each. These groups demonstrated high probabilities of Medicaid use, initiation of prenatal care in the first trimester, and report for physical abuse and lower probability of neglect compared to higher risk classes. Higher risk groups included young mothers, low probability of established paternity, later initiation of prenatal care, and higher risk of neglect or substantial risk.
The Current Study
The present study employed latent class analysis to identify profiles of perinatal health among infants with a substantiated case of maltreatment in Texas. We then explored the risk associated with each profile relative to two key outcomes—removal from the home and re-report. As such, the study was designed to address the following research questions: (1) Are there distinct profiles (latent classes) of perinatal health characteristics associated with different types of maltreatment during infancy? (2) What is the probability of removal from the home associated with these profiles? (3) What is the probability of subsequent maltreatment investigation for these profiles? The larger objective of this work is to identify patterns of risk that can be used to develop and implement population-level maltreatment prevention efforts focused on the prenatal period.
Methods
Data
Data employed in the study included linked birth certificate and Child Protective Services (CPS) investigation records from the state of Texas. Birth certificate records, representing the original filing without later modifications or amendments, were obtained for all children born in Texas between 2009 and 2014. Data from the birth certificate included demographic characteristics as well as information about the pregnancy and birth including mother’s use of prenatal care, weight gain, smoking during pregnancy, health problems (e.g., diabetes, hypertension), type of delivery, complications during labor, infant birth weight and gestational age, and whether the child was admitted to the NICU.
CPS records included information for all investigations completed between 2009 and 2015, including date opened, date closed, disposition of the case, type(s) of maltreatment, and whether the child was removed from the home. All cases with substantiated maltreatment where the first substantiated investigation was opened before the child’s first birthday were selected from the CPS data file. The type of substantiated maltreatment was also included in the analysis file. In cases where multiple types of maltreatment were documented a hierarchy was used to classify the case. Sexual abuse was coded first, followed by physical abuse, medical neglect, physical neglect, then supervisory neglect. Additionally, this study included an indicator of potential prenatal substance exposure (PSE) as a distinct type of maltreatment. In Texas, PSE resulting in harm or injury to the infant is classified as physical abuse. CPS investigations that were opened within 14 days of the infant’s birth and resulted in substantiated physical abuse were classified as presumed PSE. Cases of substantiated abandonment, failure to accept parental responsibility, sex trafficking, and sexual abuse were excluded from the analytic file due to inadequate sample size (n = 172).
Two other variables, including the final disposition of the first substantiated case of maltreatment and the total number of investigations for each child through his or her fourth birthday, were used in constructing distal outcome variables for our analyses. The disposition variable was coded into a binary indicator reflecting removal from the home (or not) at the time of the first substantiated case. A second binary variable was created indicating children who had a subsequent CPS investigation (or not) at any time before their fourth birthday following the first substantiated case of maltreatment. It must be noted that these data do not provide information as to whether the child was reunited with the family. Therefore, re-report rates may be reduced where removal rates are high and reunification rates are low.
CPS data were matched to birth certificate records using a multi-step matching algorithm. The algorithm has been described in detail in Buek, Lakey, and Mandell (2019). The match rate for substantiated maltreatment cases in the first year was over 90%, comparable to matching rates reported in other states (Putnam-Hornstein, Webster, Needell, & Magruder, 2011).
Analyses
Latent Class Analysis (LCA) Model Fit, Classification Accuracy and Likelihood Ratio Tests (LRT).
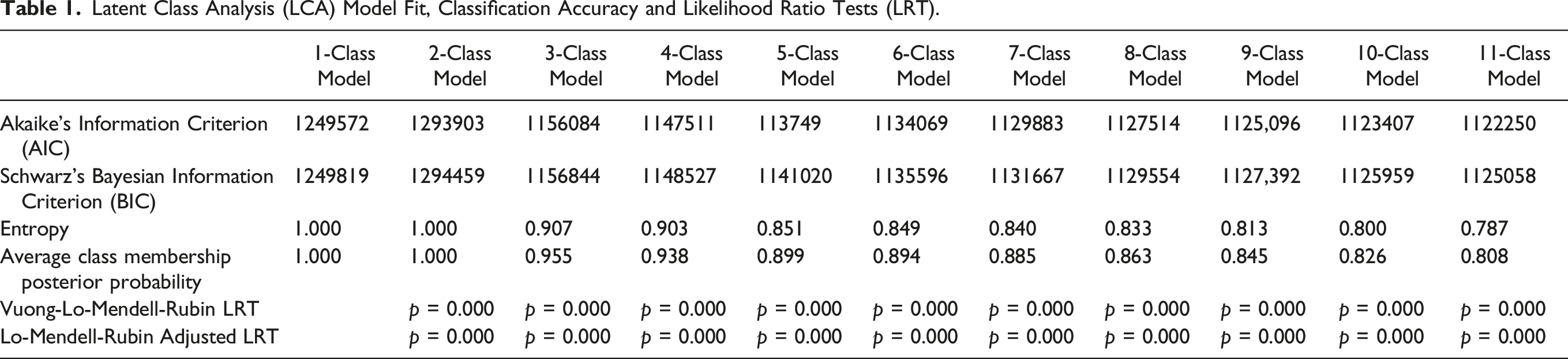
In LCA, the researcher specifies the number of classes to be derived from the dataset, starting with a single class and adding classes one at a time. At each iteration, the model is evaluated to determine its fit with the data according to a set of fit statistics, including measures of inter-class and intra-class variation, the accuracy with which individuals can be assigned to a class, and the degree to which the classes represent theoretically or logically meaningful distinctions (Nylund, Asparouhov, & Muthén, 2007). Models specifying 2 to 11 latent classes were tested, and the best-fitting model was evaluated based on (a) Aikake’s Information Criterion (AIC) and Schwarz’s Bayesian Information Criterion (BIC), with lower values indicating better model fit (Nylund et al., 2007); (b) integrated classification likelihood with Bayesian-type approximation (ICL-BIC) (McLachlan & Peel, 2000); (c) posterior classification accuracy values, with values closer to 1 representing superior accuracy (Greenbaum, Del Boca, Darkes, Wang, & Goldman, 2005; Nagin, 1999); and (d) logical-theoretical coherence of latent class distinctions (Ram & Grimm, 2009). Interpretation of latent classes was based on comparing latent class item response probabilities with the observed proportion among the total population of maltreated infants. To make this comparison, 99% confidence intervals for each response category were created for all variables in the model. Latent class probabilities that were significantly greater than the population proportion appear in bold font in Table 1 and represent defining characteristics of each latent class.
Latent classes were then regressed onto the distal outcomes (removal and re-report) to obtain odds of the occurrence for each of the latent classes. The regressions were performed in Mplus, using the DCAT option for categorical distal outcomes. The DCAT procedure operationalizes a method proposed by Lanza and Rhoades (2013) to correct for the downward bias in regression estimates that tends to occur when using latent class membership as a predictor of an outcome variable via certain procedures (Asparouhov & Muthén, 2014).
Results
Among children with substantiated maltreatment during their first year, the most common subtypes of maltreatment were supervisory neglect (40.6%) and presumed PSE (40.1%), followed by physical abuse (11.4%), physical neglect (4.8%) and medical neglect (2.3%).
Identifying the Best-Fitting Latent Class Model
Class size and fit statistics are presented for LCA models specifying 1 to 11 classes in Table 1. All the models produced classes with adequate sample size for statistical analyses. Values of the AIC and BIC improved as classes were added, and likelihood ratio tests indicated that each model was a significant improvement upon the last. Entropy and classification probabilities remained above 0.8 through the 10-class model, indicating excellent classification accuracy. An 11-class model produced a sixth class with probabilities for risk factors similar to other classes with only minor distinctions in demographic characteristics; classification accuracy was low in some classes. Thus, it was determined that the 10-class model was the better solution.
Interpreting the 10-Class Solution
Class Size and Estimated Item Response Probabilities for Latent Classes of Infant Maltreatment.
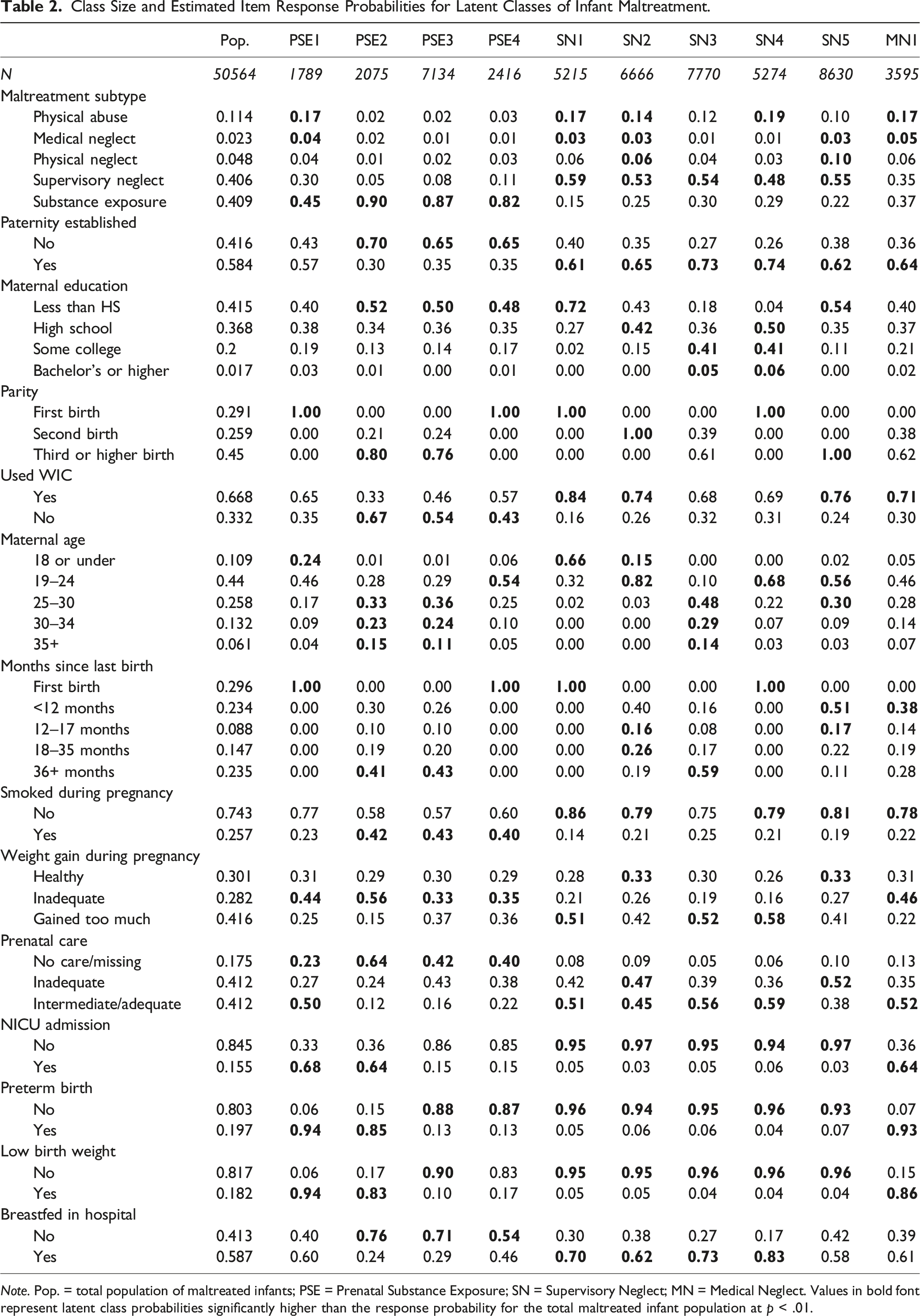
Note. Pop. = total population of maltreated infants; PSE = Prenatal Substance Exposure; SN = Supervisory Neglect; MN = Medical Neglect. Values in bold font represent latent class probabilities significantly higher than the response probability for the total maltreated infant population at p < .01.
Of the four presumed PSE classes, two consisted of young first-time mothers (PSE1 & PSE4) and two consisted of multiparous mothers (PSE2 and PSE3). The two classes of first-time mothers were distinguished from one another based on their level of prenatal care and the baby’s birth outcomes, with PSE1 having higher prenatal care use but poorer birth outcomes. The PSE1 class was notable among PSE classes for higher use of WIC services, lower rates of smoking, and higher rates of paternity establishment. The two classes of multiparous mothers were also distinguished by the birth outcomes of their infants, with PSE2 class having significantly higher rates of preterm and low-birth-weight babies.
All five SN classes had significantly higher rates of paternity establishment than any of the 4 PSE classes. The SN classes also had significantly higher rates of prenatal care and lower rates of poor birth outcomes than any of the PSE classes. Within the SN classes, two were first-time mothers (SN1 & SN4) and three were mostly multiparous mothers (SN2, SN3, & SN5). The two classes of first-time mothers were distinguished from each other based WIC utilization (84% in SN1) and maternal age—SN1 included teen mothers but SN4 did not. The three classes of multiparous mothers were distinct from one another based on several factors. Classes SN5 and SN2 were notably distinct from SN3 based on birth spacing. Both of these classes had short birth intervals, with high rates of intervals of less than 17 months. Classes SN5 and SN2 also had lower rates of breastfeeding and higher rates of inadequate prenatal care and were very similar across all risks except age, with SN2 consisting of younger mothers than SN5. SN3 is notably different from all other groups as 46% of women in this class have some college or higher. This class also has higher proportions of older mothers with significantly longer birth intervals (more than 36 months) than the other SN classes.
Latent Class Comparisons on CPS Outcomes
Regression analyses yielded estimated probabilities for removal from the home and re-report before the child’s fourth birthday for each of the 10 latent classes of infant maltreatment (Figures 1 and 2). Substance exposure classes had significantly higher-than-average probabilities of removal. The exception was PSE1, which had a removal rate significantly below the population rate. SN classes were at or significantly below the population mean for removal.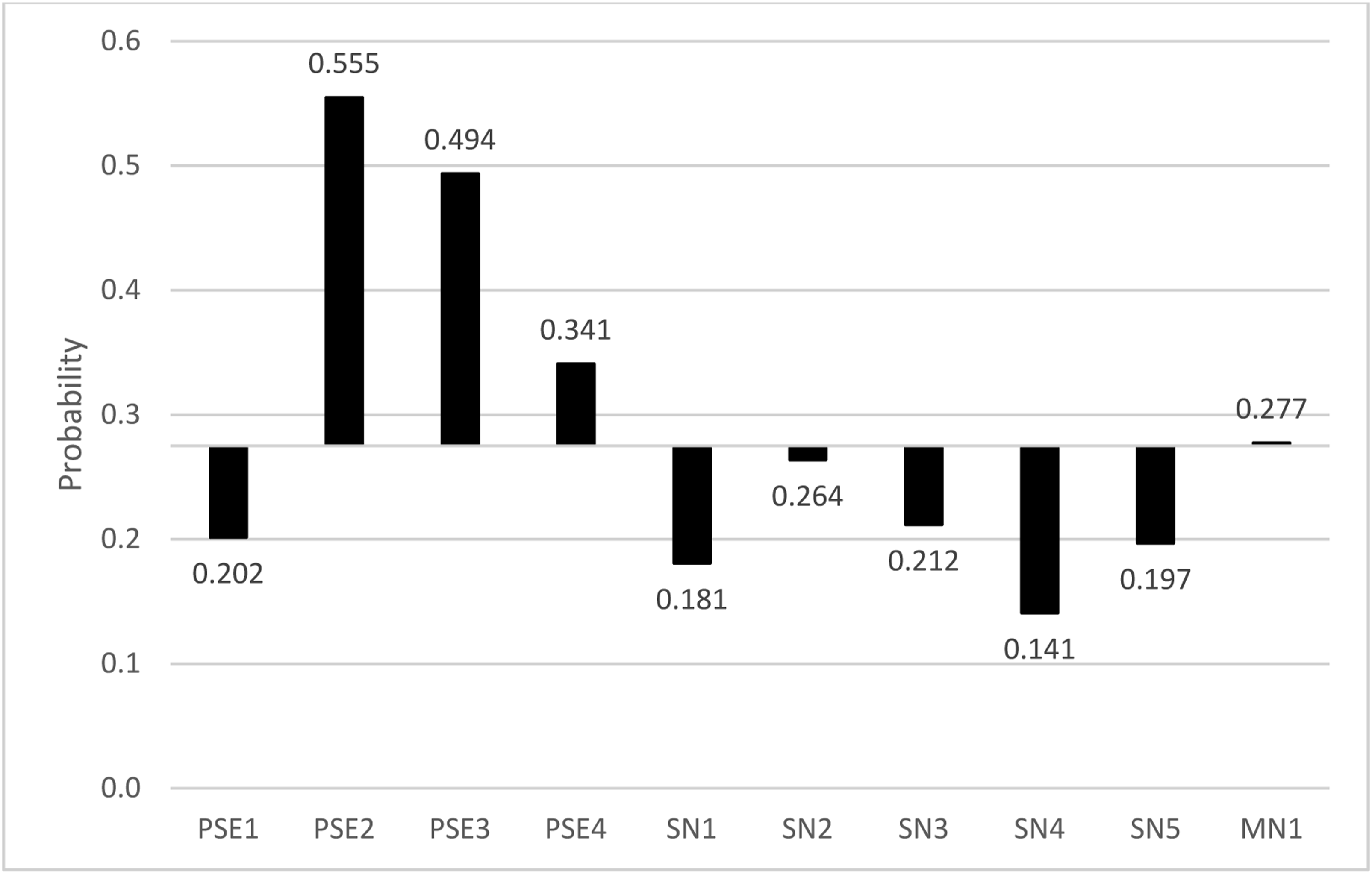
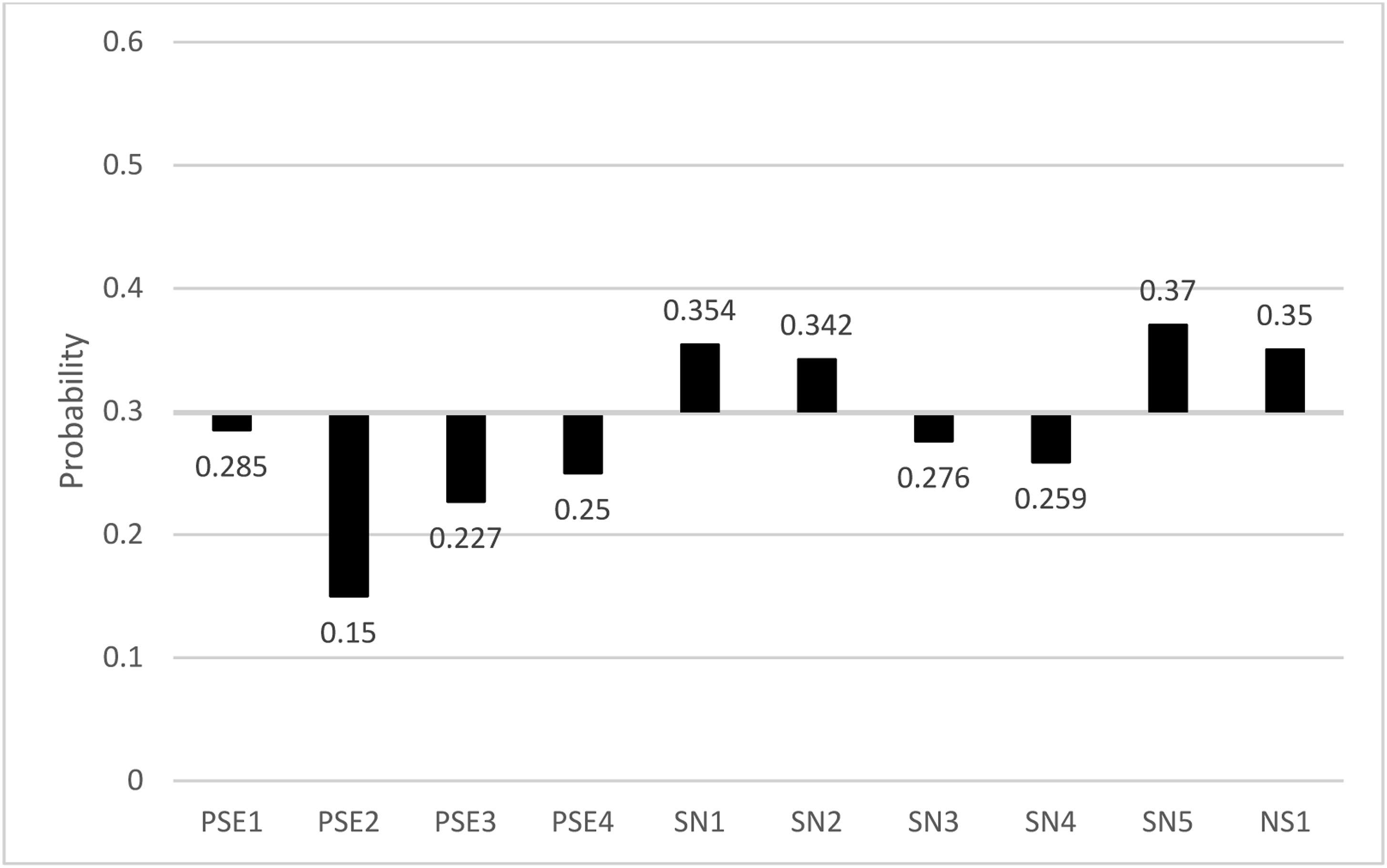
Alternately, latent classes associated with presumed PSE were at or significantly below the total population average for re-report. Whereas three of the five SN classes were at significantly higher risk of this outcome. Class SN4 was associated with a significantly lower risk of both removal and subsequent report compared to the population of maltreated infants. Class MN1, which was associated with physical abuse and medical neglect, also had a probability of re-report that was significantly higher than the population average.
Discussion
This analysis uncovered distinct perinatal health profiles among CPS-involved families which were associated with specific types of infant maltreatment. Supervisory neglect and presumed substance exposure were by far the most prevalent forms of maltreatment occurring among infants in this sample. Latent classes emerging from the analysis were therefore most strongly associated with these two forms of maltreatment. Further, our findings demonstrate how risk and protective factors cluster together in families and how these clustered risks are associated with risk for poor child welfare outcomes. Even within maltreatment subtypes, groups demonstrated distinct risk profiles suggesting distinct needs for support. Importantly, the risks examined here are not unique to families with substantiated maltreatment and point to the need to adopt a universal approach to maltreatment prevention with the goal of mitigating and preventing risk, rather than preventing the maltreatment event.
Family Profile Description and Policy Implications for Latent Classes of Infant Maltreatment.
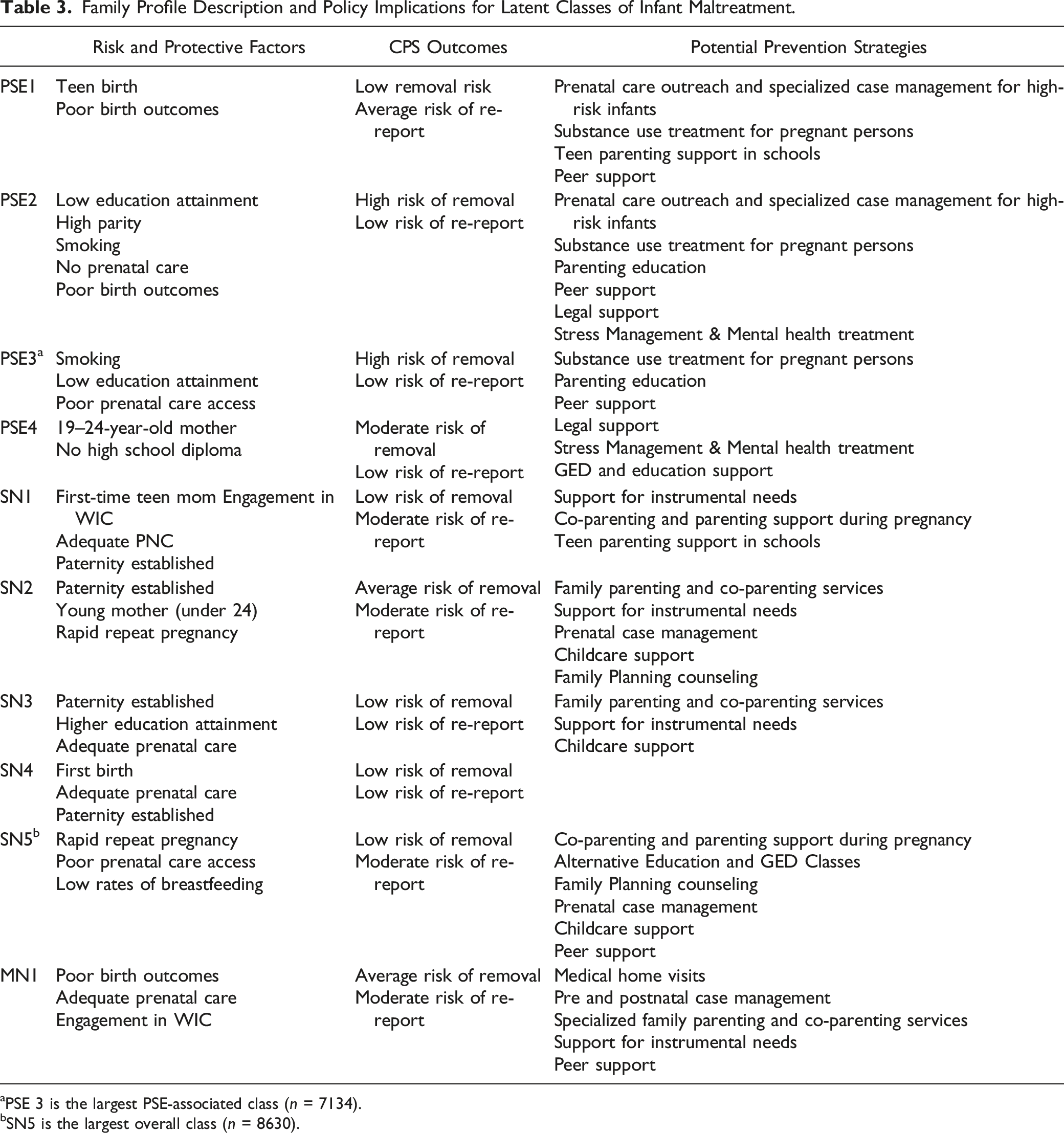
aPSE 3 is the largest PSE-associated class (n = 7134).
bSN5 is the largest overall class (n = 8630).
In addition to risk, these results point to important protective factors that should be supported in primary prevention. Complementing the findings of Eastman et al. (2016), higher probability of established paternity characterized classes with lower risk of re-report and removal. This finding points to the need to intentionally include fathers and male caregivers in prevention programs and highlights recent calls for co-parenting education for both parents in prevention efforts. Further, use of prenatal care and WIC was common in classes with low probability of poor CPS outcomes, suggesting that these points of access could be leveraged to provide preventive interventions or navigate families into prevention programs.
Two risk factors that were found in two of the largest classes associated with supervisory neglect were rapid repeat pregnancy and short birth intervals. These have long been recognized as risk factors for poor obstetric outcomes, but their significance here highlights their relevance to child welfare as well. Rapid repeat pregnancy and short birth intervals may signal increased stress on the family unit, again underscoring the need for comprehensive prenatal prevention programs that support families’ health and social needs. There are a number of maltreatment prevention and family support models that focus on reaching families after the baby is born or during pediatric care, including Family Connects, Healthy Steps, and Safe Environment for Every Kid (SEEK) (Dubowitz, Feigelman, Lane, & Kim, 2009; Goodman, Dodge, Bai, O'Donnell, & Murphy, 2019; HealthySteps, 2021). However, there are currently no maltreatment prevention programs designed for use by obstetric providers during the prenatal period. While home visiting programs, such as Nurse Family Partnership, begin in the prenatal period, many have eligibility requirements (such as being a first-time parent and timing of prenatal care access) that would exclude high-risk families with rapid repeat pregnancies that are seen in this study.
The identification of risk profiles associated with presumed PSE represents a significant contribution to the body of maltreatment prevention research. According to our results, over 40% of substantiated cases of maltreatment in infants in Texas from 2009 to 2015 can be attributed to presumed PSE, which is similar to other estimates (Prindle et al., 2018). Among families with substantiated maltreatment associated with presumed PSE, key risk factors included lack of established paternity, less than high school education, smoking during pregnancy, and lack of prenatal care. Based on these data, between 22 and 56% of these infants are removed from the home, depending on the family’s risk profile, making this group a logical target for Family First funded prevention services. It is unclear what percent of these infants were subsequently returned to their home. Give the low rate of re-report to CPS, it is likely that reunification in cases of presumed PSE is uncommon.
Family First has authorized use of federal funds for in-home parent skills building interventions to prevent children from being removed from the home. Many such programs include maltreatment prevention aims, incorporating education in child safety, feeding and nutrition, positive parent-child interaction, and parent mental health support. Our findings suggest that the eligibility criteria of some of these programs may exclude the families most in need of services. Under Family First program guidelines, only the child is eligible for services – not the family—and the child cannot receive services until they are born. Additionally, in Texas and other states, CPS cannot open an investigation prior to birth unless there are other children in the home. Thus, there is a prime opportunity to engage high-risk families in supportive, non-punitive services before the child is born and without the threat of CPS intervention. More than one fifth of infants removed from the home in these data were first births; therefore, the family would not have CPS history. States and programs may need to assess whether eligibility criteria for Family First prevention programs align with the risks and demographics of the families most in need of these services.
While the need for precision-oriented prenatal services is clear, it must be acknowledged that mothers in the PSE classes were the least likely to attend prenatal care. This finding highlights the need for states to invest in outreach to pregnant persons who use substances to increase receipt of prenatal care services and encourage seeking treatment. Additionally, states could leverage community-based implementation of Plan of Safe Care (PoSC) before CPS becomes involved. PoSC was initiated under the federal Child Abuse Prevention and Treatment Act to facilitate both mother and infant receiving treatment and support services (Lloyd, Luczak, & Lew, 2019). Evidence shows that these plans can successfully reduce the probability that the infant is removed from the home (Deutsch et al., 2022).
Within the health system, partnerships between obstetricians, delivery hospitals, treatment facilities, and social services must be developed so that those with substance use issues can receive coordinated support throughout the perinatal period (ACOG, 2015; Council on Patient Safety in Women’s Health Care). Skills such as motivational interviewing and Screening, Brief Intervention and Referral to Treatment (SBIRT) are critical to the success of efforts to engage pregnant women with substance-use problems. States and healthcare systems should invest in training staff and building institutional capacity in these areas so that pregnant persons who seek care are entering a system that is not stigmatizing and supports their treatment process.
Further, medical professionals that provide smoking cessation counselling and products during pregnancy should consider more intense behavioral health counselling for those who do not quit smoking during pregnancy. Our findings suggest that failure to quit smoking may be an indicator of multiple stressors and risk factors that should be addressed as early as possible (Lobel et al., 2008; Riaz, Lewis, Naughton, & Ussher, 2018).
Limitations
A key strength of this study is the use of linked population-level administrative data; such data sets are available to very few states. However, the study is limited by the quality of these data and the specific variables included in them. Administrative data do not permit a comprehensive exploration of social risk. Additional information about family composition and functioning is needed to develop profiles that will help states and service providers to optimally develop precision services that address diverse needs of the families they serve. Future studies should include additional variables and sources of data to advance this work and provide more information about the needs of high-risk families.
Another limitation of this study is that PSE was measured using a proxy indicator, rather than a medical diagnosis or CPS designation. Without a specific CPS code for prenatal substance use or linked health records, no direct measure of PSE is possible. However, researchers in California have linked CPS and hospital discharge data for the 2006 birth cohort; according to their estimates, approximately 30% of infants with substantiated maltreatment were diagnosed with PSE at birth (Prindle et al., 2018). This estimate provides some validation for our measure of presumed PSE (all substantiated physical abuse cases opened within 14 days of birth), which was coded for 40% of our sample. The discrepancy between ours sample and the California study likely reflects the use of older data in the California estimate. Nevertheless, it is likely that our proxy measure under-identifies substantiated cases of maltreatment due to PSE, since not all prenatal drug exposure will result in observable harm to the infant. Some portion of these cases may have been substantiated as SN, which is a common finding for infants as young as 1 week. However, we believe that our indicator generally excludes other forms physical abuse, since it is extremely unlikely that these would occur within the first 2 weeks after birth. Even if our proxy measure identifies some type of maltreatment other than PSE, it is useful know that infants with substantiated maltreatment shortly after birth demonstrate statistically distinct profiles of prenatal risks among compared to infants with maltreatment substantiated later in infancy.
Finally, it should be noted that our findings may not generalize to other states. Texas, much like California, was less impacted by the opioid epidemic during this time frame. Therefore, one would expect states that were more impacted to have a different distribution of PSE, in particular. However, given that our latent classes are largely consistent with existing evidence, there is a strong likelihood that similar results could be found in other states. Additional research would be needed to replicate these findings.
Conclusion
The Family First Prevention Services Act has created a focus on prevention of removal and recidivism of child maltreatment and opened up conversations about primary prevention at state and national levels. The results of the present study have implications both for primary prevention efforts among the general population as well as secondary prevention for CPS-involved families with infants. According to our findings, CPS-involved mothers with some combination of risk factors including high parity, smoking during pregnancy, inadequate prenatal care, and low education are at increased risk for CPS subsequent report and/or removal from the home. Prevention and intervention efforts that address the needs of these populations may be especially effective in reducing maltreatment and its consequences for CPS-involved families. At the population level, improved access to comprehensive prenatal and postnatal care that addresses women’s medical as well as social and behavioral health needs is needed. Community- and healthcare-based prevention efforts should aim to provide women with access to the information and tools they need to ensure that their pregnancies are well-spaced and adequately monitored, and that they receive assistance to address their behavioral health and social needs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this project was through the Texas Safe Babies project (IAC 24307170) from the Texas Department of Family and Protective Services. The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Texas Department of Family & Protective Services.