
Abstract
This was a record-linkage analysis of a birth cohort to examine the association between self-reported self-harm in adulthood and childhood maltreatment (CM) as prospectively notified to authorities and self-reported on the Child Trauma Questionnaire. There were 2507 participants at 30-year follow-up with data on both CM and self-reported self-harm including an intent to die. Of the participants, 304 (12.1%) had self-harmed at some time in their lives while 150 (4.2%) had wanted to die. The prevalence of self- and agency-reported maltreatment was 513 (20.5%) and 143 (5.7%) respectively. On adjusted analyses, CM irrespective of reporting source showed significant associations with both suicidal outcomes. Physical and emotional abuse showed the strongest associations while findings for neglect were mixed. The only association for sexual abuse was for self-reported maltreatment and intent to die but numbers may have been under-powered.
Keywords
Introduction
Suicidal behaviour can range in severity from suicidal ideation through to actions with a serious intent to die (Molnar et al., 2001). Suicidal behaviour is far more prevalent than death by suicide, although there is a wide variation between countries and specific populations. For instance, in a population-based cross-sectional comparison of adults in five European countries (Norway, Spain, Britain, Finland and Ireland), rates ranged from 2.3% in Spain to 14.6% in Ireland (Casey et al., 2008). Lifetime suicidal ideation in adults as measured by community surveys was just under 10% in the United States (Baca-Garcia et al., 2010) and 13% in Australians aged between 16 and 85 years old (Johnston et al., 2009). More serious suicidal ideation or attempts are much rarer at around 1–3% depending on the country and timeframe (Baca-Garcia et al., 2010; Casey et al., 2008; Ivey-Stephenson et al., 2022; Johnston et al., 2009).
Of concern is the increase in incidence in recent years. For instance, there has been a 50% increase in self-harm in middle-aged men, and a 70% increase in young people in the United Kingdom (Kapur, 2020). In a report published in 2019, the risk of suicide after self-harm in England was 50 times higher in the first year after hospital attendance than in the general population, and nearly 200 times higher in the first month (Geulayov et al., 2019).
One potential risk factor for suicidal behaviour is child maltreatment (CM). Most information concerns sexual abuse where several studies have reported strong associations with subsequent suicide attempts (Angelakis et al., 2019; Ng et al., 2018; Zatti et al., 2017). However, other CM types such as physical and emotional abuse are also associated with both suicide attempts and ideation (Angelakis et al., 2019; Zatti et al., 2017). Evidence for neglect is less clear (Zatti et al., 2017). For instance, in one meta-analysis that included cross-sectional and longitudinal designs (k=68 studies), emotional neglect was associated with subsequent suicidal ideation or attempts (Angelakis et al., 2019), while in another smaller systematic review that was restricted to longitudinal studies, it was not (Zatti et al., 2017). However, this negative finding was based on just two studies. It is therefore unclear whether these disparities by CM type reflect true differences or are due to the variations in the number of relevant studies with some types, such as neglect, receiving less attention.
Following their findings that all types of CM were associated with suicidal ideation and attempts, Angelakis and colleagues (2019) proposed that there was a single mechanism for all forms of maltreatment. One possibility is through the association between CM and underlying psychiatric illness such as depression, anxiety, or post-traumatic stress disorder (Angelakis et al., 2019; Ng et al., 2018; Zatti et al., 2017). Externalising personality traits may also be related to suicide attempts (Brezo et al., 2008). However, this does not appear to be the only explanation as the relationship between CM and suicidal ideation or attempts persists after adjustment for comorbid psychiatric symptoms in most work (Brodsky & Stanley, 2008; Marques-Feixa et al., 2021; Molnar et al., 2001) with the exception of one study (Klonsky & Moyer, 2008).
Two sources of information on CM are retrospective reports of adults and prospectively collected notifications to child protection agencies. These sources appear to identify different populations and both have limitations (Baldwin et al., 2019; Najman et al., 2020). For instance, findings from retrospective studies are limited by the potential for recall bias, the use of clinical rather than population samples, and the possibility that childhood maltreatment might be both a cause and effect (Fergusson et al., 2000; Widom et al., 2004).
Studies using prospectively collected reports to child protection agencies are less common. For instance, in two recent comprehensive systematic reviews (Angelakis et al., 2019; Zatti et al., 2017), only one of the included studies looked at agency reported CM and this did not consider subtypes (Brown et al., 1999). However, although studies of agency reported or substantiated maltreatment may not be subject to recall bias, they may underestimate the true prevalence of CM. For instance, the self-reported prevalence of child sexual abuse in one Australian study was approximately 50% in boys and 30% girls (Dunne et al., 2003), whereas agency reported abuse in a prospective study reported a prevalence of only 2% (Mills et al., 2014). As noted previously, there is also poor agreement between self- and agency-reported CM. (Baldwin et al., 2019; Najman et al., 2020). For instance, a recent meta-analysis found that 52% of individuals with prospectively recorded CM did not retrospectively report it, while 56% of those who retrospectively reported maltreatment did not have prospectively recorded data (Baldwin et al., 2019). Similarly, we found a kappa score of only 0.18 for the agreement between the two reporting sources in a previous paper using data from this cohort (Najman et al., 2020).
After investigation, a smaller number of reports to statutory agencies are substantiated. For instance, Australian-wide data indicate that this occurs in 42% of notifications (Australian Institute of Health and Welfare, 2022). However, these may be the most severe cases and therefore an even greater underestimate than notifications of true CM prevalence.
To our knowledge, there has been no study that looked at suicidal behaviour using different reporting sources in the same population. We therefore used a longitudinal, population-based birth cohort to compare self- and agency-reported and/or substantiated CM of different types in terms of their association with self-harming behaviour by 30 years of age. Self-harm with an intent to die was considered separately. We adjusted for sociodemographic characteristics, as well as internalising or externalising behaviour in the young adult years and concurrent depression or PTSD at 30-year follow up. This is because any association between maltreatment and suicidal behaviour might be influenced by pre-existing mental illness, as well as concurrent depression or PTSD, for which childhood abuse is also a risk factor. We hypothesised all forms of CM would be associated with self-harming behaviour regardless of reporting source.
Method
Data Sources
Factors significantly associated with loss to follow-up.
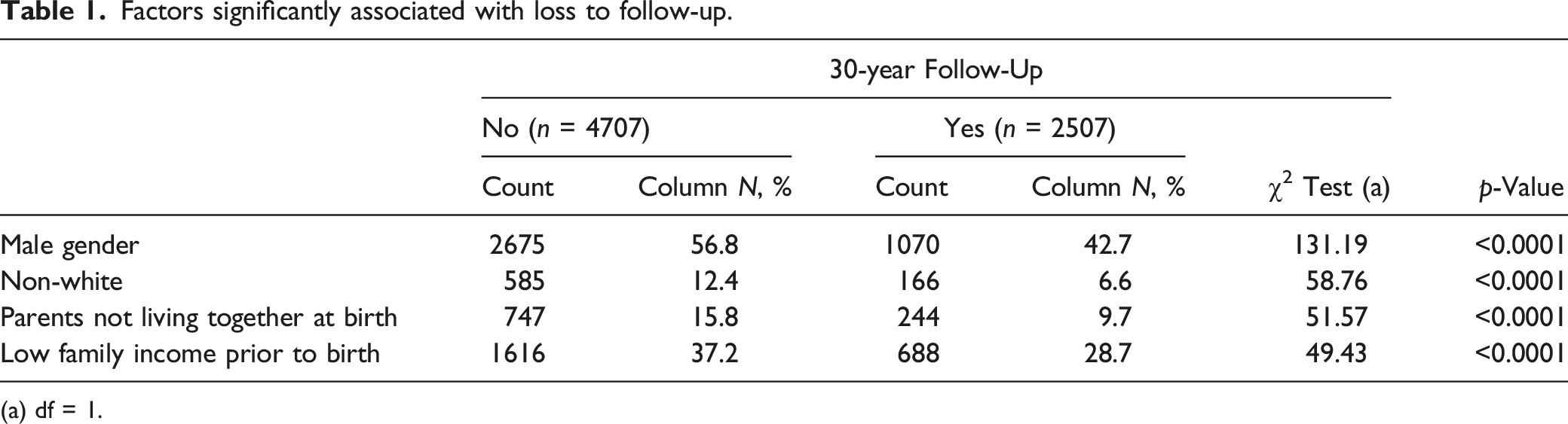
(a) df = 1.
Agency-Reported Child Maltreatment
Information on CM came from notifications to Queensland’s child protection agency, the Department of Families, Youth and Community Care (DFYCC) up to September 2000, at which time participants were approximately 16 years old. We used anonymised identification number to link these data to the MUSP dataset. (Strathearn et al., 2009). These reports were divided into the following subtypes: physical, sexual or emotional abuse, and/or neglect. If there was a reasonable belief of maltreatment after investigation, they were considered as substantiated. All variables were dichotomous in terms of the presence or absence of maltreatment.
Self-Reported CM Measures
We administered the Child Trauma Questionnaire (CTQ) at the 30-year follow-up as it has reliability, sensitivity and discriminant validity (Bernstein et al., 1997). This has 5 sub-scales with 5 items in each and covered events up 16 years old (Bernstein et al., 2003). We combined the physical and emotional neglect scales to enable comparisons with the agency-notified category of “neglect” in the present study, as well as previous MUSP studies on substance use and psychiatric outcomes (Kisely et al., 2020a, 2020b, 2021). This involved selecting the highest level of maltreatment scored on either the physical or emotional neglect sub-scales Both the Kolmogorov–Smirnov and Shapiro–Wilk tests indicated that none of the scores showed a normal distribution (p < 0.0001). In common with previous work on other outcomes in the same cohort, the continuous scores from the subscales were therefore divided into “none/low” and “moderate/severe” but sensitivity analyses were also performed of the effect of splitting the scores into “severe” versus all other categories (Kisely, Abajobir, et al., 2020; Kisely et al., 2021; Kisely et al., 2021b; Kisely et al., 2022; Najman et al., 2020). In particular, this approach was used in our comparison between self-reported and agency reported maltreatment in the same birth cohort, on which the CTQ designer was a co-author (Najman et al., 2020). However, we also undertook sensitivity analyses of using total continuous CTQ scores to facilitate comparisons with other work (Baker & Maiorino, 2010).
Self-Harm
Participants were asked two questions about self-harm coded as yes or no. The primary outcome was whether they had ever hurt themselves on purpose in any way such as by taking an overdose of pills. If so, they were asked if this had occurred in the previous 12 months. The second question was, if on any of the occasions they had self-harmed, they had ever seriously wanted to kill themselves. These questions are similar to those that have been used in other population surveys such as the National Survey on Drug Use and Health in the United States and the Australian National Survey of Mental Health and Wellbeing (Ivey-Stephenson et al., 2022; Pirkis et al., 2000).
Covariates
We adjusted for several variables given their possible association with either child maltreatment or self-harm. These included gender and parental racial origin, as was well as parental relationship status and family income at the time of study entry. This ensured these variables predated any subsequent maltreatment. To these we added internalising and externalising scores at 21 years old derived from the Young Adult Self Report (YASR) questionnaire. The YASR is widely used in the research of young people with most significant psychological symptoms included in one or the other scale. The internalising scale is the total of the subscales of withdrawal, anxious/depressed and somatic symptoms, while the externalising scale is the aggregation of aggression and delinquency symptoms. Both the youth and young adult forms show good reliability, internal consistency, and predictive validity (Achenbach, 1991; Achenbach et al., 1995). As in other work, we dichotomised the scores into the top 10% and bottom 90% (Murray et al., 2010; Spence et al., 2002). This was because of the non-normal distribution of the scores on the Kolmogorov–Smirnov and Shapiro–Wilk tests (p < 0.0001), as well as to simplify the presentation of results and ensure that differences were clinically significant (Farrington & Loeber, 2000; Spence et al., 2002). We undertook sensitivity analyses of the effect of dividing the scores into the top 20% and bottom 80%.
Finally, we adjusted for the following variables at the 30-year follow-up: the offspring’s employment status, their educational achievement, marital and employment status, as well as depression and post-traumatic stress disorder (PTSD) over the 12 months preceding the interview. The latter two were measured using the computerised version of the WHO Composite International Diagnostic Interview (CIDI), a diagnostic interview schedule based on DSM-IV criteria (Peters et al., 1998).
Statistical Analysis
We used logistic regression analysis to control for the covariates with all variables entered into each model at the same time with listwise deletion of missing data. Maltreatment in general was considered, as well as neglect and the emotional, physical, or sexual abuse categories. Each dichotomised CM category was run as a separate model for each outcome. This was because all the CM types showed highly significant associations on chi-square tests (p < 0.0001) and could not therefore be seen as truly independent variables, a requirement for inclusion in logistic regression (Ranganathan et al., 2017). We also undertook a propensity analysis of adding a variable representing the following baseline variables across the whole cohort at risk of exposure to identify possible effects of differential attrition on the association with outcomes at 30 years old: gender, parental race, family income and parental relationship status. Multiple imputation was not used, as this relies on data being missing at random (Najman et al., 2014), which could not be assumed in this case given a statistically significant result for Little's Missing Completely at Random (MCAR) Test (p < 0.0001) and previous findings from the same cohort (Mills et al., 2016).
Finally, we performed three sensitivity analyses. One was of the effect of dividing the internalising and externalising scores into the top 20% and bottom 80%. The second was of the effect of using continuous total CTQ scores. We used non-parametric statistics for bivariate analyses (the Mann-Whitney U test) and adjusted odds ratios for incremental changes in score as neither require a normal distribution. The final was of restricting analyses of our primary outcome of self-harm to events that had occurred in the previous 12 months. The Statistical Package for Social Sciences (SPSS version 27.0) was used for all analyses.
Results
Of the 2507 participants, 57% were females (n = 1437). A fifth of the cohort reported maltreatment at 30-year follow-up (n = 513), and this was severe in 274. This was most commonly neglect (n = 382), followed by emotional (n = 225), sexual (n = 198) and physical (n = 197) abuse. There was a high overlap of subtypes with 210 participants reporting more than one maltreatment category. One hundred and forty-three young adults (5.7%) had been the subject of a notification to Queensland’s child protection agency. Of the subtypes, physical abuse was the most common (n = 75), followed by neglect (n = 65), emotional (n = 61) and sexual abuse (n = 50). Of these, 84 individuals had been the subject of more than type of maltreatment notification. Eighty-three of the 143 notifications (58%) were substantiated (overall prevalence = 3.3%). In order of frequency this was for emotional (n = 39) or physical abuse (n = 34), followed by neglect (n = 31) and sexual abuse (n = 25). There was more than one substantiation type in 36 participants.
Self-Harm
Factors associated with any self-harm at 30 years old and adjusted for all covariates.
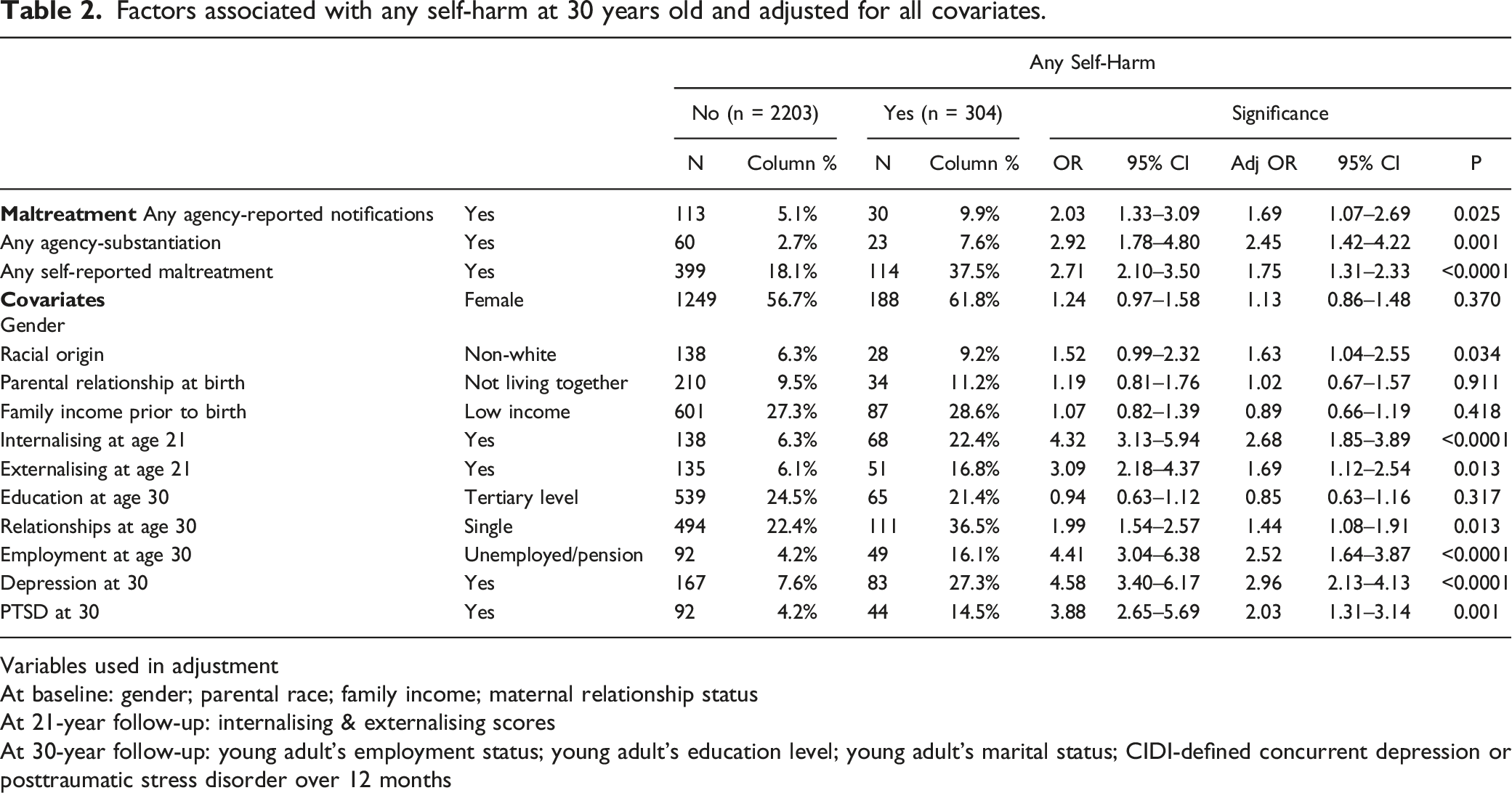
Variables used in adjustment
At baseline: gender; parental race; family income; maternal relationship status
At 21-year follow-up: internalising & externalising scores
At 30-year follow-up: young adult’s employment status; young adult’s education level; young adult’s marital status; CIDI-defined concurrent depression or posttraumatic stress disorder over 12 months
Factors associated with any self-harm at 30 years old in separate models for each maltreatment category and adjusted for all covariates.
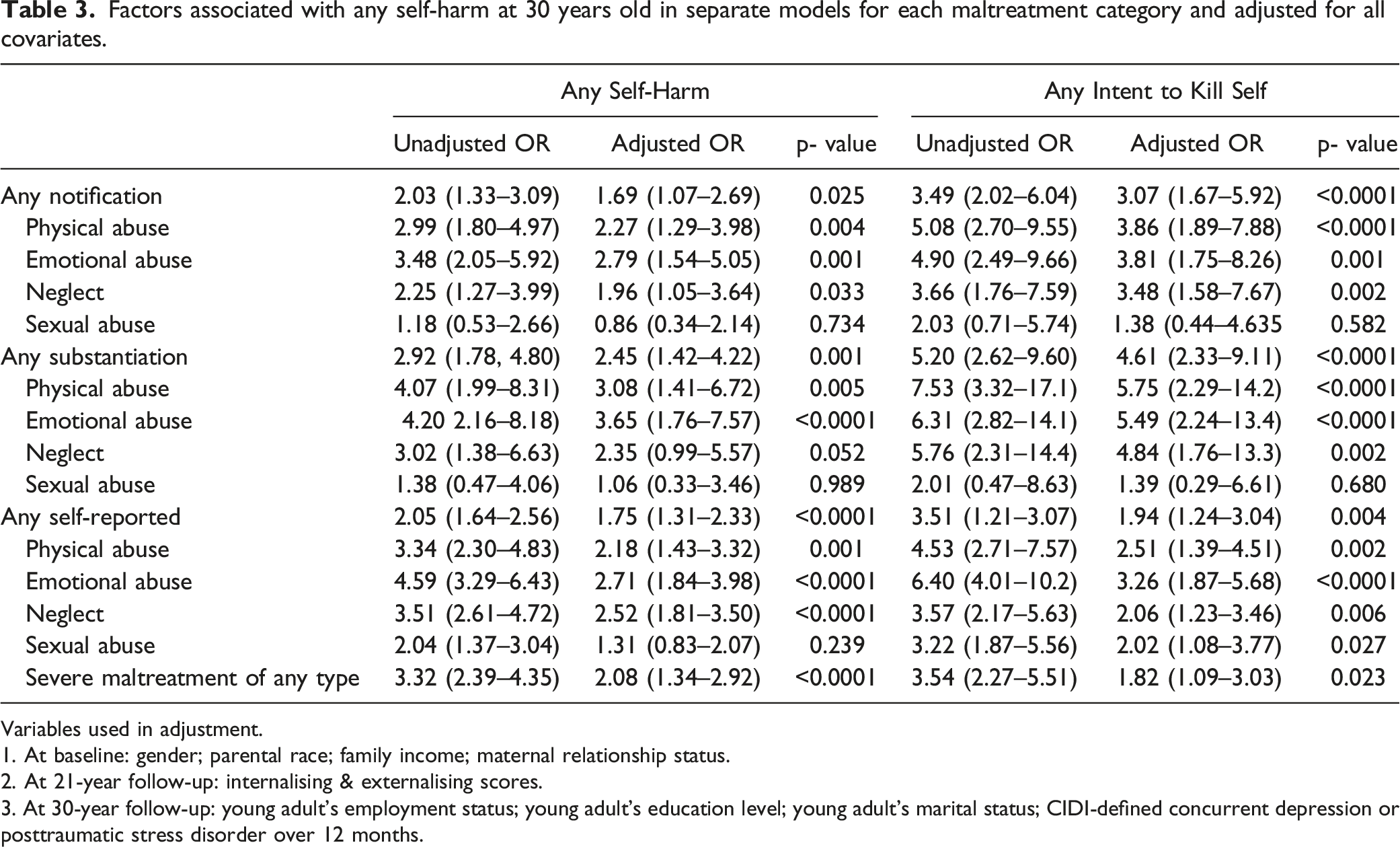
Variables used in adjustment.
1. At baseline: gender; parental race; family income; maternal relationship status.
2. At 21-year follow-up: internalising & externalising scores.
3. At 30-year follow-up: young adult’s employment status; young adult’s education level; young adult’s marital status; CIDI-defined concurrent depression or posttraumatic stress disorder over 12 months.
There were similar results for self-harm with the intent to die where all forms of self- and agency-reported maltreatment, including neglect, showed a significant association with the sole exception of agency-reported or substantiated sexual abuse (Table 3). As before, the associations were strongest for self-reported CM, moderate or severe (Table 3).
Propensity and Sensitivity Analyses
Propensity score analyses adjusted for all covariates.
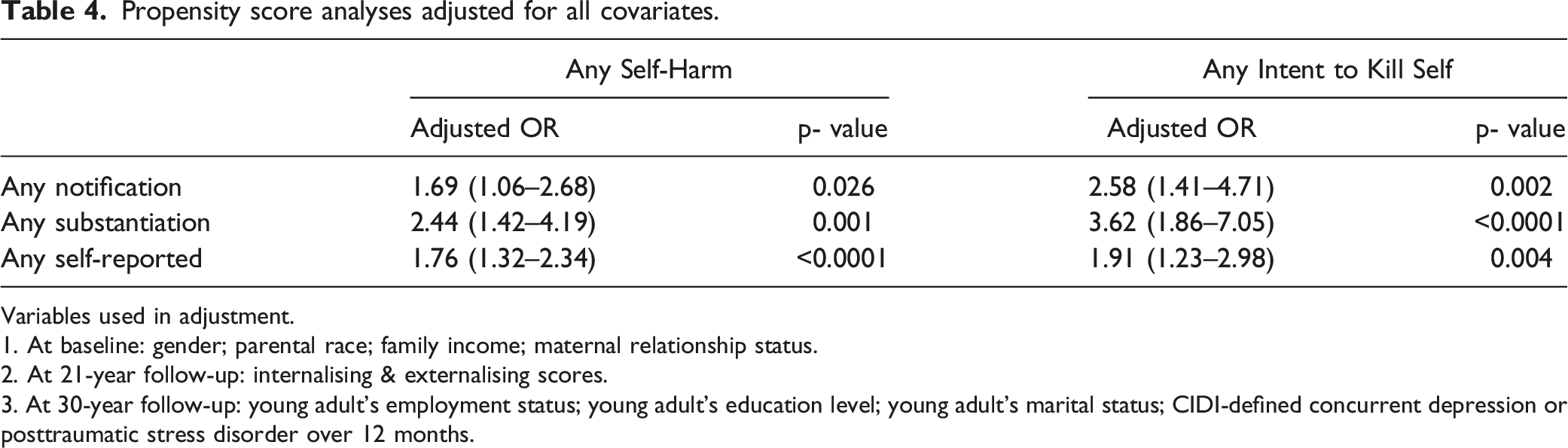
Variables used in adjustment.
1. At baseline: gender; parental race; family income; maternal relationship status.
2. At 21-year follow-up: internalising & externalising scores.
3. At 30-year follow-up: young adult’s employment status; young adult’s education level; young adult’s marital status; CIDI-defined concurrent depression or posttraumatic stress disorder over 12 months.
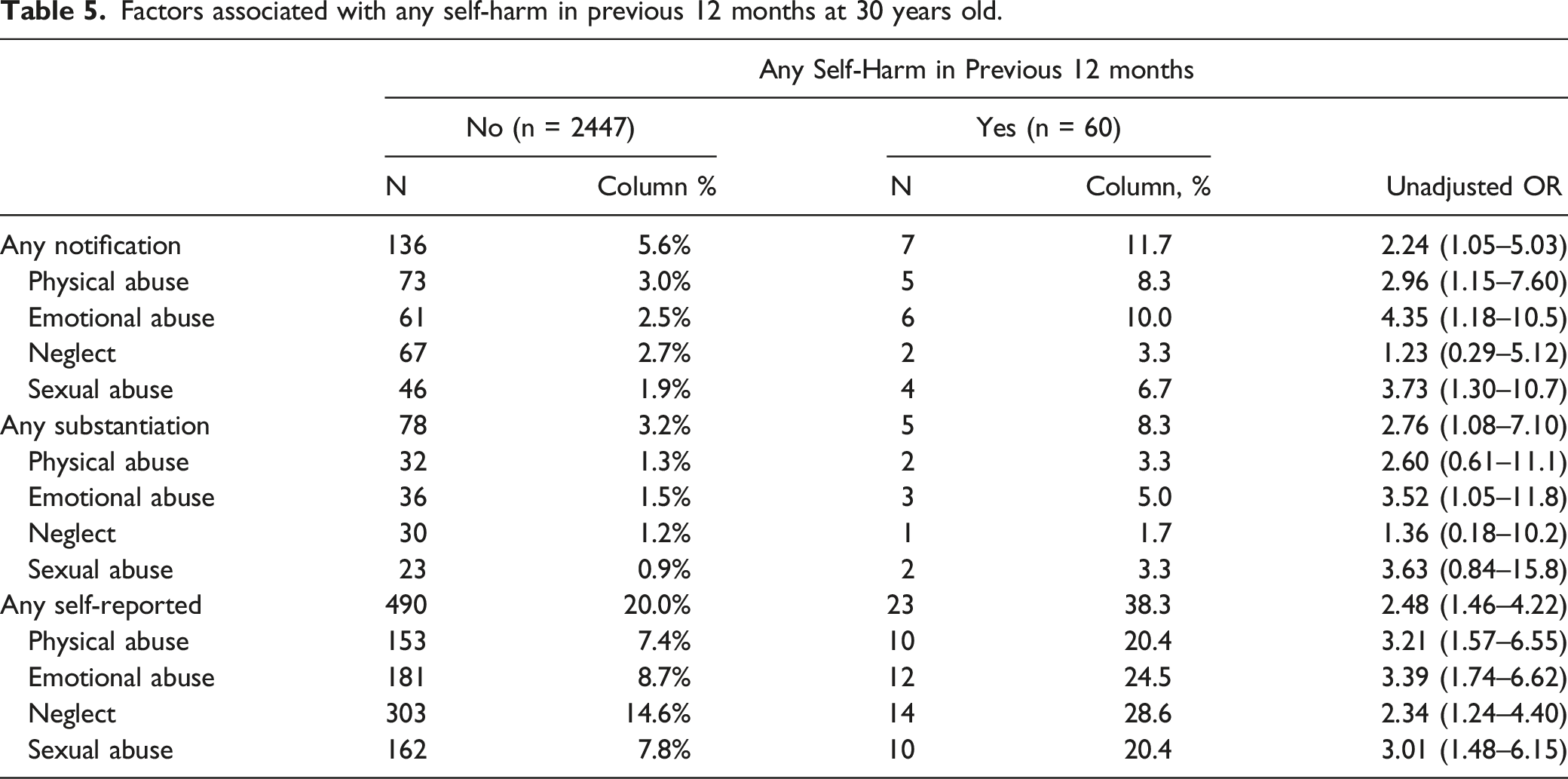
Factors associated with any self-harm in previous 12 months at 30 years old.
Discussion
Most of the information on the association on childhood maltreatment and suicidal or self-harming behaviour comes from cross-sectional or longitudinal studies of adults who retrospectively report childhood abuse (Angelakis et al., 2019; Ng et al., 2018; Zatti et al., 2017). For instance, two recent systematic reviews of the subject found only one study that looked at agency reported CM (Angelakis et al., 2019; Zatti et al., 2017), and this did not consider the subtypes (Brown et al., 1999). To our knowledge, this is therefore the first paper to consider and compare the long-term effects of both self- and agency-reported CM of all types on self-harming behaviour in adulthood in the same population-based cohort.
In terms of prevalence, 12% of the sample reported that they had self-harmed up to the age of 30 years old, of whom 105 (4.2%) said they had wanted to die. This is consistent with lifetime rates of suicidal ideation/behaviour in United States but at the higher end of cross-sectional prevalence as reported in Europe (Baca-Garcia et al., 2010; Casey et al., 2008). The presence of maltreatment irrespective of reporting source showed a significant association with both measures of self-harming behaviour. In terms of the subtypes, physical and emotional abuse, whether self- or agency reported/substantiated, were also significantly associated with self-harm of both forms. Neglect, irrespective of reporting source, was associated with an intent to die. By contrast, associations for agency reported sexual abuse were non-significant, while self-reported sexual abuse was only associated with intent to die.
Importantly, we considered both self- and agency-reported CM. This is because prospective and retrospective measures of childhood identify different groups of individuals with comparatively little overlap between the two groups (Baldwin et al., 2019; Najman et al., 2020). These differences cannot be solely attributed to recall bias as there is evidence that people are generally accurate in their reports of childhood maltreatment experiences (Pinto et al., 2014). However, discrepancies can occur in one of two directions (Baldwin et al., 2019). Over-reporting may occur through suggestibility or negative bias as a result of depression at the time of assessment. Under-reporting may be due to deficits in memory coding, consolidation or retrieval because of impaired brain function or the absence of accompanying emotional distress. Despite these disadvantages, it is also possible that self-reported data may be more comprehensive and accurate than agency-reported, which may focus on the most extreme or severe event with physical evidence to support the claim. For example, agency reports may only be submitted when there is physical risk to the child, thereby missing experiences of abuse and neglect that are less easily recognisable by others (Baldwin et al., 2019).
The above concerns especially apply to the smaller number of substantiated cases, which accounted for 58% of notifications, a similar percentage to that reported in South Australia during the same reporting period (Winefield & Bradley, 1992). There may be several reasons for the relatively high level of unsubstantiated notifications. It might be that the criteria for substantiation are too stringent or there are insufficient resources to fully investigate reports (Winefield & Bradley, 1992). Conversely, some of the notifications may be inaccurate (Winefield & Bradley, 1992). Some work suggests that the caseworker's estimate of severity is an independent predictor of substantiation (Winefield & Bradley, 1992).The latter finding would be consistent with our finding that substantiated cases had worse outcomes than those that were only notified. By contrast, other authors have reported that the distinction between notification and substantiation does not greatly affect outcome, suggesting that notified cases can be used as an overall indicator of CM (Drake, 1996; Hussey et al., 2005; Kohl et al., 2009). We have chosen to present findings for using substantiation, both as a marker of severity, and to allow comparison with work using either substantiated or notified CM.
Our finding that self-harming behaviour was consistently associated with emotional and physical abuse, irrespective of source, is consistent with that from studies restricted to self-reported cases (Angelakis et al., 2019; Zatti et al., 2017). The more equivocal findings for neglect also mirror findings in self-reported maltreatment (Zatti et al., 2017). However, unlike other papers and contrary to expectations, sexual maltreatment showed the weakest association with the only significant result being for self-reported abuse and intent to die. One explanation for the non-significant findings for agency reported sexual abuse was that our study was underpowered to detect statistical significance. This is further discussed under limitations. However, this would not explain similar findings for self-reported sexual abuse where numbers were higher.
One strength of this paper is adjustment for concurrent PTSD and depression given these are associated with both childhood maltreatment and self-harming behaviour. We also adjusted for internalising and externalising scores at 21 years old. Adding these variables into our models did not abolish the association between CM and self-harming behaviour suggesting that these are unlikely to be the only explanation for our findings. One suggestion is that depression, anxiety, PTSD and suicidality show similar and independent associations with perceptions of defeat and entrapment (Siddaway et al., 2015).
Limitations
There are several limitations to the study. This is a 30-year follow-up and so attrition, which was associated with markers of social deprivation, may limit the study’s generalisability (Kisely, Strathearn, et al., 2020). Although we were able to test for MCAR using Little's test, we cannot exclude the possibility that data were missing at random (MAR). However, recent findings from this cohort suggest that the rate of loss to follow-up, for both dependent and independent variables, has little effect on estimates of association and so is less important as a source of bias (Saiepour et al., 2019). For instance, multiple imputation of data from this cohort changes neither the estimates nor their precision (Najman et al., 2014; Saiepour et al., 2019), and this is consistent with findings of the effects of differential attrition in other longitudinal studies (Wolke et al., 2009). In addition, our findings were generally the same on propensity score analyses that considered baseline covariates across the entire at-risk cohort.
Another limitation is that the relatively few agency-notified or substantiated cases, particularly those of sexual abuse, are probably an under-estimate of the true prevalence and therefore of insufficient power to detect statistical significance for some of the outcomes. All the CM categories showed highly significant associations with each other and could not therefore be seen as truly independent variables, a requirement for inclusion in a single logistic regression model. As a result, we had to run each dichotomised CM category in separate models and so were unable to account for any overlap between the CM types. In addition, we were unable to explore the effect of the age when the CM occurred. Notified or substantiated cases may also reflect the reporting practices of 15–20 years ago.
The self-harm outcomes were self-reported and not confirmed through other sources. We therefore have no indication of the severity. Neither did we consider death by suicide. Nevertheless, suicidal or self-harming behaviour is often a precursor to non-fatal repetition or death by suicide. For instance, about 1.6% of those seen in hospital after self-harm die by suicide in the following year (House & Owens, 2020). Conversely a quarter of all suicides in the UK have attended an acute hospital after self-harm in the previous 12 months (House & Owens, 2020). Use of lifetime self-harm as the primary outcome meant that it was impossible to determine whether this preceded or followed self- and agency-reported CM. There were also insufficient numbers to comprehensively look at people who said they had self-harmed in the previous 12 months.
Implications
At the individual level, clinicians should be aware of the increased possibility of a past history of CM in people presenting with self harming behaviour and be comfortable with screening for this possibility. Similarly, those who have been subjected to CM should be asked about previous or current ideas or acts of self-harm. At a population level, interventions to prevent maltreatment may help to reduce suicide rates. Examples include home visiting by nurses particularly for those families at greatest risk (Olds et al., 1997). This can reduce both CM and its mental health consequences such as depression in adolescence and adulthood.
Further research is indicated to compare the effects of agency- and self-reported maltreatment to better reflect the more recent policies for reporting and investigating CM given the present dataset reflects the practices of 15–20 years ago. Other areas of possible investigation include the effect of when the maltreatment occurred and the characteristics of the perpetrator, as well as the impact on death by suicide.
In conclusion, these findings suggest that suicidal behaviour may be a further adverse consequence, amongst many, of childhood maltreatment, so highlighting the public health importance of the issue. In particular, these results emphasise the importance of physical and emotional maltreatment in terms of suicidal ideation and behaviour. This suggests that reducing CM may have a role in the primary prevention of deliberate self-harm and suicide. In addition, people presenting with self-harming behaviour should be screened for the possibility of CM.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.