
Abstract
Preadolescents with a history of foster care placement report suicidal ideation (SI) at higher rates than their peers, which increases their risk for suicide attempts in adolescence. Despite these increased risks, few interventions have been shown to reduce SI in these youth. This study examined the main and mediated long-term effects of a program to increase school readiness in children in foster care at age 5 years on SI when the children were ages 9–11 years, 4–6 years after the intervention ended. Children who received the intervention were less likely to report SI, although the difference did not reach statistical significance. The intervention reduced SI indirectly through its positive effect on children’s self-esteem at age 9 years. Implications for programming to reduce SI and subsequent suicide attempts in youth with a history of foster care are discussed.
Maltreatment and subsequent placement in foster care exact a heavy toll on children, placing them at risk for a range of disadvantageous social, mental, and physical health sequalae across the lifespan (Carr et al., 2020; Mills et al., 2013; Vachon et al., 2015). Although any of these sequalae can be harmful, suicidal ideation (SI) is one of the most potentially life threatening because it increases risk for both immediate and future suicide attempts (Copeland et al., 2017) and is more frequent in youth with histories of maltreatment and involvement with the child welfare system (CWS) than in other youth (Gomez et al., 2017; Katz et al., 2011; Taussig et al., 2014). Further, these higher rates are apparent as early as preadolescence (Taussig et al., 2014; Thompson et al., 2005). Despite this increased and early-onset risk for SI, there are few preventive interventions specifically designed for youth in foster care (Russell et al., 2021). To address this critical need, this study examines whether an intervention designed to promote school readiness in children with histories of maltreatment and placement in foster care could also reduce SI in preadolescence both directly and indirectly through self-esteem. If an early school readiness intervention can also impact later SI, this could broaden the range of programs available to reduce SI, and potentially later suicide attempts, in these extremely vulnerable youth.
Suicidal Ideation in Preadolescents
SI in youth is an important marker of immediate risk for suicide attempts and death by suicide, as well as a robust predictor of such behaviors into adulthood (Copeland et al., 2017). One meta-analysis of studies across primarily adolescent samples indicated that youth involved in the CWS have a 25% prevalence rate of SI versus 11% for youth not involved in the CWS (Evans et al., 2017). Although less research has examined SI in preadolescents, two large general population studies, one in the U.S. using the nationally representative Adolescent Brain Cognitive Development Study and the other in Belgium, found the prevalence of SI to be approximately 11% in 9–10-year-olds (DeVille et al., 2020; Van Hove et al., 2021). The only published study to examine SI specifically for 9–11-year-olds who had experienced both maltreatment and placement in foster care found the prevalence of SI to be 17% (Taussig et al., 2014). It should be noted that measures in these studies included both passive (thoughts of suicide without intent) and active (a desire to kill oneself) ideation.
The Need for Early Preventive Interventions
Although SI does not always lead to suicide attempts, it is a known risk factor (Copeland et al., 2017; Franklin et al., 2017). Further, an earlier onset of SI significantly increases the risk of later depression, suicide plans, and attempts (Castellví et al., 2017; Hill, et al., 2020). This suggests that intervention in childhood to forestall the development of ideation might reduce risks for longer-term ideation, attempts, and death by suicide. Unfortunately, a recent systematic review of interventions across the globe found that only two evidence-based interventions reduced SI in youth in foster care, and both were focused on adolescents (Russell et al., 2021).
Importantly, neither of those two programs targeted SI directly (Russell et al., 2021). Instead, they focused on building positive skills in the youths and/or their caregivers. A treatment foster care program provided individual therapy and training in such skills as emotional and behavioral regulation for the adolescent and training in positive parenting skills for the foster caregivers (Kerr et al., 2014), whereas the other program focused on helping adolescents develop their emotional intelligence, including their abilities to regulate emotions and their feelings of self-competence (Bonet et al., 2020). These programs’ promotion of positive skills in the adolescents and their caregivers may have had a shielding effect on youth, protecting them from a range of potential negative outcomes (Spoth et al., 2009). Researchers have recently suggested testing whether early interventions that promote potential shielding factors have effects on risk outcomes that were not originally targeted by the intervention (i.e., crossover effects), particularly in vulnerable populations for which evidence-based interventions may be limited (Reider et al., 2014; Spoth et al., 2019). Given findings that promoting positive skills in adolescents in foster care prevented SI, it is important to determine whether earlier programming to promote positive skills in children in foster care might prevent or reduce later SI.
School Readiness as a Shielding Factor
One set of positive skills that appear to confer a range of advantages on individuals across time is school readiness—a construct comprised of academic, prosocial, and self-regulation skills and contextual factors that are associated with academic achievement and behavioral success in school (e.g., Duncan et al., 2007; Goble et al., 2019; Sabol & Pianta, 2017). Long-term positive outcomes associated with school readiness include higher academic achievement, graduation rates, and educational and occupational attainment as well as better mental and physical health (Campbell et al., 2014; Jones et al., 2015; Ramey & Ramey, 2004; Reynolds et al., 2011). School readiness also reduces the likelihood of adolescent parenthood, delinquency, and substance abuse, behaviors that, like SI, may place individuals at risk for poor mental health outcomes (Goble et al., 2019; Jones et al., 2015; Reynolds et al., 2011).
The domains that comprise the broader construct of school readiness have individually and collectively been linked to a range of positive outcomes, including reduced SI. Critical academic skills include early literacy skills that are positively linked to academic achievement across elementary and middle school (Duncan et al., 2007). Academic achievement has consistently been found to be a protective factor for youth in preventing or reducing SI both concurrently and longitudinally (e.g., Godwin & Conduct Problems Prevention Research Group [CPPCRG], 2020; Zhu et al., 2019), including specifically for youth with a history of placement in foster care (Berlin et al., 2011). Children’s prosocial skills (e.g., sharing, recognizing emotions, entering peer groups, and maintaining social interactions) are also critical to school readiness, and strong interpersonal skills are associated with a lower risk of SI in both preadolescents and adolescents (Godwin & CPPCRG, 2020; Roberts et al., 2018; Thompson et al., 2005). Self-regulation skills (e.g., children’s abilities to voluntarily regulate emotions and behaviors in different situations) predict better engagement in learning, academic achievement, and social skills (Braak et al., 2022; Rademacher et al., 2021; Williford et al., 2013). Better abilities to regulate one’s own emotions and behaviors are also protective factors against SI over time (Godwin & CPPCRG, 2020; Lockwood et al., 2017), particularly for youth involved with the CWS (Yoon et al., 2018).
Contextual factors contributing to school readiness are family involvement in schooling and positive parenting. Family involvement in schooling (e.g., helping the child with home learning and school activities, attending school events) predicts better school readiness, later academic achievement, and school adjustment (Lerner & Grolnick, 2020; Slicker, et al., 2021). Greater parental involvement also reduces SI in youth (MacPherson et al., 2021; Tian et al., 2021). Positive parenting practices—supportive, consistent discipline and monitoring—predict better school readiness and school functioning (Lunkenheimer et al., 2008; Votruba-Drzal et al., 2021). Such parenting practices are also associated with a decreased risk for SI in youth (Kingsbury et al., 2020) whereas negative parenting is associated with increased risk (Kasen & Chen, 2020). Given the wide-ranging effects of school readiness and its individual components on later outcomes, and the specific associations with SI in preadolescents and adolescents, it is likely that intervention to increase school readiness in young children could reduce their risk for later SI.
School Readiness, Self-Esteem, and the Development of Suicidal Ideation
School readiness may also reduce suicidal ideation through its positive effect on another robust predictor of suicidal behaviors. Self-esteem has been shown to play a role in protecting youth in the general population against SI and attempts (e.g., Jakobsen et al., 2017; Zhu et al., 2019). Importantly, two studies have shown that self-esteem mediates the link between child maltreatment and suicidality in adolescents and emerging adults in the general population (Cero & Sifers, 2013; Duprey et al., 2019). Although studies of youth in foster care have not yet focused on the specific association between self-esteem and SI, self-esteem does appear to protect these youth against a number of behaviors that have been linked to higher risk for suicidality—namely depression, internalizing, externalizing, and criminality (Barn & Tan, 2012; Mihalec-Adkins & Cooley, 2020; Thompson et al., 2016; Valdez et al., 2015).
There are a number of reasons why school readiness might lead to increased self-esteem. First, children specifically knowing the expectations for school prior to starting has been linked to their feeling good about themselves and their school. (O’Farrelly et al., 2020). Second, specific skills that comprise school readiness are associated with self-esteem. Higher academic abilities, social competence, and self-regulatory abilities all predict better self-esteem in children and youth over time (Caprara et al., 2013; Djambazova-Popordanoska, 2016; Metsäpelto et al., 2020; Yang et al., 2019). Finally, the contextual factors that comprise school readiness affect youth self-esteem. Positive parenting is linked to increased self-esteem in children and adolescents (Pali et al., 2022; Pinquart & Gerke, 2019), and family involvement in schooling can improve children’s self-esteem (Lerner & Grolnick, 2020). Given the strong associations between self-esteem and suicidal behaviors, examining whether interventions to improve school readiness might decrease the likelihood of SI through positive effects on self-esteem is warranted.
Goals of the Study
This study examines both the direct and indirect (through increases in self-esteem) effects of an intervention designed to promote school readiness in children in foster care on their SI at ages 9–11 years. The Kids In Transition to School (KITS) Program (Pears et al., 2018) is a focused, short-term intervention for children in foster care and their caregivers to increase school readiness prior to kindergarten entry and to promote better subsequent school functioning. It occurs in the 2 months before kindergarten entry and the first 2 months of kindergarten. The program features a group-based school readiness curriculum for children with foci on early literacy, prosocial, and self-regulation skills, and groups for parents and other caregivers, that include content on caregiver involvement at home and school and positive parenting skills.
The KITS Program increases early literacy and self-regulation skills in children in foster care and decreases their teacher-reported disruptive behaviors during kindergarten (Pears et al., 2013: Pears et al., 2012). Further, children in foster care who participated in the KITS Program were less likely to have positive attitudes toward alcohol use and antisocial behaviors at age 9 years than their peers. Such positive attitudes can be precursors of later delinquency and drug use (Andrews et al., 2008), which are risk factors for SI (Franklin et al., 2017). Of particular relevance to the present study, participation in the KITS Program increased self-esteem at age 9 years, which prevented deviant peer association (Pears et al., 2016). This positive effect of KITS on later self-esteem, and the association between self-esteem and SI in the literature, warrant exploration of potential links between the KITS Program, self-esteem, and early SI.
In this study, we hypothesized that children who participated in KITS at age 5 years would be less likely to report having SI at any point when they were aged 9–11 years. We examined the presence of any SI because we were interested in whether the intervention could reduce or prevent the occurrence of any ideation and because we suspected that the behavior would not occur commonly enough to be able to examine patterns of ideation across time. We also hypothesized that the effects of KITS on SI would be at least partially mediated through the previously established link between KITS and self-esteem at age 9 years. This study expands upon previous findings by examining whether the demonstrated increases in self-esteem had longer-lasting effects on behaviors through ages 9–11 years. If an early intervention can affect later SI in children with a history of foster care, this would add to the few programs that have been shown to be efficacious for these highly-vulnerable youths and might help to reduce or prevent long-term SI and potential progression to suicide attempts in adolescence.
Method
Participants
One hundred ninety-two children and their caregivers participated in the randomized clinical trial of KITS and the subsequent longer-term follow-up (Pears et al., 2013). Children were eligible to participate if they were entering kindergarten in the fall of the year they enrolled in the study, in kinship or nonkinship foster care at the time of recruitment, and a monolingual or bilingual English speaker. Children were ineligible if they were involved in another treatment protocol closely associated with the KITS intervention. Once they were enrolled in the study, children continued to be eligible for treatment activities (if applicable) and follow-up assessments regardless of foster care involvement at those timepoints.
During the recruitment period, a research staff member first contacted an eligible child’s caseworker (i.e., the legal guardian while the child is in foster care) to request consent for the child to participate and then contacted the caregiver(s) to invite them to participate. Both the caseworker and caregiver(s) had to consent for the child to participate in the study. Because of the complexity of this multistep process, all families were randomized to the KITS group or to a foster care services as usual (SAU) group prior to contacting the caseworker and caregiver(s). If the child changed placements during the course of the study, the staff contacted the new caregivers and went through the consent process. Every effort was made to follow children across placements whenever possible, including out-of-state travel to conduct assessments.
Demographic Characteristics.
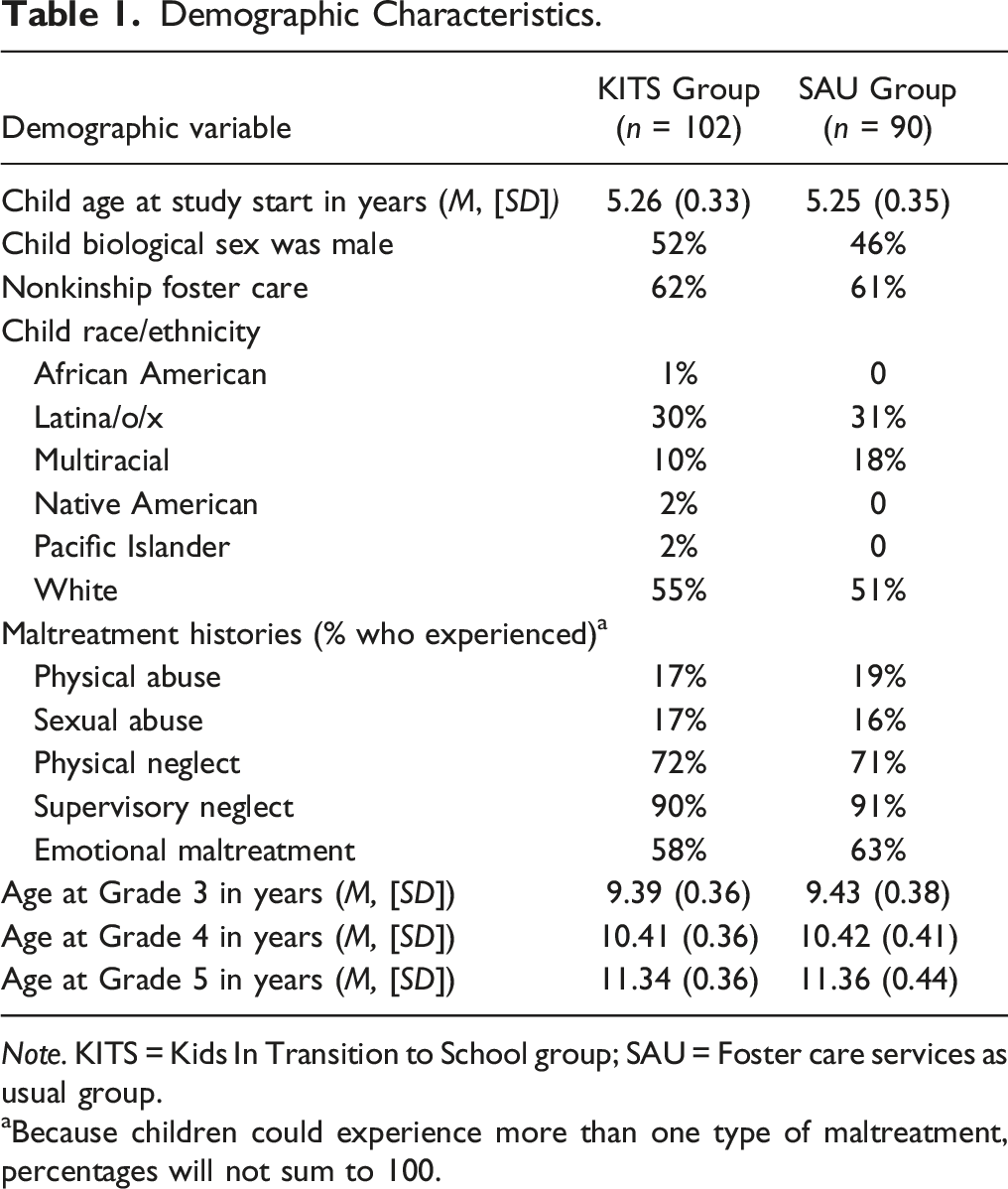
Note. KITS = Kids In Transition to School group; SAU = Foster care services as usual group.
aBecause children could experience more than one type of maltreatment, percentages will not sum to 100.
Study Design and Procedures
This study was registered with ClinicalTrials.gov (Identifier NCT00688129). Children and their caregivers participated in center-based assessments that employed standardized testing, questionnaires, and structured interviews at the beginning of the summer before kindergarten prior to the intervention, at the end of the summer just prior to kindergarten entry (age 5 years), at the end of the kindergarten year (age 6 years), and at subsequent school years through Grade 5 (ages 7–11 years). Assessments typically lasted from 1.5 to 2 hr. Caregivers were compensated for their time with a stipend. Children received a small gift at the end of each assessment until age 11 years when they were offered a small stipend. Teachers completed questionnaires (not utilized in this study) on the child’s behaviors at the end of each school year.
Intervention Protocol
The KITS intervention, consisting of child school readiness and caregiver groups, occurred during 2 months of the summer prior to kindergarten entry and the first 2 months of kindergarten in the fall. The 24-session school readiness groups (2 hr, twice weekly in the summer, 16 sessions; 2 hr, once weekly in the fall, 8 sessions) focused on promoting early literacy, prosocial, and self-regulatory skills. Coinciding with the children’s group times, the caregiver groups met for eight sessions every other week during the summer and fall (2 hr) and focused on promoting caregiver involvement in learning at home and school and positive parenting techniques. More information about the development of the intervention can be found in a prior publication (Pears et al., 2013).
School Readiness Group Structure and Curriculum.
The KITS school readiness group sessions were held in center- or school-based classrooms and had a highly structured, consistent routine similar to that of a typical kindergarten classroom. The manualized curriculum covered three critical skill areas: (a) early literacy skills (e.g., letter names, phonological awareness, conventions of print, and comprehension); (b) prosocial skills (e.g., reciprocal social interaction, social problem solving, and emotion recognition); and (c) self-regulatory skills (e.g., handling frustration and disappointment, paying attention, following multistep directions, and making appropriate transitions). The curricular objectives for each skill domain and the activities to promote these skills were clearly specified for each session. For example, the early literacy activities included a letter of the day (letter naming and letter-sound knowledge), a poem of the week (phonological awareness, concepts about print, and language), and storybook and dramatic activities (understanding of narrative). Self-regulatory and prosocial skills were taught using a blend of instruction (e.g., teachers defined calm bodies and provided verbal examples), role-playing (e.g., teachers modeled being calm and not being calm), and activity-based intervention (e.g., children were reinforced for maintaining calm during a very exciting class activity). As is noted above, it was expected that learning school readiness skills would increase children’s feelings of self-esteem both because the children might feel more confident about school and because of the links between better academic and social-emotional skills and greater self-esteem (Djambazova-Popardanoska, 2016; O’Farrelly et al., 2020). Additionally, to increase both their self-esteem and their motivation to learn new skills, the children received high rates of encouragement, feedback, and guided practice in using the target skills. A lead and two assistant teachers conducted each school readiness group that contained 12–15 children.
Caregiver Group Structure and Curriculum.
Each KITS caregiver group of 12–15 individuals was led by a facilitator and an assistant. The manualized curriculum emphasized positive parenting skills (e.g., supportive, consistent discipline and monitoring), caregiver involvement in preparing for school (e.g., helping children to develop early literacy skills, developing routines around school activities), and becoming involved at school (e.g., how to volunteer in the classroom). As is noted above, the use of positive parenting techniques and caregiver involvement in school are both positively linked to children’s self-esteem (Lerner & Grolnick, 2020; Pali et al., 2022). The group facilitator presented information, led structured group discussions, facilitated caregiver-to-caregiver support, and addressed questions and concerns. Skill acquisition was reinforced via role plays and opportunities to practice new skills. Supplemental materials to support skill practice included weekly homework assignments for the child to complete with the caregiver, weekly Home–School Connection newsletters outlining the school readiness group topics for a given week, and home practice activities for the caregiver. Facilitators visited or called any caregiver who missed a session to cover the content and materials for that session.
If a child changed placements during the intervention, their new caregiver was invited to join the groups, and the facilitator provided the content from any previous sessions. Training for implementing KITS consisted of a 20–30 hr standardized program. The intervention team met weekly to discuss children’s and families’ progress and plan strategies to address children’s behavioral and literacy needs and caregivers’ engagement within the broader curricula.
Dosage and Implementation Fidelity.
All intervention dosage (i.e., attendance at groups and make-up sessions) was documented. On average, the children attended 69% of the group sessions, with 57% of them attending 75% or more of the sessions. Caregivers received 61% of the sessions on average, with 55% receiving 75% or more of those sessions. Implementation fidelity for the school readiness groups was assessed by trained observers in vivo or via videorecording based on systematic coding of the presence or absence of key elements of the curriculum (98% of the curriculum components were covered; range = 75–100%). Observers also rated the teachers on implementation of key behavior management strategies (e.g., Pre-taught expectations) on a 3-point scale: 1 (none of the time), 2 (some of the time), and 3 (all of the time). The average rating was 2.86. Implementation fidelity for the caregiver groups was determined via caregiver ratings of whether the weekly topics had been covered (100% of the components were covered).
Foster Care Services as Usual Group
Children in the SAU group received services commonly offered by the CWS. These could include individual child psychotherapy, participation in an early childhood education program, and services such as speech therapy. No attempt was made to influence the type or amount of services received by children or their families in either the SAU or KITS groups.
Measures
Suicidal Ideation during Preadolescence.
At ages 9, 10, and 11 years, the child’s SI was measured using a single item from the Children’s Depression Inventory (Kovacs, 1992). Children were asked to choose the statement that best described them in the past 2 weeks: I do not think about killing myself, I think about killing myself but would not do it, or I would like to kill myself. For descriptive purposes, endorsing the statement, I think about killing myself but would not do it, was considered to indicate passive SI, and the statement, I would like to kill myself, was considered indicative of active SI. A single, dichotomous outcome variable was created for SI. A ‘1’ indicated any endorsement of SI across the three timepoints while a ‘0’ indicated no endorsement of ideation.
If children endorsed any SI, a follow-up was immediately conducted, which included questions about the child’s intent to attempt suicide and (if necessary) a plan. If immediate intent and/or a plan was established, a licensed clinician who was not a part of the research team conducted a follow-up assessment with the child and talked with the child’s caregiver. The child was informed during the assent process that their caregiver would be told if there was concern that they planned to harm themselves. A safety plan was established with the child and caregiver before they left the assessment, which might have included referrals for mental health services or contact with an existing mental health provider.
Self-Esteem at Age 9 Years.
Children’s self-esteem was assessed at age 9 years using the 6-item Global Self-Worth Scale of the Self-Perception Profile for Children (Harter, 1985; 1988). Children were asked to pick the option that best described them from statements phrased as follows: Some kids like the kind of person they are BUT Other kids often wish they were someone else. Once they selected the statement that best described them, they were asked to indicate if it was really true for me or sort of true for me. Higher scores indicated higher self-esteem. The scale showed strong internal reliability in the sample (standardized α = .78).
Children’s Internalizing Behavior at Baseline.
At the baseline assessment at age 5 years, caregivers completed the Child Behavior Checklist for ages 4–18 years (Achenbach, 1991). The raw subscale scores for internalizing (standardized α = 0.85) were utilized to control for baseline levels of internalizing behavior.
Analytic Plan
Main and mediation models for binary outcomes were estimated in Mplus version 8.4 (Muthén & Muthén, 1998–2017) using WLSMV estimation with a probit link and delta parameterization. The mediated intervention effect was tested using the MODEL INDIRECT command and 95% bootstrapped confidence intervals (with 5000 random draws) using the product of coefficients method (i.e., a*b). Child internalizing behaviors at age 5 years were included as a predictor of SI to control for any potential differences that could be explained by differences in earlier internalizing behaviors. In addition, to utilize the full sample and accommodate missing data, the variance of child internalizing behaviors at baseline was included in both models. To obtain standardized model results, both child internalizing behaviors at age 5 years and self-esteem at age 9 years were standardized based on all available data, and intervention condition was dummy coded (1 = KITS group, 0 = SAU group). We first descriptively examined the prevalence of both passive and active SI in the sample. Second, we tested the hypothesis that there would be a significant main effect of the KITS intervention on reduced SI at ages 9–11 years. Finally, we tested the hypothesis that the KITS intervention would have an indirect effect on reducing SI through improved self-esteem at age 9 years.
As would be expected in a longitudinal study of a highly mobile sample, there were some missing data. Of the 192 youth, 125 answered the SI item at least one time between the ages of 9 and 11 years (ns =113 at age 9, 104 at age 10, and 103 at age 11 years). Eighty-three youth had data at all three assessments, 29 at two, and 13 at a single assessment. Regarding missing data patterns for the study variables, 110 youth had no missing data; 62 had baseline internalizing scores only; 11 were missing self-esteem only; 3 were missing internalizing behaviors only; 1 was missing suicide ideation only; 1 was missing both self-esteem and internalizing; and finally, 4 had no data and were thus excluded from the analyses. There were no differences between the KITS and SAU groups on the likelihood of missing data for SI, self-esteem, or internalizing.
Results
Descriptive Analyses
Predictor and Outcome Variable Descriptives by Group.
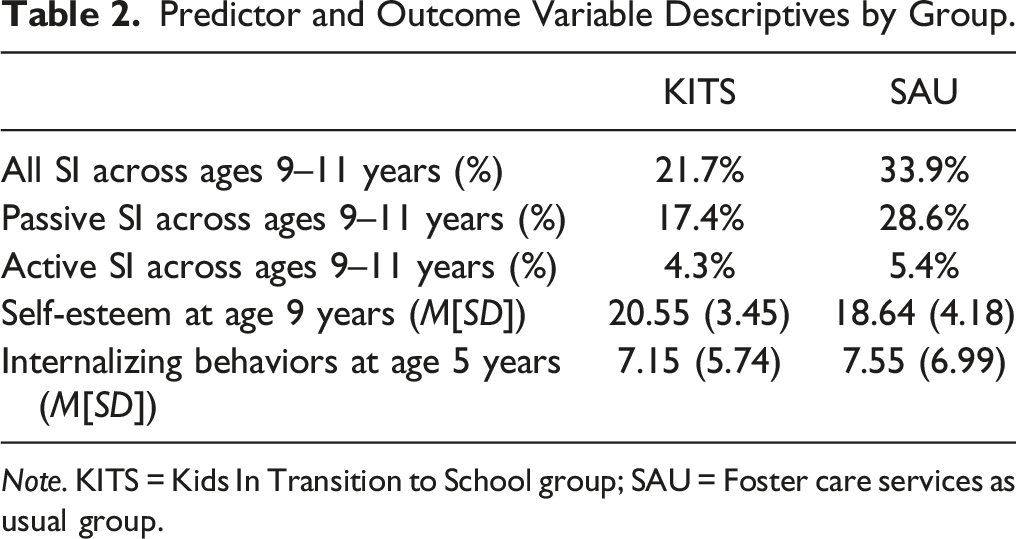
Note. KITS = Kids In Transition to School group; SAU = Foster care services as usual group.
Prevalence of Suicidal Ideation.
Between the ages of 9 and 11 years, 27.2% of youth endorsed SI with or without intent at one or more assessments. The prevalence across the sample of endorsing passive SI (i.e., I think about killing myself but I would not do it) was higher (22.4%) than that for active SI (i.e., I would like to kill myself; 4.8%). As shown in Table 2, the overall rate of SI was higher in the SAU group (33.9%) than in the KITS intervention group (21.7%); however, this difference did not reach statistical significance (OR = .54, 95% CI = [.24–1.20], χ2(1) = 2.32, p = .128).
Model Analysis
Model results did not support a main intervention effect of KITS on SI at ages 9–11 years (β[SE] = −0.37 [.25], p = .138; 95% CI = [−0.85, 0.12]), nor were child internalizing behaviors significantly associated with subsequent self-reported SI (β[SE] = 0.05 [.13], p = .678; 95% CI = [−0.22, 0.28]). However, as depicted in Figure 1, the KITS intervention was effective at increasing youth self-esteem at age 9 years, which was in turn associated with a reduced likelihood of endorsing SI at ages 9–11 years (ab[SE] = −0.18 [0.09], p< .05; 95% CI = [−0.40, −0.05]). Thus, improved self-esteem is a key mechanism through which the KITS intervention reduces concurrent or subsequent SI, beyond differences that can be explained by children’s scores at age 5 years on the broader spectrum of internalizing behaviors. Model of Indirect Effects of the Kids In Transition to School Group Intervention on Suicidal Ideation in Preadolescents. Note. Numbers denote β(SE), 95% CI; Indirect effect ab(SE) = −0.18 (0.09)*, 95% CI = (−0.40, −0.05); RMSEA = root mean square error of approximation; CFI = comparative fit index; TLI = Tucker-Lewis index; SRMS = standardized root mean square residual; **p < .01. *p < .05.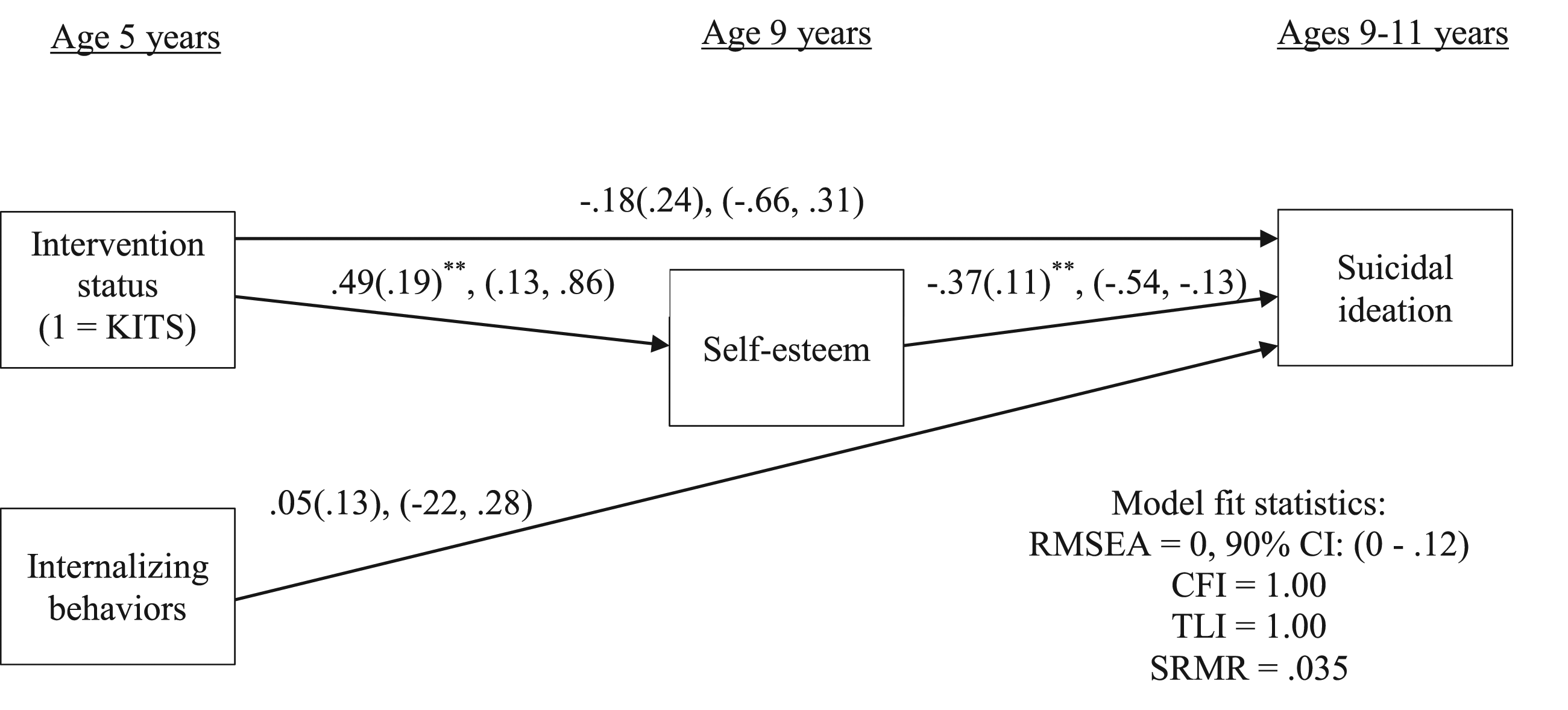
Discussion
Over one quarter of preadolescents (27.2%) with a history of placement in foster care in this study experienced either passive or active SI, a rate more than double that in the general population of preadolescents (DeVille et al., 2020; Van Hove et al., 2021). Research shows that SI increases in adolescence; thus, the relatively high prevalence in these preadolescents suggests that these rates (and the likelihood of suicide attempts) could continue to grow as they get older (Castellví et al., 2017; Copeland et al., 2017). Preventing the development of SI could avert long-term difficulties and growing risks to these youths’ lives.
This study examined whether strengthening children’s readiness for school would directly and indirectly reduce later SI. The KITS Program was specifically designed to improve the early literacy, prosocial and self-regulation skills of children in foster care, as well as their caregivers’ involvement in learning and positive parenting skills, factors shown to reduce SI in both general and foster care populations (e.g., Godwin & CPPRG, 2020; Yoon et al., 2018). In this study, the direct effect of the KITS Program on youths’ SI 4–6 years after the intervention was not significant. However, the rates of SI were 12% lower in the youths who were randomly assigned to receive the KITS intervention than in those assigned to foster care services as usual.
The KITS Program had a significant indirect effect on SI in preadolescence through its positive effects on the children’s self-esteem at age 9 years. The finding that the KITS intervention indirectly affected SI through self-esteem is perhaps not surprising, given that the intervention was not originally designed to target SI. A burgeoning literature has begun to highlight the positive crossover effects of early preventive interventions (e.g., Connell et al., 2021; Reider et al., 2014) on a range of negative outcomes. As is noted above, researchers have suggested that such crossover effects may be due to the positive influence of the interventions on skills or other factors that shield the youth from involvement in later problematic behaviors (Reider et al., 2014; Spoth et al., 2009). The current study’s finding that positive intervention effects on self-esteem led to reduced SI adds to the literature suggesting that self-esteem may be a particularly important shielding factor for children with a history of foster care (Barn & Tan, 2012; Mihalec-Adkins & Cooley, 2020; Pears et al., 2016; Thompson et al., 2016; Valdez et al., 2015). Importantly, this study used prospective longitudinal data to demonstrate this effect in preadolescents, whereas most prior studies have focused on adolescents and young adults.
Limitations and Future Directions
Although this study has a number of strengths—including the use of prospective, longitudinal data and the inclusion of early internalizing behavior as a control variable—some limitations should be noted. The sample size was relatively small, especially compared to some larger population-based studies of suicidal ideation. However, unlike the present study, these larger studies have not often focused on youth in foster care, who can be highly mobile and thus difficult to follow over time. There was also temporal overlap between the proposed mediator, self-esteem, and one timepoint at which SI was assessed. Further, to assess SI in the youth, only one self-report item was utilized. The one other study of SI in preadolescents in foster care specifically targeted this behavior and thus utilized multiple measures (Taussig et al., 2014). Additionally, in the current study, the measure of ideation was combined across three timepoints to indicate whether the youth had ever experienced SI. Although the rate of SI in this sample was high relative to the youth without a history of foster care, it was still a low-base rate behavior at any one timepoint, making it difficult to examine frequency or patterns of SI. The low base rate and sample size also precluded exploring moderation by child biological sex or race or ethnicity. Future studies, particularly those with larger samples, should include multiple measures of both SI and attempts as well as examine patterns of ideation and moderation by factors such as race.
Conclusion
This study has shown that early intervention to improve school readiness for children in foster care reduces later SI, adding to past studies showing that school readiness programming can have broad positive effects on long-term outcomes that were not originally targeted by the interventions (e.g., Campbell et al., 2014; Jones et al., 2015; Reynolds et al., 2011). It has also highlighted the positive effects of self-esteem on outcomes for youth with a history of foster care. Such evidence suggests targets for interventions that might be less stigmatizing than other more negatively viewed behaviors, such as aggression or depression. Additionally, such broadly impactful programs could be particularly cost effective if they reduce the need for multiple programs designed to intervene after the youths develop problematic behaviors, although interventions to address acute suicidality in the moment, such as safety planning (Rogers et al., 2022), are likely to always be needed. Overall, this study underscores the critical importance of early intervention for youth in foster care to strengthen positive skills and long-term resilience.
Footnotes
Acknowledgment
The authors thank Sally Schwader for editorial assistance, and the staff and families of the Kids In Transition to School project for their ongoing dedication and participation.
Declaration of Conflicting Interests
Katherine Pears is a developer of the Kids in Transition to School Program.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We received funding for this project through grant R01DA021424 from the National Institute on Drug Abuse, U.S. PHS and grant R01MH124437 from the National Institute of Mental Health, U.S. PHS. The content of this article is solely the responsibility of the authors and does not necessarily represent the official views of the funding organizations.