
Abstract
Maternal exposure to childhood maltreatment (CM) is associated with offspring behavioral problems; however, little work has examined these associations longitudinally across child development. This study examined the effects of maternal history of CM on trajectories of child internalizing and externalizing behavior measured from toddlerhood to preschool, and the role of maternal depressive symptoms and parenting behavior as potential mediators. Participants included 115 mother–child dyads recruited from a hospital maternity ward. Maternal CM was measured at 3-months postpartum. At 18, 36, and 60 months, maternal depressive symptoms and child behavior were assessed via maternal report and parenting behavior was assessed through direct observation. Findings indicated that children of mothers exposed to CM demonstrated poorer trajectories of problem behavior across early childhood. Maternal depressive symptoms mediated the relation between CM and children’s internalizing problems. Findings highlight the importance of screening for maternal depressive symptoms and early intervention for maternal and child mental health.
Introduction
Emerging research on the intergenerational transmission of trauma demonstrates that parental experiences of childhood adversity are associated with compromised developmental outcomes in offspring. Specifically, children of mothers exposed to child maltreatment (CM), including emotional, physical, and sexual abuse, and emotional and physical neglect, are at a greater risk for increased internalizing and externalizing behavior problems in early childhood (Plant et al., 2018). The intergenerational effects of CM may operate by negatively influencing various aspects of the caregiving context, such as parenting behavior (Collishaw et al., 2007; Rijlaarsdam et al., 2014) and maternal mental health (Choi et al., 2019; Plant et al., 2017). While this evidence base is growing substantially, there is a notable gap, with few studies examining associations between maternal history of CM, trajectories of child problem behaviors, and relevant mediators across various developmental stages.
Therefore, the purpose of this study was to examine the effects of maternal exposure to CM on patterns of change in internalizing and externalizing behavior measured from toddlerhood to preschool. Furthermore, we investigated potential indirect effects of CM on child behavior through maternal depressive symptoms and parenting behavior. The study design and analyses are informed by the ecological-translational model of child maltreatment, which describes the interaction of several ecological contexts, including family environment and ontogenetic development, that carry risk and protective factors for the parent (Belsky, 1980). When risk factors outweigh protective factors, dysfunctional parental mood and behavior, and compromised child outcomes are more likely to occur. Given that behavioral and social-emotional difficulties in early childhood are risk factors for impairment across multiple domains, including lower academic achievement (Turney & McLanahan, 2015) and future psychopathology (Mesman & Koot, 2001), longitudinal investigations are important in understanding the pervasive effects of parental CM on offspring adjustment. Such research can help inform approaches to intervention to reduce the long-term consequences associated with the intergenerational transmission of risk.
Maternal Child Maltreatment and Patterns of Change in Child Behavioral Problems
Exposure to CM has a widespread influence on adult functioning, including increased risk of physical and mental health concerns (Norman et al., 2012). In addition, an emerging literature provides evidence for the effects of CM across generations. These effects are evident early and have been shown across multiple domains of offspring development and functioning, including low birth weight (Racine et al., 2018) and insecure attachment (Berthelot et al., 2015). Notably, links between maternal CM and internalizing and externalizing difficulties in offspring have been demonstrated at various ages across early childhood (Cooke et al., 2019; Madigan et al., 2015; Pereira et al., 2018; Thomas-Argyriou et al., 2020) through adolescence (Negriff et al., 2020). In a recent cross-sectional study, child age (range = 1.5 to 18 years) did not emerge as a significant moderator in the relationship between maternal CM and children’s problem behaviors, suggesting that this association persists across development (Stepleton et al., 2018). These findings highlight that maternal experiences of CM may constitute a risk for offspring behavioral problems. Despite the consistency of these cross-sectional findings at various ages, significant gaps remain regarding the relation between maternal CM and longitudinal patterns of change in internalizing and externalizing behavior across child developmental stages.
Patterns of change in child behavioral problems during sensitive developmental periods is important to model in order to understand how maternal CM may be related to maladaptive trajectories in offspring. While externalizing behaviors during toddlerhood are to some extent age-appropriate and typically peak around 2 years, children experience normative declines in these behaviors throughout early childhood (Fanti and Henrich, 2010; Gilliom & Shaw, 2004) through the development of adaptive skills and behavioral regulation (Campbell, 2002). In contrast, internalizing behaviors gradually increase during this period, likely reflective of increased cognition and improvements in the capacity to remember and anticipate negative events (Fanti and Henrich, 2010; Gilliom & Shaw, 2004). However, some children demonstrate persistent externalizing problems or elevated trajectories of internalizing behavior across early childhood, which are associated with a higher risk of adjustment problems in early adolescence, including engagement in risky behaviors and peer relationship difficulties (Fanti and Henrich, 2010; Sterba et al., 2007). Predictors of such elevated symptomatology include maternal psychopathology (Sterba et al., 2007) and socioeconomic disadvantage (Fanti and Henrich, 2010). To our knowledge, only one study to date has examined associations between maternal childhood abuse and trajectories of child behavior. Children whose mothers reported severe abuse had a greater persistence of adjustment problems, including conduct problems and emotional symptoms, between ages 4 and 7 years, in comparison to other children (Collishaw et al., 2007). Further research is needed to understand how maternal history of CM contribute to different patterns of child externalizing and internalizing behavior, and whether parental exposure to CM is related to the persistence or escalation of symptoms overtime.
The Role of Maternal Depressive Symptoms
Maternal depressive symptoms may be an important mediating factor in the intergenerational transmission of CM. The associations between and adult mental health outcomes are well established, with higher risk of a diagnosis of depression and higher depression symptoms scores in individuals exposed to CM (Humphreys et al., 2020). In addition, children of mothers with depressive symptomatology have been shown to display higher levels of internalizing and externalizing behavior (Goodman et al., 2011), likely through negative influences on infant stress physiology (Khoury et al., 2016) and the disruption of secure attachment (Atkinson et al., 2000). In line with this evidence, maternal depressive symptomatology has been identified as an important mediator in the relation between maternal CM and child internalizing and externalizing behavior (Choi et al., 2019; Cooke et al., 2019; Madigan et al., 2015). For example, in a community sample, maternal depressive symptoms partially mediated the association between maternal maltreatment history and child internalizing and externalizing behavior at 5 years (Pereira et al., 2018).
The Role of Parenting Behavior
Maternal history of CM may also be linked to later child outcomes through negative parenting practices. Caregivers exposed to CM face challenges across different domains of parenting behavior, including decreased sensitivity (Gonzalez et al., 2012) and use of authoritarian or permissive parenting (Leslie & Cook, 2015). A recent meta-analysis by Savage and colleagues (2019) showed evidence for a small, but significant association between maternal history of maltreatment and insensitive caregiving behavior. The impact of maternal CM on parenting may be attributed to underlying influences on parental stress physiology (Gonzalez et al., 2012) and attachment (Gonzalez et al., 2009), which in turn, also undermine a parent’s capacity to sensitively attend and respond to their child’s needs. Importantly, positive caregiving behavior is also a strong predictor of healthy social and emotional development in children. Longitudinal studies have demonstrated links between insensitive parenting behavior and internalizing (Kok et al., 2013) and externalizing problems (Halligan et al., 2013) in early childhood. Sensitive parenting shapes the development of secure attachment and models adaptive processes for regulating emotions (Halligan et al., 2013; Madigan et al., 2015). Children are then less susceptible to developing internalizing and externalizing behaviors. Accordingly, findings support an indirect pathway linking parental experiences of CM to offspring problem behaviors via dysfunctional parenting processes, including maternal hostility and harsh discipline (Collishaw et al., 2007; Rijlaarsdam et al., 2014), although other studies have failed to find such evidence (Bosquet Enlow et al., 2016; Madigan et al., 2015).
The Current Study
Despite a growing body of literature on the intergenerational effects of CM, a better understanding of the impact of maternal history of CM on child behavior across various developmental stages, and mechanisms that may underlie these associations, is needed. Using a longitudinal approach, the objectives of the current study are to (1) investigate whether maternal CM predicts differences in patterns of change in child internalizing and externalizing behavior from toddlerhood (18 months) to preschool (60 months), and (2) test whether the associations between maternal CM and child behavioral problems is mediated by either maternal depressive symptoms or parenting behavior. Modeling associations between maternal CM and trajectories of child behavioral problems, and the identification of aspects of the caregiving environment that may be implicated, can inform the development of preventative interventions to mitigate the intergenerational effects of CM and promote positive child development.
Methods
Design and Participants
Mothers and their children were part of a longitudinal study focused on the effects of maternal cognitive function on parenting and child development from birth to age 5 years. Participants were recruited from the maternity ward at St. Joseph’s Healthcare, Hamilton, Ontario. Study inclusion included the following: (a) age 18 years or older at time of birth; (b) gave birth to a full-term, healthy infant; (c) custody and access of their infants at the time of home visits; and (d) able to read, write, and speak English. Any barriers to completion of research measures, such as severe disability were exclusion criteria. Ethics approval was obtained by the McMaster Research Ethics Board and the St. Joseph’s Healthcare Hamilton Research Ethics Board. Visits took place between May 2011 to January 2018, when children were approximately 3 (n = 141), 18 (n = 108), 36 (n = 96), and 60 months (n = 91) of age.
Maternal age ranged from 19 to 43 years (M = 31.31, SD = 5.18) at recruitment. The majority of mothers were married or living common law (92.5%) and were university educated (56.2%). Child mean ages at each visit were as follows: visit 1: 4.03 (SD = 1.28), visit 2: 19.28 (SD = 1.32), visit 3: 39.79 (SD = 1.22), and visit 4: 61.81 (SD = 2.17) months. The median household income ranged between $80,000–112,999 CAD. Fifty-four percent of children were female and 82.4% were White. At each visit, dyads participated in a 2-hour home assessment completed by two trained female research assistants. At the first visit, mothers retrospectively reported on their history of childhood maltreatment. At 18, 36, and 60 months, mother–child interactions were videotaped, and mothers completed questionnaires about their depressive symptoms and their child’s socioemotional functioning and behavior (Harris et al., 2021).
Measures
Child Maltreatment
The Childhood Trauma Questionnaire (CTQ; Bernstein & Fink, 1998) is a 28-item retrospective, self-report questionnaire measuring exposure to maltreatment before the age of 18, including five sub-types: emotional, physical and sexual abuse, and emotional and physical neglect, with higher total scores indicating greater severity of trauma exposure. Standard cut-off scores define the severity of exposure to each of the childhood maltreatment subtypes ranging from none to low, moderate, or severe. The CTQ has demonstrated strong psychometric properties (α = .96; Paivio & Cramer, 2004). Participants received a score of “1” for each type of maltreatment exposure (i.e., emotional, physical and sexual abuse, and emotional and physical neglect) based on low to moderate cut-offs from the CTQ. Responses were summed for a total score ranging from 0 to 5. Internal consistency in the present sample was high (Cronbach’s α = .91).
Child Internalizing and Externalizing Behavior
To assess child behavior, mothers completed the Child Behavior Checklist for ages 1.5–5 years (CBCL/1.5–5; Achenbach and Ruffle, 2000), consisting of 99 items representing parent perceptions of child internalizing and externalizing behaviors within the preceding 2 months. The internalizing scale consists of four subscales: emotionally reactive, anxious depressed, withdrawn, and aggressive behaviors. The externalizing scale includes two subscales: attention problems and aggressive behaviors. The psychometric properties of the CBCL are excellent (Achenbach and Ruffle, 2000). In the current study, the CBCL demonstrates good internal consistency at each time point for internalizing (.77 ≥ Cronbach’s α ≤ .86) and externalizing (.89 ≥ Cronbach’s α ≤ .92) scales. Total internalizing and externalizing scores were used in the current study. Both subscale scores can range from 20 to 80, with higher scores indicating greater problematic child behaviors.
Parenting Behavior
Parenting behavior was measured through videotaped interactions between the mother and child at 18, 36, and 60 months postpartum. At the 18-month visit, dyads participated in a free play interaction (5 minutes), a “play with toys” interaction in which a standardized set of toys were provide (5 minutes), and then a “divided attention task” in which mothers were asked to complete a short survey in the presence of their infant (10 minutes). At the 36-month visit, dyads were instructed to engage in a free play interaction (4 minutes) followed by a challenging puzzle task (4 minutes) and the divided attention task (4 minutes). At the 60-month visit, dyads engaged in a free play interaction (5 minutes) and then an Etch-a-Sketch task (Stevenson-Hinde & Shouldice, 1995). Mothers and their children were each assigned a knob and instructed to use the Etch-a-Sketch to replicate two pictures provided: two stacked rectangles (practice trial) and a house (test trial). No set time for completion was given.
All videos were scored by four trained and certified coders using the Emotional Availability (EA) Scales, fourth Edition (Biringen et al., 2014), a measure of the emotional quality of mother–child interactions. The EA Scales consist of four caregiver dimensions: sensitivity, structuring, nonintrusiveness, and nonhostility. Across all dimensions, scores range from 1 to 7, with higher values reflect higher emotional availability. The EA scales have been validated across a range of child ages (infancy to middle childhood) and in low and high-risk populations (Biringen et al., 2014). Interrater reliability was established for 10% of the videos. Intraclass correlation coefficients (ICCs) for pairs of raters before discrepancy resolution were .75 at 18 months, .75 at 36 months, and .81 at 60 months. The four caregiver dimensions were significantly correlated (r > .35); therefore, a mean score was computed as an indicator of parenting behavior at each time point.
Maternal Depressive Symptoms
The Center for Epidemiological Studies Depression (CES-D) Scale was used to assess maternal depressive symptoms. The CES-D is a 20-item self-report questionnaire designed to assess depressive symptoms in the past 7 days (Radloff, 1977). Scores >16 indicate clinically significant levels of depression. The CES-D has demonstrated strong psychometric properties in diverse groups (Weinberg et al., 2001). In the present sample, the scale demonstrated high internal consistency at each time point (.88 ≥ Cronbach’s α ≤ .91).
Statistical Analyses
Missing Data
Participants missing child behavioral data at all three time points were excluded from the analysis (n = 26). Therefore, included participants were 115 mothers and their children. Independent samples t-tests and chi-square tests were run to assess whether participants included in analyses differed from those not for several variables (i.e., maternal CM, depressive symptoms, maternal age, and maternal education). Participants included in the analysis did not differ significantly from those excluded. For included participants, 65% had child behavioral data for all three visits, 22% of participants had data from two time points, and 13% had data at one time point. Results indicated no significant differences between participants with data at all three time points and those without in variables including maternal CM, depressive symptoms, maternal age, maternal education, and household income. Missing data at each wave of data collection ranged from 0% to 6.59% for main study variables. Full-information maximum likelihood (FIML) estimation was used to account for missing data in analyses (Enders, 2010).
Growth Curve Analyses
To address our first objective, multilevel modeling (MLM) was used to model child internalizing and externalizing behavior trajectories (Singer & Willett, 2003). Growth curves were estimated in Mplus 8 software (Muthén & Muthén, 1998–2017). The time variable corresponded to child age, in months. Observations at child age 18, 36, and 60 months were coded as 0, 18, and 42 months, respectively, to set the starting point of the analysis to zero. First, unconditional growth curves were estimated separately for internalizing and externalizing behavior to identify significant variance in the intercept and slope (Model A). A linear growth model, including fixed and random linear time effects, and a fixed quadratic model were tested. A quadratic slope can be tested with three time points; however, the variance of the quadratic slope needs to be fixed to zero (Hoffman, 2015). Unconditional growth curve models were used to model changes in child behavior overtime, on average, without including confounding factors. Next, potential covariates, including household income, maternal age, marital status, number of siblings, and child sex, were added individually to the model. Covariates that were significant or approached significance (p < .10) and that improved the fit of the model were retained in order to control for variables related to outcomes, while providing a parsimonious representation of findings (Singer & Willett, 2003): Household income (sum of mothers’ and partners’ salaries) and child sex (coded as 1 = male and 0 = female). Externalizing behavior was included as a covariate in the growth model of internalizing behavior, and vice versa, to control for confounding effects. Then, maternal CM was added to the model to examine effects on both intercept (i.e., average level at 18 months) and slope (i.e., rate of change overtime; Model B). Predictors were grand-mean centered (i.e., intercept represents the estimated initial status for an individual with an average value for that predictor). Model fit was assessed by comparing Bayesian information criterion (BIC) and Akaike’s information criterion (AIC) values between models, with lower values indicative of better fit.
Mediation Analyses
To address our second objective, multilevel mediation analyses were conducted to investigate whether patterns of parenting behavior and maternal depressive symptoms mediated the association between maternal CM and child behavior (Supplemental Figure 1). A 2→1→1 approach was employed, in which a Level-1 (time-varying) variable mediates the effect of a Level-2 (time-invariant) variable on time-varying outcomes (Krull & MacKinnon, 2001). Estimates of the a pathways (i.e., relation between the independent variable and the mediator), the c pathways (i.e., relation between the independent variable and the outcome), and the ab indirect pathways must occur at a between-person level, given that the independent variable is constant within an individual. Estimates of the b pathway (i.e., the relation between the mediator and the outcome at level-1) were disaggregated into between- and within-person effects (Krull & MacKinnon, 2001). Between-person effects were assessed using time-averaged measures (i.e., average level across assessment waves) that were grand-mean centered and entered at Level-2, and focused on the effects of CM on child behavior at age 60 months. Within-person effects (i.e., within-person variations in the predictor across time) were entered as person-mean centered predictors at Level-1. The significance of the ab pathway was tested by building 95% confidence intervals (CIs) in RMediation using the distribution of the product method (Tofighi & MacKinnon, 2011).
Results
Descriptives and Correlations
Descriptives of the Analysis Variables.
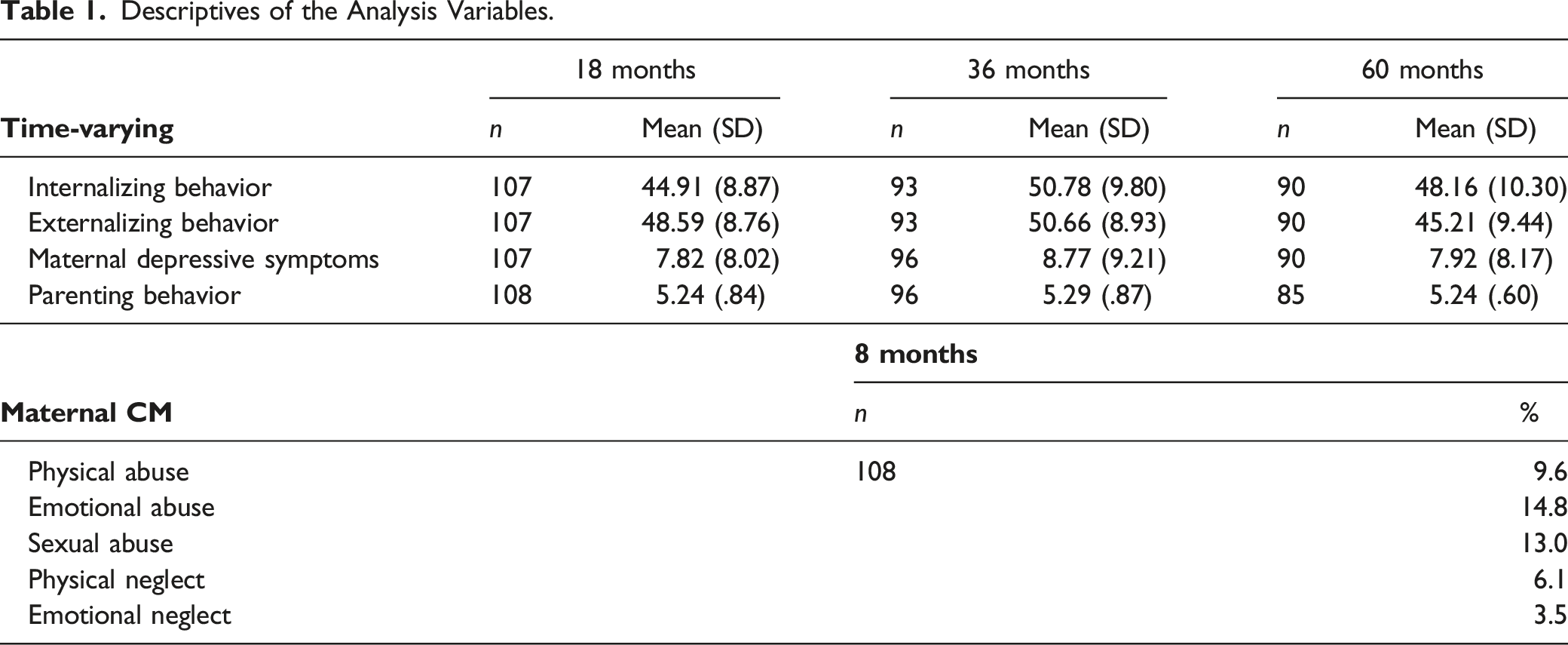
Bivariate Correlations Among Study Variables.
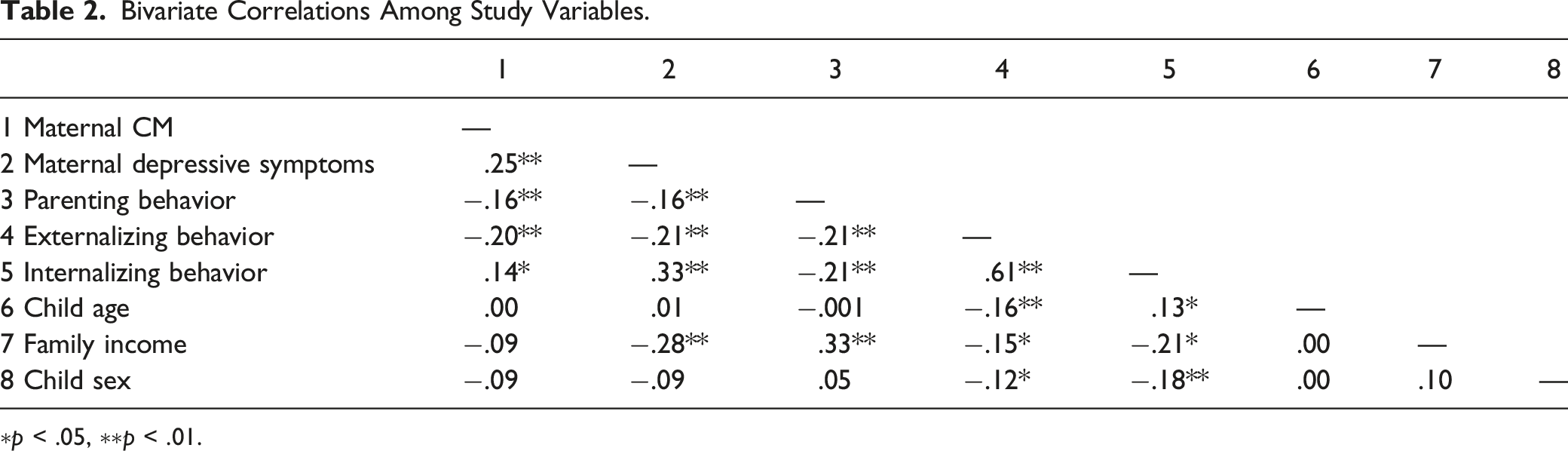
∗p < .05, ∗∗p < .01.
Growth Curve Analyses
Internalizing and Externalizing Behavior Growth Curves
Internalizing and Externalizing Behavior Growth Curves.
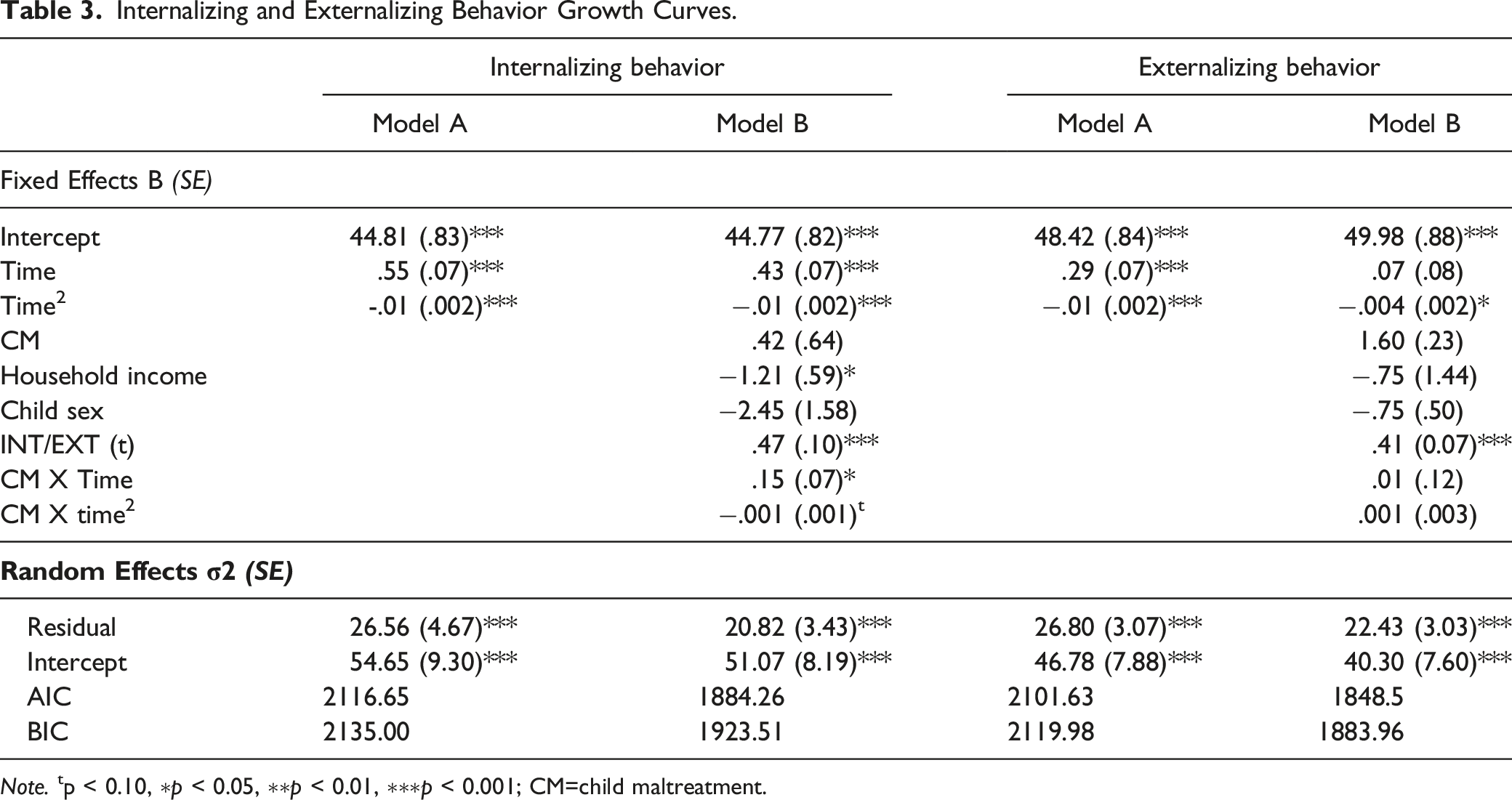
Note. tp < 0.10, ∗p < 0.05, ∗∗p < 0.01, ∗∗∗p < 0.001; CM=child maltreatment.
Maternal Child Maltreatment as a Predictor
As shown in Table 3, Model B, while there was no main effect of maternal CM on internalizing behavior at child age (Fanti & Henrich, 2010; Gilliom & Shaw, 2004; Thomas-Argyriou et al., 2020; Tofighi & MacKinnon, 2011; Turney & McLanahan, 2015) 18 months, there was a significant interaction between CM and time (linear component) (B = .15, p < .05), suggesting that increase in the number of maternal CM is associated with an accelerated increase in internalizing behavior problems over time. To better describe this interaction, the intercept was re-centered to child age 36 and 60 months to examine changes in the strength of effects of CM on child internalizing behavior across development. Results indicated that maternal CM was significantly associated with internalizing behavior at 36 (B = 2.26, p < .05) and 60 months (B = 2.37, p < .01; not shown in Table 3). This association is depicted in Figure 1. Association Between Maternal CM and Patterns of Change in Child Internalizing Behavior.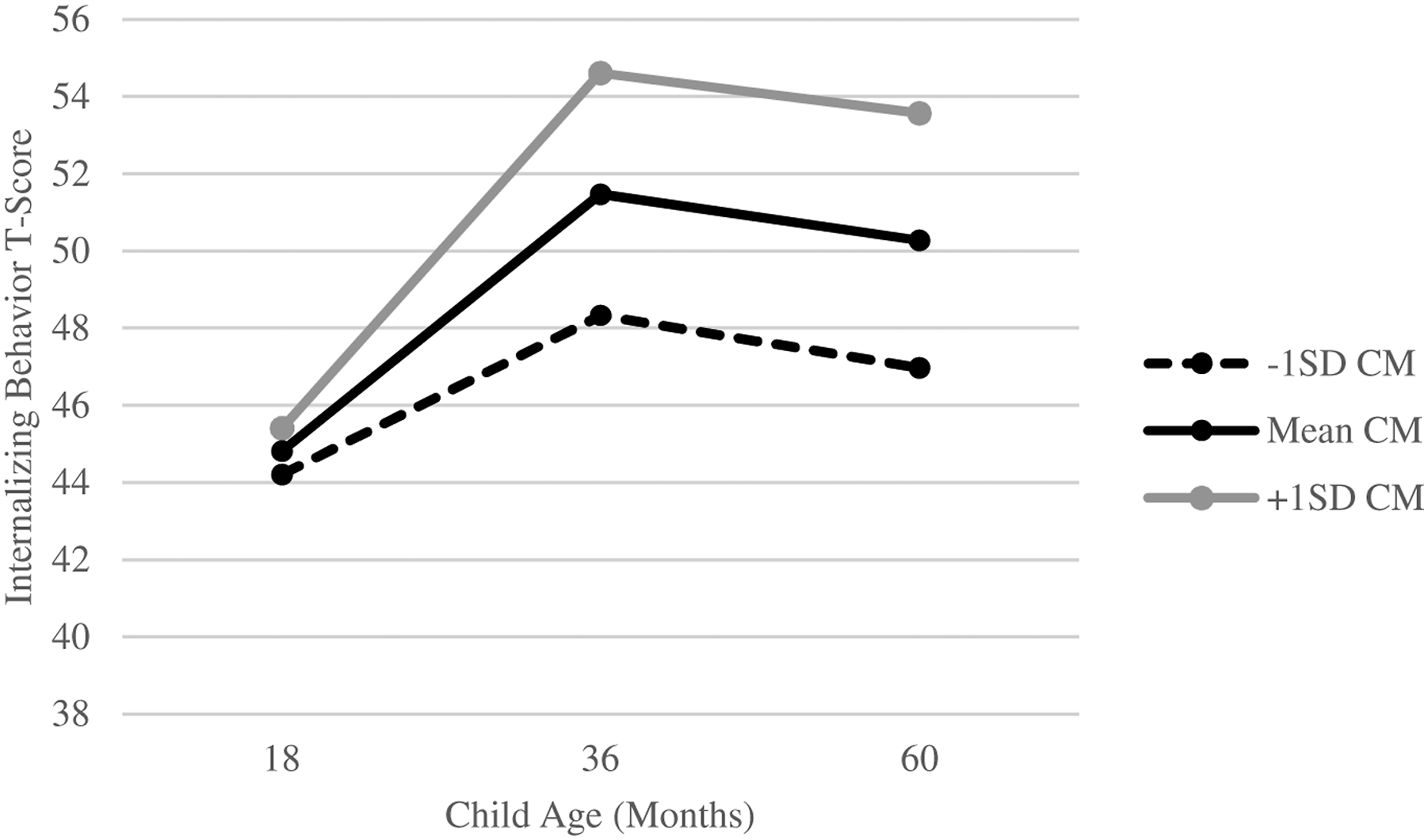
The effect of maternal CM on the intercept of externalizing behavior was insignificant and positive (B = 1.60, p = .18) (see Table 3, Model B). The maternal CM by time interaction was also not significant, indicating that CM was not associated with a significant increase or decrease in rate of change of externalizing behavior. Re-centering the intercept showed that the effects of maternal CM on externalizing behavior were in the same direction at older child ages. However, these effects were significant at these time points, including child age 36 (B = 2.34, p < .05) and 60 months (B = 4.23, p < .001; not shown in Table 3). This association is depicted in Figure 2. Association Between Maternal CM and Patterns of Change in Child Externalizing Behavior.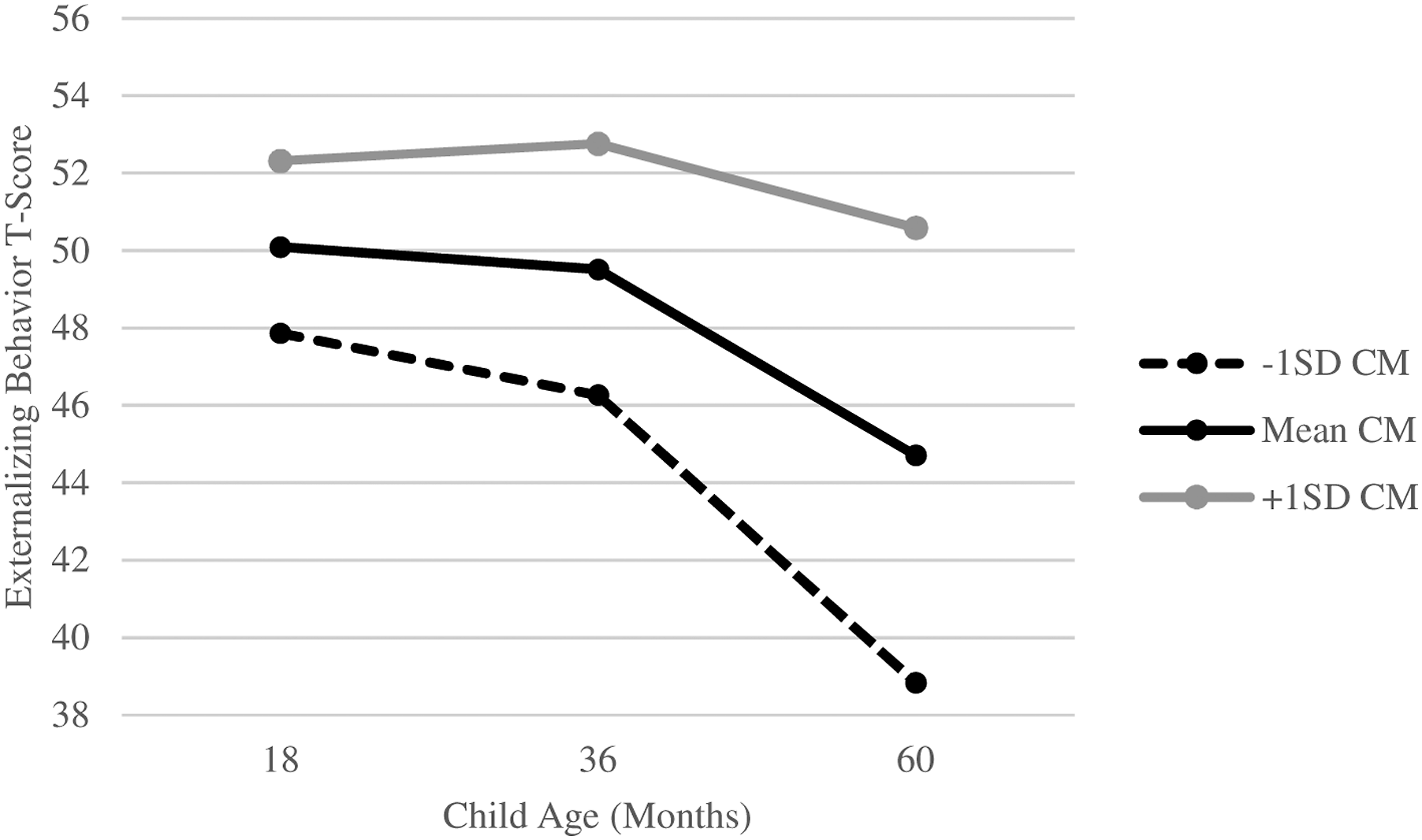
Mediation Analyses
Maternal Depressive Symptoms
Maternal depressive symptoms mediated the association between maternal CM and internalizing behavior. Maternal CM predicted higher levels of depressive symptoms, measured at 18, 36, and 60 months postpartum (Path a = 3.84, SE = .85, p < .001). At the between-persons level, elevated symptoms of maternal depression were related to higher levels of child internalizing problems at age 60 months (Path b = .33, SE = .13, p < .05). At the within-persons level, elevated symptoms of maternal depression at one time point were not significantly associated with higher levels of child internalizing problems at the same time point (Path b = .07, SE = .07, p = .32. As a result, at the between-persons level (but not the within-persons level), maternal depressive symptoms mediated the relation between maternal CM and child internalizing behavior at 60 months (Path ab = 1.27, SE = .47, 95% CI [.34, 2.20]). The direct effect of maternal CM on internalizing behavior was not significant, after accounting for maternal depressive symptoms (Path c= .17, SE = 1.07, p = .87). Maternal depressive symptoms were not significantly associated with levels of child externalizing difficulties at the between- (Path b = .13, SE = .16, p = .42) or within-persons (Path b = .03, SE = .07, p = .66) level.
Parenting Behavior
Maternal exposure to CM was associated with lower levels of positive parenting behavior, measured at 18, 36, and 60 months postpartum (Path a = −.14, SE = .06, p < .05), but the association between parenting behavior and child internalizing difficulties was not significant at the between- (Path b = −2.16, SE = 1.31, p = .11) or within-persons (Path b = 0.97, SE = 1.31, p = .30) level. Similarly, the relation between parenting behavior and child externalizing behavior was not significant at the between- (Path b = −1.71, SE = 1.08, p = .11) or within-persons (Path b = 0.84, SE = .81, p = .12) level. As such, parenting behavior was not a significant mediator for internalizing or externalizing behavior.
Discussion
To our knowledge, this current study is the first study to examine the influence of maternal CM on patterns of change in child internalizing and externalizing difficulties. Children of mothers exposed to CM demonstrated elevated levels of internalizing and externalizing behavior at age 36 and 60 months. Moreover, the association between maternal CM and child internalizing behavior at age 60 months operated indirectly through maternal depressive symptoms. Parenting behavior did not emerge as a significant mediator.
Consistent with typical developmental trajectories (Fanti and Henrich, 2010; Gilliom & Shaw, 2004), an average increase in internalizing behavior, and a decrease in externalizing behavior was seen in children from toddlerhood (i.e., 18 months) to the later preschool years (i.e., 5 years). Longitudinal analyses also showed that between-person differences in trajectories of child behavior were related to their mother’s exposure to CM. Specifically, maternal CM was not significantly associated with internalizing or externalizing behavior measured at 18 months. However, significant positive associations emerged at age 3 and 5 years. These findings are likely due to later onset ages for internalizing symptoms (Liu et al., 2011). Furthermore, given the normative peak of externalizing behaviors around 2 years (Fanti and Henrich, 2010; Gilliom & Shaw, 2004), significant differences in children of mothers exposed to CM may only be seen at later ages, when normative declines in externalizing behavior typically occur. While accumulating evidence suggests that maternal CM is a risk factor for poor behavioral and social-emotional functioning in offspring (Plant et al., 2018), little prior research has addressed how maternal CM may influence child behavior across development. These results are important as they suggest an enduring effect of CM on the development of child problem behaviors, beginning at 3 years and extending throughout the preschool period.
Maternal CM predicted elevated symptoms of maternal depression, measured on average from 18 to 60 months postpartum, which in turn, predicted higher levels of internalizing symptoms in children at 5 years. This pathway is consistent with earlier findings that showed maternal depressive symptoms is a mediator in the association between maternal CM and increased risk of psychopathology in the next generation (Choi et al., 2019; Cooke et al., 2019; Pereira et al., 2018). Exposure to CM during childhood is linked to physiological dysregulation, including impaired stress responses (Shonkoff et al., 2012), that can lead to increased rates of mental illness in adulthood (Humphreys et al., 2020; Norman et al., 2012). In turn, maternal depressive symptoms may confer risk to the child through biological mechanisms (e.g., shared genetic risk factors and stress physiology) and environmental risk factors, including exposure to negative maternal affect, cognitions, and behavior (Berens et al., 2017; Goodman & Gotlib, 1999).
Importantly, the direct effect of maternal CM on internalizing behavior was no longer significant after accounting for the mediating role of maternal depressive symptoms, suggesting that maternal mental health is an important mechanism in the intergenerational transmission of CM to offspring internalizing difficulties. In contrast, maternal depressive symptoms was not a significant predictor of child externalizing behavior. While this conflicts with previous findings that have identified relations between maternal depression and child externalizing difficulties (Goodman et al., 2011), externalizing behavior may be better predicted by other forms of maternal mental health difficulties, such as maternal substance use or antisocial behavior (Mesman et al., 2017; Rhule et al., 2004).
Mothers exposed to CM demonstrated more negative parenting practices, measured on average between 18 and 60 months postpartum. This finding is consistent with meta-analytic findings linking maternal CM to various indices of caregiving behavior (Savage et al., 2019) and suggests that mothers exposed to CM are at a greater risk for parenting difficulties. However, parenting behavior was not significantly associated with internalizing or externalizing difficulties in children. While previous research has demonstrated modest associations between sensitive parenting and child behavioral problems (Kok et al., 2013; Halligan et al., 2013), other studies have found non-significant results (Bosquet Enlow et al., 2016; Madigan et al., 2015). One possibility for a non-significant association may be that other aspects of caregiving, such as harsh and potentially abusive forms of parenting, are more predictive of child behavioral outcomes. For instance, previous studies report that parental discipline (Rijlaarsdam et al., 2014), and child maltreatment potential (Bosquet Enlow et al., 2016) mediate relations between maternal CM and child behavior. Future research is needed to investigate the role of other forms of parenting behavior in the relationship between maternal CM and child outcomes.
Strengths, Limitations, and Future Directions
Despite important strengths, including a longitudinal design, which allowed us to examine trajectories of child internalizing and externalizing behavior across a sensitive developmental period, several limitations should be noted. First, the majority of study participants represent a relatively low sociodemographic risk sample (i.e., mostly married or in common-law relationships, highly educated, and with a high household income). Second, children’s internalizing and externalizing behavior scores were primarily in the normative range. While our findings are important as they demonstrate that intergenerational effects of CM are evident in non-clinical samples with sociodemographic advantages, generalizability of the results may be limited. Future research should examine these associations in socio-demographically diverse populations and clinical samples as well. Furthermore, mothers retrospectively reported on their exposure to CM, which may result in underreporting due to perceived stigma, recall bias, or other factors affected by the mother’s current mental state. However, such retrospective reports have been found to be valid measures (Karatekin & Hill, 2018). Additionally, maternal depressive symptoms and child behavior were measured via maternal report. Replication of findings using clinical interviews, observational measures, or multi-informant reports (e.g., teacher and other caregivers) is important to control for possible informant bias. Another limitation is the small sample size (N = 115), emphasizing the need to replicate the results in larger samples. Finally, no significant mediators emerged in the pathway between maternal CM and externalizing behavior, suggesting that other intermediary mechanisms may account for this direct effect (e.g., social support and paternal characteristics). These should be considered in future studies to gain a more comprehensive understanding of the intergenerational effects of CM.
Implications and Conclusions
In summary, our findings suggest that children of mothers exposed to CM are at increased risk for elevated trajectories of emotional and behavioral difficulties across early childhood. In addition, maternal depressive symptoms may be an important mechanism through which maternal CM increases risk of internalizing problems in the next generation. The present study contributes to a growing body of evidence demonstrating intergenerational effects of CM, and further suggests that the associations between maternal CM and child behavior are relatively enduring from toddlerhood to the preschool period.
Our findings also highlight the importance of being alert to depressive symptoms among mothers who experienced CM in clinical settings (e.g., well-baby visits), and the value of referral to early intervention for maternal depression to interrupt intergenerational cascades of risk from parent to child before maladaptive behavioral trajectories in children are established. For example, psychotherapy for maternal depression has been shown to improve offspring mental health (Cuijpers et al., 2014). Continued investigation into the associations between maternal CM and child behavioral problems across various developmental stages is needed, including the use of additional mediators and longer follow-ups to determine whether these effects are persistent in older children.
Supplemental Material
sj-pdf-1-cmx-10.1177_10775595221074364 – Supplemental Material for Maternal Childhood Maltreatment History and Child Behavior Problems: Developmental Patterns and Mediation via Maternal Depressive Symptoms and Parenting Behavior
Supplemental Material, sj-pdf-1-cmx-10.1177_10775595221074364 for Maternal Childhood Maltreatment History and Child Behavior Problems: Developmental Patterns and Mediation via Maternal Depressive Symptoms and Parenting Behavior by Madeleine Harris, Harriet MacMillan, Jennifer Mepham, Divya Joshi, Christine Wekerle, Leslie Atkinson, and Andrea Gonzalez in Child Maltreatment
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Canada Research Chairs and Social Sciences and Humanities Research Council of Canada (410‐2010‐2079, 430‐2‐12‐879).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.