
Abstract
Two parenting capacity assessment (PCA) protocols, with a short parent-child intervention embedded in each protocol, evaluated the potential for enhanced parenting to orient child placement decision. Parents (n = 69), with substantiated reports of maltreatment by child protective services, and their children (0–6) were randomly assigned to one of two PCAs with either the Attachment Video-feedback (PCA-AVI) or a psychoeducational intervention (PCA-PI) as the embedded intervention component. The PCA-AVI group showed the highest increases in parent-child interaction quality at post-test. Also, at PCA completion, evaluators’ conclusions about the parents’ capacity to care for both PCA groups were associated with parent-child interactive improvements at post-test, the court’s placement decision at post-test, and child placement one year later. However, only conclusions drawn by PCA-AVI evaluators were predictive of child re-reports of maltreatment in the year following PCA. PCAs, relying on short attachment interventions to assess the potential for enhanced parenting, are promising tools to orient child placement decisions.
Keywords
When children are notified for abuse or neglect to Child Protection Services (CPS), parental caregiving comes into question and caseworkers may consider out-of-home placement to ensure child development and physical and emotional safety. To assist in decision-making, caseworkers or judges frequently request an evaluation of parental capacities to document the factors (e.g., mental health problems, unstable family life, social support) likely to influence parents’ behaviors and their potential for change, the child’s functioning in relation to the parental skills and deficits, and the risks that would arise from placement. On the basis of these parenting capacity assessments (PCA), caseworkers provide direction for intervention and make recommendations to judges as to whether a parent has the capacity for minimal standards of child care and, accordingly, if the child should be removed from, maintained or reunited with their parent. As a result, PCAs have major consequences in a child’s life.
While we know PCAs are critically important, decision-making in child placement cases is prone to bias due to individual characteristics of the caseworkers, such as their mind-set regarding the parents’ ability to change or their attitudes towards out-of-home placement (De Haan et al., 2019). Furthermore, to better support placement decisions, improvements to PCAs have been proposed via the use of more structured and dynamic protocols in which parenting capacities would be assessed based on parents’ responses to a short and manualized parent-child intervention (e.g., Cyr & Alink, 2017; Harnett et al., 2018; van IJzendoorn et al., 2018). The current randomized control-trial (RCT) examines, in a sample of maltreating parents and their children, if a PCA with the evidence-based Attachment Video-feedback Intervention (AVI; Moss et al., 2011), embedded as an intervention component to assess the potential for enhanced parenting, is valuable to orient child placement decisions.
Assessing Parental Capacity to Change Using an Attachment Framework
Models and approaches for carrying out PCAs have been proposed by the child maltreatment and social services fields (e.g., Budd, 2005; Houston, 2016; Steinhauer et al., 1995). In short, PCAs should tap into the many aspects of parental cognitive, social, and emotional functioning in relation to the fit between parental competencies and child needs. PCAs should show how parental limitations and strengths in these domains represent risk or protective factors for the child’s development and the parent’s capacity to benefit from rehabilitative services. Also, PCAs should rely on direct observations of the parent-child dyad during daily activities. Despite these guidelines, it was found that PCAs often relied on a single meeting with the parent, included more information on parental limitations than strengths, and relied on limited observations of the child and the parent-child interaction (e.g., Budd et al., 2001).
Furthermore, because PCAs are generally conducted during a few sessions with parents, there is limited time for parents to show their potential for enhanced parenting and for evaluators to assess capacity to change. For example, enhanced or unchanged, low parental sensitivity with the child, after a brief intervention during the assessment process, could provide highly relevant information on parental capacities and help guide placement decisions (Cyr & Alink, 2017; van IJzendoorn et al., 2018). On the basis of an extensive PCA literature review, White (2005) concludes that good enough parenting capacities are observed in parents who respond to their child’s actual and evolving needs with interest, warmth, and sensitivity, and are able to set appropriate boundaries and find solutions to the daily struggles they encounter as parents. Multiple factors, associated with each of the ecological systems in which families are embedded, may impinge on parenting capacities. For example, the parent’s cultural values, community, financial, and psychological resources, history of maltreatment, and social support may impact parenting capacities (Houston, 2016; Steinhauer et al., 1995). Optimal PCA protocols should assess all of these factors and their influence on children to document placement decisions. Yet, the addition of a short attachment intervention to such PCA protocols would be much suited for the evaluation of the potential for enhanced parenting, given that the behaviors targeted by these interventions are precisely those we would like to see improve in maltreating parents.
As an overview, RCT studies of short attachment interventions for maltreating (or at very high-risk) parents and their children have reported for the target group increases in maternal sensitivity and child attachment security, and decreases in parental harsh discipline, abuse risk, child behavior problems, and attachment disorganization (e.g., Lind et al., 2014; Moss et al., 2011; Negrão et al., 2014; Thomas & Zimmer-Gembeck, 2011). Each of these interventions focuses on the parent-child relationship, includes the parent and child during the sessions, and gives positive video or in-the-moment feedback to the parent as means of enhancing sensitive parenting. They all rely on the assumption that modifying interactions via positive comments to the parent elicits changes in parental sensitivity and child functioning.
In addition to parental sensitivity or quality of parent-child interaction, a critical indicator of enhanced parenting in child protection cases is the diminished risk of the recurrence of maltreatment. One way to better orient placement decisions would be to provide caseworkers and judges with information on the risk of recidivism. Fewer re-reports of maltreatment were found for the target group two to four years after the intervention (Chaffin et al., 2004; Thomas & Zimmer-Gembeck, 2011). In the Thomas and Zimmer-Gembeck study, children who were not re-reported for maltreatment had mothers who showed greater improvements in sensitivity after the intervention.
More recently, two studies, one with maltreating parents (Van der Asdonk et al., 2020) and another with at very high-risk pregnant mothers (Harnett et al., 2018), tested a PCA protocol with an embedded video-feedback parent-child intervention to assess the potential for enhanced sensitivity, but mixed results were shown. The RCT study of Van der Asdonk et al. (2020) showed that children of the target and control groups experienced similar recurrence rates of maltreatment 10 months after the intervention Also, evaluators of the target group did not feel more confident about their child placement recommendations. As authors argued, given that the evaluators were part of different clinics, they could not rely on a standardized evaluation protocol. As for the study of Harnett et al. (2018), infants of the target group, compared to those assigned to the routine care assessment, were more likely to remain in the care of their mothers 12 months after birth. This study did not, however, rely on an RCT design, thus precluding any firm conclusions.
The Current Study
In 2007, the Youth Protection Act of the province of Quebec (Canada) was amended to improve placement stability for children removed from their home (Hélie et al., 2012). The act established age-specific durations of out-of-home stay, after which the court must make a ruling to provide a permanent living situation for the child. The new provisions restated that decisions made by CPS must seek to keep children with their parents or, if removed, to return them to their parents as soon as possible; otherwise, to provide them with a stable, long-term placement. As a result, the need to improve the decision-making process regarding child placement became of paramount importance. In collaboration with CPS, we thought that gaining a more thorough appreciation of the parents’ capacity to care, via the assessment of their potential for enhanced parenting, would better orient placement decisions.
In response to these revisions, the CPS agency of the city of Montreal (in Quebec), implemented a specialized clinic, whose specific mandate was to carry PCAs of what they defined as difficult-to-assess cases (e.g., cases with siblings, with parents not speaking official national languages). Across different countries, various mental health professionals (social workers, psychologists, etc.) are sought out to perform PCAs. In Quebec, these professionals mainly include psychoeducators and they are hired by CPS agencies to conduct PCAs. Following substantiation of maltreatment, cases were referred to the clinic by the CPS social workers, who requested a PCA to help determine if the child should remain in their home, be removed or returned (some children are temporarily placed for immediate protection or as a safe haven strategy while parents are being assessed; Hébert et al., 2018). The question asked was whether the parents had the potential to care for their child adequately.
Objectives and Hypotheses
The overarching objective of this RCT study is to examine if a PCA protocol, including the AVI as a means to assess the capacity for enhanced parenting, is a valuable method to orient placement decisions. We randomly assigned maltreating parents and their children to one of two PCA protocols with an embedded intervention component, either the evidence-based AVI (PCA-AVI) or a psychoeducational intervention (PCA-PI).
Prior to investigating which of the two PCA protocols better orients placement decisions, we first tested whether the AVI intervention effectively led to parental and child benefits on four indicators of parental capacity. Namely, in comparison to the PCA-PI group we expected the PCA-AVI group to show: 1) a higher quality of parent-child interaction at post-test, 2) a greater number of court decisions in favor of the child remaining with the parent at post-test, 3) fewer child placements 1 year after PCA and 4) fewer re-reports of maltreatment 1 year after PCA.
Second, we examined case orientation benefits. To do so, we tested whether the parents’ capacity to care at PCA completion, as concluded by CPS evaluators in their assessment reports, is differentially associated with the four parental capacity indicators across the two PCA groups. For the PCA-AVI protocol to be considered an effective tool in the decision-making regarding child placement, PCA-AVI parents who are judged as capable of care should show better outcomes (i.e., higher quality of parent-child interaction at post-test, fewer child placement at post-test and 1 year after PCA, and fewer child re-reports of maltreatment 1 year later) than those in the PCA-AVI group judged as not capable of care or those in the PCA-PI group.
Method
Participants
The final sample of this study includes 69 maltreated children with a mean age of 18.66 months (SD = 19.75, range 0.26–69.54 months; 44 boys) and their biological parent (M = 28.26, SD = 7.46; 12 fathers as primary caregiver). These families are drawn from a larger sample (N = 123) recruited through CPS agencies of the city of Montreal. We only selected families that were submitted to randomization, that is 69 families recruited at a specialized clinic. In comparison to regular PCA services outside this clinic, which are usually conducted within four meetings, PCAs at the clinic could include up to 12 meetings. Approximately 20% of the families with substantiated reports of maltreatment from the Montreal area were referred to the clinic. All families speaking French or English and about to begin a PCA were eligible, except those with children with severe medical or developmental problems (e.g., autism spectrum disorder). For families participating with siblings, only one child was appointed as the target child for this research. This study was approved by the ethics committee of the Montreal CPS agency. Prior to their first PCA meeting, parents met with the research coordinator, who explained the research protocol. PCAs, once requested by caseworkers, are mandatory by law, but all parents were free to refuse participation in our research. Those who agreed to participate signed a consent form.
Following a simple randomization procedure with a 1:1 allocation sequence, families at the clinic were randomly assigned to a PCA protocol with either the AVI or the PI as the embedded intervention component. A generated list by the study's principal investigator was provided to the chief of practitioners at the clinic, who allocated the families according to the list. CPS assigned three psychoeducators to each group. We were totally dependent on CPS to provide evaluators for our project. As a result, when two PI evaluators left for medical reasons, they were not replaced promptly. This led to a non-equivalent number of evaluators in both groups for several months. This loss of personnel explains why the numbers of participants in the two groups are different after randomization. Overall, 137 families were assessed for eligibility, 69 families started pre-test and went through randomization (PCA-AVI n = 42, PCA-PI n = 27), 48 families completed post-test, and 65 files were opened for examination 1 year after PCA. Figure 1 is a flow chart of the families’ attrition and participation through the project phases. No significant differences in sociodemographic, child maltreatment, or parent-child interaction quality were found between participants who completed the pre-/post-tests and those who started pre-test but dropped out (n = 21; ts between 0.24 and −0.70, X2 between 0.03 and 2.26).
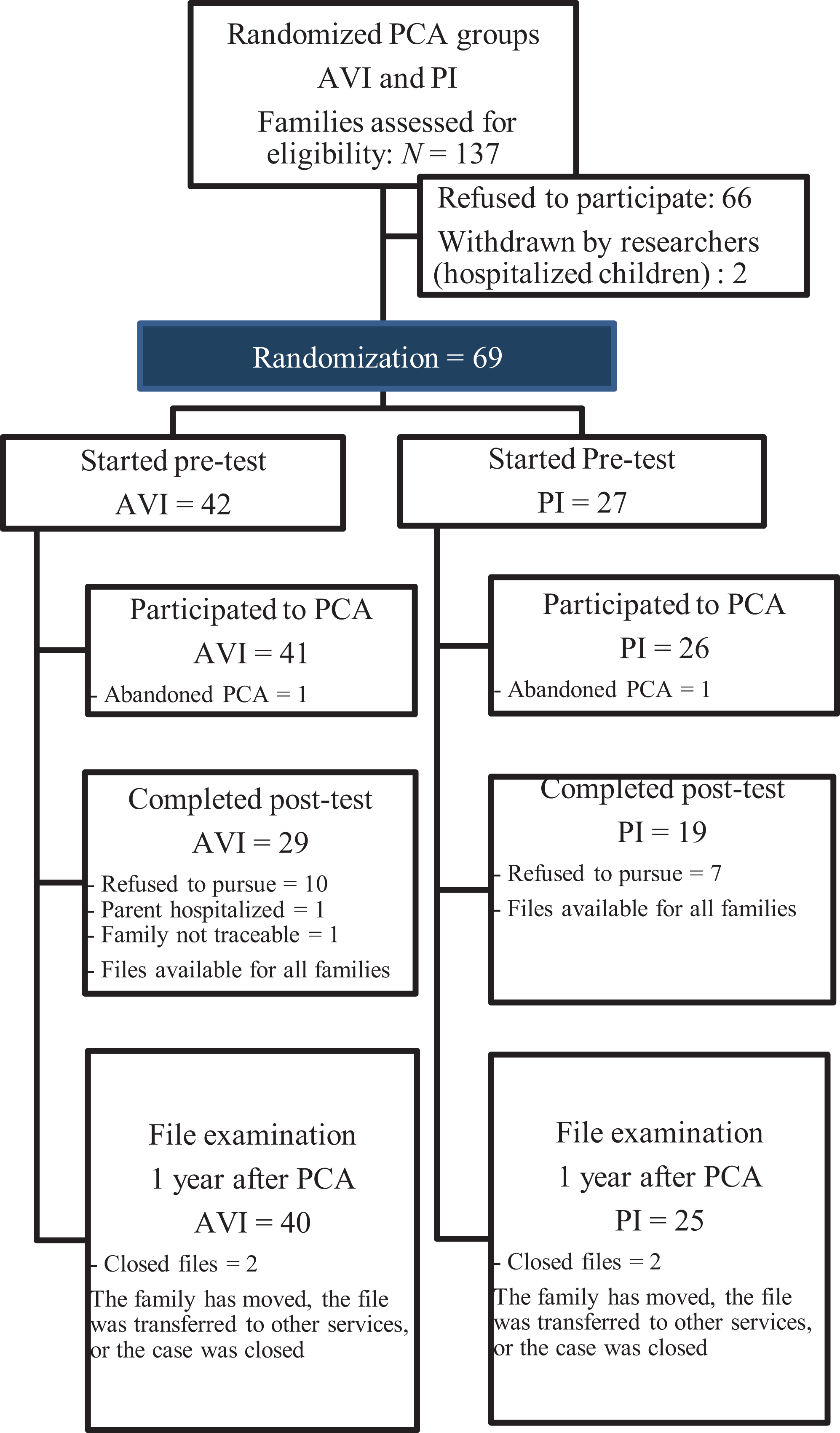
Flow chart of the study’s progress, detailing participant’s participation, attrition, and number of opened files.
Table 1 presents sociodemographic and child maltreatment information for PCA groups. In all, 23% of the children were born to adolescent mothers, 80% of the caregivers did not complete high school, 28% of the families were part of ethnic minority groups, and 87% were receiving social welfare or were unemployed. Child maltreatment was substantiated by CPS and maltreatment types corresponded to widely accepted definitions. In all, 81% of the children experienced neglect, 29% physical abuse, 9% sexual abuse, and 28% emotional abuse. At intake, some children were in foster families as a temporary placement (n = 18; mean duration of placement = 2.97 months, SD = 4.06; range = 1 week to 6 months). There were no significant differences in any of the socio-demographic, child maltreatment, and child placement variables between the two randomized groups (ts between −0.34 and 1.29, X2 between 0.01 and 1.24). PCA groups at pre-test were also not different on the quality of parent-child interaction (d = −0.12, CI [−0.60, 0.37]). We conclude from these analyses that our randomization procedure was effective.
Descriptive Statistics for the PCA Groups on Sociodemographic, Child Maltreatment, and Placement Variables at Pre-Test.
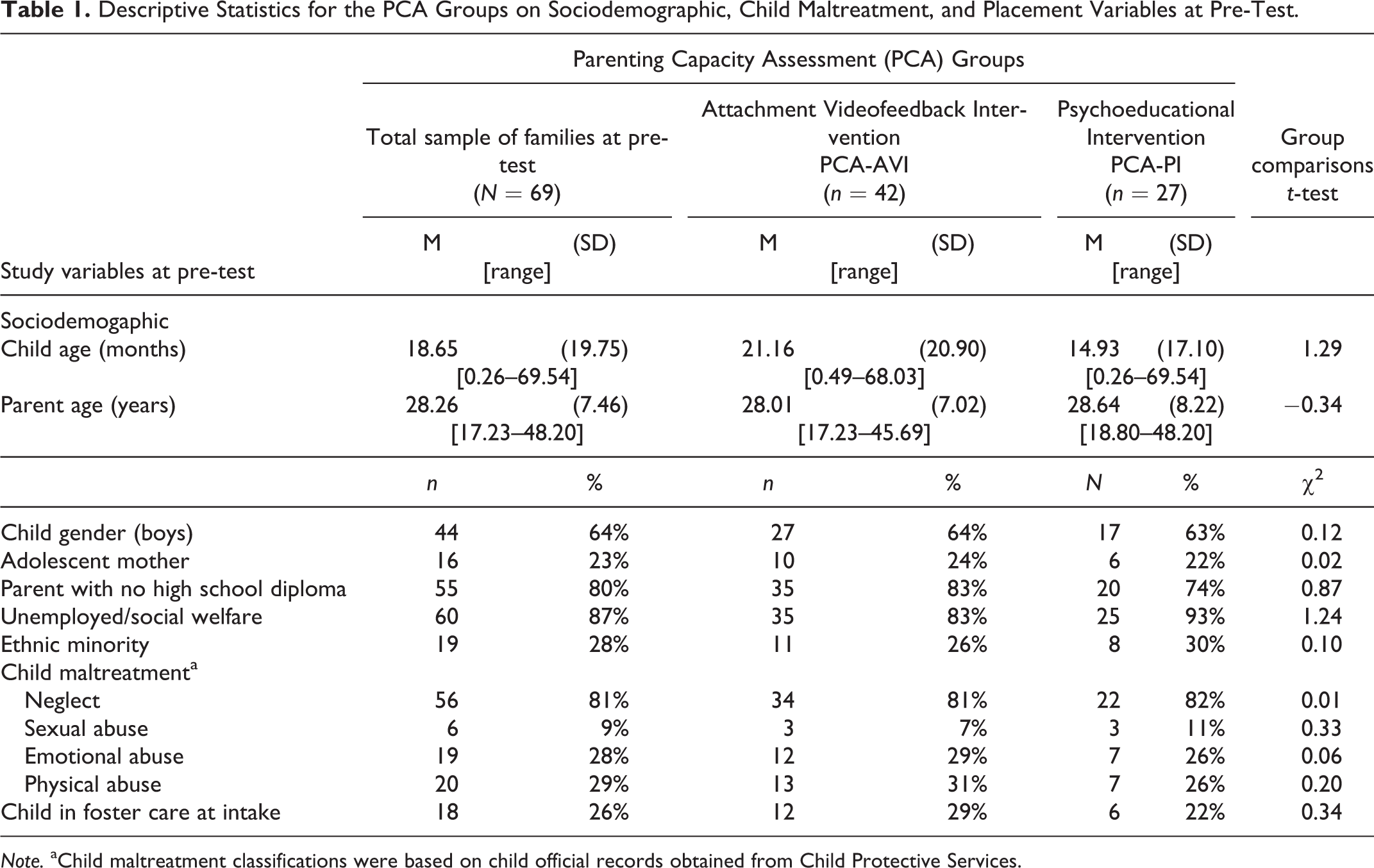
Note. aChild maltreatment classifications were based on child official records obtained from Child Protective Services.
Procedure
Families completed pre-test measures during two visits (1-hour home and 1-hour lab visits) scheduled 1 week apart and the PCA started the following week. For children living in out-of-home care, both visits took place at the laboratory with their biological parent. Two almost identical post-test visits took place 2 weeks after the end of PCA. CPS files were also examined at pre-test, post-test, and 1 year after PCA to document child maltreatment types, the court’s decisions, child placements and re-reports of maltreatment.
The PCA Protocols
The protocols were conducted within a 2-month period (PCA-AVI M = 2.00 months; PCA-PI M = 1.75 month). PCA-AVI families received on average 9.21 sessions, the PCA-PI group received 8.33 sessions. The two protocols did not significantly differ in their length (t = 1.73, p = .09, d = 0.10, CI [−0.39, 0.58]) or number of sessions (t = 1.15, p = .25 d = 0.29, CI [−0.20, 0.77]). To assess parental capacities, evaluators of both groups relied on the adapted French-version of the Steinhauer guidelines (De Rancourt et al., 2006), which helps collect, with the use of parental interviews and family observations, information on the social and family contexts (social support, financial resources, psychopathology, drug/alcohol problems, etc.), the children’s development and health, the parents’ impulse control and parenting practices, and the family’s history of prior clinical services. All psychoeducators working as PCA evaluators in CPS agencies in Montreal are trained by CPS to use the Steinhauer’s guidelines. In addition, they conducted a short parent-child intervention (AVI or PI) during the evaluation process to assess the potential for enhanced parenting. All evaluators had a college degree in psychoeducation, with at least 5 years of experience in working with CPS.
PCA-AVI group
Evaluators conducted the Attachment Video-feedback Intervention (AVI, see Moss et al., 2011). The AVI is a short-term, strength-based intervention seeking to promote changes in parental sensitivity by reinforcing parents’ positive behavior throughout the sessions and during a video-feedback period. At each session, a 5- to 10-minute parent-child play or caregiving activity in line with child age and parental challenges, and including simple prompts (e.g., follow your child’s lead, describe what your child is doing/feeling during the activity), is filmed by the practitioner. Immediately following this film, a video-feedback is done with the parent, during which the practitioner intentionally stops the film on positive sequences to reinforce parental sensitive behaviors and positive impact on the child. Parents are also invited to rely on their growing sensitive behavioral repertoire to repair inappropriate, frightening or frightened behaviors. Evaluators were trained by attachment experts and used a manual describing the AVI and age-appropriate parent-child activities. To ensure treatment integrity, evaluators received group supervision every two to four weeks by an attachment expert (the first author) also trained as a child psychologist. Supervision involved PCA-AVI evaluators and two other psychologists with a PCA expertise, who gradually took charge of supervision.
PCA-PI Group
Evaluators conducted Psychoeducational Intervention activities. The PI consisted of educational and didactic activities generally used by CPS practitioners. These activities were selected out of existing programs (e.g., the ALI program) showing increases in cognitive and language development of preschoolers from high-risk backgrounds (e.g., Verreault et al., 2005). Throughout the sessions, parents are given information on parental practices and child development as ways to promote parenting abilities and child functioning. During daily activities (e.g., change of diaper, feeding, nap-time) and prompted educational activities (e.g., interactive reading, learning games), parents are asked, through modeling, to behave in manners (as demonstrated by the provider) that stimulate the child’s participation. PCA-PI evaluators discussed cases among themselves during team meetings not involving PCA-AVI evaluators.
Instruments
Socio-Demographic Questionnaire (Pre-Test)
This questionnaire with items on demographic information (e.g., parental education, child age) was completed by parents.
Quality of Parent-Child Interaction (Pre- and Post-Tests)
During the lab visits, parent-child dyads were invited to a 10-minute filmed snacktime where toys and magazines were available. Quality of parent-child interaction was coded from the filmed snack-time with the Moss et al. (2005) observational system. This system includes nine 7-point scales (i.e., coordination, communication, partner roles, emotional expression, sensitivity, tension, mood, enjoyment, and overall score). The overall scale score is rated independently of other scales’ scores, and represent overall interactive functioning of the dyad (high quality: i.e. reciprocal, sensitive parenting, positive shared affect) to poor quality: i.e. insensitive, indifferent, conflictual). Scores 4 or greater are indicative of a more optimal interaction, while scores 3 and below are indicative of a dysfunctional interaction in need of clinical attention. These scales have shown concurrent and longitudinal associations with attachment and behavior problems of children from low and high socioeconomic risk backgrounds and with mothers and fathers as primary caregivers (e.g., Bureau et al., 2017; Moss et al., 2005). Interrater reliability of four coders on 20% of the sample ranged from ricc .62 to .89. Coders were blind to other study measures. A principal component factor analysis of all scales yielded a single factor explaining 81% of the variance. Hence, this study only used the overall scale score.
Children’s CPS Files
Files were consulted to document the children’s types of maltreatment, the number of re-reports of maltreatment since the end of the PCA, and whether the child was placed at intake, at post-test (placement decisions made by the court after PCA), and 1 year after the end of the PCA.
Evaluators’ Conclusions About Parents’ Capacity to Care at PCA Completion (Post-Test)
Parental capacity to care was documented on the basis of the evaluators’ PCA reports. To inform the social workers’ and the court’s decision-making, evaluators do not make any specific recommendation about child placement in their report, but rather write a qualitative description of the parent’s capacity to care in the form a short conclusion. Two independent coders, blind to other study measures, rated PCA’s conclusions. Using a 0-1 categorical scheme, a score of 1 was given to the parents described as capable of care. Such parents, although often described as having weaknesses, were also portrayed as having caregiving strengths (e.g., parental sensitivity, reflective stance), capacity for growth and change, or social support. Interrater reliability on 15% of the sample was excellent (κ = .85).
Statistical Analyses
Between the pre- and post-tests, 21 participants were lost to attrition for the parent-child interaction variable (13 PCA-AVI and 8 PCA-PI). There were no missing data on child placement decisions nor on the ratings of parental capacity to care, as both were retrieved at post-test in children’s CPS files. At the 1-year file examination, child placement and re-reports of maltreatment data were, however, missing due to 4 closed CPS files (see Figure 1). To maximize sample size and account for all participating families, we performed a multiple imputation (MI) procedure as an intent-to-treat approach (ITT) to replace missing values. MI has been used as an ITT method in past RCT studies (e.g., Dijkstra et al., 2019) and is recommended to other procedures (e.g. LOCF; Lachin, 2017) and under the missing completely at random (MCAR) assumption, which was demonstrated for this study (Little’s test χ2 = 44.61, p = .18).
Data were imputed using the fully conditional specification method of SPSS 26, which relies on an iterative Markov Chain Monte Carlo (MCMC) method. We specified 100 iterations with 25 imputed data sets as recommended in the literature (Enders, 2010). Relevant covariates were included as predictors to maximize the precision of imputed data. The PCA grouping variable was not used as a predictor. Analyses were run on each imputed data set and results were pooled. Due to unavailable pooling methods in SPSS 26 for estimates of ANCOVAs and χ2s, we averaged Fs or χ2s estimates across imputed results. Then, we used the median of the p values as a method for significance testing of categorical variables in χ2s (Eekhout et al., 2017). For significance of F tests, we used available pooled means and standard errors to compute a d effect size and a 95% CI (Lipsey & Wilson, 2001).
To test for the robustness of significant findings, we repeated the analyses using the full information maximum likelihood (FIML) estimation method (MPlus, version 8.4; Muthén & Muthén, 1998–2019). For estimation of models, FIML retains all available information from each participant, even information of participants with missing data by maximizing the covariance matrix. Also, we performed complete case (CC) analyses, which exclude participants with any missing data. When missing data are MCAR, CC analyses are not considered biased, but may be underpowered due to reduced sample size (Jakobsen et al., 2017). Hereafter are the results using the MI approach with the MCMC algorithm. CC and FIML analyses are detailed in a supplement file. Results of each scenario are then examined to see if effect sizes converge. To facilitate the comparison of effect sizes, the d statistic was computed from available estimates. Overlapping CIs indicates no significant differences in effect sizes across methods.
MI analyses. A first set of analyses examined parent-child benefits of the PCA-AVI. ANCOVAs and χ2s tested effects on the four indicators of parental capacity (i.e., parent-child interaction quality, court child placement decision at PCA completion, and child placement and re-reports of maltreatment 1 year after the PCA). Results are reported in Table 2. The second set tested case orientation benefits. One 2 × 2 ANCOVA and three 3-way χ2s (with one marginal and two partial tables) tested if parents involved in the PCA-AVI and rated as capable of care by their evaluators were more likely to keep their child at home after PCA and 1 year later, and refrain from further maltreating behaviors than PCA-AVI parents rated as not capable of care and those exposed to the PCA-PI protocol. Results are reported in Table 3.
Statistics for Indicators of Parental Capacity at Pre- and Post-Tests as a Function of PCA Groups.
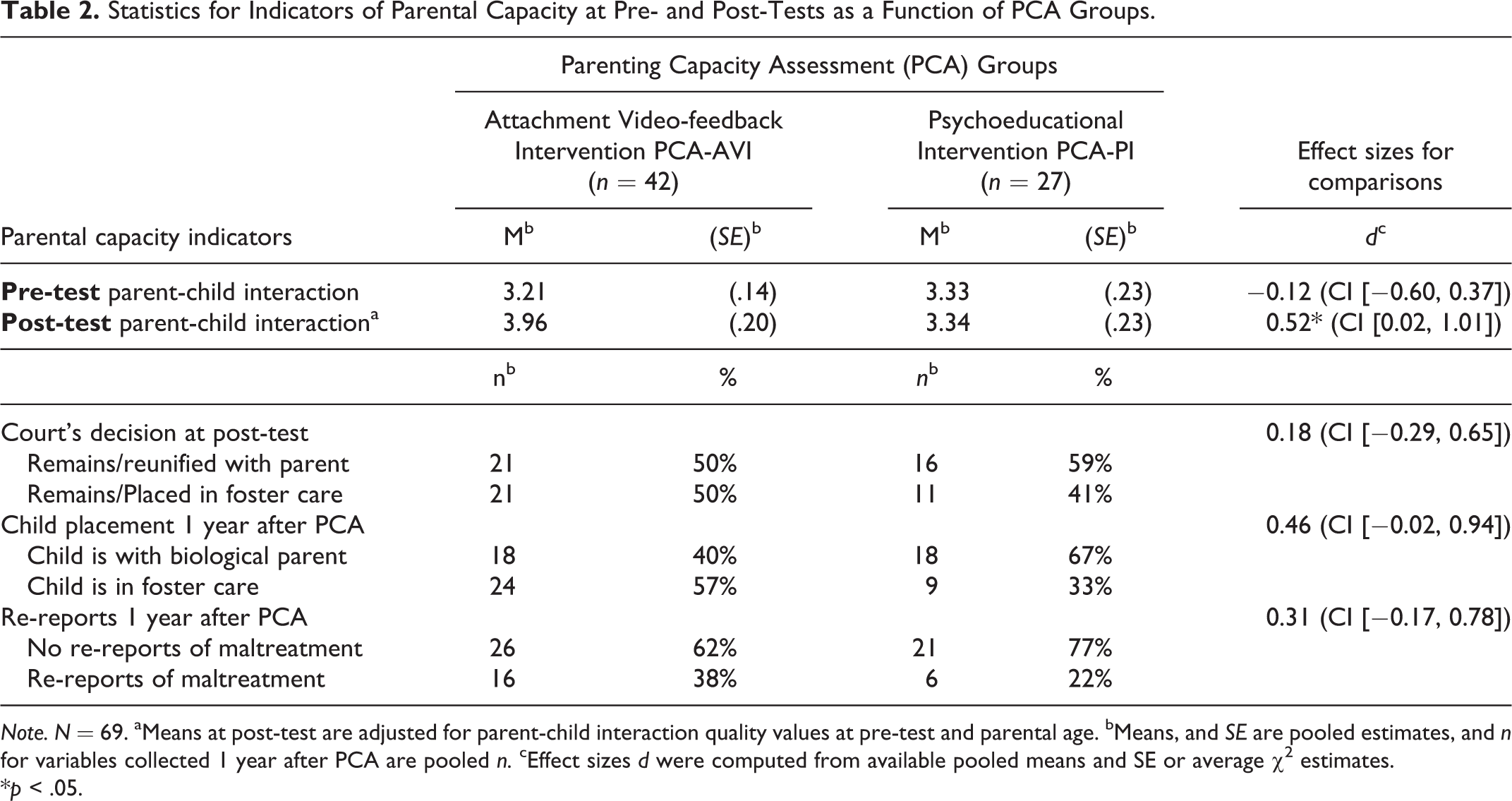
Note. N = 69. aMeans at post-test are adjusted for parent-child interaction quality values at pre-test and parental age. bMeans, and SE are pooled estimates, and n for variables collected 1 year after PCA are pooled n. cEffect sizes d were computed from available pooled means and SE or average χ2 estimates.
*p < .05.
Statistics for Indicators of Parental Capacity at Pre- and Post-Tests as a Function of PCA Groups and Parental Capacity to Care.
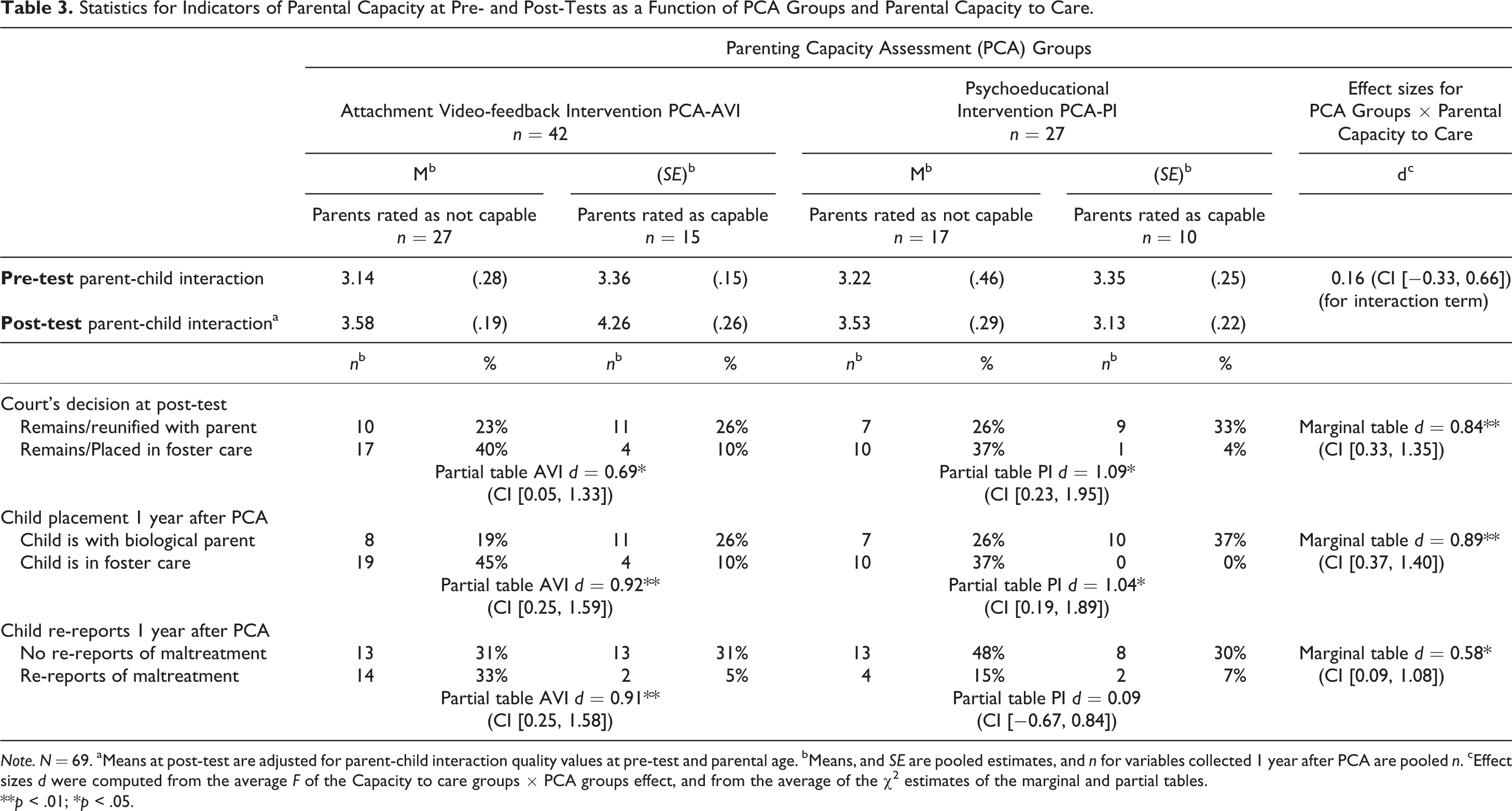
Note. N = 69. aMeans at post-test are adjusted for parent-child interaction quality values at pre-test and parental age. bMeans, and SE are pooled estimates, and n for variables collected 1 year after PCA are pooled n. cEffect sizes d were computed from the average F of the Capacity to care groups × PCA groups effect, and from the average of the χ2 estimates of the marginal and partial tables.
**p < .01; *p < .05.
Results
Preliminary Analyses
Potential sociodemographic covariates were examined in relation to the four indicators of parental capacity at post-test and at the 1-year file examination. There were no significant associations between any of the variables (ts between −.39 and 1.62, rs between −0.03 and .24), except that younger parents had a lower quality of interaction at post-test (r = .26, p = .04). Parental age was used as a control variable in analyses with the parent-child interaction variable.
Parent and Child Benefits
Parent-Child Interaction Quality
An ANCOVA on parent-child interaction quality at post-test, with parental age and interaction quality at pre-test as covariates, showed a significant group effect, with the PCA-AVI group showing a greatest increase in interaction quality (F(1, 68) = 9.89, d = 0.52, CI [0.02, 1.01]). FIML and CC analyses showed similar moderate effect sizes with overlapping CIs (FIML: d = .53, CI [0.04, 1.02]; CC: d = 0.62, CI [0.03, 1.22]).
Child Placement Court Decisions after PCA (at post-test), and Child Placement and Re-reports of Maltreatment One Year after PCA. First, descriptive data indicate that 44 parents (64%) were rated as not capable of care at PCA completion (post-test) and court decisions led to 32 children (46%) being placed or remaining in out-of-home care. During the year following PCA, re-reports of maltreatment were filed for 22 children (32%), and 33 children (48%) were in out-of-home care 1 year after PCA. χ2s showed no PCA group differences on the proportions of children in placement at post-test following the court’s decision (χ2(1, N = 69) = 0.57, p = .45, d = 0.18, CI [−0.29, 0.65]), in placement 1 year after PCA completion (χ2(1, N = 69) = 3.51, p = .06, d = 0.46, CI [−0.02, 0.94]), or with re-reports of maltreatment in the year following the end of the PCA (χ2(2, N = 69) = 1.59, p = .17; d = 0.31, CI [−0.17, 0.78]).
Case Orientation Benefits
Parent-child Interaction Quality
We performed a 2 × 2 ANCOVA on quality of parent-child interaction at post-test, with pre-test values of interaction quality and parental age as covariates, and with PCA groups and evaluators’ ratings about the parental capacity to care as the between factors. As shown previously, a significant main effect for the increase in quality of parent-child interaction was observed for the PCA-AVI group in comparison to the PCA-PI group (F(1, 68) = 5.13, d = 0.62, CI [0.11, 1.12]). The main effect for the evaluators’ ratings about parental capacity to care (F(1, 68) = 4.26, d = 0.52, CI [0.02, 1.02]) was significant and of moderate magnitude. Thus, parents rated as capable of care, irrespective of their PCA group, were more likely to show increases in parent-child interactive quality. FIML and CC analyses showed similar moderate effect sizes for this result with overlapping CIs (FIML: d = .70, CI [0.20, 1.20]; CC: d = 0.63, CI [0.04, 1.23]). The interaction of PCA Groups × Capacity to care groups was not significant (F(1, 68) = 0.41, d = 0.16, CI [−0.33, 0.66]; also with FIML: d = .05, CI [−0.43, 0.54] and CC: d = 0.19, CI [−0.39, 0.77]).
Child Placement Court Decisions after PCA (Post-Test)
Results showed a significant three-way χ2 (χ2(1, N = 69) = 10.33, p = .001, d = 0.84, CI [0.33, 1.35]), with two significant partial tables showing strong effect sizes (PCA-AVI: χ2(1, N = 42) = 4.49, p = .02, d = 0.69, CI [0.05, 1.33]; PCA-PI: χ2(1, N = 27) = 6.22, p = .01, d = 1.09, CI [0.23, 1.95]). Hence, for both groups, the court’s decisions at PCA completion were more likely to be in favor of the child staying at home for parents rated as capable of care than for those rated as not capable.
Child Placement 1 Year After PCA
Results showed a significant three-way χ2 (χ2(1, N = 69) = 11.33, p = .001, d = 0.89, CI [0.37, 1.40]). Partial tables were significant for both the PCA-AVI (χ2(1, N = 42) = 7.33, p = .006, d = 0.92, CI [0.25, 1.59]) and PCA-PI (χ2(1, N = 27) = 5.74, p = .02, d = 1.04, CI [0.19, 1.89]) groups. Hence, parents rated as capable of care by evaluators of both groups were more likely than those rated not capable of care to have kept their child at home 1 year after the PCA. FIML and CC analyses showed similar strong effect sizes with overlapping CIs (PCA-AVI FIML: d = 1.24, CI [0.70, 1.78]; CC: d = 0.99, CI [0.30, 1.69]; PCA-PI FIML: d = 2.33, 1.69 – 2.97; CC: d = 1.28, CI [0.17, 1.95]).
Child Re-reports of Maltreatment 1 Year After PCA
A significant three-way χ2 was found (χ2(1, N = 69) = 5.42, p = .01, d = 0.58, CI [0.09, 1.08]). The partial table for the PCA-PI group was not significant, with 45% of the cases correctly predicted (χ2(1, N = 27) = 0.05, p = .83, d = 0.09, CI [−0.67, 0.84]), but it was significant for the PCA-AVI group, with 64% of the cases correctly predicted (χ2(1, N = 42) = 7.25, p = .01, d = 0.91, CI [0.25, 1.58]). CC and FIML analyses showed strong effect sizes for the PCA-AVI group with overlapping CIs (FIML: d = 1.42, CI [0.86, 1.98]; CC: d = 0.94, CI [0.26, 1.63]), but effect sizes for the PCA-PI group remained low and not significant (FIML: d = 0.09, CI [−0.41, 0.59]; CC: d = .06, CI [−0.73, 0.84]).
Discussion
This is the one of the first RCT study to examine the value of a PCA protocol, with a short parent-child training embedded as an intervention component, to orient child placement decisions in cases of maltreatment. The necessity of evidence-based PCA protocols with a focus on the evaluation of the potential for enhanced parenting had been underscored in the attachment field (Van der Asdonk et al., 2020; van IJzendoorn et al., 2018). Two sets of findings emerged from this study. First, results indicate direct benefits of the AVI for the parent-child relationship. Second, findings present the AVI as a valuable addition to a PCA protocol for case orientation and child placement decision, with ratings of capacity to care by AVI evaluators being effective predictors of child placement and re-reports of maltreatment 1 year following the PCA. The stakes are high for maltreated children at risk of home removal, and placement decisions are prone to error and bias (De Haan et al., 2019). With this study, the AVI brings short attachment trainings to the forefront of clinical approaches that could be included to comprehensive PCAs to orient placement decision.
Parent and Child Benefits
Precisely, the first set of results reveals that the PCA-AVI group showed the highest improvements in parent-child interaction quality, that is, parents were more sensitive to child needs, and dyads engaged in more shared positive affect and reciprocal interactions than those of the PCA-PI group. The PCA-PI mean levels of interactive quality remained relatively the same from pre- to post-test, showing the AVI’s effectiveness over a psychoeducational intervention. Noteworthy, are the moderate d effect sizes of this comparison ranging from 0.52 to 0.62 (depending on the MI, FIML, or CC method). This is in line with the vast majority of attachment interventions showing enhanced parental sensitivity in vulnerable parents and supporting the role of caregiving quality in children’s well-being (Steele & Steele, 2018).
We found a similar, slightly lower rate of re-reports of maltreatment in this study (32%) in comparison to the rate reported in the latest 2008 Quebec Incidence study (42%, Hélie et al., 2012). However, contrary to our expectations, the PCA-AVI protocol, compared the PCA-PI protocol, did not lead to fewer re-reports of maltreatment in the following year, nor did it lead to fewer child placements at the end of the PCA or 1 year after PCA. This in contrast to studies showing fewer re-reports of maltreatment in the years following the Parent-Child Interaction Therapy (Chaffin et al., 2004; Thomas & Zimmer-Gembeck, 2011) or even to an ongoing AVI study indicating fewer child placements after intervention (Tarabulsy et al., 2019). Families in the control groups of these studies received regular services, whereas in our study, both groups had enhanced services which may have led to a lack of group differences. Still, given that we recruited families before a decision about placement was made, it may be that the multiple problems (psychopathology, domestic violence etc.) of parents in our sample were quite severe at intake. Very high-risk parents are often burdened with a heavy trauma history that has shown to impede treatment effects (Moran et al., 2005; Steele et al., 2019). A parent-child relationship of better quality following the AVI may not be sufficient to overcome the general toxicity that characterizes the lives of multi-problem parents, and treatment gains may gradually be lost in time. More research is needed to identify therapeutic targets that can address the multi-problems of very high-risk parents or that could help with sustaining therapeutic gains.
Case Orientation Benefits
The second set of results first shows that, regardless of the type of PCA, decisions to keep the child with the parent were more likely to occur for parents rated as capable of care than for those rated as not capable by their evaluators. Clearly, results of this study show that conclusions drawn by PCA evaluators guided social workers and judges’ placement decisions. But, we must ask: were these decisions any good? In our sample, more than half of the parents were rated as not capable of care (64%), while, only 42% of the children were placed or remained in placement at the end of the PCA. As in the jurisdictions of other countries (e.g. USA), the legal provisions of the Quebec Youth Protection Act clearly state that reasonable efforts to preserve (or reunify) families must be made by CPS, unless the child’s safety is not possible (Hélie et al., 2012). This may explain why placement rates are lower than what is being suggested by evaluators.
Another result of our study is that conclusions drawn by both groups of evaluators were associated with parent-child interactive improvements at PCA completion. Also, we found that parents rated as capable of care by evaluators of both protocols were more likely to live with their children 1 year after PCA. Given these results, it seems appropriate to think that assessment protocols with an embedded intervention component are valuable to orient the court’s placement decisions. The longer duration of the PCAs performed in our study over usual PCA services (about nine sessions instead of four for regular PCA services in the province of Quebec), and their dynamic (non-static) structure allowing for information gathering on the potential for enhanced parenting, may have helped evaluators, along with the assessment of other risk and protective factors, portray a comprehensive picture of the parents’ strengths and weaknesses. Future RCT studies with a control group providing regular PCA services will help confirm this.
However, when we examined rates of re-reports of maltreatment, only ratings made by PCA-AVI evaluators significantly predicted child re-reports of maltreatment in the year after PCA, with 64% of the cases correctly predicted. With this prediction, yielding strong d effect sizes ranging from 0.91 to 1.43 (depending on the MI, FIML, or CC method), we conclude that the PCA-AVI protocol is helpful to orient child placement decisions. For the PCA-PI group, this percentage only reached 45%. Also, given that PCA-AVI parents showed the highest scores in interaction quality at post-test and that such scores did not vary with the interplay of evaluators’ conclusions about capacity to care × PCA groups, results suggest that conclusions drawn by PCA-AVI evaluators are not solely based on the parent’s improvements in quality of interaction. As a result, this study proposes that relying solely on caregiving improvements to orient placement decisions would be a serious mistake. Relying on the parents’ potential for enhanced caregiving, while also considering other family risk and protective factors, as understood within an attachment framework, seems a rather accurate and promising avenue to guide placement decisions. We hypothesize that some parents with improved parent-child interaction at the end of the AVI may still be vulnerable to the negative influences of their environment or may show unpredictable care in the absence of support from their practitioner or because of psychological limitations, and thus would be rated as not capable of care by their PCA-AVI evaluators.
In our view, there are three key ingredients of the AVI that have helped PCA-AVI evaluators better predict re-reports of maltreatment than PCA-PI evaluators. The first key component is the training in attachment theory and in the observation of sensitive, insensitive and frightening/frightened parental behaviors. With more sharpened observational skills, it may have been easier for PCA-AVI evaluators to identify the daily parental behaviors relevant to maltreatment and to good enough care, and consequently to better understand how the potential for good enough parenting may be impacted by risk factors of the families’ larger ecological environment. Ongoing group supervision also served as continued learning opportunities for them. The second key ingredient is the use of positive reinforcement. AVI evaluators learned to search for parental strengths. This can help parents let down their defenses, better benefit from the AVI intervention, but also increase their openness towards the evaluation process. As representatives of the law, CPS evaluators are perceived as a potential threat by parents who are afraid to see their parental rights terminated. A third key component is the use of video-feedback, which has the potential to stimulate reflective functioning (Steele et al., 2014). Parents who exhibit frightening/frightened behaviors are mostly unaware of such behaviors often linked to past unresolved loss, abuse or trauma that have led to dissociative processes (Hesse & Main, 2006). Through video-feedback, parents are learning to observe their own and their child’s behaviors, to translate these behaviors into words, and then to relate them to emotions and intentions, thereby facilitating reflective functioning. When practitioners highlight positive parental behaviors, parents may gradually witness their own frightening/frightened behaviors, learn to use their growing sensitive behavioral repertoire to repair and reduce the occurrence of such distressing situations for the child, and engage in a process of change and reparation. In the context of a parenting capacity assessment, video-feedback may have facilitated the assessment of the parent’s reflective functioning, which can be quite useful to evaluate the extent with which parents become aware of their maltreating behaviors or their limitations as a parent.
Study Limitations and Strengths
As with many other maltreatment samples (e.g., Thomas & Zimmer-Gembeck, 2011), the attrition rate found in this study was relatively high (for the parent-child interaction quality variable). A MI procedure was used to replace missing values, though MI requires to be conservative. Thus, to ensure the robustness of our findings, analyses of significant results were repeated with a FIML and CC procedures. Moderate and strong effect sizes were found and convergence was shown across analyses. In addition, the sample sizes of the PCA groups did not include a comparable number of participants due to CPS not replacing evaluators promptly in the PCA-PI group. Yet, we maintained the randomization throughout the project, and this is an important strength considering that field RCTs are rare and challenging. A block randomization, as opposed to a simple randomization procedure, would have been preferable in our study of less than 100 participants (Kim & Shin, 2014). Another limitation is that some children were already placed at the beginning of PCA, as a temporary measure, and their chance of remaining placed may have been higher than for others. These children represented only a small proportion of the sample. Also, this study did not assess the predictive value of other risk and protective factors (e.g., parental social network, psychopathology) in the prediction of parenting capacities, although they were considered by PCA evaluators during their assessment. Finally, future studies should consider a less crude parental capacity to care measure (capable / not capable) and collect such data at intake to obtain a longitudinal and more precise measure of change from evaluators.
Conclusion
The PCA-AVI protocol successfully led to increases in parent-child interaction quality that were not found in dyads in the PCA-PI control group. Moreover, although conclusions drawn by both groups of evaluators were associated with parent-child interactive improvements, only those of PCA-AVI evaluators were predictive of child re-reports of maltreatment in the year following PCA. Therefore, the results of this study suggest that PCAs with an attachment intervention embedded as a means to assess the potential for enhanced parenting can successfully inform child placement decisions, as long as conclusions drawn by evaluators are not solely based on the parent’s improvements in parent-child interaction. We suggest caregiving improvements should be considered in relation to other family risk and protective factors. We also invite replication studies to further substantiate results of this study.
Supplemental Material
Supplemental Material, sj-pdf-1-cmx-10.1177_1077559520967995 - An Attachment-Based Parental Capacity Assessment to Orient Decision-Making in Child Protection Cases: A Randomized Control Trial
Supplemental Material, sj-pdf-1-cmx-10.1177_1077559520967995 for An Attachment-Based Parental Capacity Assessment to Orient Decision-Making in Child Protection Cases: A Randomized Control Trial by Chantal Cyr, Karine Dubois-Comtois, Daniel Paquette, Leonor Lopez and Marc Bigras in Child Maltreatment
Footnotes
Authors’ Note
We thank the participating families as well as the practitioners and the directors of the Child Protection Services for their valuable involvement in the project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by grants received from the Social Sciences and Humanities Research Council of Canada and the Fonds de Recherche du Québec—Santé to Chantal Cyr and by grants from the Fondation Lucie & André Chagnon to Marc Bigras, Daniel Paquette, and Chantal Cyr. Financial support was also provided to Chantal Cyr by the Canada Research Chairs Program.
Supplemental Material
Supplemental Material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.