
Abstract
Medicare home health coverage is an important resource for Medicare beneficiaries requiring health care at home. However, there have been changes in the United States health care system that might impact home health utilization such as pressures to constrain Medicare spending, growth in Medicare Advantage (MA) plan enrollment, decline in institutional long-term care and growth of Medicaid home- and community-based services. Given these changes, we examined home health care use trends among beneficiaries enrolled in traditional Medicare (TM) and MA from 2010 to 2020. We separately examined home health episodes that were initiated after a hospital or skilled nursing facility discharge and those initiated within the community and among dually and non-dually eligible beneficiaries. Home health use decreased among TM enrollees for both community-initiated and post-discharge needs but increased among MA enrollees for community-initiated home health use. Increases in community-initiated home health use were concentrated in non-dually eligible beneficiaries.
Introduction
Medicare home health coverage is an important resource for Medicare beneficiaries who need care at home. Home health agencies (HHAs) provide such services to homebound beneficiaries requiring skilled nursing, physical, occupational, or speech therapies. In 2019, about 3.3 million traditional Medicare (TM) beneficiaries received home health care, costing Medicare $17.8 billion (Medicare Payment Advisory Commission, 2021).
Home health care episodes can be classified into two distinct categories: post-discharge home health, initiated after a discharge from hospital, skilled nursing facility (SNF), or other institutional settings, and community-initiated home health. While post-discharge home health is typically designed to manage rehabilitation needs after an acute event, community-initiated home health care often addresses temporary skilled needs associated with long-term chronic conditions or functional decline. Recognizing these differences is essential for understanding trends and optimizing the delivery of home health services.
Recent pressures to constrain Medicare spending have led to increased demand for home health services due to its lower costs compared to institutional care (Navathe et al., 2017; Werner et al., 2024). Also, receiving care at home when possible is often more consistent with patient preferences. From 2002 to 2018, the number of home health episodes paid by TM increased by 56% and the share of beneficiaries using home health care increased by 22%, with most of the growth occurring before 2010 (Medicare Payment Advisory Commission, 2019).
At the same time, there has been substantial growth in Medicare Advantage (MA) enrollment. In 2023, 51% of Medicare beneficiaries were enrolled in MA (Ochieng et al., 2023). Institutional post-acute care use in inpatient rehabilitation facilities or SNFs is lower among beneficiaries enrolled in MA than TM, with a higher discharge rate to home without institutional post-acute care or home health (Skopec et al., 2020). Whether differences in home health use between MA and TM has changed with the growth in MA is unknown.
Furthermore, decline in institutional long-term care and growth of home-based long-term care may increase demand for home health care (Chidambaram & Burns, 2024). While Medicare’s home health benefit depends on having a skilled need, it does provide nonskilled services for beneficiaries receiving skilled services. Also, under the law, Medicare coverage of home health care is available for people with acute and/or chronic conditions, and for services to improve, maintain, or slow decline of an individual’s condition (Centers for Medicare and Medicaid Services, 2023; Glenda Jimmo et al. v. Kathleen Sebelius, 2012). These provisions may result in an increased demand for home health care as more older adults opt to age in place.
Additional factors may also affect the demand for both post-discharge and community-initiated home health care, including the declining availability of nursing home beds (Miller et al., 2023), which may increase need for help at home, and the growth of Medicaid home- and community-based services among dually eligible Medicare beneficiaries, which may increase home health care demand (Skira et al., 2022). Payment reforms, including the introduction of the Payment-Driven Groupings Model in 2020 and alternative payment models, may also affect the use of home health care.
Given these changes, we examined trends in Medicare-funded home health care over the past decade. We separately studied these trends among beneficiaries enrolled in TM and MA as well as among those who are and are not dually eligible. We also separately examined home health episodes initiated after a discharge from hospital or SNF and those initiated within the community.
New Contribution
To our knowledge, only one previous paper has compared trends in home health episodes initiated from the community versus post-discharge (Zuckerman et al., 2020). Zuckerman et al. showed from 2011 to 2016, the share of Medicare beneficiaries using home health grew faster among MA enrollees than TM enrollees for both community-initiated and post-discharge episodes. Our work confirms and updates these results through 2020 and also extends these results by comparing trends for duals and non-duals.
Study Data and Methods
Data Sources and Study Population
We included all home health episodes reported in the Outcome and Assessment Information Set (OASIS) data from January 1, 2010 to November 1, 2020. The OASIS includes all assessments for home health episodes provided by Medicare-certified HHAs, including beneficiaries enrolled in both TM and MA. We linked these data to the 100% Master Beneficiary Summary File (MBSF) to identify Medicare enrollees aged 65 or older and classify them as either enrolled in TM or MA during their home health episode. We excluded home health episodes where the beneficiary switched between TM and MA. We classified beneficiaries as dually eligible if qualified for full-state Medicaid benefits alongside Medicare and were enrolled in both during the home health episode.
We further classified home health episodes as being either community-initiated or post-acute care (or post-discharge). Post-discharge home health episodes were identified by linking the OASIS data with hospital and SNF discharge dates from the 100% Medicare Provider Analysis and Review file (MedPAR). Home health admissions that were not within 14 days of a hospital or SNF discharge were classified as community initiated. Home health episodes that occurred within 14 days of hospital or SNF discharge but where the assessment was labeled as a “resumption of care,” indicating that the episode had started prior to hospital or SNF admission, were also considered community initiated. Remaining episodes with an admission assessment that occurred within 14 days of discharge from an acute care hospital or an SNF were considered post-acute care.
Measures of Home Health Care Use
Our unit of analysis was the home health episode. During most of the period we study, Medicare defined a home health episode as 60 days, and home health episodes could be recertified as many times as needed if the beneficiary was still eligible for home health. For analyses, we included the initial episode and all recertifications as one episode of care. We deemed an episode concluded upon the beneficiary’s discharge from the HHA, hospitalization without indication of reentry into home health or death.
We first describe the beneficiaries’ characteristics at admission to home health, including age, sociodemographic information (from the MBSF file), independence in six activities of daily living (ADLs), which were bathing, dressing, toileting, transferring, continence, and eating, summary ADL score indicating overall independence from OASIS (Katz et al., 1963), and clinical conditions including Alzheimer’s disease and related dementia (ADRD) (Bélanger et al., 2023), diabetes, heart failure, hypertension, ischemic heart disease, rheumatoid arthritis/osteoarthritis (from OASIS).
We then calculated quarterly county-level home health initiation over the study period among beneficiaries enrolled in TM and MA. Community-initiated and post-discharge use were calculated separately for each group. To account for changes in enrollment over time, we divided the episode count by the number of Medicare beneficiaries enrolled in TM or MA in each county.
We also calculated the use for dually and non-dually eligible beneficiaries in TM and MA to examine whether trends in home health use were more pronounced in either group. This involved dividing the number of home health episodes initiated in each quarter among dually or non-dually eligible beneficiaries by the total number dually or non-dually eligible individuals within the same Medicare plan category (TM or MA) in each county-quarter.
To account for changes in MA and TM enrollment over the study period, we adjusted rates of home health use in each group for patient characteristics. We used individual-level data from MBSF to calculate quarterly county-level averages of age, sex, race/ethnicity, and dual eligibility in the group of Medicare beneficiaries of interest (TM or MA). Linear regression was used to adjust the county-level rates of home health episodes among each group for these beneficiary characteristics plus county and time-fixed effects, clustering standard errors at the county level. The regression analyses were weighted by the county-level number of TM, MA, dually eligible in TM, dually eligible in MA, non-dually eligible in TM or non-dually eligible in MA, depending on the outcome variable. We opted to include race/ethnicity as a covariate in our base models, as we had sparse information on individual-level beneficiary characteristics and race/ethnicity is correlated with disease burden and illness severity. However, as a sensitivity check, we also ran our models without adjusting for race/ethnicity.
Finally, we report each home health episode median length in days, stratified by place of initiation (community versus post-discharge) and by Medicare enrollment (TM versus MA), adjusting county-quarter-level medians using Poisson regression.
We report differences in home health utilization between 2010 and the first quarter of 2020. We selected the first quarter of 2020 as the reference time point for these comparisons as subsequent quarters were affected by the onset of the COVID-19 pandemic, which introduced significant disruptions to health care systems, patient care, and utilization trends. Therefore, we decided to use the first quarter of 2020 as the comparison for trend from 2010.
We test whether the trends from Q1 2010 to Q1 2020 are statistically significantly different from zero using linear regression, examining the outcomes as a function of a continuous measure of time as the independent variable.
All analyses were performed using Stata 18.0.
Results
Our individual-level data included 48,623,075 home health episodes between 2010 and 2020 from 20,535,900 Medicare beneficiaries. TM paid for over two-thirds of these episodes (71.7% TM and 28.3% MA) and about half of all episodes were community-initiated (49.6% community and 50.4% post-discharge initiated).
Patient Characteristics
Table 1 contains patient characteristics at initiation of each home health episode. Compared to those initiating home health post-discharge, those initiating from the community were older (80.8 years vs. 78.9 years), more likely to be female (65.0% vs. 60.9%), racial/ethnic minorities (19.9% vs. 15.2%), and dually enrolled (20.2% vs. 12.8%). Beneficiaries with community-initiated home health episodes were more likely to have ADRD (28.1% vs. 16.5%) or rheumatoid arthritis/osteoarthritis (23.5 vs. 20.0) but less likely to have heart failure (16.2% vs. 23.4%) or ischemic heart disease (15.6% vs. 21.9%).
Description of Home Health Cohort.
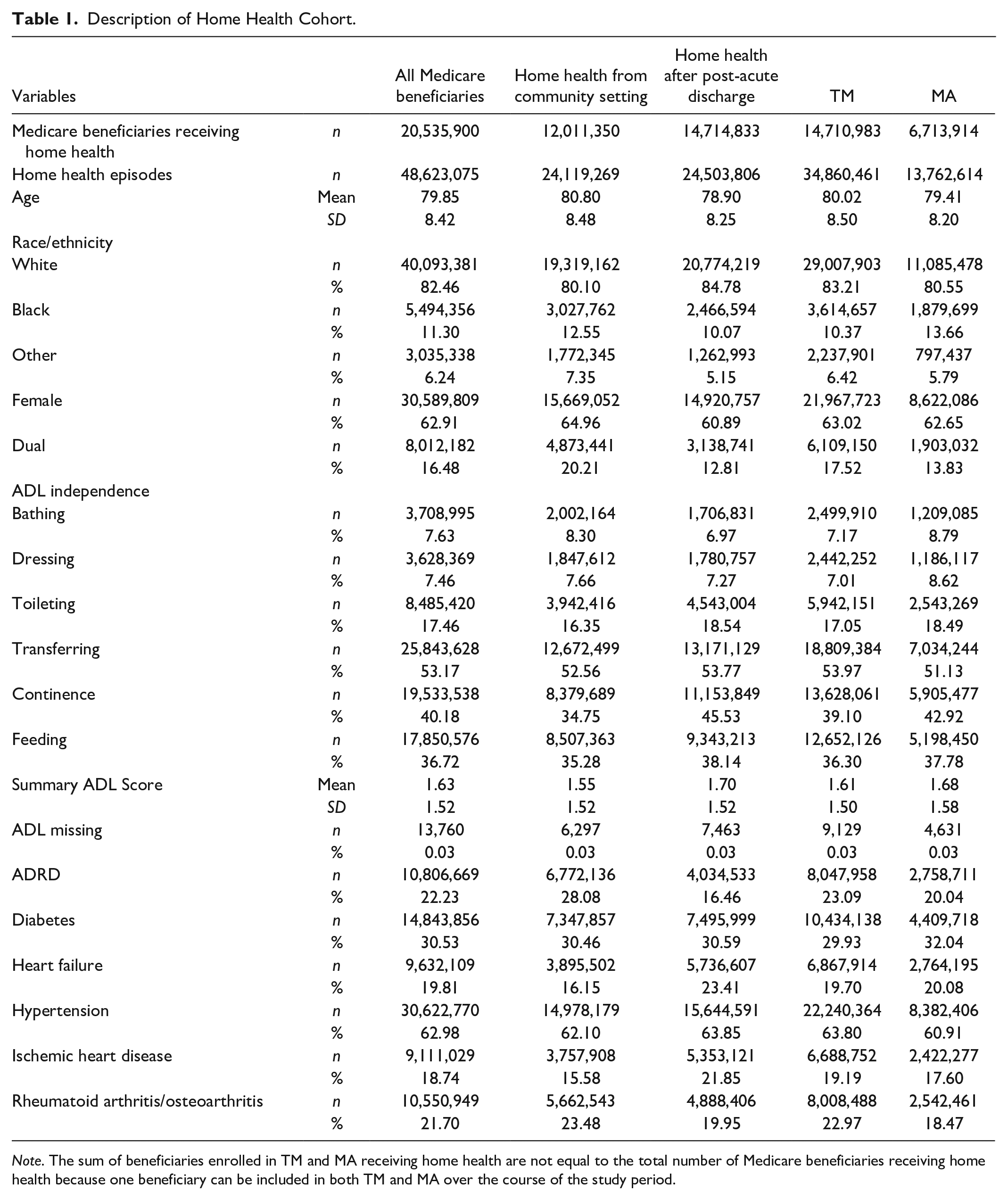
Note. The sum of beneficiaries enrolled in TM and MA receiving home health are not equal to the total number of Medicare beneficiaries receiving home health because one beneficiary can be included in both TM and MA over the course of the study period.
Patients covered by TM and MA were similar, but the TM cohort of home health users had more dually eligible beneficiaries (17.5% vs. 13.8%).
Home Health Use
Figure 1 shows adjusted trends in home health use, calculated as the quarterly number of community- and post-discharge-initiated home health episodes per 1,000 enrolled beneficiaries. Overall, home health use rate was lower among MA enrollees than TM enrollees. TM-covered home health use declined slightly for both community-initiated (13.4 episodes in 2010 Q1 to 12.7 in 2020 Q1; p = .005) and post-discharge episodes (16.6 in 2010 Q1 to 14.4 in 2020 Q1; p = .010), particularly in the latter half of the period. MA-covered community-initiated episodes increased over the period (11.0 in 2010 Q1 to 12.9 in 2020 Q1; p < .001). MA-covered post-discharge episodes increased through 2018 (p < .001) and then declined to levels similar to 2010 (p = .028). For all groups, there was a decrease in home health use starting in the second quarter of 2020, which coincided with the COVID-19 pandemic.
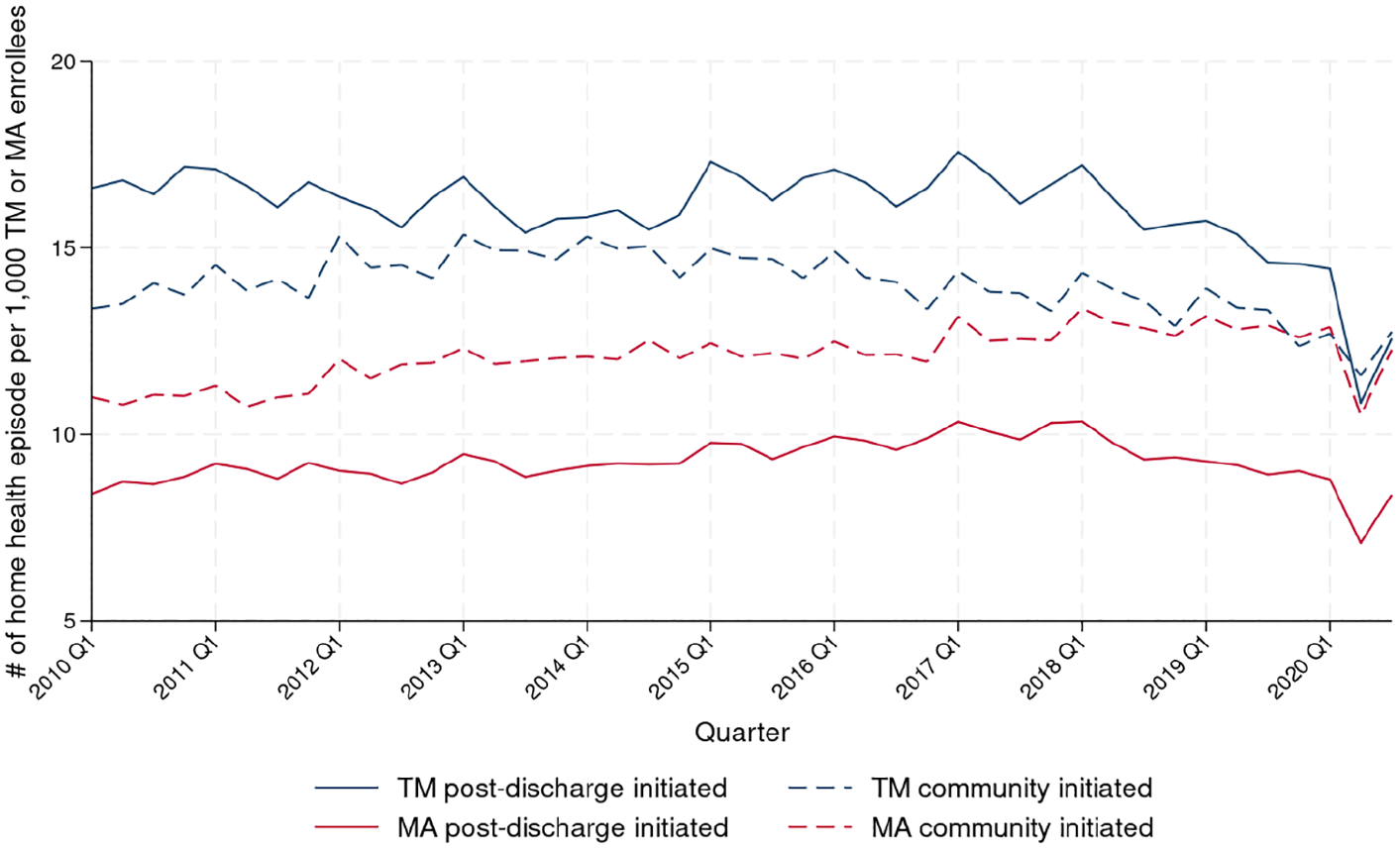
Number of Home Health Episodes Initiated per 1,000 Enrolled Medicare Beneficiaries, Stratified by Whether the Episode Was Covered by TM or MA and Whether It Was Initiated in the Community or After Hospital or SNF Discharge.
Among dually eligible beneficiaries enrolled in TM, community-initiated home health use decreased (Figure 2; 30.5 episodes in 2010 Q1 to 27.0 in 2020 Q1; p < .001) while post-discharge episodes were stable (21.0 episodes in 2010 Q1 to 20.2 in 2020 Q1; p = .237). At the same time, the change in home health use was small and not statistically significant among dually eligible beneficiaries enrolled in MA for community-initiated (20.4 episodes in 2010 Q1 to 20.0 in 2020 Q1; p = .119). For post-discharge episodes, the change was also small but statistically significant (12.6 in 2010 Q1 to 11.7 in 2020 Q1; p = .014). Similar to all Medicare enrollees, home health use decreased among dually eligible beneficiaries in the second quarter of 2020.
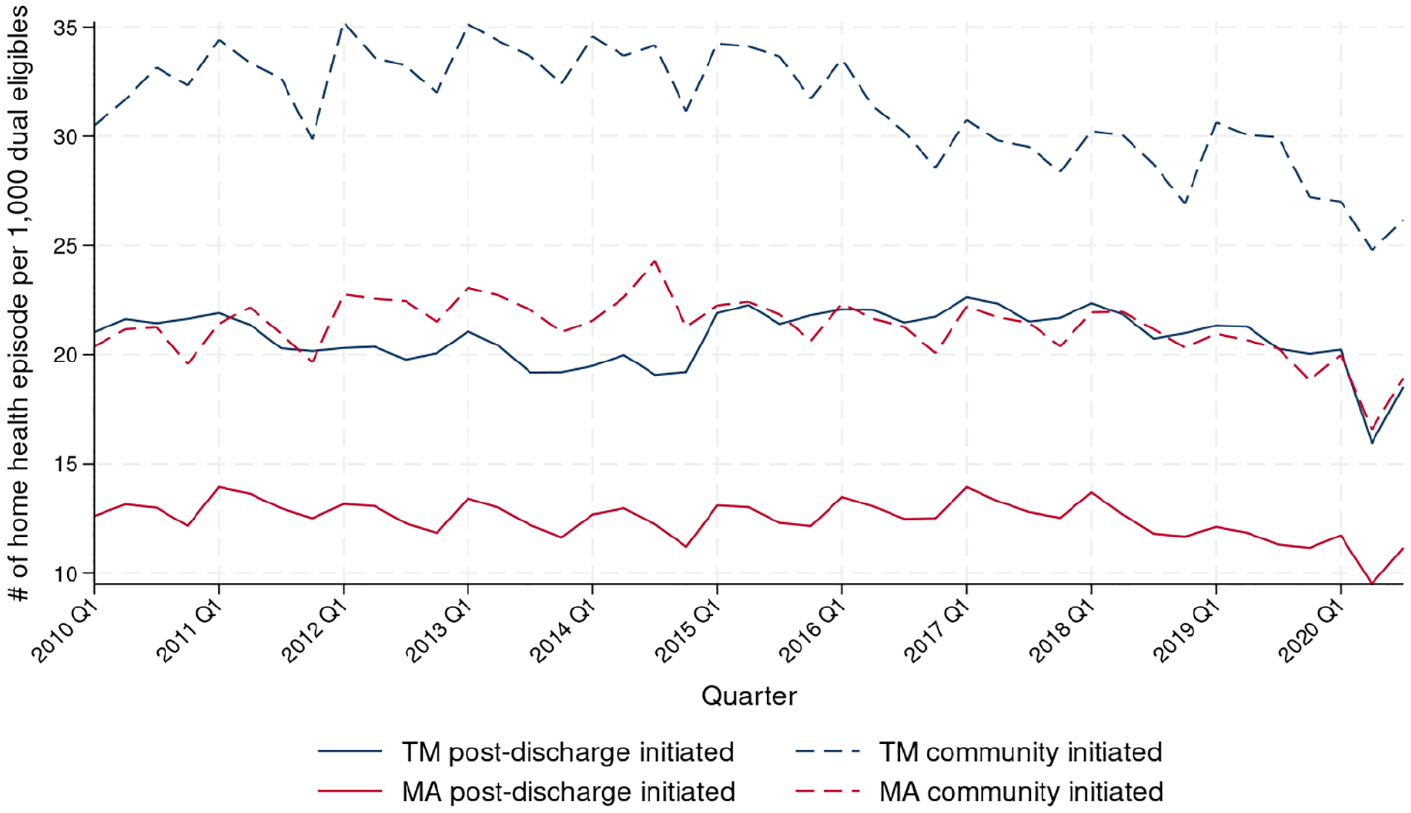
Number of Home Health Episodes for Dually Eligible Beneficiaries per 1,000 Individuals Who Are Either Dually Eligible and Enrolled in TM or Dually Eligible and Enrolled in MA, Stratified by Whether the Episode Was Covered by TM or MA and Whether It Was Initiated in the Community or After Hospital or SNF Discharge.
Non-dually eligible beneficiaries used less home health than dually eligible beneficiaries (Figure 3). Among non-dually eligible beneficiaries in TM, community-initiated home health use increased through the first quarter of 2018 (10.9 in 2010 Q1 to 12.8 episodes in 2018 Q1; p < .001) and then declined to 11.5 episodes in first quarter of 2020 (p = .014). For post-discharge episodes, home health use decreased among non-dually eligible beneficiaries in TM, particularly in the later years (16.0 in 2010 Q1 to 13.9 in 2020 Q1; p = .010). For those in MA, community-initiated home health use increased (10.3 episodes per 1,000 non-dually eligible in MA enrollees in 2010 Q1 to 12.0 in 2020 Q1; p < .001) as did post-discharge home health use until the first quarter of 2018 (8.1 episodes in 2010 Q1 to 10.0 in 2018 Q1; p < .001), but then dropped to 8.4 episodes in the first quarter of 2020 (p < .001).
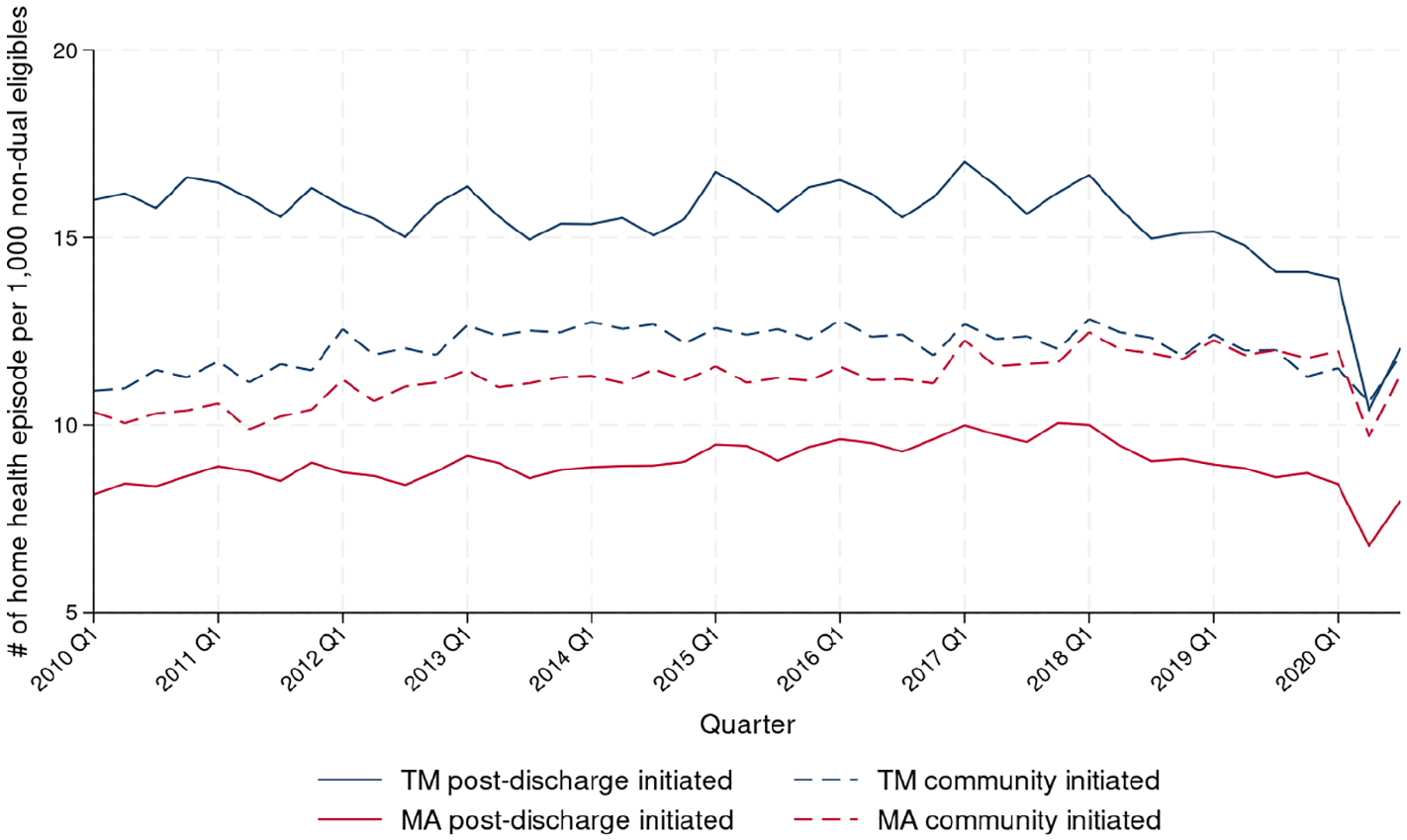
Number of Home Health Episodes for Non-Dual-Eligible Beneficiaries per 1,000 Individuals Who Are Either Not Dually Eligible and Enrolled in TM or Not Dually Eligible and Enrolled in MA, Stratified by Whether the Episode Was Covered by TM or MA and Whether It Was Initiated in the Community or After Hospital or SNF Discharge.
The median length of home health episodes from 2010 to 2020 is shown in Figure 4. Overall, episodes were shorter for MA-covered episodes than the corresponding TM-covered episodes. Over time, post-discharge-initiated episode lengths remained constant for both TM and MA-covered episodes. Community-initiated TM- and MA-covered episodes decreased in length between 2010 and 2020 (from 53.2 days in 2010 to 44.3 days in 2020 Q1 for TM and from 45.8 days in 2010 to 36.7 days in 2020 Q1 for MA; p < .001 for both TM and MA). Starting in the second quarter of 2020, during the COVID-19 pandemic, episode lengths increased across all groups, then decreased in the third quarter.
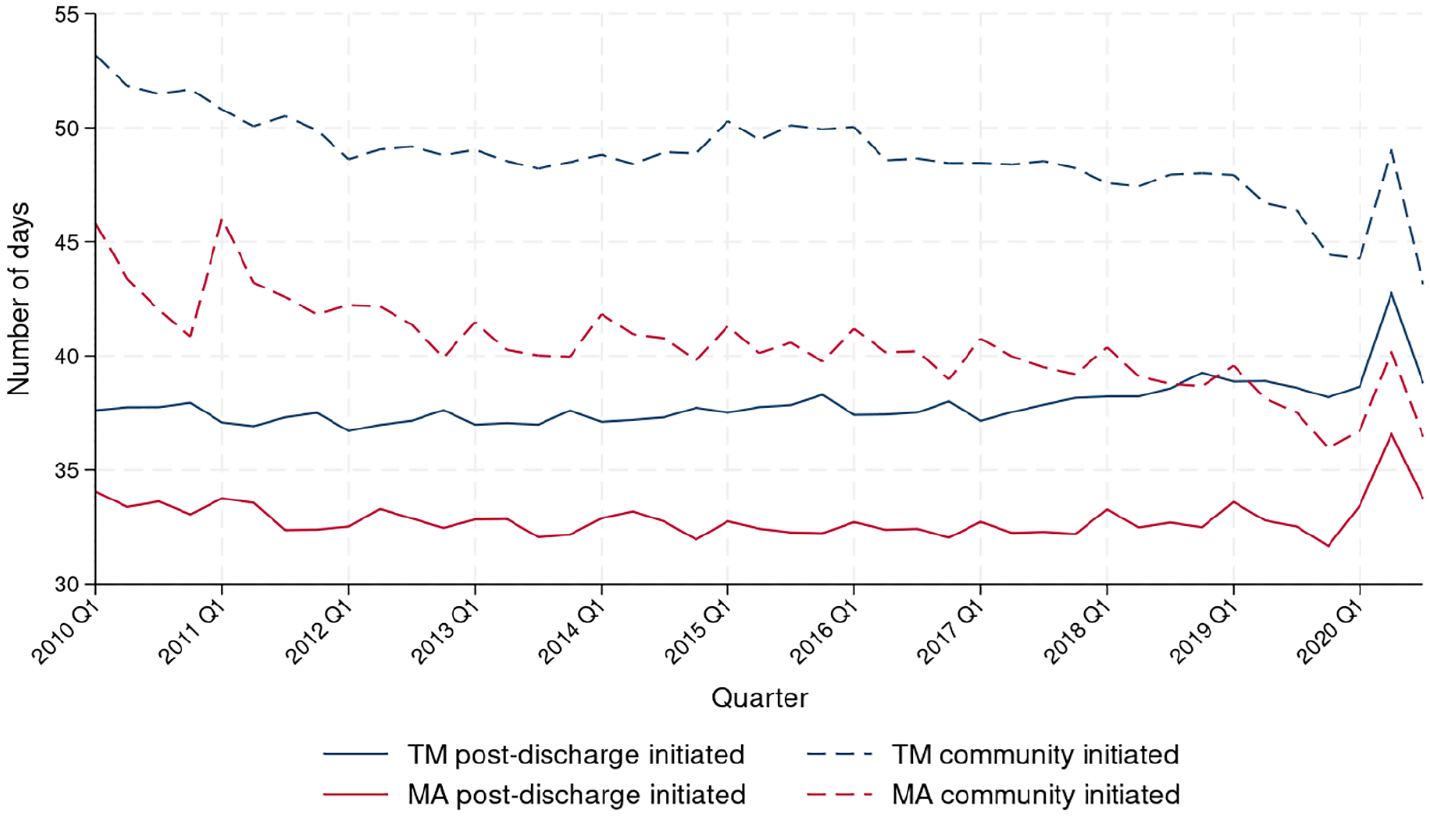
Median Length of Home Health Episode (in Days), Stratified by Whether the Episode Was Covered by TM or MA and Whether It Was Initiated in the Community or After Hospital or SNF Discharge.
Excluding race/ethnicity from risk adjustment did not alter the findings qualitatively and results remained consistent (Supplemental Appendix Figures A1–A4).
Discussion
From 2010 to 2020, home health use was higher among TM enrollees compared to MA enrollees but declined for both community-initiated and post-discharge needs. Meanwhile, among MA enrollees, community-initiated home health use increased. When examining dually and non-dually eligible populations separately, dually eligible enrollees had higher home health use, but community-initiated home health use increased only among non-dually eligible beneficiaries. In addition, the median duration of community-initiated home health episodes decreased over most of this period for MA enrollees.
Prior research has examined trends in home health care use, focusing on differences in use between TM and MA enrollees. One study, comparing post-acute care use in TM and MA in 2015 to 2016 for three common conditions, found that home health use was lower among MA enrollees compared to TM enrollees (Skopec et al., 2020). Similar findings were reported for the years 2010 to 2011 (Huckfeldt et al., 2017). Prior work also showed home health episodes were shorter for MA enrollees than TM enrollees (Waxman et al., 2016). Research focusing on patients with ADRD found that most patients referred to home health from the community had ADRD (Ankuda et al., 2020; Burgdorf et al., 2020) and patients with ADRD had more and longer home health episodes (Burgdorf et al., 2024).
Zuckerman et al. also compared trends in home health episodes initiated from the community versus after post-discharge (Zuckerman et al., 2020). The authors found that the share of Medicare beneficiaries using home health grew faster among MA enrollees than TM enrollees for both community-initiated and post-discharge episodes from 2011 to 2016. Our work confirms and updates these results through 2020. We find that for MA enrollees, home health care use increased by 17.1% for community-initiated home health and by 4.6% for post-acute home health from 2010 Q1 to 2020 Q1. Conversely, home health care use decreased for TM enrollees by 4.9% for community-initiated home health and by 13.0% for post-acute home health from 2010 Q1 to 2020 Q1. We also extend these results by comparing trends for duals and non-duals and show that home health use among TM enrollees declined after 2016, while it continued to grow for MA enrollees.
Zuckerman et al. (2020) also looked at changes in the length of home health episodes, examining means rather than the medians we use, and found decreased episode length between 2011 and 2016 for both MA and TM as well as for community-initiated and post-discharge episodes.
Several explanations may account for the trends in home health use we observe. First, it is possible that home health is increasingly used as a substitute for long-term care. While the Medicare-funded home health care benefit is not designed to provide long-term care, it may temporarily fill gaps in care for people with unmet long-term care needs by covering home-based care for skilled needs. Although eligibility for Medicare’s home health benefit depends on having a skilled need, it does provide nonskilled services for beneficiaries receiving skilled services. This substitution could explain the increase in community-initiated home heath episodes among non-dually eligible beneficiaries but not dually eligibles beneficiaries, as dually eligible beneficiaries have access to Medicaid-covered long-term care services, and thus may rely less on Medicare-funded home health care.
Home health may have expanded to fill some of the gaps in our current long-term care system in the United States particularly for MA enrollees in community-based settings. The increasing community-initiated home health use among MA enrollees, along with the flexibilities provided by MA in covering nonskilled in-home care services (Gondi & Gebremedhin, 2021), may suggest that beneficiaries are increasingly relying on home health care to fill gaps in long-term care.
It is also possible that the differential trends between MA and TM that we observe are driven in part by patient selection. That is, as more beneficiaries switch from TM to MA (Unuigbe et al., 2022; Xu et al., 2023), if those switchers are more likely to use community-initiated home health care, it could result in the trends we observe. We adjust trends statistically to try to account for this but may do so incompletely given the limited data we have on patient characteristics. Also, the rise in in-home risk assessments in MA plans to capture more comorbidities may contribute to the increasing trend in home health use in MA (Jacobs, 2024).
Lower median length of home health episode for beneficiaries enrolled in MA could be explained by the MA plan’s payment structure (Waxman et al., 2016). HHAs are allocated a monthly fixed rate per enrollee which incentivizes them to reduce cost. In addition, qualitative evidence suggests that payment per visit is lower for MA than TM (Waxman et al., 2016).
Concurrent trends in health care delivery over the last decade may influence observed home health care use. For example, with the implementation of alternative payment models, more hospital discharges are to home rather than to a SNF (Werner et al., 2024). Ongoing work to further decompose and understand the drivers of these trends will be important to fully understand their implications.
There were several limitations to this study. First, this study was not designed to understand the mechanisms behind observed trends in home health care use and does not provide a detailed exploration of the factors driving the changes in home health care utilization among TM and MA enrollees. Second, we are unable to distinguish whether the trends we observe are due to the shifting of surgical procedures from inpatient to outpatient settings (Burke et al., 2023). If a patient received home health care after such procedures, we may have misclassified these patients as receiving community-initiated home health care instead of post-discharge home health care. Third, the COVID-19 pandemic started in the final year of our data (2020), which is also the year that Medicare payment for home health was substantially altered through the Patient-Driven Grouping Model; these may both confound the 2020 numbers. Despite these limitations, this study serves as a valuable starting point, highlighting the need for more in-depth research on the drivers of changes in home health care trends and their implications.
Recognition of the changing use of home health care is important. With rapid MA growth (Unuigbe et al., 2022), particularly among dually eligible individuals (Xu et al., 2023), trends of increasing use in these populations may be expected to continue. With prior research showing that MA beneficiaries are typically served by lower-quality HHAs than TM (Schwartz et al., 2019), further investigation into how the growth of home health care among MA enrollees differentially impacts patient outcomes is needed.
Supplemental Material
sj-docx-1-mcr-10.1177_10775587251318407 – Supplemental material for Home Health Care Use Among Medicare Beneficiaries From 2010 to 2020
Supplemental material, sj-docx-1-mcr-10.1177_10775587251318407 for Home Health Care Use Among Medicare Beneficiaries From 2010 to 2020 by Seiyoun Kim, Mingyu Qi, R. Tamara Konetzka and Rachel M. Werner in Medical Care Research and Review
Footnotes
Acknowledgements
The authors thank Rhys Chua for her valuable assistance with the data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Work on this study was supported by the National Institute on Aging (grant nos. R01-AG066114 and K24-AG047908).
Ethnical Approval and Informed Consent Statement
The study was approved with a waiver of informed consent by the University of Pennsylvania Institutional Review Board and Centers for Medicare & Medicaid Services Privacy Board because the research using large administrative data sets could not be carried out practicably without a waiver of consent.
Data Availability Statement
Access to the data used in this study is restricted and subject to the regulations and policies of the Centers for Medicare and Medicare Services. Therefore, the data cannot be shared publicly. For further inquiries, please contact the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.