
Abstract
Post-acute care users in Medicare Advantage (MA) plans may seek coverage changes if facing issues with plan benefits. In 2019, the Centers for Medicare and Medicaid Services extended the deadline to disenroll from an MA plan from February 14 to March 31 and, for the first time, permitted beneficiaries to switch to a different MA plan instead of traditional Medicare. Using 2016–2019 Medicare administrative data, we implemented a difference-in-differences approach to evaluate the impact of this policy on disenrollment from a plan within 1 month of initiating skilled nursing facility or home health services. When MA disenrollment rules became more flexible, overall rates of exiting MA plans did not change. Switching to a different MA plan increased after the policy change, but this outcome was so rare that this increase did not affect overall rates of exiting MA plans.
Introduction
Medicare beneficiaries must choose whether to receive their benefits under traditional Medicare (TM) or through a Medicare Advantage (MA) plan. The MA program has grown in popularity over time, with 51% of beneficiaries participating in MA private plans in 2023 (Ochieng et al., 2023). Beneficiaries enrolled in MA face trade-offs about how important services like post-acute care are covered. MA plans receive risk-adjusted capitated payment rates and have discretion to implement varied benefit designs, narrow networks, and utilization management tools to control costs. To ensure their care is covered, enrollees must remain in their plan’s network, potentially limiting their choice of post-acute provider. Plans also have financial incentives to steer patients toward lower acuity settings, limit their stay in a skilled nursing facility (SNF) (Gadbois et al., 2018), or refuse prior authorization for this care (Skopec et al., 2020). In exchange for these limitations, enrollees receive lower premiums, an out-of-pocket maximum, and supplemental benefits not included under TM coverage.
During the year, Medicare beneficiaries have two enrollment periods they can use to change their coverage (outside of special circumstances). The annual Medicare Open Enrollment Period is open to all Medicare beneficiaries, while the Medicare Advantage Open Enrollment Period is only available to MA enrollees. The annual Medicare Open Enrollment Period occurs each fall from October 15 to December 7, with the beneficiary’s enrollment choice becoming effective the following January. During this period, beneficiaries can switch MA plans, switch from MA to TM, or switch from TM to MA. To limit favorable selection (Mcguire et al., 2011; Newhouse et al., 2015), beneficiaries are largely locked into their choice for the year. However, the Centers for Medicare & Medicaid Services (CMS) provides MA enrollees the opportunity to change coverage before a deadline set by the agency (i.e., Medicare Advantage Open Enrollment Period). This deadline provides protection to beneficiaries enrolled in MA by giving them the opportunity to reassess and change their enrollment choice during the first few months of the calendar year.
Beginning January 2019, CMS extended the deadline to reassess MA coverage from February 14 to March 31 and, for the first time, permitted beneficiaries to switch to a different MA plan as opposed to having to enter TM. MA enrollees admitted to a SNF or initiating home health care may be particularly motivated to switch coverage if they encounter difficulties with their plan’s post-acute benefits prior to this disenrollment deadline. Beneficiaries who use home health or nursing home services (Goldberg et al., 2017) have higher rates of leaving MA for TM than other beneficiaries (Rahman et al., 2015). More broadly, patients who are dual-eligible (Meyers, Belanger, et al., 2019), have Alzheimer’s Disease and Related Dementias (Meyers et al., 2021), have high health care needs (Lissenden, 2019; Meyers, Belanger, et al., 2019; Park et al., 2021), or disabilities (Ankuda et al., 2020) are more likely to disenroll from MA. MA enrollees have also reported less functional improvement when using post-acute-care services (Achola et al., 2023) and prior evidence suggests that MA enrollees are more likely to use lower quality SNFs compared with TM beneficiaries (Meyers et al., 2018). These results indicate the MA program may not meet the needs of post-acute care users.
This extension of the disenrollment deadline could provide beneficiaries who encounter problems accessing post-acute care through their plan the opportunity to quickly gain coverage that better meets their needs. We examine the effect of this policy change on overall rates of switching within 1 month of initiating post-acute care. We also examine the type of switch (switching from MA to TM or switching to a different MA plan) among individuals using SNF or home health care.
Conceptual Framework
There are likely several mechanisms motivating a beneficiary’s switch to different coverage, particularly for those who are initiating use of post-acute care. Beneficiaries can experience several hurdles when seeking post-acute services. MA plans may control the use of SNF care by ensuring beneficiaries receive prior authorization for initial and subsequent care or limiting the amount of time a beneficiary can stay in a SNF (Gadbois et al., 2018). MA plans may also have narrow networks for this type of care, limiting a patient’s choice of provider. This could be suboptimal for beneficiaries who desire to remain closer to home when receiving care, which has been documented as a large factor in a patient’s choice of facility (MedPAC, 2018). These barriers in MA may cause a beneficiary to seek new coverage that either provides them with less restrictions on choices of providers or has better post-acute benefits with fewer hurdles. This study focuses on enrollment switches that occur shortly after initiating post-acute care to understand how greater flexibility to leave MA plans affected enrollment among those actively trying to access SNF or home health care.
Method
Data Sources and Study Population
We used 2016–2019 Medicare Master Beneficiary Summary File enrollment data to assess monthly MA enrollment status. To determine post-acute care use, we used the Minimum Data Set nursing home assessment data and Outcome and Assessment Information Set (OASIS) home health assessment data. Finally, we used records from the Medicare Provider Analysis and Review (MedPAR) file, which captures information on hospital admissions, to identify MA enrollees with hospitalizations preceding SNF or home health use. MedPAR data capture hospitalizations for MA enrollees who receive care at hospitals receiving Disproportionate Share Hospital (DSH) payments or medical education payments, though other hospitals also submit inpatient encounters to MedPAR (Kumar et al., 2018). Roughly 90% of Medicare hospital stays occur at hospitals receiving DSH or medical education payments (Huckfeldt et al., 2017; Kumar et al., 2018).
Our study population included MA beneficiaries admitted to a nursing home or initiating a home health episode in January, March, or April of 2016–2019 within 7 days of hospital discharge. While beneficiaries using post-acute services in the latter half of February would potentially be affected by the policy change, we excluded beneficiaries with February post-acute use because beneficiaries always had the option of disenrolling from MA prior to February 14. Focusing on January and March admissions relative to April admissions allowed us to make cleaner comparisons. We excluded beneficiaries who were dual-eligible for Medicare and Medicaid at the time of admission since these beneficiaries have differing lock-in rules than the Medicare-only population. We also excluded beneficiaries with post-acute care use in the prior year to capture incident post-acute use, and beneficiaries missing enrollment data. Within the home health cohort, we excluded home health episodes that were preceded by a SNF stay.
Study Design
We used a difference-in-differences (DiD) approach to examine MA plan changes among individuals with post-acute SNF or home health use before and after the extension of the disenrollment deadline. Our control group included beneficiaries using post-acute care in April since these beneficiaries were not affected by the policy and were largely locked into their enrollment choices unless there are exceptional circumstances that trigger eligibility for disenrollment. Our first treatment group consisted of January post-acute users: this group was always able to leave MA but under the new policy could switch to a different MA plan. Our second treatment group consisted of March post-acute users: under the extended deadline for disenrollment, these beneficiaries gained the option to leave MA for TM or change MA plans.
Study Measures
Our main outcome was any disenrollment from a beneficiary’s MA plan in the month following new post-acute care use. We also examined beneficiaries’ subsequent coverage choice: MA program exit (i.e., disenrollment from their MA plan to TM) or MA plan switch (i.e., switching MA plans). Beneficiaries’ enrollment changes are effective on the first day of the subsequent month. For example, a beneficiary who selects a new plan on January 10 will be enrolled in that plan on February 1. Because beneficiaries may have not immediately decided to change their coverage after initiating post-acute services, for January and April admissions we also measured the outcomes of interest 2 and 3 months post-post-acute care use as sensitivity analyses.
Our model included beneficiary sociodemographic and clinical characteristics: age, Research Triangle Institute (RTI) race/ethnicity (Eicheldinger & Bonito, 2008), gender, reason for Medicare entitlement, hospital length of stay, year and county fixed effects, and hospital diagnosis-related group (DRG) during the beneficiary’s preceding hospital stay.
Analytic Approach
To assess the validity of the DiD design, we visually inspected plots of the unadjusted outcomes and formally tested whether there were pre-period differences in changes in outcomes between the treated and control groups. We report these event study coefficients in the appendix of the paper (Supplemental eTables 1 and 3). We fit linear probability models for all outcomes, adjusting for patient sociodemographic and clinical characteristics, included year and county fixed effects, and clustered standard errors at the beneficiary level. Analyses were conducted using STATA/MP 17.0; results were 2-sided and considered statistically significant at p < .05.
Results
Cohort Characteristics
Our study included 330,428 nursing home admissions and 288,811 home health episodes. Across SNF users with different months of admission, there were small statistically significant differences in age and prevalence of specific DRGs during preceding hospital stays, but there were not practically meaningful differences between the treatment and control groups. We observed no racial or gender differences between the admission groups or differences in hospital length of stay (Table 1). Similarly, there were few clinically meaningful differences between beneficiaries based on the month a home health episode began. Beneficiaries with March (10.3%) home health episodes were more likely to be Black relative to beneficiaries with January (9.4%) and April (9.9%) home health episodes (p-value = .001). Beneficiaries with home health episodes in March stayed 0.1 days longer in the hospital relative to beneficiaries with January and April episodes (p-value = .029). We observed no differences in age, gender, or Medicare entitlement reason among the groups (Table 1).
Characteristics of Post-Acute Care Users, 2016.
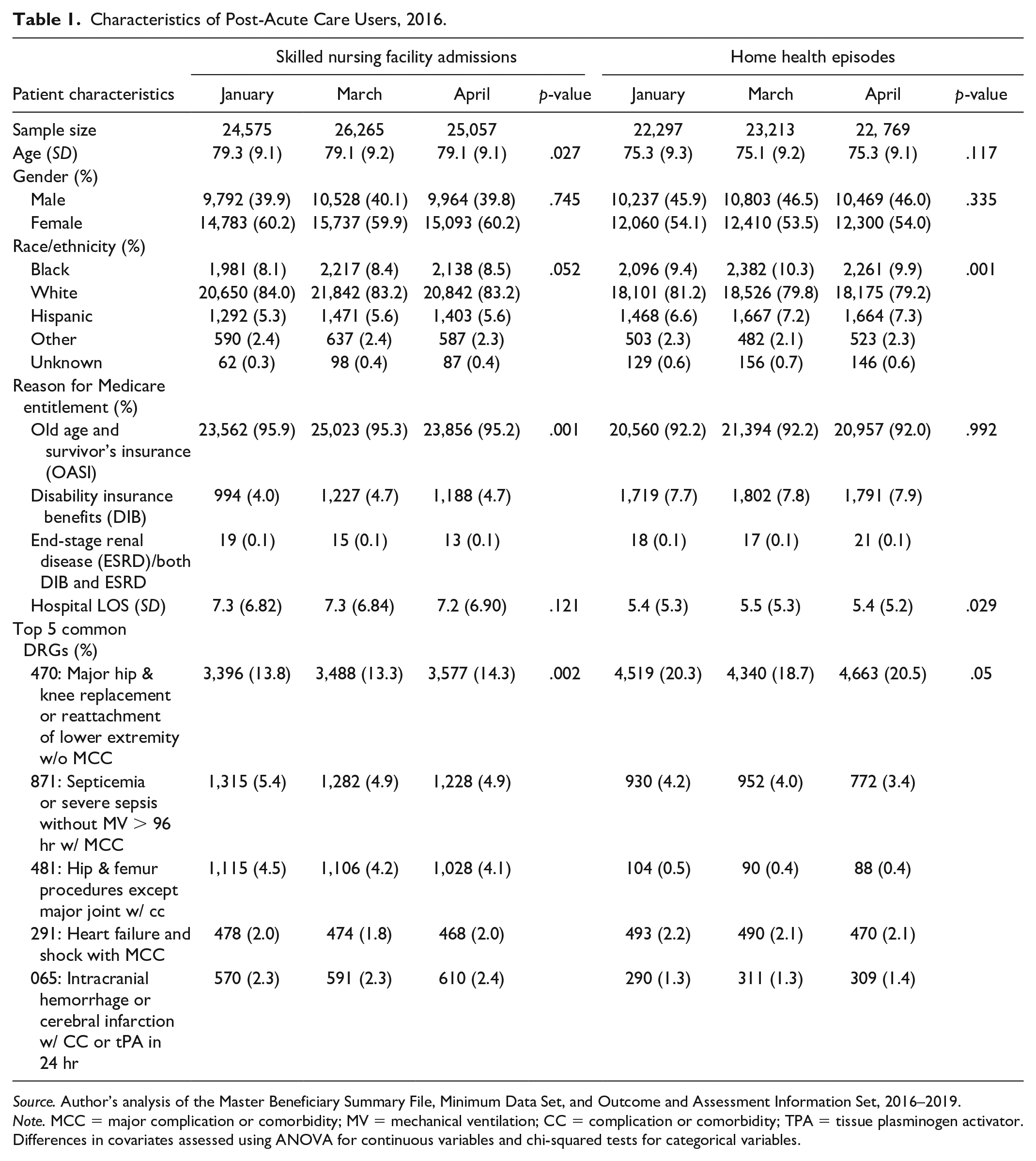
Source. Author’s analysis of the Master Beneficiary Summary File, Minimum Data Set, and Outcome and Assessment Information Set, 2016–2019.
Note. MCC = major complication or comorbidity; MV = mechanical ventilation; CC = complication or comorbidity; TPA = tissue plasminogen activator. Differences in covariates assessed using ANOVA for continuous variables and chi-squared tests for categorical variables.
Skilled Nursing Facility Users
Our visual assessment of unadjusted outcomes among SNF admissions in the treated groups (i.e., January and March admissions) relative to the control group (i.e., April admissions) showed no clear pre-trends from 2016 to 2018 (Figure 1, Supplemental eFigures 1 and 2). Event study estimates confirmed this conclusion (Supplemental eTable 1). From the pre-period to the post-period, the percentage of beneficiaries disenrolling from their MA plans changed from 5.5% to 5.7% for January admissions, 5.0% to 5.3% for March admissions, and 4.6% to 5.1% for April admissions (Table 2). As expected, given enrollment rules prior to the policy change, switches to TM were much more common than switches to another MA plan. For example, for beneficiaries with January admissions, only 0.22% exited to another MA plan in the pre-period, which increased to 0.52% in the post-period. In contrast, 5.3% and 5.2% exited the MA program to TM in the pre-and post-period, respectively.
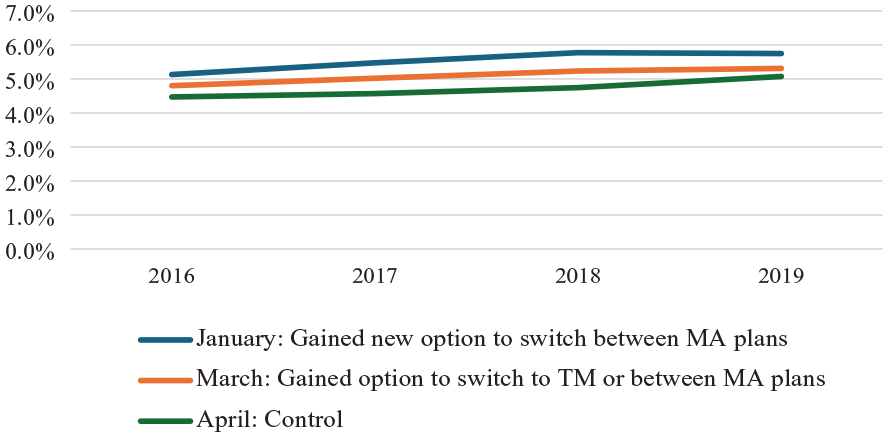
Unadjusted Rates of Plan Disenrollment by Month of Skilled Nursing Facility Admission, 2016–2019.
Changes in Medicare Enrollment After Extended MA Open Enrollment Period.
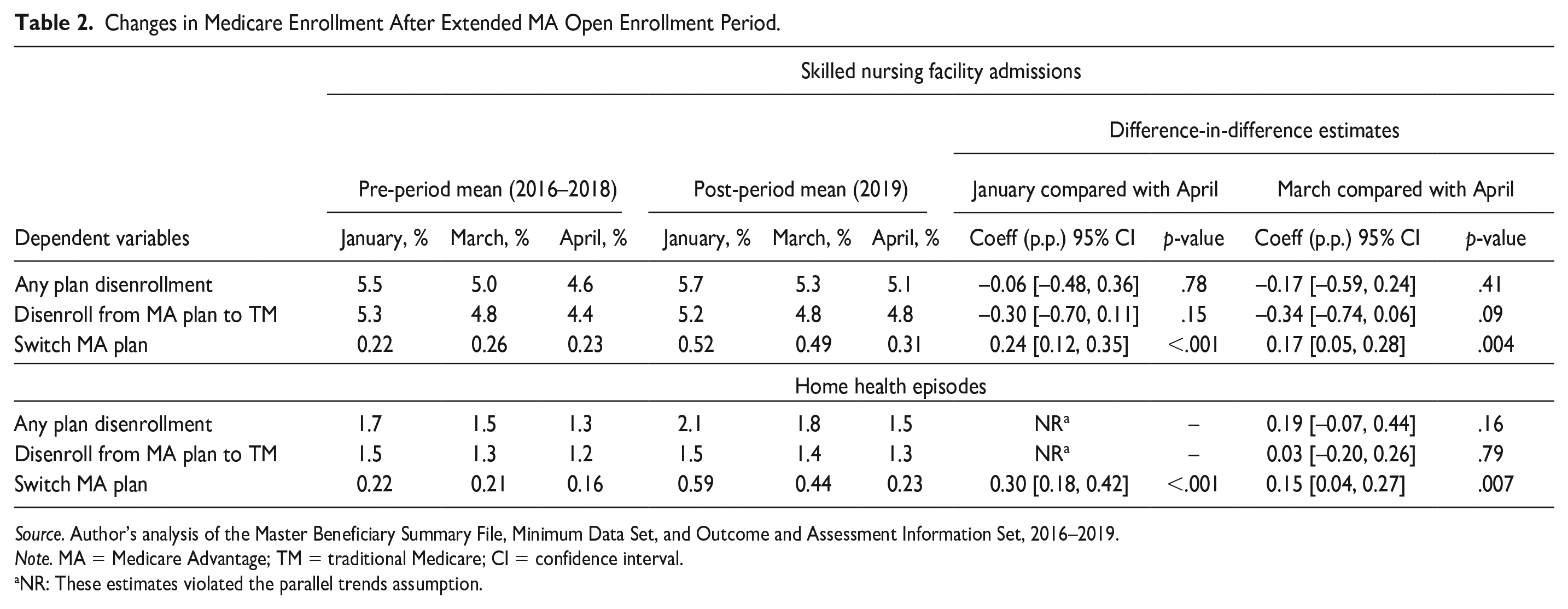
Source. Author’s analysis of the Master Beneficiary Summary File, Minimum Data Set, and Outcome and Assessment Information Set, 2016–2019.
Note. MA = Medicare Advantage; TM = traditional Medicare; CI = confidence interval.
NR: These estimates violated the parallel trends assumption.
When examining our DiD estimates, we observed no increased likelihood of any plan disenrollment with policy implementation (Table 2, DiD −0.06 percentage points; 95% confidence interval [CI]: [−0.48, 0.36]; p-value = .78), nor did we observe increased MA program exit (DiD −0.30 percentage points; 95% CI: [−0.70, 0.11]; p-value = .15). However, January admits were 0.24 percentage points (95% CI: [0.12, 0.35]; p-value <.001) more likely and March admits were 0.17 percentage points (95% CI: [0.05, 0.28]; p-value = .004) more likely to switch to a new MA plan relative to beneficiaries admitted in April in the post-period. These results represented a 109% and 65% relative increase from the pre-period in switching to another MA plan, respectively.
Home Health Users
When examining outcomes for beneficiaries with home health episodes (Table 2), beneficiaries with April episodes had the lowest pre-period disenrollment rates (1.3%), while those with January and March episodes had slightly higher rates, 1.7% and 1.5%, respectively. After the policy change, disenrollment increased the most for the group with January episodes (2.1%), while March episode switching rates increased to 1.8%. We did not report a formal DiD estimate for January disenrollment rates or switching to TM because trends in these outcomes varied by admission month and failed the parallel trend test in our event study estimates (Figure 2, Supplemental eTable 1). The DiD estimates for March home health users were statistically insignificant.
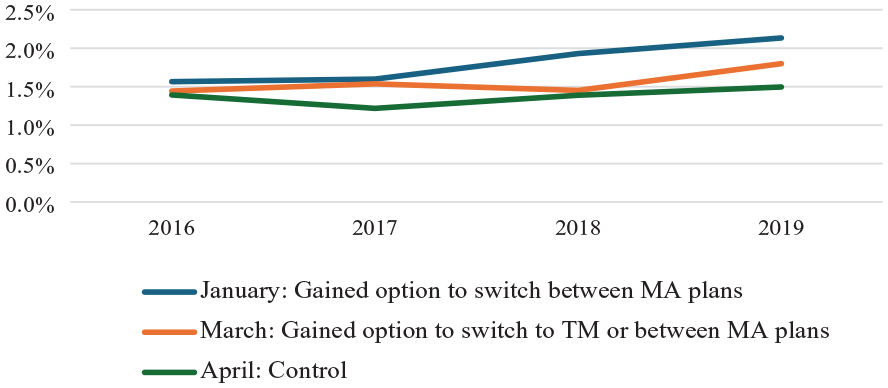
Unadjusted Rates of Plan Disenrollment by Month of Home Health Episode, 2016–2019.
Consistent with results for beneficiaries with SNF use, home health users rarely switched to a new MA plan, but this outcome did increase post-policy change. Rates of switching to a new plan increased from 0.22% in the pre-period to 0.59% in 2019 for beneficiaries admitted in January. Our DiD estimates showed that those with home health episodes in January were 0.30 percentage points (95% CI: [0.18, 0.42]; p-value < .001) more likely to switch their MA plan relative to beneficiaries with an April episode (136% relative increase from the pre-period) in the post-period, while patients with March home health episodes were 0.15 percentage points (95% CI: [0.04, 0.26]; p-value = .007) more likely to switch (a 71% relative increase from the pre-period; Table 2).
Sensitivity Analysis
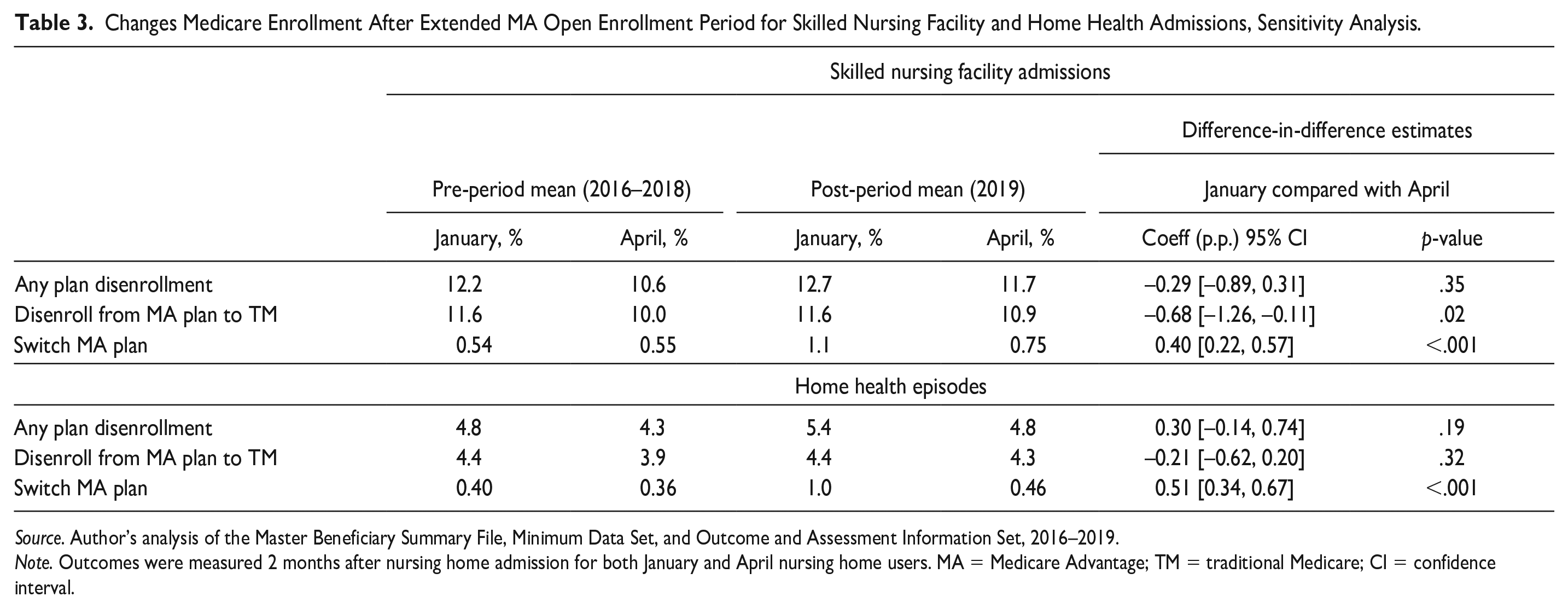
When analyzing whether beneficiaries changed enrollment within 2 months of initiating SNF use, we observed no clear pre-period trends in any of our outcomes (Supplemental eTable 1). From 2016 to 2018, January SNF users had a 12.2% rate of any change in enrollment, while April SNF admits had a 10.6% rate. In 2019, both groups experienced increased rates in plan disenrollment (12.7% for January admissions and 11.7% for April admissions; Table 3). Similarly, there were no pre-period trends in outcomes among home health episodes. There were low rates of plan disenrollment (4.8% among January episodes and 4.3% among April episodes; Table 3).
Changes Medicare Enrollment After Extended MA Open Enrollment Period for Skilled Nursing Facility and Home Health Admissions, Sensitivity Analysis.
Source. Author’s analysis of the Master Beneficiary Summary File, Minimum Data Set, and Outcome and Assessment Information Set, 2016–2019.
Note. Outcomes were measured 2 months after nursing home admission for both January and April nursing home users. MA = Medicare Advantage; TM = traditional Medicare; CI = confidence interval.
DiD estimates indicated no effect on overall plan disenrollment. However, when we disaggregated and examined the type of switch, we saw that the policy was associated with decreased rates of leaving MA to TM but increased rates on switching MA plans among SNF users. Specifically, January admits had a 0.68 percentage point (95% CI: [−1.26, −0.11]; p-value = .02) decrease in leaving the MA program but were 0.40 percentage points (95% CI: [0.22, 0.57]; p-value <.001) more likely to exit their MA plan for a new plan relative to those with April admissions in the post-period. Among home health users, there was no significant difference in MA program exit in January episodes relative to April episodes. However, there was a 0.51 percentage point (95% CI: [0.34, 0.67]; p-value <.001) increase in MA plan switch among January episodes relative to April episodes in the post period (Table 3).
Our analyses looking at outcomes 3 months post-admission or home health episode were similar (Supplemental eTable 2) to the other analyses although were unable to report results for January SNF admissions for two outcomes (any disenrollment and disenrollment from MA to TM) due to violations of the parallel trends assumption (Supplemental eTable 3).
Discussion
Our study examined the effect of a revised policy that gave beneficiaries additional time to redetermine their MA enrollment choice and a new option to change their MA plan as opposed to enrolling in TM. For beneficiaries using SNF or home health services, we found no evidence that the policy increased overall rates of disenrolling from their MA plans in the month after initiating post-acute care use. While beneficiaries did take advantage of the new option to remain in the MA program and select a different plan, this option was still relatively rare and elected by less than 1% of post-acute users. In our sensitivity analyses where we examined enrollment choices over a longer time window (2 months), we found that the policy was associated with decreases in rates of leaving MA to TM but increases in switching to a new MA plan for SNF users. These results suggest that individuals who would have been forced to enter TM if they left their MA plan may instead use this new option to remain in MA with a different plan.
Even in the midst of a post-acute episode, our results consistently demonstrated most beneficiaries in need of complex care remain in MA when given the option to leave. There are several possible explanations for these results. First, MA plans are popular in part because they are available with lower premiums than the most common alternative, TM with supplemental Medigap coverage. In all but eight states, Medicare beneficiaries with pre-existing conditions may be denied Medigap coverage or be required to pay higher premiums if they do not enroll in Medigap at age 65. Without a Medigap plan, MA enrollees switching to TM face 20% coinsurance for many services and have no limits on out-of-pocket costs. State-level policies that ensure guaranteed issue or community rating for Medigap policies are associated with lower rates of re-entering MA among individuals who left MA for TM (Meyers, Trivedi, et al., 2019). However, even with those protections, beneficiaries may have difficulty affording Medigap plans. Beneficiaries may also value benefits that are available in MA but not in TM, including supplemental benefits like dental and vision coverage. The new policy provides beneficiaries the option to remain in MA and select a plan with better benefits. Future work should investigate whether beneficiaries choose more generous plans in the midst of using post-acute care.
Second, our results could also be explained by how Medicare requires beneficiaries to navigate confusing and complex enrollment choices (Medicare Payment Advisory Commission, 2024; Ochieng et al., 2022; Rivera-Hernandez et al., 2021). Although Medicare’s open enrollment period is heavily advertised by MA insurers, many beneficiaries may not be aware that they can switch out of their plan prior to April 1. For beneficiaries who are in the midst of an episode that requires post-acute care use, it may be particularly difficult to navigate enrollment choices without significant assistance from family members or other advocates.
Third, CMS has taken other steps in recent years to improve post-acute benefits in MA plans, including setting maximum copayment amounts for these services (Keohane et al., 2015, 2018, 2021). Mandatory reductions in SNF copayments were associated with reductions in plan exit among SNF users (Keohane et al., 2021), suggesting that these types of regulations may encourage continued MA participation.
Overall, our study indicates that beneficiaries may face great burdens when choosing to change coverage whether that be limited options for supplemental coverage if they enroll in TM or the numerous choices, restrictive networks, or utilization management tools if they remain in MA. There are several possible financial and access barriers beneficiaries must weigh when determining Medicare coverage. Our modest findings may also support the fact that beneficiaries rarely redetermine their coverage options once they are made, even when there may be better options available (Heiss et al., 2021; Ochieng et al., 2024).
There were several limitations to our analysis. First, our results do not generalize to dual-eligible beneficiaries with Medicare and Medicaid, a population that is not locked into their plan choice and can switch insurance options throughout the calendar year, or other health care settings since we focus on beneficiaries who used post-acute care. Second, while we aim to increase the internal validity of our analysis by employing a DiD design, our estimates could be biased if there were other changes in Medicare enrollment rules that differentially affected those using PAC in January and March versus April. To our knowledge, no other policy changes occurred during this time. Third, we only have 1 year of post-period data, which could explain our small effect estimates. The impact of the policy may increase if beneficiaries become more aware of this option over time. These new options for MA enrollees may not have been adequately communicated to beneficiaries, which could also explain our modest estimates. Fourth, some outcomes were rare, especially among home health users, and it may be difficult to detect an effect even with our large sample size. Fifth, CMS has other special enrollment periods that allow beneficiaries to make redeterminations to their coverage in exceptional circumstances. If beneficiaries already rely on these protections to make coverage changes mid-year, then this new policy may have minimal additional impact. Finally, we cannot observe the exact timing within a month of a beneficiary’s decision to change their Medicare coverage. Some beneficiaries may have made this choice prior to initiating post-acute services. Our sensitivity analyses that look at enrollment choices over a longer time window provide greater assurance that the disenrollment choice was subsequent to post-acute care use. However, we are able to provide novel evidence that relaxing enrollment rules did not lead to immediate large exits from MA or exacerbate favorable selection within the MA program.
Conclusion
Our study found that the new policies that relaxed the deadline to exit an MA plan and gave beneficiaries the option of selecting a different MA plan did not have any effects on overall rates of plan disenrollment or exits from MA to TM among those using post-acute care. However, the policy was associated with a modest increase in the rate of switching to a new MA plan.
Supplemental Material
sj-docx-1-mcr-10.1177_10775587241313092 – Supplemental material for The Effect of Extending the Window to Disenroll From Medicare Advantage Among Post-Acute Users
Supplemental material, sj-docx-1-mcr-10.1177_10775587241313092 for The Effect of Extending the Window to Disenroll From Medicare Advantage Among Post-Acute Users by Emma M. Achola, Amal N. Trivedi, Daeho Kim, David J. Meyers, Hiren Varma and Laura M. Keohane in Medical Care Research and Review
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Ms. Achola, Dr. Keohane, Dr. Kim, Dr. Trivedi, and Mr. Varma report no conflicts of interest. Dr. Meyers serves as a senior advisor to the Center for Medicare and Medicaid Innovation on Medicare Advantage on a part-time basis. CMMI had no role in this manuscript and this work does not reflect any official views of CMS.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the NIH grant 2P01AG027296-11.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.