
Abstract
This study evaluated the impact of an interdisciplinary care teams (IDCT) care management program on cost and quality outcomes using a novel algorithm to identify 400 high-risk patients out of 48,235 Medicare Advantage (MA) beneficiaries. Of the 400, 252 were enrolled in the IDCT care management intervention program, while the remaining 148 were not enrolled. A second comparison group consisted of 660 who were referred to the IDCT program but not selected by the algorithm. The program’s effectiveness was evaluated 1-year postintervention. Analyses found that health care costs for members enrolled in the IDCT program were reduced by US$1,121.76 and US$1,625.61 per member per month, respectively, relative to those not enrolled and those enrolled by referral. The cost reduction from the program generated a net savings of US$1.9MM, covering the program’s cost. Findings suggest IDCTs can cost-effectively manage populations of high-risk patients with better selection and fostering greater interdependence.
Keywords
Introduction
It is well known that a relatively small percentage of patients are responsible for a large portion of the fast-growing cost of medical care (Allen et al., 2000; Johnson et al., 2015; Riley, 2007). Payers and providers struggling to manage the rising costs of care have intervened with a variety of strategies targeting complex, high-needs patients in the hope that these efforts will prevent costly and preventable utilization. A variety of programs have been employed in this respect, including medical homes, disease and case management programs, transitional care programs, and others (Price-Haywood et al., 2018; Quinton et al., 2021). Similarly, these programs have employed a variety of strategies for identifying patients for program inclusion, ranging from selection based on provider referral to selection using complex data-driven algorithms (Hong et al., 2014). While some of these programs have shown improvements in the quality of care, few have successfully reduced the costs of care for their target population (McCarthy et al., 2015; Peikes et al., 2009).
One potential reason why care management programs have not demonstrated cost-effective improvements in quality is suboptimal enrollee selection. That is, despite the robust services provided, they may have been targeted at individuals who were not as likely to be impacted by them. The purpose of this study was to evaluate the financial and quality outcomes of a unique health insurance company’s program that combined an interdisciplinary care team (IDCT) approach to providing comprehensive services to enrollees and a data-driven predictive algorithm to select enrollees into the program.
New Contributions
Research has found that IDCT care management programs can improve quality (Coleman et al., 2006; Litaker et al., 2003; Rothman et al., 2005; Willens et al., 2011). For example, Litaker et al. (2003) found IDCTs improved A1C levels in diabetics, while Laurant et al. (2005) found that IDCTs deliver better preventive care, provide more health advice, and achieve higher patient satisfaction than solo practitioners (Laurant et al., 2005). Despite these potential advantages of IDCTs, they can be difficult for a health plan to implement due to limited resources, costs of recruiting and employing a diverse range of team members, and limitations in the number of members that an IDCT can manage. Consequently, current research has primarily shown that IDCTs can improve quality, with few studies showing a corresponding cost reduction. We submit that one reason for this pattern is that care management programs using IDCTs have ineffectively identified enrollees who may benefit the most from their comprehensive approach to managing health. This study addresses this potential disconnect by examining the quality and financial outcomes of a program that combined IDCT concepts with a claims data-based predictive algorithm to select complex, high-need enrollees. Moreover, our study extends beyond previous research to directly assess the return on investment of implementing the program.
The findings of the study are important for organizations that may be considering developing or adopting these programs and stakeholders who are interested in supporting their use. Likewise, patients may benefit from the findings through a better understanding of what care management programs are more effective.
Background
Program Context
The study was conducted using data from a large health insurer located in the Southeastern United States. The health plan has approximately 105,000 members distributed across multiple insurance products, including HMO, TPA (Self-Funded), and Medicare Advantage (MA). The investigative team included F. Cardwell Feagin, Jr., DSc, Larry R. Hearld, PhD, Nathan W. Carroll, PhD, Stephen O’Connor, PhD, and Bisakha Sen, PhD. The IDCT care management program that is the focus of this analysis concentrates on MA enrollees.
IDCTs
Interdisciplinary care teams (IDCTs) can be defined as a group of health care professionals that come together to leverage the knowledge and skills of diverse professionals with the patient at the center (Baldwin, 2007). IDCTs were originally developed in community health centers in the 1940s as part of President Johnson’s vision for the Great Society (Baldwin, 2007), and more recently, health plans have begun to implement IDCT concepts into their case and care management programs to manage the health of their patient populations (Bielaszka-DuVernay, 2011; Hong et al., 2014; Peikes et al., 2012). The IDCT care management program being evaluated in this study was started in 2010 and, at the time of this study, consisted of a team of care navigators, community health workers, care coordinators, care managers, pharmacists, behavioral health clinicians, internists, and psychiatrists, geriatricians, social workers, nurses, and medical directors. The health plan also had the option to call on any specialty physician affiliated with the partner university medical center. Each team member was expected to play unique yet complementary roles for members enrolled in these care management programs. The registered nurse, for example, may handle transitions of care from an inpatient facility to home or other locations like a skilled nursing facility. Once the member is home, a social worker may assist the member in finding needed community resources. A pharmacist, in turn, may perform medication reconciliation for members to ensure that changes in a member’s prescriptions and/or dosages made during an inpatient stay are reflected in the member’s prescriptions when discharged from the hospital. Despite these unique roles, there was an expectation that the team would meet on a scheduled monthly meeting and as needed to discuss enrollees’ goals and care needs and communicate with each other between meetings to revise care plans as necessary.
IDCT Care Management Program Member Selection Process
The health plan uses a data-driven approach (“algorithm”) to identify members who are at greater risk of hospitalization and, thus, may be more likely to be affected by the program. Specifically, the algorithm uses historical claims and enrollment data to model: (a) the absolute risk of hospitalization and (b) recent (since the previous year) changes in the risk of hospitalization. Based on a member’s likelihood of hospitalization, she or he is invited to participate in the IDCT care management program. This research is novel because, to date, no research could be found on combining an algorithm with an IDCT. The algorithm enables the IDCT to be used to its optimal capacity. We submit that this data-driven approach is able to more consistently and comprehensively take into consideration pertinent information to reach conclusions about a member’s suitability for the IDCT program. That is, by focusing on members with the greatest risk of hospitalization, the IDCT care management program can provide early and sustained support for members who may benefit the most.
Members are selected for participation in the IDCT care management program in one of two primary ways: (a) data-driven algorithm or (b) by referral. The data-driven selection algorithm of members begins with the application of a predictive analytic. The predictive analytic estimates a likelihood of hospitalization (LOH) score using a multivariable logistic regression model with age, gender, medical diagnoses, outpatient pharmacy usage, and other health care utilization metrics common to claims data as covariates to estimate the likelihood a particular person will experience a hospitalization within the next six months. Members are then ranked based on their LOH score. Members with a LOH score of 0.18 or higher and a current LOH that is 58% higher than their previous LOH six months ago are selected for further consideration. Next, the algorithm uses real-time claims data to eliminate claims lag and to identify and select members who experienced three or four ED visits in the last 6 months. Members with more than four ED visits are eliminated from further consideration because they are considered overly complex and not suitable for the program.
Theoretical Framework
We adopted two complementary theoretical perspectives to examine the impact of IDCTs on cost and quality outcomes. Team interdependence helped us consider why an IDCT may be more effective than more individualized efforts at understanding and meeting enrollee care needs (Courtright et al., 2015). Social cognitive theory, in turn, helps explain why enrollees engage with the program and may be more likely to respond to IDCT efforts to foster healthy behaviors.
IDCT Interdependence
A critical factor in team design and effectiveness is structural interdependence (LePine et al., 2008; Wageman & Gordon, 2005). Structural interdependence refers to the features of the team that define the interconnectedness of the team or the degree to which team members must work together to accomplish its goals. Such features include task-related inputs such as resources, workflows, and reward systems that can be controlled by team leaders and members (Wageman & Gordon, 2005). Teams may function with low structural interdependence, where tasks are completed on a more individualized basis with a pooled product, or with high structural interdependence, where members work simultaneously on tasks. Structural interdependence can be further broken down into two subtypes. Structural task interdependence refers to how much team members depend on each other to coordinate work tasks (Courtright et al., 2015; Wageman & Gordon, 2005). Outcome interdependence relates to how much the outcomes of the taskwork are measured, rewarded, and communicated at the team level to emphasize collective outputs rather than individual contributions (Courtright et al., 2015; Wageman & Gordon, 2005).
We submit that, due to their focus on a shared cohort of members enrolled in a program with clearly defined parameters (e.g., program duration, types of services offered), IDCTs are higher in their structural interdependence—both task and outcome—than more traditional teams or individualized efforts to provide services to enrollees. Moreover, consistent with Courtright et al. (2015), higher levels of structural interdependence will be associated with better quality and lower costs. This is because higher levels of structural interdependence will foster greater behavioral interdependence—that is, interaction and familiarity between team members (Bolton et al., 2021), which is associated with higher levels of information sharing, coordination, and joint decision-making regarding patient care needs (Gruenfeld et al., 1996; Okhuysen, 2001; Rockett & Okhuysen, 2002). Likewise, through closer, more repeated interactions, structural interdependence can help team members learn about the capabilities of other team members and, in doing so, foster greater confidence in the team’s capacity to complete important tasks (Rockett & Okhuysen, 2002).
Social Cognitive Theory
An interdependent IDCT is likely insufficient by itself to improve cost and quality outcomes. The members/enrollees of a program using IDCT principles must also be motivated to make changes based on the efforts of the IDCT team. Social Cognitive Theory helps explain why members/enrollees may be more responsive to IDCT efforts. Social Cognitive Theory consists of three interacting factors: behavior, cognition, and the external environment (Bandura, 1995). Individuals are both products of their environment and influence their environment in a process called reciprocal determinism (Bandura, 1995). The theory examines how people can take control of their own lives and, in the context of this study, how they take control of their health. People’s self-beliefs of efficacy enhance or impair their motivation to perform and, in doing so, are critical determinants of how well people seek out and acquire new skills and abilities (Bandura, 2011).
Social Cognitive Theory states that people can develop three different modes of agency: direct agency, proxy agency, and collective agency (Bandura, 2001). All three modes are applicable to IDCT care management member engagement. The direct agency is taking control of and achieving goals in an independent fashion (Bandura, 2001). IDCT programs foster direct agency by setting customized goals and educating members about the most effective ways to achieve these goals. Proxy agency refers to the ability to influence others who have access to resources to act on their behalf (Bandura, 2001). IDCT care management programs educate members and raise awareness of resources available to them, enabling members to better utilize these resources. For example, a care manager can act as a proxy for members with providers. Likewise, a social worker has access to resources in the community to help members. Collective agency refers to socially coordinated and interdependent efforts to achieve goals (Bandura, 2001), such as the IDCT working on a member’s behalf to achieve health goals.
IDCT care management programs may be effective at improving cost and quality outcomes because they foster all three modes of agency, thereby creating greater levels of self-efficacy among members and supporting members’ efforts to seek out the right resources in a timely manner, which in turn can reduce the need for unnecessary health services and their associated costs. For example, IDCT care management enrollees are taught subtle changes in symptoms can indicate exacerbation of a condition, and escalation to their treatment team is often appropriate. While there will always be those admissions and illnesses that cannot be avoided, an effective IDCT team can improve enrollees’ confidence and capacity to access the right level of care at the right time.
In sum, based on these complementary theoretical perspectives, we hypothesized that:
Assuming the IDCT care management program can reduce utilization enough, it will generate enough cost savings to cover the cost of the program. Thus, it is hypothesized that:
Opportunities for an IDCT to be most impactful are likely not uniform across a population of enrollees. Variability in underlying health conditions, social determinants of health, and interest in engaging in shared medical decision-making (Cockerham et al., 2017; Robinson & Thomson, 2001) suggests that some patients may be better suited for care management programs). Historically, many care management programs have relied on provider or self-referral to identify enrollees, which may be problematic, particularly for primary care providers and/or for some conditions (Horwitz et al., 2015). This is due to referrals requiring accurate identification of conditions that warrant care management, awareness of the availability of a care management program, and timely referral to a program. The availability of “Big Data” and its associated applications, such as the algorithm considered in our study, may provide a more effective means of identifying suitable enrollees for these programs. Algorithms use a more objective, proactive, and arguably more comprehensive (i.e., historical claims data across the continuum of care) approach. In comparison, for members who are referred by providers, the program must rely on the provider’s judgment of members’ needs and potential responsiveness. Therefore, we hypothesize that:
Method
Sample Selection
There were 400 members selected (from 48,235 MA beneficiaries) by this algorithm for the IDCT care management program in 2018, the intervention year for this study. However, due to a lack of IDCT resources available to manage these members, only 252 members were enrolled in the IDCT care management program, while the remaining 148 members were not enrolled due to unavailable employee resources or the member declined enrollment. For this study to be included in the IDCT care management group, members must also have been enrolled and completed the program in the intervention year (2018). The 248 members selected by the algorithm and then enrolled in IDCT are our treatment group of interest (hereafter “algorithm-selected IDCT care management group.”). The 148 members selected by the algorithm but not enrolled in IDCT due to resource constraints are hereafter “comparison-group 1.” Finally, an additional 660 members who were in the IDCT care management program but were not selected by the algorithm and instead referred to the program by a health care provider or the IDCT or a self-referral constitute “comparison-group 2.” Members may refuse admission into the IDCT care management program. Figure 1 illustrates the IDCT Care Management Program Selection Process.
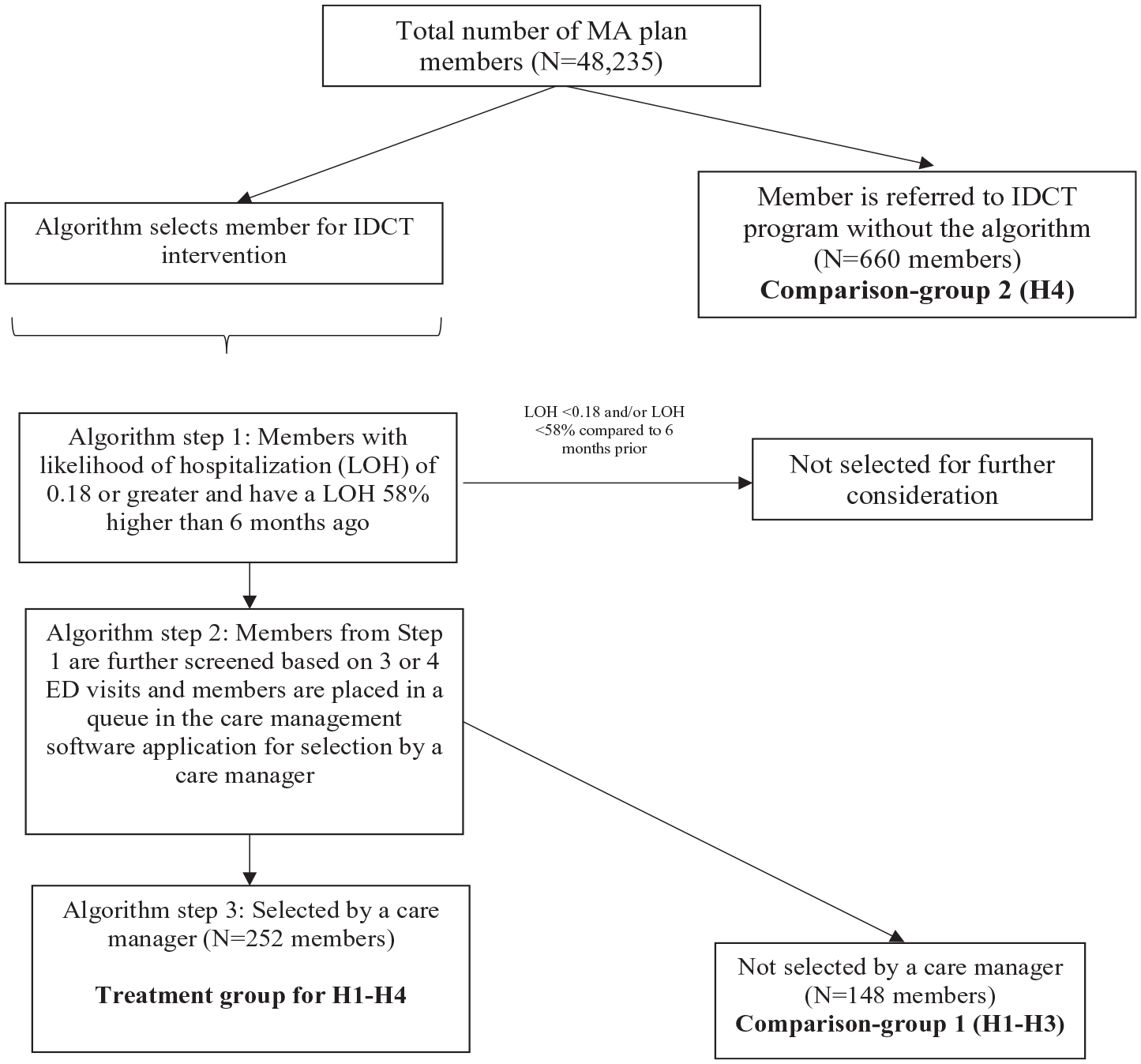
IDCT Care Management Program Selection Process.
A quasi-experimental, difference-in-differences approach was used to evaluate the effect of the program on inpatient utilization and cost outcomes. This method is particularly applicable when allocation to treatment and comparison groups does not happen via strict randomization. Dimick and Ryan (2014) found that employing the differences-in-differences approach addresses other time-dependent factors or trends unrelated to the IDCT care management intervention. The study design addresses this concern by comparing the intervention group to a control group. The quasi-experimental difference-in-differences approach was used to compare members in the different treatment conditions (i.e., IDCT care management program participants vs. nonparticipants) and test our study hypotheses. Given our goal of not only assessing the effectiveness of the IDCT care management program but also the member selection algorithm, our analytic strategy entailed two different comparison groups and, thus, two different sets of analytic models. One set compared pre-to-post changes in the dependent variables between IDCT care management program participants and nonparticipants. The purpose of this set of models was to evaluate the effectiveness of the IDCT care management program. A second set of models compared pre-to-post changes in the dependent variables between IDCT care management program participants selected by the data-driven algorithm and IDCT care management program participants not selected by the algorithm. The purpose of this second set of models was to assess the effectiveness of the member selection algorithm. Estimates of cost savings were then compared to program costs to calculate the return on investment.
Within each of these two sets of models, we estimated two regression models corresponding with the two dependent variables. The distribution of inpatient hospital admissions was discrete and did not form a normal distribution. Therefore, a negative binomial regression was employed to examine inpatient admissions (Hypotheses 1 and 4). We also estimated the marginal effects (i.e., predicted probabilities) to facilitate a more intuitive interpretation of these relationships. Ordinary least squares regression models were employed to evaluate health care costs (Hypotheses 2, 3, and 4).
Data Sources
Claims data for MA beneficiaries were used in the analysis. The study used claims data for members 1 year prior to enrollment in the IDCT care management program (2017) and 1 year after completing the IDCT care management program (2019). Professional and facility claim data were obtained from the MA plan medical claims adjudication system. Pharmacy claims were collected from the pharmacy claims adjudication system. Claims in the comparison group were reviewed for the same period of time.
Dependent Variables
The evaluation included three dependent variables: (a) Inpatient utilization; (b) Cost; and (c) Return on investment. Inpatient utilization was measured as the number of inpatient admissions in a calendar year. The cost was calculated as the total medical, behavioral, and pharmacy claims cost per year. Return on investment was estimated by subtracting the direct cost of employing the IDCT staff from the savings generated by the IDCT program (i.e., the estimated cost difference between the algorithm-selected IDCT care management group and non-IDCT care management group from our multivariable regression models). The direct cost of the interdisciplinary care management team was based on the salaries plus benefits of the employees and other direct costs. All three dependent variables encompassed 1 year pre-enrollment and postenrollment in the IDCT program.
Independent Variable
For Hypotheses 1 to 3, the independent variable of interest was the IDCT care management program (1 = member enrolled in IDCT program; 0 = member not enrolled in IDCT program). For the fourth hypothesis, the independent variable of interest was the use/selection by the data-driven algorithm (1 = member selected by the algorithm; 0 = member selected by provider referral, not by the algorithm). For member enrollees selected by the algorithm, those member enrollees were then selected randomly by the IDCT into the program.
Control Variables
The study controlled for member gender, age, socioeconomic status (a proxy dichotomous variable was created to reflect two benefit plans associated with socioeconomic status: 0 = Regular plan and 1 = Dual Medicare-Medicaid Plan), and health status using the Centers for Medicare and Medicaid Services (CMS) risk code. The inclusion of these control variables was informed by previous literature showing differences in cost and utilization based on these characteristics (Arredondo & Aviles, 2015; Economou et al., 2008; McPhail, 2016).
Analytic Strategy
Univariate analyses were used to describe the study sample and compare the different groups. Bivariate analyses were used to compare the study groups in the pre-IDCT care management program period. For the continuous variables, independent t-tests were used to test for differences between the groups in the pre-IDCT care program period. Likewise, for categorical variables, chi-square tests of association were used to test for differences between the IDCT care management and comparison groups in the preintervention period.
The study received ethical approval from the University of Alabama at Birmingham’s Institutional Review Board (Protocol #: 300006488). The investigative team included three health services researchers (Larry R. Hearld, PhD, Nathan W. Carroll, PhD, Stephen O’Connor, PhD, and Bisakha Sen, PhD) and an employee from the health plan (F. Cardwell Feagin, Jr., DSc.).
Results
Sample Descriptives
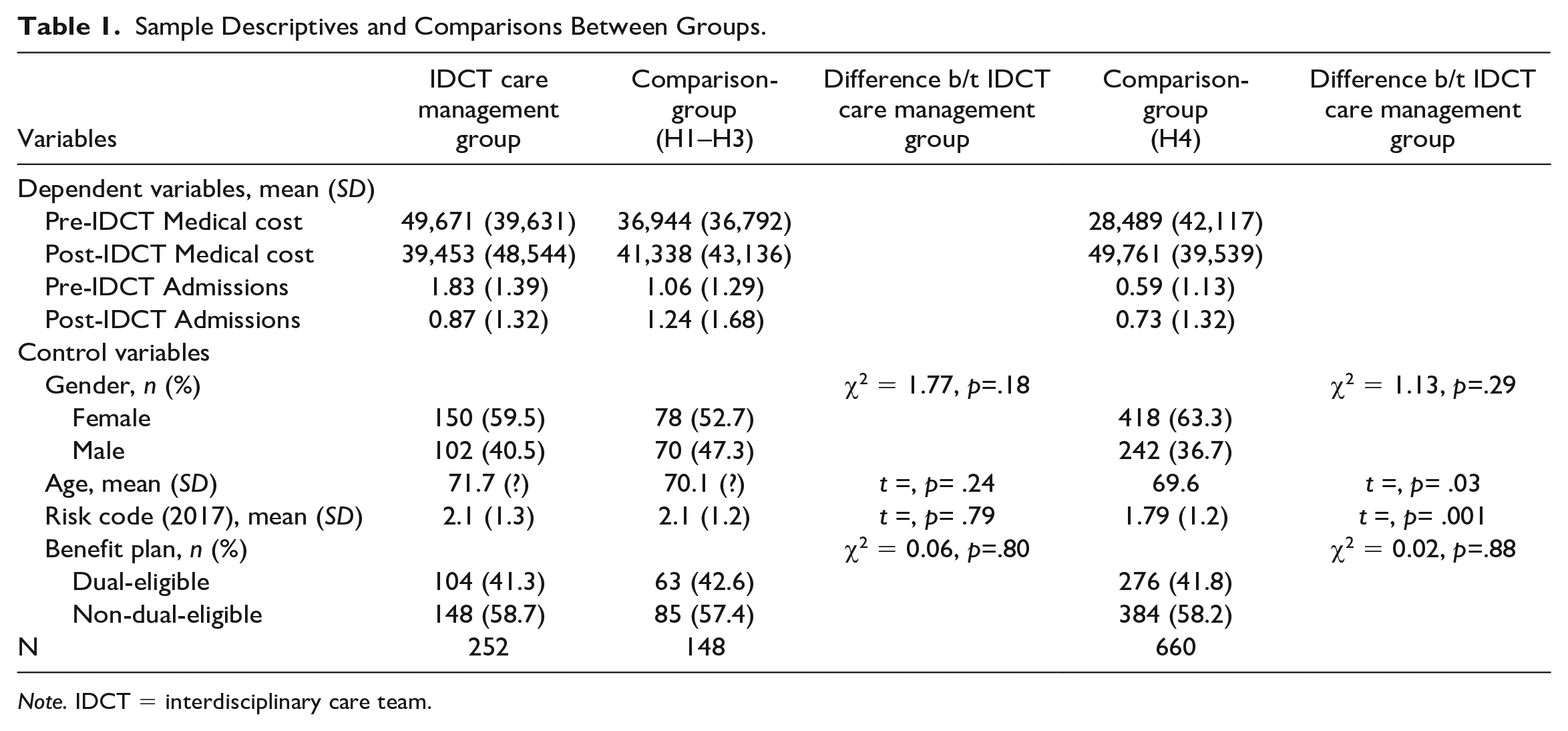
Table 1 illustrates the study variables and descriptive statistics. There were 252 members in the algorithm-selected IDCT care management group, 148 members in comparison-group 1 (Hypotheses 1–3), and 660 members in comparison-group 2 (Hypothesis 4). The number of admissions for the algorithm-selected IDCT care management group decreased by an average of 0.96 admissions per member from 2017 to 2019, a 52% decrease. The number of admissions for comparison-groups 1 and 2 increased by an average of 0.18 (17%) and 0.14 (24%) admissions per member from 2017 to 2019, respectively. The medical cost for the algorithm-selected IDCT care management group decreased by an average of $10,218 per member from 2017 to 2019, a 21% decrease in medical cost. Medical costs for comparison-group 1 increased by an average of $4,394 per member, a 12% increase. Medical costs also increased for comparison-group 2 by $21,272 per member per year, on average, or approximately 75 percent.
Sample Descriptives and Comparisons Between Groups.
Note. IDCT = interdisciplinary care team.
Baseline Comparisons of Study Group Characteristics
There were no significant differences between the algorithm-selected IDCT care management group and comparison-group 1 in the baseline period with respect to age, gender, risk code, and benefit plan (dual-eligible status; Table 1). When comparing comparison-group 2 to the algorithm-selected IDCT care management group in the baseline period, there were no significant differences in gender and benefit plan. However, there was a significant difference in age and risk code between the algorithm-selected IDCT care management group and comparison-group 2. Consequently, we included these and the other member characteristics in multivariable regression models when estimating the differences between groups.
IDCT Care Management—Inpatient Hospital Admissions Regression Results
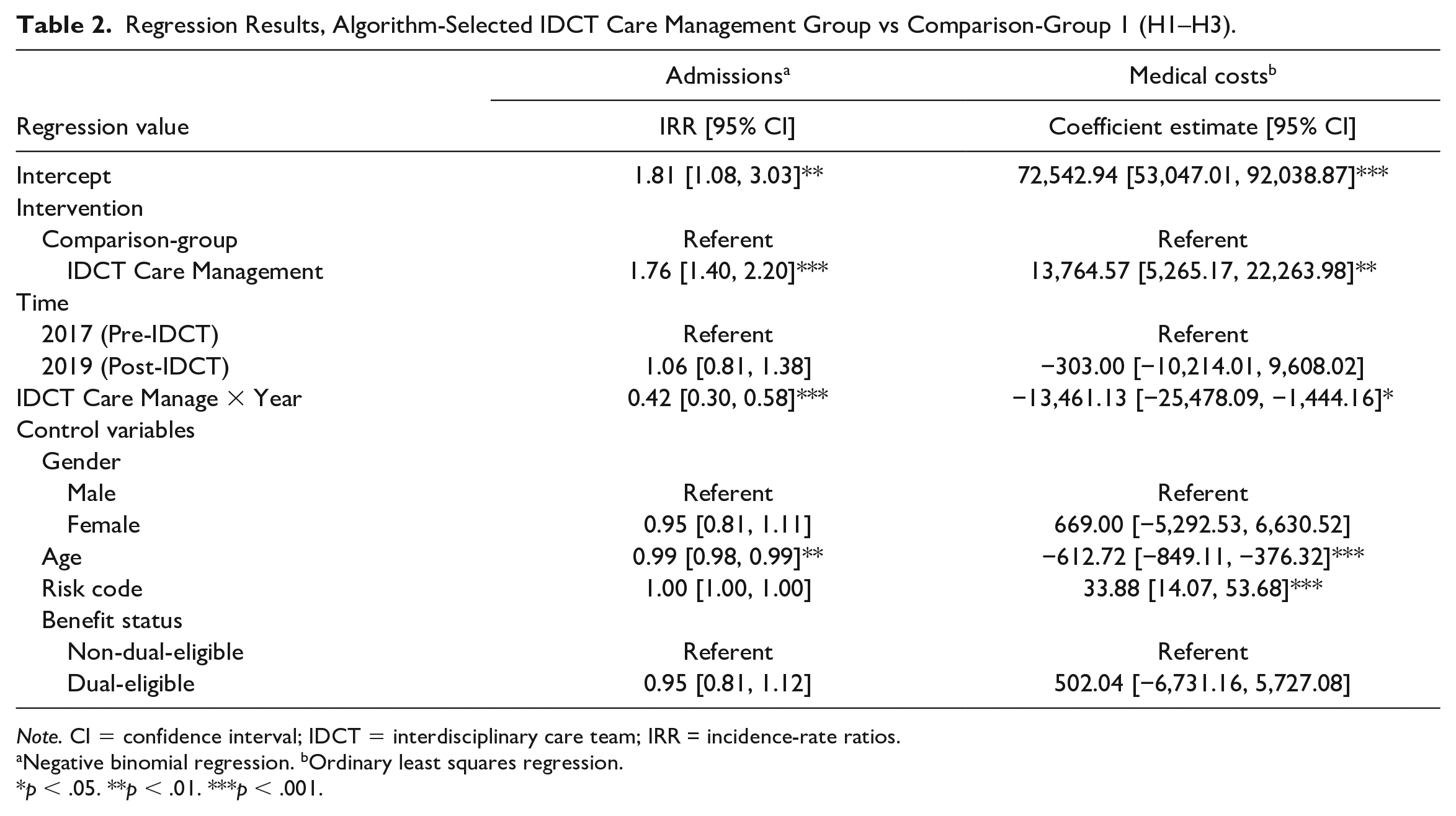
Relative to comparison-group 1, members in the algorithm-selected IDCT care management group experienced a 0.42 greater decline in admissions, on average, between the preintervention and postintervention periods (incidence-rate ratios [IRR] = 0.42, 95% confidence interval [CI] = [0.30, 0.58]; Table 2). Estimates of the marginal effects show that adjusted for other model covariates, non-IDCT members in comparison-group 1 had 1.10 admissions, on average, in 2017, which increased by 5% to 1.16, on average, in 2019 (Table 4). In comparison, members of the algorithm-selected IDCT care management group had 1.93 admissions on average in 2017, which decreased by 56% to 0.85 admissions, on average, in 2019. In sum, these results provide support for hypothesis 1.
Regression Results, Algorithm-Selected IDCT Care Management Group vs Comparison-Group 1 (H1–H3).
Note. CI = confidence interval; IDCT = interdisciplinary care team; IRR = incidence-rate ratios.
Negative binomial regression. bOrdinary least squares regression.
p < .05. **p < .01. ***p < .001.
IDCT Care Management—Medical Costs Regression Results
Relative to comparison-group 1, members in the algorithm-selected IDCT care management group experienced a $13,461.13 decline in their medical costs, on average, between the preintervention and postintervention period (p = .028; Table 2). Adjusted for other model covariates, non-IDCT members in the comparison group had $38,276.71 in medical costs, on average, in 2017, which decreased by 0.8% to $37,973.71 in medical costs, on average, in 2019 (Table 4). In comparison, the enrolled members of the algorithm-selected IDCT care management group had $52,041.28 in medical costs on average in 2017, which decreased by 26% to $38,277.16 in medical costs, on average, in 2019. These results provide support for Hypothesis 2.
IDCT Care Management Program With an Algorithm—Inpatient Hospital Admissions Regression Results
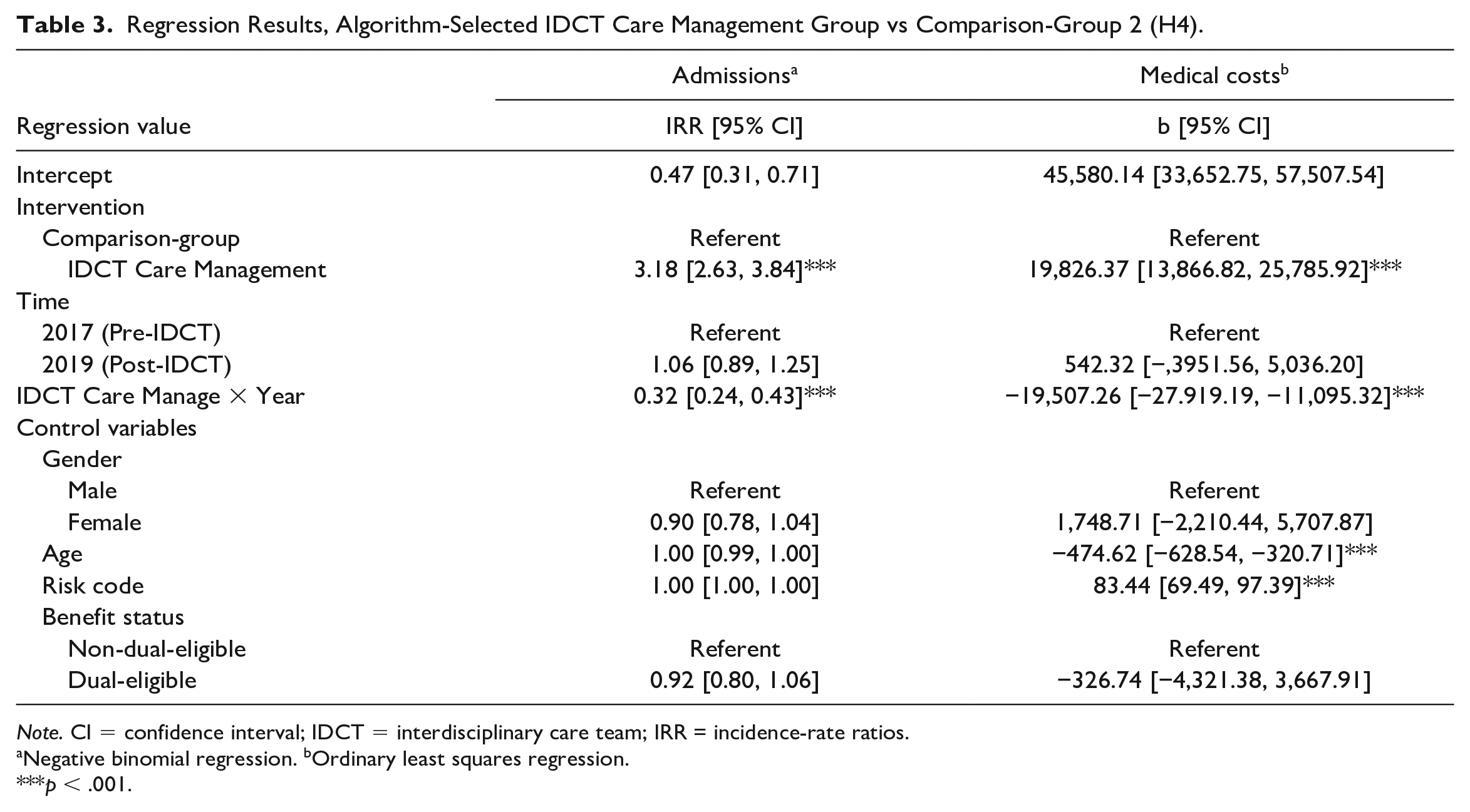
Relative to IDCT members not selected by the algorithm (comparison-group 2), members in the algorithm-selected IDCT care management group experienced a 0.32 greater decline in admissions, on average, between the preprogram and the postprogram periods (IRR = 0.32, 95% CI = [0.24, 0.43]; Table 3). Adjusted for other model covariates, IDCT members not selected by the algorithm had 0.65 admissions, on average, in 2017, which increased by 6 percent to 0.69, on average, in 2019 (Table 4). In comparison, algorithm-selected IDCT care management group members had 2.09 admissions on average in 2017, which decreased by 66% to 0.71 admissions on average in 2019.
Regression Results, Algorithm-Selected IDCT Care Management Group vs Comparison-Group 2 (H4).
Note. CI = confidence interval; IDCT = interdisciplinary care team; IRR = incidence-rate ratios.
Negative binomial regression. bOrdinary least squares regression.
p < .001.
Pre and Post Predicted Values of Dependent Variables by Group.
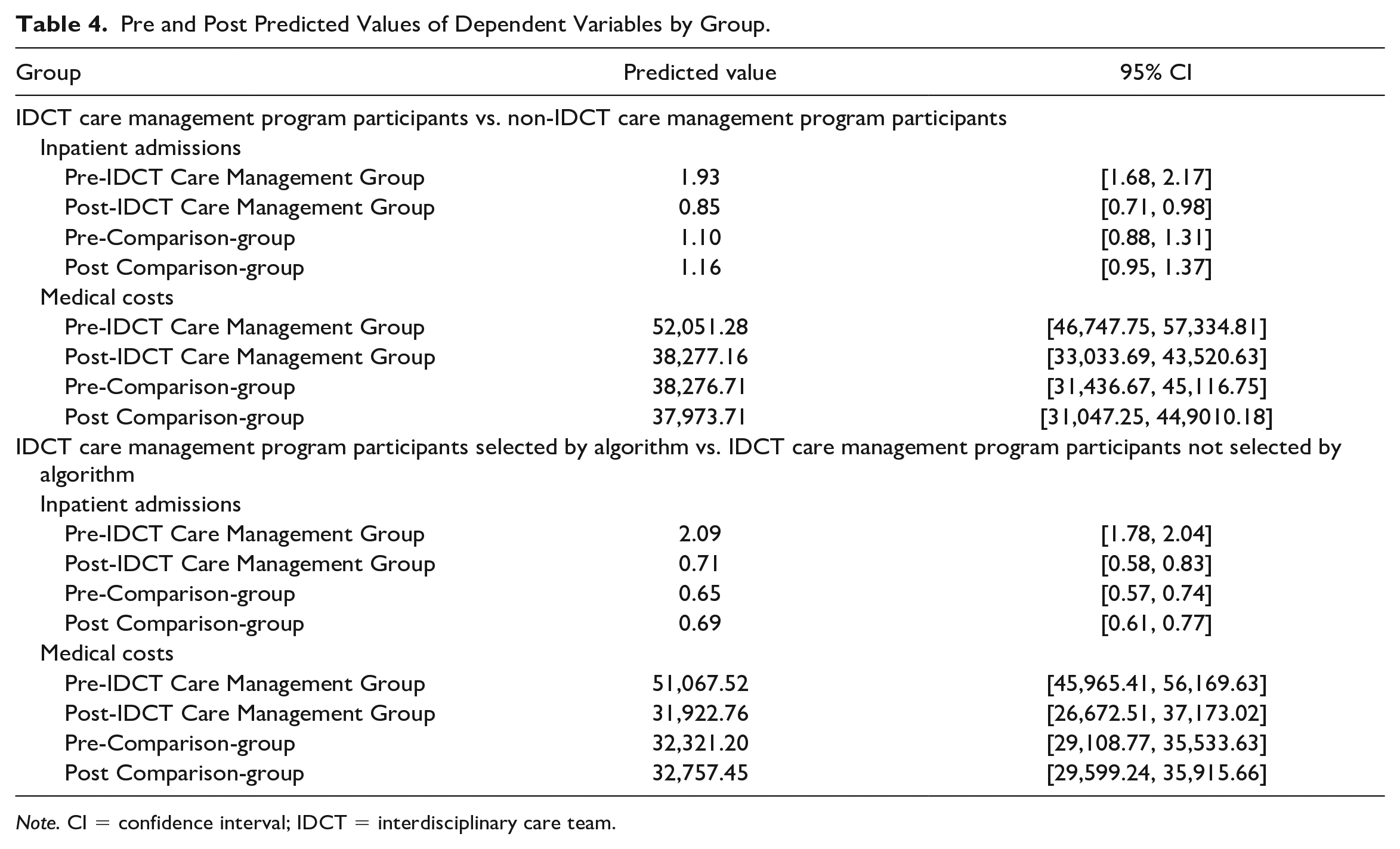
Note. CI = confidence interval; IDCT = interdisciplinary care team.
IDCT Care Management Program With an Algorithm—Medical Costs Regression Results
Relative to IDCT members not selected by the algorithm (comparison-group 2), members in the algorithm-selected IDCT care management group experienced a US$19,507.26 decline in their medical costs, on average, between the preintervention and postintervention period (p < .001; Table 3). Collectively, these findings provide support for hypothesis 4.
Return on Investment
To calculate the return on investment, the US$13,461.13 decrease in medical costs from the linear regression analysis was multiplied by the 252 members in the algorithm-selected IDCT care management group, which resulted in an estimated savings of US$3,392,204.76 for the IDCT care management program (Table 5). This estimate was then subtracted from the IDCT direct cost, which included salaries, benefits, and all other direct costs, such as the cost of the algorithm software and mileage. The IDCT is a subdepartment of the Health Services Department. The nonsalary direct cost for this IDCT care management subdepartment was calculated from the percentage of the direct cost of salaries for the Health Services Department, with the exception of mileage. The IDCT care management subdepartment has a disproportionate share of mileage because the team is field-based and travels to members of the community. Therefore, the entire mileage expense of the whole department was attributed to the IDCT care management subdepartment, which presents a more conservative estimate of the return on investment. The IDCT program’s total direct cost was US$1,532,816.07. Thus, the IDCT program’s annual return on investment was estimated to be US$1,859,388.69, or US$614.88 per member per month, which provides support for Hypothesis 3.
IDCT Care Management Program Savings and Return on Investment.
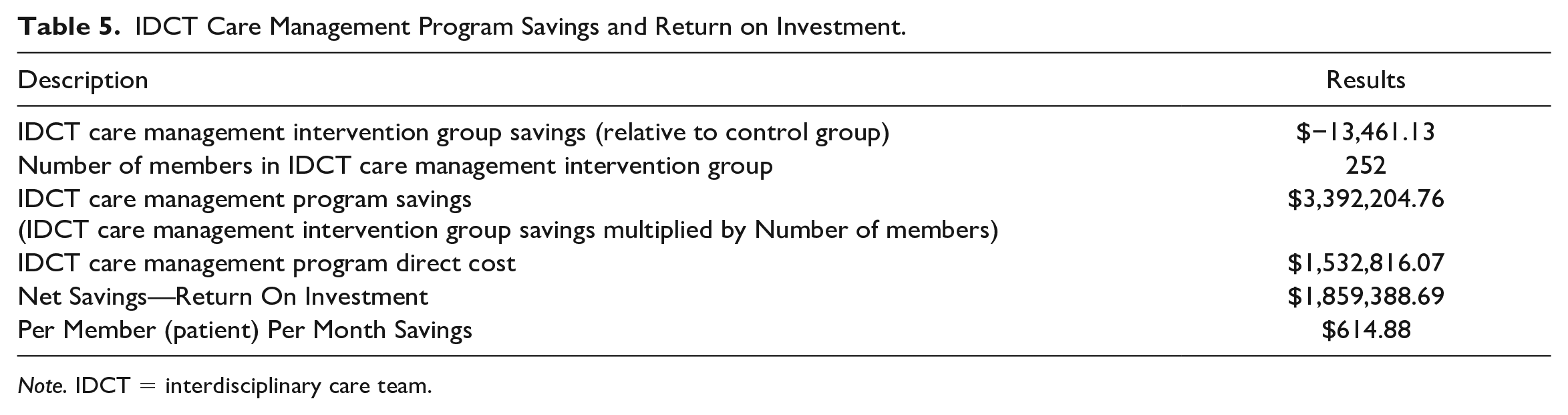
Note. IDCT = interdisciplinary care team.
Discussion
The purpose of this paper was to present the findings of our evaluation of an IDCT care management program using an algorithm to select members to be enrolled in the program. Our analysis found that participants selected by the algorithm and enrolled in the IDCT care management program compared to a control group also selected by the algorithm but not enrolled in the IDCT care management program showed a reduction in inpatient admissions and a reduction in health care costs. Importantly, the cost reductions generated enough savings to cover the program’s cost. Moreover, the analysis revealed that one of the key components of the program was the use of a data-driven member selection algorithm.
One explanation for the effectiveness of the overall program is that by creating more expectations and opportunities for interdependence, the IDCT is more effective than traditional, individualistic approaches at coordinating activities and promoting perceived and actual self-efficacy and agency. According to Social Cognitive Theory, people’s beliefs of self-efficacy can enhance or impair their motivation to perform, and self-efficacy beliefs are critical determinants of how well people seek out and acquire new skills and abilities (Bandura, 2011). IDCT programs set customized goals and educate members about the most effective ways to achieve these goals. They also raise awareness of resources available to members and enable members to take advantage of these resources. In sum, by helping participants take control of their situation, IDCT can help them become an agent of change in their own health and health care (Bandura, 2011). Our findings are consistent with other studies that have shown improvement in quality by IDCTs (Coleman et al., 2006; Litaker et al., 2003; McLendon et al., 2019; Rothman et al., 2005; Willens et al., 2011).
In contrast to the studies of the effects of IDCTs on utilization and quality, few other studies have found IDCTs can reduce cost. For example, only one of the 15 care management programs in a study by Peikes et al. (2009) found a reduction in cost. Moreover, for studies that have found cost reductions, the reduction was small and did not cover the cost of the program (Bielaszka-DuVernay, 2011; Peikes et al., 2009), with only two care management programs covering the cost of the program (Hong et al., 2014; Peikes et al., 2012). Our evaluation found a substantial reduction in health care costs of $1,121.76 per member per month that provided a US$614.88 per member per month return on investment. Comparatively, the Washington University program studied by Peikes et al. (2012) was the only care management program found in the literature that described sufficient savings to cover the cost of the program, saving US$217 per member per month, with the cost of the program at US$151 per member per month and a net return on investment of US$66 per member per month.
One potential explanation for the cost reduction and overall positive return on investment relates to the reduction in inpatient admissions findings noted above. That is, the IDCT care management program likely reduces expenditures, in part, by reducing and avoiding costly inpatient admissions. It may also do so by reducing the severity of an admission (e.g., length of stay). It is also notable that, like the Washington University program that saved money, the program evaluated here also used face-to-face visits as opposed to telephonic visits. While face-to-face visits are more time and labor-intensive and thus cost more money, it is conceivable that these additional costs are offset by avoiding more intensive and more costly services (e.g., inpatient admissions).
A potential reason why the IDCT program in our study achieved more substantial savings and return on investment than the Washington University program is the use of a data-driven approach to select members into the program. In our evaluation, compared to members enrolled in the IDCT care management program but not selected by the algorithm, the algorithm-selected IDCT care management members had a 66% reduction in admissions and a health care cost savings of $19,507.26. The data-driven algorithm may be more effective at selecting members that are responsive to IDCT care management programs, which can provide a greater return on investment. This finding is reinforced by the fact that there were no significant differences between the treatment group selected by the algorithm and the control group. This finding also suggests that participant selection may matter for the cost-effectiveness and sustainability of an IDCT care management program and presents an opportunity for future research.
Limitations and Opportunities for Future Research
One limitation of this study is that it focuses on an IDCT care management program in one MA plan, which may limit the generalizability of the findings. Future research should consider replicating the study and including multiple health plans across multiple regions in the United States. Those regions should include rural and urban areas of the country, although rural areas are likely harder to reach with a field-based IDCT.
Another potential limitation is selection bias. Members who were selected by the algorithm for the IDCT care management program were the most promising members to manage. Consequently, the cost and utilization reductions observed in this study may represent a “best-case” scenario. For the health plan where this evaluation was conducted, this limitation was mitigated (for the time being) by the fact that the health plan had more members eligible for the program than it could enroll, given staffing constraints. Also, this study should be reviewed in future analysis to ensure there are no health inequity issues with the selection by the algorithm. The assumption is the likelihood of hospitalization is higher for the most vulnerable and underserved populations and that these populations are well represented in the sample. Likewise, we assumed that the program would reduce unnecessary inpatient utilization, not appropriate stays. However, these assumptions should be tested in future research.
A third limitation is that the study only looked at a 1-year postperiod and did not assess the longer-term effects of the IDCT care management program. We chose to focus the analysis on the most recent data available (2019) on one hand while avoiding more recent data (i.e., 2020) that was confounded by COVID-19, which not only strongly affected health utilization patterns but also presented major disruptions to IDCT activities. COVID-19, in addition to the way the program was structured (i.e., duration), also prevented us from applying other analytic approaches (e.g., ITS). Studies that included 2 or 3 postyears of data could provide insight as to whether the observed improvements and cost savings are sustainable. Future research may also want to consider different outcomes. For example, patient satisfaction and experience of care might be considered to assess more subjective aspects of care quality. Medication adherence and clinical outcomes are additional quality-dependent variables that could be considered.
Finally, the quantitative design of our evaluation means that our explanations of why the IDCT care management program was associated with lower inpatient utilization and costs are speculative. While our rationale for these relationships was rooted in a solid theoretical foundation (team interdependence and social cognitive theory), additional research is needed to more directly examine these concepts and their explanatory role. Likewise, future research should explore why health care providers refer and members self-refer into these programs, to better understand how these motivations may affect the enrollee selection process and the differences between these selection mechanisms. Such questions, however, will likely require primary data collection and may be especially well suited to qualitative approaches.
Implications for Practice and Policy
The findings of this study point to several practical implications. One important implication for health care delivery organizations (e.g., hospitals, accountable care organizations) and payers (e.g., insurers, employers) is the importance of considering how members are selected for participation in care management programs. Our study suggests that careful consideration of who gets enrolled can make a difference in whether the program pays for itself or not and, thus, can be sustained. Moreover, careful attention to the selection of participants in these programs can be leveraged to support and extend services that may not be profitable. For example, in this evaluation, the MA plan managed 912 members in the IDCT care management program. Six hundred sixty of these members were enrolled in the IDCT care management but not selected by the algorithm, while the remaining 252 members were enrolled in IDCT care management via the algorithm—savings relating to 252 members paid for the entire program of 912 members.
Assuming future studies of this algorithm find no evidence of adverse effects of such programs on health equity, policymakers may also want to consider conducting larger-scale demonstration programs. The Centers for Medicaid and Medicare Services (CMS) conducted a demonstration program for care coordination in 2006 (Peikes et al., 2009). However, none of the health plans in the demonstration program showed a return on investment. With a new demonstration program, CMS might consider different member selection mechanisms as key components of these programs.
Conclusion
This study provided a rigorous evaluation of an IDCT care management program with a novel, data-driven approach to selecting members for participation. We found that consistent with other studies, utilization was improved for members participating in the IDCT care management program. More importantly, this study is one of the few studies that demonstrate that IDCT care management using a data-driven algorithm to select members can pay for itself.
Our analyses found that health care costs for members enrolled in the IDCT care management program were reduced by US$1,121.76 and US$1,625.61 per member per month, respectively, relative to those not enrolled and those enrolled by physician referral. The cost reduction from the program generated enough savings to cover the program’s cost and a net savings of US$1.9MM. Our findings suggest that IDCTs may be able to cost-effectively manage populations of high-risk patients by fostering greater interdependence and better selection of suitable enrollees.
Thus, extending care through an IDCT can lead to healthier lives for members while at the same time addressing unstainable increases in health care costs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.