
Abstract
Veterans enrolled in the Veterans Affairs (VA) health care system gained greater access to non-VA care beginning in 2014. We examined hospital and Veteran characteristics associated with hospital choice. We conducted a longitudinal study of elective hospitalizations 2011 to 2017 in 11 states and modeled patients’ choice of VA hospital, large non-VA hospital, or small non-VA hospital in conditional logit models. Patients had higher odds of choosing a hospital with an academic affiliation, better patient experience rating, location closer to them, and a more common hospital type. Patients who were male, racial/ethnic minorities, had higher VA enrollment priority, and had a mental health comorbidity were more likely than other patients to choose a VA hospital than a non-VA hospital. Our findings suggest that patients respond to certain hospital attributes. VA hospitals may need to maintain or achieve high levels of quality and patient experience to attract or retain patients in the future.
Introduction
The Veterans Affairs (VA) health care system cares for more than 9 million Veterans eligible for care nationwide through its 171 integrated care delivery systems. The VA also purchases care from community providers when care cannot be provided on-site or within certain access standards. Veterans who are dually enrolled in the VA and another insurance program can access non-VA care as well. Veterans gained greater access to non-VA care beginning in 2014 through the Veterans Choice Act, (“Access, Veterans Choice, and Accountability Act of 2014,” 2014), which increased the VA’s purchase of community care when Veterans experienced distance, wait time, or hardship barriers to care, and expansions to Medicaid programs in states that increased adult eligibility under the Affordable Care Act (Kizer, 2012). Subsequently, many Veterans who needed acute inpatient care had more choices for hospital care (Yoon et al., 2022).
Increased access to hospital care enables patients to choose hospitals that provide better care or have other attributes that they prefer such as closer hospitals that have lower travel costs, smaller or larger hospitals, or hospitals providing more specialized services. Greater choice of hospitals could also potentially improve patients’ outcomes if patients choose hospitals that provide better quality or timeliness of care. VA hospitals are typically smaller in size than private hospitals and often provide a more narrow set of specialty services (Nuti et al., 2016). Therefore, VA hospitals face new pressures to compete for patients, and they may not retain patients if they cannot provide care that meets Veterans’ needs and preferences.
Prior Literature
Several studies documented patients’ preferences for hospital care in the general population that included greater hospital effectiveness and safety, better quality of care, closer proximity, and lower out-of-pocket patient costs (Groenewoud et al., 2015; Gutacker et al., 2016; Luft et al., 1990; Moscelli et al., 2016; Mühlbacher et al., 2016). While most studies focused on hospital characteristics, one study examined both patient and hospital attributes that were related to rural Medicare patients bypassing their closest rural hospital to obtain care from an urban hospital (Tai et al., 2004). This study found that overall patients were more likely to choose hospitals that were larger, had greater scope of services, and were closer to them, but patients who were more medically complex, White, and more educated were more likely to bypass their closest rural hospital for an urban teaching hospital compared to other patients. Other studies on hospital care found that higher risk patients were willing to travel farther to their hospital and more likely to choose larger hospitals (Adams et al., 1991; Phibbs et al., 1993). Therefore, patient characteristics are important to consider in understanding patients’ choice of hospital.
New Contribution
The expansion of non-VA care options for Veterans provides us with a unique opportunity to observe which hospitals patients chose and how factors such as VA affiliation, patient experience, size, and other factors affected their choices. As most Veterans in the VA are covered by insurance programs (e.g., Medicare, Medicaid, and employer-based coverage) and often make choices between VA and non-VA care, we include non-VA hospital care purchased by the VA as well as covered by insurance. We also examined the characteristics of patients that were related to choosing a VA or non-VA hospital because VA hospitals have to plan for services around a changing patient population in an era of greater choice. We use a unique data set of VA and non-VA hospitalizations for Veterans enrolled in the VA system from 2011 to 2017 to examine these questions. This work has relevance outside the VA system as private health plans can limit or expand their provider networks for hospital care, so private sector patients make similar choices for care.
Method
Conceptual Model
We use a model of hospital choice based on McFadden’s conditional choice model, which is an economic model used to explain discrete choices (McFadden, 1973). Underlying the McFadden model is patients’ utility gained from hospital and other health care services which is based on characteristics of hospitals/providers such as quality and patients’ access to them. In our conceptual model, Uij is the utility or value of the jth choice for the ith patient that is composed of both a systematic (γ) and random (ε) component: Uij = γ ij + ε ij
Patients or their providers choose a hospital among several alternatives based on certain hospital attributes (Adams et al., 1991; Shahian et al., 2000; Wilson et al., 2007). In the conditional logit model, the probability of choice j can be expressed as:
H represents the characteristics of hospitals that affect choice of hospital, and X represents the characteristics of patients, such as age, gender, and comorbidity that influence choice of hospital. Since the Choice Act expanded patients’ access to non-VA care, we can estimate this effect on VA enrollees’ use of VA and non-VA hospitals.
Study Design and Sample
We conducted a longitudinal study with repeated cross-sections of Veterans enrolled in the VA system with a hospitalization from 2011 to 2017 in 11 geographically diverse states (AZ, CA, CT, FL, IL, LA, MA, MO, NY, PA, and SC) which allowed linkage between all-payer state discharge data and personal identifiers of Veterans enrolled in the VA (no 2012 data were obtained for IL). These states represented the Northeastern, Southeastern, Midwestern, and Western regions of the United States, and approximately 38% of all VA enrollees lived in these 11 states (National Center for Veterans Analysis and Statistics, 2018). We included non-VA hospitalizations covered by all types of insurance and those provided through VA-purchased care.
We focused on elective hospitalizations because they are typically pre-planned where patients exert some choice of hospital rather than nonelective or emergent hospitalizations where patients may be transported by ambulance to a nearby hospital or admitted from the emergency department in the closest hospital. Elective hospitalizations in non-VA hospitals were determined based on the admission type reported in discharge records. VA inpatient data do not report admission type, so we assigned VA hospitalizations as elective when they had the same diagnosis related group (DRG) and primary diagnosis code combinations of non-VA hospitalizations identified as elective.
We included acute medical/surgical hospital stays and excluded psychiatric and long-term stays. If patients had more than one hospitalization during the study period, we randomly selected one hospitalization per patient. Veterans’ VA inpatient utilization records were obtained from the Inpatient Encounter files in the VA Corporate Data Warehouse (US Department of Veterans Affairs, n.d.). Veterans’ non-VA inpatient records were obtained from state inpatient discharge data linked to VA enrollment data using personal identifiers of VA enrollees through research requests to state public health agencies.
We obtained patients’ sociodemographic characteristics from the Assistant Deputy Under Secretary for Health (ADUSH) Enrollment Files (US Department of Veterans Affairs Information Resource Center, 2013) and the VA Observational Medical Outcomes Partnership (OMOP) Files (Lynch et al., 2019). Veterans’ and VA hospitals’ location, including longitude and latitude coordinates, were obtained from the VA Geospatial Services Support Center Files (US Department of Veterans Affairs, 2011–2017a). Non-VA hospital location was obtained from state discharge data linked to the Centers for Medicare and Medicaid Services Provider of Service file (Centers for Medicare & Medicaid Services, n.d.). VA hospital characteristics were obtained from data in the Veterans Health Administration Support Services Center, (US Department of Veterans Affairs, 2011–2017b) and non-VA hospital characteristics were obtained from Centers for Medicare & Medicaid Services hospital cost reports and provider files (Cutting et al., 2007). The study was approved by the Stanford University, University of Utah, and Greater Los Angeles VA IRBs.
Dependent Variable
We created a hospital typology for hospitals within a Veterans’ Hospital Service Area (HSA) as defined by the Dartmouth Atlas; HSAs represent the local market for hospital care (Wennberg et al., 2008). HSAs are delineated by zip codes for hospitals where the greatest proportion of Medicare beneficiaries were hospitalized. In our study, all hospitals within an HSA were assigned to one of the three following types: (1) VA hospital, (2) Large non-VA hospital 200+ beds, and (3) Small non-VA hospital < 200 beds. Large and small hospitals were based on prior studies categorizing hospitals by number of beds (Giancotti et al., 2017). Analysis was limited to Veterans who lived in an HSA with a VA hospital and at least one small or large non-VA hospital. While not all Veterans had access to all types of non-VA hospitals in their HSA due to limited provider networks covered by their insurance, lack of non-VA insurance, or lack of participation by hospitals in a VA’s community care network, we used all hospital types in an HSA as a proxy for patients’ choice sets.
Independent Variables
We examined the association of patient and hospital characteristics with hospital choice. Patients’ age, gender, race/ethnicity, marital status, and VA priority for VA health care were obtained for the year of patients’ discharge. VA priority status was based on Veterans’ military service-connected disability rating and income below the VA means test and ranged from high to low priority (group 1–8). We also measured patients’ comorbidity for each stay using the Elixhauser–van Walraven index calculated from all recorded inpatient diagnosis codes (van Walraven et al., 2009). We indicated patients’ mental health comorbidity based on secondary inpatient diagnosis codes for mood disorders including depression, serious mental illness (SMI), substance use disorders (SUDs), or posttraumatic stress disorder (PTSD). We also obtained zip code-level median household income from the U.S. Census and zip code-level unemployment rates from the Bureau of Labor Statistics because we did not have these measures for individual patients.
Hospital characteristics were measured in each year including academic affiliation to indicate major teaching hospital, patient experience rating using the percent of patients reporting they were most likely to recommend their hospital to others (Siddiqui et al., 2014) and number of hospitals of each type in an HSA. Patients’ distance to their hospital and their alternatives was calculated using the straight-line distance using street addresses. For descriptive purposes, we measured the number of staffed beds and the mean bed occupancy rate which was calculated as the mean of the number of beds occupied divided by the number of beds staffed during the year.
Statistical Analysis
We modeled patients’ choice of hospital using the alternative-specific conditional logit (ASCLogit) model known as McFadden’s Choice model (McFadden, 1973). In the ASCLogit model each patient represents a case, and each hospital type within a patient’s HSA represents an alternative. It is the equivalent to a conditional logit model including interaction terms between case variables and each alternative. Each observation represents a patient’s hospital alternative that may be chosen, and we estimate a binary outcome for the chosen alternative among all alternatives within an HSA. We adjusted for both alternative-specific variables and case-specific variables in the model. Hospital or alternative-specific variables included distance to patients’ residence, academic affiliation, patient experience rating, and number of hospitals. Patient or case-specific variables included year, post-Choice Act period, age, gender, race/ethnicity, VA enrollment priority, marital status, comorbidity score, mental health comorbidity, area-level median income and unemployment rate, and state of residence.
We used one conditional logit model for all patients predicting choice of a VA hospital or small non-VA hospital relative to a large non-VA hospital. We obtained one set of odds ratios for hospital variables, and two sets of odds ratios for patient variables for the two hospital types relative to large non-VA hospitals.
We conducted several sensitivity analyses to test the robustness of our findings. We restricted analysis to Veterans who lived in an HSA with all three hospital types. Since most older adults are covered by Medicare and may face a different choice set given most hospitals accept Medicare coverage while younger adults may have less non-VA insurance coverage and have a more constrained set of hospital choices, we separated patients by age group into those under 65 years of age and those 65 years and older in separate ASCLogit models. Since VA hospitals vary widely in size and availability of services, we also categorized VA hospitals as small and large based on the VA complexity model and conducted ASCLogit models with four alternatives: (a) Small VA hospital, (b) Large VA hospital, (c) Small non-VA hospital, and (d) Large non-VA hospital. We also predicted patients’ hospital choices using hospital referral regions instead of HSAs since these are larger areas that represent markets for tertiary care.
We tested the independence of irrelevant alternatives (IIAs) assumption using the Hausman test (McFadden, 1987), and results suggest that the IIA assumption failed, so we conducted a nested logit model with VA and non-VA hospitals separated at the top level. However, our primary model was an ASCLogit because our hospital types often provide different levels and range of services, so they may not be close substitutes.
Results
Sample Patient and Hospital Characteristics
There was a total of 290,050 patients who were enrolled in the VA in one of the 11 study states and had at least one elective hospitalization in a VA or non-VA hospital between 2011 and 2017. The mean age of study patients was 66 years (SD = 14), and the vast majority (93%) were male (Table 1). Almost three quarters (69%) of the sample was White while 17% of patients were Black, 6% were Hispanic, and 8% were another or unknown race/ethnicity. About half of patients (51%) were currently married, and half of patients were eligible for VA care through a service-connected disability. The mean Elixhauser–van Walraven comorbidity score was 4.1 (SD = 6.7), and mood disorders including depression (17%) were the most common type of mental health comorbidity among patients. Patients traveled a mean of 29 miles (SD = 33) to their hospital. Patients were distributed across 11 states with California, and Florida being the most common states in which patients resided.
Patient and Hospital Characteristics for Elective Hospitalizations in VA and Non-VA Hospitals in 11 States, 2011–2017.
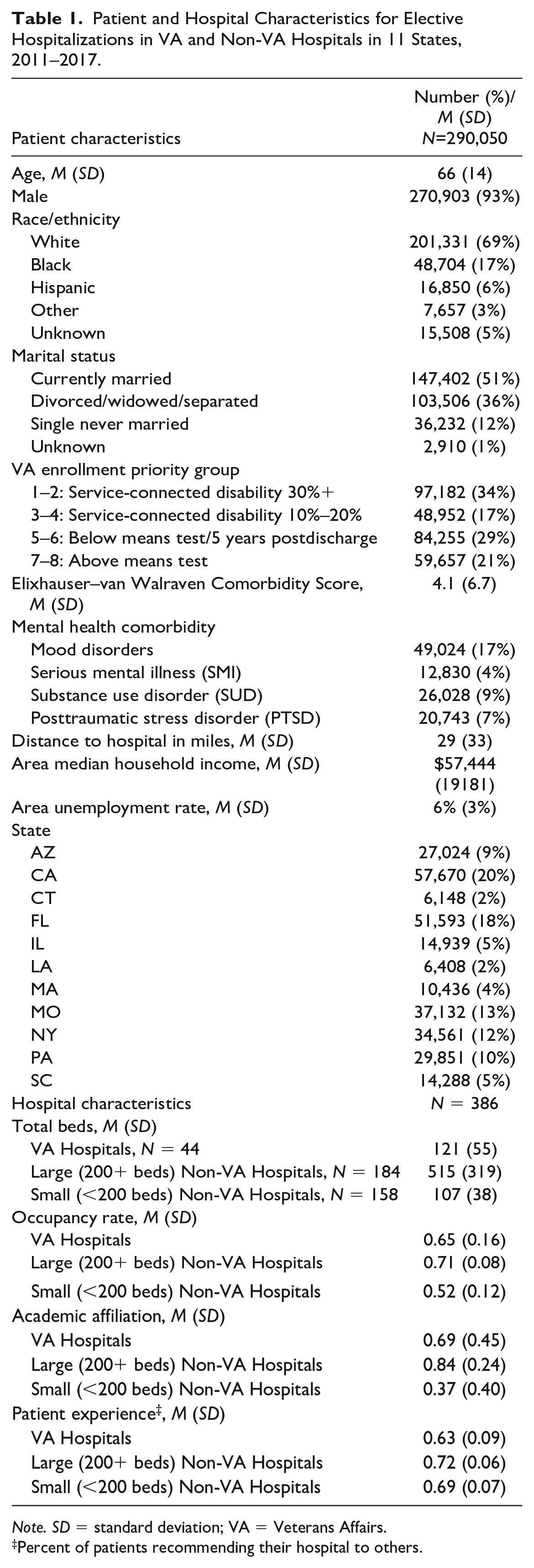
Note. SD = standard deviation; VA = Veterans Affairs.
Percent of patients recommending their hospital to others.
Among the three hospital types that patients visited, hospital characteristics varied. Small non-VA hospitals, M = 107 (SD = 38) and VA hospitals, M = 121 (SD = 55) had fewer mean number of beds compared to large non-VA hospitals, M = 515 (SD = 319). The mean occupancy rates of VA (0.65) and large non-VA hospitals (0.71) were higher than the occupancy rate of small non-VA hospitals (0.52). The mean proportion of hospitals with an academic affiliation ranged from 0.37 of small non-VA hospitals to 0.69 of VA hospitals, and 0.84 of large non-VA hospitals. Mean patient experience scores as measured by the proportion of patients recommending their hospital to others were higher in large (0.72) and small (0.69) non-VA hospitals than in VA hospitals (0.63).
There was a mean of one VA hospital and almost six large and small non-VA hospitals in a Veteran’s HSA (Table 2). Overall, when patients had a choice of a VA or other hospital, patients chose a VA hospital more than half of the time (0.53) compared to a probability of 0.40 of choosing a large non-VA hospital and 0.10 of choosing a small non-VA hospital in their HSA. Most patients in an HSA with a VA hospital had all three types of hospitals.
Frequency of Hospital Type Chosen in a Hospital Service Area. a
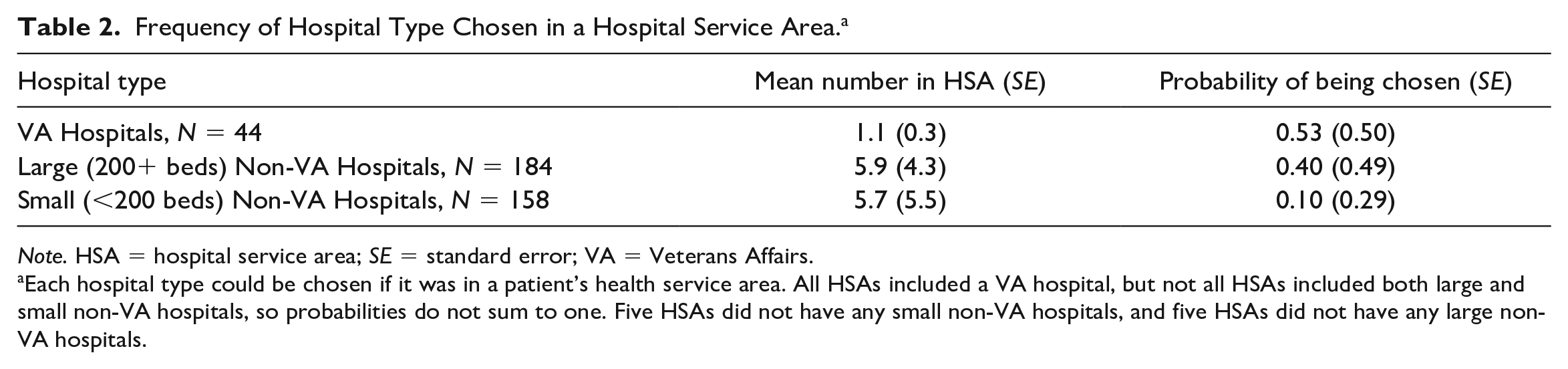
Note. HSA = hospital service area; SE = standard error; VA = Veterans Affairs.
Each hospital type could be chosen if it was in a patient’s health service area. All HSAs included a VA hospital, but not all HSAs included both large and small non-VA hospitals, so probabilities do not sum to one. Five HSAs did not have any small non-VA hospitals, and five HSAs did not have any large non-VA hospitals.
Hospital Factors Affecting Hospital Choice
In a conditional logit model predicting patients’ choice of hospital type, the odds of choosing a hospital with an academic affiliation was 77% higher than choosing hospitals without an academic affiliation (odds ratio [OR] = 1.77) (Table 3). Patients were 8% more likely to choose a hospital with a one-standard deviation higher patient experience rating than a hospital with a lower rating (OR = 1.08). A 1-mile increase in travel distance to a patient’s hospital reduced patients’ odds of choosing that hospital by 5% (OR = 0.95). The more hospitals of a given type in patient’s HSA, the more likely a patient was to select that type of hospital (OR = 1.11). All results noted were significant at p < .01.
Hospital and Patient Factors Predicting Choice of Hospital Type in a Hospital Service Area, N = 290,050 Patients.
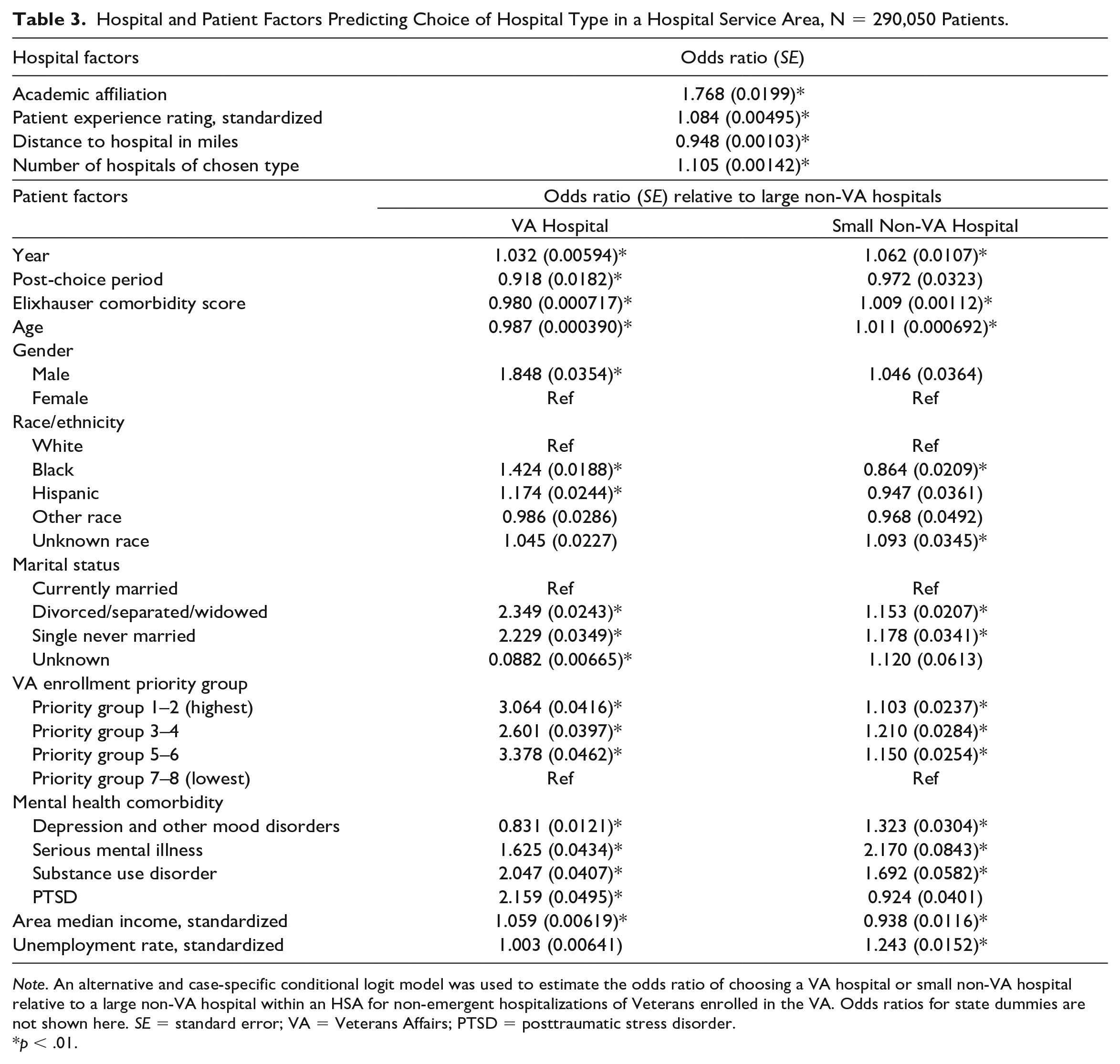
Note. An alternative and case-specific conditional logit model was used to estimate the odds ratio of choosing a VA hospital or small non-VA hospital relative to a large non-VA hospital within an HSA for non-emergent hospitalizations of Veterans enrolled in the VA. Odds ratios for state dummies are not shown here. SE = standard error; VA = Veterans Affairs; PTSD = posttraumatic stress disorder.
p < .01.
Patient Factors Affecting Hospital Choice
There were also significant patient factors related to the likelihood of choosing between hospital types. Patients were significantly more likely to choose a VA hospital over a large non-VA hospital over time but less likely to choose a VA hospital after the Choice Act (p < .01). Male patients compared to female patients, and Black and Hispanic patients compared to White patients were significantly more likely to choose a VA hospital over a large non-VA hospital in their HSA (all p < .01). Patients not currently married relative to married, patients with higher VA enrollment priority due to service-related conditions relative to lower priority, and patients diagnosed with a comorbid SMI, SUD, or PTSD relative to those without those conditions, and those living in higher income areas were also more likely to choose a VA hospital over a large non-VA hospital (all p < .01). Patients who were older, had greater comorbidity, and diagnosed with a mood disorder were less likely to choose a VA hospital when they had the option of a large non-VA hospital (all p < .01).
There were similar patient factors related to patients’ choosing small non-VA hospitals over large non-VA hospitals. Patients were more likely to choose a small non-VA hospital over a large non-VA hospital over time (p < .01). Older compared to younger patients, more comorbid compared to less-comorbid patients, not currently married compared to married, higher compared to lower VA enrollment priority Veterans, and those living in areas with higher unemployment rates were more likely to choose small non-VA hospitals over large non-VA hospitals (p < .01). Black patients compared to White patients and those living in higher income areas were less likely to choose small over large non-VA hospitals (p < .01).
Sensitivity Analyses
When restricting the study sample to patients who had all three hospital types in their HSA, results for patient and hospital factors were very similar as in the original models (Online Appendix). In models stratified by patients’ age less than 65 years or 65 years and older, results were similar for most of the patient factors. However, for patients less than 65 years of age, older age significantly predicted greater likelihood of choosing a VA hospital over a large non-VA hospital while for patients 65 years and older, older age significantly predicted less likelihood of choosing a VA hospital over a large non-VA hospital. We conducted analysis with separate hospital types for large and small VA hospitals because VA hospitals vary in their size and complexity. Large VA hospitals tend to have more services available and close academic affiliation to a medical school similar to academically affiliated non-VA hospitals. Many of the same patient factors predicted choice of both VA hospital types over large non-VA hospitals. However, patients were significantly more likely to choose large VA hospitals and less likely to choose small VA hospitals over a large non-VA hospital after the Choice Act. Results using larger hospital referral regions instead of HSAs as patients’ choice set were similar with respect to significant hospital and patient factors related to choice of hospital. Finally, in a nested logit model, results on hospital and patient factors affecting choice of VA or non-VA hospital were very similar as the original model comparing VA versus large non-VA hospital.
Discussion
This is the first study using all-payer data to document hospital and patient characteristics that affected Veterans’ choice of VA or non-VA hospital at a time when Veterans had expanded access to non-VA hospitals. We found that patients were more likely to choose VA or non-VA hospitals based on certain hospital characteristics. Hospitals’ academic affiliation was positively associated with patients choosing a hospital. Hospital teaching status has been previously related to better hospital outcomes such as process measures of care and lower mortality in several studies (Allison et al., 2000; Burke et al., 2017; Sloan, 2021). Therefore, patients’ choice of academic hospitals over other hospitals may be partly based on higher perceived quality from publicly available measures of technical quality, anecdotal information, or prior experiences. Academic hospitals are also more likely to offer specialized services and more advanced technologies, so it may be easier for patients to obtain a specific procedure or service from a large academic non-VA hospital when that service cannot be provided at a VA hospital or small non-VA hospital.
We also found that patients were more likely to select hospitals closer to them which has been previously reported (Chou et al., 2014; Mooney et al., 2000; Smith et al., 2017). A 1-mile increase in distance to a hospital decreased patients’ odds of visiting that hospital; therefore, patients were sensitive to even small differences in distance for elective hospitalizations. Since many Veterans live far from a VA hospital, VA’s latest policy under the Maintaining Internal Systems and Strengthening Integrated Outside Networks (MISSION) Act of expanded eligibility for Veterans to receive non-VA care due to drive time and other access barriers is expected to have further increased the number of Veterans seeking care from a closer non-VA hospital (MISSION Act, 2018).
Patient experience rating was another significant hospital factor that affected patients’ choice of hospital. Other research found that patients’ perceptions of quality of care was related to patients’ willingness to recommend their hospital (Klinkenberg et al., 2011; Sofaer et al., 2005; Xu et al., 2022), so patients appear to be able to discern between hospitals that provide better quality and experience than others. In our study sample, VA hospitals had a lower mean patient experience rating than non-VA hospitals, and we did not have information on what aspects of care negatively impacted patients’ experience scores in VA hospitals. However, a prior study found that VA hospitals had lower scores on nursing and physician communication, responsiveness, quietness, and pain management in addition to overall patient experience (Blay et al., 2017). While the VA has a long history with quality improvement initiatives such as tracking and reporting technical measures of inpatient performance and patient experience (Graham & Tetroe, 2009; Jha et al., 2003; Khuri et al., 2008), VA hospitals may need to make further improvements in care to attract or retain patients within the VA system. Increasing affiliations with medical schools and schools for other health professions by VA hospitals could be one mechanism to improve patient experience and quality although many VA hospitals already maintain affiliations with medical schools. Salaries of VA providers and nurses have been documented to be lower than nonfederal health care professionals (Weeks et al., 2009), so increasing salaries to be competitive with other health care organizations may also improve recruitment of providers. Still, more work is needed to understand what specific aspects of patients’ experiences with VA inpatient care could be improved further.
We also found that the greater the number of hospitals of a certain type, the greater the likelihood that patients chose that type of hospital. It is likely that the more small or large non-VA hospitals available to a patient, the fewer access barriers patients had, such as shorter waiting times for a procedure or shorter distance to travel to one of these hospitals. Therefore, the more non-VA hospitals available to patients, the less likely a patient would be to choose a VA hospital.
We found a negative association between the Choice Act and choice of a VA hospital, and this appeared to be driven by patients less likely to choose small VA hospitals but not large VA hospitals after the Choice Act. Patients were also significantly less likely to choose small non-VA hospitals over large non-VA hospitals after the Choice Act, potentially due to the fact that VA-purchased care involved contracts with larger hospitals. Patients appeared to prefer large hospitals when given more choice which may be due to higher perceived quality or wider range of services available at larger hospitals (Escarce & Kapur, 2009; Kennedy et al., 2014).
There were also significant patient factors that affected which type of hospital patients chose when they had different alternatives, and many of these patient factors have been previously documented to affect patients’ use and reliance of VA care (Hynes et al., 2007; Liu et al., 2011; Petersen et al., 2010). Among nonelderly patients, older patients preferred VA hospitals while elderly patients preferred non-VA hospitals, likely due to Medicare eligibility and a larger choice set of hospitals. Older patients also preferred small non-VA hospitals to large non-VA hospitals. Male patients were more likely to prefer VA hospitals than female patients which is unsurprising because some VA hospitals cannot provide gender-specific services on-site. Black and Hispanic patients were more likely to choose a VA hospital than White patients, and their greater reliance on VA care has been documented in prior research (Hynes et al., 2007; Liu et al., 2011). Similarly, Veterans with service-connected disabilities also were more likely to choose VA hospitals as they also have greater reliance on VA care partly due to specialty VA services such as traumatic brain injury and spinal cord injury programs to treat conditions related to military service as well as lower patient cost-sharing for care. Patients with greater comorbidity preferred non-VA hospitals to VA hospitals. Patients with mental health conditions including SMI, SUD, and PTSD were more likely to seek care from a VA hospital.
Limitations
While Veterans had increased access to non-VA hospital care sponsored by the VA under the Veterans’ Choice Act, Veterans without non-VA insurance were limited to hospitals under contract with their VA facility, and some geographic areas had narrow or sparse community care networks with few available providers. Therefore, some Veterans had few options for non-VA care. Our findings showing greater likelihood of patients visiting hospitals with certain hospital attributes may be due to which hospitals participated in VA community care networks or Veterans’ insurance networks rather than patients’ true preferences for care. We did not have data on which non-VA hospitals were part of VA community care or specific insurance networks, so we were unable to account for this in patients’ choice sets. Our data were also limited to data in 11 states that allowed for the linkage of state discharge data with VA data, and we were not able to obtain data following the MISSION Act implemented in 2018. Therefore, our findings may not be representative of Veterans and their non-VA hospital care nationally or generalizable to more recent choices of Veterans for hospital care. We did not account for wait times for care even though they affect the relative use of VA and non-VA care (Yee et al., 2022).
Conclusion
Veterans have more choices for health care providers in both the private and public sector after recent health care reforms, most recently with the MISSION Act which increased access to VA community care on a larger scale. VA hospitals must now compete with private hospitals to be the provider of choice for Veterans. Our findings suggest that if VA hospitals maintain or achieve high levels of quality and patient experience and maintain affiliation to medical schools or offer a wide range of services, they may be more successful in attracting or retaining patients in the future. The VA makes many performance measures on VA care publicly available on Hospital Compare, so making greater gains on measures accessible to patients can benefit both patients’ care and VA hospital patient volumes in the future. Without continued modernization, VA hospitals may face questions over their long-term sustainability.
Supplemental Material
sj-docx-1-mcr-10.1177_10775587231194681 – Supplemental material for Hospital and Patient Factors Affecting Veterans’ Hospital Choice
Supplemental material, sj-docx-1-mcr-10.1177_10775587231194681 for Hospital and Patient Factors Affecting Veterans’ Hospital Choice by Jean Yoon, Michael K. Ong, Megan E. Vanneman, Yue Zhang, Matthew P. Dizon and Ciaran S. Phibbs in Medical Care Research and Review
Footnotes
Acknowledgements
The authors wish to thank Adam Chow, BA, Andrew Redd, PhD, and Hao Jiang, MS, for programming assistance and Emily Wong, MPH, MHA, for project support. Chow, Jiang, and Wong are employees of the VA Palo Alto. Andrew Redd is an employee at the University of Utah School of Medicine.
Disclaimer
The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the United States government or any of the state agencies listed above.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Health Services Research and Development (HSR&D), Veterans Health Administration (VHA), Department of Veterans Affairs (VA) Award #IHX002653-01A1. M.E.V. is also supported by an HSR&D Career Development Award (CDA 15-259, award 1IK2HX002625). The funding organization had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; or decision to submit the manuscript for publication.
Data Accessibility
Data used for this project will not be made available to others because data were obtained under separate memorandum of understanding agreements with state public health agencies. Statistical code used in this analysis is available by request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.