
Abstract
The objective of this study is to examine access to care based on gender identity in urban and rural areas, focusing on transgender and gender diverse (TGD) populations. Data on TGD (n = 1,678) and cisgender adults (n = 403,414) from the 2019 to 2020 Behavioral Risk Factor Surveillance System were used. Outcome measures were four barriers to care. We conducted bivariate and multivariable logistic regressions to assess associations between access, rurality, and gender identity. Bivariate results show that TGD adults were significantly more likely to experience three barriers to care. In multivariable models, TGD adults were more likely to delay care due to cost in the full sample (adjusted odds ratio [AOR]: 2.00, p < .001), rural subsample (AOR: 2.14, p < .01), and urban subsample (AOR: 1.97, p < .01). This study revealed greater barriers to care for TGD adults, with the most frequent barriers found among rural TGD adults. Increased provider awareness and structural policy changes are needed to achieve health equity for rural TGD populations.
Keywords
Introduction
Transgender and gender-diverse (TGD) adults in the United States face more barriers to optimal health and accessing health care than cisgender adults (Gonzales & Henning-Smith, 2017; Streed et al., 2017). Some explanations for TGD health inequities include issues of systemic transphobia, as seen in recent anti-transgender legislation (Ronan, 2021), and health care providers with insufficient training in TGD-specific health (Obedin-Maliver et al., 2011; Romanelli & Lindsey, 2020; Stroumsa, 2014). TGD Americans are also more likely to face financial hardship, police brutality and abuse, and discrimination in places of employment, education, and public accommodations (Grant et al., 2011). Moreover, the effects of discrimination based on gender identity are compounded by structural racism for TGD people of color (Grant et al., 2011). Despite strides made through the Affordable Care Act (ACA), including new health insurance regulations prohibiting insurers from denying coverage based on sex (U.S. Department of Health and Human Services, 2010), and the Biden administration’s decision to define sex-based non-discrimination in the ACA that is inclusive of gender identity (Goldstein, 2021), barriers to health insurance coverage and affordable, appropriate, and high-quality health care remain (Gonzales & Henning-Smith, 2017; Meyer et al., 2017).
Although more than 15% of the U.S. population resides in rural areas, rural adults in the United States also face adverse health outcomes and greater barriers to care than urban adults (Probst et al., 2019), due to issues ranging from a lack of transportation (Akinlotan et al., 2021), an insufficient number of health care providers in rural areas (Colwill & Cultice, 2003), and urban-centric policies, which often fail to address the unique health care needs of rural residents (Probst et al., 2019). For instance, urban-centric policies can be seen in the market-oriented U.S. health care system, which requires high patient volume to provide quality services and in population-focused public health initiatives that allocate funds toward high-population communities (Probst et al., 2019). Moreover, rural areas have been disproportionately impacted by recent hospital closures (Frakt, 2019), hospitalizations and deaths due to COVID-19 (Ullrich & Mueller, 2022; Zhu et al., 2023), and other leading causes of mortality, such as heart disease, cancer, and unintentional injuries (Yaemsiri et al., 2019).
New Contributions
Many TGD people call rural areas home and demonstrate resilience and resourcefulness within those settings (Lahr et al., 2022). In addition, research demonstrates greater social cohesion in the form of “knowing each other well” in rural areas as compared with urban areas (Henning-Smith et al., 2022). However, very little representative research has examined barriers to care among rural TGD populations. Although research has illuminated health inequities based on gender identity (Gonzales & Henning-Smith, 2017) and rurality (Kozhimannil & Henning-Smith, 2021), more research is critically needed on the differential experience of health care access experienced by TGD populations in rural versus urban areas. This topic is of particular importance as, contrary to popular culture representations, many Lesbian, Gay, Bisexual, and Transgender (LGBT) people live in rural areas, enjoy living in rural areas, and find rurality to be a salient part of their identity (Movement Advancement Project, 2019b). Wide research gaps remain, partially because very few nationally representative datasets include information on health care access coupled with data on geographic location and gender identity (Henning-Smith et al., 2019; Lett & Everhart, 2022). This study begins to fill this important research gap using the largest, and one of the only available, population-based data sources in the United States that includes rurality, gender identity, and health care access information.
Methods
Data, Measures, and Sample
This study uses data from the 2019 to 2020 Behavioral Risk Factor Surveillance System (BRFSS), a nationally representative telephone survey of the civilian, non-institutionalized population aged 18 years and older. The BRFSS is conducted annually by the Centers for Disease Control and Prevention (CDC) in conjunction with state health departments. Approximately, 400,000 adults are randomly selected for the survey every year and are asked a core set of questions, including information about demographic and socioeconomic characteristics, health conditions, health care access, and health services utilization (Centers for Disease Control and Prevention, 2019a). The median state-level response rate was 49% in 2019 and 48% in 2020 (Centers for Disease Control and Prevention, 2020a, 2021A).
Currently, BRFSS data are separated into three sections: the core component, standardized optional modules for states to add, and state-designed questions (Centers for Disease Control and Prevention, 2019a). The core component does not ask questions about gender identity; however, many states have elected to use the unified Sexual Orientation and Gender Identity (SOGI) module provided by the CDC. Figure 1 presents the states that have added the SOGI module to their statewide surveys. In 2019, 30 states used the SOGI module, and in 2020, 32 states used the SOGI module (Centers for Disease Control and Prevention, 2020b, 2021c). This cross-sectional observational study analyzed BRFSS data from states who elected to use the SOGI module in 2019 and/or 2020.
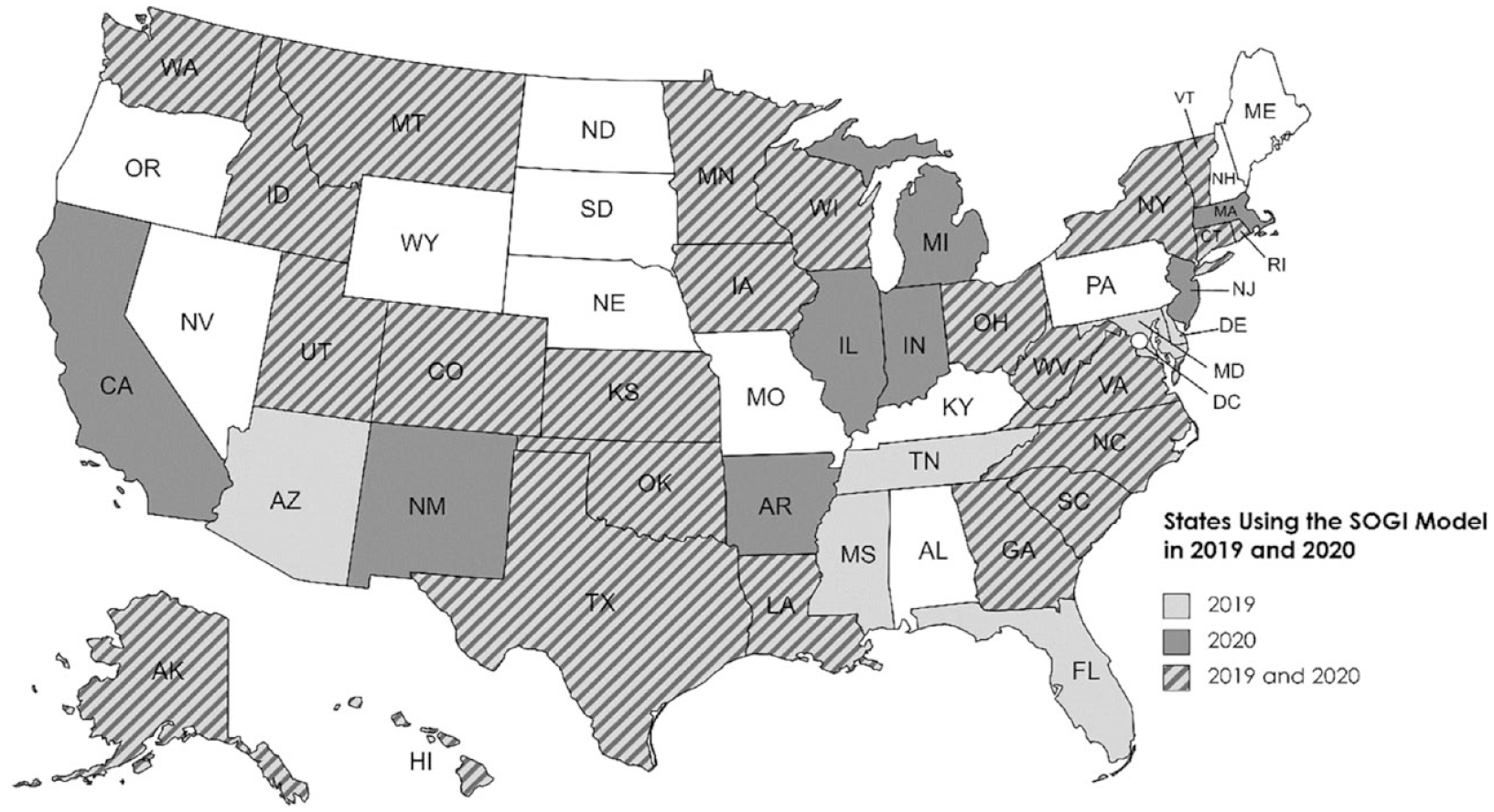
States Using the SOGI Module 2019 and 2020.
In the SOGI module, respondents are asked “Do you consider yourself to be transgender?” and can respond “Yes, transgender male-to-female”; “Yes, transgender female-to-male”; “Yes, gender non-conforming”; “No”; “Don’t know/Not Sure”; or “Refused.” Due to small sample sizes, we coded gender identity as a binary variable: “Yes, transgender or gender non-conforming” or “Cisgender.” However, it is important to note that after applying survey weights, .18% of respondents identified as “Transgender Male-to-Female,” .2% of respondents identified as “Transgender Female-to-Male” and .15% of respondents identified as “Gender Non-Conforming.” If asked about the meaning of transgender, participants were provided a definition for transgender and gender non-conforming. Rural status was defined at the county level using the 2013 National Center for Health Statistics (NCHS) Urban-Rural Classification Scheme to include all non-metropolitan counties; urban status included all metropolitan counties (Centers for Disease Control and Prevention, 2019b). Non-metropolitan counties are defined as those with an urbanized center of 49,999 people or fewer and those with no urbanized center. We included the following self-reported sociodemographic variables: race/ethnicity, highest grade, or year of school completed, annual household income, and age.
Data on the four outcome variables were based on the following BRFSS survey questions. Delayed care due to cost was based on the question, “Was there a time in the past 12 months when you needed to see a doctor but could not because of cost?” No health insurance coverage was based on the question, “Do you have any kind of health care coverage including health insurance, prepaid plans such as HMOs, or government plans such as Medicare or Indian Health Service?” No doctor was based on the question, “Do you have one person you think of as your personal doctor or health care provider?” Finally, No checkup was based on the question “About how long has it been since you last visited a doctor for a routine checkup?” This question was coded as “no” if the respondent had not had a checkup in the past 12 months and “yes” if the respondent had a checkup within the last 12 months.
The final weighted sample from 2019 and 2020 included 146,222 rural respondents (14.6%). This sample included 1,931 total TGD respondents (unweighted prevalence = 0.42%) 471 of whom lived in rural areas. However, after applying survey weights to the sample, 0.54% of survey respondents were transgender, 13.2% of whom were rural residents. Despite the relatively small sample size, it is notable that over 10% of transgender respondents were rural residents, especially given that these numbers are likely an undercount (Crissman et al., 2017; Meerwijk & Sevelius, 2017). There are several reasons this may be an undercount, including not all gender diverse individuals identifying with terms used in the BRFSS or other surveys and because not all gender diverse individuals will feel safe revealing their gender identity in a survey (Crissman et al., 2017; Meerwijk & Sevelius, 2017).
Analysis
In our analysis, we accounted for missingness using indicator variables and found that regarding the question of gender identity, there were a total of 469,997 respondents and 5,775 missing responses (1.23%). We weighted all variables in accordance with BRFSS guidelines using strata and primary sample unit variables and states and sample years 2019 and 2020 were combined also following BRFSS guidance (Centers for Disease Control and Prevention, 2021b).
Consistent with previous research (Gonzales & Henning-Smith, 2017), this study examined four health care access barriers: (a) delayed care due to cost, (b) no health insurance coverage, (c) no personal doctor, and (d) no routine checkup in the past 12 months. Collectively, these measures are routinely used by the CDC to monitor barriers to care for adults across the United States (Okoro et al., 2017). We used bivariate chi-square tests to examine the four health care access outcomes by gender identity and rurality looking first at the full sample (rural and urban respondents) and then at rural and urban subpopulations.
Next, we conducted four multivariable logistic regressions, also using survey weights, to examine the four health care access barriers separately while adjusting for gender identity, rurality, race/ethnicity, age, educational attainment, and household income. It is crucial to include factors, such as race and socioeconomic status when examining health care access barriers as research shows that Black, Indigenous, and People of Color (BIPOC) are disproportionately more likely to be uninsured/underinsured (Baumgartner et al., 2021) and face inequitable access to care (Yearby et al., 2022) due to structural racism. Moreover, studies demonstrate income is highly related to morbidity and mortality, and many low-income individuals remain excluded from accessing high-quality health care (Khullar & Chokshi, 2018). By including sociodemographic factors in our model, we recognize the intersecting identities held by rural TGD residents. We conducted logistic regression models first for the full sample and then stratified them for rural and urban dwellers. Stratification is our primary approach because it essentially allows for all differences, measured and unmeasured, that may intersect with gender and access to care. Finally, we conducted four additional multivariable logistic regression models that included the addition of a variable for the interaction between geographic location and gender identity. We used post-estimation analysis to show adjusted predicted percentages for these interactions. All analyses were conducted in Stata version 17.
Results
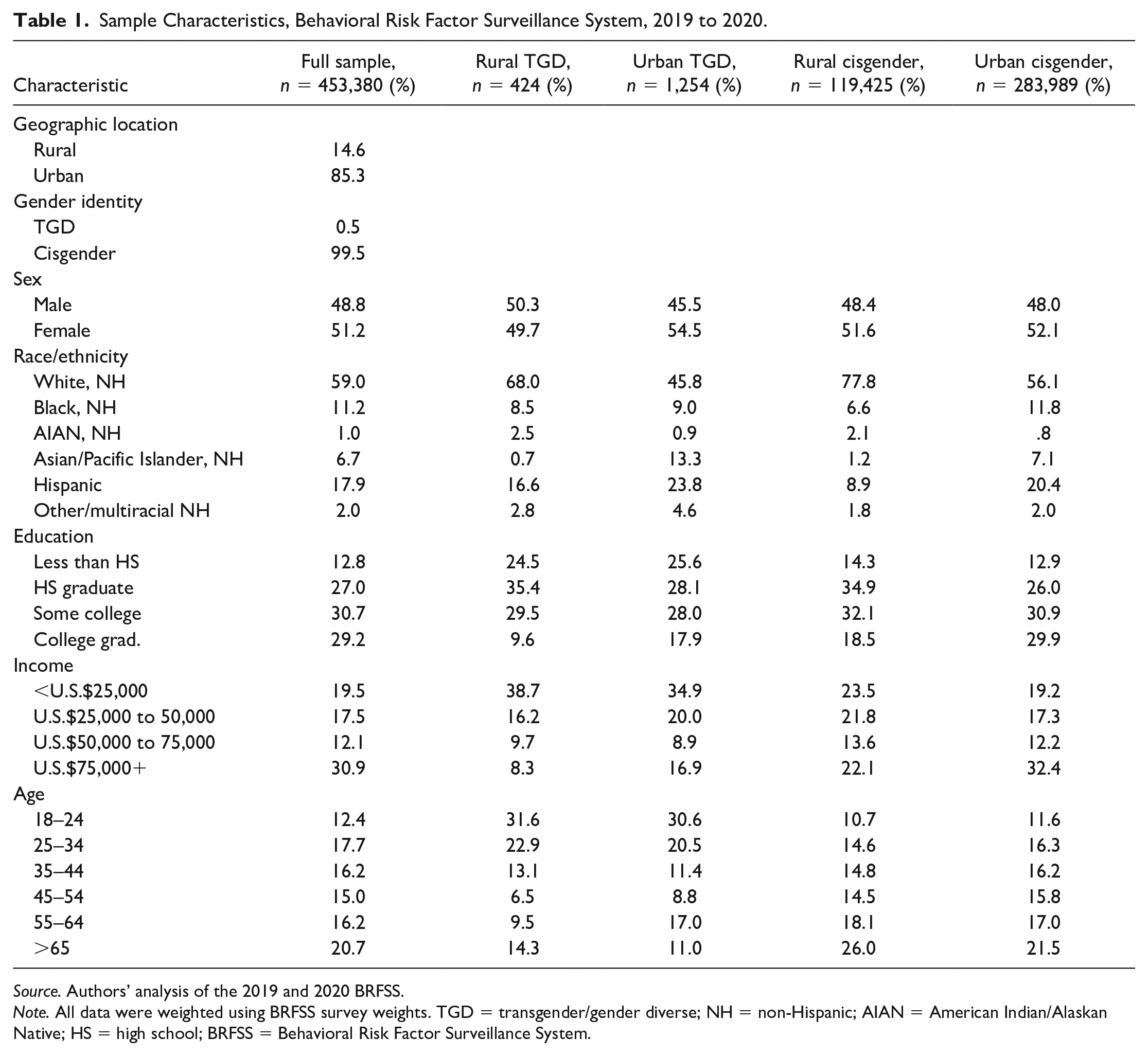
Table 1 presents the sociodemographic characteristics of our study sample by gender identity and rurality. Compared with their urban TGD peers, rural TGD adults were more likely to be non-Hispanic White, over the age of 65, and report lower levels of educational attainment and household income. Approximately, 24% of rural TGD adults reported less than a high school education, and nearly, 40% of rural TGD respondents reported household incomes less than U.S.$25,000 per year. Rural cisgender respondents were most likely to be non-Hispanic White and be over the age of 65 compared with rural TGD respondents, cisgender urban respondents, and TGD urban respondents. Compared with all rural subpopulations, urban cisgender respondents were most likely to be college graduates and in households earning more than U.S.$75,000 annually.
Sample Characteristics, Behavioral Risk Factor Surveillance System, 2019 to 2020.
Source. Authors’ analysis of the 2019 and 2020 BRFSS.
Note. All data were weighted using BRFSS survey weights. TGD = transgender/gender diverse; NH = non-Hispanic; AIAN = American Indian/Alaskan Native; HS = high school; BRFSS = Behavioral Risk Factor Surveillance System.
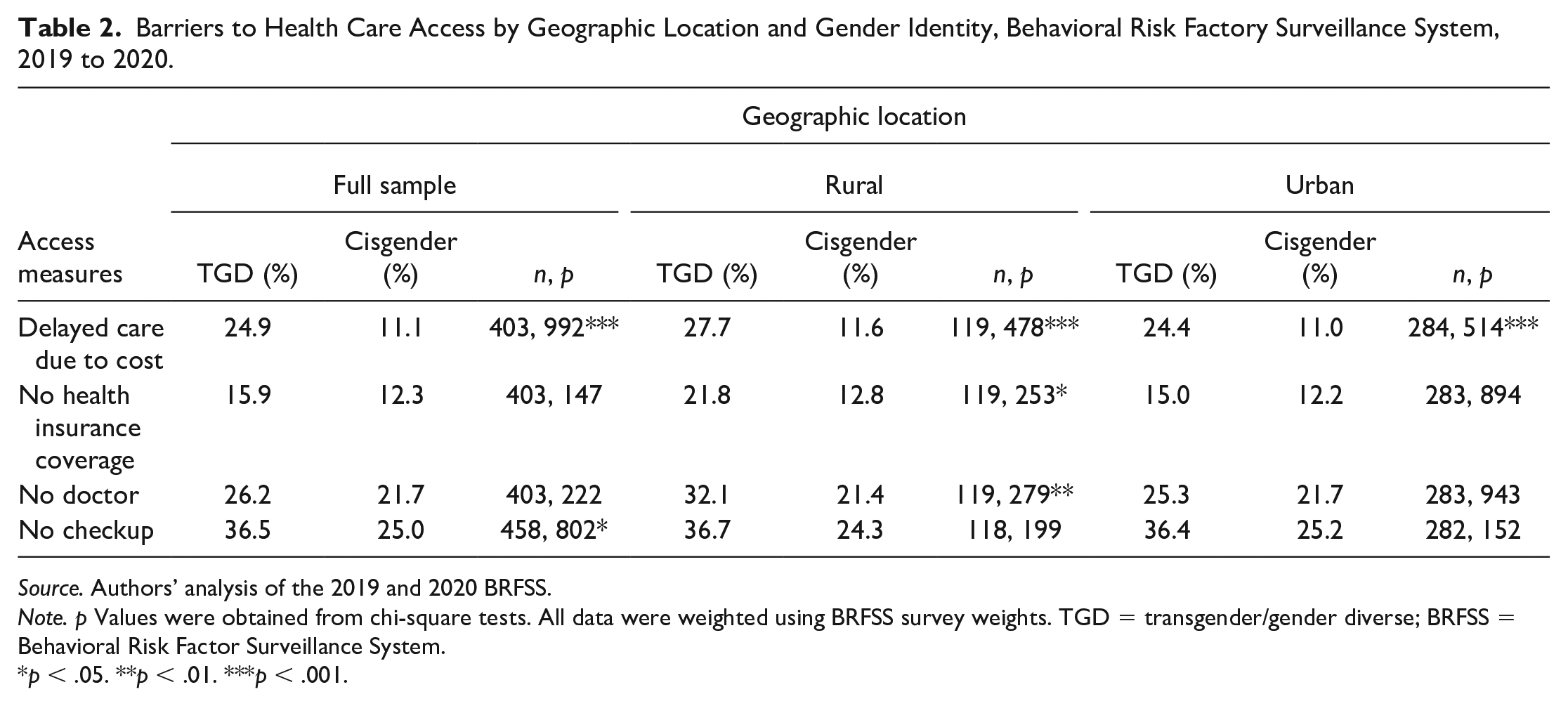
Findings from our bivariate analysis (presented in Table 2) demonstrate that in the full sample of urban and rural respondents, TGD respondents were significantly more likely to have delayed care due to cost and report not having a routine checkup in the past 12 months as compared with their cisgender peers. Among the rural-only subpopulation, TGD respondents were significantly more likely than cisgender respondents to delay care due to cost (27.7% vs 11.6%, p < .001); to have no health insurance coverage (21.8% vs 12.8%, p < .05); and to have no personal doctor (32.1% vs 21.4%, p < .01). Urban TGD respondents reported significantly higher levels of delaying care due to cost (24.4% vs 11.0% p < .001) compared with urban cisgender respondents. For all four barriers to care measured, the highest levels of each barrier to care were found among rural TGD respondents.
Barriers to Health Care Access by Geographic Location and Gender Identity, Behavioral Risk Factory Surveillance System, 2019 to 2020.
Source. Authors’ analysis of the 2019 and 2020 BRFSS.
Note. p Values were obtained from chi-square tests. All data were weighted using BRFSS survey weights. TGD = transgender/gender diverse; BRFSS = Behavioral Risk Factor Surveillance System.
p < .05. **p < .01. ***p < .001.
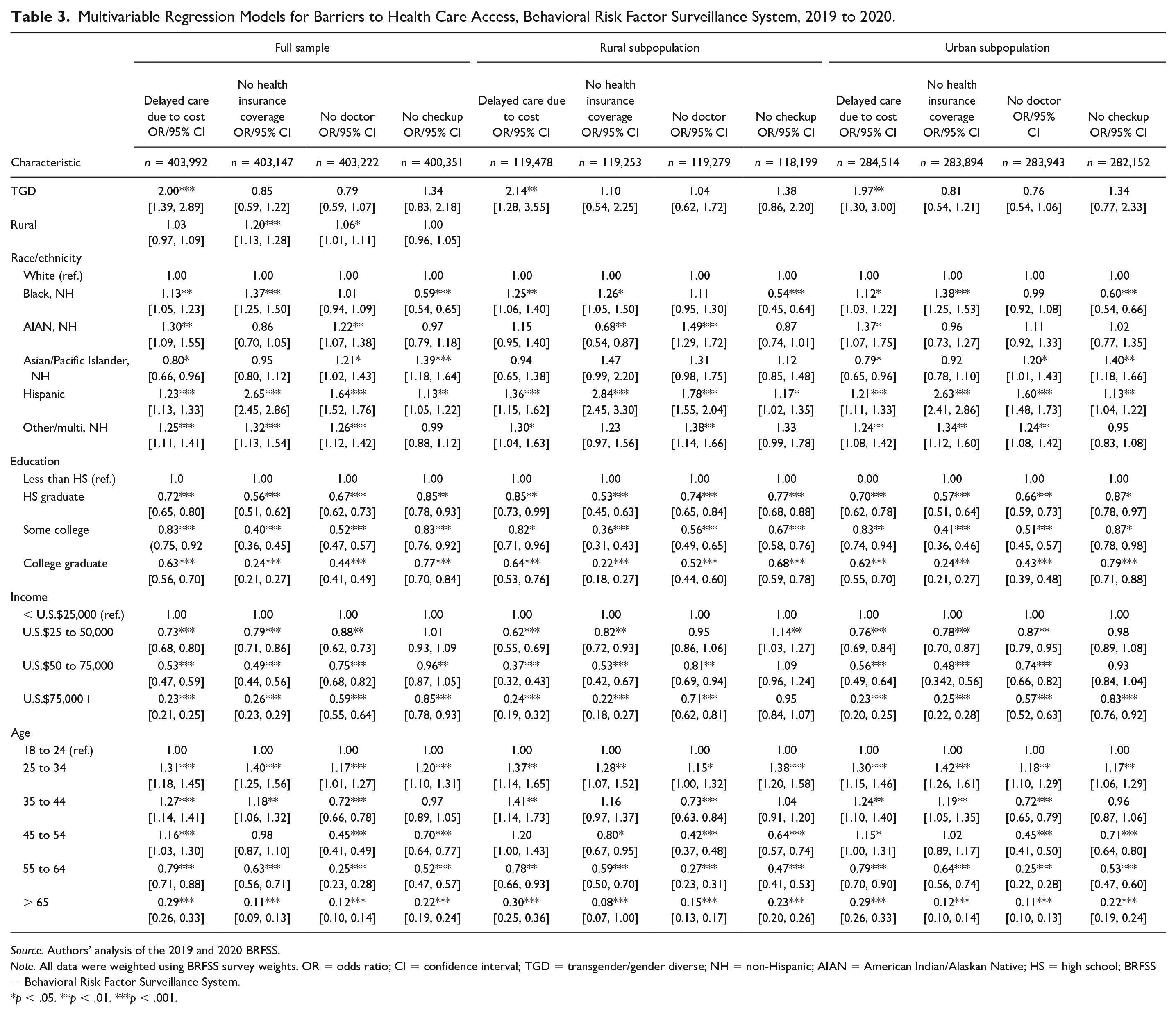
Findings from our first multivariable logistic regression analyses (reported in Table 3) revealed that among the full sample of rural and urban adults, TGD adults exhibited significantly higher odds of reporting delayed medical care due to cost (adjusted odds ratio [AOR]: 2.00; confidence interval [CI]: 1.39–2.89, p < .001) compared with cisgender respondents. Rural adults in the full model reported statistically significantly higher odds of having no health insurance coverage (AOR: 1.20; CI: .59–1.22; p < .001) compared with urban adults and statistically significantly higher odds (AOR: 1.06; CI: 1.01–1.11; p < .05) of having no doctor as compared with urban respondents.
Multivariable Regression Models for Barriers to Health Care Access, Behavioral Risk Factor Surveillance System, 2019 to 2020.
Source. Authors’ analysis of the 2019 and 2020 BRFSS.
Note. All data were weighted using BRFSS survey weights. OR = odds ratio; CI = confidence interval; TGD = transgender/gender diverse; NH = non-Hispanic; AIAN = American Indian/Alaskan Native; HS = high school; BRFSS = Behavioral Risk Factor Surveillance System.
p < .05. **p < .01. ***p < .001.
In the stratified model restricted to rural adults only, TGD adults reported higher odds of delaying medical care due to cost (AOR: 2.14; CI: 1.28–3.55; p < .01) compared with cisgender rural adults. In the stratified model restricted to urban adults, TGD adults reported significantly higher odds of delaying medical care due to cost (AOR: 97; CI: 1.30–3.00; p < .01, compared with cisgender urban adults. We did not find other statistically significant differences when isolating samples to rural and urban adults, respectively.
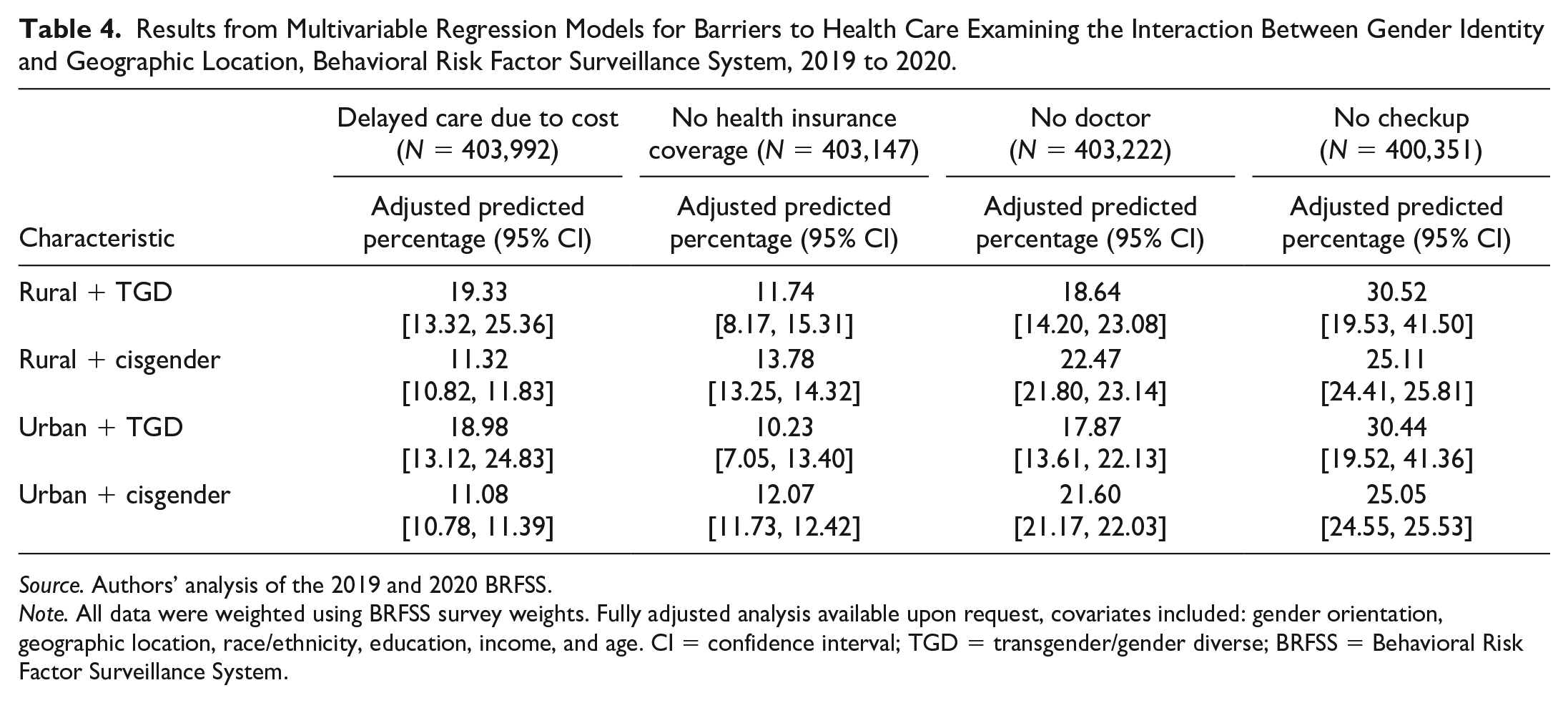
Finally, in the multivariable logistic regression model that added a variable showing the interaction between geographic location and gender identity, we found no statistically significant association between the interaction terms and the four barriers to accessing health care (Table 4). Respondents who both lived in a rural area and identified as TGD had the highest predicted probability of delaying care due to cost (19.33%, CI: 13.32–25.36) and having no checkup (30.52%, CI: 19.53–41.50), however, these differences were not significant. Despite the lack of statistical significance, the magnitudes suggest the possibility of meaningfully large differences, consistent with our stratifications.
Results from Multivariable Regression Models for Barriers to Health Care Examining the Interaction Between Gender Identity and Geographic Location, Behavioral Risk Factor Surveillance System, 2019 to 2020.
Source. Authors’ analysis of the 2019 and 2020 BRFSS.
Note. All data were weighted using BRFSS survey weights. Fully adjusted analysis available upon request, covariates included: gender orientation, geographic location, race/ethnicity, education, income, and age. CI = confidence interval; TGD = transgender/gender diverse; BRFSS = Behavioral Risk Factor Surveillance System.
Discussion
In this study, bivariate analysis of 2019 to 2020 BRFSS data reveal that rural TGD adults may face increased barriers to care compared with cisgender adults in rural and urban areas. Notably, the prevalence of delaying care due to cost was statistically significantly higher for TGD adults as compared with cisgender adults in the full sample of rural and urban respondents (24.95% vs 11.1%) the rural subsample (27.7% vs 11.6%) and the urban subsample (24.4% vs 11.0%). Admittedly, data for some health care access outcomes may not be statistically significant due to small sample sizes and wide confidence intervals.
Yet, multivariable logistic regression results reveal that TGD respondents in the full sample and rural and urban subsamples also report significantly (p < .05) higher odds of forgoing medical care due to cost. Some TGD participants may experience cost-related barriers to care if they are unable to afford gender-affirming health services like hormonal therapy or gender-affirming surgeries. Unfortunately, the BRFSS does not ask about access to gender-affirming health services, but 55% of the participants in the 2015 U.S. Transgender Survey reported being denied coverage for transition-related surgery and procedures (James et al., 2016). Without health insurance coverage, TGD people may not be able to afford gender-affirming health care. Such barriers might be heightened in rural areas, where access to care, especially specialty care, is more restricted. Accessing care may require additional travel costs, time off work, and other related expenses. Furthermore, cost-related barriers to care go beyond gender-affirming care to include all other types of health care. Our findings show that rural transgender adults have lower incomes to begin with, and such financial barriers may particularly impact them and impede health care seeking.
Cost-related barriers to care may also be indicative of limited financial resources or less comprehensive health insurance coverage for TGD adults. Across the United States, TGD adults are more likely to experience employment discrimination (Bradford et al., 2013; Kattari et al., 2016), which may systematically restrict access to well-paying jobs, financial security, and health insurance benefits. This has implications for being able to afford out-of-pocket costs associated with health care, as shown in this study, as well as for other cost-related necessities, like housing and food (Kushel et al., 2006; Russomanno & Jabson Tree, 2020). While some states have passed legislation prohibiting discrimination on the basis of gender identity, many have not (Movement Advancement Project, n.d.). Without federal anti-discrimination legislation, cost-related inequities in access to care for TGD adults may persist.
Findings from this analysis are partially influenced by small sample sizes and serve as a call for future high-quality, nationally representative surveys, such as the 2022 U.S. Trans Survey (USTS) (U.S. Trans Survey, n.d.). However, these findings also reveal that other intersecting identities and demographics, such as age, race, ethnicity, education, and income play a role in barriers to health care access (Kattari et al., 2021). Rural TGD adults are a heterogeneous group with differing health care challenges, and future research should prioritize intersectional inequities when possible. The 2022 USTS and national health surveys should oversample both rural and TGD populations to better inform targeted and community-based interventions for improving access to care for rural TGD people.
Limitations
There are several limitations that affect the generalizability of our study. Approximately, 30 states participated in gender identity data collection during the study period (Lett & Everhart, 2022). Our study may be missing states from more conservative and/or rural portions of the country where hostile attitudes against TGD populations are more prevalent. Moreover, opting to include the SOGI module may be a signal that states are more socially accepting of TGD people, which could lead to a concerted effort to remove barriers to care for TGD populations. To the extent that states included in this study have worked to address barriers to care for TGD individuals, our findings may underestimate the health care inequities that TGD individuals face in other states. Still, the states represented in this analysis are diverse in terms of region, demographics, and policy preferences.
Meanwhile, some public health researchers have raised concerns regarding the reliability of the BRFSS survey question in identifying transgender individuals that must be taken into consideration (Lett & Everhart, 2022). More research is critically needed to understand gaps in national surveillance on gender identity, but we urge the CDC to include SOGI questions on the main BRFSS questionnaire. Other nationally representative surveys on health and health care (e.g., the U.S. National Health Interview Survey) should consider adding questions on gender identity. The Center for Transgender Excellence recently recommended a two-step question:
What is your sex or current gender? (check all that apply) Male/man; female/woman, trans male/trans man, trans female/trans woman, non-binary/genderqueer, additional category, declined to state.
What sex were you assigned at birth? Male, female, decline to state (Center of Excellence for Transgender Health, 2009).
These questions account for the complexity of gender identity to a greater extent than past questions and importantly allow participants to select multiple responses. In addition, researchers have begun examining questions on gender expression that may account for differences across developmental stages (National Academies of Sciences, Engineering, and Medicine, 2020). Collecting and analyzing data on diverse gender identities and expressions is an important step in understanding and eliminating health disparities among the rural TGD population. However, the quality and accuracy of gender identity survey questions is critical to achieving this goal.
Finally, this study is subject to common limitations when using cross-sectional data from the BRFSS. All responses were self-reported, which may be subject to social desirability, recall, non-response, and interviewer (e.g., possible negative tones when asking sensitive questions) biases. This analysis does not attempt to establish causality. Finally, important subpopulations are missing from our analysis, including homeless, incarcerated, or other institutionalized populations. Previous research has noted that TGD individuals are more likely to be homeless (Deal et al., 2023), incarcerated (Herring & Widra, 2022), or institutionalized than their cisgender peers.
Public Health Implications
To improve access to care for rural TGD adults, public health policymakers and practitioners should consider multifaceted approaches. Policymakers, for instance, should address workplace and educational discrimination to improve the economic wellbeing—and access to employer-sponsored health insurance—for TGD adults. This includes passing—and enforcing—anti-discrimination policies inclusive of gender identity. Moreover, experts in rural LGBT health have recommended updating health forms and marketing materials with inclusive language and images, evaluating programs and services to ensure they are LGBT inclusive and affirming, and advocating for LGBT-inclusive community needs assessments (Movement Advancement Project, 2019a). More employers and private health insurers have removed transgender exclusions from their health plans and are now offering gender-affirming care, and more should follow suit to reduce barriers to care by gender identity (Human Rights Campaign Foundation, 2022). State-level policymakers should avoid creating barriers to life-saving medical care for transgender populations, including transgender youth and young adults (Lee & Rosenthal, 2023).
Meanwhile, medical and nursing schools should promote training to ensure that our future health care professionals are prepared to provide gender-affirming care regardless of where they practice. Relatedly, some practicing physicians continue to feel uncomfortable providing gender-affirming care despite wanting to be helpful without malice (Johnston & Shearer, 2017; Vance et al., 2015). Continuing medical education (CME) may be an option for rural providers wanting to learn more and help fill gaps in gender-affirming care in rural settings. While our study did not specifically address barriers to gender-affirming care, the more general barriers to health care—such as lacking a personal doctor or maintaining routine heath visits—for TGD individuals in this study signal a need for improvement in all areas.
Finally, state and federal governments along with private health care systems should expand health care access options in urban gender identity or transgender clinics through telehealth to link rural TGD adults with specialty care providers that may be more difficult to access in rural settings. In turn, efforts should be made to expand training for urban health care providers on gender-affirming care for people living in rural contexts. Telehealth should be coupled with expanded broadband internet to ensure that rural residents have access to internet and telehealth services.
Conclusion
Our study adds new evidence on the demographics and access to health care at the intersections of gender identity and rurality using large-scale population-based data. We find that rural TGD adults frequently report barriers to care across four commonly used dimensions of health care access. Furthermore, both rural and urban TGD adults experience significant cost-related barriers to medical care. Rural populations have too often been mischaracterized as homogeneous. However, this study sheds new light on the gender diversity of rural populations and the critical need for further research and resources to ensure that rural TGD adults receive needed care. Improving access to care—and, ultimately, health—at the intersection of geographic location and gender identity requires attention to structural factors, such as access to health insurance and financial resources as well as non-discrimination in policy and practice.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Federal Office of Rural Health Policy (FORHP), Health Resources and Services Administration (HRSA), US Department of Health and Human Services (HHS) under PHS Cooperative Agreement No. 5U1CRH03717. This research was also supported by the NIH National Center for Advancing Translational Sciences, grant UL1TR002494.