
Abstract
Individuals who have HIV who also use drugs experience increased age-matched morbidity and mortality in comparison with those with HIV who do not use drugs. A systematic review was conducted to describe models of integrated HIV and opioid use disorder (OUD) services, enablers of and barriers to integrated service access, and the coordinated systems and tools at the state and service delivery levels required for implementation. Database searches yielded 235 candidate articles, of which 22 studies met the inclusion criteria. Analysis found that integrated programs operated with minimal coordinated policy and systems guidance at the state level. Service delivery systems and tools used for integration, including use of integrated protocols, risk assessment tools, case management tools, and referral systems, were similar across integration models. Concerted efforts to coordinate state-level systems and develop supportive policies, guidelines, and standardized tools may facilitate integration at the service delivery level.
Introduction
Opioid use and overdose rates are on the rise. Recent data from the Centers for Disease Control and Prevention (CDC) report that there were greater than 92,000 deaths from opioid overdose in 2020, up from 71,000 deaths from opioid overdose reported in 2019 (CDC, 2021). More than 10,250,000 Americans age 12 and above reported opioid misuse and approximately 47,000 died from an opioid overdose in 2018 (CDC, 2019). The connection between opioid use disorder (OUD) and HIV infection has been well established. It is estimated that 25% to 90% of people with HIV experience chronic pain, with 21% to 53% receiving opioid prescriptions and more often at higher doses than their HIV-negative counterparts (Dobalian et al., 2004; Edelman et al., 2013; Frich & Borgbjerg, 2000; Tsao et al., 2007). Opioid addiction also increases vulnerability to HIV infection via sharing syringes and other drug equipment, which has contributed to HIV outbreaks, including a highly publicized one in Scott, Indiana, from 2011 to 2015 (Conrad et al., 2015; Mateu-Gelabert et al., 2020). Injection drug use is the third-leading cause of HIV transmission in the United States, contributing to the estimated 1.2 million individuals ages 13 and above who have HIV, among whom nearly 3,900 new cases in 2018 were linked to injection drug use (CDC, 2018). People with HIV who use drugs, including opioids, experience increased age-matched morbidity and mortality in comparison with those who do not use drugs (Altice et al., 2010). Concerted efforts are required to prevent HIV among people who use opioids, and the risk of opioid misuse and overdose among people with HIV (CDC, 2019).
Despite the increasing prevalence of OUD and the proven efficacy of medications for addiction treatment (MAT), rigorously collected national estimates on the number of individuals who receive medication for OUD are not available (National Academies of Sciences Engineering and Medicine, 2019), although it is broadly understood that OUD treatment access rates are low (CDC, 2020). Studies conducted among people who use drugs identify mistrust of providers, fear of mistreatment, and feeling stigmatized, judged, and devalued by providers as key barriers to accessing treatment (Deren et al., 2017).
Comparatively, using CDC definitions, HIV care continuum data from 2018 demonstrate that 86% of individuals had diagnosed HIV; 65% received some form of care; 50% were retained in care; and 56% were virally suppressed (CDC, 2018). Studies show that people who inject drugs experience worse outcomes at each point along the HIV care continuum, including lower testing rates and delayed entry to care and treatment (Altice et al., 2010; CDC, 2018; Conrad et al., 2015; Mateu-Gelabert et al., 2020). In contrast, studies also show that people with HIV who are prescribed MAT are more likely to access HIV services, adhere to their HIV medication regimen, and achieve viral suppression, demonstrating the potential contribution of HIV and OUD service integration to control the HIV epidemic (Karki et al., 2016; Low et al., 2016).
Previous systematic reviews have focused on describing models of HIV and OUD integration and associated outcomes. Oldfield and colleagues (2019b) described programmatic outcomes of integrated buprenorphine/naloxone services in HIV clinics and found increased antiretroviral treatment (ART) initiation, decreased drug use equipment sharing, and decreased opioid use. OUD treatment settings that integrate HIV testing and counseling were found to have increased HIV testing rates. A systematic review by Rich and colleagues described models of integrated HIV, hepatitis C virus (HCV), and OUD care wherein integrated models were found within HIV specialty care, primary care, opioid treatment programs (OTPs), transitional clinics (for recently incarcerated individuals), and a community-based harm reduction program. Findings indicated that integration of OUD, HIV, and HCV within primary care services optimized access and retention in services (Rich et al., 2018).
New Contributions
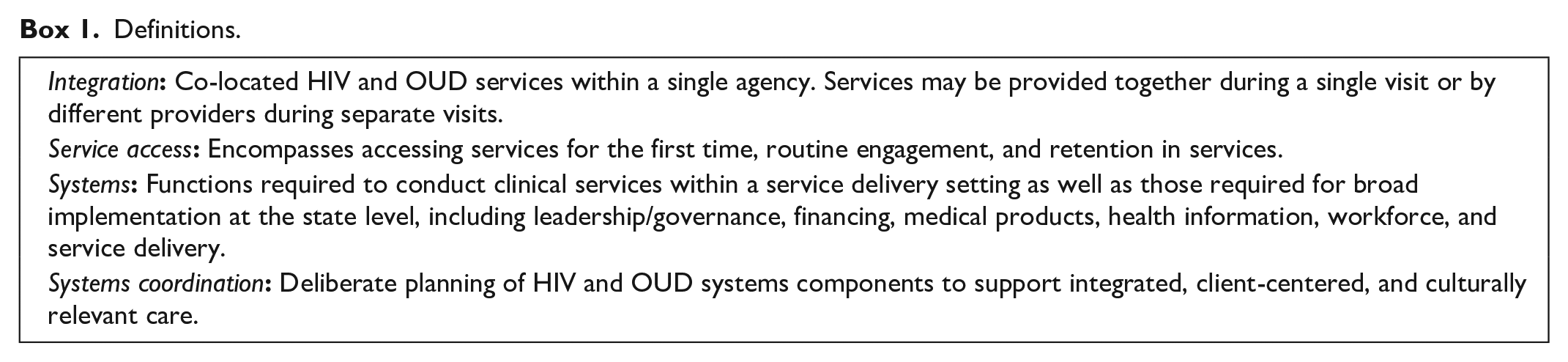
Our project, Strengthening Systems of Care for People with HIV and Opioid Use Disorder, is working to strengthen and leverage coordinated HIV and OUD systems of care (Box 1) across nine states. The project’s ultimate aim is sustained systems coordination and increased availability of integrated HIV and OUD services to ensure that people with HIV and OUD have access to care, treatment, and recovery services that are client-centered and culturally responsive. While previous reviews have focused on describing integrated models and their outcomes, none has sought to understand the systems coordination aspects required for implementation, which can provide important information for implementers designing integrated programs. To fill this gap and inform our project’s efforts at the state level, this systematic review describes enablers of and barriers to integrated OUD and HIV service access, models of co-located integrated HIV and OUD services, and the associated coordinated systems and tools at the state and service delivery levels used for their implementation.
Definitions.
Conceptual Framework
We employed the Health Systems Framework wherein each levels of the health system—the individual client, the care team of health providers, the organization or service delivery setting, and the larger political and economic environment—are all interconnected (Figure 1; “Building a Better Delivery System: A New Engineering/Health Care Partnership,” 2005). At the individual level, we identified information on enablers and barriers to integrated service access for clients. At the care team level, we similarly identified information on enablers and barriers to providing integrated service access for clients. At the organization or service delivery level, we identified systems and tools that support integrated service access. At the policy level, we examined systems and tools that facilitate integrated service provision across the broader state and/or at the organization level.
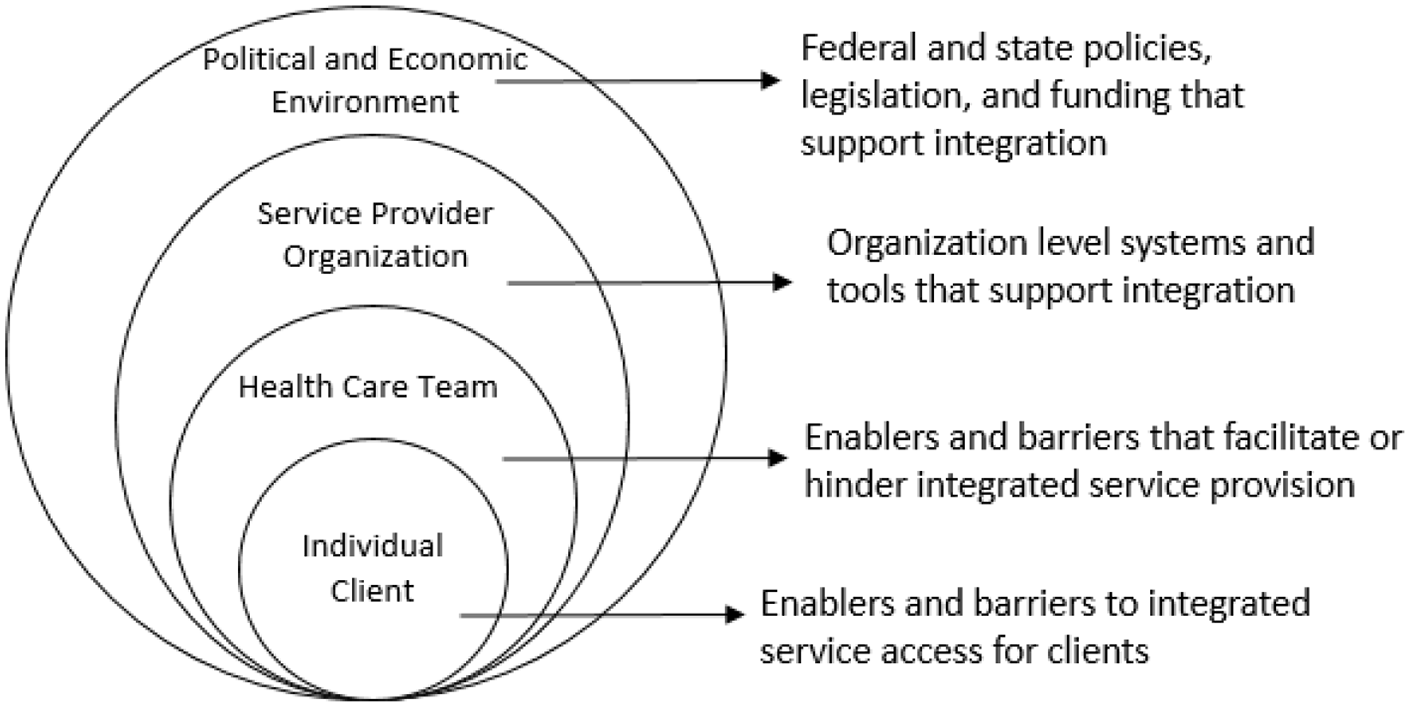
Conceptual Framework to Influence HIV/OUD Clinical Care Coordination.
Method
We followed the PRISMA standards of quality for reporting systematic reviews (Moher et al., 2009). We developed a study protocol that outlined the systematic review process, identified study team member’s roles, and clearly defined eligibility criteria for articles included in this study. This study was not considered human subjects research and was exempted by the JSI Institutional Review Board.
Search Strategies
The study team conducted an electronic database search including PubMed and CINAHL using the medical subject heading (MeSH) and title and abstract terms related to integrated care combined with (AND) HIV, combined with terms (AND) related to OUD, including buprenorphine, MAT, heroin, methadone, mental health, and behavioral health or the equivalent MeSH terms provided in the databases. Duplicates were removed automatically using a filter during the initial search. A systematic review process was employed, wherein two study team members independently reviewed titles and abstracts to determine inclusion eligibility. When there was a disagreement, a third study team member made the final decision (inter-rater reliability 82%). Full-text articles of included abstracts were then independently reviewed by two study team members to make final determinations of inclusion eligibility. Again, when there was a disagreement, a third study team member made the final determination on inclusion (inter-rater reliability 75%).
We used the PICOS framework of person, intervention, comparison, outcome, study design to determine inclusion. Articles were included if they were published between January 2016 and March 2021 and were published in English. We selected these dates to increase our understanding of the models of integration reflective of current policies and practices. Articles were also included with study subjects of any age, race/ethnicity, and genders (person). Articles in the United States or Canada were included as they were most relevant to inform our Health Resources and Services Administration (HRSA) cooperative agreement, and some studies included a mix of study locations in both countries. Articles also were included if they provided information on HIV and OUD integration where services were co-located in a single setting or on barriers to or enablers of integrated HIV or OUD services and the associated systems and tools required (intervention); or compared different integrated models (comparison). Integrated service models were included if they covered inpatient settings (hospitals, treatment facilities), outpatient settings (community health clinics, outpatient treatment facilities, drop-in-centers, outreach, etc.), and supported service agencies that provide medical case management (e.g., Ryan White HIV/AIDS Program [RWHAP] service providers). Services could include any HIV or OUD service including prevention, screening/testing, treatment, and harm reduction. While the main outcome of interest was identification of systems and tools associated with integrated HIV (including prevention, care, and treatment) and OUD services, other outcomes included enablers of and barriers to integrated service access, HIV testing, HIV treatment initiation and adherence, viral load suppression, OUD treatment initiation, and client retention. Any study design was acceptable, with the exception of study protocols and reviews, wherein we searched the reference lists for further articles. We also searched the reference lists of each included article to identify and review articles that may have been missed in the initial search.
Study Quality Assessment Rating
The methodological quality of the included studies with quantitative components was scored using the Effective Public Health Practice Project (EPHPP, 2010) quality assessment tool wherein randomized and clinical controlled trials were of strong quality; quality cohort analytic, case control, cohort design, or interrupted time series were of moderate quality; and studies that used any other method or did not report the method were of weak quality. Using the EPHPP criteria, we adjusted the initial rating related to selection bias, study design, confounders, blinding, data collection, and dropouts. According to EPHPP criteria, studies that had no weak ratings received an overall “strong” score, studies with only one weak rating received an overall “moderate” score, and studies with two or greater weak ratings received an overall “weak” score. We scored the methodological quality of qualitative studies using the Critical Appraisal Skills Programme (CASP) Qualitative Studies checklist, which uses a series of 10 questions to examine the quality of the qualitative studies.
Data Extraction and Integration
A realist synthesis framework was applied wherein the study team defined the scope of the review, examined the evidence base, and extracted data using a data extraction table, which was pre-tested and refined prior use to provide a framework for synthesis (Rycroft-Malone et al., 2012) which informed the narrative. The data extraction table included elements for study design, study description, setting, study population, as well as the broad themes of enablers/barriers to service access, integration strategies, associated systems and tools, human resources required, and associated outcomes. Included studies underwent a detailed process of examination to extract the relevant data for each theme. A comparison of characteristics for data elements within the themes across the studies facilitated groupings, which we synthesized and integrated into the results. Data extraction and integration occurred concurrently with the quality assessment rating, and all data were independently verified by an additional study team member.
Results
Overview of Studies
Sixty-six studies met the criteria for a full-text review (Figure 2). Of these, 22 were identified for inclusion covering both the United States and Canada (Table 1). The studies encompassed 46,756 individuals including HIV and OUD clients, buprenorphine-waivered providers and other clinicians, health officials, policy makers, and agency leaders who may represent overlapping participants across the studies. Eighteen studies provided descriptions of integrated HIV and OUD services, two studies provided a theoretical description to assess acceptability of an integrated model, one formative research study examined how health information technology can be used to address substance use among people with HIV, and one modeling study provided a theoretical description to determine cost-effectiveness. Twenty-one studies provided information on enablers of and barriers to integrated service provision, and all studies provided some description of required systems, tools, or human resources required for implementation. Program models were broken into two categories: OUD Service Integration with HIV Service Components (n = 12) and HIV Service Integration with OUD Service Components (n = 10).
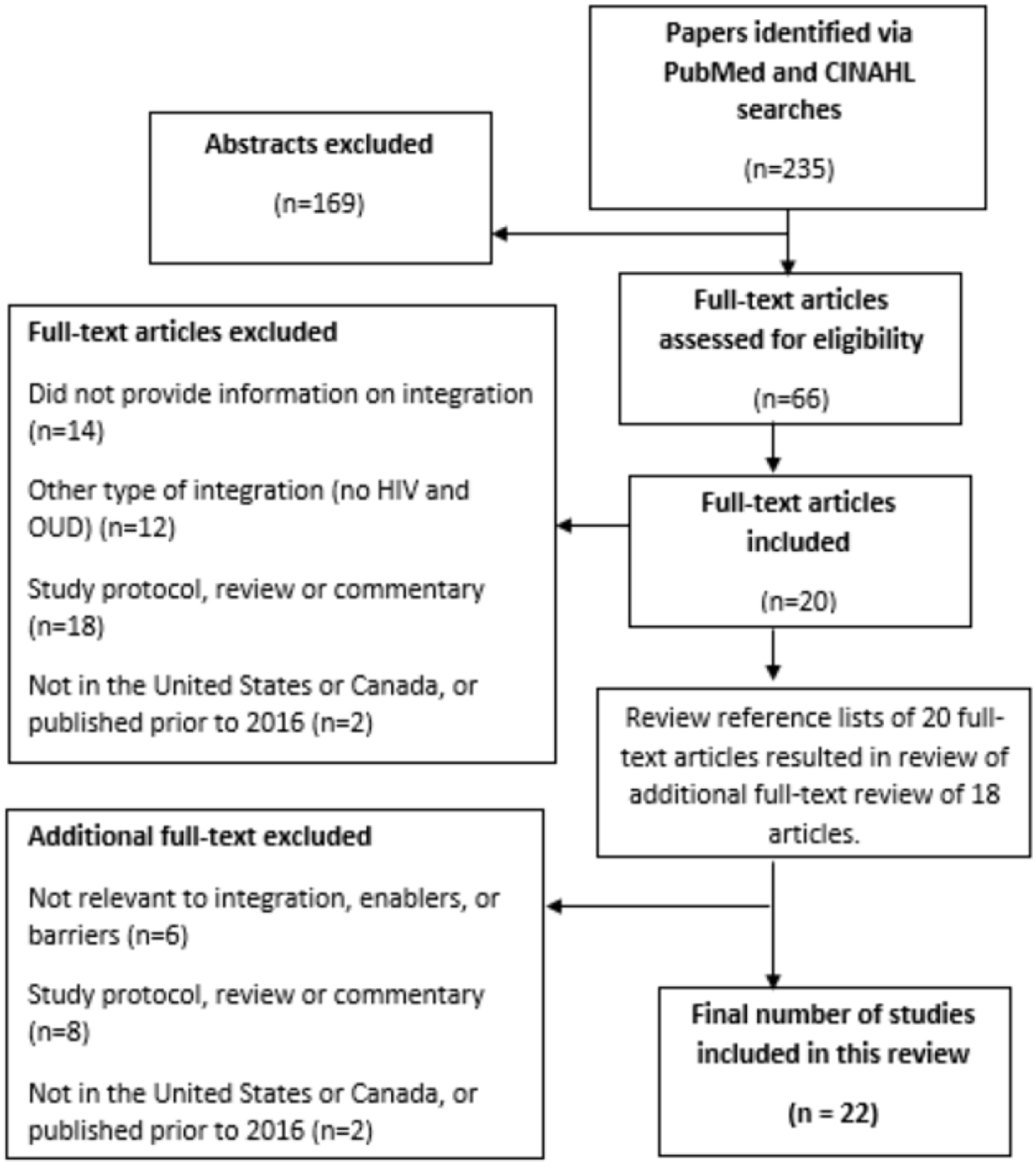
PRISMA Flowchart of Study Selection.
Summary of Integrated HIV and OUD Programs From Included Studies.
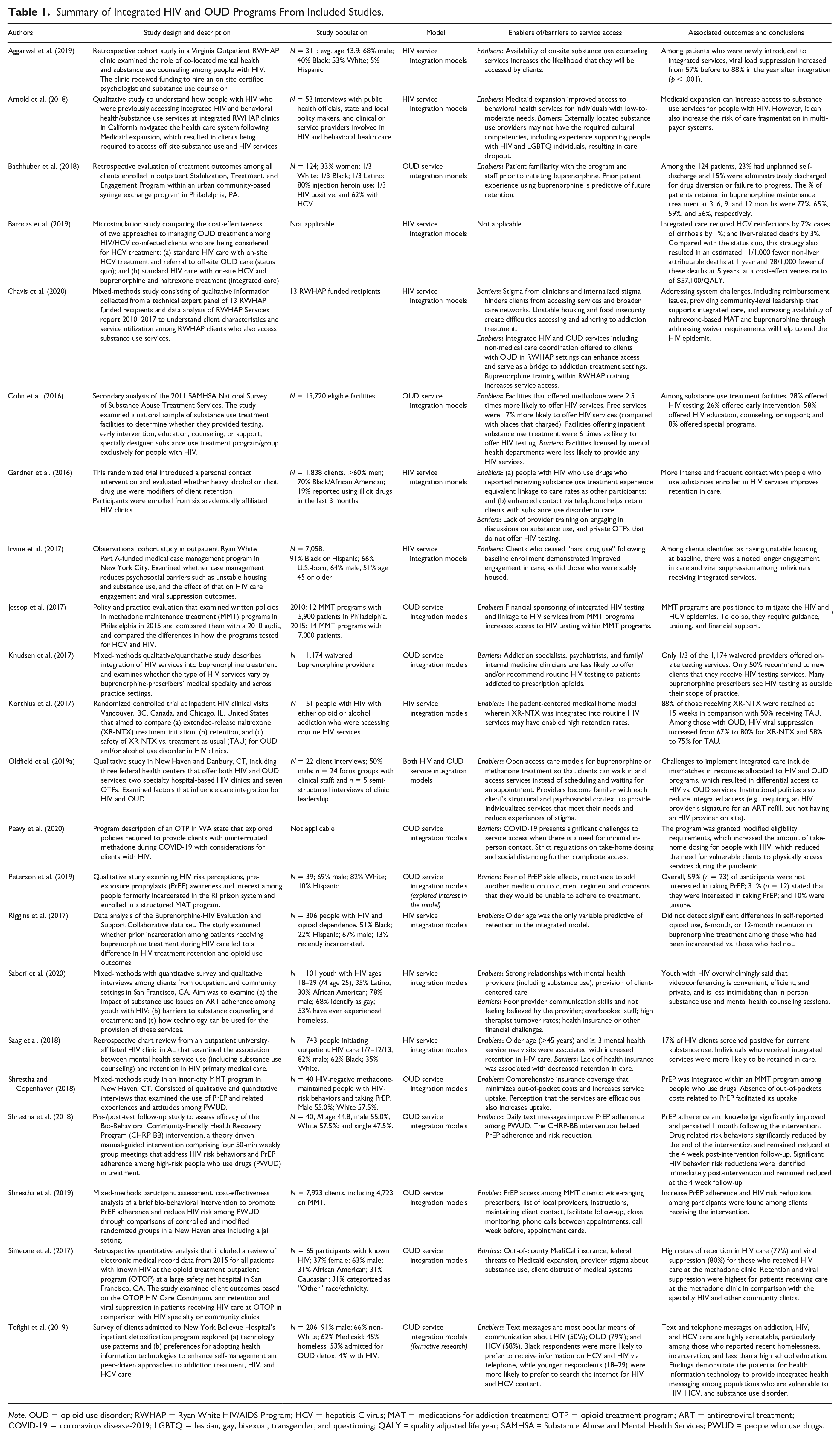
Note. OUD = opioid use disorder; RWHAP = Ryan White HIV/AIDS Program; HCV = hepatitis C virus; MAT = medications for addiction treatment; OTP = opioid treatment program; ART = antiretroviral treatment; COVID-19 = coronavirus disease-2019; LGBTQ = lesbian, gay, bisexual, transgender, and questioning; QALY = quality adjusted life year; SAMHSA = Substance Abuse and Mental Health Services; PWUD = people who use drugs.
HIV and OUD Integrated Program Models
Two general models of integration were identified: OUD Service Integration with HIV Service Components and HIV Service Integration with OUD Service Components. There was wide variation in the types of services that were integrated within each of the models. For both models, we identified three sub-categories of integration: (a) comprehensive integration, which included a vast range of HIV and OUD services; (b) simple integration, which included standard HIV or OUD care as the entry point with only one service integrated into it (e.g., HIV testing integrated into MAT services or OUD screening integrated into HIV services); and (c) theoretical integration or formative research in which potential models of integration were explored via client acceptability and modeling studies. These sub-categories are described below.
OUD Service Integration With HIV Service Components
Comprehensive Integration
Two studies described comprehensive programs. In Philadelphia, a program described the entry point of comprehensive harm reduction and OUD treatment services, including syringe distribution and exchange, overdose education, naloxone distribution, and buprenorphine maintenance treatment. The program integrated HIV testing and referral to HIV treatment. A second comprehensive San Francisco methadone maintenance treatment (MMT) program integrated opt-out HIV screening, HIV primary care, and psychiatric services. Clients enrolled in this program could select HIV services that were co-located, at a nearby clinic, or anywhere else in the city (Simeone et al., 2017).
Simple Integration
Other OUD treatment programs with integrated HIV services that were limited in scope included recruiting participants from an urban comprehensive MMT program to deliver weekly group meetings and text messages for clients to reduce sex and drug use behaviors that increase HIV risk and to enhance PrEP adherence. The program sought to overcome challenges associated with neurocognitive impairment, which is common among people who use drugs and contributes to poor treatment adherence (Shrestha et al., 2019). Three other studies described integration of HIV prevention (including risk assessment, education, and testing) into OTPs (Jessop et al., 2017; Knudsen et al., 2017; Peavy et al., 2020). Another study surveyed 13,000 substance use treatment facilities to identify models of HIV integration. The study described different types of HIV services that were integrated into substance use treatment programs: HIV testing; early intervention services; and education, counseling, or support. The study found that substance use treatment programs that provided MMT, were inpatient, or provided services free-of-charge were more likely to integrate at least one type of HIV service (Cohn et al., 2016).
Theoretical Integration
Two studies explored potential interest of clients seeking OUD treatment to engage in integrated HIV services: integrating PrEP into a prison MAT program and the potential of health information technology to optimize HIV treatment for clients enrolled in an inpatient detoxification program (Peterson et al., 2019; Tofighi et al., 2019). Client acceptability of PrEP integration into MMT was also examined within the program described above (Shrestha & Copenhaver, 2018; Shrestha et al., 2019).
HIV Service Integration With OUD Service Components
Comprehensive Integration
A randomized pilot trial at two large HIV primary care facilities integrated extended-release naltrexone into HIV services among clients with diagnosed OUD and alcohol use disorder and referred clients to external counseling sessions (Korthius et al., 2017). Another randomized trial in six HIV clinics examined differences in effectiveness of an enhanced contact intervention among a control group and a group that screened positive for potential anxiety and/or depression or harmful alcohol or substance use. Enrolled clients with HIV received integrated mental health and alcohol and substance use screens via audio computer-assisted self-interviews. Study findings indicated that participants who were at high risk for mental health disorder or alcohol and substance use were less likely to be available for telephone follow-up for the intervention, rendering the enhanced contact intervention ineffective. However, for those high-risk clients who were available for enhanced contact, the intervention was effective (Gardner et al., 2016).
Simple Integration
Programs that integrated one aspect of substance use into HIV services include a RWHAP Part A medical case management program that established a medical home model for people with newly diagnosed HIV or with retention challenges to enhance engagement in care. The model included outreach, case management with active links to substance use, mental health care, and psychosocial services as well as patient navigation to assist them in attending appointments (Irvine et al., 2017). Another study integrated buprenorphine treatment in 10 HIV treatment settings using three different approaches: Each HIV clinician was trained to prescribe buprenorphine; a few HIV clinicians in each practice were trained to prescribe buprenorphine to all clients in need, or separate HIV and buprenorphine specialists providing services at the same location (Riggins et al., 2017). A study examining retention in care examined outcomes from a model that included HIV clinical care and mental health care (including co-located substance use assessments and counseling). Two studies described integrating RWHAP clinical services with on-site substance use counseling and referrals and case management to enhance linkages to external services such as OUD treatment (Aggarwal et al., 2019; Arnold et al., 2018).
Theoretical Integration
A formative research study examined how health information technology can be used to address substance use among people with HIV, including tele-health and video conferencing as well as social media to build online support communities (Saberi et al., 2020). Finally, a cost-effectiveness study simulated two different scenarios of HIV and OUD integration: standard HIV care with referral to off-site OUD services or standard HIV with co-located buprenorphine treatment (Barocas et al., 2019).
Enablers to Integrated Service Access
Enablers were not unique to model type, and most themes were identified across both models. Five broad themes enabled integrated service access.
Provider Knowledge and Skills
Enablers of service access included provider familiarity and understanding of the client’s psychosocial context so the provider can administer effective client-centered care and build a trusting relationship. Providers who were trained to help clients overcome barriers to entering care and who demonstrated empathy were also cited as enablers of initiating and maintaining service engagement (Saberi et al., 2020). Training RWHAP providers to prescribe buprenorphine was also noted as an important opportunity to increase integrated service access (Chavis et al., 2020).
Client Characteristics and Experiences
Older age, patient familiarity with staff, and experience accessing services within a facility increased client access to and retention in services. Stable housing and abstinence from drug use also increased HIV and OUD service access (Bachhuber et al., 2018; Chavis et al., 2020; Irvine et al., 2017; Riggins et al., 2017; Saag et al., 2018).
Care Engagement Between Appointments
Between-appointment text messages on adherence and appointment reminders facilitated continued client engagement and increased knowledge and information sharing between clients and providers. Increased PrEP uptake was also noted among clients on methadone when they received clear information on where they could access PrEP providers, and when they received frequent communication, including phone calls, from a provider to enhance adherence and keep them engaged in care (Gardner et al., 2016; Shrestha et al., 2018, 2019; Tofighi et al., 2019).
Convenience
Clients were more likely to access services when they were co-located within the same building. Open-access models that did not require an appointment and allowed clients to walk in whenever it was convenient also facilitated service access. On-site HIV testing at MMT facilities enabled HIV service access via referrals (Gardner et al., 2016; Jessop et al., 2017; Oldfield et al., 2019a; Shrestha et al., 2019).
Insurance
Insurance coverage that minimized out-of-pocket costs increased service access. State Medicaid expansion enhanced the number of people eligible for substance use services (Arnold et al., 2018; Korthius et al., 2017).
Barriers to Service Access
Three broad themes were identified related to barriers to service access.
Client Fear and Distrust
Fear associated with PrEP side effects or potential consequences of adding PrEP to an existing regimen reduced likelihood of service uptake. A history of mistrust of the medical system impeded client engagement in care (Peterson et al., 2019).
Provider Knowledge and Attitudes
A lack of cultural competencies in working with individuals who are LGBTIQ+ (lesbian, gay, bisexual, transgender, intersex, and questioning) reduced likelihood of client’s accessing services. Anticipated stigma from providers and providers who were perceived as having inadequate HIV and/or OUD services training further hindered client care engagement (Arnold et al., 2018; Chavis et al., 2020; Knudsen et al., 2017; Saberi et al., 2020).
Systems Challenges
Insurance billing, reimbursement challenges, and out-of-pocket costs reduced service access (Arnold et al., 2018; Cohn et al., 2016; Gardner et al., 2016; Saag et al., 2018; Simeone et al., 2017). One study conducted early in the coronavirus disease-2019 (COVID-19) pandemic found that regulations that required case-by-case decisions on take-home dosing of methadone for clients with HIV created further challenges to continued engagement in services, due to their clinical vulnerability (Peavy et al., 2020).
Organizational Processes and Protocols at the Service-Delivery Level
Overall, systems and tools required to implement the integrated models were similar across both types, with a few exceptions (Table 2). A comprehensive program under the OUD Service Integration model described the training systems required to orient staff to basic OUD treatment specifications (e.g., mechanisms of action, side effects, and drug interactions), as well as the requirements and expectations for staff and clients within the integrated model (Bachhuber et al., 2018). Also unique to the OUD Service Integration model was quality of care assessment tools which were adapted to integrate measurement of HIV care provision (Simeone et al., 2017), as well as specific HIV testing protocols and supplies (Knudsen et al., 2017; Simeone et al., 2017). Systems and tools unique to the HIV Service Integration models included setting aside non-clinical space within the HIV facility for private OUD counseling (Aggarwal et al., 2019); developing OUD acuity assessments to determine payer responsibility within a multi-payer system (Arnold et al., 2018); introducing PrEP screening forms and adherence assessments (Shrestha et al., 2018); and introducing buprenorphine prescribing protocols for HIV providers (Riggins et al., 2017).
Systems Components Used Within the Integrated Models.
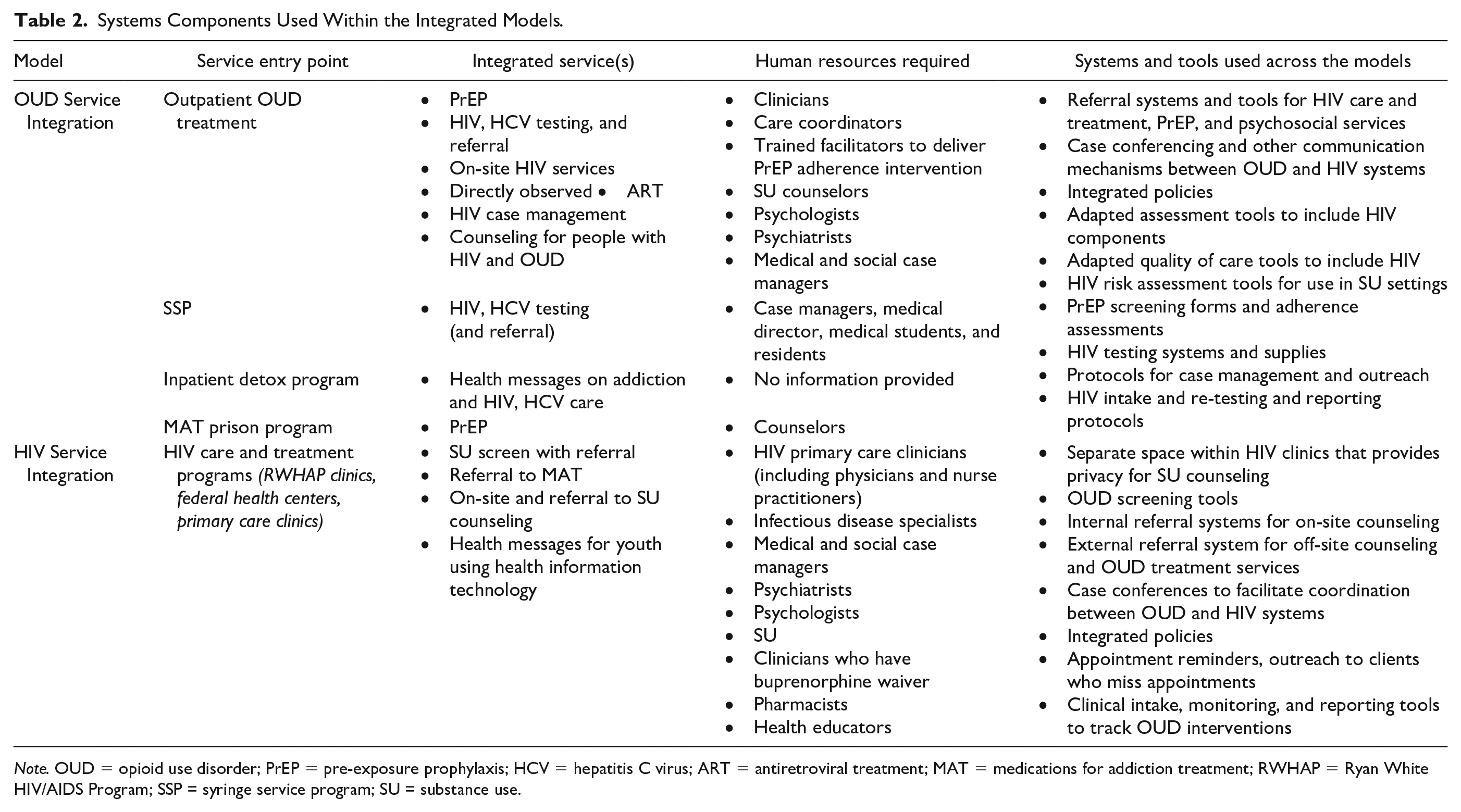
Note. OUD = opioid use disorder; PrEP = pre-exposure prophylaxis; HCV = hepatitis C virus; ART = antiretroviral treatment; MAT = medications for addiction treatment; RWHAP = Ryan White HIV/AIDS Program; SSP = syringe service program; SU = substance use.
Across both model types, referral and linkage systems and associated tools were described wherein clients were able to access an array of HIV care and treatment, PrEP, OUD counseling and treatment services, and other psychosocial services that were available either on-site, at adjacent sites, or at separate facilities (Aggarwal et al., 2019; Irvine et al., 2017; Saag et al., 2018). Both model types referred to developing integrated referral systems to ensure that clients were able to move between services effectively (Aggarwal et al., 2019; Irvine et al., 2017; Oldfield et al., 2019a). Both models also introduced integrated risk assessment tools to identify clients with HIV who may require OUD treatment, and to identify clients with OUD who may be at risk for HIV (Gardner et al., 2016; Irvine et al., 2017; Oldfield et al., 2019a; Shrestha et al., 2018, 2019). Both models developed intake, clinical monitoring, and reporting tools for clients accessing HIV and/or OUD services (Gardner et al., 2016; Jessop et al., 2017). Additional tools required to implement both models included protocols for case management and outreach; case conferencing systems (Irvine et al., 2017; Riggins et al., 2017); and integrated policies to provide an overall supportive framework (Aggarwal et al., 2019; Jessop et al., 2017; Peavy et al., 2020).
A range of human resources were required to implement programs within each model type, with a significant amount of overlap between the models. For OUD Service Integration models, when the entry point was a syringe exchange program, the human resources required included a case manager to coordinate the entire integrated approach, and additional case managers to provide patient education and counseling. A medical director provided clinical oversight to medical residents and postgraduate trainees to implement the integrated program (Bachhuber et al., 2018). Another OUD Service Integration program, wherein outpatient OUD treatment was the entry point, integrated HIV risk counseling and PrEP adherence-trained graduate-level facilitators delivered the intervention in person and followed up with clients between sessions via adherence reminder text messages (Shrestha & Copenhaver, 2018; Shrestha et al., 2018). A similar intervention was also implemented within the New Haven MAT prison program and five surrounding MAT facilities (Shrestha et al., 2019). The Opioid Outpatient Treatment program (in which outpatient methadone treatment was the service entry point that provides integrated HIV testing and treatment) uses primary care clinicians, psychiatrists, and medical and social case managers to deliver comprehensive services (Simeone et al., 2017).
An HIV Service Integration program provided substance use counseling at a RWHAP clinic that used HIV clinicians to link clients to substance use counselors on-site (Saag et al., 2018). A microsimulation study examined the cost of HIV primary care clinicians and infectious disease specialists providing integrated buprenorphine and methadone (Barocas et al., 2019). Two additional studies examined the efficacy of employing psychiatrists, psychologists, and substance use counselors within HIV primary care to identify changes in clinical outcomes and retention in care (Aggarwal et al., 2019; Saag et al., 2018). A study that examined integration of buprenorphine into HIV clinical services in seven different facilities either trained HIV clinicians to prescribe buprenorphine or collaborated with buprenorphine-waivered clinicians to provide coverage within HIV clinics. In this same study, nurse practitioners, substance use counselors, health educators, and pharmacists also acted as care coordinators to help clients move between HIV clinical care and substance use counseling (Riggins et al., 2017). Another study trained HIV clinicians to inject naltrexone during HIV clinical visits (Korthius et al., 2017). A study that included both models, where entry points included both HIV and OUD services, described collaborating with clinicians and care coordinators to examine the quality of integrated care (Oldfield et al., 2019a).
Associated Systems and Tools at the State Level
There was no evidence of coordinated systems and tools at state levels that assisted in the implementation of integrated service delivery models.
Quality Appraisal
Appraisal of the studies with quantitative method (Table 3) components demonstrated that one received a strong quality rating; seven a moderate quality rating; and 10 a weak quality rating. Weak components included selection bias (Knudsen et al., 2017; Shrestha et al., 2018), research design (Bachhuber et al., 2018; Chavis et al., 2020; Cohn et al., 2016; Jessop et al., 2017; Knudsen et al., 2017; Saag et al., 2018; Saberi et al., 2020; Shrestha & Copenhaver, 2018; Simeone et al., 2017; Tofighi et al., 2019), confounders (Bachhuber et al., 2018; Barocas et al., 2019; Korthius et al., 2017; Shrestha & Copenhaver, 2018; Tofighi et al., 2019), blinding (Aggarwal et al., 2019; Barocas et al., 2019; Chavis et al., 2020; Cohn et al., 2016; Jessop et al., 2017; Knudsen et al., 2017; Korthius et al., 2017; Saberi et al., 2020), data collection (Chavis et al., 2020; Cohn et al., 2016; Jessop et al., 2017; Knudsen et al., 2017; Korthius et al., 2017; Riggins et al., 2017; Saberi et al., 2020; Tofighi et al., 2019), and dropouts (Gardner et al., 2016; Irvine et al., 2017). Appraisal of the studies with qualitative method (Table 4) components demonstrated that all three qualitative studies’ results were valid (Arnold et al., 2018; Oldfield et al., 2019a; Peterson et al., 2019).
EPHPP Quality Assessments for Quantitative Studies
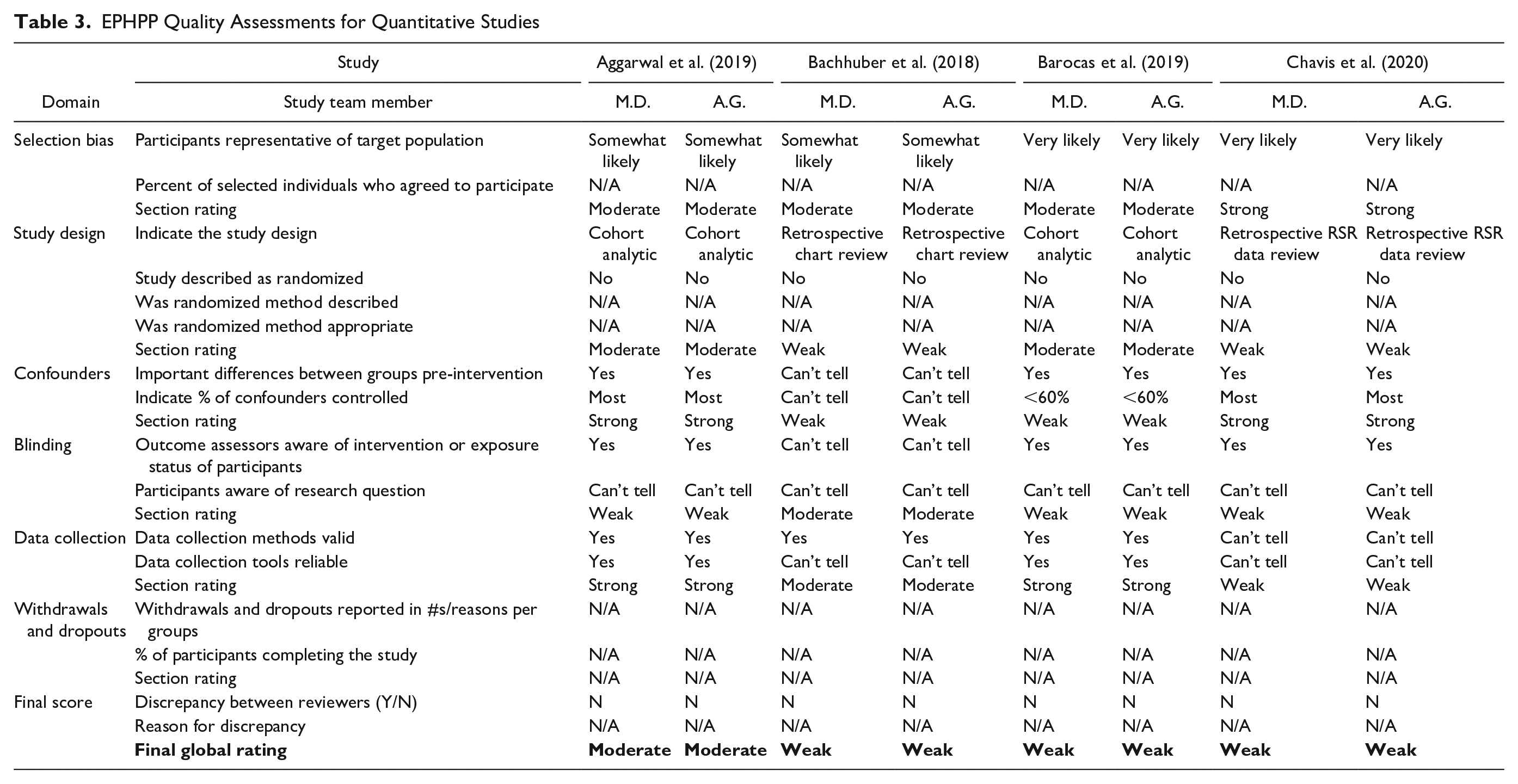
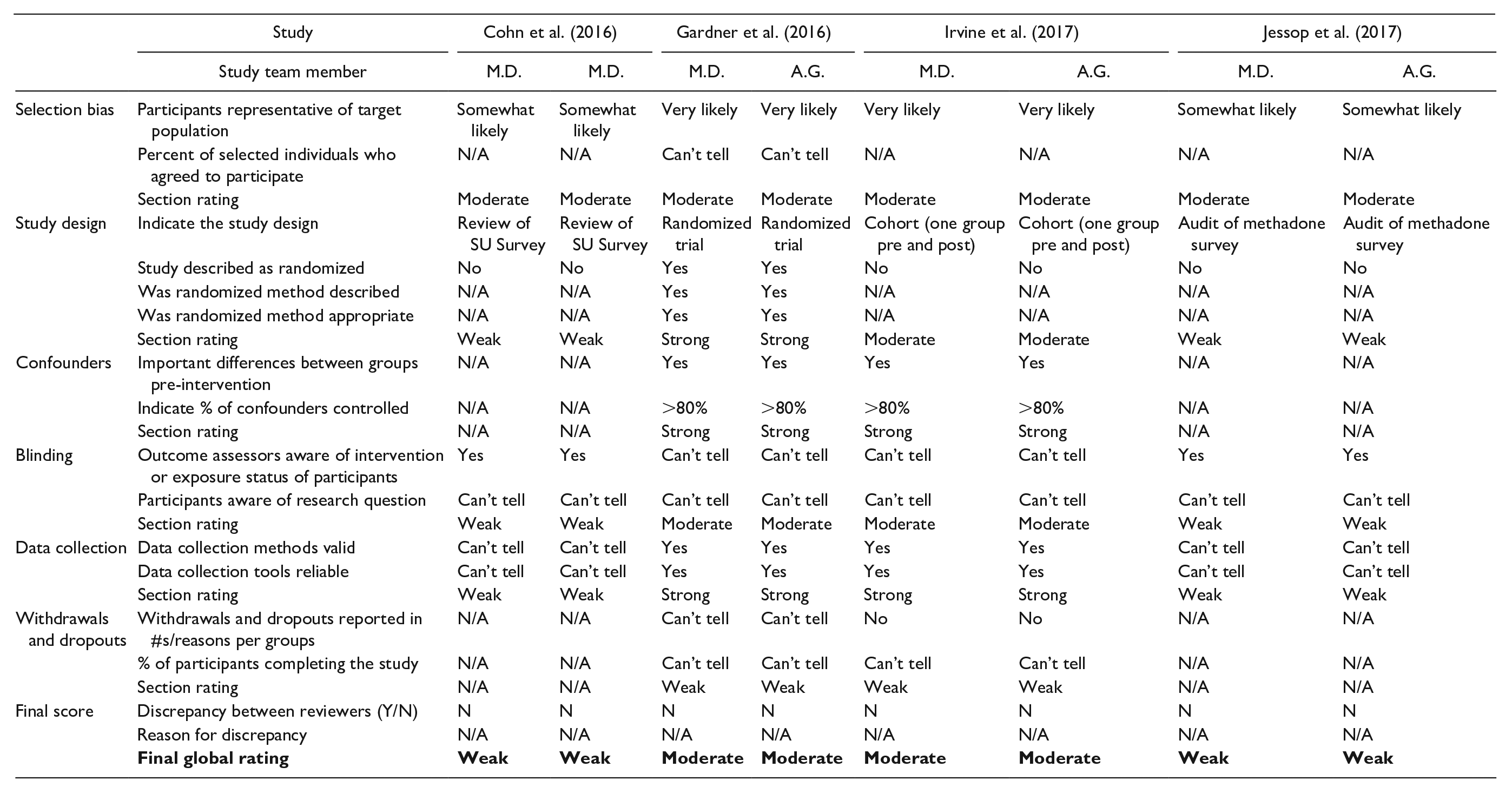
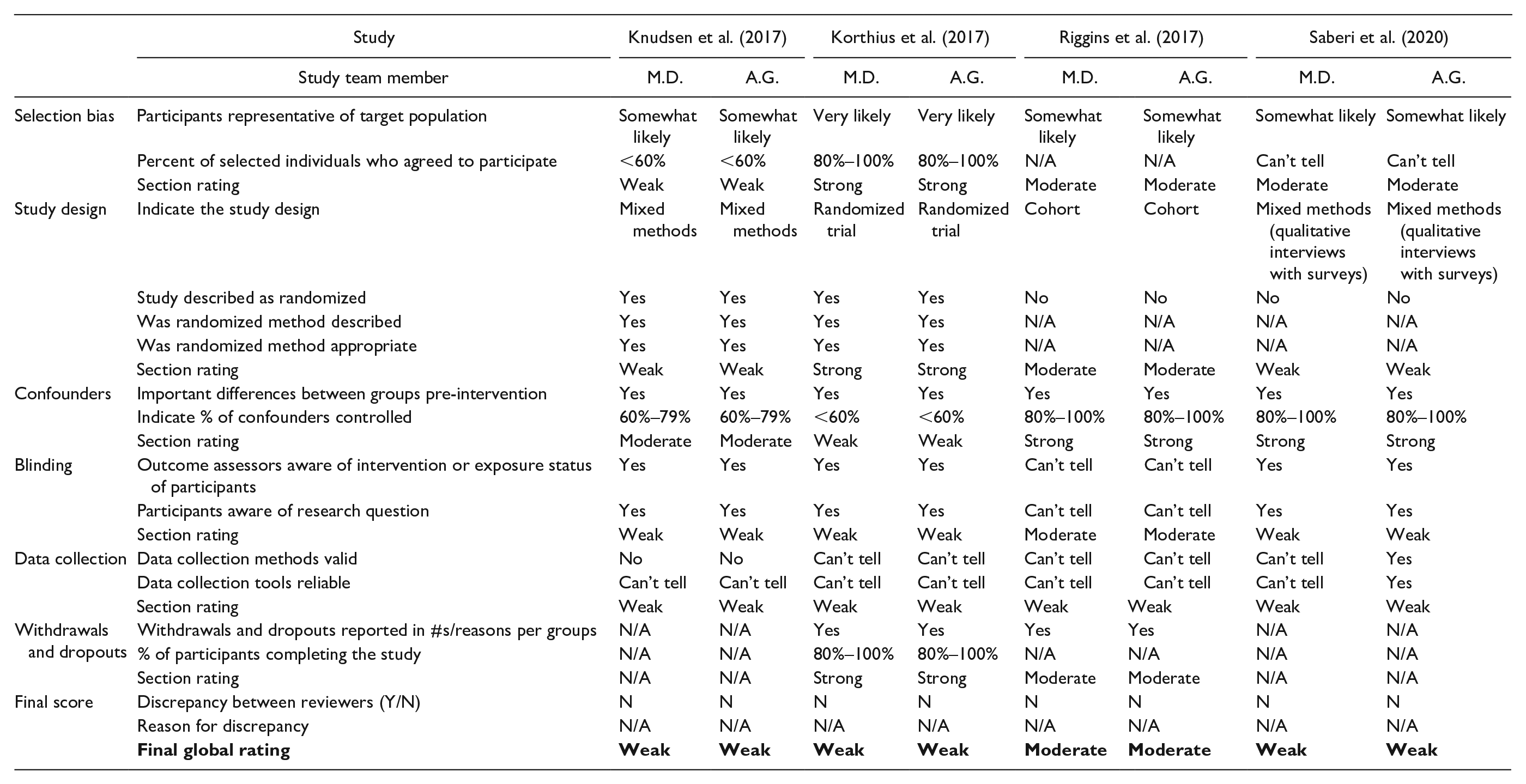
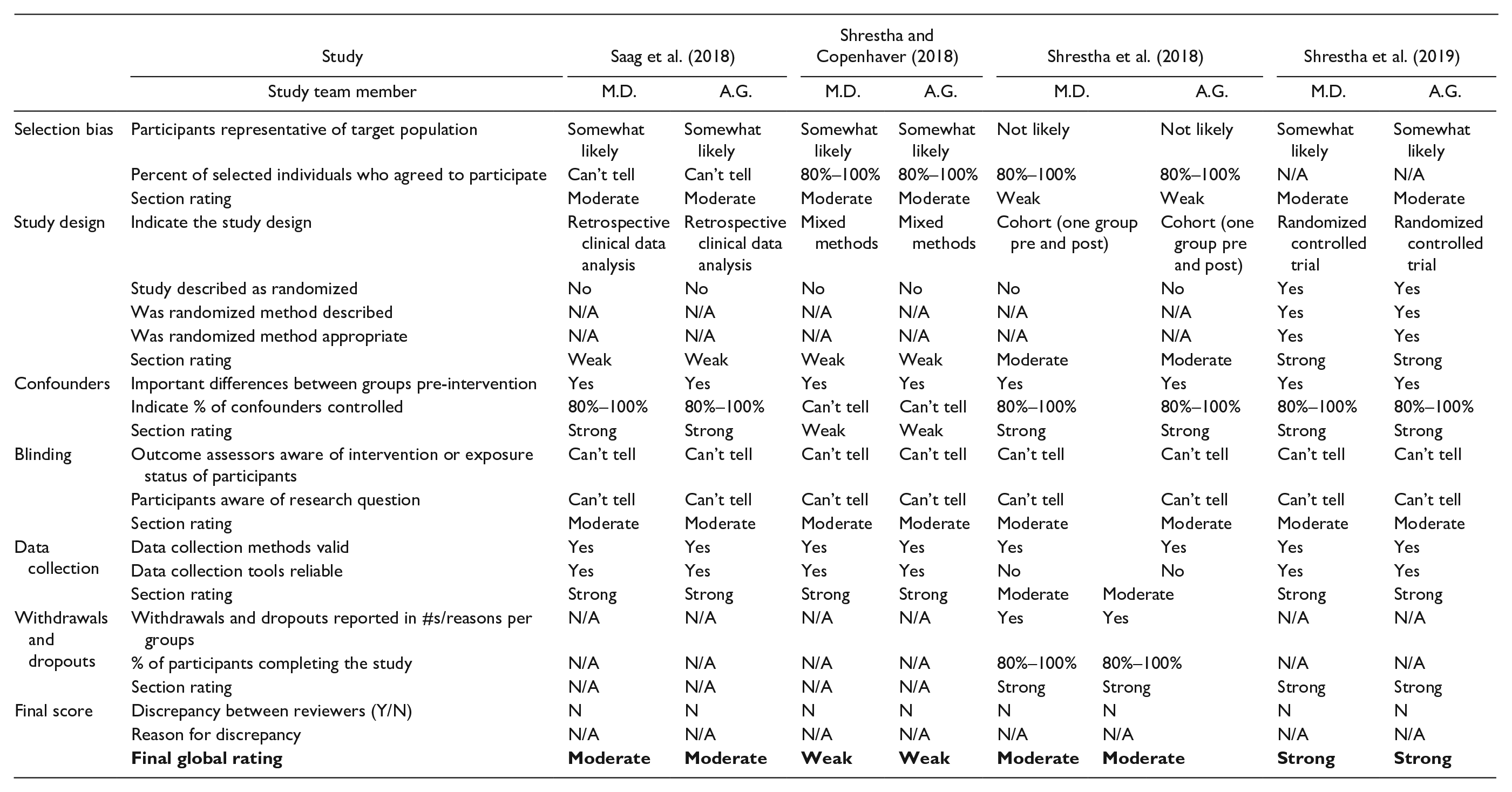
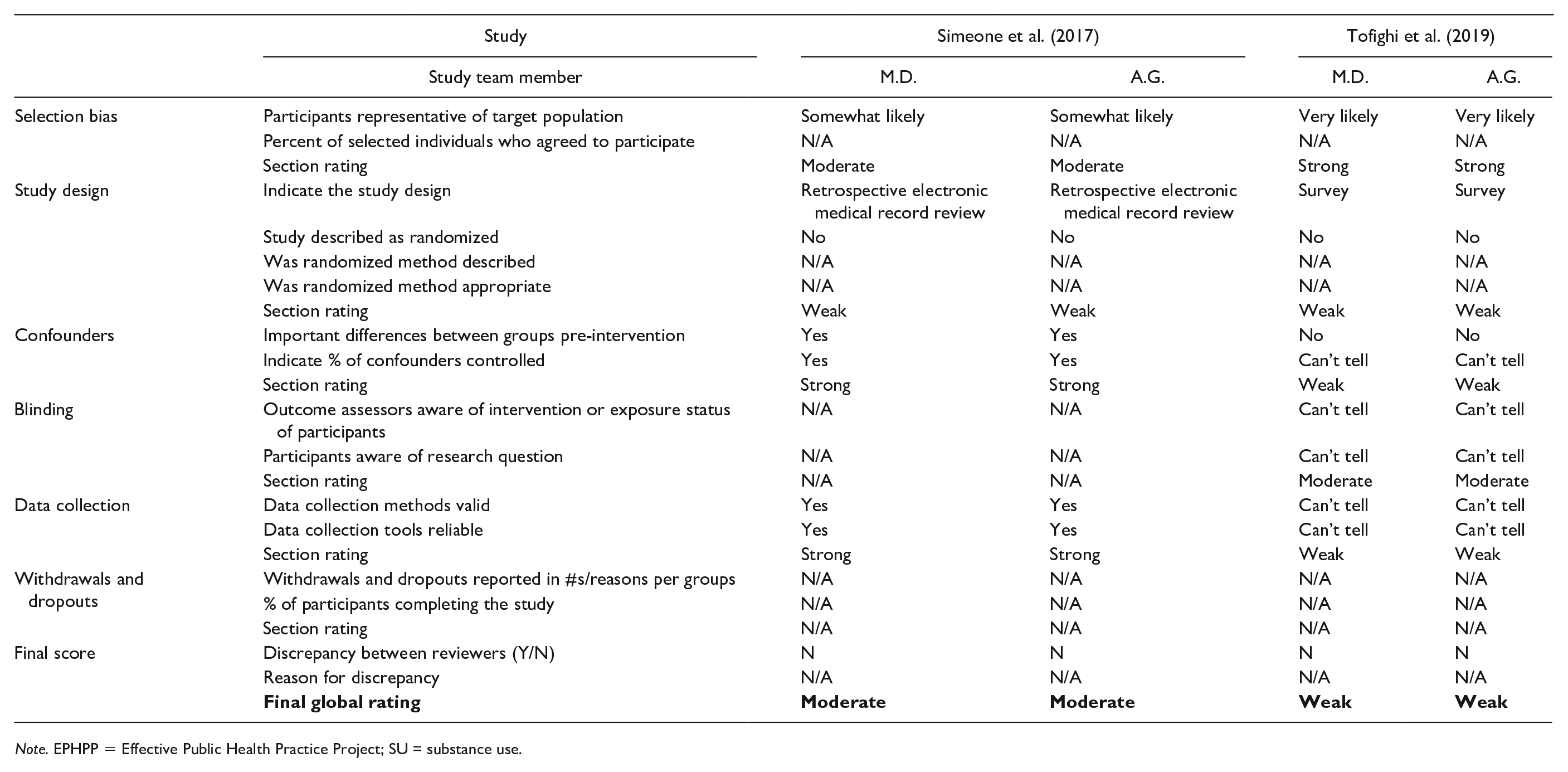
Note. EPHPP = Effective Public Health Practice Project; SU = substance use.
CASP Checklist for Qualitative Studies.
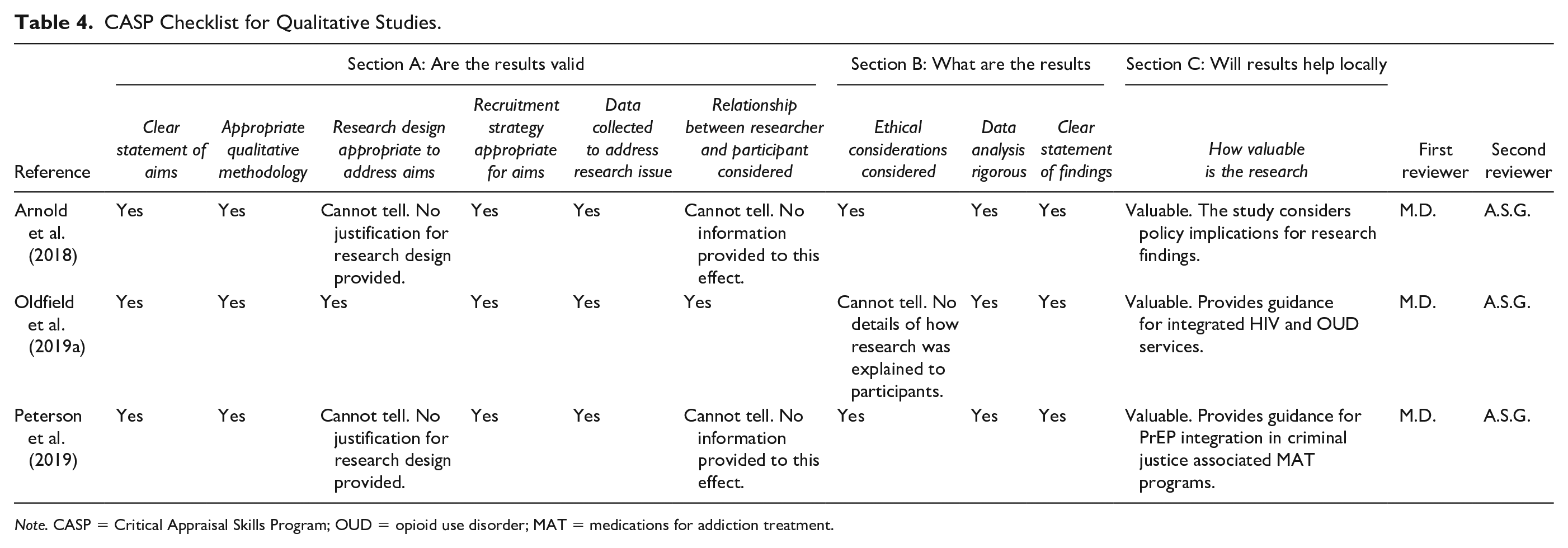
Note. CASP = Critical Appraisal Skills Program; OUD = opioid use disorder; MAT = medications for addiction treatment.
Discussion
Integrated HIV and OUD service delivery can improve HIV clinical outcomes, treatment, PrEP adherence, and HIV and OUD treatment retention, and reduce drug-related risk behaviors (Aggarwal et al., 2019; Barocas et al., 2019; Gardner et al., 2016; Shrestha et al., 2018, 2019; Simeone et al., 2017). Despite this, the majority of the integrated approaches identified in this review took place within a single facility or reported on differing models across facilities without evidence of broad implementation. The systems and tools required for integration across the studies were developed to implement each specific integrated approach. There was no evidence of systems coordination at the state level or within a health delivery network that facilitated coordinated implementation of integrated service delivery programs. Identifying opportunities to coordinate HIV and OUD systems of care may increase efficiencies and help to sustain the models. Such opportunities may include coordinated funding procurement across HIV and OUD; enhanced data-sharing and coordination across HIV and OUD care; expanded Medicaid to remove financial barriers; and quality improvement and data systems to support care coordination and monitor implementation.
Facilitating Service Access
This review identifies numerous opportunities to address enablers and barriers to integrated HIV/OUD service access. At the provider level, integrating empathy building and stigma reduction exercises, including toward LGBTIQ+, within HIV/OUD trainings may help to improve provider communication skills while increasing knowledge of the client’s psychosocial context (Beach et al., 2015). Prioritization of RWHAP providers for buprenorphine trainings may further facilitate access (Chavis et al., 2020). Client-level enablers include assigning patient navigators for clients with HIV and OUD who are unstably housed (Rajabiun et al., 2020). Given opioid abstinence also facilitates HIV/OUD service access, open access models that provide rapid access to methadone treatment initiation should be considered (Madden et al., 2018). Use of text messaging for appointment reminders, adherence support, and PrEP service locater information also can further enable service access (Gardner et al., 2016; Shrestha et al., 2018; Tofighi et al., 2019). Addressing client fear and mistrust through peer support models may also be beneficial (Hoffman et al., 2019). At the systems level, evidence-based integrated approaches identified through grant-funded opportunities have the challenge of not being sustained once funding ends. Further consideration of Medicaid or private insurance to sustain HIV/OUD integration is a critical step toward scale-up and sustainability (Bailey et al., 2021; Frank et al., 2021). In addition, future studies can assess case management models to further facilitate service access given that HIV and OUD often intersect with HCV, psychiatric conditions, and a host of other illnesses (Rich et al., 2018).
Site-Level Systems That Support Integration
Four studies noted the need to adapt existing site-level policies to provide a supportive framework under which the integrated programs can be delivered (Arnold et al., 2018; Jessop et al., 2017; Peavy et al., 2020; Shrestha et al., 2018). However, rather than recommending expansion beyond the specific facility, these studies only mentioned adapting existing policies to support increasing take-home medication prescribing flexibility, with no policy guidance beyond that specific area. Site-level policy frameworks should consider the breadth of systems affected by integrated services and develop frameworks that support changes in job descriptions, clinical service delivery, data capture and reporting, and policies for communication between HIV and OUD services within an integrated network, including case conferencing and integrated referral systems when off-site referrals are required (Vimalananda et al., 2019).
Development of integrated referral systems, risk assessments, and communication protocols were most often mentioned as tools developed to support integrated service delivery across both Model types. Only one study mentioned developing clinical protocols to support integrated service delivery, and this was limited to HIV intake and testing protocols within an OUD setting (Knudsen et al., 2017). Several studies mentioned introducing HIV risk assessment tools and substance use screening into HIV and OUD settings, respectively. These included an integrated quality of care assessment, PrEP adherence assessments, and HIV risk reduction assessments (Shrestha & Copenhaver, 2018; Shrestha et al., 2018, 2019; Simeone et al., 2017). Further compiling and introducing evidence-based tools that have been validated in HIV and OUD settings may help standardize integrated approaches and increase quality of care across providers.
Information on monitoring and evaluation of integrated services was limited across the studies. One study discussed developing an integrated quality of care matrix, but it had not been piloted at the time of publication (Oldfield et al., 2019a). Another study introduced a quality improvement tracking system within a methadone clinic to monitor clients across the care continuum including measuring retention and viral suppression (Simeone et al., 2017). Introducing integrated monitoring and evaluation tools may help to reduce duplication, and increase understanding of the specific care needs of HIV and OUD clients, as well as the potential benefits of integrated services.
There was a significant amount of overlap of the types of staffing models that were required to implement the integrated approaches across the studies. Overwhelmingly, the studies demonstrated that client familiarity with their provider and accordingly provider familiarity with the client and their social context are enablers of access and retention in care (Bachhuber et al., 2018; Saberi et al., 2020). The research also demonstrates that convenience and increasing service access points across communities further enables client service access (Jessop et al., 2017; Oldfield et al., 2019a; Simeone et al., 2017). Innovative models wherein trained professionals rotate across service access points either within a single facility or within a network of facilities that provide integrated care may help to increase efficiencies and convenience for clients while increasing their opportunities to interact with known and experienced providers. Such instances could also reduce experiences of stigma, particularly when providers are skilled working with LGBTIQ+ individuals which was identified as a barrier to client’s seeking care in multiple studies in this review (Arnold et al., 2018; Oldfield et al., 2019a). Rotation models have demonstrated increased service access and higher provider satisfaction when psychiatrists and psychologists worked within integrated care team models in primary care (Schreiter et al., 2014). They have also demonstrated reduced provider burnout and improved quality of care (Zoberi et al., 2009; Zubatsky et al., 2018).
State-Level Systems That Support Integration
Collaboration between state health systems, Medicaid, and private insurance for HIV and OUD is needed to ensure that integrated HIV and OUD service delivery is grounded within coordinated systems of care. State-level collaborative protocol development for integrated service delivery can reduce the burden at the facility level and provide instructions for implementing different types of integration. Protocols can be supported by developing integrated tools or a comprehensive HIV and OUD toolkit that contains validated job aids; monitoring, evaluation, and reporting guidance; and other materials for the service delivery level that facilitates integration. Once developed at the state level, protocols and other tools could be adapted at the organizational level to ensure that they are context-specific and reflect available resources within a facility. Provider training requirements and tools and information on patient education, case management and referral systems, supply chains, and data collection and monitoring should be considered during protocol development. State-level systems should consider the required contract funding procurement processes and expectations, billing and reimbursement limitations, licensing requirements, and monitoring systems to fully support and sustain integration initiatives.
Research on state-level policy frameworks to support health and social service integration demonstrates the need for a comprehensive policy framework to include governance and partnerships, workforce and staffing, financing and payment, and data sharing and use (Wodchis et al., 2020). In addition, policy frameworks should have established amendment mechanisms to reflect shifting patterns of substance use, HIV risk behaviors, and implementation contexts (Oldfield et al., 2019b). State-level comprehensive and fully integrated policy frameworks should define the parameters of HIV and OUD integration and the systems requirements and opportunities in place to fully implement at the service delivery level. These policy frameworks should consider barriers to client service access, including insurance coverage problems inclusive of pre-authorization requirements from Medicaid, inadequate referral systems, and low provider knowledge and skills (Andrews et al., 2019).
Identifying methods to report data from integrated programs in a manner that facilitates state cross-bureau monitoring and evaluation and coordinated planning will be critical to fully understanding the fluctuating HIV and OUD epidemics and continually working toward improved programmatic and service delivery. Systems for sharing data across HIV and OUD care systems, and examining data through Medicaid claims may also contribute to systems coordination efforts. Increased coordination between Medicaid and Ryan White Care act funding may also help to reduce fragmentation, increase efficiencies, and sustain systems coordination efforts (Sanborn, 2018).
While this review provides helpful information to better understand systems that support integrated services, there exist several limitations. PubMed and CINAHL were the only databases used so that the authors could have information ready for the project team in an efficient manner. There may be additional literature available on this topic outside of these two databases that the study team did not identify. The study team also limited the search to the past 5 years and studies published in English in the United States and Canada to increase the relevancy for the information gathered for the project. The majority of the articles included in this review were scored as weak quality. This was largely due to selection bias and failure to report dropouts or account for confounding factors. However, these components did not limit the ability to extract systems information from the studies. In addition, the majority of the studies were programmatic evaluations or exploratory studies that were less focused on describing the specific state or service delivery level systems components required for integration. However, where these elements were described, they were extracted and included in this review. Future research should specifically focus on examining elements of HIV and OUD systems coordination that strengthen availability of integrated service provision.
Conclusion
To our knowledge, this is the first systematic review of enablers of and barriers to integrated HIV and OUD service access and the systems and tools required to implement them. This review provides a meaningful contribution to the literature given it identifies a clear need for coordinated systems to support integration and tools to enable integrated HIV/OUD service provision. Findings demonstrate innovative service delivery approaches across a variety of settings, but there are opportunities to support broader coordination across HIV and OUD care systems at the state and service delivery levels. Concerted efforts to coordinate state-level systems and develop supportive policies, guidelines, and tools may facilitate integration at the service delivery level.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This product was supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) as part of an award totaling $2,095,039.00 with 0 percentage financed with non-governmental sources. The contents are those of the author(s) and do not necessarily represent the official views of, nor an endorsement, by HRSA, HHS or the U.S. Government.