
Abstract
Our review establishes the empirical evidence for patient mobility for elective secondary care services in countries that allow patients to choose their health care provider. PubMed and Embase were searched for relevant articles between 1990 and 2015. Of 5,994 titles/abstracts reviewed, 26 studies were included. The studies used three main methodological models to establish mobility. Variation in the extent of patient mobility was observed across the studies. Mobility was positively associated with lower waiting times, indicators of better service quality, and access to advanced technology. It was negatively associated with advanced age or lower socioeconomic backgrounds. From a policy perspective we demonstrate that a significant proportion of patients are prepared to travel beyond their nearest provider for elective services. As a consequence, some providers are likely to be “winners” and others “losers,” which could result in overall decreased provider capacity or inefficient utilization of existing services. Equity also remains a key concern.
Introduction
A number of high-income countries have introduced policies that enable patients to select a health care provider of their choice with the aim of increasing service capacity, enhancing efficiency, and improving the quality of health care delivered (Dixon, Robertson, & Bal, 2010; France & Taroni, 2005; Magnussen, Vrangbæk, & Saltman, 2009). It is expected that by publicly reporting information on the quality of providers’ services, patients will select a provider that best meets their needs. From the provider perspective, it is anticipated that this “competition in the market” offers a stimulus to become more responsive and patient-centered, thus improving performance (Berwick, James, & Coye, 2003).
Given the costs associated with reconfiguring the health care system to support patient choice and to encourage competition between providers, it is essential to understand how patients have responded to the introduction of these policies. A key question is therefore whether “patient choice” policies have encouraged patients to actively choose their provider (Dusheiko, 2014).
Studies attempting to answer this question have predominantly used data derived from surveys, asking individuals about recent health care episodes or their responses to hypothetical scenarios (Dixon, Robertson, Appleby, Burge, & Devlin, 2010; Finlayson, Birkmeyer, Tosteson, & Nease, 1999; Schwartz, Woloshin, & Birkmeyer, 2005; Victoor, Delnoij, Friele, & Rademakers, 2012). Other studies have used actual patient data from hospital or primary care episodes (Haynes, Lovett, & Sunnenberg, 2003). However, the latter studies are limited as they can only ascertain where patients were being treated and not whether they made an active choice. Furthermore, it is not possible to determine to what extent these choices were influenced by primary care physicians.
Given the inherent challenges associated with establishing active choice, one can instead ask a different empirical question: namely, whether there is evidence that patients seek care at hospitals other than their nearest. This question is related to the concept of “patient mobility.”
Even accounting for individual characteristics, the extent to which patients are able to move to alternative providers will depend on a number of circumstances, including area characteristics (e.g., urban vs. rural), the health care setting (e.g., primary vs. secondary care), the urgency of the clinical condition requiring medical support (e.g., emergency vs. elective), and the severity of the intervention (e.g., cataract surgery vs. coronary artery bypass grafting). Furthermore, the configuration of the health care market varies significantly between countries, with patient opportunity to choose dependent on organizational structures, systems of financing, and the geographical organization of specialist services.
Therefore, in this systematic review we aim to establish the evidence for patient mobility for elective services in the secondary care setting in countries that have introduced policies that enable patients to choose their health care provider. We also assess the methodological approaches used to describe patient mobility and analyze to what extent patient mobility is associated with patient, provider, and area characteristics.
Method
Search Strategy
A combined search was performed in Pubmed and Embase for articles published between January 1, 1990 and June 30, 2015 (Appendix A). Search terms were defined and modified iteratively following an initial broad search of the literature and a consultation with the authors of some retrieved studies.
Inclusion Criteria
Published full text empirical studies that investigated patient mobility and its determinants using information on the patients’ residence (e.g., zip code, county) and their actual secondary care episodes were considered for inclusion.
Two distinct types of study relating to patient mobility were identified from the preliminary analysis. The first type determines whether or not patients travel beyond their nearest secondary care provider(s) to receive care. The second type assesses the relative impact that distance on one hand and provider characteristics (e.g., quality) on the other hand have on patients’ choice of provider. Both study types were considered for inclusion and we describe the different models within these types in our “Results” section.
Only studies investigating patient mobility in European, North American (Canada and the United States) and Australasian countries, (Australia and New Zealand only) were considered. Countries had to have introduced patient choice policies in which providers are expected to compete on the basis of quality, mainly through publicly reporting indicators of provider-level performance (http://www.nhs.uk/pages/home.aspx; http://www.kiesbeter.nl/; Swedish Association of Local Authorities and Regions, 2013; Vrangbæk, Robertson, Winblad, Van de Bovenkamp, & Dixon, 2012)
Study participants must have been enrolled in a voluntary, tax-based, or social health insurance scheme and received elective (or non-emergency) outpatient/inpatient services in a secondary care setting. Only studies published in English and in peer-reviewed journals were considered for inclusion.
Exclusion Criteria
A key aspect of our study is to understand the patient and provider factors that influence where patients receive care. Therefore, we excluded studies that review patterns of mobility primarily reflecting insurer preferences for particular providers (e.g., through selective contracting and use of explicit financial incentives to channel patients to preferred providers; Boonen, Donkers, & Schut, 2011; Rosenthal, Li, & Milstein, 2009). For the same reason, we also excluded studies focusing on physician referral patterns because they primarily reflect physician preferences (Ringard, 2010).
Studies reviewing cross-border mobility were excluded. Also, studies reviewing patient mobility in the acute care setting (i.e., emergency hospital visits) were excluded as decisions regarding location of secondary care are constrained by the patients’ clinical condition and the necessity for urgent treatment.
Longitudinal studies that looked at the impact of the publication of performance indicators on hospital volumes or the effect of hospital competition on treatment outcomes, were excluded as they provide no explicit information on the impact of patient and provider characteristics on mobility or assessment of where patients are expected to receive their treatment based on their residence (Cooper, Gibbons, Jones, & McGuire, 2011; Cutler, Huckman, & Landrum, 2004; Laverty et al., 2012).
Articles that were published after 1990 but which used pre-1990 patient-level data were also excluded for the following reasons. First, introduction of provider choice policies did not occur before 1990 in most European countries. Second, reconfiguration of specialist services due to centralization after 1990 has influenced the choice of available providers. Third, there has been an increase in the quantity and quality of publicly available information to inform provider choice over the same period.
Data Selection
AA and DL independently selected articles that met the inclusion criteria based on titles and abstracts. When there was uncertainty about whether an article fulfilled the inclusion criteria, it was included for full text review. In the next stage, full text articles were reviewed independently by AA and DL. Final inclusion was based on consensus. Disagreements were resolved following discussion with JvdM. Reference lists from included studies were hand-searched for additional potentially relevant articles.
Data Extraction
AA independently extracted study data and consulted DL and JvdM in case of uncertainty. Data extracted included: location of study; geographical unit of analysis (regional vs. national); secondary care context (intervention/service[s] patients received), source of data (e.g., hospital discharge records); time-frame of analysis; study sample size and exclusion criteria; model for estimating patient mobility; definition of “expected” provider; construction of hospital “choice sets”; proportion of patients travelling beyond their expected provider(s); patient and provider characteristics analyzed; statistical analysis.
For “expected” provider(s) we refer to the nearest provider(s) offering the relevant intervention given the patient’s clinical condition. For hospital “choice sets,” we refer to the selection of hospitals that offer the relevant intervention as defined by the study authors. For example, this may include all hospitals within a threshold distance or region.
Study Assessment
The studies selected are best described as cross-sectional studies. A review of published checklists and scoring scales for systematic reviews was undertaken to identify the appropriate tool to assess the selected studies (Higgins & Green, 2008; Sanderson, Tatt, & Higgins, 2007); however, no suitable tool was found. A 10-item checklist was therefore created and validated (Appendix B) with reference to previously published relevant checklists for observational studies (Loney, Chambers, Bennett, Roberts, & Stratford, 1998; Munn, Moola, Riitano, & Lisy, 2014; Vandenbroucke et al., 2007).
One of the methodological challenges faced in using patient mobility as a proxy for patient choice is to separate the impact of patient choice from that of other factors. Patient mobility has been conceptualized as conforming to three distinct categories (Ringard, Rico, & Hagen, 2005; Tessier, Contandriopoulos, & Dionne, 1985). First, mobility due to patient choice; second, mobility due to primary care or secondary care referral preferences induced by physicians; and third, mobility due to insufficient local supply. In reality there are inherent difficulties in separating mobility due to patient choice and physician preferences given that these decisions are rarely mutually exclusive.
A key component of our checklist was therefore to assess whether the authors had accounted for, and adequately measured, relevant patient and health system factors that influenced patient mobility in order to identify “true movers.” “True movers” are considered to be individuals who travel beyond their nearest provider to an alternative provider without the biasing effect of health system factors (e.g., explicit financial incentives to choose particular providers). AA and DL independently assessed the selected articles according to each item on the checklist. Disagreements were resolved following discussion with JvdM.
Results
A total of 5,994 titles and abstracts were assessed for eligibility of which 54 were selected for full text review (Figure 1). Twenty-two publications were included in the final analysis (Balia, Brau, & Marrocu, 2014; Basu, 2005; Beukers, Kemp, & Varkevisser, 2014; Chernew, Scanlon, & Hayward, 1998; Cook et al., 2009; Escarce & Kapur, 2009; Fabbri & Robone, 2010; Fattore, Petrarca, & Torbica, 2014; Hanning, Ahs, Winblad, & Lundstrom, 2012; Howard, 2006; Kronebusch, 2009; Losina et al., 2007; Messina, Forni, Collini, Quercioli, & Nante, 2013; Nostedt et al., 2014; Pope, 2009; Radcliff, Brasure, Moscovice, & Stensland, 2003; Roh, Lee, & Fottler, 2008; Roh & Moon, 2005; Saunders, Bellamy, Menachemi, Chukmaitov, & Brooks, 2009; Sivey, 2012; Varkevisser & van der Geest, 2007; Varkevisser, van der Geest, & Schut, 2010, 2012). The reference lists of selected articles were hand-searched and a further four articles (Beckert, Christensen, & Collyer, 2012; Ho, 2006; Moscone, Tosetti, & Vittadini, 2012; Roh & Moon, 2005) met the inclusion criteria. A total of 26 articles were included in the final analysis. All articles were retrospective cross-sectional studies using administrative data on actual patient visits.
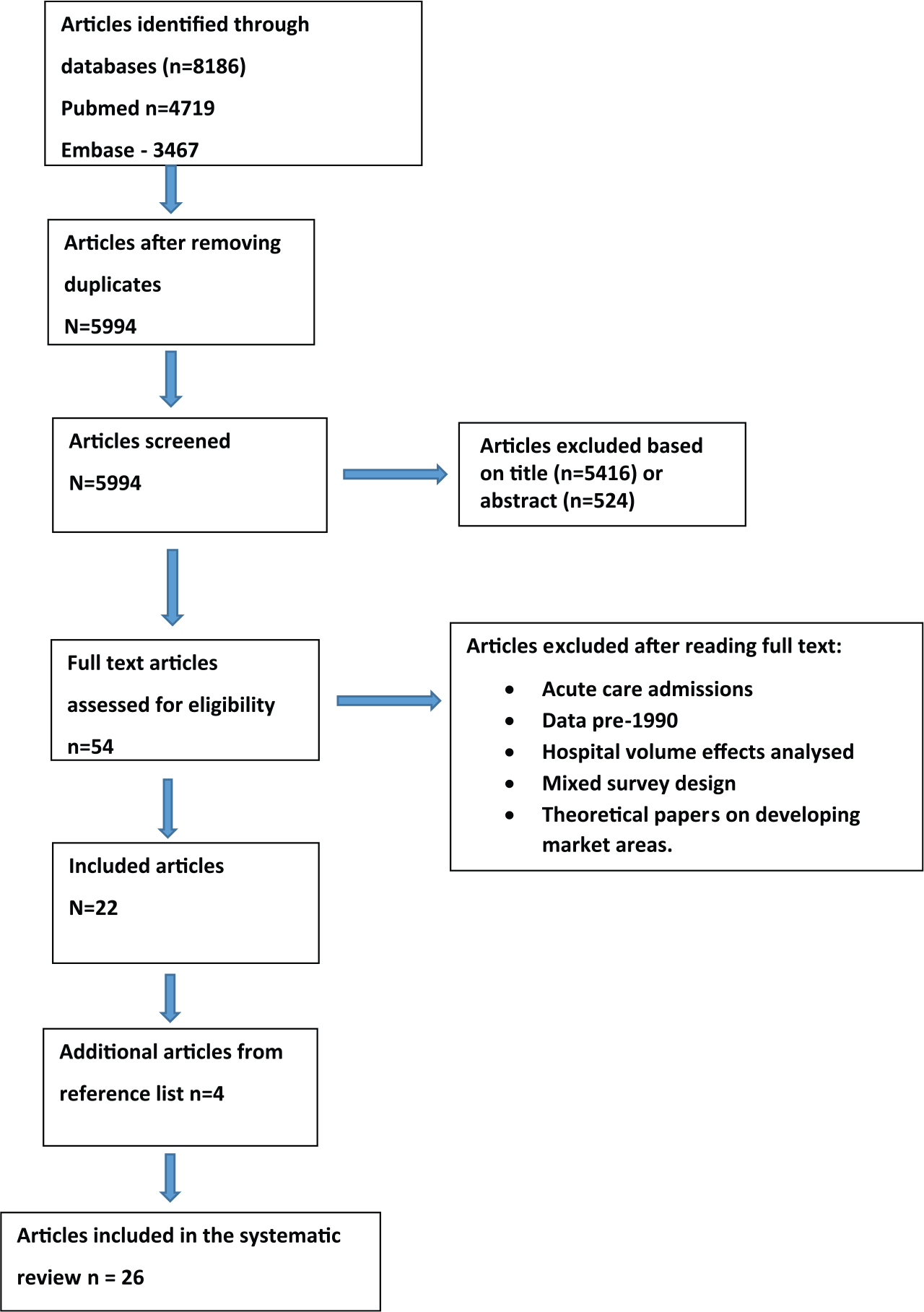
Flowchart of study selection.
Models to Assess Patient Mobility
We found that the studies used three main methodological models to assess mobility. Two of the models fit within the first type of studies (determining whether or not patients travel beyond their nearest provider; see the “Method” section). We refer to these as the “hospital bypassing model” (estimating the proportion of patients travelling beyond their expected provider for a particular intervention/service) and as the “regional model” (estimating the proportion of patients traveling outside a predefined geographical region based on their place of residence).
A third model fits within the second type of studies (assessing the relative impact of distance and provider characteristics on the choice of provider). In this article, this is referred to as the “patient choice model.”
Table 1 outlines the key characteristics of each study according to the three models that we used to assess mobility. The studies were conducted in six countries: United States—12 studies; Italy—5 studies; Netherlands—4 studies; England—3 studies; Sweden—1 study; and Canada—1 study. Of the five studies analyzing regional mobility, four were from Italy. Seven of the 10 studies using the hospital bypassing model were undertaken in the United States.
Descriptive Analysis of Selected Articles (n = 26) Stratified According to Methodological Model.
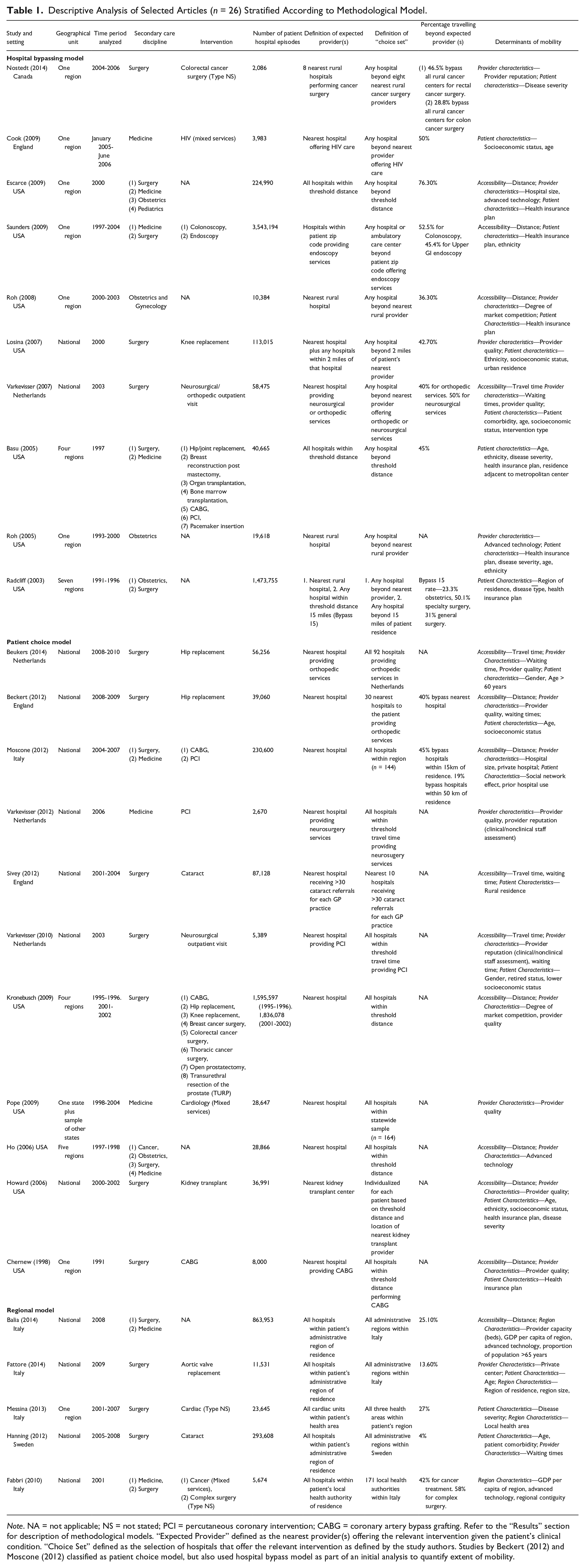
Note. NA = not applicable; NS = not stated; PCI = percutaneous coronary intervention; CABG = coronary artery bypass grafting. Refer to the “Results” section for description of methodological models. “Expected Provider” defined as the nearest provider(s) offering the relevant intervention given the patient’s clinical condition. “Choice Set” defined as the selection of hospitals that offer the relevant intervention as defined by the study authors. Studies by Beckert (2012) and Moscone (2012) classified as patient choice model, but also used hospital bypass model as part of an initial analysis to quantify extent of mobility.
Coronary artery bypass grafting, percutaneous coronary intervention (Chernew et al., 1998; Moscone et al., 2012), cataract surgery, and joint replacement surgery (Beckert et al., 2012; Beukers et al., 2014; Losina et al., 2007) were the commonest elective interventions analyzed. Other studies looked at a mix of surgical and medical admissions or a variety of admission types related to a particular secondary care discipline (e.g., neurosurgical services, HIV services, cancer; Cook et al., 2009; Varkevisser & van der Geest, 2007).
Definition of “Expected Provider” and “Choice Set”
A number of different definitions for the expected provider were used across the selected studies (Table 1). In the majority of studies using the hospital bypassing model this was the nearest provider. However, other definitions included all providers within a threshold distance or a specific area code (Escarce & Kapur, 2009; Saunders et al., 2009). The expected provider(s) in studies using the regional model were all hospitals within an administrative or governmental region.
The choice set was constrained in some of the studies using the patient choice model to providers within a defined regional area (Moscone et al., 2012; Pope, 2009). However, other definitions were evident. For example, in a Dutch study using the patient choice model for neurosurgical services, only hospitals within an hour of the patient’s residence were included in the choice set. The authors assumed that individuals traveling further were away from home when they needed health care (Varkevisser et al., 2010). Similarly in a U.K. study, the choice set only included the nearest 10 hospitals receiving more than 30 cataract referrals from the patients’ primary care physicians (Sivey, 2012).
Extent of Mobility
All studies showed evidence of patient mobility in response to provider choice policies. For those studies using the hospital bypassing mode, rates ranged from 23% to 76% (Basu, 2005; Cook et al., 2009; Escarce & Kapur, 2009; Losina et al., 2007; Nostedt et al., 2014; Radcliff et al., 2003; Roh et al., 2008; Saunders et al., 2009; Varkevisser & van der Geest, 2007).
Distant Admission
Threshold distances were also used to define local and distant admissions (Basu, 2005; Escarce & Kapur, 2009; Radcliff et al., 2003; Saunders et al., 2009). In most cases, these thresholds were defined arbitrarily; however, one study created a threshold based on average distances travelled to local hospitals by patients living within the same county. Different thresholds were subsequently created according to admission type and county of residence (Basu, 2005).
Two studies used a series of increasing threshold distances to analyze patterns of mobility (Radcliff et al., 2003; Saunders et al., 2009). The results of both studies demonstrated that while patients are prepared to bypass their nearest provider, there is a threshold distance above which patients are rarely prepared to travel to receive care at an alternative center. Furthermore, the Saunders study showed that rates of hospital bypassing increased between 10 and 20 miles to 30 to 50 miles but sharply decreased beyond 30 to 50 miles (Saunders et al., 2009).
Other studies, assessed not only whether rural patients bypassed their nearest provider but whether their destination provider was a rural or urban center (Roh et al., 2008; Roh & Moon, 2005). Urban admissions were considered as a proxy for distant admission and analyzed separately to those admissions at other rural providers.
Determinants of Patient Mobility
As can be expected, all studies, irrespective of the model they used to study patient mobility, showed that accessibility to a provider has an important effect on patient mobility. Patients are more likely to receive treatment from their nearest provider (either measured in terms of distance or travel time) or at a hospital located within their region (Balia et al., 2014; Beckert et al., 2012; Beukers et al., 2014; Chernew et al., 1998; Escarce & Kapur, 2009; Ho, 2006; Howard, 2006; Kronebusch, 2009; Moscone et al., 2012; Roh et al., 2008; Saunders et al., 2009; Sivey, 2012; Varkevisser et al., 2010, 2012; Varkevisser & van der Geest, 2007).
Studies using the hospital bypassing or patient choice models considered the impact of patient and provider characteristics at the patient level on decisions to bypass or choose a particular provider (Tables 1 and 2). In contrast, the studies using the regional model considered measures describing providers at a regional level and their impact on the flow of patients between regions.
Study Checklist (Articles Listed by Date of Publication)—See Appendix B for a More Detailed Description of the Items.
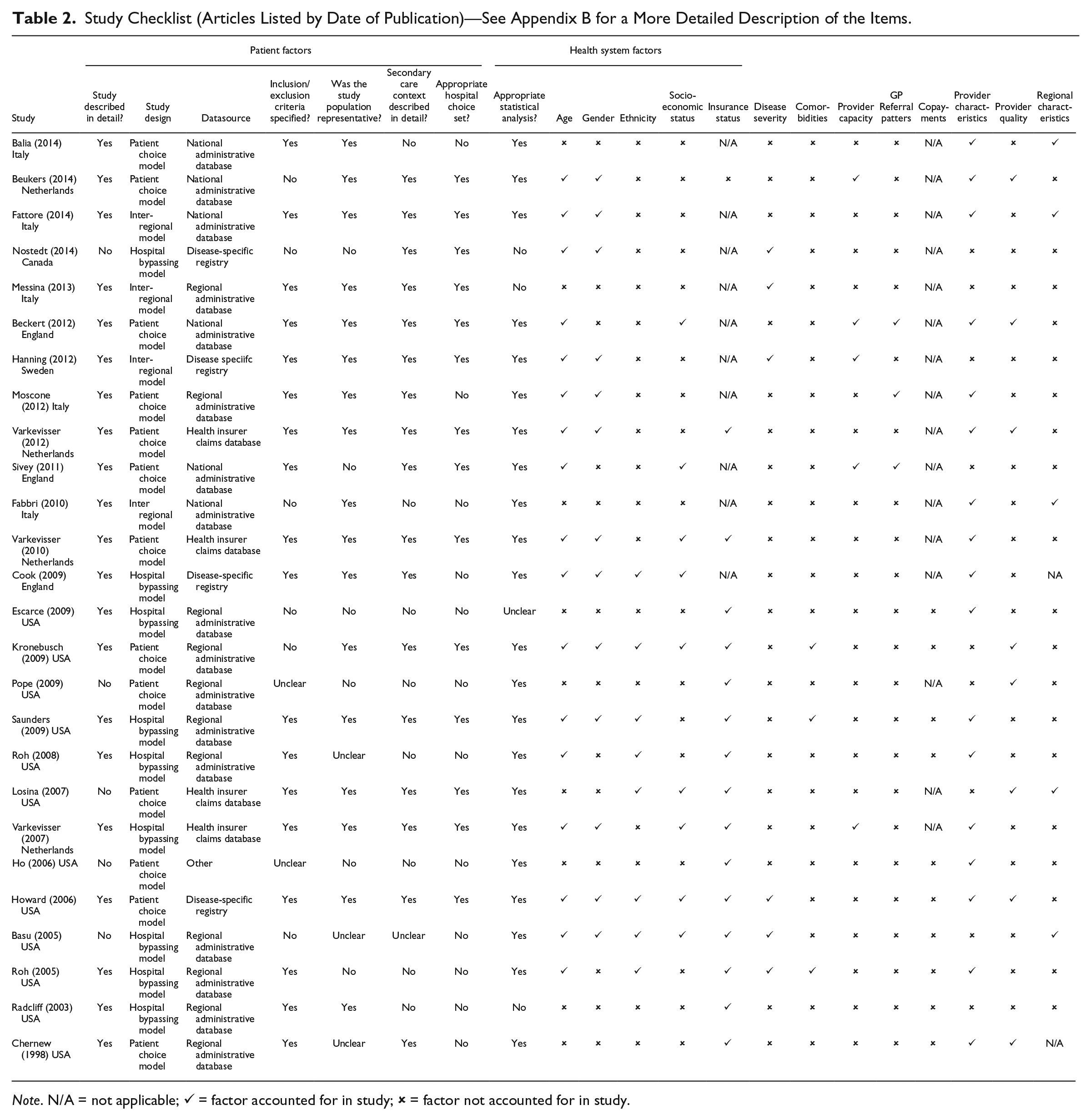
Note. N/A = not applicable; ✓= factor accounted for in study; ×= factor not accounted for in study.
For patient characteristics, 10 out of the 17 studies that reported results demonstrated that older patients were more likely to receive treatment from their nearest hospital (Balia et al., 2014; Basu, 2005; Beckert et al., 2012; Beukers et al., 2014; Cook et al., 2009; Fattore et al., 2014; Hanning et al., 2012; Howard, 2006; Roh & Moon, 2005; Varkevisser & van der Geest, 2007). Six out of nine studies demonstrated that patients in lower socioeconomic groups were more likely to receive treatment from their nearest providers (Beckert et al., 2012; Cook et al., 2009; Howard, 2006; Losina et al., 2007; Varkevisser et al., 2010; Varkevisser & van der Geest, 2007).
Six of the eight studies reviewing the impact of ethnicity on patterns of mobility found a statistically significant association (Table 1). Of these, four studies demonstrated that non-White patients were less likely to bypass local rural hospitals than White patients when controlling for all other factors (Basu, 2005; Roh et al., 2008; Roh & Moon, 2005; Saunders et al., 2009). These studies also demonstrated that non-White patients are less likely to travel as far as White patients to receive treatment, especially to providers based in out-of-area urban settings. Two studies found that non-White men and women were less likely to receive care at higher quality hospitals for total hip replacement surgery and kidney transplantation (Howard & Kaplan, 2006; Losina et al., 2004).
In eight of the nine U.S. studies that included patients affiliated with different health insurance plans, the extent of mobility varied depending on health plan type (Basu, 2005; Chernew et al., 1998; Escarce & Kapur, 2009; Howard, 2006; Radcliff et al., 2003; Roh et al., 2008; Roh & Moon, 2005; Saunders et al., 2009). It is not possible to make comprehensive conclusions as to overall trend in patient mobility according to insurance plan type. However, the increased rates of mobility reported for patients with commercial health insurance plans may be due to the potentially greater number of alternative providers that are available to choose from compared with what would be the case with Health Maintenance Organizations, Medicaid, and Medicare plans (Basu, 2005; Roh et al., 2008). Another explanation could be that younger patients and those with employer-sponsored coverage were more responsive to quality-of-care differences between providers and had the means (physical/financial) to access more distant hospitals (Radcliff et al., 2003).
All six studies analyzing the effect of provider capacity (i.e., measured in terms of waiting times for a particular treatment) on patient mobility demonstrated that patients were more likely to move to providers with shorter waiting times (Beckert et al., 2012; Beukers et al., 2014; Hanning et al., 2012; Sivey, 2012; Varkevisser et al., 2010; Varkevisser & van der Geest, 2007).
All eight studies analyzing the effect of proxy measures for provider quality on patient mobility demonstrated that patients are more likely to travel further to receive treatment from providers who deliver a better quality of care according to these measures (Beckert et al., 2012; Beukers et al., 2014; Chernew et al., 1998; Howard, 2006; Kronebusch, 2009; Losina et al., 2007; Moscone et al., 2012; Pope, 2009; Varkevisser et al., 2012; Varkevisser & van der Geest, 2007). Different measures of provider quality were used in each of the studies (e.g., generic mortality rates, hospital infection rates, heart failure readmission rates, transplant failure rates, high volume surgical unit, hospital ranking). Other provider factors that are associated with a willingness to travel further are the availability of advanced technology (although not necessarily for the specialty in question) and a larger hospital (Balia et al., 2014; Escarce & Kapur, 2009; Fabbri & Robone, 2010; Ho, 2006; Roh & Moon, 2005).
In administrative regions with older populations (age >65 years) and high levels of affluence (measured as GDP per capita) patients were less likely to move to providers outside their region. Similarly patients were more likely to seek care within regions that were accessible by public and private transport (Balia et al., 2014; Fabbri & Robone, 2010; Fattore et al., 2014).
Study Assessment
Articles were assessed according to the checklist described in the “Method” section (Table 2). When reviewing the hospital choice sets, we found that 12 of the 26 studies did not state explicitly whether the alternative hospitals offered the particular service in question (Balia et al., 2014; Basu, 2005; Chernew et al., 1998; Cook et al., 2009; Escarce & Kapur, 2009; Fabbri & Robone, 2010; Ho, 2006; Moscone et al., 2012; Pope, 2009; Radcliff et al., 2003; Roh et al., 2008; Roh & Moon, 2005). Also, it is likely that the fitness of the patients and severity of the disease will have an effect on patient mobility, but only six studies assessed disease severity (Basu, 2005; Hanning et al., 2012; Howard, 2006; Messina et al., 2013; Nostedt et al., 2014; Roh & Moon, 2005) and three comorbidity (Kronebusch, 2009; Roh & Moon, 2005; Saunders et al., 2009).
Another important checklist item was that studies accounted for possible effects of copayments on decisions where to have their care or treatment. While some of the U.S. studies chose particular subpopulations (e.g., Medicare patients for whom copayments are generally fixed between providers; Losina et al., 2007; Pope, 2009), 10 of the 12 studies which looked at patients enrolled in a variety of insurance schemes made no account of the impact of variation in copayments on their destination hospital (Basu, 2005; Chernew et al., 1998; Escarce & Kapur, 2009; Ho, 2006; Howard, 2006; Kronebusch, 2009; Radcliff et al., 2003; Roh et al., 2008; Roh & Moon, 2005; Saunders et al., 2009).
Discussion
This is the first review to systematically describe and analyze the published empirical literature on patient mobility for elective services in the secondary care setting. Our review demonstrates that patients travel to a hospital other than their nearest provider for a wide variety of health care interventions.
A further major finding of this review is the identification of three main methodological models (hospital bypassing, regional, and patient choice models) used to analyze patient mobility in different health care markets. Our results demonstrate that the model used to define mobility is influenced by the health care context with no single model providing a single policy frame. For instance, the regional model has been used almost exclusively in the Italian studies, with the key variable being whether or not patients receive treatment in the administrative region they reside in. This is because the organization and administration of publicly financed health care in Italy was decentralized to 20 regions following constitutional reform in 2001 (Balia et al., 2014). Rates of inflow and outflow of patients are analyzed to assess the effectiveness of regional health care supply, and look for flow imbalances which may have an impact on regional budgets (France, Taroni, & Donatini, 2005). Sweden adopts a similar system with health care decentralized to county councils (Vrangbæk, Østergren, Birk, & Winblad, 2007).
In contrast, the United Kingdom, Netherlands, and the United States do not exhibit the same level of regional decentralization and therefore the hospital bypassing and patient choice models were used to study mobility between health care providers. While clear differences in the nature of the health care market and extent of competition exist, the response of patients to perceived differences in provider quality is an essential component of all these three countries.
A number of the U.S. studies in our review used the hospital bypassing model to analyze the extent of “rural hospital bypassing” (i.e., the proportion of rural residents bypassing their nearest rural provider[s] to access an urban center for a particular intervention; Escarce & Kapur, 2009; Roh & Moon, 2005). The extent to which this is occurring is a particular concern in the United States due to long-standing concerns related to the availability and quality of health care resources in rural settings (Bronstein & Morrisey, 1991; Buczko, 1997; Escarce & Kapur, 2009).
The review demonstrated that variation exists in the proportion of patients moving to alternative providers for elective secondary services (23%-77%). However, we found that the extent of mobility depends on a number of factors. These include, apart from the secondary health care intervention in question, the study methods used and the geographical unit of analysis (national vs. regional).
It is unclear from the available evidence whether such mobility is sufficient for effective competition and improvements in quality. However, the results of this review demonstrate that there are actual changes in market share which may represent a major driver given the extent of mobility reported.
We found that patients were more likely to move to providers considered to be of higher quality, or that offered advanced technologies. However, mobility may have a negative effect on competition by providing increased incentives for risk selection of patients by providers in order to improve their apparent performance according to the selected indicators.
Service capacity may also be an emerging issue for high-performing centers that receive a net gain of patients due to mobility. Without adequate planning, an increased flow of patients from outside the provider catchment area may result in lengthening waiting lists. At the same time, it may result in unused capacity and resources within centers that have a net loss of patients, creating health system inefficiencies.
The effect of patient choice policies on equity remains a key concern, given that older patients and lower socioeconomic groups are less likely to travel beyond their nearest health care provider. The impact of disease complexity or comorbidities on the decision to move between providers is unclear. On the other hand, the outflow of patients from hospitals located in socioeconomically deprived settings may provide the necessary stimulus to improve provider performance and in this way benefit the majority of nonmovers.
One of the challenges in reviewing these studies is to ascertain whether they are able to identify true movers (i.e., mobility due to patient choice rather than health system factors). Our checklist sought to assess the extent to which these factors have been accounted for (Table 2). We found, particularly in the U.S. studies, that there was limited information on the choice set of hospitals available to each patient. As a result, it was not always possible to ascertain whether the choice of available hospitals considered in the study actually provided the service or intervention in question.
It was also not possible to assess the extent of selective contracting of providers by different insurers in the U.S. market, and how centralization of services contributed to patterns of mobility. A further issue in the U.S. studies was the paucity of information on the extent of variation in copayments. It was therefore not always possible to disentangle the impact between price and quality on mobility.
Primary care referral patterns and capacity of available providers (e.g., waiting lists) were rarely considered in the selected studies (Table 2), predominantly because of data constraints. Provider capacity as measured through waiting lists is an important health system factor (Dawson, Gravelle, Jacobs, Martin, & Smith, 2007) which can directly affect patient mobility (Beckert et al., 2012; Beukers et al., 2014; Sivey, 2012).
Conclusion
Provider choice policies have previously been criticized due to the lack of empirical evidence that such policies influence where patients receive treatment (Pollock et al., 2012). Our findings provide substantial evidence that patients are prepared to travel beyond their nearest provider for their care or treatment. It has been hypothesized that the driver for improving provider performance would be the threat of losing market share and that even movement of only 5% to 10% of patients would provide the necessary incentive to improve quality (Berwick et al., 2003; Le Grand, 2009). However, these results suggest that there are likely to be “winners” and “losers” from health care market reforms, which could have an impact on the configuration of existing health care markets if some providers continue to lose market share. There is therefore potentially a trade-off between the effects of mobility on improving provider quality but at the same time decreasing provider capacity.
Equity also remains an issue given that the elderly and low socioeconomic groups are less likely to travel beyond their nearest provider for health care. This in turn may result in hospitals within socioeconomically deprived areas with older demographic profiles having to manage far more complex patient cohorts (both medically and socially), which subsequently affects their quality outcomes.
Further work is required to understand the drivers of patient mobility (e.g., quality, reputation, referral patterns) and its impact on equity in access to services and patient outcomes. In this regard, our checklist for studies of patient mobility provides a framework for developing future research facilitating the comparability of study results.
Footnotes
Appendix A
Appendix B
Authors’ Note
The views expressed in this publication are those of the authors and not necessarily those of the NHS, the National Institute for Health Research or the Department of Health.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Ajay Aggarwal is funded by a Doctoral Research Fellowship from the National Institute for Health Research.