
Abstract
Objective
Continuously tracking and monitoring the changes in indicators of anticoagulation and fibrinolysis in healthy pregnant women during different pregnancy periods, to establish trimester-specific reference intervals.
Methods
A total of 200 healthy pregnant women registered in Peking University First Hospital were enrolled. Venous blood samples were collected at different pregnancy periods, and thirteen related anticoagulation and fibrinolysis indicators were tested. The impact of pregnancy periods on these indicators were analyzed, and corresponding reference intervals were established.
Results
Significant differences were observed among the non-pregnant group and the first trimester(6–8weeks), second trimester(24–28weeks), and third trimester(36–38weeks) groups for antithrombin (AT), protein S activity (PS Ac), free protein S (FPS), protein C (PC), D-Dimer, fibrin/fibrinogen degradation products (FDP), plasmin inhibitor (PI), plasminogen (PLG), von Willebrand factor activity (vWF:Ac), von Willebrand factor antigen (vWF:Ag), lupus anticoagulant. AT, PS Ac, and FPS showed a downward trend with increasing gestational period. PI was significantly increased in the first trimester. PLG and vWF:Ag was higher in the second trimester and the third trimester. vWF:Ac, D-Dimer and FDP showed an continuously upward trend with increasing gestational period; the normalized SCT ratio (SCT TR)was significantly lower in the third trimester; the normalized dRVVT ratio (dRVVT TR)was significantly higher in the second and third trimester.
Conclusion
This study established reference intervals for thirteen anticoagulant and fibrinolytic indicators in healthy pregnant women in Beijing, China. Additionally, pregnancy periods affect the test results of anticoagulant and fibrinolytic indicators in pregnant women, and the reference intervals should be established separately according to pregnancy periods.
Introduction
Due to the change of hormone levels in the body, pregnant women show obvious hypercoagulability, which is manifested by an increase in physiological procoagulant factors and a decrease in anticoagulant proteins, and the changes in the fibrinolytic system.1,2 This is a protective physiological change, on one hand, the changes are conducive to the nurturing, delivery, and postpartum recovery of the fetus and the mother. On the other hand, it also increases the risk of venous thromboembolism (VTE) and disseminated intravascular coagulation (DIC). 3 Common complications of pregnancy, such as preeclampsia and hemorrhage during delivery, are also closely related to the hypercoagulable state. 4 Therefore, accurate assessment of coagulation function in pregnant women is crucial. However, most of the biological reference intervals currently used in laboratory for coagulation and fibrinolysis tests are derived from the general population. Due to the difficulty in enrolling pregnant women and the high cost of establishing reference intervals, there are currently no reference intervals for relatively comprehensive indicators related to anticoagulation and fibrinolysis in healthy pregnant women. And only a few laboratories have established reference intervals for some items. Moreover, due to the different instruments and reagents used in different laboratories, the various test results also show significant variation. Therefore, the purpose of this study was to establish biological reference intervals for the thirteen items in healthy pregnant women in Beijing, China, including AT, PS Ac, Free PS, PC, DDHS, DDHS500, FDP, PI, PLG, vWF:Ac, vWF:Ag, SCT TR, and dRVVT TR based on Werfen system, in order to observe the differences of these indicators in different pregnancy period.
Materials and Methods
Study Subjects
This study was a cohort study. 297 pregnant women from the Department of Obstetrics, Peking University First Hospital, Beijing, China were recruited randomly for informed consent and questionnaire, from December 2019 to December 2020. 122 refused to participate or excluded. The exclusion criteria were as follows: (1) Acute or chronic diseases (including heart, liver, kidney diseases), hematological diseases, thyroid diseases, diabetes, autoimmune diseases, and infections; (2) Personal or family history of hemorrhagic disease, thrombotic diseases, tumors; (3) Use of antiplatelet drugs, anticoagulants, nonsteroidal anti-inflammatory drugs, contraceptives, etc, within one week; (4) History of more than two miscarriages; (5) Presence of obstetric complications such as pregnancy-induced hypertension, gestational diabetes, placental abnormalities, etc; (6) Multiple pregnancies (twins or more). In the 175 pregnant women that were selected, the questionnaire and medical examination indicate that they are in good health, with no complications during the pregnancy period. Written informed consent was obtained from the patients for their anonymized information to be published in this article.
Peking University First Hospital is one of the largest comprehensive hospitals in Beijing. Its Department of Obstetrics is a national key discipline and a key clinical specialty. There are three wards in the obstetrics department, nearly 300 medical staff including doctors, nurses and technicians, 102 beds and about 6000 deliveries per year. The patients of the Department of Obstetrics in Peking University First Hospital mainly come from Beijing and its surrounding areas in North China.
The study protocol, informed consent, questionnaire, statement of the principal investigator were submitted to the Ethics Committee of Peking University First Hospital on August 12, 2019, The study was approved by the Ethics Committee of Peking University First Hospital on November 11, 2019.
Reagents and Instrument
All assays were performed on the ACL TOP 750 automatic coagulation analyzer (Instrumentation Laboratory, Spain), and reagents for AT, PS Ac, Free PS, PC, DDHS, DDHS500, FDP, PI, PLG, vWF:Ac, vWF:Ag, lupus anticoagulant (SCT and dRVVT), calibrators, and quality control materials.
Sample Collection
Blood samples were collected by sterile venipuncture of a vein into vacuum BD Vacutainer™ tubes with sodium citrate, the total volume was 2.7 mL. The samples are from the pregnant women at different period of pregnancy (6-8 weeks, 24-28 weeks, and 36–38 weeks). All samples were centrifuged at 2000 g for 15 min to separate the plasma and all plasma were frozen and stored. The storage period for the frozen plasma did not exceed six months.
Sample Detection
The ACL TOP 750 automatic coagulation analyzer was calibrated, and quality controlled according to standard operating procedures (SOP). All assays were performed by batch using the frozen plasma (incubate at 37 °C) on the instrument.
Statistical Methods
The data were entered using Microsoft Excel. Two experienced senior technicians are arranged to independently enter the data. We used comparison function to compare the data and identify the inconsistent parts. For the discrepant data found through the comparison, We checked the original test data and make modifications. Statistical analysis was conducted using SPSS version 25 software. If the data were normally distributed, the reference interval was defined as the mean ± 1.96 SD; if not, the reference interval was defined as (P2.fifth, P97.fifth). For comparisons between two groups, if the data met the normal distribution, the completely randomized design of ANOVA was used; otherwise, the Wilcoxon rank-sum test of comparison between two independent samples was used. For multiple group comparisons, if the data met the normal distribution, the completely randomized design of ANOVA was used, and the LSD test is used for pair comparison between groups. if the data did not meet the normal distribution, Kruskal-Wallis rank sum test was used for inter-group comparison, and multiple comparison in Kruskal-Wallis single factor ANOVA test in SPSS 25 was used for pound-for-group comparison. A P-value <0.05 was considered significant.
Results
Inclusion and Completion of Study Objects
A total of 200 healthy pregnant women were screened by questionnaire for this study. And those who did not meet the eligibility criteria were excluded from the enrolled population, 175 pregnant women were finally included for analysis in the first trimesters. During the subsequent study, some study objects dropped out, and 123 were collected in the second trimester and 112 in the third trimester. Details of the study objects are shown in Table 1.
Characteristics of the Population in This Study.

Establishment of Reference Intervals for Healthy Pregnant Women
Normality tests were performed on the result of anticoagulation and fibrinolytic indexes of healthy pregnant women during different pregnant period and corresponding reference intervals were established. The test results and reference intervals are shown in Table 2-5.
Test Results and Reference Interval of Anticoagulant and Fibrinolytic Indicators in First Trimester (N = 175, Ages 24-43).

* Note: AT and dRVT-TR are subject to normal distribution, and reference intervals are established with mean ±1.96SD. Other test assays are not subject to normal distribution, and reference intervals are established with (P2.5, P97.5).
Test Results and Reference Interval of Anticoagulant and Fibrinolytic Indicators in the Second Trimester (N = 123, age 24-39).

* Note: AT, PS Activity, vWF:Activity in type non-O, SCT-TR, dRVT-TR are subject to normal distribution, and reference intervals are established with mean ±1.96SD. Other test assays are not subject to normal distribution, and reference intervals are established with (P2.5, P97.5).
Test Results and Reference Interval of Anticoagulant and Fibrinolytic Indicators in the Third Trimester (N = 112, Ages 24∼40).

* Note: vWF:Activity in type Non-O, vWF:Activity in type-O, PC, PI, PS Activity are subject to normal distribution, reference intervals are established with mean ±1.96SD. Other assays are not subject to normal distribution, and reference intervals are established with (P2.5, P97.5).
Test Results of Anticoagulant and Fibrinolytic Indicators in the non-Pregnancy (N = 22, Ages 20∼40).
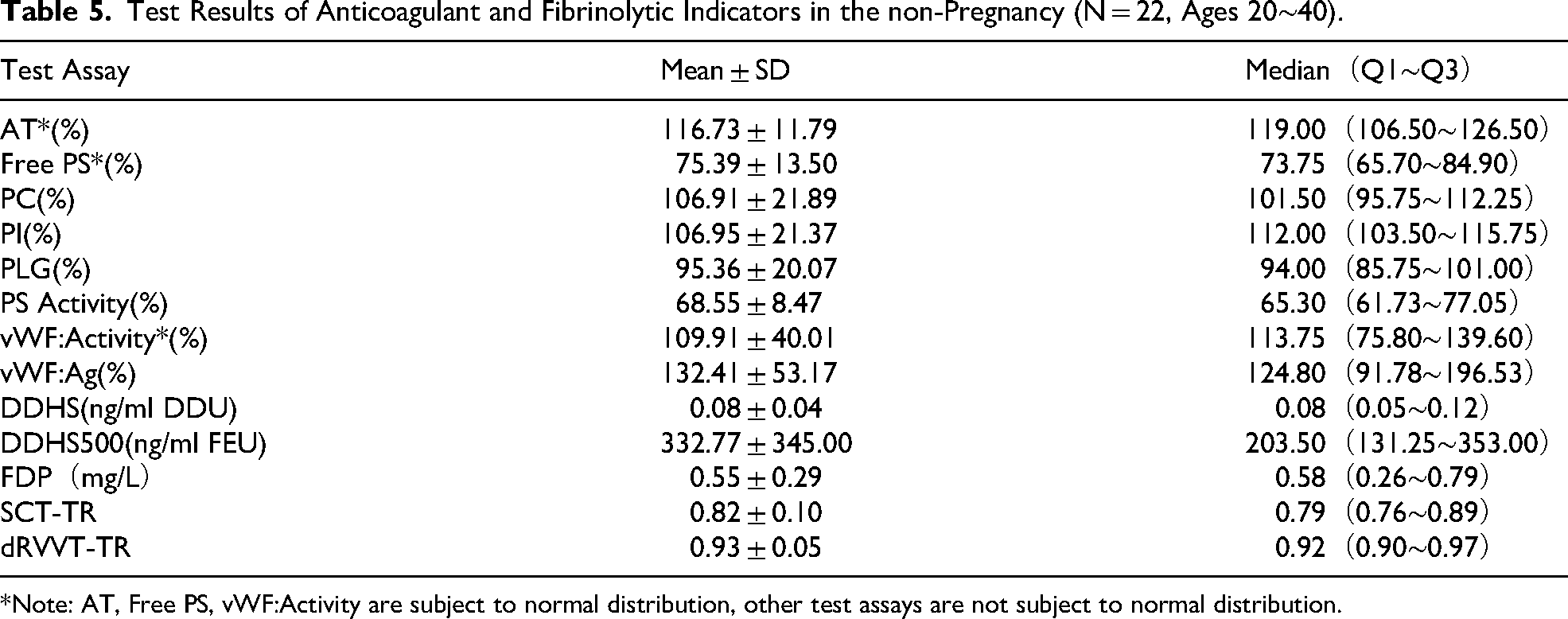
*Note: AT, Free PS, vWF:Activity are subject to normal distribution, other test assays are not subject to normal distribution.
Comparison of Anticoagulant and Fibrinolysis Indicators During Different Pregnant Period
There were significant differences in anticoagulant and fibrinolysis indicators among different pregnant period (all P < 0.001).
The results of different pregnancy period were compared in pairs. It was found that AT in the first trimester, second trimester and third trimester was significantly lower than the non-pregnant (all P < 0.001), AT in the third trimester is significantly lower than the first trimester and second trimester (P = 0.004; P < 0.001); there was no significant difference between the first trimester and second trimester (P = 0.381). FPS in the first trimester, second trimester and third trimester were significantly lower than in the non-pregnant state (all P < 0.001), with FPS in the first trimester and third trimester significantly lower than in the second trimester (P < 0.001; P = 0.011), and no significant difference between the first trimester and the third trimester (P = 0.539). PS Ac in the first trimester, second trimester and third trimester were significantly lower than in the non-pregnant state (all P < 0.001), with PS Ac in the third trimester significantly lower than the first trimester (P < 0.001), and no significant difference between the first trimester and second trimester (P = 0.100), or between second trimester and third trimester (P = 0.185). PC showed no significant difference between the non-pregnant state and the first trimester and the third trimester (P = 1.000; P = 0.750), but was significantly higher in the second trimester than in the non-pregnant state, the first trimester, and the third trimester (P = 0.012; P < 0.001; P = 0.035), with PC in the third trimester significantly higher than in the first trimester (P < 0.001). PI showed no significant difference between the non-pregnant state and the second trimester and third trimester (P = 0.927; P = 1.000) but was significantly higher in the first trimester than in the non-pregnant state, second trimester and third trimester (P = 0.005; P = 0.001; P < 0.001), with no significant difference between the second trimester and third trimester (P = 0.060). PLG showed no significant difference between the non-pregnant state and the first trimester (P = 0.072), and no significant difference between the second trimester (P = 0.106) but was significantly higher in the second trimester and third trimester than in the non-pregnant state and the first trimester (both P < 0.001). DDHS was significantly higher in the first trimester, second trimester and third trimester than in the non-pregnant state (all P < 0.001), and significantly higher in the second trimester and third trimester than in the first trimester (both P < 0.001), with the third trimester significantly higher than the second trimester (P = 0.011). DDHS500 was higher in the first trimester than in the non-pregnant state, but the difference was not statistically significant (P = 0.053); it was significantly higher in the second trimester and third trimester than in the non-pregnant state and the first trimester (both P < 0.001), with the third trimester significantly higher than the second trimester (P < 0.001). FDP was significantly higher in the first trimester, second trimester and third trimester than in the non-pregnant state (P = 0.001; P < 0.001; P < 0.001), and significantly higher in the second trimester and third trimester than in the first trimester (both P < 0.001), with the third trimester significantly higher than the second trimester (P < 0.001). The lupus anticoagulant normalized SCT ratio was significantly lower in the third trimester than in the non-pregnant state, the first trimester, and second trimester (P = 0.006; P < 0.001; P < 0.001), with no significant difference between the non-pregnant state and the first trimester and second trimester (both P = 1.000), and no significant difference between the first trimester and second trimester (P = 1.000). The lupus anticoagulant normalized dRVVT ratio showed no significant difference between the non-pregnant state and the first trimester (P = 1.000), and no significant difference between the second trimester and third trimester (P = 1.000), but was significantly higher in the second trimester and third trimester than in the non-pregnant state (P = 0.018; P = 0.008), and significantly higher in the second trimester and third trimester than in the first trimester (both P < 0.001).
Comparison of vWF:Ag Results in Different Blood Types
vWF:Ac was significantly higher in the first trimester, second trimester and third trimester than in the non-pregnant state (P = 0.038; P < 0.001; P < 0.001), and significantly higher in the second trimester and third trimester than the first trimester (both P < 0.001), with the third trimester significantly higher than the second trimester (P = 0.001). vWF: Ag showed no significant difference between the non-pregnant state and the first trimester (P = 0.066), and no significant difference between the second trimester and third trimester (P = 0.745) but was significantly higher in the second trimester and third trimester than in the non-pregnant state and the first trimester (all P < 0.001). A differential analysis of vWF: Ac and vWF: Ag between different blood types was conducted. As in the non-pregnant population, the results showed that there were statistical differences between blood type O and non-O in all pregnancy period. vWF: Ac and vWF: Ag results with type non-O is significantly higher than type O, reference intervals should be established according to blood type.Therefore, separate reference intervals should be established for blood type O and non-O and for each pregnant period.
Discussion
The hemostasis system consists of procoagulant, anticoagulant, and fibrinolytic system, which interact with endothelial cells and blood cells to maintain a complex balance that prevents hemorrhage and thrombosis. Pregnancy is a unique physiological state that physiological changes make pregnant women more susceptible to hemorrhage and thrombosis. The placental vascular interface is prone to maternal bleeding, hence the maternal body exhibits compensatory hypercoagulable state, including increased factor VIII, von Willebrand factor, fibrinogen, thrombin generation and increased plasminogen activator inhibitors, as well as resistance to activated protein C, decreased free protein S, etc. 5
Hypercoagulable during pregnancy may lead to life-threatening complications. Timely monitoring and assessment of the hemostasis status of pregnant women, and with appropriate intervention, can help reduce the risk of mortality. 6 A reasonable reference interval is the foundation of laboratory testing, and an important criterion for clinical disease diagnosis. Due to physiological changes, the procoagulant, anticoagulant, and fibrinolytic indicators of pregnant women are significantly different from those in the normal population. Reference intervals for routine coagulation tests have been published at home and abroad,7,8 but there are very few studies on the anticoagulant and fibrinolytic indicators reference intervals for healthy pregnant women at different pregnant periods. In this study, strict screening criteria were adopted to select healthy pregnant women for the tests of anticoagulation and fibrinolysis indicators and preliminarily reference intervals for thirteen related indicators of anticoagulation and fibrinolysis in healthy pregnant women at different pregnant periods were established.
In this study, the changes in anticoagulant proteins at different pregnant periods are shown in Figure 1. It was found that AT, FPS, and PS Ac during pregnancy are significantly lower than those during non-pregnancy, and there are obvious changes and differences in AT, FPS, and PS Ac during different pregnant periods, and corresponding reference intervals should be established separately. Our study is consistent with previous domestic studies.9,10-12 However, some studies on Caucasians show that AT activity remains unchanged during pregnancy, which may be related to racial and geographical environmental differences.1,13PS is a large molecular VK-dependent protein, more than half of which is bound to C4b, and only free PS acts as anicoagulant through two mechanisms, one is as a cofactor of PC, accelerating the inactivation of FVa and FVIIIa, and the other is that PS can directly inhibit FXa and prothrombin. This study found that FPS gradually decreases as the gestational age increases, this is consistent with a series of previous studies.1,10,14,15,16 Similar results were also observed in PS:as gestational age increased, PS gradually decreased, and PS Ac in the third trimester was significantly lower than in the first trimester. Clark P and other studies also confirmed that total protein S and free protein S decreased with the increase of gestation age increases. 14 The decrease in free PS and PS with gestational age may be due to reduced physiological synthesis. The physiological decrease of anticoagulant proteins activity such as AT, PS Ac, and FPS in the third trimester is beneficial for hemostasis of placenta abscission surface and prevent massive hemorrhage in parturient women.

a-m: Box Plots of Anticoagulant and Fibrinolysis Indicators in non-Pregnant Group and at Three Pregnant Trimesters. Note: 1 Represents the non-Pregnant Group, 2 Represents the First Trimester, 3 Represents the Second Trimester, and 4 Represents the Third Trimester. the Upper and Lower Edges of the box Plots Represent the 75th Percentile and the 25th Percentile, and the Middle Black Line in the box Plot Represents the Median.
This study found that PC activity during non-pregnancy was no significant difference with it in the first trimester and the third trimester. PC activity in the second trimester was obviously higher than the non-pregnancy, the first trimester and the third trimester, while PC activity in the third trimester was higher than the first trimester. The PC changing trend showed some difference with some studies,9,10 this may be due to biases in the selection of research objects, experimental operation related factors or other unknown reasons. otherwise, our results are consistent with more studies.14,13,17 The studies of Mahieu B et al shows that there is a strong negative correlation between APC-R and protein C during pregnancy and postpartum, which proved that when there was a high level of protein C during pregnancy, APC-R activity will decrease may be due to steric hindrance of PC to APC binding sites on FV and/or PS during pregnancy. 18 The level of PC during pregnancy cannot represent its anticoagulant activity, and the change of APC-R degree is more obvious. Paternoster DM et al showed that the ratio of activated protein C began to decrease significantly after the second trimester, and the decrease was most obvious in the third trimester. Compared with normal pregnancy, the ratio of activated protein C in preeclampsia patients was significantly lower. 19
In order to clarify which indicator is related to the increased fibrinolytic activity during pregnancy, we tested PI and PLG. There is controversy about the changes in the fibrinolytic activity during pregnancy. Some studies showing a decrease in plasminogen, 20 others showing an increase 21 or no change. 22 Plasminogen (PLG) is a single-chain glycoprotein synthesized by the liver. When the vascular endothelium is damaged, a large amount of tissue plasminogen activator secreted by endothelial cells transforms plasminogen into plasmin, which can lead to fibrinolysis. In this study, during the second and third trimester PLG was significantly higher than that during non-pregnancy and the first trimester. The body is in a hypercoagulable state during the second and third trimester, and the increase of PLG may be related to increased fibrinogen and reduced anticoagulant function. A domestic study shows that the fibrinolysis indicators in the PIH group and the healthy third trimester group are significantly higher than the healthy non-pregnant group, and compared with the healthy pregnancy group, the fibrinogen, PLG, D-dimer, and PI in the second trimester of severe PIH group are significantly increased, and showed an increasing trend with the aggravation of the disease. The detection of fibrinolysis indicators has certain clinical significance for preventing the development of PIH and the formation of disseminated intravascular coagulation. 23 The study of Natalia B et al also shows that the plasminogen activity decreasing in pregnant women in the first trimester indicates a disorder of the hemostasis system, which is related to the formation of subchorionic hematoma, and it is recommended to measure plasminogen activity during pregnancy for prevention. 24
Plasminogen inhibitors (PI) is rarely involved in previous studies, but as an important part of the fibrinolytic balance, it can neutralize free plasmin to form inactive plasmin-antiplasmin complexes, so that fibrinolysis is limited to the coagulation place, effectively preventing hyperfibrinolysis, and it is also important in the detection of fibrinolysis function. In this study, PI in the first trimester was significantly higher than in the non-pregnancy, the second trimester and the third trimester. As the increase of pro-coagulation indicators, such as fibrinogen, FVIII, vWF: Ag in the second and third trimesters, the increase of PLG while the non-increase of PI can enhance fibrinolytic activity and maintain the dynamic balance of pro-coagulation and anticoagulation.
DDimer and FDP, as the fibrinolytic products, are important screening indicators for venous thrombosis and disseminated intravascular coagulation. In patients with moderate and severe pregnancy-induced hypertension, the DDimer was significantly higher than healthy pregnant women in the third trimester. Increased DDimer indicates intravascular micro-thrombosis, and secondary fibrinolysis enhancement significantly increase the DDimer level. 20 In this study, the levels of DDHS and FDP gradually increased throughout the pregnancy and peaked in the third trimester, which is consistent with the results of previous studies.7,10,25−30 There are two commonly used units for DDimer measurement, the unit for DDHS is DDU, and for D-DHS500 is FEU. These two tests detect different DDimer fragments, and there are significant differences in the values, so they can not use the same reference ranges. Therefore, this study ran and analysed these two tests separately. FDP is a marker of primary fibrinolysis. In this study, the change of FDP during pregnancy was similar to DDimer, which was significantly higher than non-pregnancy and gradually increased throughout the pregnancy, being consistent with previous studies.11,31 DDimer and FDP increases throughout the pregnancy. So using of DDimer and FDP reference intervals derived from the non-pregnant population for pregnant women has limited clinical value and may lead to misdiagnosis of thrombotic diseases.12,32,33
LA is a pathological anticoagulant protein, an antiphospholipid antibody, which is closely associated with thrombosis, recurrent miscarriage, and preeclampsia.34,35 In this study, SCT at the third trimester was significantly lower than in the non-pregnancy, the first trimester and the second trimester. The lupus anticoagulant normalized SCT ratio is a silicon-activated clotting test. A decrease in the normalized SCT ratio may be related to shortening of SCT clotting time due to factors such as increased factor VIII, fibrinogen, and thrombin generation, as well as decreased anticoagulant in the late pregnancy. Another LA test— the normalized ratio dRVVT showed an increase in the second trimester and the third trimester of pregnancy, which is consistent with previous studies. 12 This may indicate a slight increase in antiphospholipid antibodies during the second and third trimester of pregnancy. Monitoring LA during pregnancy is very important. As the trend of lupus anticoagulant tested by two methods in the third trimester of pregnancy may be inconsistent, leading to difficulties in clinical judgment. Therefore, the application of reference interval for pregnant women of corresponding gestational age makes clinical diagnosis more secure.
vWF plays an important role in platelet adhesion and aggregation. In this study, vWF:Activity and vWF:Ag increased throughout the pregnancy, which is consistent with the results of previous studies. 25 ABO blood type is a genetic factor affecting vWF levels. We analyzed the vWF levels of pregnant women with type O and type non-O in different gestational stages. Type non-O was significantly higher than type O. So, reference intervals should be established separately. Studies have shown that antiphospholipid antibodies in patients with anti-phospholipid syndrome promote platelet activation by increasing plasma vWF activity and increase the risk of arterial thrombosis. 36 To establish vWF:Ac and vWF:Ag reference intervals separately according to pregnancy periods is helpful to predict the risk of thrombosis in pregnancy.
Our study has some limitations, lacking postpartum data and being a single-center source. Therefore, it is necessary to continue to conduct large-sample and multi-center studies in the future.
In summary, timely monitoring and evaluation of the anticoagulant and fibrinolysis status of pregnant women will help to promptly discover obstetric hypercoagulation-related complications. There are obvious differences between anticoagulation and fibrinolysis indexes in pregnant woman and the normal population, and using the reference interval of normal adults for pregnant woman may lead to misdiagnosis. It is necessary to establish exclusive reference ranges for pregnant women at different pregnant period. In this study, strict screening criteria were adopted to screen healthy pregnant women, and reference intervals of anticoagulation and fibrinolysis indicators were established in different pregnant period, which provided necessary references for the clinical use of these indicators.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.