
Abstract
Carotid artery stenosis (CAS) is one of the main risk factors of ischemic stroke (IS), which needs a screening and monitoring biomarker. The study focused on the clinical significance of long non-coding RNA (lncRNA) HCG11 in CAS patients aiming to identify a potential therapeutic target for CAS. Serum samples were collected from 70 CAS patients and 80 age- and gender-matched healthy people. HCG11 levels were measured via quantitative real-time PCR (qRT-PCR), and its significance in CAS identification and development prediction was also assessed. HCG11 was enriched in the serum of CAS patients, and serves as a possible biomarker for disease diagnosis with the area under the curve (AUC) of 0.930. Elevated expression of HCG11 was significantly correlated with hypertension, dyslipidemia, and degree of carotid stenosis. HCG11 was highly expressed in severe CAS cases compared to moderate ones, which was positively related to the disease severity. Cox regression analysis determined the close relationship of serum HCG11 with the occurrence of cerebral ischemia events. CAS patients with high HCG11 expression showed a high occurrence rate of cerebral ischemia events. The upregulation of HCG11 could serve as a potential diagnostic biomarker for CAS and is positively related to the disease severity. Serum HCG11 can independently predict the occurrence of following cerebral ischemia events.
Introduction
Carotid artery stenosis (CAS) refers to vascular stenosis occurring in a large cervical artery caused by atherosclerosis (AS). 1 The incidence of CAS is one of the main risk factors of ischemic stroke (IS) clinically, which seriously threatens the life safety of patients. 2 Dyslipidemia, diabetes, and hypertension are independent risk factors for CAS. 3 Clinically, digital subtraction angiography (DSA) and magnetic resonance imaging (MRI) are common methods for the diagnosis of AS. 4 However, due to their invasive or exorbitant price, their clinical application is limited.5,6 Although CAS progresses slowly, it can be fatal when occurs. 7 Therefore, early diagnosis of CAS at the asymptomatic stage, may contribute to stroke prevention and therapeutic intervention, thereby reducing the incidence of IS.
Recently, the role of non-coding RNAs (ncRNAs) in the onset and progression of human diseases has been focused widely. 8 As a portion of the epigenetic posttranscriptional regulation landscape, long non-coding RNA (lncRNA) can mediate the pathophysiology of CAS, favoring the development of CAS, such as GAS5 9 and SNHG1. 10 Here we focused on the human vascular endothelial cell (HUVEC)-enriched lncRNA HCG11. 11 An independent study has demonstrated that HCG11 is altered in acute coronary syndrome patients with vulnerable plaque. 11 Functionally, HCG11 downregulation can partially offset the inhibitory role of oxidized low-density lipoprotein (ox-LDL) in the cell viability of HUVECs. 12 In vascular smooth muscle cells (VSMCs), overexpression of HCG11 facilitates cell proliferation and suppresses cell apoptosis. 13 The existing reference implies the essential role of HCG11 in AS, as well as AS-related CAS.
The present study aimed to delve into the dysregulation and diagnostic value of lncRNA HCG11 in CAS patients. Moreover, we also got insight into the correlation of HCG11 with disease severity, and its prognostic value was also examined.
Materials and Methods
Patients’ Inclusion
Seventy individuals with CAS and 80 age and gender-matched healthy people who were admitted to Yantaishan Hospital were recruited in the present study. Patients’ recruitment, participation, and sample collection were approved by the Ethics Committee of Yantaishan Hospital. Each patient signed a written informed consent for the use of the samples.
Inclusion criteria of CAS patients: (1) age ≥30 years old; (2) ability to provide informed consent. Exclusion criteria: (1) previous history of stroke, transient ischemic attack, or coronary artery disease to avoid data bias; (2) subjects on active antiplatelet and/or anticoagulant therapy within 6 months; (3) patients with related intracranial diseases that can trigger ischemic attacks, including severe leukoencephalopathy (Fazekas grade II/III), cerebrovascular malformation or family history of cerebrovascular malformation and intracranial infection; (4) participants with severe heart (LVEF ≤ 40% or Pro-BNP >1800 pg/ml), liver (ALT or AST >200 U/L), kidney failure (urea >8 mmol/L and creatinine >106 ml/min); and (5) patients with neurodegenerative diseases including Parkinson's disease or Parkinson's combination. All cases underwent carotid ultrasonography for routine health screening tests, then the CAS suspicious patients received MRI and CTA examination for the final diagnosis. All image sets were evaluated by two cerebrovascular radiologists with >4 years of experience in interpreting MRA and CTA studies. Based on the MRA or CTA examination results, patients with the vascular diameter stenosis percentage of more than 50% were classified into the CAS group. If cases with tandem or multiple stenosis, the highest stenosis site was considered in the analysis. Based on the degree of carotid artery stenosis, all CAS patients were categorized into moderate group (50% ≤ carotid artery stenosis < 70%) and severe group (carotid artery stenosis ≥ 70%). 14 Based on the carotid ultrasonography, carotid CTA or postoperative plaque pathology results at the time of admission, at least two examinations were required to indicate a vulnerable plaque for inclusion in the vulnerable plaque group; otherwise, the stable plaque group was included. Participants with carotid artery stenosis <20% were selected in the control group, who underwent carotid artery ultrasound to avoid the appearance of CAS.
Collection of General Clinical Data and Laboratory Indicators
Demographic, medical history, and blood biochemical results were collected from each subject. Age, sex, body mass index (BMI), previous smoking history, hypertension history, diabetes history, systolic blood pressure (SBP), and diastolic blood pressure (DBP) were recorded. Routine laboratory tests were performed for the data collection of fasting blood glucose and levels of total cholesterol (TC) and triglycerides (TG).
Hypertension was defined as DBP ≥ 90 mmHg/SBP ≥ 140 mmHg or the administration of anti-hypertensive agent. 15 The diagnosis of diabetes was determined based on the results of oral glucose tolerance test (OGTT) or the use of insulin/oral hypoglycemic agent. 16 The diagnosis of hyperlipidemia was confirmed based on the 2016 Chinese guidelines for the management of dyslipidemia in adults. 17
Quantitative Real-Time PCR (qRT-PCR)
After fasting for 12 h, 5 ml of upper limb vein blood was obtained from each subject. Using TRIzol reagent (Invitrogen, USA), total RNA was isolated from the serum samples. For reverse transcription, one microgram RNA was applied for the synthesis of first-strand cDNA under the help of FastKing gDNA Dispelling RT SuperMix (TIANGEN Biotech, Beijing, China) and PCR amplification. Then, the primers for the amplification of each gene were added, which were synthesized by Sangon (Shanghai, China). mRNA levels were measured using a SuperReal PreMix Plus (SYBR Green) (TIANGEN Biotech, Beijing, China). Following PCR, quantification data were normalized with the GAPDH, applying the 2−ΔΔCt method.
Follow up
All cases with CAS were followed up for 24 months to monitor the occurrence of cerebral ischemia events. The end-point events include transient ischemic attack (TIA), stroke, and related mortality caused by CAS. 18
Statistical Analysis
All statistical analysis and plotting were accomplished by SPSS Statistics 21.0 and GraphPad 7.0 software. The data were presented as mean and standard deviation (SD). Based on HCG11 levels in different groups, the receiver operating characteristic (ROC) curves were drawn for the diagnostic significance evaluation. The survival analysis was accomplished via Kaplan–Meier (K–M) curve with the help of log-rank test. The independent influence factors related to survival were assessed through cox regression analysis. The P value less than 0.05 was set as the criteria for a significant difference.
Results
Basic Information of the Study Objects
The primary clinical information is depicted in Table 1. The recruited healthy individuals and CAS patients showed matched age and gender composition with insignificant differences. In addition, the BMI, history of smoking, hypertension, diabetes, and dyslipidemia were also not significantly different (P > 0.05). Concerning laboratory indicators, CAS cases had elevated levels of TC, LDL-C, and SBP with significant differences relative to the healthy people (P < 0.05). Other indicators exhibited no significant difference between the two groups, including TG, HDL-C, FBG, and DBP (P > 0.05).
Basic Information of the Study Objects.

Abbreviations: CAS, carotid artery stenosis; BMI, body mass index; TC, total cholesterol; TG, triglyceride; HDL-C, high-density lipoproteincholesterol; LDL-C, low-density lipoproteincholesterol; FBG, fasting blood glucose; SBP, systolic blood pressure; DBP, diastolic blood pressure. Bold items indicate statistically significant differences.
Dysregulated lncRNA HCG11 in CAS Patients
As displayed in Figure 1A, qRT-PCR analysis results determined the enrichment of lncRNA HCG11 in the serum of CAS patients relative to the controls (P < 0.001). Based on serum HCG11 levels in the control and CAS groups, the usefulness of serum HCG11 as a possible biomarker for CAS was evaluated. It was implied from the ROC curve that serum HCG11 was a good serum biomarker to differentiate CAS from healthy individuals (AUC = 0.930, P < 0.01; Figure 1B). Moreover, based on the carotid ultrasonography, carotid CTA, or postoperative plaque pathology results, 29 cases with vulnerable plaque among 70 CAS patients. And cases in the vulnerable group owned high levels of HCG11 (P < 0.001; Figure 1B).

Dysregulated lncRNA HCG11 in CAS patients. (A) LncRNA HCG11 was enriched in the serum of CAS patients. (B) ROC curve of serum HCG11 in differentiating CAS from healthy controls. (C) Cases in the vulnerable group owned high levels of HCG11.
Association of lncRNA HCG11 with the Clinical Parameters in CAS Patients
The relationship between HCG11 expression and clinical parameters was explored. Based on the mean value of HCG11, 70 CAS patients were classified into low HCG11 expression group (n = 31) and high HCG11 expression group (n = 39). As seen in Table 2, in patients with high HCG11 values, a larger proportion of patients had a history of hypertension, hyperlipidemia, and a higher degree of carotid stenosis (P < 0.05). The data implied that elevated expression of HCG11 was significantly correlated with hypertension, dyslipidemia, and degree of carotid stenosis.
Association of lncRNA HCG11 with the Clinical Parameters in CAS Patients.

Abbreviation: CAS, Carotid artery stenosis. *P < 0.05.
Correlation of HCG11 with CAS Severity
All CAS patients were stratified depending on the degree of carotid stenosis, in which 26 cases had moderate CAS and the remaining 44 individuals had severe CAS. As seen in Figure 2A, we found that the expression of HCG11 was higher in severe CAS cases compared to moderate ones, and the result was statistically significant (P < 0.001).

Correlation of HCG11 with CAS severity. (A) The expression of HCG11 was higher in severe CAS cases compared to moderate ones. (B) Forest plot of logistic regression analysis to show CAS severity-related factors. ***P < 0.001.
Next, we assessed the potential impact of HCG11 on CAS severity using logistic regression analysis (Table 3). Subsequent analysis implied that high values of dyslipidemia (OR = 2.998, 95%CI = 1.013-8.786, P = 0.047) and HCG11 (OR = 3.307, 95%CI = 1.142-9.572, P = 0.027) were positively related to the disease severity after adjusting to other confounding factors (Figure 2B).
Association of Clinical Parameters with the Degree of Carotid Stenosis in CAS Patients.

Abbreviations: BMI, body mass index; OR, odds ratio; CI, confidence interval.
Prognostic Value of serum HCG11 for CAS
Then the Cox regression analysis was conducted for the prognostic value evaluation, and the results were displayed in Table 4 and Figure 3A. According to the results, both HCG11 (HR = 4.858, 95%CI = 1.174-21.106, P = 0.029) and CAS degree (HR = 5.413, 95%CI = 1.360-21.541, P = 0.017) exhibited positively association with the occurrence of cerebral ischemia events. Moreover, the K–M plot was plotted to show the prognostic performance of serum HCG11. As displayed in Figure 3B, CAS patients with high HCG11 expression showed a high occurrence rate of cerebral ischemia events relative to those with low HCG11 expression.

Prognostic value of serum HCG11 for CAS. (A) Forest plot of Cox regression analysis to show independent factors related to the occurrence of cerebral ischemia events. (B) K–M plot to show the prognostic performance of serum HCG11 in the occurrence of cerebral ischemia events.
Association of Clinical Parameters with Clinical Prognosis in CAS Patients.
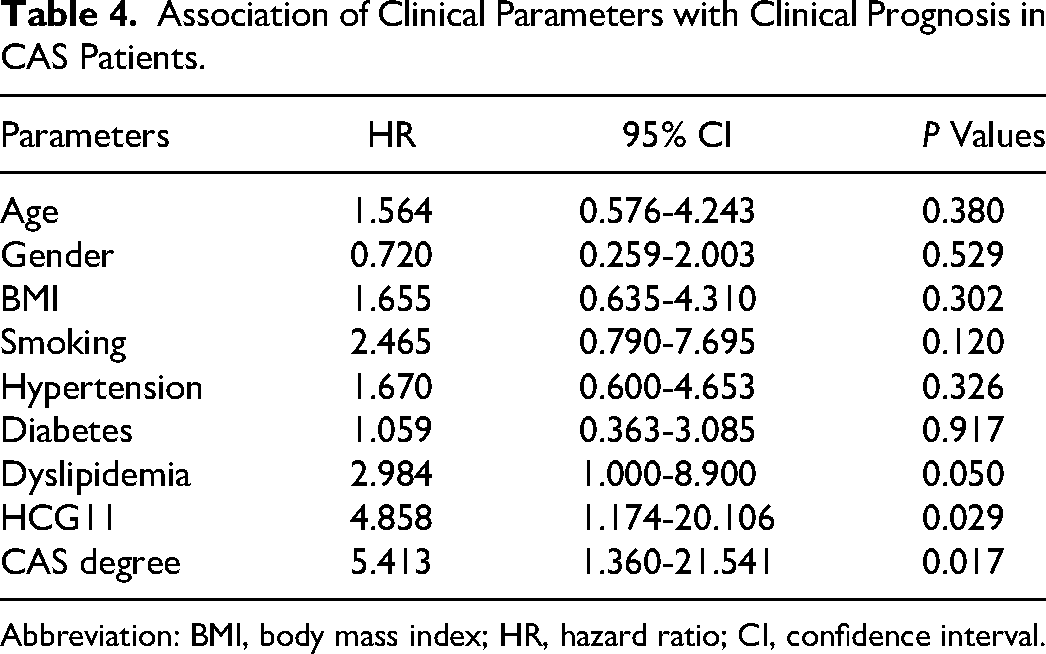
Abbreviation: BMI, body mass index; HR, hazard ratio; CI, confidence interval.
Discussion
Existing evidence has presented that CAS is the major inducing factor of cerebral circulation insufficiency, with the initial factor of AS. 19 Stenosis degree is the main risk factor for the malignant development of IS. 20 But the mechanism that affected the development of CAS is unclear. There is sufficient evidence that increased levels of TC, TG, LDL are major risk factors for AS and can lead to thickening of the arterial wall. 21 In this study, CAS cases had elevated levels of TC, LDL-C, which is consistent with the previous reports. In addition, the progression of AS is associated with hypertension, in which the role of SBP is more prominent.22,23 In the present cases, CAS patients presented higher values of SBP than the controls, the phenomenon was consistent with previous findings.22,23 However, the distribution of both dyslipidemia and dyslipidemia carriers between the case and control group was not in significantly different. Although CAS group had a high proportion of cases with a history of dyslipidemia and hypertension, the difference did not reach significant levels. The most likely reason for the inconsistent results might be the inadequate sample size.
With the progress of molecular mechanisms, the identification of CAS development-related molecules has received wide attention. Several lncRNAs have been determined to be closely related to the occurrence and development of CAS. For instance, lncRNA GAS5 is determined to be downregulated in the serum of CAS patients, its function is related to the regulatory effect on VSMCs. 9 Upregulated lncRNA THRIL is also identified as a biomarker for CAS, that can distinguish asymptomatic CAS patients and predict the poor prognosis. 24 In the present study, the enrichment of lncRNA HCG11 was determined in the serum of CAS patients relative to the controls. Moreover, the usefulness of serum HCG11 as a possible biomarker for CAS was evaluated. It was determined that serum HCG11 was a good serum biomarker to differentiate CAS from healthy individuals. Moreover, the relationship between HCG11 expression and clinical parameters was explored. The results indicated that elevated expression of HCG11 was significantly correlated with hypertension and dyslipidemia. The close relationship offers promising research directions in view of the involvement of hypertension and dyslipidemia in the progress of CAS. 25
Moreover, in patients with high HCG11 values, a larger proportion of cases had high degree of carotid stenosis, implying the potential value of HCG11 in CAS severity. Consistently, the significantly high value of serum HCG11 was detected in severe CAS patients. Based on the logistic regression analysis results, serum HCG11 was determined to be an independent mediator for CAS severity. HCG11 is a HUVEC-enriched lncRNA, and its role in HUVEC function has been widely reported. In ox-LDL-induced HUVECs, elevated HCG11 was tested, which was correlated with the cell viability decline and inflammation. 12 That can accelerate the progress of AS. 12 Impaired endothelial function accompanied by the elevated HCG11 might be the underlying mechanism in AS. In addition, HCG11 is also determined to promote the proliferation of VSMCs. 13 It is known that the restriction of HUVECs and immoderate proliferation of VSMCs contribute to the formation of the neointima membrane, ultimately accelerating the progress of CAS. 26 Moreover, in patients with acute coronary syndrome, enhanced HCG11 is also detected in cases with vulnerable plaque. 27 Fragile atherosclerotic plaques are closely related to cerebral ischemia events, their rupture and caused distal embolization is the major cause of acute cerebrovascular events.28,29 Therefore, all patients included in the current study were followed up for two years to record the occurrence of cerebral ischemia events. As expected, the independent influence relationship was identified between serum HCG11 and the occurrence of cerebral ischemia events according to the Cox regression analysis results. Moreover, the K–M plot was plotted to assess the prognostic performance, and CAS patients with high HCG11 expression showed a high occurrence rate of cerebral ischemia events relative to those with low HCG11 expression. However, the sample size was relatively small and the follow-up time was limited, that might be the limitations of our study. In the future, the present findings should be confirmed in much larger sample size, optimally in multi-centric studies. In addition, a longer follow-up time should be considered. And other biochemical carotid plaque features except for plaque stability are absent in the current study, which should be included in the future for a deep understanding of HCG11 in the development of CAS.
Taken together, the upregulation of HCG11 in CAS could serve as a potential diagnostic biomarker screening the occurrence of CAS. Moreover, serum HCG11 levels are positively related to the disease severity, and can independently predict the occurrence of following cerebral ischemia events.
Footnotes
Availability of Data and Materials
The data used and analyzed can be obtained from the corresponding author under a reasonable request.
Consent to Participate
A signed written informed consent was obtained from each patient.
Consent for Publication
A written informed consent for publication was obtained from each participant.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval
The experimental procedures were all in accordance with the guideline of the Ethics Committee of Yantaishan Hospital and have approved by the Ethics Committee of Yantaishan Hospital. This study complies with the Declaration of Helsinki.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.