
Abstract
To investigate the significance of thrombelastography (TEG) in patients who have lung adenocarcinoma in situ (LAIS) complicated with type 2 diabetes (T2D), 120 subjects were enrolled: 40 with LAIS, 40 with LAIS and T2D (LAIS + T2D), and 40 healthy controls (HCs). Correlation analysis was used to assess the relationships of TEG with indicators of T2D. The LAIS + T2D group had lower reaction time (R), rate of clot formation (K), estimated percentage of lysis (EPL), and lysis after 30 min (LY30), but higher maximum amplitude (MA), angle (α), and coagulation index (CI) than other group. Compared with the HC group, the LAIS group had lower R, K, EPL, and LY30, but higher MA, α, and CI. In LAIS + T2D group, R and LY30 had negatively correlations with fasting blood glucose (FBG) and triglycerides (TGs); α and MA had positive correlations with FBG and TG; K had negative correlations with FBG; EPL had negative correlations with FBG and low-density lipoprotein (LDL); and CI had positive correlations with FBG and LDL. TEG may be a useful indicator of blood coagulation dysfunction in these patients rather the healthy individuals.
Introduction
Lung cancer is a malignant tumor whose worldwide morbidity and mortality rates are increasing more rapidly than those of any other cancer. 1 Tumor cells often affect the coagulation function of patients during the processes of invasion, metastasis, and secretion, and the blood of these patients is often in a state of hypercoagulation. 2 Type 2 diabetes (T2D) is a common metabolic disorder that can also cause anticoagulation dysfunction, in addition to vascular endothelial injury and platelet dysfunction. 3 Lung cancer is among the top three malignant tumors in patients with T2D. Thus, it is likely that the increasing incidence of T2D is related to the increasing incidence of lung cancer. 4 Lung adenocarcinoma is one of the three main histological types of lung cancer, and patients with advanced stages of lung adenocarcinoma have poor outcomes. Patients with aggressive lung adenocarcinomas can even reach the survival rate of 70%. 5 Given the rising co-occurrence of lung adenocarcinoma complicated with T2D, 6 it is critical to identify additional indicators or biomarkers for the diagnosis, selection of therapy, and prognostic evaluation of these patients.
Thrombelastography (TEG) is one of the most important methods for monitoring coagulation function in clinical practice. 7 TEG monitors the process of blood coagulation and dissolution based on the levels and functions of fibrin and platelets. 8 At present, TEG is widely used to guide clinical blood transfusion and the use of medications that affect platelet function, for real-time monitoring of coagulation in patients with a variety of conditions, and to predict the risk of venous thrombosis. 9 Patients with lung adenocarcinoma in situ (LAIS) who receive prompt diagnosis and surgery have excellent prognoses, but untreated LAIS can progress to invasive lung adenocarcinoma. Few studies have examined the relationship of thrombelastography results with LAIS in patients with T2D.
In the present study, we aim to compare the TEG results of healthy controls, patients with LAIS, and patients with LAIS complicated with T2D (LAIS + T2D). Our general purpose was to identify the clinical significance of changes in the thrombelastogram in patients with LAIS + T2D rather healthy individuals.
Methods
General Information
From June 2020 to December 2020, 40 patients with LAIS and 40 patients with LAIS + T2D were enrolled. There were 20 females per group and the average age was 65.65 ± 9.12 years in the LAIS + T2D group and 61.20 ± 8.56 years in the LAIS group. All these patients had confirmed LAIS based on postoperative pathology. The diagnosis of LAIS was according to the 2011 TNM staging criteria for tumor in situ (TIS) from the 2011 guidelines of the International Association for the Study of Lung Cancer (IASLC) and the American Thoracic Society (ATS) and the European Respiratory Society (ERS). 10 T2D diagnosis was according to the 1999 WHO diabetes diagnostic criteria. 2 A total of 40 healthy individuals (20 males and 20 females) who were 60.48 ± 11.87 years-old were in the healthy control (HC) group, all of whom received oral glucose tolerance tests (OGTTs) to exclude T2D. This study was approved by the ethics committees of The First Affiliated Hospital of Soochow University (2020-072), and this study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. Written informed consent was obtained from all participants prior to their enrollment.
Inclusion and Exclusion Criteria
The inclusion criteria for the LAIS and LAIS + T2D groups were diagnosis of LAIS with or without T2D. The exclusion criteria for all three groups were: type 1 diabetes, special type of diabetes, gestational diabetes, cardiovascular or cerebrovascular disease, hypertension, autoimmune disease, acute or chronic infection, severe liver or kidney disease, any endocrine system disease, or receipt of any anticancer or anticoagulant therapy. Data were collected from LAIS + T2D patients prior to surgery.
Experimental Methods
Venous blood samples (15 mL) were collected from all participants 12 h after fasting. A 5 mL sample was used for complete biochemical testing using a Hitachi 7600 automatic biochemical analyzer that determined total cholesterol (TC), triglycerides (TGs), high density lipoprotein cholesterol (HDL-C), low density lipoprotein cholesterol (LDL-C), and fasting blood glucose (FBG). Another 5 mL sample was used for TEG measurements using a Haemonetics TEG 5000 Hemostasis Analyzer System. Seven key parameters from these TEG results were used for analyses: reaction time (R, min), rate of clot formation (K, min), maximum amplitude (MA, mm), angle (α, degrees), estimated percentage of lysis (EPL, %), coagulation index (CI, dimensionless), and percentage of clot lysed after 30 min (LY30, %).
Data Analysis
Prism version 7 software was used for statistical analysis. Measurement data were expressed as means ± standard deviations. Comparisons of the three groups were performed using a multivariate one-way analysis of variance (ANOVA) and a t-test was used for comparisons of two groups. Correlation analysis was performed by calculation of Pearson's r. A P value below 0.05 was considered significant.
Results
Demographic and Clinical Characteristics of the Three Groups
The LIAS, LAIS + T2D, and HC groups had no significant differences in gender, age, TG, TC, or HDL-C (all P > 0.05; Table 1). However, ANOVA indicated the LDL-C level was greater in the LAIS + T2D group than in the LAIS and HC groups (both P < 0.05) and that the FBG was greater in the LAIS + T2D group than in the LAIS and HC groups (both P < 0.01).
Demographic and Clinical Characteristics of the Three Groups.
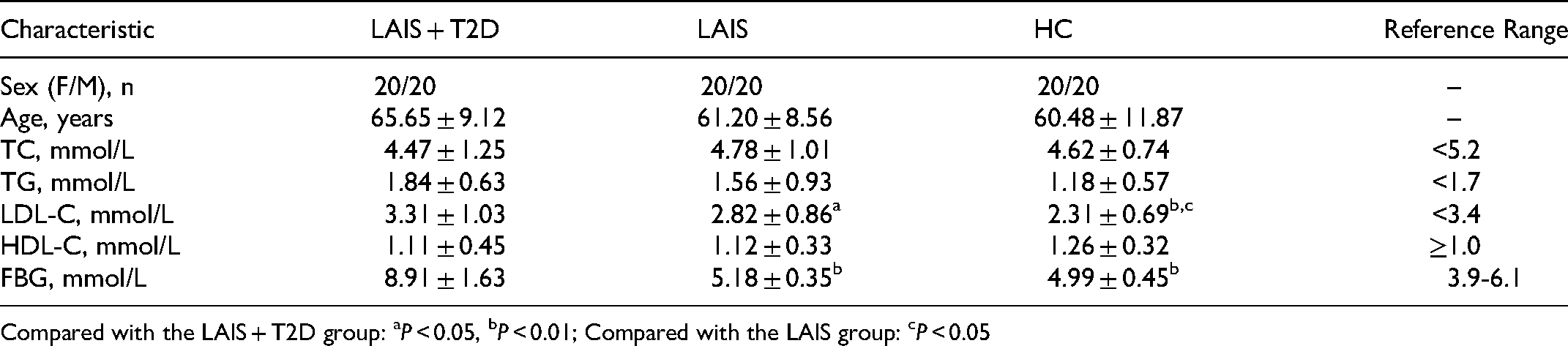
Compared with the LAIS + T2D group: aP < 0.05, bP < 0.01; Compared with the LAIS group: cP < 0.05
Postoperative TEG of Coagulation Function of the Three Groups
We compared seven key postoperative TEG parameters (R, MA, K, α, EPL, LY30, and CI) in the three groups (Figure 1, Table 2). The R of the LAIS + T2D group was lower than in the LAIS group (P < 0.05) and the HC group (P < 0.01), and the R of the LAIS group was lower than in the HC group (P < 0.05). The MA of the LAIS + T2D group was higher than in the LAIS group (P < 0.05) and the HC group (P < 0.01), and the MA of LAIS group was higher than in the HC group (P < 0.01). The K of the LAIS + T2D was lower than in the LAIS group (P < 0.05) and the HC group (P < 0.01), and the K of the LAIS group was lower than in the HC group (P < 0.01). The α of the LAIS + T2D group was higher than in the LAIS group (P < 0.05) and the HC group (P < 0.01), and the α of the LAIS group was also higher than in the HC group (P < 0.05). The EPL of the LAIS + T2D was lower than in the LAIS group (P < 0.01) and HC group (P < 0.01), and the EPL of the LAIS group was lower than in the HC group (P < 0.01). The LY30 of the LAIS + T2D group was lower than in the LAIS group (P < 0.01) and the HC group (P < 0.01), and the LY30 in the LAIS group was lower than in the HC group (P < 0.01). The CI of the LAIS + T2D was higher than in the LAIS group (P < 0.05) and HC group (P < 0.01), and the CI of the LAIS group was higher than in the HC group (P < 0.05). Taken together, these findings indicate that for all seven TEG parameters, the LAIS group had greater deviations from the reference range than the HC group, and the LAIS + T2D group had greater deviations from the reference range than the LAIS group.

Postoperative TEG results in the HC, LAIS, and LAIS + T2D groups. Compared with the LAIS + T2D group: aP < 0.05, bP < 0.01; compared with the LAIS group: cP < 0.05, dP < 0.01.
Postoperative Thrombelastography Parameters in the Three Groups.
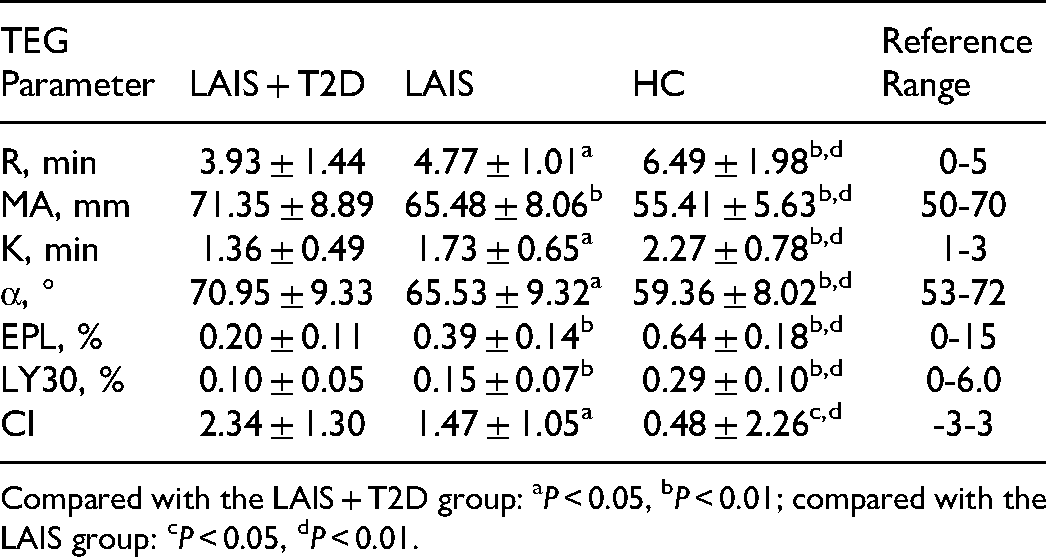
Compared with the LAIS + T2D group: aP < 0.05, bP < 0.01; compared with the LAIS group: cP < 0.05, dP < 0.01.
Correlation of TEG Parameters and T2D Indicators in the AIS + T2D Group
We also analyzed the correlations of different TEG parameters with different T2D indicators in the LAIS + T2D group (Table 3, Figure 2). The R value was negatively correlated with FBG and positively correlated with TG; MA was positively correlated with FBG and TC; K was negatively correlated with FBG; α was positively correlated with FBG and TG; EPL was negatively correlated with FBG and LDL-C; LY30 was negatively correlated with FBG and TC; and CI was positively correlated with FBG and LDL-C. Taken together, these results indicate alterations of T2D indicators in the LAIS + T2D group correlated with alterations in multiple TEG parameters.

Correlation of TEG parameters (abscissas) and T2D indicators (ordinates) in patients with LAIS + T2D.
Pearson Correlation Analysis of TEG Parameters and T2D Indicators in the LAIS + T2D Group.

The bold values are statistically significant.
Discussion
TEG is a novel method for assessing coagulation function, because it monitors the entire coagulation process from coagulation to fibrinolysis. 11 This method is thus a simple, fast, and accurate method that provides important information about the entire coagulation process. In particular, TEG considers the rate of blood clot formation and the strength of a blood clot, and can be used to assess the overall risk of bleeding, platelet dysfunction, lack of clotting factors, and fibrinolytic hyperthyroidism. 12 The R value is the time from the beginning of the test to the onset of blood coagulation. The K value is the time at which fibrin and platelets interact to form blood clots, and α reflects the speed of blood clot aggregation. MA (maximum amplitude) reflects the strength of fibrinogen and platelet coagulation. LY30 represents the percentage of blood clot dissolution within 30 min after the appearance of MA, and reflects fibrinolytic activity. EPL is clot ablation after the presence of the MA. CI is the overall coagulation index, and indicates the overall state of coagulation under different conditions.10,13
The long-term presence of high blood glucose levels in patients with T2D can contribute to impaired endothelial cell structure and function, endocrine metabolic disorders, reduced levels of nitric oxide, and increased production of endothelin-1, angiotensin-II, and glycosylation end products, all of which can lead to blood hypercoagulation. 2 Lung adenocarcinoma is also closely related to increased blood coagulation. In particular adenocarcinoma cells can activate the coagulation system through a variety of mechanisms that involve the release cytokines, such as TNF-α and IL-1β, or angiogenic factors. 14 Lung adenocarcinoma cells can also directly invade and damage the intima of blood vessels, exacerbate damage to the vascular endothelium, and promote an obvious hyper-coagulation state. 15 The occurrence, progression, metastasis, and recurrence of lung adenocarcinoma are closely related to increases in serum hypercoagulability. Several previous studies confirmed altered TEG parameters that were indicative of blood hypercoagulability in patients with AIS and in patients with T2D.14,16
Our comparisons of the TEG results in the LAIS + T2D and LAIS groups indicated the LAIS + T2D group had lower values of R, K, EPL, and LY30, but greater values of MA, α, and CI. Similarly, our comparisons of the TEG results in the LAIS and HC groups indicated the LAIS group had lower values of R, K, EPL, and LY30, but greater values of MA, α, and CI. These results suggest that patients with LAIS + T2D had the greatest clotting factor activity and fibrinogen function, the shortest blood coagulation time, the greatest thrombotic projectile strength, and overall more severe blood hypercoagulation. Our correlation analysis in LAIS + T2D patients showed that FBG had significant positive correlations (MA, α, CI) or significant negative correlations (R, K, EPL, LY30) with all TEG parameters. This is in agreement with the baseline biochemical indexes among the three groups, which showed that FBG, TG, and LDL-C levels were greater in the LAIS and LAIS + T2D groups than in the HC group. Elevated levels of blood lipids can damage to the intima of blood vessels, resulting in the deposition and adhesion of platelets and fibrinogen, and lead to the formation of atheromatous plaques, 17 increased blood viscosity, and inhibition of fibrinolysis. 18 Some indicators of TEG in the present paper were within the reference range, but we observed that there were statistical differences among the indicators in each group. Further research is needed to determine whether a more detailed reference range can be set for patients with LAIS combined with type 2 diabetes.
There are also some limitations of our study. Firstly, the sample size of the patients was a little small. Secondly, we found that TEG was quite different in patients with LAIS + T2D from T2D patients or healthy controls. However, whether TEG is correlated with the duration and severity of patients with LAIS + T2D. Thirdly, we didn't include the patients with T2D only, which was a negligence for the study. Further investigation should be conducted to perfect the significance of the present study.
Conclusion
In summary, all 40 of our patients with LAIS + T2D had abnormal TEG parameters, presumably due to their increased levels of FBG. This indicated that the blood of these patients was in a state of significant hypercoagulation, and that these patients therefore had an increased risk of thrombosis and embolism. We suggest the use of TEG for the monitoring of patients with LAIS, and especially those with LAIS + T2D, for the evaluation of preoperative blood clotting function because it may aid in the timely diagnosis of blood hypercoagulation. TEG can also help to predict the risk for intraoperative and postoperative deep vein thrombosis and pulmonary embolism. In clinical practice, patients with LAIS + T2D who have abnormal TEG parameters can be given appropriate preventive measures to reduce the probability of hypercoagulation and improve the quality of life.
Footnotes
Abbreviations
Author Contributions
Y.Z. and L.N. concepted, designed the study and revised the manuscript. K.C. analyzed the data and contributed to the discussion of the article. Q.W. created the artwork. X.D. and J.H. interpretation of the data. All authors have read and approved the final version of the manuscript.
Data Availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethic Approval
This study was approved by the ethics committees of The First Affiliated Hospital of Soochow University (2020-072), and this study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Suzhou Science, Technology and Health Bureau, (grant number SKJY2021055 to Yingyi Zhou).
Informed Consent
Written informed consent was obtained from all participants prior to their enrollment.