
Abstract
Background
High-density lipoprotein cholesterol (HDL-C) and monocytes are associated with coronary artery disease, and the ratio of monocytes to high-density lipoprotein (MHR) is associated with long-term adverse outcomes and the recurrence of atrial fibrillation. Currently, the trend of coronary heart disease proned to young people is becoming prominent. However, the relationship between MHR and in-stent restenosis (ISR) in patients with premature coronary heart disease (PCHD) has not been investigated. Therefore, we aimed to assess the relationship between MHR and ISR in patients with PCHD.
Methods
We retrospectively included 257 patients (men ≤ 55 years old, women ≤ 65 years old) with PCHD who underwent drug-eluting stent implantation and follow-up coronary angiography at the First Affiliated Hospital of Zhengzhou University from September 2016 to September 2019. Patients were divided into ISR and non-ISR groups depending on their follow-up coronary angiography results. Relative clinical information was recorded and analyzed. A receiver operating characteristic curve analysis was used to determine the optimum pre-procedural MHR cutoff value to predict ISR.
Results
Logistic regression analysis showed that MHR, smoking history, and fibrinogen were independent risk factors for ISR in patients with PCHD. The area under the receiver operating characteristic curve (AUC) of MHR was 0.750 (95% confidence interval, 0.695-0.820; P < .001), the cutoff value was 546.88, and the specificity and sensitivity were 65.2% and 78%, while the AUC of monocytes was 0.631 (95% confidence interval, 0.638-0.794; P < .001), the cutoff value was 590, and the specificity and sensitivity were 77.1% and 60.0%.
Conclusion
MHR is an independent risk factor for ISR in patients with PCHD and showed a certain predictive value.
Keywords
Introduction
With improvements in living conditions, the incidence of coronary heart disease (CHD) is rising, and the age of onset is gradually decreasing. The National Cholesterol Education Program's Third Report of the Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults defined CHD with an onset age ≤ 55 years in men or ≤ 65 years in women as premature CHD (PCHD). 1 Percutaneous coronary intervention (PCI) has become the main treatment for revascularization, but in-stent restenosis (ISR) remains a challenging problem. Although the emergence of drug-eluting stents has greatly reduced the risk of ISR, the rate of ISR is still about 5% to 10%.2,3 At present, the mechanism of ISR is unclear, but some studies have found that inflammation may be related to ISR. 4 Recently, the ratio of monocytes to HDL-C (MHR) has received widespread attention as a new inflammatory marker. 5 Inflammation and lipid accumulation are two basic characteristics of atherosclerosis. Monocytes are the main source of pro-inflammatory species during the formation of atherosclerosis, while HDL-C has a protective effect against the oxidation of low-density lipoprotein (LDL) and also directly acts on monocytes to inhibit inflammation.6,7 MHR can reflect inflammation and oxidative stress in the body. This study aims to explore the relationship between MHR and ISR in PCHD.
Methods
Study Population
This was a single-center, retrospective study. A total of 294 patients who had been diagnosed with PCHD and subjected to drug-eluting stent implantation at the Department of Cardiology of the First Affiliated Hospital of Zhengzhou University between September 2016 and September 2019 were retrospectively enrolled. According to the study exclusion criteria, we finally selected 257 patients for enrollment, including men ≤ 55 years old and women ≤ 65 years old. According to their review results, study participants were divided into a restenosis group and a non-stenosis group, with 30 cases in the restenosis group (49.89 ± 1.75 years) and 227 cases in the non-stenosis group (53.63 ± 0.60 years), respectively. Figure 1 shows the study flowchart.

Study flow chart.
Patients were excluded from this study for the following reasons: (1) clinical data or coronary angiography (CAG) data were missing; (2) their New York Heart Association functional classification was grade III or IV; (3) their cardiac color Doppler ultrasound suggested a left ventricular ejection fraction ≤ 30%; (4) they had a history of coronary artery bypass graft surgery, (5) another type of heart disease was diagnosed (eg, cardiomyopathy, congenital heart disease, or severe valvular disease); (5) they had severe liver or kidney dysfunction, a malignant tumor, an infectious disease (eg, chronic hepatitis B, chronic hepatitis C, or acquired immunodeficiency syndrome), or an autoimmune disease (Figure 2).

Receiver operating characteristic curve of the MHR in predicting ISR in patients with PCHD.
Demographic, Clinical, and Laboratory Characteristics
All data were gathered from the case records of inpatients at the First Affiliated Hospital of Zhengzhou University, including demographic, laboratory, and surgical data. We recorded gender, age, family history of CHD, hypertension, diabetes, smoking, and alcohol use as demographic and clinical data. In addition, we collected plasma and biochemical indicators, such as counts of white blood cells, neutrophils, lymphocytes, monocytes, and platelets and levels of hemoglobin, total cholesterol, uric acid (UA), creatinine, and albumin. All blood samples were venous blood collected after fasting in the morning on the second day after admission. The pre-procedure MHR was calculated by dividing the absolute count of monocytes by the HDL-C value. The surgical data included the number, length(s), and diameter(s) of stents (Figure 3).

Receiver operating characteristic curve of the MHR in predicting ISR in non-diabetic patients with PCHD.
CAG and PCI Information
Two professional interventionists performed CAG through the radial artery or femoral artery according to the standard protocol. CHD was defined during this study as the presence of more than 50% stenosis in the main trunk (left anterior descending, left circumflex, or right coronary artery) and/or the main branches of the main trunk. All patients took aspirin (loading dose, 300 mg; maintenance dose, 100 mg/day) in combination with another P2Y12 receptor antagonist, such as clopidogrel (loading dose, 600 mg; maintenance dose, 75 mg/day) or ticagrelor (loading dose, 180 mg; maintenance dose, 90 mg/twice a day). After the operation, patients were instructed to take aspirin for life and clopidogrel/ticagrelor for at least 1 year. Follow-up CAG was performed either when patients developed recurrent chest pain or between 9 and 15 months after surgery. The procedure was performed by two experienced interventionists who were unaware of the baseline test results. ISR was defined as the presence of restenosis ≥ 50% inside the stent or 5 mm proximally.
Statistical Analysis
Categorical variables are expressed as numbers and relative frequencies (percentages) and were compared using the chi-squared test. Data were tested for normal distribution using the Kolmogorov–Smirnov test. Continuous variables are expressed as mean ± standard deviation values or median (quartiles 1-3) values based on the normality assumption and were compared using the independent-samples t-test or the Mann–Whitney U test, as appropriate. A multivariate Cox regression analysis was performed, including parameters that differed significantly between the groups, in order to identify the independent predictor for ISR. A receiver operating characteristic (ROC) curve analysis was used to determine the optimum cutoff MHR in predicting ISR. A P value < .05 (two-sided test) was considered to be statistically significant. Statistical analyses were performed using SPSS version 22.0 (IBM Corporation, Armonk, NY, USA).
Results
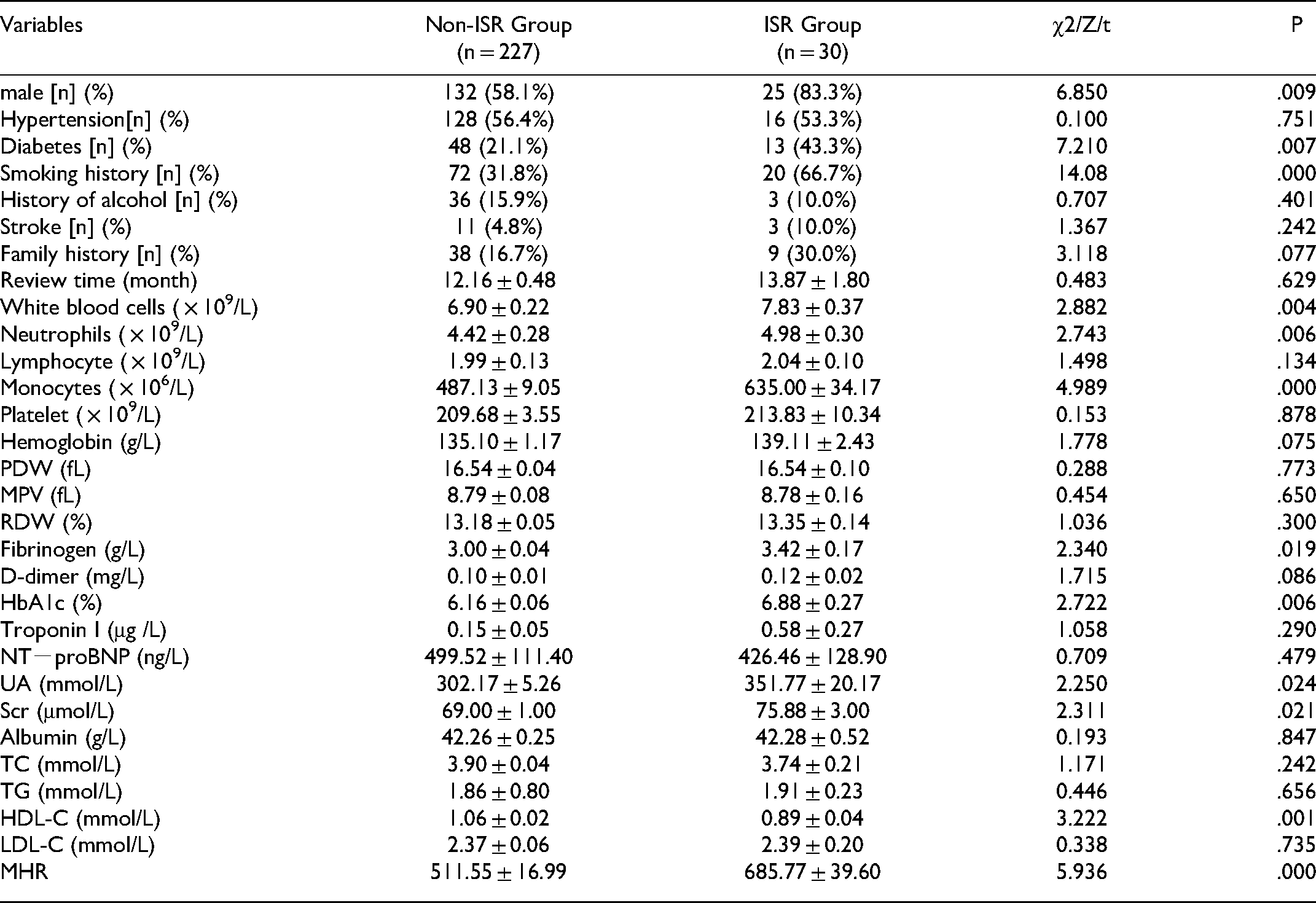
As shown in Table 1, we found that several variables were not statistically different between the two groups, including age, high blood pressure, history of drinking, family history, brain natriuretic peptide level, troponin level, lymphocyte count, hemoglobin concentration, platelet count, platelet distribution width, mean platelet volume, red blood cell distribution width, D-dimer level, albumin level, total cholesterol level, >and triglycerides. We also found that the proportion of patients with diabetes, proportion of patients with a smoking history, proportion of male patients, hemoglobin A1c value, white blood cell count, neutrophil count, fibrinogen level, UA concentration, creatinine level, monocyte count, HDL-C level, and MHR in the ISR group were higher than those in the non-ISR group, and the differences were statistically significant (P < .05).
Baseline characteristics of patients [n (%), `x ± s]
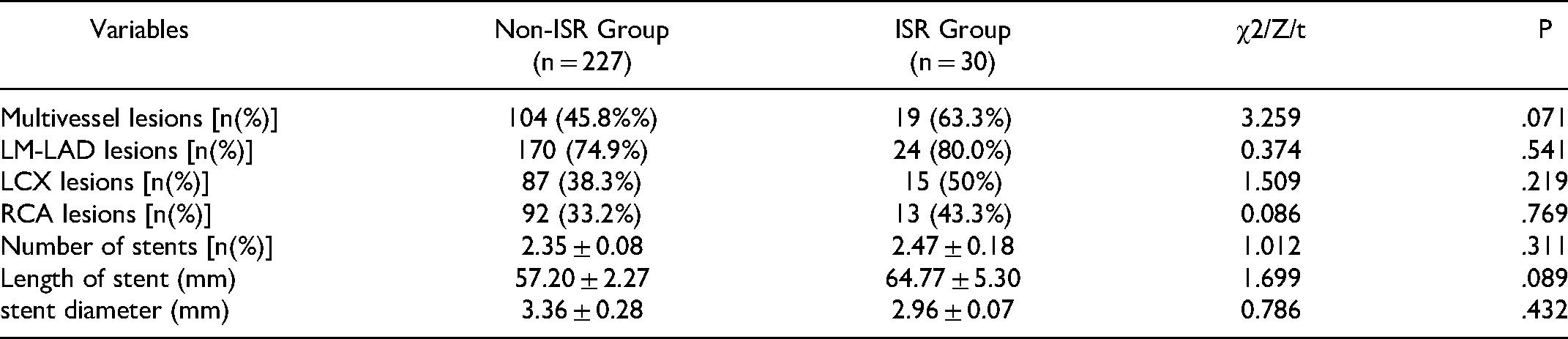
As shown in Table 2, there were no statistically significant differences in the number of target vessels, location or number of stents, stent length, and stent diameter between the two groups (P > .05).
Coronary angiography and PCI in the two groups [case (%), `x ± s].
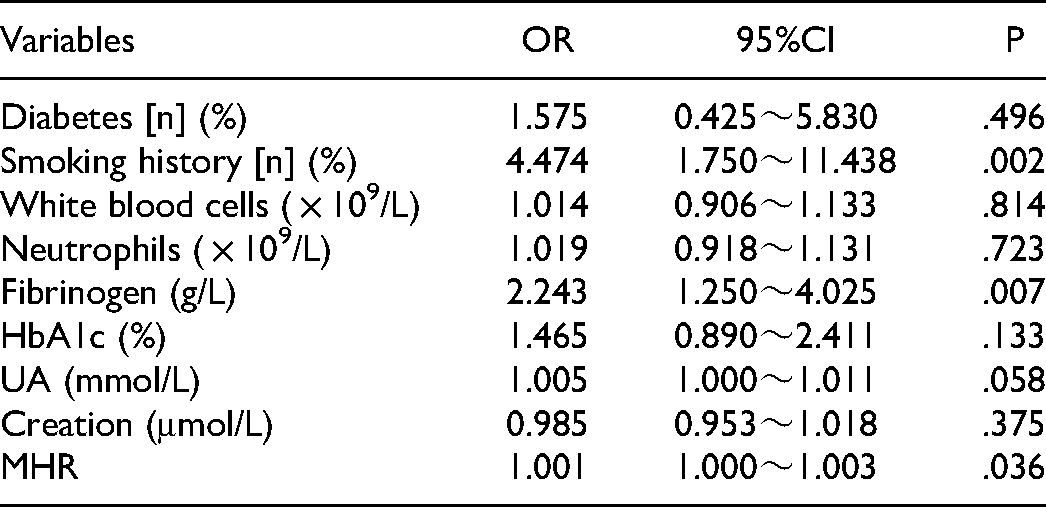
Parameters with P < .05 in the univariable analysis and parameters demonstrated to be associated with the development of ISR in our studies were included in the multivariable Cox analysis. As shown in Table 3, the results indicated that a smoking history, fibrinogen, and higher MHR were independent risk factors for ISR in the multivariate Cox regression analysis (P < .05).
Risk factors of premature coronary heart disease analyzed by Logistic regression analysis.
ROC curves were used to explore the relationship between MHR and ISR. The ROC curve was used to assess the value of MHR in predicting the occurrence of ISR in patients with PCHD. The results showed that the area under the ROC curve (AUC) was 0.750 (95% confidence interval, 0.695-0.820; P < .001), the cutoff value was 546.88, and the specificity and sensitivity were 65.2% and 78%. In addition, the AUC of monocytes was 0.725 (95% confidence interval, 0.638-0.794; P < .001), the cutoff value was 590.00, and the specificity and sensitivity were 77.1% and 60.0%.
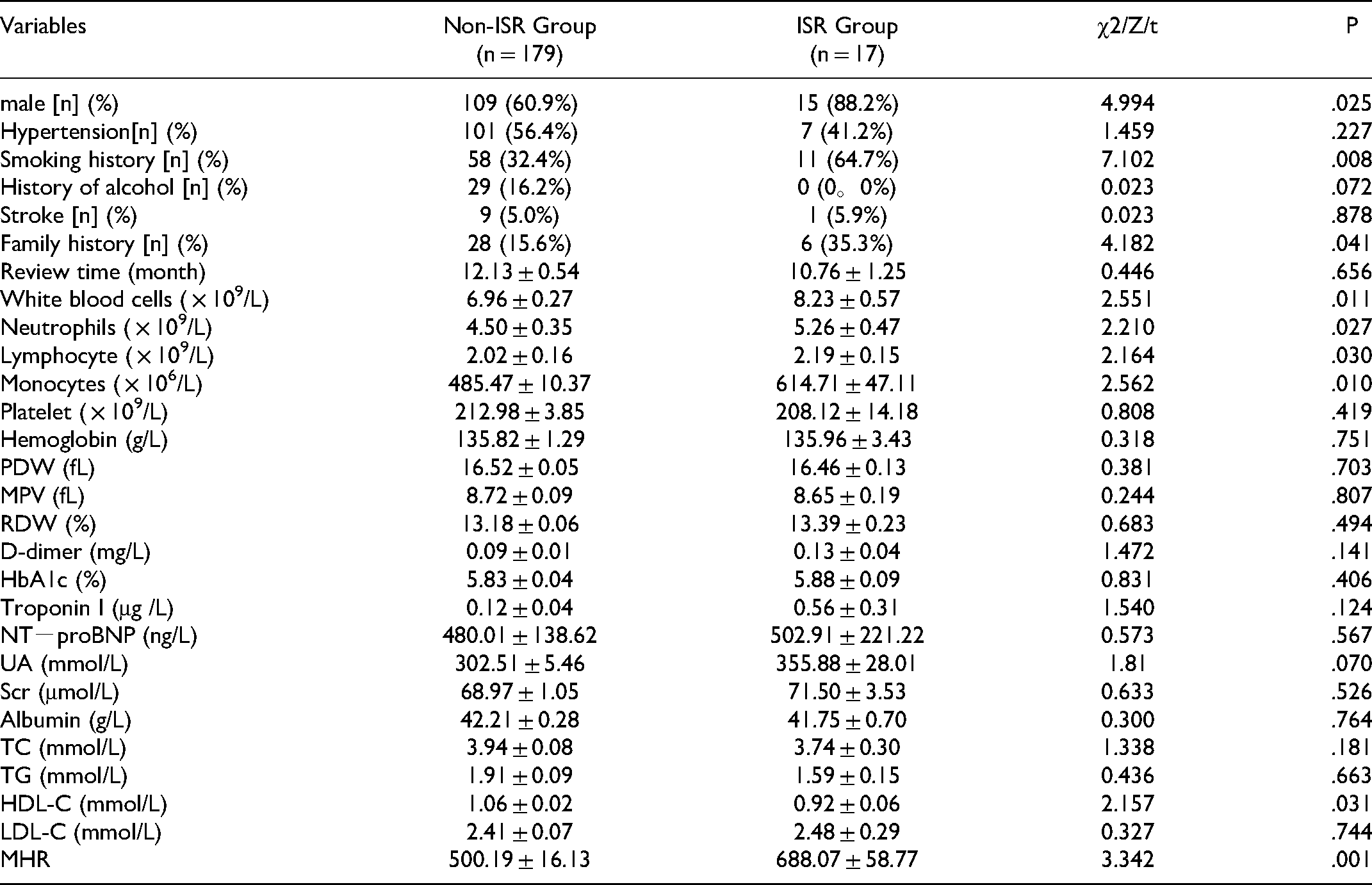
As shown in Table 4, we found that a number of variables were not statistically different between the two groups, including age, high blood pressure, a history of drinking, brain natriuretic peptide level, troponin level, hemoglobin concentration, platelet count, D-dimer level, albumin level, total cholesterol level, and triglycerides. We also found that the proportion of patients with diabetes, proportion of patients with a smoking history, and proportion of male patients; counts of white blood cells, neutrophils, lymphocytes, and monocytes; HDL-C level; and MHR in the ISR group were higher than those in the non-ISR group, and the differences were statistically significant (P < .05).
Baseline characteristics of non-DM patients [n (%), `x ± s].
As shown in Table 5, there were no statistically significant differences in the number of target vessels, location or number of stents, stent length, and stent diameter between the two groups (P > .05).
Coronary angiography and PCI in the two groups with non-DM [case (%), `x ± s].

Parameters with P < .05 in the univariable analysis and parameters demonstrated to be associated with the development of ISR in our studies were included in the multivariable Cox analysis. As shown in Table 6, the results indicated that a smoking history and higher MHR were independent risk factors for ISR in the multivariate Cox regression analysis (P < .05).
Logistic regression analysis of risk factors for non-diabetic premature coronary heart disease.

ROC curves were used to explore the relationship between MHR and ISR. A ROC curve was also used to assess the value of MHR in predicting the occurrence of ISR in non-diabetic patients with PCHD. The results showed that the AUC was 0.745 (95% confidence interval, 0.645-0.846; P < .001), the cutoff value was 520.25, and the specificity and sensitivity were 60.3% and 82.4%.
Discussion
PCI is a common interventional operation for the treatment of CHD. ISR is a difficult challenge to overcome in the treatment of CHD by PCI, and it is also a hotspot area of current research. Some studies have pointed out that inflammation, vascular endothelial injury causing vascular intimal hyperplasia and remodeling, and smooth muscle cell migration and proliferation can all lead to ISR. 8 We retrospectively reviewed the clinical data, laboratory indicators, CAG parameters, and stent features of PCHD patients after PCI. In this retrospective investigation, patients with PCHD were divided into an ISR group and a non-ISR group based on the reexamination results. A total of 257 patients were enrolled, including 30 (11.7%) who developed ISR during follow-up. We found that the proportion of patients with diabetes, proportion of patients with a smoking history, proportion of male patients, hemoglobin A1c level, white blood cell count, neutrophil count, fibrinogen level, UA level, creatinine level, monocyte count, HDL-C level, and MHR in the ISR group were higher than those in the non-ISR group. Further logistic regression analysis found that a smoking history, and higher MHR were independent risk factors for ISR.
MHR combines two interactable risk factors and protection factors, as a new type of inflammatory marker, and has aroused the attention of scholars. Kanbay et al. 9 found that an increase in MHR in patients with chronic renal insufficiency is related to the occurrence of cardiac adverse events, and Canpolat et al. 10 determined that MHR can be used as a predictor of atrial fibrillation recurrence. The mechanism of ISR may be that vascular endothelial cells express leukocyte adhesion molecules when they are damaged, and monocytes can adhere to abnormal vascular endothelium, thereby participating in the formation of atherosclerotic plaques. 11 Monocytes are the main source of pro-inflammatory factors and pro-oxidant factors. Monocytes in the blood circulation are also a source of tissue macrophages and foam cells. Macrophages generate foam cells through scavenger receptors and oxidized LDL-C, 12 releasing more inflammatory factors and pro-oxidant factors to the stent site, thereby interacting with platelets and smooth muscle cells, eventually leading to inflammation and ISR. HDL can promote an efflux of cholesterol in cells, especially in macrophages, thereby supporting the reverse transport of cholesterol in the arterial wall to the liver and inhibiting the process of atherosclerosis. 13 HDL-C also has anti-inflammatory and antioxidant effects. By preventing LDL-C oxidation and monocytes from entering the blood vessel walls, the endothelium or blood vessels are protected from inflammation and oxidative stress. HDL-C can also directly act on monocytes to inhibit the occurrence of inflammation. 14 The abovementioned mechanism reflects the inflammatory effect of monocytes in CHD and the anti-inflammatory and antioxidant effects of HDL-C. Therefore, combining the inflammatory effects of monocytes and the anti-inflammatory and anti-atherosclerotic effects of HDL-C, MHR can be used as a new predictor of restenosis in PCHD patients after PCI. Previous studies have found that elevated MHR values correlate with the occurrence of ISR in patients with stable or unstable angina pectoris after PCI. Tok D, Ucar research found that elevated MHR levels are related to the occurrence of ISR in patients with stable and unstable angina pectoris after PCI.15,16 It is consistent with the research results of us. To demonstrate the predictive power of MHR for ISR in patients with PCHD, we performed a subgroup analysis in the non-diabetic population. We found that MHR remains an independent risk factor for ISR in patients with PCHD. This is consistent with our findings.
We found that counts of white blood cells, neutrophils, and monocytes in the ISR group were higher than those in the non-ISR group. Coronary atherosclerosis is the most important pathophysiological basis of CHD. It is an inflammatory process that occurs in combination with an age increase, intimal thickening, lipid streaks, calcification nodules, and hardening plaque formation. 17 Previous studies have found that many inflammatory markers, including the ratio of lymphocytes to monocytes, ratio of neutrophils to lymphocytes, and C-reactive protein level, are related to the occurrence of ISR.18,19 Neutrophils can cause plaque rupture by producing superoxide free radicals, arachidonic acid, proteolytic enzymes, and other metabolites and can aggregate with platelets to block blood vessels and cause myocardial ischemia and infarction. 20 Vascular endothelial cells express leukocyte adhesion molecules when they are damaged, and monocytes can adhere to abnormal vascular endothelium, thereby participating in the formation of atherosclerotic plaques. 11 Multivariate logistic regression analysis was further performed to evaluate the significance of independent inflammatory indicators for the diagnosis of ISR in PCHD, and the results suggested that neutrophils and monocytes could not be independent risk factors for ISR in PCHD, which may be due to the interference of multiple factors in inflammatory indicators.
In this study, we also found that the levels of UA and serum creatinine in the ISR group were higher than those in the non-ISR group, suggesting that both serum creatinine and UA may be correlated with the occurrence of PCHD. UA has a pro-inflammatory effect and is positively correlated with levels of tumor necrosis factor and interleukin-6. It can also promote the secretion of C-reactive protein, which is vulnerable to the persistence of inflammatory stimuli in plaque, which leads to cell proliferation. Finally, UA can stimulate the proliferation of vascular smooth muscle cells. 21 Creatinine is considered to be one of the indicators capable of reflecting kidney function. Research by Okada et al. 22 found that serum creatinine is very closely linked to ISR in patients with CHD. Specifically, their study found that arteriosclerotic changes (eg, endothelial damage), which are associated with glomerular damage, may lead to stent malexpansion and/or malapposition and induce stent restenosis. Numasawa et al. found that patients with high levels of creatinine may have a hypercoagulable condition, which can increase the thrombotic risk. Moreover, activation of sympathetic nerves and the renin-angiotensin-aldosterone system, chronic inflammation oxidative stress, and endothelial dysfunction may also be associated with high levels of creatinine. 23 Multivariate logistic regression analysis showed that serum creatinine and UA are not independent risk factors for ISR in PCHD. These findings may be attributable to the patients we selected, and we will include more patients in the future to improve our research.
We also found that the level of fibrinogen in the ISR group was higher than that in the non-ISR group. Multivariate logistic regression analysis showed that fibrinogen was an independent risk factor for in-stent restenosis in patients with PCHD. Fibrinogen is the precursor of fibrin and is related to the inflammatory and thrombosis processes. Fibrinogen and its metabolites may stimulate endothelial cell deterioration and tissue disorders, increase the release of growth factors derived from endothelial cells, and cause endothelial cell dysfunction. In addition, fibrinogen may stimulate the growth of smooth muscle cells, leading to restenosis in the vascular stent. 24
The predictive value of MHR for ISR in patients with PCHD was further evaluated by ROC curve analysis. We found that MHR has a certain predictive value for ISR in patients with PCHD, and the predictive value of MHR for ISR in patients with PCHD is higher than the predictive value of monocytes or HDL-C alone.
Limitations
There are some limitations to this study. First, this study was a single-center, retrospective investigation with a small sample. Second, for the evaluation of ISR, we should have used more precise quantitative measurement methods, such as intravascular ultrasound or optical coherence tomography. Third, we measured MHR only at baseline; serial MHR changes were not assessed. Fourth, follow-up CAG was conducted when ischemic symptoms were suspected, and the rate of ISR might be underestimated in clinical practice as a result, so a prospective study is needed.
Conclusion
MHR has a good correlation with the occurrence of ISR after stent implantation in patients with PCHD and has a certain predictive value for the occurrence of ISR. Going forward, high-risk ISR patients may be screened using MHR, and early clinical interventions should be carried out to avoid ISR and serious cardiovascular events, enhance the efficacy of PCI, and improve the prognosis of patients.
Footnotes
Acknowledgments
The authors are grateful to members of the Department of Cardiology at the First Affiliated Hospital of Zhengzhou University for their help and expertize in conducting this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Authors’ Contributions
According to the definition given by the International Committee of Medical Journal Editors, the authors listed above qualify for authorship by making one or more of the substantial contributions to the intellectual content of the following:
(I)Conception and design:Bo-Wen Chen, Hai-Long Tao. (II) Provision of study materials or patients:All authors. (III) Collection and assembly of data: Bo-Wen Chen, Jia-Jing Liu. (IV)Data analysis and interpretation:Bo-Wen Chen, Jun-Hui Xing, Heng-Dao Liu. (V)Manuscript writing:Bo-Wen Chen, Jun-Hui Xing, Heng-Dao Liu, Yu-Zhen Wei, Hai-Long Tao.
All authors read and approved the final manuscript.